 Calogera Claudia Spagnolo1†
Calogera Claudia Spagnolo1† Rosaria M. Ruggeri2†Angela Alibrandi3Martina Laganà2Desirèe Speranza4Salvatore Cannavò2Massimiliano Berretta5,6
Rosaria M. Ruggeri2†Angela Alibrandi3Martina Laganà2Desirèe Speranza4Salvatore Cannavò2Massimiliano Berretta5,6 Mariacarmela Santarpia5,7*
Mariacarmela Santarpia5,7*- 1Department of Biomedical and Dental Sciences and Morphofunctional Imaging (BIOMORF), University of Messina, Messina, Italy
- 2Endocrinology Unit, Department of Human Pathology of Adulthood and Childhood DETEV “G. Barresi”, University of Messina, Messina, Italy
- 3Unit of Statistical and Mathematical Sciences, Department of Economics, University of Messina, Messina, Italy
- 4Department of Chemical, Biological, Pharmaceutical and Environmental Sciences, University of Messina, Messina, Italy
- 5Division of Medical Oncology Unit, “Gaetano Martino” Hospital, Messina, Italy
- 6Department of Clinical and Experimental Medicine, University of Messina, Messina, Italy
- 7Department of Human Pathology of Adulthood and Childhood DETEV “G. Barresi”, University of Messina, Messina, Italy
Immune checkpoint inhibitors (ICIs) have radically changed the therapeutic landscape of several cancers. However, only a limited number of predictive factors are currently available in clinical practice to select patients for immunotherapy. The impact of excess weight on ICI toxicity and efficacy is presently under debate. This study was aimed at evaluating the occurrence of immune-related adverse events (irAEs) among cancer patients on ICI therapy according to baseline body mass index (BMI) and gender. The association with clinical outcomes was also analyzed.
Patients and methods: One-hundred thirty patients (93 males, 37 females, median age 67 years) with diverse types of advanced cancer treated with ICIs at a single university hospital were included in the study. Patients with a previously diagnosed thyroid dysfunction were excluded from this analysis.
Results: A number of irAEs occurred in 51 patients (39.2%; 33 males, 18 females). Their development significantly correlated to BMI. Overweight/obese patients experienced a higher (59.5% vs 40.5%; p<0.001), and earlier (8 vs 10.6 weeks; p=0.003) occurrence of irAEs than normal weight patients. About 65% of overweight/obese patients had an associated dysmetabolic state (i.e., hypertension, glycemic disturbances and/or dyslipidemia) and displayed higher prevalence of irAEs than those without comorbidities (p=0.019). At multivariate regression analyses, BMI was confirmed as an independent predictor of risk for developing AEs (p<0.001), with an odds ratio (OR) of 3.182 for overweight/obese patients. No differences in BMI or gender emerged in progression-free survival (PFS) and overall survival (OS) rates.
Conclusions: irAEs occurred more frequently in overweight/obese patients, mainly with metabolic abnormalities. These data underline the importance of a comprehensive clinical assessment, including weight and dysmetabolic comorbidities, of patients at baseline and during ICI therapy.
1 Introduction
Immune checkpoint inhibitors (ICIs) can restore the immune response against cancer by blocking inhibitory molecules, such as cytotoxic T lymphocyte-associated protein 4 (CTLA-4), programmed death-1 (PD-1) and its ligand (PD-L1), expressed on immune and/or tumor cells, the so-called immune checkpoints (1–3). Their use has revolutionized the standard of care of cancer patients, providing therapeutic options for many advanced stage tumors considered otherwise untreatable (4–9). ICI treatment has been associated with excellent response rates and improved survival when administered as either first-line therapy or after other treatments (10–12). Some tumor characteristics, such as the expression of PD-L1 on cancer cells, a T-cell inflamed profile (T-cell infiltration), and the mutational and/or neoantigen burden are currently known to predict response to ICIs, although the identification of predictive biomarker for ICI-based therapy is still challenging (13, 14). In particular, the impact of patient-related factors, like sex, age or BMI, remains to be elucidated, as well as the predictive and/or prognostic role of ICI adverse events, to be considered “on-target” side effects (15).
Indeed, as indications for ICI therapy have expanded and numbers of treated patients have increased, a unique profile of toxicity has emerged, characterized by the occurrence of immune-mediated damage of several tissues and organs (16). These immune-related adverse events (irAEs), autoimmune in etiology, are reported in up to 50% and more of treated patients and can potentially affect all organs. Dermatologic, gastrointestinal, hepatic, and endocrine manifestations are the most frequently reported irAEs, while neurological, cardiac or pulmonary side effects rarely occur (16). In particular, thyroid disorders are among the most common endocrine irAEs, mostly under anti-PD-1/PD-L1 treatment, and include hyperthyroidism, hypothyroidism and destructive thyroiditis (thyrotoxicosis progressing to hypothyroidism) (17–19). Other less common endocrinopathies include hypophysitis, adrenal insufficiency, type 1 diabetes, and hypoparathyroidism (19–21). Although ICI-based therapies are typically well tolerated, the risk of potentially severe irAEs, compromising organ function and/or quality of life, is not negligible and increases with combination regimens (17).
Moreover, some (22, 23) but not all (24) studies have found an association between female sex and occurrence of irAEs.
A growing body of evidence suggests that overweight/obesity may be associated with increased immunotoxicity on the one hand (25) and with improved efficacy of immunotherapy on the other hand (26, 27). The mechanisms behind this unexpected favorable association, the so-called “obesity paradox”, are still not clear (28, 29), and the real impact of overweight on irAE development and efficacy still remains to be further defined. The present study was aimed at evaluating the occurrence of irAEs among cancer patients on ICI therapy according to baseline BMI and gender. Further, we analyzed survival outcome difference in these subgroups of patients.
2 Materials and methods
2.1 Patients
We performed a retrospective/prospective analysis of patients with different types of cancer, at early or advanced stage of disease, treated with ICIs at the Medical Oncology Unit of the University Hospital “Gaetano Martino” of Messina from January 2020 to December 2024. For each patient, we collected the following data: demographic characteristics (gender and age at the start of ICI therapy), type of cancer [non-small-cell lung carcinoma (NSCLC), melanoma, renal cell carcinoma, and others], type and duration of ICI treatment (nivolumab, pembrolizumab, atezolizumab, ipilimumab, cemiplimab, and durvalumab) weight, BMI, and Eastern Cooperative Oncology Group performance status (ECOG PS) (30). Inclusion criteria were age > 18 years, any type of cancer under ICI treatment, a minimum follow-up duration of 3 months. Exclusion criteria were a previously diagnosed thyroid dysfunction, or evidence of abnormal thyroid function tests at baseline, previous treatment with antithyroid drugs or levothyroxine, or ongoing therapy with corticosteroids or immunosuppressive therapy, and the unavailability of important data from medical records before or after treatment. More in detail, 70 patients were not considered for analysis because of incomplete information, 30 patients were further excluded because were not euthyroid at baseline and/or were already under therapy with L-T4. In total, 130 patients with complete information were included in the study.
The study was carried out in accordance with the World Medical Association’s Declaration of Helsinki. Informed consent from each subject for using anonymized data was obtained.
2.2 Methods
Clinical and pathological data for all patients treated with ICIs were collected by consulting medical records. BMI was calculated as body weight (kg) divided by height (m) squared and patients were categorized as being underweight (BMI <18.5), normal weight (BMI 18.5 – 24.9), overweight (BMI 25 – 29.9), or obese (BMI >30) based on cut offs suggested by the World Health Organization [https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight]. The overweight or obese status were also distinguished based on the presence of a dysmetabolic clinical status, defined as the presence of hypertension, glycemic disturbances (diabetes mellitus, and/or insulin resistance and/or impaired glucose tolerance) and/or dyslipidemia. irAEs were reported and graded according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events (CTCAE), version 5.0 (31).
Treatment efficacy was assessed in terms of overall survival (OS), which was recorded from the beginning of treatment until the observation of death from any cause during follow-up or loss, and in term of progression-free survival (PFS) recorded from the beginning of treatment until the progression of disease, according to the RECIST v 1.1 criteria (32). All biochemistry serum measurements, including hormonal assessment, were performed centrally at the laboratory of the University Hospital of Messina, and were measured both at baseline and at each hospital admission using commercial kits with routine methods.
2.3 Statistical analysis
Numerical data are expressed as median and interquartile range and the categorical variables as number and percentage. The examined variables were not normally distributed, as verified by a Kolmogorov–Smirnov test. Consequently, the nonparametric approach was used. In order to compare patients with or without irAE occurrence, the Mann–Whitney test was applied for numerical variables and the Chi Square test (or Likelihood ratio test or exact Fisher test, as appropriate) for categorical variables. Some boxplots were generated to better visualize the differences between two groups of patients. In order to identify possible significant predictors of irAE occurrence (yes or no), logistic regression models were estimated. The explicative power of the following covariates was tested: age, sex, weight, BMI, performance status, type of cancer, type (anti-PD-1, anti-PD-L1, anti-CTLA-4) and duration of ICI treatment, etc. In addition, the predictive power of the interactions between BMI and cancer type, gender, or treatment type was also evaluated. Therefore, a multivariate logistic regression model was estimated inserting only the covariates that were statistically significant at univariate approach [i.e., weight, BMI category, performance status (sec. ECOG) and positive family history of autoimmune disease]. The results were expressed as odds ratio (OR), 95% confidence interval (95%C.I.) and p-value. Kaplan Meier curves were generated to better visualize patient survival time, with reference to OS and PFS, taking into account two stratification factors: AEs and BMI category. The survival analysis was detailed reporting the number of subjects, the number of events, the number and percentage of censored data, the median time with its standard error and its 95% confidence interval, and the Log-Rank test for comparing stratification factors. Statistical analyses were performed using SPSS Statistics for Window v22.0. A p-value < 0.05 was considered to be statistically significant.
3 Results
3.1 Study cohort
One hundred thirty patients (93 males and 37 females; male/female ratio was 2.51) with complete information were included in the study. Baseline characteristics of the overall cohort are presented in Table 1.
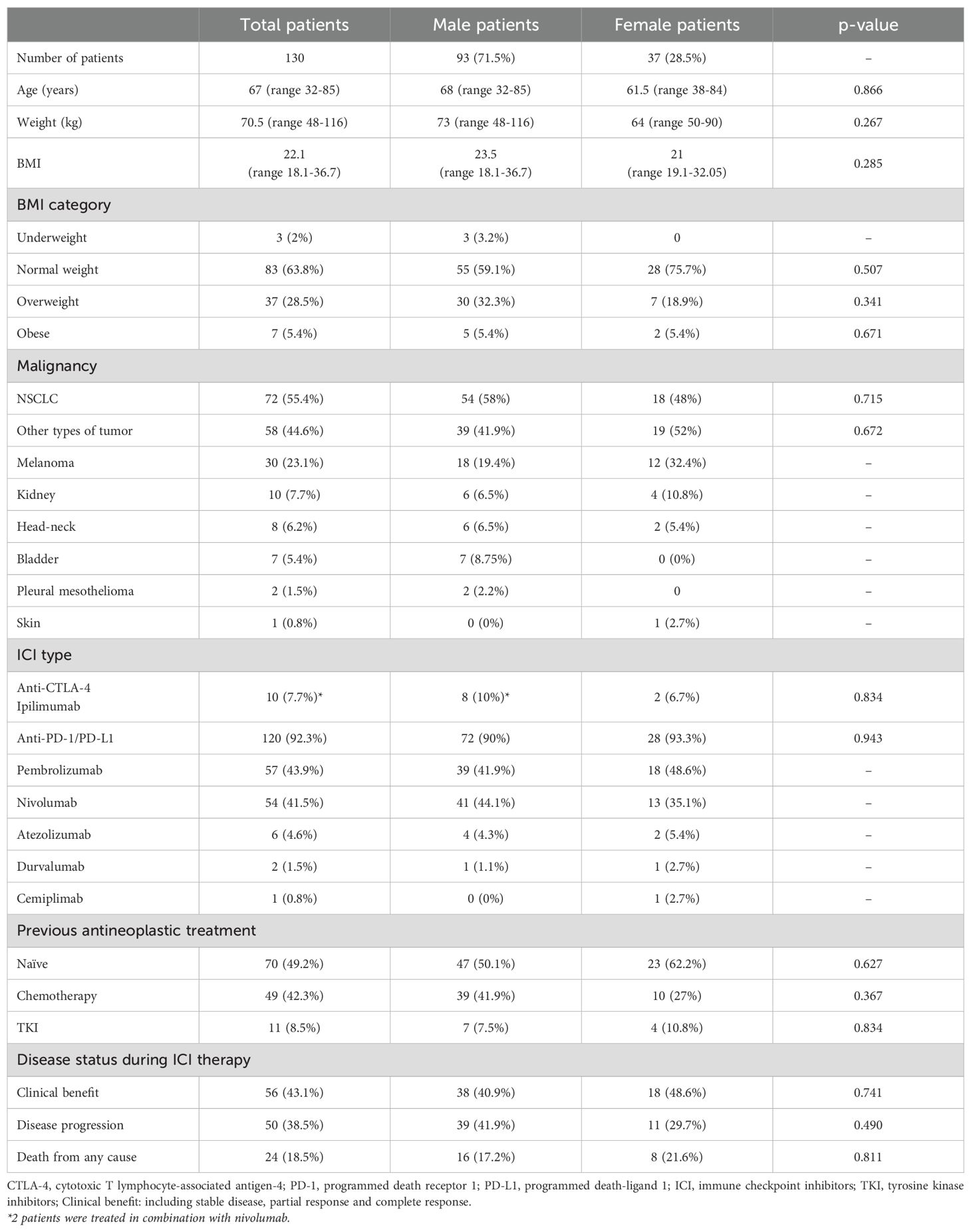
Table 1. Baseline characteristics of the overall cohort of cancer patients.
The median age was 67 years (range 32-85). Primary tumors were non-small cell lung carcinoma (NSCLC) (n=72, 55%), melanoma (n=30, 23%), renal cell carcinoma (n=10, 7.7%), and others (n=18, 14.3%). Cancer patients received anti-PD-1 (nivolumab/pembrolizumab/cemiplimab, n= 112, 86%), anti-PD-L1 (atezolizumab/durvalumab, n=8, 6%), anti-CTLA-4 (ipilimumab, alone n=10; or in association with nivolumab, n=2), as first-line (n=63) or subsequent lines (n=60) of therapy (after conventional chemotherapy and/or TKI), or as adjuvant treatment (n=7).
At baseline evaluation, median BMI in the whole cohort was 22 kg/m2 (range 18-37); median body weight 70.5 kg (range 48 – 116). According to WHO classification, 3 patients (2.3%) were defined as underweight, 83 patients (63.8%) as having a normal weight, 37 patients (28.5%) as overweight and 7 patients (5.41%) as obese. Overall, 33.9% of patients (n=44) had a BMI ≥25 kg/m2, and 65.9% of them had a history of hypertension, and/or glycemic disturbances and/or dyslipidemia (that is an associated dysmetabolic status).
Thyroid function tests at baseline were within normal limits in all patients, but fifteen (11%) had positive thyroid autoantibodies (TPOAb and/or TgAb) at baseline. None of them was under L-T4 therapy or was taking any drugs interfering with thyroid function.
3.2 Incidence and spectrum of adverse events
During treatment, irAEs occurred in 51 patients (39.2%; 33 males and 18 females; median age 69 years), without significant differences between the two sexes (p=0.289). Among them, 41 (78%; 31.5% of the whole cohort) developed thyroid dysfunction (either hypothyroidism or thyrotoxicosis) without difference in sex (p= 0.578). Primary hypothyroidism was the most common irAE, occurring in 39 patients (30% of the whole cohort), including 14 patients who experienced transient thyrotoxicosis with subsequent progression to hypothyroidism, and 25 patients who developed hypothyroidism without any preceding recognized thyrotoxicosis. The 39 patients who developed hypothyroidism received levothyroxine (mean dose of 1.6 μg/kg/day) for the entire duration of ICI treatment. Persistent hyperthyroidism requiring anti-thyroid treatment occurred in two patients. None of the patients who experienced transient thyrotoxicosis was prescribed with glucocorticoids.
Patients who experienced thyroid irAEs showed a higher prevalence of non-thyroidal irAEs (p=0.003). Overall, 29 patients (22.3% of the entire cohort) developed non-thyroid irAEs [cutaneous (n=9), gastro-intestinal (n=9), pulmonary (n=2), rheumatic (n=8), and a single case of adrenalitis], and difference by sex was significant (p=0.007), female patients being more frequently affected than male patients. Among these, 19 patients developed thyroid dysfunction as an irAE, without differences between the two sexes (p=0.08). Overall, irAEs were more frequently recorded in female patients, but thyroid disorders occurred equally in both sexes (Table 2). Interestingly, no patient in our cohort developed severe irAEs (grade 3–4 according to the Common Terminology Criteria for Adverse Events) and none had to permanently discontinue ICI treatment. This is partially in line with data from the literature since thyroid irAEs, the most common type of irAEs in our cohort, are usually low grade if promptly diagnosed. However, even with regards to non-endocrinological irAEs, no event of grade >2 and no patient had to permanently discontinue ICI treatment in our series. This unexpected finding may be due to the design of the study, that was first conceived to assess endocrinological irAEs. Hence, we excluded patients with a previously diagnosed thyroid dysfunction that could potentially represents an important predisposing factor for other irAEs. Moreover, only patients with fully documented hormone status at baseline and during follow-up were included, further decreasing the sample size.
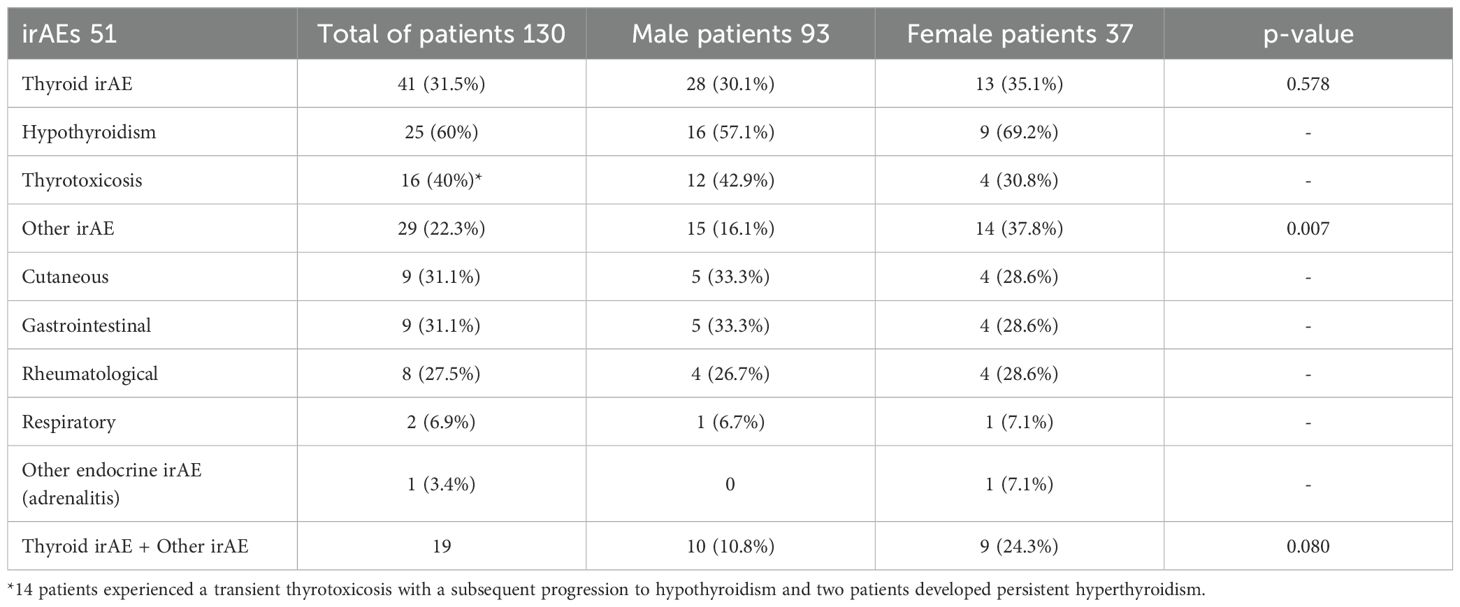
Table 2. Incidence of irAEs according to gender.
3.3 Predictors of irAEs and time of onset
Patients who developed irAEs under ICI treatment had similar age and gender distribution. However, despite no differences by gender emerging between patients experiencing thyroid dysfunction (p=0.578), non-thyroidal irAEs occurred more frequently in female than male patients and the difference was significant (p=0.007).
Development of irAEs was associated with higher BMI (Figures 1A, B). The prevalence of irAEs was 59.5% in overweight/obese patients vs 40.5% in normal weight patients (p<0.001). Patients who developed irAEs had higher body weight (75.5 ± 12 kg vs 70.2 ± 11 kg, p = 0.017) and higher BMI (25 ± 3.5 kg/m2 vs 22.7 ± 3 kg/m2, p = 0.002) than patients who did not, in both sexes. The prevalence of irAEs was higher among overweight/obese patients compared to normal weight patients, whether they are considered (59.5% vs 40.5%; p<0.0001) or divided by sex (males, 67% vs 33%; p=0.001; females, 57% vs 43%, p=0.011). About 65% of overweight/obese patients had an associated dysmetabolic state, defined as the presence of hypertension and/or glycemic disturbances (insulin resistance, diabetes, impaired glucose tolerance) and/or dyslipidemia (n=29/44). These dysmetabolic overweight/obese patients had a higher prevalence of irAEs compared to those who did not have these associated comorbidities (22/29 vs 6/15; p=0.019) (Figure 2).
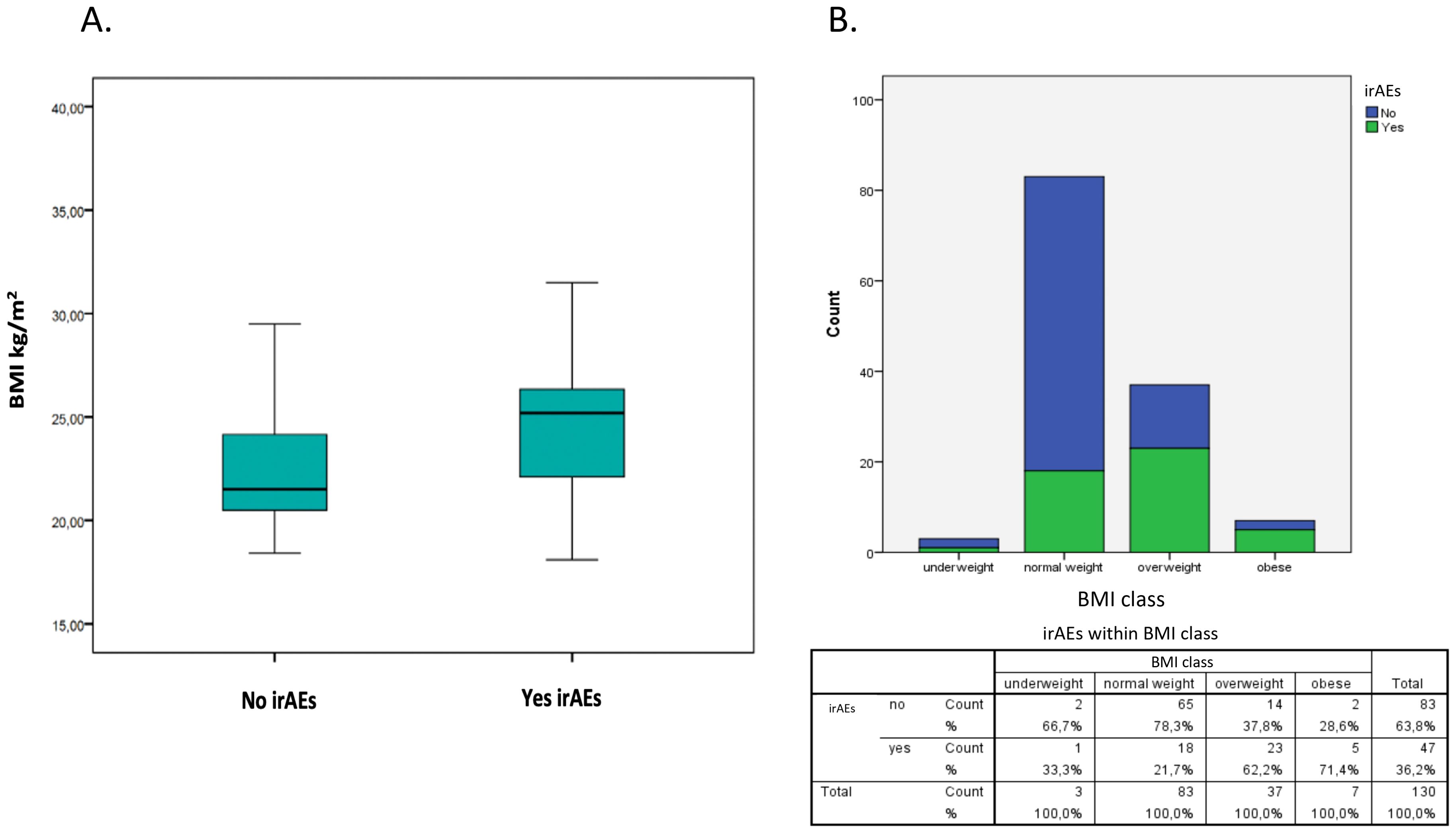
Figure 1. Development of irAEs and BMI. (A) The boxplot on the left shows the distribution of patients who did not develop irAEs (no) based on BMI, while on the right it shows the distribution of those who developed irAEs (yes). Development of irAEs was associated with higher BMI. The prevalence of irAEs was 59.5% in overweight/obese patients vs 40.5% in normal weight patients (p<0.001). (B) The graphic shows the prevalence of irAEs according to BMI category.
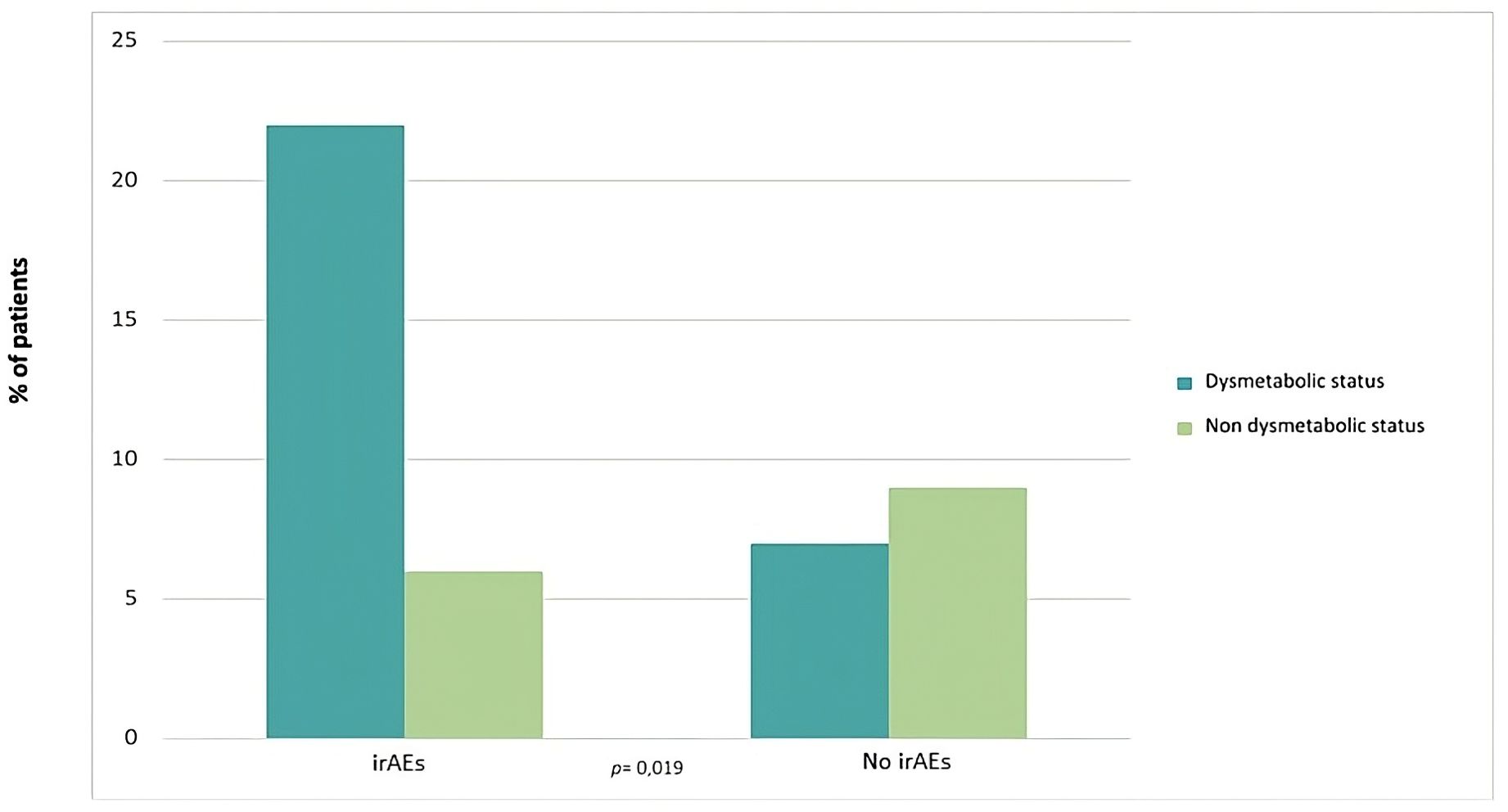
Figure 2. Prevalence of irAEs in dysmetabolic overweight/obese patients. The graphic shows the prevalence of irAEs according to the presence of a dysmetabolic state in overweight/obese patients. Dysmetabolic overweight/obese patients had a higher prevalence of irAEs compared to those who did not have these associated comorbidities (22/29 vs 6/15; p = 0.019).
At uni- and multivariate regression analyses, BMI, more in detail BMI category, was confirmed as an independent predictor of risk for developing irAEs (p<0.001), with overweight/obese patients having an OR of 3.182 compared to normal weight/underweight patients. Higher BMI and a better ECOG performance status were associated with the occurrence of irAEs (p<0.001, and p=0.013, respectively). Also, a positive family history of any autoimmune disease was a predictor of risk (p< 0.001) (Table 3).
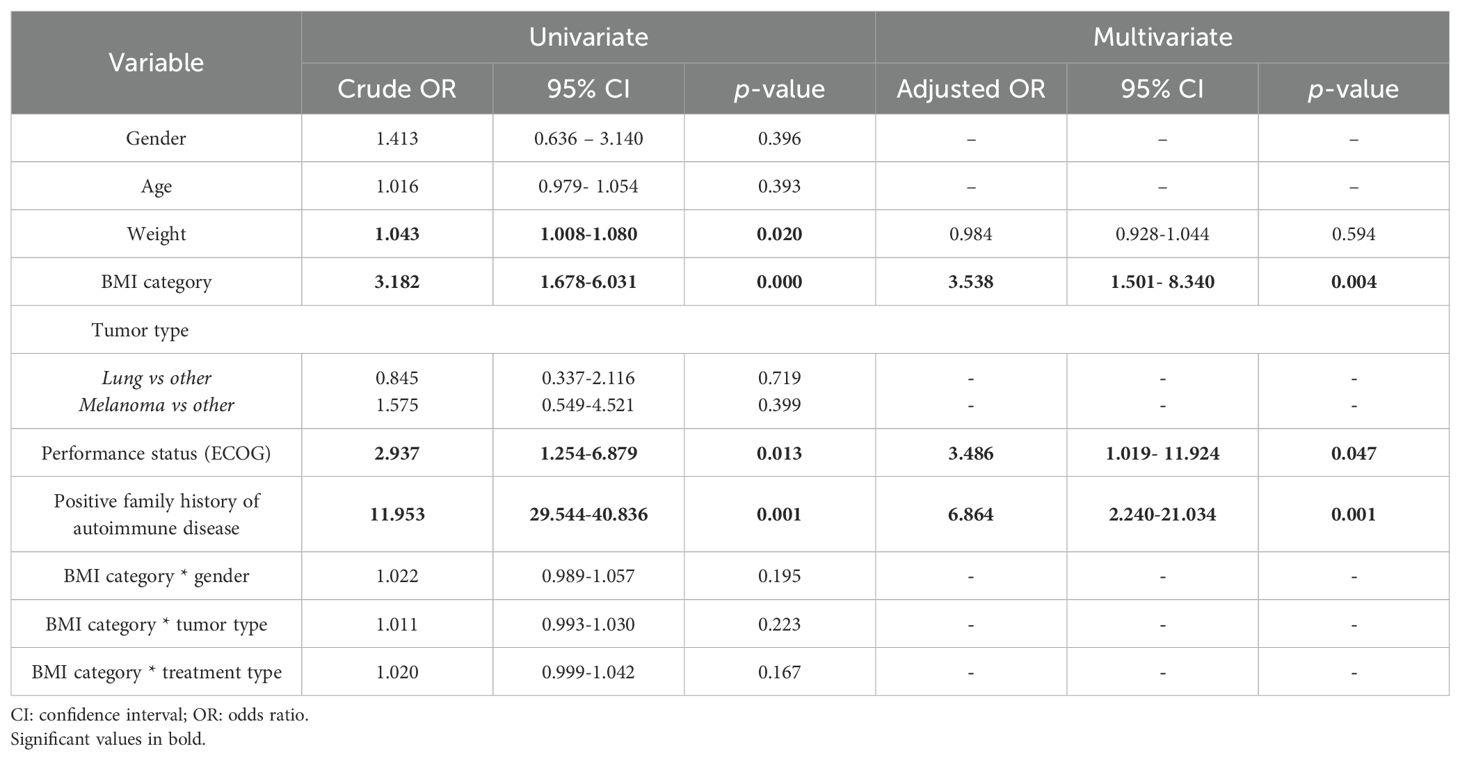
Table 3. Results of univariate and multivariate logistic regression models for the occurrence of irAEs.
The median time from first treatment with ICI to the development of any irAE was 8 weeks (range 1–60 weeks), and about 60% of irAEs occurred within the first 9 weeks. Thyroid irAEs usually preceded or coincided with the occurrence of non-endocrine irAEs, being the first side effects reported in almost all patients in our cohort. When subdividing our patients according to gender, median time to first appearance of irAEs was 6 weeks (range 2–12 weeks) in females and 8 weeks (range 1–60 weeks) in males, with female patients experiencing an earlier onset of irAEs than males (p = 0.047). When stratifying time to first appearance of irAEs by BMI category, the median time to develop any irAE was 7 weeks (mean 8.5 ± 6.5 weeks, range 3–60 weeks) in overweight/obese patients compared to 8 (mean 10.7 ± 12.7 weeks, range 3-30) in normal weight/underweight patients, so that irAEs occurred earlier in patients with higher BMI (p=0.003). Thus, overall, overweight/obese patients experienced irAEs more frequently and earlier than normal weight/underweight patients.
Overall, no significant statistical differences in PFS and OS emerged. The median PFS and OS were, respectively, 14 and 16 months. Neither PFS nor OS were significantly different both between the group of patients that developed irAEs compared to those who did not develop irAEs (median PFS 15 months vs. 14 months, p = 0.662; median OS 22 months vs. 16 months, p = 0.446) (Figures 3A, B) (Tables 4A, B), and between the group of overweight/obese patients compared to normal weight/underweight patients (median PFS 9 months vs. 15 months, p = 0.313; median OS 16 months vs. 16 months, p = 0.629) (Figures 4A, B) (Tables 4C, D). However, it is worth noting the 6-month advantage in OS in the group of patients that developed irAEs, as well as a longer, although not statistically significant, PFS in the normal weight/underweight patient group.
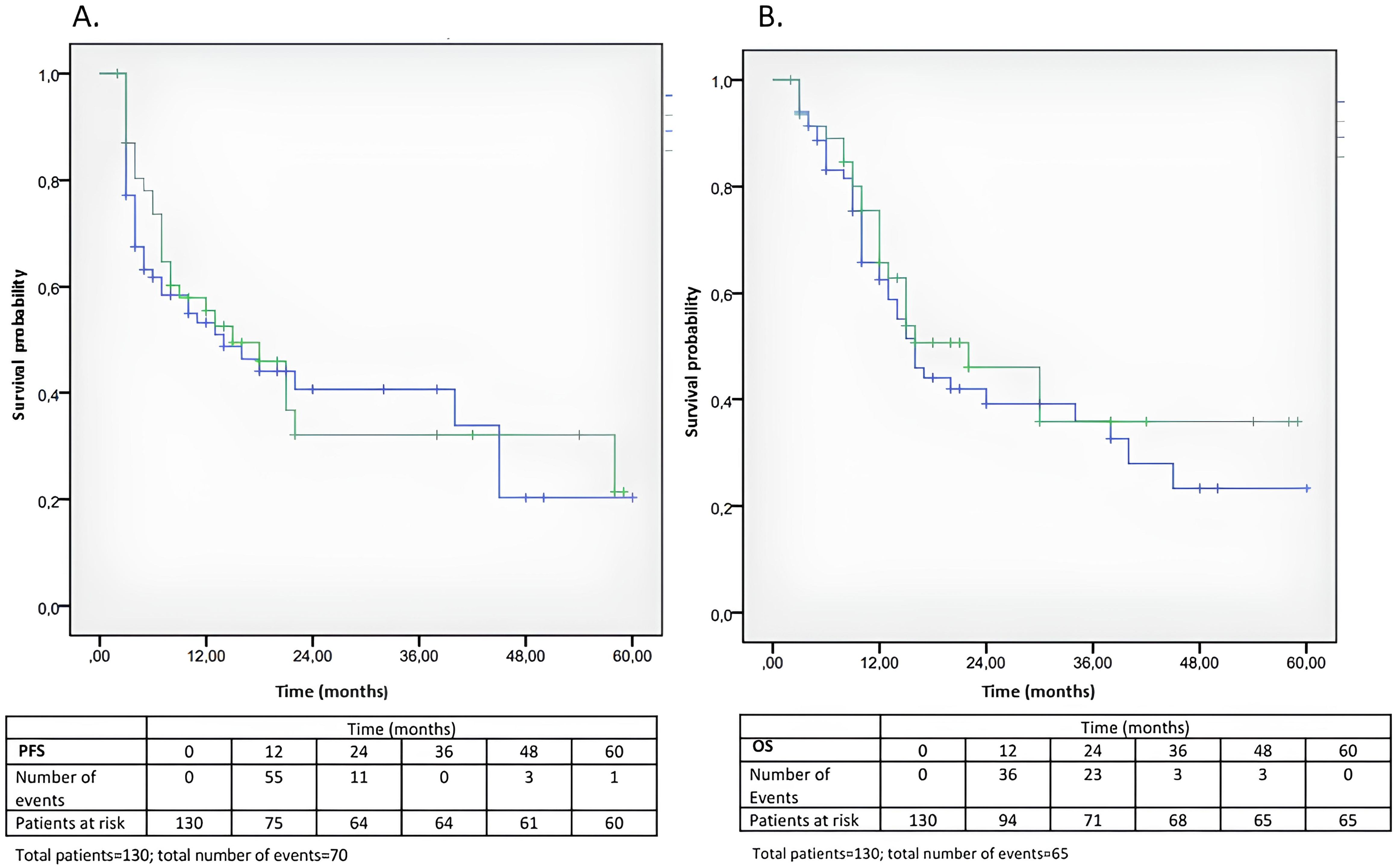
Figure 3. (A, B) Kaplan-Meier analysis of PFS and OS according to the development of irAEs. (A) Kaplan-Meier curves of PFS in the group of patients that developed irAEs (green) and in those who did not develop irAEs (blue) (median PFS 15 months vs. 14 months, p = 0.662) (B) Kaplan-Meier curves of OS in the group of patients that developed irAEs (green) and in those who did not develop irAEs (blue) (median OS 22 months vs. 16 months, p = 0.446) (see Tables 4A, B).
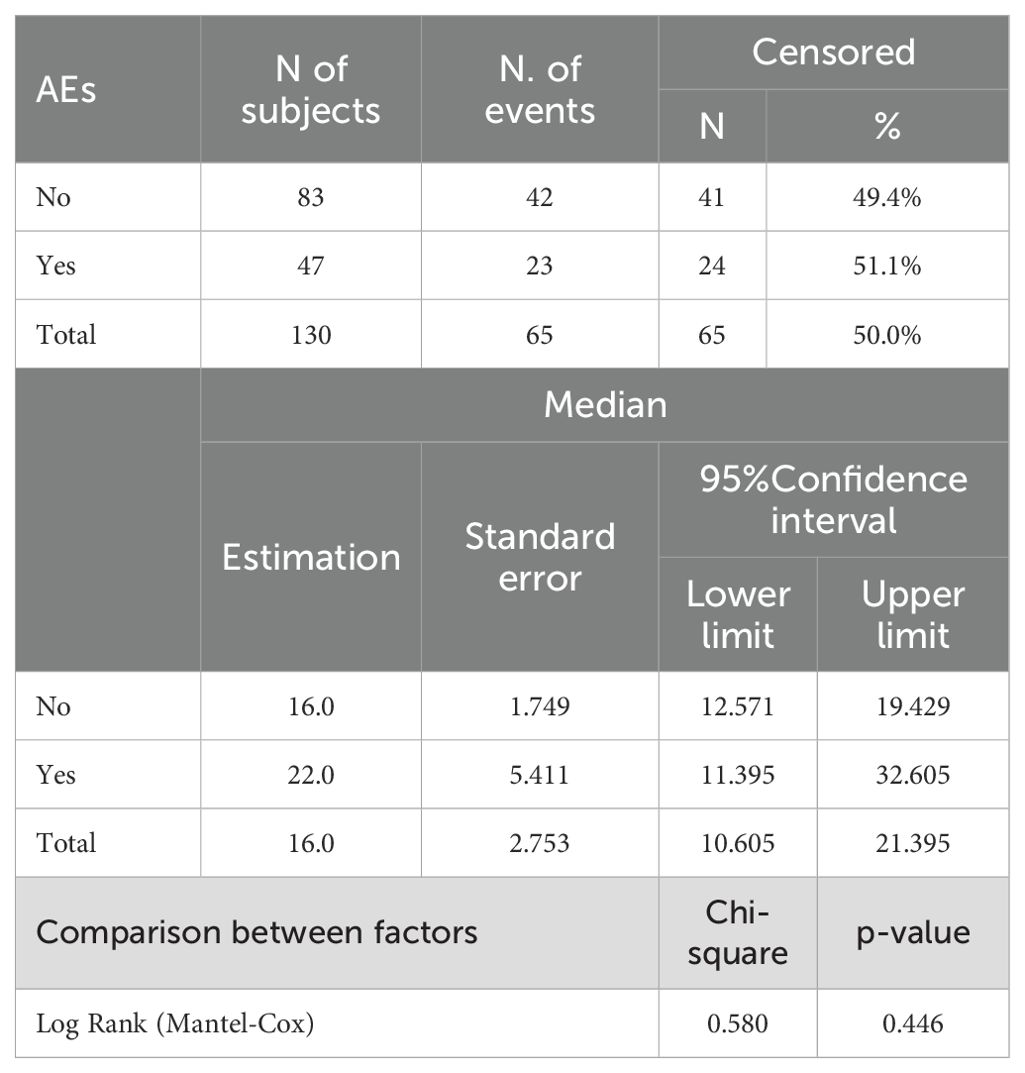
Table 4A. Kaplan-Meier curves for OS (factor: AEs).
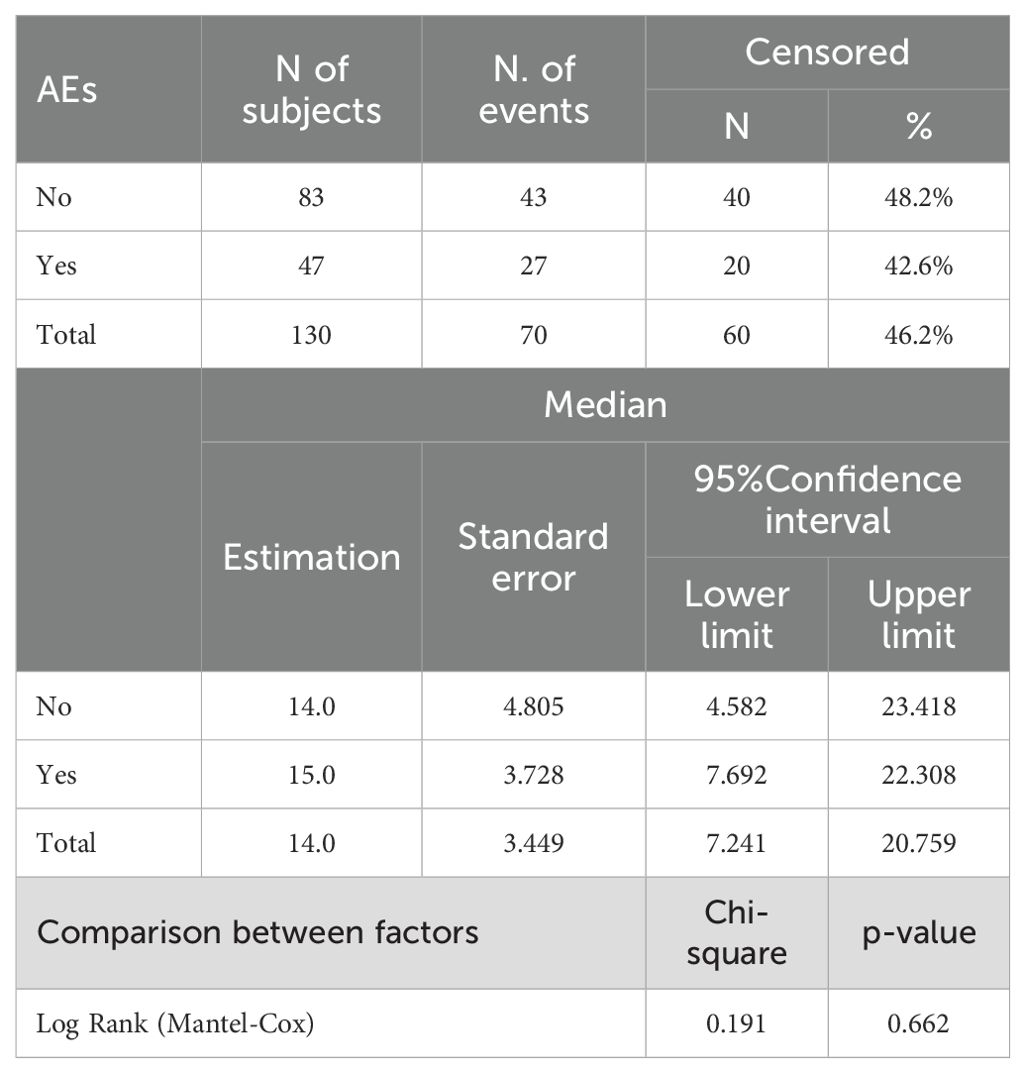
Table 4B. Kaplan-Meier curves for PFS (factor: AEs).
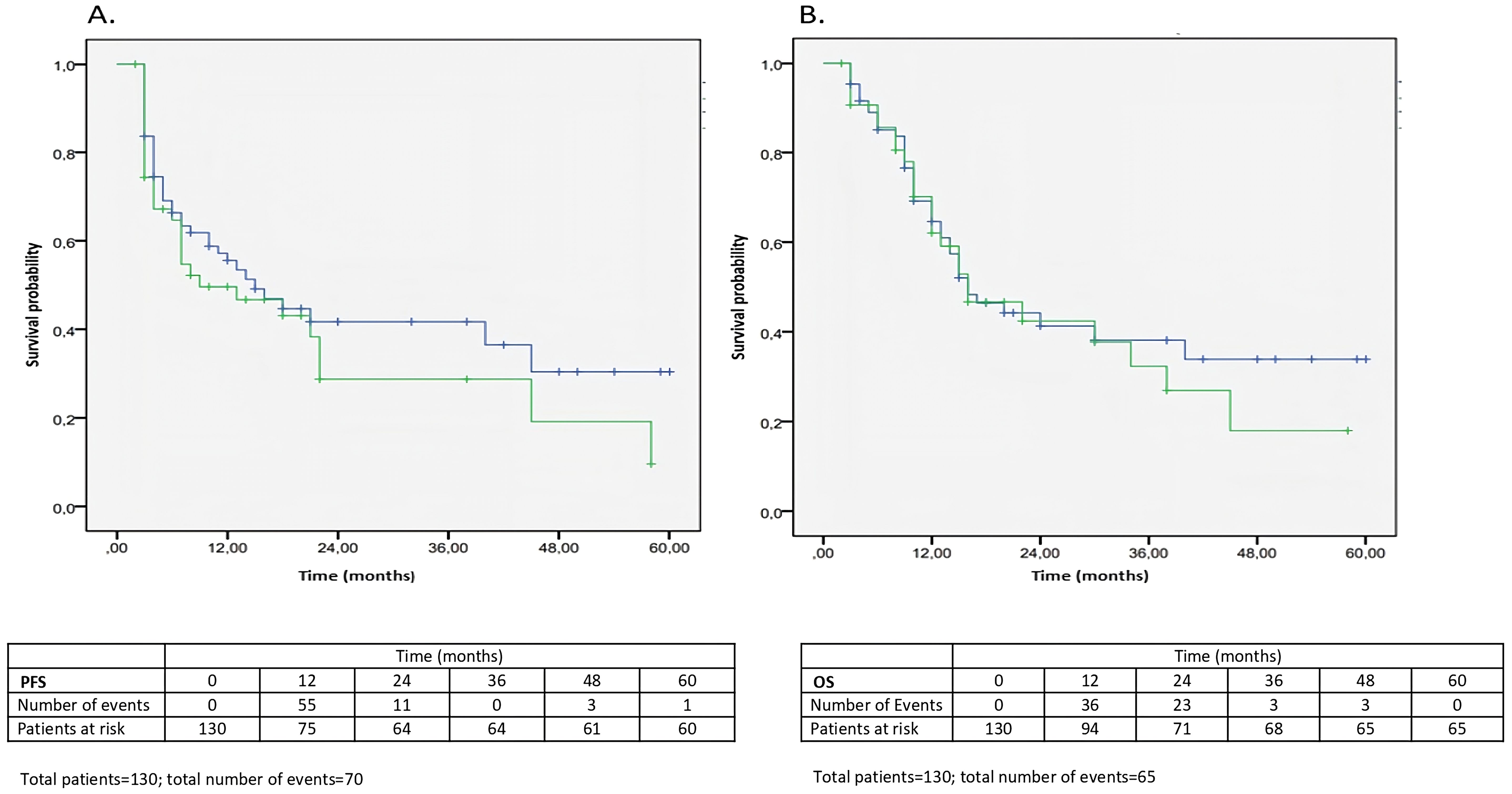
Figure 4. (A, B) Kaplan-Meier analysis of PFS and OS according to BMI category (overweight/obese or normal weight/underweight). (A) Kaplan-Meier curves of PFS in the group of overweight/obese patients (green) and normal weight/underweight patients (blue) (median PFS 9 months vs. 15 months, p = 0.313). (B) Kaplan-Meier curves of OS in the group of overweight/obese patients (green) and normal weight/underweight patients (blue) (median OS 16 months vs. 16 months, p = 0.629) (see Tables 4C, D).
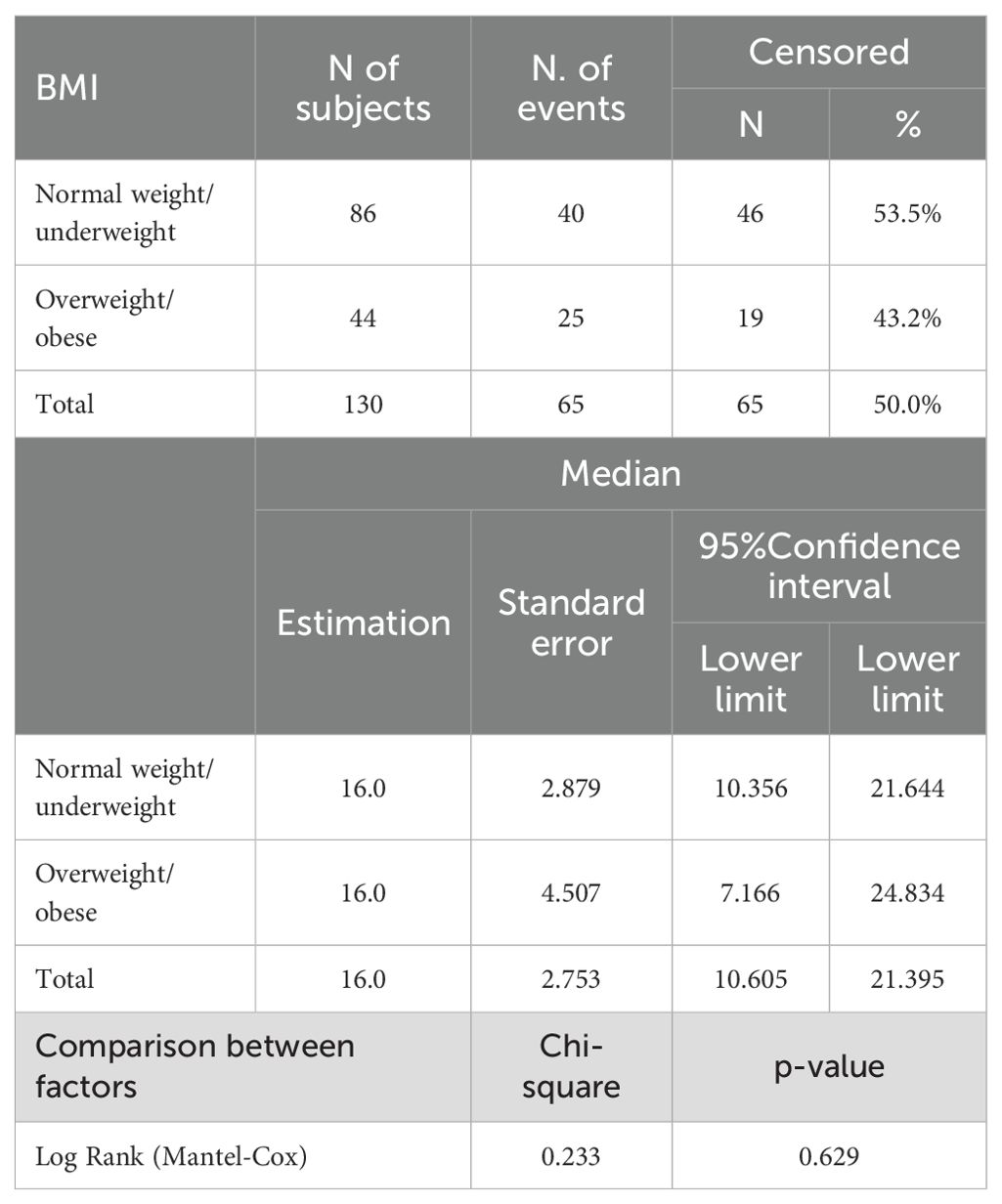
Table 4C. Kaplan-Meier curves for OS (factor: BMI).
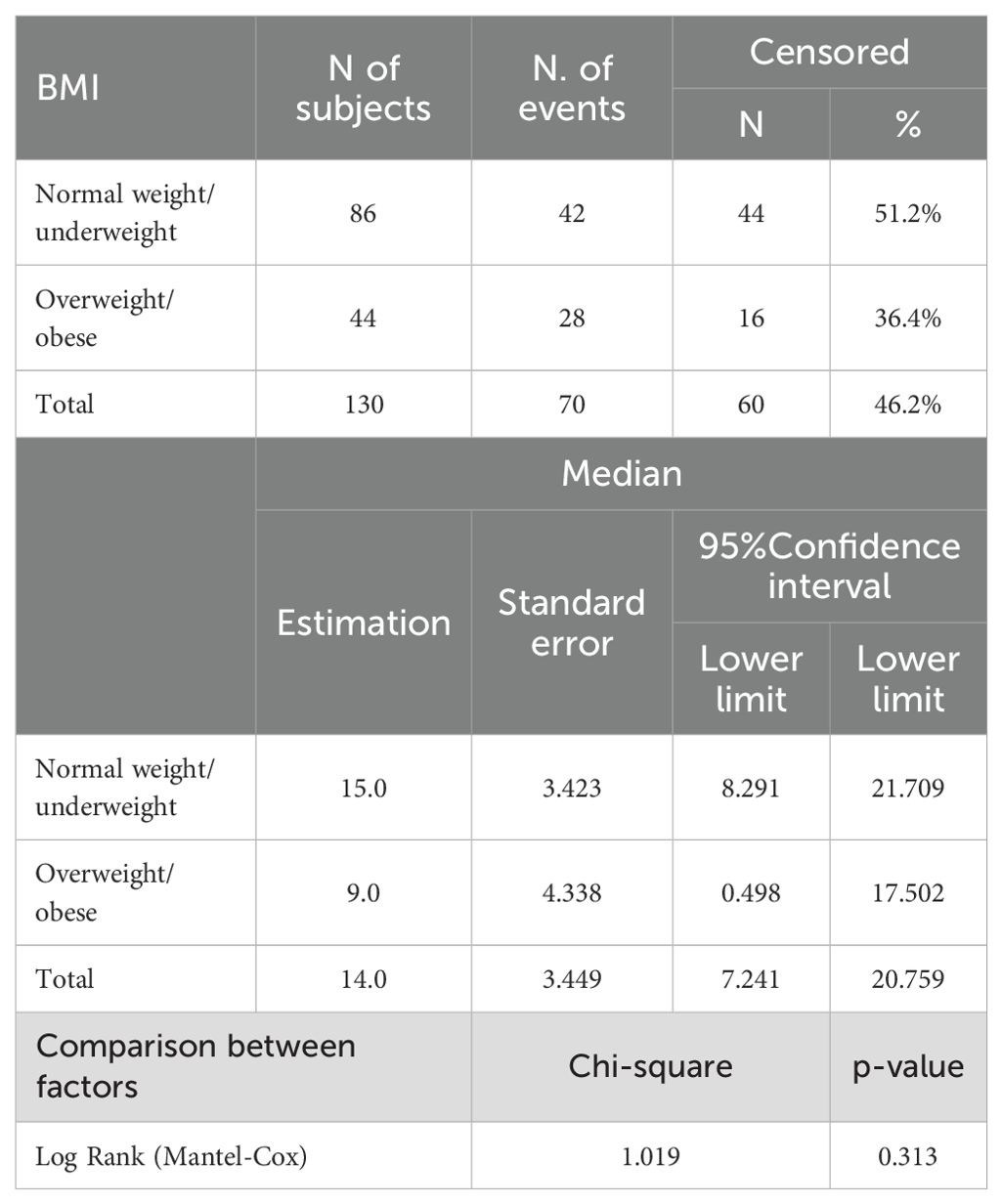
Table 4D. Kaplan-Meier curves for PFS (factor: BMI).
4 Discussion
The present study investigated the impact of gender and BMI on irAE development and efficacy in a cohort of patients with different types of cancer. In our single center cohort, 51 patients (39.2%) developed an irAE, thyroid dysfunction being the most common one, consistent with previously published real-world data (33–36).
With regard to gender differences, overall, irAEs were more frequently observed in female patients, with the relevant exception of thyroid disorders that occurred equally in both genders. Unlike other studies including a large number of patients with lung cancer (37–39), we found a female prevalence in irAEs, as reported in other series (23). Moreover, female patients experienced an earlier onset of irAEs than males.
Regarding the impact of BMI, we found that it was strongly associated with the occurrence of irAEs. Indeed, the prevalence of irAEs was significantly higher among overweight/obese patients compared to normal weight patients in both sexes, and patients with higher BMI were at increased risk of developing an irAE, with an OR of 3.182 compared to normal weight/underweight patients.
Evidence regarding the association between BMI and irAEs among cancer patients receiving ICIs is limited, and sometimes conflicting. Some studies reported a significantly higher incidence of irAEs in patients with higher BMI (25, 35, 39), while other studies failed to demonstrate such an association. Two meta-analyses explored the association between BMI and irAEs among patients with cancer receiving ICIs, and both concluded that high BMI was associated with a higher rate of irAEs (40, 41). Our study provides further evidence in support of a positive correlation between BMI and development of irAEs, reporting a 3-fold increase of the risk of irAEs among overweight/obese patients. Moreover, irAEs occurred earlier in overweight/obese patients than in normal weight/underweight patients, although without any difference in severity.
The mechanisms of such an intriguing association between BMI, a surrogate measure of body fat, and ICI therapies are not completely understood. Obesity is a low-grade inflammatory metabolic condition that has been associated with both cancer and autoimmunity (42, 43). Indeed, obesity is associated with increased adipose tissue, metabolic disturbances (hyperglycemia), higher levels of insulin, and insulin-like growth factors (IGFs), with potent mitogenic activity (44–46). Moreover, it has been associated with increased secretion by adipocytes of pro-inflammatory cytokines (TNF-α, IL-6 and IL-1β) and adipokines (leptin, adiponectin, resistin), which could affect T cell function, resulting in Th1/Th2 imbalance and promoting a pro-inflammatory state (47, 48). Such a pro-inflammatory condition is well known to predispose to the occurrence of autoimmune disorders (49, 50); hence, excess body weight may promote the development of irAEs. Moreover, fat accumulation leads to enhanced infiltration of pro-inflammatory CD8+ T cells into adipose tissue, accompanied by a reduction in adipose-resident regulatory T cells (Tregs) (51). Additionally, other obesity related factors such as dietary habits, genetic susceptibility, and microbiome may contribute to increased occurrence of irAEs in obese patients.
Worthy of note, our study is the first to suggest that irAEs occur more frequently in overweight/obese patients with a concurrent dysmetabolic state, defined as the presence of hypertension and/or glycemic disturbances and/or dyslipidemia, suggesting that low grade meta-inflammation, well known to be associated with obesity and related metabolic disorders, may represent a predisposing condition for development of irAEs in patients with higher BMI. Therefore, baseline BMI and related dysmetabolic conditions should be considered among the potential risk factors for the development of irAEs, along with other potential predictors, such as a family or personal history of autoimmune disorders, the use of immunotherapeutic combinations or previous TKI treatment. This would help clinicians in identifying patients who are at higher risk for irAEs, thereby personalizing therapeutic choices and clinical monitoring.
Alternatively, overexposure to treatment may occur in overweight patients due to an increased dose calculation based on mass weight (52). In this light, sarcopenic obesity, a not rare condition in oncologic patients, represents a complex and emerging factor in cancer patients undergoing ICI therapy. Characterized by the coexistence of low muscle mass and excess adiposity, it has been associated with increased toxicity and poorer clinical outcomes in various cancer settings (53–55). Recently, a systematic review and meta-analysis examining the impact of sarcopenia on cancer patients treated with ICIs found that sarcopenia is associated with an increased risk of irAEs, though the relationship with irAEs was less clear (56). Moreover, sarcopenic obesity may act as a confounding factor, influencing both the incidence of irAEs and treatment efficacy, complicating the interpretation of clinical outcomes (53). This dual role underscores the importance of considering body composition, beyond simple measures of body weight, when interpreting clinical associations. Further studies are needed to elucidate its precise impact and underlying mechanisms.
Even more complex is the relationship between obesity, cancer outcomes and response to cancer treatment in the context of ICI treatment. Obesity has been recognized as a risk factor and a negative prognostic factor for several cancers, worsening oncological outcomes, including recurrences, disease-free survival, all-cause and cancer specific mortality (29). Nevertheless, evidence suggests that overweight and obesity may be associated with better oncological outcomes than normal weight, and an inverse relationship between BMI and mortality (the so-called ‘obesity paradox’) has been found in several cancers at advanced stage, although the underlying mechanisms are not fully understood (29, 50).
A possible suggested mechanism could be the better objective responses to immunotherapy observed in obese compared to non-obese patients, with significantly longer PFS and OS (57). A high BMI has been associated with better clinical outcomes to ICI therapy. Complex interactions between the adipose tissue and tumor cells have been described (58). The modulation of the tumor microenvironment by obesity-associated molecules, including hormones and pro-inflammatory cytokines (e.g. TNF-α, IL-6) can play a key role in promoting tumor development and progression and, at the same time, in enhancing T-cells function and immune responses to ICIs. Besides inflammation, other mechanisms can modulate the effects of obesity in cancer patients, including alterations of insulin-like growth factor pathways, induction of hypoxia and HIF-1α signaling, and modulation of microbiota (59). The role of BMI as a predictor of toxicity from anti-neoplastic drugs should be further explored. In advanced cancer patients treated with ICIs, several studies reported better outcomes, in terms of longer PFS and/or OS, in overweight/obese patients compared to patients with normal BMI, with differences by sex (26, 27, 60, 61).
In our cohort, we failed to find any relationship between obesity, occurrence of irAEs and treatment efficacy in terms of either PFS and/or OS. However, it is widely known that survival outcomes can be influenced by several factors related to patients and/or cancer. We hypothesize that this may be due to several factors. First, the sample size of the study was limited, and our patient cohort included various tumor types and stages — although the majority were advanced — which can independently be associated with different prognoses, regardless of treatment. Moreover, since this was a real-world, observational study, patients with some significant comorbidities (i.e., cardiovascular) and with ECOG PS 2, who are usually excluded from large registration trials, were also included. Finally, other important factors could have potentially affected survival outcomes, including previous therapeutic lines and the great variability among patients in the timing and methods used for disease response evaluation, as for clinical practice. However, we decided to assess PFS and OS because these outcomes can better reflect the long-term efficacy of immunotherapy compared to treatment response.
Some limitations should also be noted, including: (i.) the retrospective design; (ii.) the relatively limited number of patients; (iii.) the inclusion of patients with different types of cancer, introducing some clinical heterogeneity and potential biases. Interestingly, our cohort of 130 patients had no grade 3/4 irAEs or irAEs leading to treatment discontinuation, which is lower than would be expected according to literature data (25, 27). In the multi-center retrospective study by Cortellini and coworkers, including 1070 advanced cancer patients treated with PD-1/PD-L1 inhibitors, higher BMI was significantly related to higher occurrence of G3/G4 irAEs and therapy discontinuation (25). The absence of high-grade irAEs in our series may be due to the small sample size compared to larger studies, and/or to recruitment bias. Indeed, our study was first designed to assess endocrinological AEs, hence we excluded patients with a previously diagnosed thyroid dysfunction that could potentially represents an important predisposing factor for other irAEs. Endocrinological AEs, the most common type of irAEs, are usually low grade, and, if promptly diagnosed and treated in the context of an experienced team of endocrinologists and oncologists, do not worse and/or lead to treatment discontinuation. Overall, this should be acknowledged as a limitation of our work, preventing us from conducting a more in-depth investigation into the relationship between BMI and the severity of irAEs, as demonstrated in other studies.
Overall, major strengths of the study are: (i.) access to complete information (hospital-based data) regarding patients at baseline and during ICI-treatment; (ii.) a real-life scenario, that assesses irAEs presentation and management in regular clinical practice, thereby reflecting real adherence to treatment/intervention and outcomes; (iii.) a homogeneous cohort of patients belonging to the same geographical area followed-up at a single center. Thus, this real-life study provides evidence on how treatments perform in routine clinical practice, capturing a broader and more heterogeneous patient population than controlled trials. It offers valuable insights into effectiveness, safety, and feasibility in everyday care, complementing existing literature. We have to acknowledge that the small number of patients limits subgroup analyses and precludes drawing definitive conclusions, while noting that the observed trend of higher irAE rates in overweight/obese patients with metabolic comorbidities remains an interesting finding. Further studies on larger series are needed to verify whether these results can be extrapolated to other populations and confirmed on large series.
5 Conclusions
In conclusion, despite advances in the knowledge of the peculiar profile of toxicity of ICI-based therapies, many questions regarding irAEs remain to be fully addressed. These include the role of predisposing factors like BMI and gender, as well as the possible association between occurrence of irAEs and response to ICI treatment. Also, clinical and biochemical predictors of the risk for developing irAEs are needed. In our well-characterized cohort of patients treated with ICIs, we confirmed that overweight/obesity is associated with increased risk of irAEs, with a notable predictive value, mostly when accompanied by dysmetabolic conditions. However, no clear association between BMI and immunotherapy efficacy was observed, in terms of either PFS or OS. These results may help oncologists to identify the patients who are most likely to develop irAEs, improving the management of their patients in a real-life scenario.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent from each subject for using anonymized data was obtained.
Author contributions
CS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. RR: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. AA: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. ML: Data curation, Writing – review & editing. DS: Data curation, Writing – original draft. SC: Data curation, Writing – review & editing. MB: Data curation, Writing – review & editing. MS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. (2012) 12:252–64. doi: 10.1038/nrc3239
2. Postow MA, Callahan MK, and Wolchok JD. Immune checkpoint blockade in cancer therapy. J Clin Oncol. (2015) 33:1974–82. doi: 10.1200/JCO.2014.59.4358
3. Twomey JD and Zhang B. Cancer immunotherapy update: FDA-approved checkpoint inhibitors and companion diagnostics. AAPS J. (2021) 23:39. doi: 10.1208/s12248-021-00574-0
4. Motzer RJ, Escudier B, McDermott DF, George S, Hammers HJ, Srinivas S, et al. Nivolumab versus everolimus in advanced renal-cell carcinoma. N Engl J Med. (2015) 373:1803–13. doi: 10.1056/NEJMoa1510665
5. Robert C, Schachter J, Long GV, Arance A, Grob JJ, Mortier L, et al. Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med. (2015) 372:2521–32. doi: 10.1056/NEJMoa1503093
6. Ferris RL, Blumenschein G Jr., Fayette J, Guigay J, Colevas AD, Licitra L, et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N Engl J Med. (2016) 375:1856–67. doi: 10.1056/NEJMoa1602252
7. Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csoszi T, Fulop A, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. (2016) 375:1823–33. doi: 10.1056/NEJMoa1606774
8. Overman MJ, McDermott R, Leach JL, Lonardi S, Lenz HJ, Morse MA, et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): an open-label, multicentre, phase 2 study. Lancet Oncol. (2017) 18:1182–91. doi: 10.1016/S1470-2045(17)30422-9
9. Fuchs CS, Doi T, Jang RW, Muro K, Satoh T, MaChado M, et al. Safety and efficacy of pembrolizumab monotherapy in patients with previously treated advanced gastric and gastroesophageal junction cancer: phase 2 clinical KEYNOTE-059 trial. JAMA Oncol. (2018) 4:e180013. doi: 10.1001/jamaoncol.2018.0013
10. Neoadjuvant PD-1 Blockade in Resectable Lung Cancer; Nivolumab and Ipilimumab in Advanced Melanoma; Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma; Prolonged Survival in Stage III Melanoma with Ipilimumab Adjuvant Therapy; Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma; Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma; Nivolumab and Ipilimumab versus Ipilimumab in Untreated Melanoma; Rapid Eradication of a Bulky Melanoma Mass with One Dose of Immunotherapy; Genetic Basis for Clinical Response to CTLA-4 Blockade; Genetic Basis for Clinical Response to CTLA-4 Blockade in Melanoma; Nivolumab plus Ipilimumab in Advanced Melanoma; Safety and Tumor Responses with Lambrolizumab (Anti-PD-1) in Melanoma; Hepatotoxicity with Combination of Vemurafenib and Ipilimumab. N Engl J Med. (2018) 379:2185. doi: 10.1056/NEJMx180040
11. Antonia SJ, Borghaei H, Ramalingam SS, Horn L, De Castro Carpeno J, Pluzanski A, et al. Four-year survival with nivolumab in patients with previously treated advanced non-small-cell lung cancer: a pooled analysis. Lancet Oncol. (2019) 20:1395–408. doi: 10.1016/S1470-2045(19)30407-3
12. Tawbi HA, SChadendorf D, Lipson EJ, Ascierto PA, Matamala L, Castillo Gutierrez E, et al. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N Engl J Med. (2022) 386:24–34. doi: 10.1056/NEJMoa2109970
13. Gibney GT, Weiner LM, and Atkins MB. Predictive biomarkers for checkpoint inhibitor-based immunotherapy. Lancet Oncol. (2016) 17:e542–e51. doi: 10.1016/S1470-2045(16)30406-5
14. Galon J and Bruni D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat Rev Drug Discov. (2019) 18:197–218. doi: 10.1038/s41573-018-0007-y
15. Timar J and Uhlyarik A. On-target side effects of targeted therapeutics of cancer. Pathol Oncol Res. (2022) 28:1610694. doi: 10.3389/pore.2022.1610694
16. Postow MA, Sidlow R, and Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med. (2018) 378:158–68. doi: 10.1056/NEJMra1703481
17. Barroso-Sousa R, Barry WT, Garrido-Castro AC, Hodi FS, Min L, Krop IE, et al. Incidence of endocrine dysfunction following the use of different immune checkpoint inhibitor regimens: A systematic review and meta-analysis. JAMA Oncol. (2018) 4:173–82. doi: 10.1001/jamaoncol.2017.3064
18. Chang LS, Barroso-Sousa R, Tolaney SM, Hodi FS, Kaiser UB, and Min L. Endocrine toxicity of cancer immunotherapy targeting immune checkpoints. Endocr Rev. (2019) 40:17–65. doi: 10.1210/er.2018-00006
19. Ruggeri RM, Campenni A, Giuffrida G, Trimboli P, Giovanella L, Trimarchi F, et al. Endocrine and metabolic adverse effects of immune checkpoint inhibitors: an overview (what endocrinologists should know). J Endocrinol Invest. (2019) 42:745–56. doi: 10.1007/s40618-018-0984-z
20. Spagnolo CC, Giuffrida G, Cannavo S, FranChina T, Silvestris N, Ruggeri RM, et al. Management of endocrine and metabolic toxicities of immune-checkpoint inhibitors: from clinical studies to a real-life scenario. Cancers (Basel). (2022) 15. doi: 10.3390/cancers15010246
21. Spagnolo CC, Campo I, Campenni A, Cardile D, Cannavo S, Silvestris N, et al. Challenges and pitfalls in the management of endocrine toxicities from immune checkpoint inhibitors: a case presentation of synchronous thyrotoxicosis and primary adrenal insufficiency in a melanoma patient. Hormones (Athens). (2024) 23:759–64. doi: 10.1007/s42000-024-00535-0
22. Muir CA, Clifton-Bligh RJ, Long GV, Scolyer RA, Lo SN, Carlino MS, et al. Thyroid immune-related adverse events following immune checkpoint inhibitor treatment. J Clin Endocrinol Metab. (2021) 106:e3704–e13. doi: 10.1210/clinem/dgab263
23. Rubino R, Marini A, Roviello G, Presotto EM, Desideri I, Ciardetti I, et al. Endocrine-related adverse events in a large series of cancer patients treated with anti-PD1 therapy. Endocrine. (2021) 74:172–9. doi: 10.1007/s12020-021-02750-w
24. Ruggeri RM, Spagnolo CC, Alibrandi A, Silvestris N, Cannavo S, and Santarpia M. Predictors of thyroid adverse events during cancer immunotherapy: a real-life experience at a single center. J Endocrinol Invest. (2023) 46:2399–409. doi: 10.1007/s40618-023-02096-2
25. Cortellini A, Bersanelli M, Santini D, Buti S, Tiseo M, Cannita K, et al. Another side of the association between body mass index (BMI) and clinical outcomes of cancer patients receiving programmed cell death protein-1 (PD-1)/Programmed cell death-ligand 1 (PD-L1) checkpoint inhibitors: A multicentre analysis of immune-related adverse events. Eur J Cancer. (2020) 128:17–26. doi: 10.1016/j.ejca.2019.12.031
26. Cortellini A, Bersanelli M, Buti S, Cannita K, Santini D, Perrone F, et al. A multicenter study of body mass index in cancer patients treated with anti-PD-1/PD-L1 immune checkpoint inhibitors: when overweight becomes favorable. J Immunother Cancer. (2019) 7:57. doi: 10.1186/s40425-019-0527-y
27. Wang Z, Aguilar EG, Luna JI, Dunai C, Khuat LT, Le CT, et al. Paradoxical effects of obesity on T cell function during tumor progression and PD-1 checkpoint blockade. Nat Med. (2019) 25:141–51. doi: 10.1038/s41591-018-0221-5
28. Lennon H, Sperrin M, Badrick E, and Renehan AG. The obesity paradox in cancer: a review. Curr Oncol Rep. (2016) 18:56. doi: 10.1007/s11912-016-0539-4
29. Gallo M, Adinolfi V, Barucca V, Prinzi N, Renzelli V, Barrea L, et al. Expected and paradoxical effects of obesity on cancer treatment response. Rev Endocr Metab Disord. (2021) 22:681–702. doi: 10.1007/s11154-020-09597-y
30. Azam F, Latif MF, Farooq A, Tirmazy SH, AlShahrani S, Bashir S, et al. Performance status assessment by using ECOG (Eastern cooperative oncology group) score for cancer patients by oncology healthcare professionals. Case Rep Oncol. (2019) 12:728–36. doi: 10.1159/000503095
31. Freites-Martinez A, Santana N, Arias-Santiago S, and Viera A. Using the common terminology criteria for adverse events (CTCAE - version 5.0) to evaluate the severity of adverse events of anticancer therapies. Actas Dermosifiliogr (Engl Ed). (2021) 112:90–2. doi: 10.1016/j.ad.2019.05.009
32. Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. (2009) 45:228–47. doi: 10.1016/j.ejca.2008.10.026
33. Pollack RM, Kagan M, Lotem M, and Dresner-Pollak R. Baseline tsh level is associated with risk of anti-pd-1-induced thyroid dysfunction. Endocr Pract. (2019) 25:824–9. doi: 10.4158/EP-2018-0472
34. Basak EA, van der Meer JWM, Hurkmans DP, Schreurs MWJ, Oomen-de Hoop E, van der Veldt AAM, et al. Overt thyroid dysfunction and anti-thyroid antibodies predict response to anti-PD-1 immunotherapy in cancer patients. Thyroid. (2020) 30:966–73. doi: 10.1089/thy.2019.0726
35. Pollack R, Ashash A, Cahn A, Rottenberg Y, Stern H, and Dresner-Pollak R. Immune checkpoint inhibitor-induced thyroid dysfunction is associated with higher body mass index. J Clin Endocrinol Metab. (2020) 105. doi: 10.1210/clinem/dgaa458
36. Presotto EM, Rastrelli G, Desideri I, Scotti V, Gunnella S, Pimpinelli N, et al. Endocrine toxicity in cancer patients treated with nivolumab or pembrolizumab: results of a large multicentre study. J Endocrinol Invest. (2020) 43:337–45. doi: 10.1007/s40618-019-01112-8
37. Yamauchi I, Yasoda A, Matsumoto S, Sakamori Y, Kim YH, Nomura M, et al. Incidence, features, and prognosis of immune-related adverse events involving the thyroid gland induced by nivolumab. PloS One. (2019) 14:e0216954. doi: 10.1371/journal.pone.0216954
38. Kurimoto C, Inaba H, Ariyasu H, Iwakura H, Ueda Y, Uraki S, et al. Predictive and sensitive biomarkers for thyroid dysfunctions during treatment with immune-checkpoint inhibitors. Cancer Sci. (2020) 111:1468–77. doi: 10.1111/cas.14363
39. Zhang D, Shah NJ, Cook M, Blackburn M, Serzan MT, Advani S, et al. Association between body mass index and immune-related adverse events (irAEs) among advanced-stage cancer patients receiving immune checkpoint inhibitors: A pan-cancer analysis. Cancers (Basel). (2021) 13. doi: 10.3390/cancers13236109
40. Lorincz AM and Sukumar S. Molecular links between obesity and breast cancer. Endocr Relat Cancer. (2006) 13:279–92. doi: 10.1677/erc.1.00729
41. Picon-Ruiz M, Morata-Tarifa C, Valle-Goffin JJ, Friedman ER, and Slingerland JM. Obesity and adverse breast cancer risk and outcome: Mechanistic insights and strategies for intervention. CA Cancer J Clin. (2017) 67:378–97. doi: 10.3322/caac.21405
42. Sagliocchi S, Acampora L, Barone B, Crocetto F, and Dentice M. The impact of the tumor microenvironment in the dual burden of obesity-cancer link. Semin Cancer Biol. (2025) 112:36–42. doi: 10.1016/j.semcancer.2025.03.001
43. Hotamisligil GS. Inflammation, metaflammation and immunometabolic disorders. Nature. (2017) 542:177–85. doi: 10.1038/nature21363
44. Marzullo P, Minocci A, Tagliaferri MA, Guzzaloni G, Di Blasio A, De Medici C, et al. Investigations of thyroid hormones and antibodies in obesity: leptin levels are associated with thyroid autoimmunity independent of bioanthropometric, hormonal, and weight-related determinants. J Clin Endocrinol Metab. (2010) 95:3965–72. doi: 10.1210/jc.2009-2798
45. Ong KK, Kuh D, Pierce M, Franklyn JA, Medical Research Council National Survey of H, Development S, et al. Childhood weight gain and thyroid autoimmunity at age 60–64 years: the 1946 British birth cohort study. J Clin Endocrinol Metab. (2013) 98:1435–42. doi: 10.1210/jc.2012-3761
46. Eun Y, Kim IY, Sun JM, Lee J, Cha HS, Koh EM, et al. Risk factors for immune-related adverse events associated with anti-PD-1 pembrolizumab. Sci Rep. (2019) 9:14039. doi: 10.1038/s41598-019-50574-6
47. Yeung C, Kartolo A, Holstead R, Moffat GT, Hanna L, Hopman W, et al. No association between BMI and immunotoxicity or clinical outcomes for immune checkpoint inhibitors. Immunotherapy. (2022) 14:765–76. doi: 10.2217/imt-2021-0250
48. Guzman-Prado Y, Ben Shimol J, and Samson O. Body mass index and immune-related adverse events in patients on immune checkpoint inhibitor therapies: a systematic review and meta-analysis. Cancer Immunol Immunother. (2021) 70:89–100. doi: 10.1007/s00262-020-02663-z
49. You Y, Jiang C, Peng K, He W, Wang L, Jin Y, et al. The predictive value of body mass index on prognosis and adverse events of cancers treated with immunotherapy: a systematic review and meta-analysis. Cancer Immunol Immunother. (2021) 70:2323–35. doi: 10.1007/s00262-021-02858-y
50. Trestini I, Carbognin L, Bonaiuto C, Tortora G, and Bria E. The obesity paradox in cancer: clinical insights and perspectives. Eat Weight Disord. (2018) 23:185–93. doi: 10.1007/s40519-018-0489-y
51. Deiuliis J, Shah Z, Shah N, Needleman B, Mikami D, Narula V, et al. Visceral adipose inflammation in obesity is associated with critical alterations in tregulatory cell numbers. PloS One. (2011) 6:e16376. doi: 10.1371/journal.pone.0016376
52. DerSimonian R and Laird N. Meta-analysis in clinical trials. Control Clin Trials. (1986) 7:177–88. doi: 10.1016/0197-2456(86)90046-2
53. Xue D, Li N, Yang J, Men K, Li L, Jiang H, et al. Sarcopenia predicts immune-related adverse events due to anti-PD-1/PD-L1 therapy in patients with advanced lung cancer. Front Oncol. (2024) 14:1450020. doi: 10.3389/fonc.2024.1450020
54. Hu JB, Ravichandran S, Rushing C, Beasley GM, Hanks BA, Jung SH, et al. But not sarcopenia, is associated with pembrolizumab-related toxicity in patients with advanced melanoma. Anticancer Res. (2020) 40:5245–54. doi: 10.21873/anticanres.14528
55. Wang W, Xu X, Liu H, Cui Y, Han Q, Yang T, et al. The prognostic value of sarcopenia and sarcopenic obesity in patients with lung cancer receiving immunotherapy: a propensity score matching study. Oncologist. (2025) 30. doi: 10.1093/oncolo/oyaf114
56. Li S, Bao YG, and Wu B. Letter to the editor concerning “Causal associations between Sarcopenia-related traits and intervertebral disc degeneration: a two-sample mendelian randomization analysis” by Qi W, et al. Eur Spine J. (2024) 33:3291–2. doi: 10.1007/s00586-024-08291-w
57. Murphy WJ and Longo DL. The surprisingly positive association between obesity and cancer immunotherapy efficacy. JAMA. (2019) 321:1247–8. doi: 10.1001/jama.2019.0463
58. Kulkarni A and Bowers LW. The role of immune dysfunction in obesity-associated cancer risk, progression, and metastasis. Cell Mol Life Sci. (2021) 78:3423–42. doi: 10.1007/s00018-020-03752-z
59. Assumpcao JAF, Pasquarelli-do-Nascimento G, Duarte MSV, Bonamino MH, and Magalhaes KG. The ambiguous role of obesity in oncology by promoting cancer but boosting antitumor immunotherapy. J BioMed Sci. (2022) 29:12. doi: 10.1186/s12929-022-00796-0
60. Richtig G, Hoeller C, Wolf M, Wolf I, Rainer BM, Schulter G, et al. Body mass index may predict the response to ipilimumab in metastatic melanoma: An observational multi-centre study. PloS One. (2018) 13:e0204729. doi: 10.1371/journal.pone.0204729
61. Naik GS, Waikar SS, Johnson AEW, Buchbinder EI, Haq R, Hodi FS, et al. Complex inter-relationship of body mass index, gender and serum creatinine on survival: exploring the obesity paradox in melanoma patients treated with checkpoint inhibition. J Immunother Cancer. (2019) 7:89. doi: 10.1186/s40425-019-0512-5
Keywords: immune checkpoint inhibitor, body mass index, immune-related adverse events, obesity, gender
Citation: Spagnolo CC, Ruggeri RM, Alibrandi A, Laganà M, Speranza D, Cannavò S, Berretta M and Santarpia M (2025) Immune checkpoint inhibitor-induced toxicity: a real-world analysis of the role of BMI. Front. Oncol. 15:1659977. doi: 10.3389/fonc.2025.1659977
Received: 04 July 2025; Accepted: 21 October 2025;
Published: 06 November 2025.
Edited by:
Zoe Quandt, University of California, San Francisco, United StatesReviewed by:
Muhammad Zaki Fadlullah Wilmot, The University of Utah, United StatesSwastik Pandita, Rajiv Gandhi University of Health Sciences, India
Copyright © 2025 Spagnolo, Ruggeri, Alibrandi, Laganà, Speranza, Cannavò, Berretta and Santarpia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mariacarmela Santarpia, bWFyaWFjYXJtZWxhLnNhbnRhcnBpYUB1bmltZS5pdA==
†These authors have contributed equally to this work and share first authorship