 Nicoleta Zenovia Antone1,2
Nicoleta Zenovia Antone1,2 Roxana Pintican1,3,4*Bogdan Fetica1,5*Carmen Lisencu1,3
Roxana Pintican1,3,4*Bogdan Fetica1,5*Carmen Lisencu1,3 Daria Marian4
Daria Marian4 Andrei Roman1,3,4
Andrei Roman1,3,4 Adrian Trifa1,6,7Vlad Gâta1,2Maximilian Muntean1,8Bogdan Pop1,5Catalin Vlad1,8Patriciu Achimaş Cadariu1,2,8
Adrian Trifa1,6,7Vlad Gâta1,2Maximilian Muntean1,8Bogdan Pop1,5Catalin Vlad1,8Patriciu Achimaş Cadariu1,2,8- 1Breast Cancer Center, Prof. Dr Ion Chiricuta Oncology Institute, Cluj-Napoca, Romania
- 2Department of Oncological Surgery and Oncological Gynecology, “Iuliu Hatieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania
- 3Department of Radiology, Prof. Dr Ion Chiricuta Oncology Institute, Cluj-Napoca, Romania
- 4Department of Radiology, “Iuliu Hatieganu” University of Medicine and Pharmacy, Cluj-Napoca, Romania
- 5Department of Pathology, Prof. Dr Ion Chiricuta Oncology Institute, Cluj-Napoca, Romania
- 6Discipline of Medical Genetics, Center for Research and Innovation in Personalized Medicine of Respiratory Diseases, “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania
- 7Center of Expertise on Rare Pulmonary Diseases, Clinical Hospital of Infectious Diseases and Pneumophysiology “Dr. Victor Babes”, Timisoara, Romania
- 8Department of Surgery, Prof. Dr Ion Chiricuta Oncology Institute, Cluj-Napoca, Romania
Background: Accurate axillary lymph node assessment is critical in breast cancer staging. This study aimed to evaluate whether ultrasound (US)-based measurements, particularly cortical thickness and comparison with contralateral lymph nodes, could improve diagnostic accuracy in detecting axillary metastasis.
Methods: In this prospective study, 110 breast cancer patients underwent bilateral axillary US. Ipsilateral and contralateral lymph nodes were assessed for shape, size, cortical characteristics, and hilum preservation. Quantitative features were compared between metastatic and non-metastatic nodes. Diagnostic accuracy was evaluated using ROC analysis, and various cut-off values were tested.
Results: Metastatic nodes showed significantly increased cortical thickness (median 7.5 mm vs. 2.1 mm, p<0.001), larger short axes, and irregular shapes. The cortical thickness of ipsilateral lymph nodes had an AUC of 0.967 with a 3.4 mm cut-off yielding 97.7% sensitivity and 89.1% specificity. Comparing ipsilateral and contralateral cortical thickness revealed a 2.05 mm difference as optimal (AUC 0.926, 86% sensitivity, 89.1% specificity). US-based assessment outperformed traditional imaging in accuracy (92.66% vs. 82.73%).
Conclusions: Quantitative US assessment of axillary lymph nodes, especially cortical thickness and bilateral comparisons, enhances diagnostic accuracy in breast cancer. Integrating these measures may reduce unnecessary biopsies and improve staging efficiency.
1 Introduction
Survival outcomes in breast cancer are influenced by the extent of axillary lymph node involvement, which serves as a prognostic factor and directly influences treatment planning. Patients with node-negative breast cancer generally have better long-term survival, while increasing numbers of metastatic axillary nodes are associated with higher rates of recurrence and worse overall survival (1, 2). Accurate axillary staging is therefore essential to define optimal surgical and systemic treatment strategies and avoid under- or overtreatment. In the context of the evolving de-escalation of axillary surgery in clinically node-negative patients, the need for improved imaging techniques to reliably predict nodal status is increasingly recognized (3–5).
Various imaging modalities have been investigated to improve preoperative axillary staging. Ultrasound (US) is widely used due to its accessibility, affordability, and lack of ionizing radiation, with studies reporting sensitivities ranging from 49% to 64% and specificities between 78% and 92%, depending on the criteria used to define suspicious nodes (6, 7). Contrast-enhanced ultrasound (CEUS) has shown promise in enhancing the detection of subtle neovascularity in metastatic nodes, with sensitivity exceeding 80% in some cohorts, though its use remains limited to specialized centers (8, 9). Magnetic resonance imaging (MRI), particularly diffusion-weighted imaging, offers excellent soft-tissue contrast, with reported sensitivity between 67% and 84% and specificity up to 92%, but its routine application in axillary staging is limited by cost, availability, and variability in diagnostic performance (10–12). PET-CT offers high specificity for detecting nodal metastases, particularly in patients with more advanced disease, but its spatial resolution limits detection of small metastases (less than 1 cm), and its use in early-stage breast cancer remains controversial (13, 14).
Despite the range of available imaging options, none consistently achieve the accuracy required to fully replace sentinel lymph node biopsy (SLNB) in early-stage breast cancer. Moreover, imaging studies typically focus on the ipsilateral axilla, with little attention given to the potential diagnostic value of comparing nodes bilaterally within the same patient. Asymmetry between ipsilateral and contralateral nodes in cortical thickness, shape, and hilum preservation could provide important clues to metastatic involvement. By integrating comparative ultrasound analysis into the axillary evaluation process, we hypothesize that diagnostic accuracy could be improved, leading to better patient selection for biopsy and potentially reducing unnecessary invasive procedures.
Thus, the aim of our study is to evaluate the diagnostic and prognostic value of comparative US analysis of ipsilateral and contralateral axillary lymph nodes in breast cancer patients.
2 Methods
This prospective, unicentric study included consecutive breast cancer (BC) patients evaluated at our institution between October 2022 and October 2024. The study was IRB approved and all patients signed a written consent. Inclusion criteria comprised patients with histologically confirmed BC, without previous axillary surgery, who underwent bilateral axillary US assessment, prior to any treatment. We excluded patients with bilateral breast cancer, and patients with concurrent systemic diseases such as lymphoma, leukemia or autoimmune diseases (eg rheumatoid arthritis), as they may potentially affect the imaging appearance of the lymph nodes.
All US were performed using 2 US vendors (Samsung RS80 and GE 2022) with high-frequency linear transducers (7–12 MHz) by dedicated breast radiologists with at least 2 years of breast imaging experience. Lymph nodes were assessed for shape (oval, round, irregular), long and short axis, cortical thickness (value, focal or diffuse, homogeneous or heterogeneous with hyperechoic or cystic areas), presence of hyperechoic halo, and fatty hilum preservation. We considered suspicious lymph nodes, round, without fatty hilum, and diffuse or focal cortical thickening of 3mm. All suspicious nodes were US-guided biopsied using core needle biopsy with an automated 14G needle device, and confirmed on pathology. For the contralateral assessment, we selected the lymph node with the greatest cortical thickness for comparison, applying the same set of suspicious criteria as on the ipsilateral side All patients underwent surgery for the primary tumor, with concomitant sentinel lymph node biopsy (SNLB) or axillary dissection (ALND). Pathology data for the breast tumor included histologic type (invasive ductal, invasive lobular, etc.), tumor grade (Nottingham system), hormone receptor status (ER-positive if ≥1% nuclear staining; PR-positive if ≥1% nuclear staining), and HER2 status (positive if IHC 3+ or FISH amplified).
All the data from the study was analyzed using IBM SPSS Statistics 25 and illustrated using Microsoft Office Excel/Word 2021. Quantitative variables were tested for normal distribution using the Shapiro-Wilk Test and were expressed as means with standard deviations or medians with interquartile ranges. Independent quantitative variables with a non-parametric distribution were compared between groups using the Mann-Whitney U Test, while related samples were analyzed using Wilcoxon’s Test. Qualitative independent variables were presented as counts or percentages and tested between groups using Fisher’s Exact Test or Pearson’s Chi-Square Test. To further detail contingency table results, Z-tests with Bonferroni correction were applied, and McNemar’s Test was used for qualitative variables in related samples, with Bonferroni correction when necessary. ROC curves were employed to determine diagnostic performances and cut-offs for lymph nodes dimensions in predicting metastases, with performance assessed using AUC values and 95% confidence intervals. Optimal cut-offs were selected based on the highest Youden index, and corresponding sensitivities and specificities were calculated. Univariable and multivariable logistic regression models were used to estimate the effect of predictive variables on the presence of lymph nodes metastases, with effects quantified through odds ratios and 95% confidence intervals. These models were evaluated for significance, goodness-of-fit, and multicollinearity, with all statistical tests using a significance threshold of α=0.05.
3 Results
3.1 Study population
A total of 110 breast cancer patients were included, with a median age of 57 years (IQR: 49-65). Of these, 43 (39.1%) had histologically confirmed axillary lymph node metastases. Invasive ductal carcinoma of no special type (IDC-NST) was the most common histologic subtype, found in 77.3% of cases. Tumors were predominantly hormone receptor-positive (ER-positive in 85.8%, PR-positive in 73.6%), while HER2 positivity was detected in 16.8% of cases. Median tumor size was 22 mm (IQR 15–29 mm), and high proliferation (Ki-67% ≥20%) was present in 76.2% of tumors (Table 1).
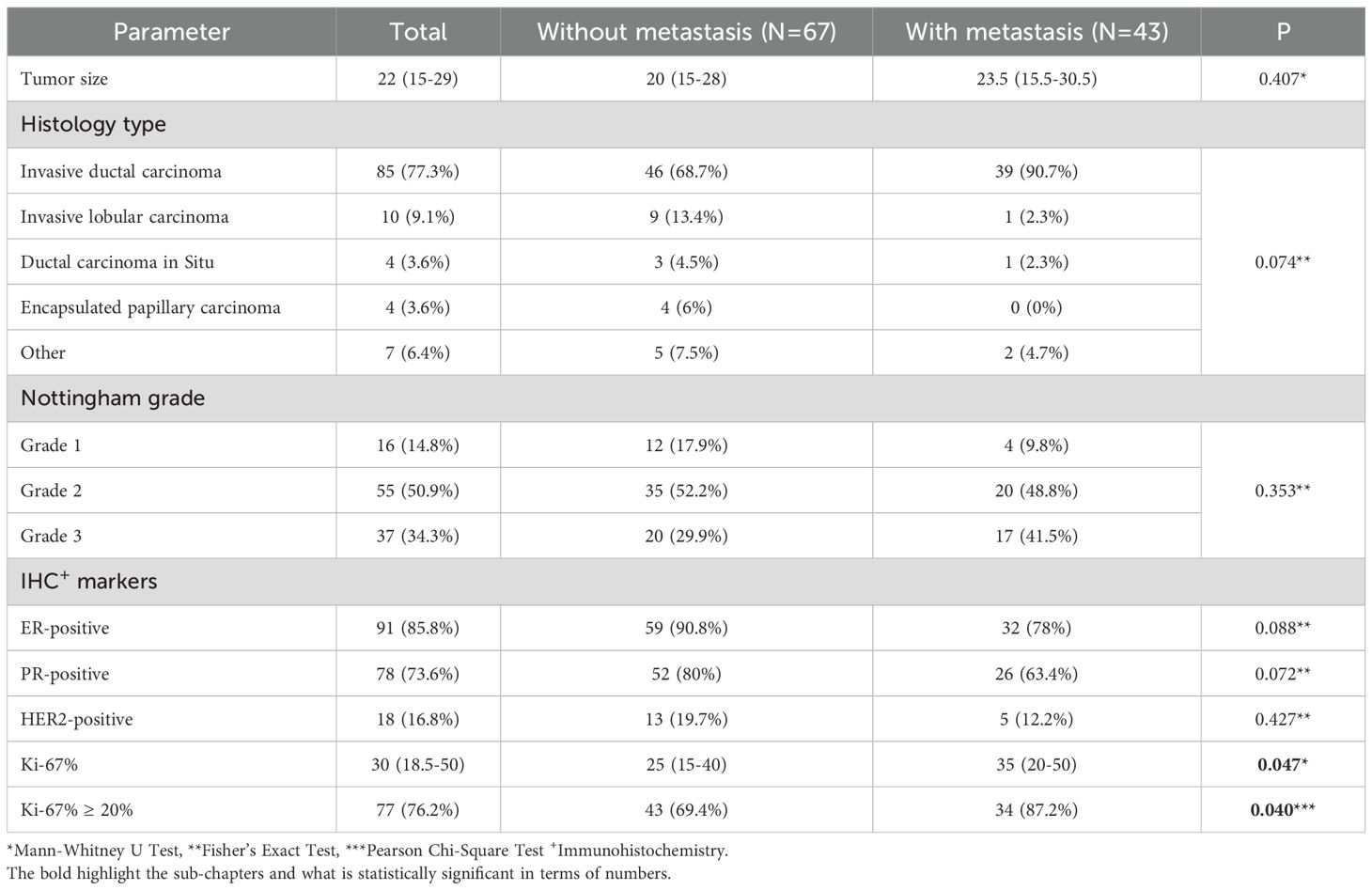
Table 1. Clinical and pathological characteristics of the study population.
3.2 Ipsilateral axillary assessment
Metastatic lymph nodes were found more frequent with irregular shape (20.9% vs. 1.5%, p<0.001), and longer short axis (median 10 mm vs. 6.55 mm, p<0.001). Preservation of the fatty hilum was seen in 97% of non-metastatic nodes and only in 58.1% of metastatic cases (p<0.001). Patients with lymph node metastases had significantly thicker ipsilateral lymph nodes, with a median cortical thickness of 7.5 mm (IQR 4.8–12 mm) compared to 2.1 mm (IQR 1.6-2.82 mm) in non-metastatic cases (p<0.001) (Table 2).
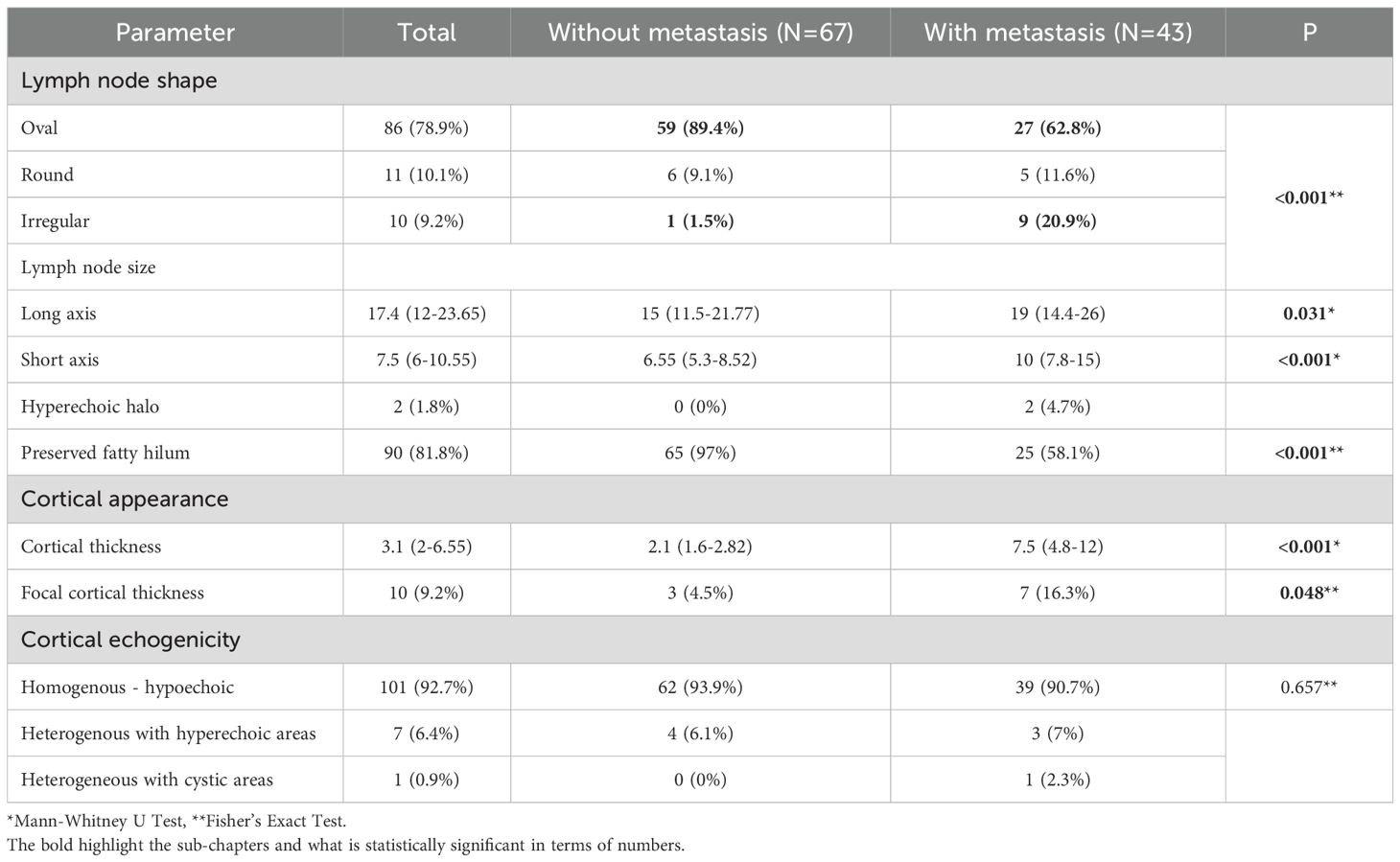
Table 2. US characteristics of the ipsilateral lymph nodes proved to be metastatic.
3.3 Ipsilateral compared to contralateral axillary assessment
The US showed the majority of the contralateral nodes with oval shape (97.2%), diffuse (98.1%) and homogenous - hypoechoic (97.1%) cortical appearance. The median for cortical thickness was 1.3 mm (IQR=1-2), long axis – 12 mm (IQR=9.8-18) and short axis – 6 mm (IQR=5-8.5) (Figure 1).
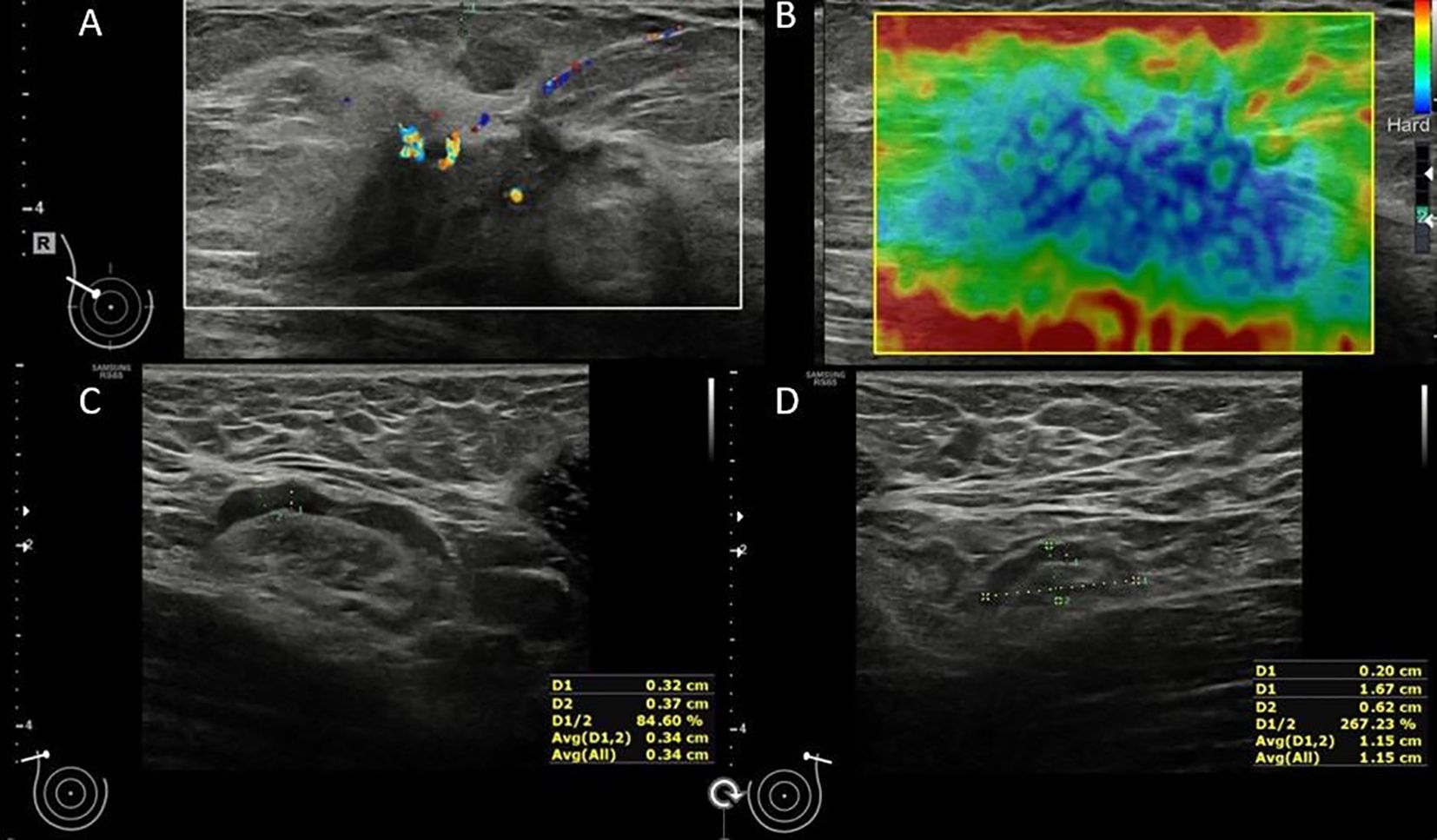
Figure 1. 54 y old patient with right lobular breast cancer: In the upper-outer quadrant of the right breast, there is a hypoechoic mass, with internal vascularity (A) and stiff elastography appearance (B) – HP confirmed breast cancer; The ipsilateral lymph node (C) has preserved fatty hilum and a diffuse cortical thickness up to 3.2mm (HP confirmed metastasis); the contralateral lymph node shows a uniform cortex up to 2mm (D).
In patients with a confirmed axillary metastasis, the ipsilateral and contralateral lymph nodes showed significant morphological differences with larger nodes and thickened cortex in ipsilateral ones, compared to contralateral lymph nodes (all p-value < 0.05). The focal aspect was significantly more frequent in ipsilateral lymph nodeslymph nodes(9.5% vs. 1.9%, p=0.039), while cortical appearance did not differ significantly between ipsilateral and contralateral lymph nodeslymph nodes (Table 3).
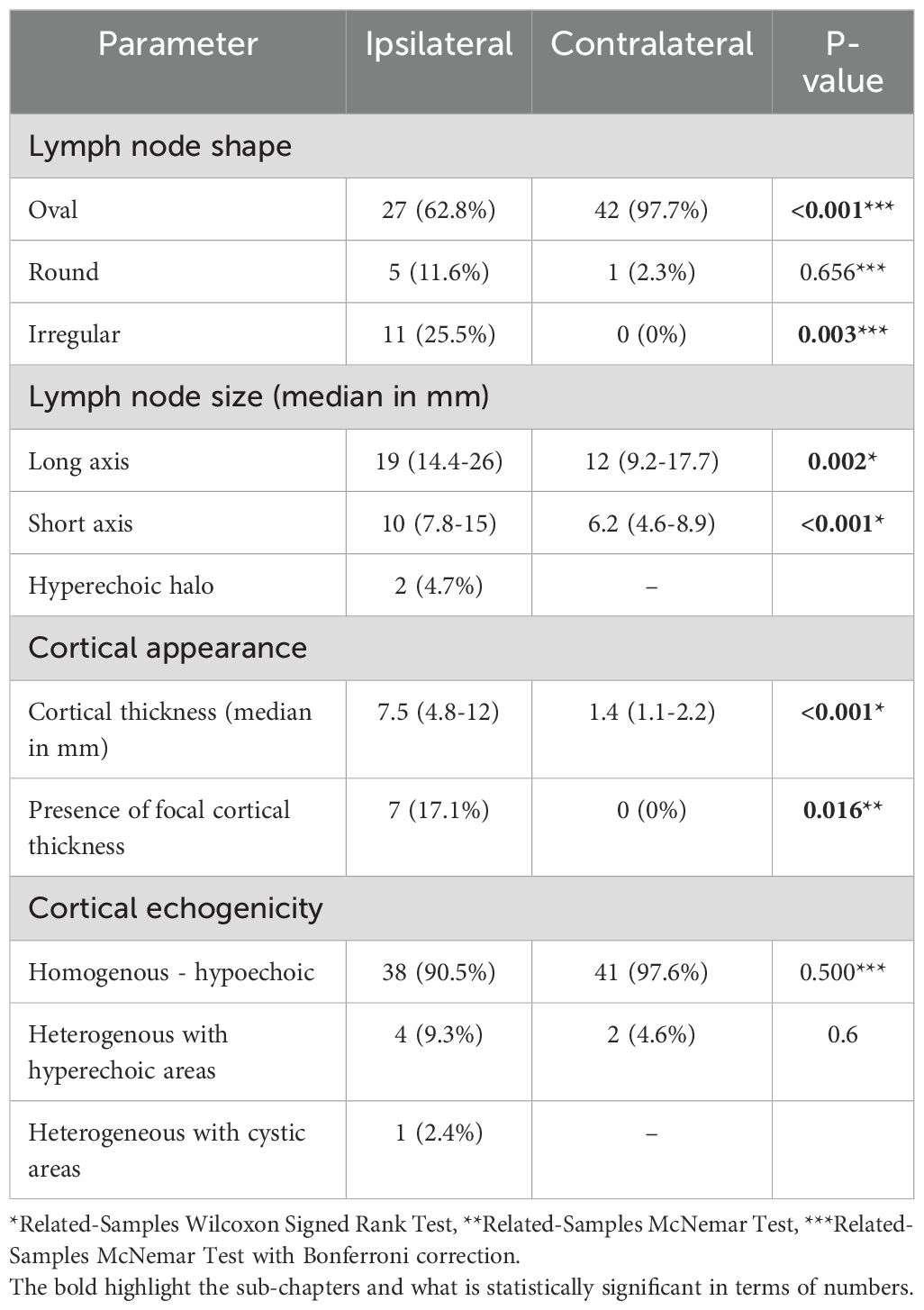
Table 3. Differences of US characteristics between ipsilateral and contralateral axillary lymph nodes for patients with proved axillary metastasis.
The same US features were found to be different in ipsilateral metastatic lymph nodes when compared to the contralateral ones (Figure 2). Patients with differing lymph node shapes between ipsilateral and contralateral sides were significantly more likely to have metastases (39.5% vs. 12.3%, p=0.002). Significant differences were observed in cortical thickness (median=5.9 mm, IQR=3.4–10.7 vs. median=0.7 mm, IQR=0.12–1.37, p<0.001) and short axis (p – value < 0.001) between ipsilateral and contralateral lymph nodes, with greater differences found in patients with metastases compared to those without. A similar trend was noted for the long axis, though it did not reach statistical significance (p=0.077). In contrast, differences in cortical echogenicity (p=1.000) between ipsilateral and contralateral lymph nodes was not statistically associated with the presence of metastases (Table 4).

Figure 2. 64 y old patient with left NST breast cancer; Axillary assessment is showing an ipsilateral abnormal lymph node, with preserved fatty hilum, but with cortical thickness >3mm, that was confirmed as metastasis (A). The contralateral lymph node shows a fatty hilum and uniform cortex up to 1.9mm (B). There was a cortical difference >2mm between the ipsilateral cortical thickness and the contralateral lymph node.
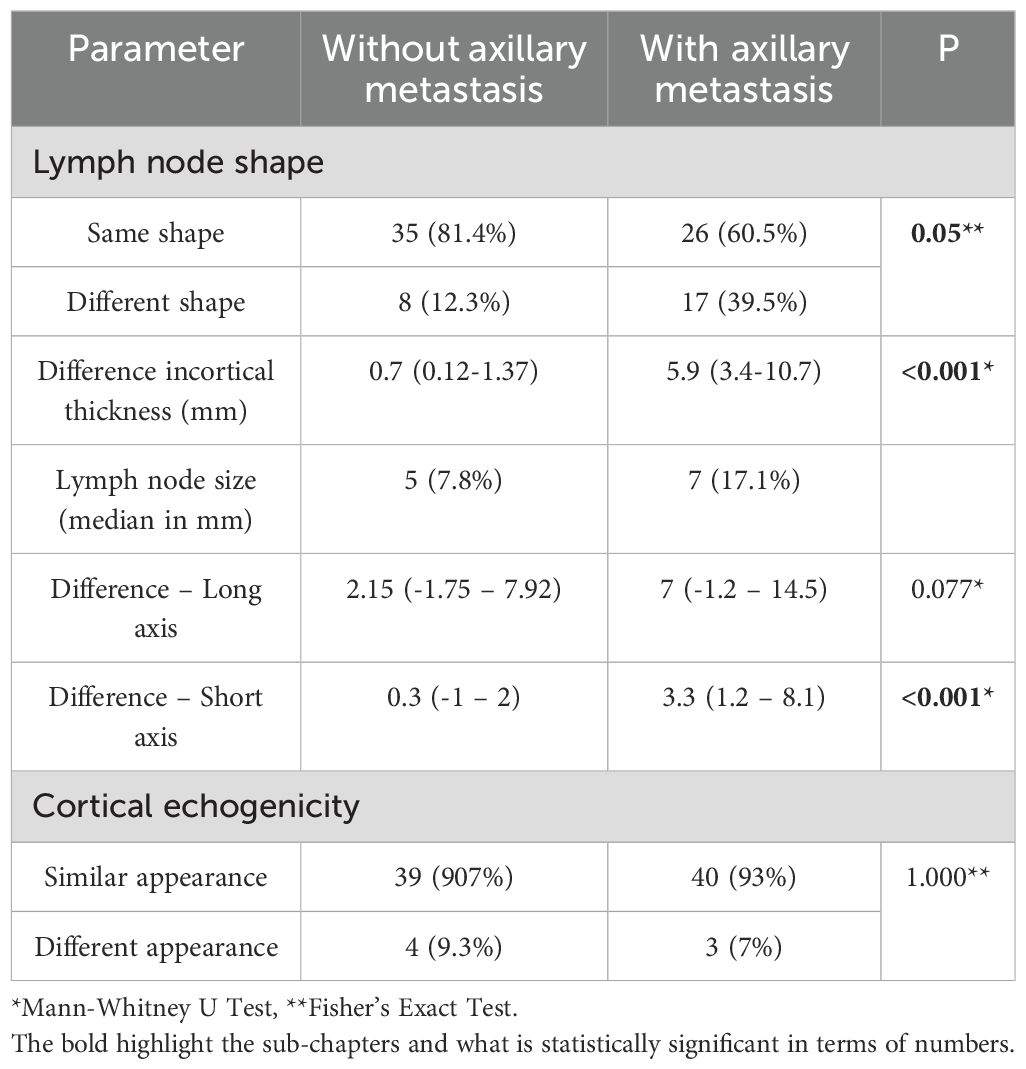
Table 4. Comparison of the differences between ipsilateral and contralateral lymph nodes.
4 Diagnosis and prognosis analysis
The cortical length of ipsilateral lymph nodes showed an AUC of 0.967 (95% CI: 0.937–0.998, p<0.001). A cut-off value of 3.4 mm yielded a sensitivity of 97.7% and specificity of 89.1%, while a cut-off of 4.55 mm resulted in a sensitivity of 76.7% and specificity of 95.3%. The difference in cortical length between ipsilateral and contralateral lymph nodes had an AUC of 0.926 (95% CI: 0.870–0.983, p<0.001), with a 2.05 mm cut-off providing 86% sensitivity and 89.1% specificity. At a 3 mm cut-off, the sensitivity was 79.1% and specificity 95.3%, while a 3.95 mm cut-off resulted in 69.8% sensitivity and 96.9% specificity.
The short axis of ipsilateral lymph nodes had an AUC of 0.776 (95% CI: 0.686–0.865, p<0.001), with a 7.7 mm cut-off yielding a sensitivity of 76.7% and specificity of 70.3%. The difference in short axis between ipsilateral and contralateral lymph nodes had an AUC of 0.729 (95% CI: 0.625–0.833, p<0.001), with a 2.05 mm cut-off providing 67.4% sensitivity and 76.6% specificity. The long axis of ipsilateral lymph nodes had an AUC of 0.623 (95% CI: 0.514–0.732, p=0.032), with a 15.35 mm cut-off yielding 74.4% sensitivity and 51.6% specificity (Table 5, Figure 3).
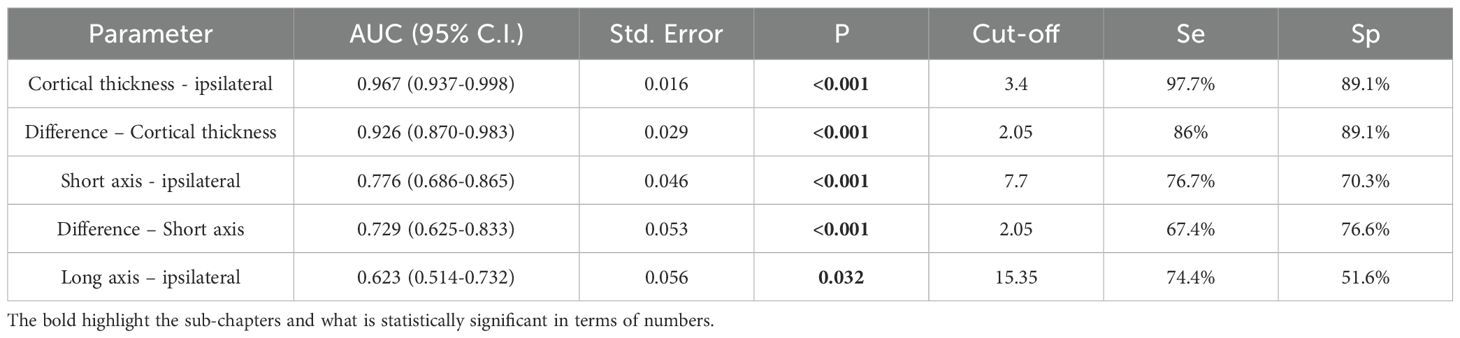
Table 5. ROC curves analyses used in estimation of lymph node metastases prediction.
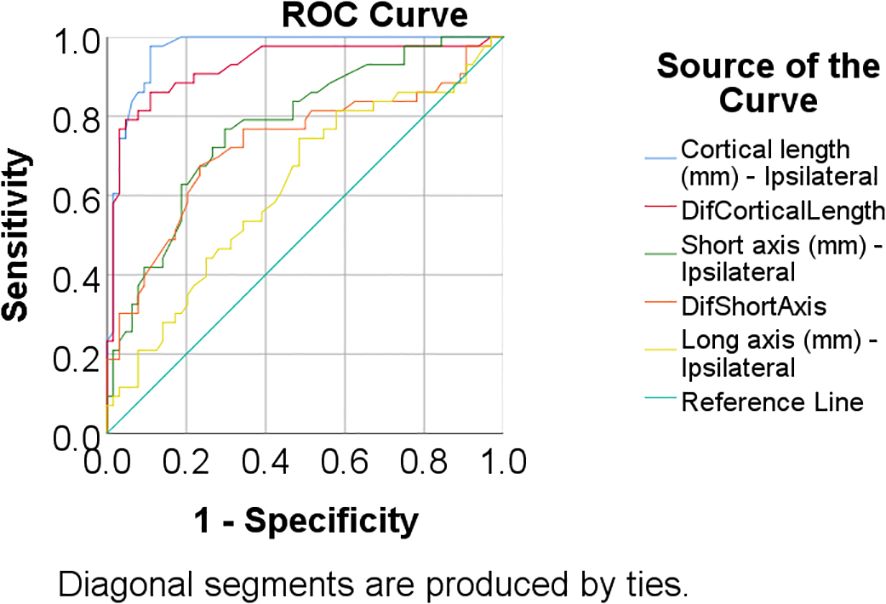
Figure 3. ROC curve used in the prediction of lymph node metastases based on US features.
Ultrasound correctly classified 37 metastatic lymph nodes and 54 benign lymph nodes. Furthermore, on US, there were 13 cases incorrectly labeled as metastatic (false positives) and 6 metastatic lymph nodes missed (false negatives). Overall, this resulted in a sensitivity of 86.05%, specificity of 80.6%, positive predictive value of 74%, negative predictive value of 90%, and an accuracy of 82.73% for detecting axillary metastasis.
The 3.4 mm cortical length cut-off for ipsilateral lymph nodeslymph nodes identified 59 true positives, 1 false positive, 7 false negatives, and 42 true negatives, with a sensitivity of 97.67%, specificity of 89.39%, positive predictive value of 85.71%, negative predictive value of 98.33%, and overall accuracy of 92.66%. The 2.05 mm cortical length difference cut-off identified 57 true positives, 6 false positives, 7 false negatives, and 36 true negatives, with a sensitivity of 85.71%, specificity of 89.06%, positive predictive value of 83.72%, negative predictive value of 90.48%, and overall accuracy of 87.74%. Forty-four patients (40%) underwent lymph nodeslymph nodes biopsy, with 11 (25%) testing negative for metastases. Among these, 6 patients (54.5%) had an ipsilateral cortical length < 3.4 mm or a cortical length difference < 2 mm.
5 Discussion
The results of this study reinforce axillary US as a key imaging modality for the prediction of lymph node metastasis in breast cancer patients. Comparative analysis between ipsilateral and contralateral axillary lymph nodes demonstrated significant morphological differences, with metastatic lymph nodes exhibiting larger dimensions, irregular shape, and increased cortical thickness. The cortical thickness of ipsilateral lymph nodes emerged as a strong predictor, with an AUC of 0.967 and a cut-off of 3.4 mm yielding a sensitivity of 97.7% and specificity of 89.1%. Additionally, the difference in cortical thickness between ipsilateral and contralateral nodes also demonstrated high predictive accuracy, with an AUC of 0.926 and an optimal cut-off of 2.05 mm providing 86% sensitivity and 89.1% specificity. These findings highlight the potential of using quantitative US measurements to refine lymph nodes assessment and improve diagnostic performance.
US remains the most widely used imaging modality for axillary staging in newly diagnosed breast cancer due to its accessibility, low cost, and ability to assess nodal morphology in real time. Multiple studies have shown that axillary US provides moderate to high diagnostic performance, with reported sensitivities of 60–80% and specificities of 80–95% (15–18). Recent advances in US technology have improved diagnostic accuracy in the contemporary literature (19), although this improvement has not been consistently observed in patients receiving neoadjuvant therapy (20). Despite the development and testing of several classification systems, substantial variability persists across countries and institutions (21). The NODE-RADS system has been introduced to enable a structured and harmonized assessment of lymph nodes on both US and MRI, and recent work has demonstrated comparable AUC performance in IDC and ILC, albeit with lower sensitivity in ILC (22–24). However, the system lacks validated biopsy thresholds, and its adoption in routine practice remains limited, as clinicians continue to favor simpler and more practical criteria such as cortical thickness cut-offs.
In our institution, a cortical thickness threshold of 3 mm is routinely applied, and the results of the present study are in line with previously published reports, yielding a sensitivity of 86.05%, specificity of 80.6%, positive predictive value of 74%, negative predictive value of 90%, and an overall accuracy of 82.73% for the identification of axillary metastases. When the cut-off for ipsilateral cortical thickness was increased to 3.4 mm, the overall accuracy improved to 92.66%, with a sensitivity of 97.67% and specificity of 89.39%. Likewise, applying a 2.05 mm inter-side cortical thickness difference cut-off resulted in an accuracy of 87.74%, with a sensitivity of 85.71% and specificity of 89.06%. These findings suggest that incorporation of quantitative criteria into routine axillary US assessment may improve diagnostic reliability and reduce both false-positive and false-negative classifications.
Compared with clinical examination alone, US provides substantially higher sensitivity for detecting axillary lymph node metastases (25, 26). However, when compared with advanced imaging such as MRI and PET/CT, the results are generally comparable. The existing literature on axillary imaging has focused almost exclusively on ipsilateral lymph node assessment (27–30), while reports addressing contralateral lymph nodes are scarce. When contralateral evaluation is mentioned, it is typically based on pathological examination and most often in the context of suspected or confirmed metastases (30, 31). More recently, interest has increased in the prognostic and therapeutic implications of synchronous contralateral axillary lymph node metastasis (CAM). Several studies have reported that patients with synchronous CAM demonstrate more favorable overall survival than those with other sites of distant metastasis, suggesting that CAM may represent a biologically distinct subgroup eligible for treatment with curative rather than palliative intent (30). In inflammatory breast cancer, CAM has been observed in approximately 8.3% of cases at presentation, with ultrasound identified as the most effective imaging modality for its detection. On this basis, recent authors recommend incorporating contralateral axillary US into the initial staging protocol for patients with inflammatory breast cancer (31).
To our knowledge, no prior study has systematically evaluated the contralateral axilla on imaging at initial breast cancer diagnosis. Our study addresses this significant gap by prospectively assessing the diagnostic appearance of contralateral axillary lymph nodes using US in newly diagnosed breast cancer patients. This approach could provide early insight into potential bilateral disease or atypical lymphatic drainage patterns and has the potential to inform staging and treatment planning in a way not previously explored in the imaging literature. US correctly classified lymph nodes as benign or malignant, with.
Our results highlight the potential to reduce unnecessary biopsies through the integration of bilateral cortical thickness assessments. In our cohort, a cortical thickness below 3.4 mm and a contralateral difference of only ~2 mm were not indicative of metastatic disease. These findings suggest that bilateral comparison primarily serves to reduce overdiagnosis in cases with mild and symmetrical cortical thickening, rather than increasing the sensitivity. Accordingly, contralateral assessment may help reduce false-positive interpretations and avoid unnecessary biopsies. Among the 44 patients who underwent lymph node biopsy, 11 (25%) had negative results for metastases. Of these, 6 patients (54.5%) had an ipsilateral cortical thickness below 3.4 mm or a cortical thickness difference of less than 2 mm, suggesting that in these cases, a negative biopsy could have been avoided. These findings suggest that incorporating cortical thickness measurements as part of a structured diagnostic workflow may assist in better patient selection for biopsy, thereby reducing the burden of invasive procedures without compromising diagnostic accuracy.
Besides classical imaging modalities, radiomics, artificial intelligence (AI), and machine learning are rapidly emerging as promising tools in breast imaging, including axillary lymph node assessment. Recent studies have shown that AI algorithms can enhance diagnostic accuracy, reduce inter-observer variability, and assist in risk stratification, particularly when integrated with clinical and pathological data (32–34). However, while initial results are encouraging, these technologies are still in early stages for routine axillary evaluation. Their performance is highly dependent on data quality, imaging standardization, and robust training across diverse populations. Thus, although AI and radiomics show strong potential, they are not yet ready to replace expert radiologist assessment in clinical practice, but rather serve as decision-support tools in well-validated workflows.
However, there are a few limitations: the study is unicentric, with a limited number of patients; other imaging modalities were not compared to US (such as breast MRI); future studies should further validate these cut-offs in larger, multi-institutional cohorts to assess their generalizability and clinical utility.
6 Conclusion
Quantitative US-based assessment of axillary lymph nodes, particularly cortical thickness measurements and comparative ipsilateral-contralateral analysis, enhances diagnostic accuracy in detecting metastatic involvement. The integration of objective measurement criteria, such as cortical thickness cut-offs, has the potential to refine patient selection for biopsy and reduce unnecessary invasive procedures. Further validation in larger cohorts is warranted to establish these criteria as standard practice in axillary staging for breast cancer patients.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving humans were approved by The Ethics Committee of Prof Dr. Ion Chiricuta Oncology Institute, Cluj-Napoca, Romania. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
NZ: Conceptualization, Methodology, Validation, Supervision, Project administration, Data curation, Investigation, Writing – review & editing, Formal analysis, Funding acquisition, Writing – original draft, Visualization, Software, Resources. RP: Funding acquisition, Writing – original draft, Formal analysis, Supervision, Writing – review & editing, Data curation, Software, Investigation, Conceptualization, Project administration, Resources, Methodology, Validation, Visualization. BF: Funding acquisition, Writing – review & editing, Software, Formal analysis, Writing – original draft, Resources, Project administration, Supervision, Visualization, Conceptualization, Methodology, Validation, Investigation, Data curation. CL: Software, Investigation, Supervision, Writing – review & editing, Funding acquisition, Conceptualization, Visualization, Formal analysis, Writing – original draft, Validation, Resources, Project administration, Data curation, Methodology. DM: Project administration, Validation, Funding acquisition, Writing – original draft, Formal analysis, Supervision, Visualization, Investigation, Methodology, Data curation, Software, Writing – review & editing, Conceptualization, Resources. AR: Formal analysis, Methodology, Writing – original draft, Visualization, Resources, Data curation, Supervision, Project administration, Investigation, Validation, Writing – review & editing, Conceptualization, Software, Funding acquisition. AT: Validation, Formal analysis, Project administration, Methodology, Supervision, Data curation, Writing – review & editing, Writing – original draft, Conceptualization, Resources, Investigation, Visualization, Software, Funding acquisition. VG: Supervision, Funding acquisition, Writing – review & editing, Conceptualization, Resources, Investigation, Writing – original draft, Project administration, Validation, Formal analysis, Software, Data curation, Visualization, Methodology. MM: Project administration, Validation, Writing – review & editing, Funding acquisition, Supervision, Formal analysis, Data curation, Software, Writing – original draft, Resources, Conceptualization, Investigation, Methodology, Visualization. BP: Writing – original draft, Formal analysis, Supervision, Data curation, Software, Conceptualization, Methodology, Funding acquisition, Resources, Investigation, Visualization, Validation, Project administration, Writing – review & editing. CV: Software, Funding acquisition, Supervision, Conceptualization, Writing – review & editing, Project administration, Resources, Formal analysis, Writing – original draft, Data curation, Methodology, Visualization, Validation, Investigation. PC: Software, Data curation, Writing – original draft, Resources, Visualization, Conceptualization, Investigation, Methodology, Funding acquisition, Validation, Writing – review & editing, Project administration, Formal analysis, Supervision.
Funding
The author(s) declare that financial support was received for the research, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Giuliano AE, Hunt KK, Ballman KV, Beitsch PD, Whitworth PW, Blumencranz PW, et al. Axillary dissection vs no axillary dissection in women with invasive breast cancer and sentinel node metastasis: a randomized clinical trial. JAMA. (2011) 305:569–75. doi: 10.1001/jama.2011.90
2. Galimberti V, Ribeiro Fontana SK, Maisonneuve P, Steccanella F, Vento AR, Intra M, et al. Sentinel node biopsy after neoadjuvant treatment in breast cancer: Five-year follow-up of patients with clinically node-negative or node-positive disease before treatment. Eur J Surg Oncol. (2016) 42:361–8. doi: 10.1016/j.ejso.2015.11.019
3. Gennaro M, Maccauro M, Sigari C, Casalini P, Bedodi L, Conti AR, et al. Selective axillary dissection after axillary reverse mapping to prevent breast-cancer-related lymphoedema. Eur J Surg Oncol. (2013) 39:1341–5. doi: 10.1016/j.ejso.2013.09.022
4. Pilewskie M and Morrow M. Axillary nodal management following neoadjuvant chemotherapy: A review. JAMA Oncol. (2017) 3:549–55. doi: 10.1001/jamaoncol.2016.4163
5. El Hage Chehade H, Headon H, Kasem A, and Mokbel K. Refining the performance of sentinel lymph node biopsy post-neoadjuvant chemotherapy in patients with pathologically proven pre-treatment node-positive breast cancer: an update for clinical practice. Anticancer Res. (2016) 36:1461–71.
6. Houssami N, Ciatto S, Turner RM, Cody HS 3rd, and Macaskill P. Preoperative ultrasound-guided needle biopsy of axillary nodes in invasive breast cancer: meta-analysis of its accuracy and utility in staging the axilla. Ann Surg. (2011) 254:243–51. doi: 10.1097/SLA.0b013e31821f1564
7. Balasubramanian I, Fleming CA, Corrigan MA, Redmond HP, Kerin MJ, and Lowery AJ. Meta-analysis of the diagnostic accuracy of ultrasound-guided fine-needle aspiration and core needle biopsy in diagnosing axillary lymph node metastasis. Br J Surg. (2018) 105:1244–53. doi: 10.1002/bjs.10920
8. Liu X, Wang M, Wang Q, and Zhang H. Diagnostic value of contrast-enhanced ultrasound for sentinel lymph node metastasis in breast cancer: an updated meta-analysis. Breast Cancer Res Treat. (2023) 202:221–31. doi: 10.1007/s10549-023-07063-2
9. Li J, Wang SR, Li QL, Zhu T, Zhu PS, Chen M, et al. Diagnostic value of multiple ultrasound diagnostic techniques for axillary lymph node metastases in breast cancer: A systematic analysis and network meta-analysis. Front Oncol. (2023) 12: 1043185 doi: 10.3389/fonc.2022.1043185
10. Harnan SE, Cooper KL, Meng Y, Ward SE, Fitzgerald P, Papaioannou D, et al. Magnetic resonance for assessment of axillary lymph node status in early breast cancer: a systematic review and meta-analysis. Eur J Surg Oncol. (2011) 37:928–36. doi: 10.1016/j.ejso.2011.07.007
11. Chang JM, Leung JWT, Moy L, Ha SM, and Moon WK. Axillary nodal evaluation in breast cancer: state of the art. Radiology. (2020) 295:500–15. doi: 10.1148/radiol.2020192534
12. Chen M-Y, Wu W-P, Lai H-W, Sae-Lim C, Chen S-T, Chen D-R, et al. Diagnostic accuracy of pre-operative breast magnetic resonance imaging in predicting axillary lymph node metastasis: variations in intrinsic subtypes, and strategy to improve negative predictive value—an analysis of 2473 invasive breast cancer patients. Breast Cancer. (2023) 30:1044–52. doi: 10.1007/s12282-023-01488-9
13. Heusner TA, Kuemmel S, Hahn S, Koeninger A, Otterbach F, Hamami ME, et al. Diagnostic value of full-dose FDG PET/CT for axillary lymph node staging in breast cancer patients. Eur J Nucl Med Mol Imaging. (2009) 36:1543–50. doi: 10.1007/s00259-009-1145-6
14. Kitajima K, Fukushima K, Miyoshi Y, Katsuura T, Igarashi Y, Kawanaka Y, et al. Diagnostic and prognostic value of (18)F-FDG PET/CT for axillary lymph node staging in patients with breast cancer. Jpn J Radiol. (2016) 34:220–8. doi: 10.1007/s11604-015-0515-1
15. Assing MA, Patel BK, Karamsadkar N, Weinfurtner J, Usmani O, Kiluk JV, et al. A comparison of the diagnostic accuracy of magnetic resonance imaging to axillary ultrasound in the detection of axillary nodal metastases in newly diagnosed breast cancer. Breast J. (2017) 23:647–655. doi: 10.1111/tbj.12812
16. Di Micco R, Hartmann S, Banys-Paluchowski M, de Boniface J, Schmidt E, Ditsch N, et al. Diagnostic performance of axillary ultrasound after neoadjuvant chemotherapy in initially node-positive breast cancer patients - Results from the prospective AXSANA registry triaL. Eur J Cancer. (2025) 226:115607. doi: 10.1016/j.ejca.2025
17. Riedel F, Schaefgen B, Sinn HP, Feisst M, Hennigs A, Hug S, et al. Diagnostic accuracy of axillary staging by ultrasound in early breast cancer patients. Eur J Radiol. (2021) 135:109468. doi: 10.1016/j.ejrad.2020
18. Liu Y, Wang Y, Feng S, Xu Z, Yao M, Huang X, et al. Axillary ultrasound after neoadjuvant therapy reduces the false-negative rate of sentinel lymph node biopsy in patients with cytologically node-positive breast cancer. Breast Cancer Res Treat. (2023) 197:515–523. doi: 10.1007/s10549-022-06817-8
19. Pesapane F, Mariano L, Magnoni F, Rotili A, Pupo D, Nicosia L, et al. Future directions in the assessment of axillary lymph nodes in patients with breast cancer. Med (Kaunas). (2023) 59:1544. doi: 10.3390/medicina59091544
20. Brabender D, Ballard A, Kim S, Hovanessian-Larsen L, and Sener SF. Use of ultrasound and MRI to stage the axilla for breast cancer before and after neoadjuvant chemotherapy prior to targeted sentinel lymphadenectomy. Breast Cancer Res Treat. (2024) 206:595–602. doi: 10.1007/s10549-024-07332-8
21. van Nijnatten TJA, Poplack SP, Wijgers RA, Kilburn-Toppin F, Athanasiou A, Chang JM, et al. Differences in axillary ultrasound protocols among prospective de-escalating axillary surgical staging trials in clinically node negative early breast cancer patients. Eur J Radiol. (2024) 181:111775. doi: 10.1016/j.ejrad.2024.111775
22. Lu F, Zhao Y, Wang Z, and Feng N. Diagnostic accuracy of node-RADS for the detection of lymph node invasion: a systematic review and meta-analysis. Eur Radiol. (2025) 35:4429–37. doi: 10.1007/s00330-025-11387-6
23. Pediconi F, Maroncelli R, Pasculli M, Galati F, Moffa G, Marra A, et al. Performance of MRI for standardized lymph nodes assessment in breast cancer: are we ready for Node-RADS? Eur Radiol. (2024) 34:7734–45. doi: 10.1007/s00330-024-10828-y
24. Kim HJ, Chae EY, Eom HJ, Choi WJ, Shin HJ, Cha JH, et al. Node reporting and data system evaluation of axillary nodes in invasive ductal and lobular carcinoma. Radiology. (2025) 316:e243823. doi: 10.1148/radiol.243823
25. Schipper RJ, van Roozendaal LM, de Vries B, Pijnappel RM, Beets-Tan RG, Lobbes MB, et al. Axillary ultrasound for preoperative nodal staging in breast cancer patients: is it of added value? Breast. (2013) 22:1108–13. doi: 10.1016/j.breast.2013.09.002
26. Chen MY and Gillanders WE. Staging of the Axilla in Breast Cancer and the Evolving Role of Axillary Ultrasound. Breast Cancer. (2021) 13:311–323. doi: 10.2147/BCTT.S273039
27. Jahed DA, Dekeyzer S, Vanwambeke K, Antic M, Vanhoenacker C, and Vanhoenacker F. Automated Breast Ultrasound (ABUS): A Pictorial Essay of Common Artifacts and Benign and Malignant Pathology. J Ultrason. (2022) 22:e222–e235. doi: 10.15557/jou.2022.0037
28. Yan Y, Jiang T, Sui L, Ou D, Qu Y, Chen C, et al. Combined conventional ultrasonography with clinicopathological features to predict axillary status after neoadjuvant therapy for breast cancer: A case-control study. Br J Radiol. (2023) 96:20230370. doi: 10.1259/bjr.20230370
29. Shang Q, Feng K, Wei Y, Wang K, Yang C, Zhao S, et al. Evaluation of Male Breast Cancer and the Application of Sentinel Lymph Node Biopsy: A Multicenter Retrospective Study. Oncologist. (2023) 28:e1170–e1178. doi: 10.1093/oncolo/oyad189
30. Díaz-Roldán J, Eguía-Larrea M, Rubio-Sánchez T, and Muñoz-Bellvís L. Systematic review of synchronous contralateral axillary metastases in breast cancer: really M1 disease? Breast Cancer. (2022) 29:9–18. doi: 10.1007/s12282-021-01293-2
31. Postlewait LM, Teshome M, Adesoye T, DeSnyder SM, Lim B, Kuerer HM, et al. Contralateral axillary metastasis in patients with inflammatory breast cancer. Ann Surg Oncol. (2021) 28:8610–21. doi: 10.1245/s10434-021-10148-1
32. Liu W, Li R, Zhan Y, Bi Y, and Peng M. Ultrasound-based radiomics model for predicting axillary lymph node metastasis of breast cancer. BMC Med Imaging. (2025) 25:434. doi: 10.1186/s12880-025-01978-6
33. Fruchtman Brot H and Mango VL. Artificial intelligence in breast ultrasound: application in clinical practice. Ultrasonography. (2024) 43:3–14. doi: 10.14366/usg.23116
Keywords: axilla, lymph nodes, axillary metastasis, breast cancer metastasis, contralateral lymph nodes, contralateral axilla
Citation: Zenovia Antone N, Pintican R, Fetica B, Lisencu C, Marian D, Roman A, Trifa A, Gâta V, Muntean M, Pop B, Vlad C and Cadariu PA (2025) Ultrasound-based comparative assessment of ipsilateral vs. contralateral axillary lymph nodes in breast cancer patients — a pilot study. Front. Oncol. 15:1658446. doi: 10.3389/fonc.2025.1658446
Received: 02 July 2025; Accepted: 14 November 2025; Revised: 03 November 2025;
Published: 28 November 2025.
Edited by:
Kosuke Kawaguchi, Kyoto University, JapanReviewed by:
Aya Noro, Mie University Hospital, JapanYumi Kashikura, Saiseikai Matsusaka Sogo Byoin, Japan
Copyright © 2025 Zenovia Antone, Pintican, Fetica, Lisencu, Marian, Roman, Trifa, Gâta, Muntean, Pop, Vlad and Cadariu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roxana Pintican, Um94YW5hLnBpbnRpY2FuQGdtYWlsLmNvbQ==; Bogdan Fetica, ZmV0aWNhYkB5YWhvby5jb20=