 Henrique Lima Couto1,2*
Henrique Lima Couto1,2* Bertha Andrade Coelho2,3,4†
Bertha Andrade Coelho2,3,4† Bernardo Ferreira de Paula Ricardo5†
Bernardo Ferreira de Paula Ricardo5† Paola Hartung Toppa6,7
Paola Hartung Toppa6,7 Aleida Nazareth Soares6,8Bruna Torres Silvestre da Silva1†Douglas de Miranda Pires1,2,9†
Aleida Nazareth Soares6,8Bruna Torres Silvestre da Silva1†Douglas de Miranda Pires1,2,9† Tereza Cristina de Oliveira Ferreira1†Paula Clarke1,2,10
Tereza Cristina de Oliveira Ferreira1†Paula Clarke1,2,10 Shirley das Graças Ferreira1,2†Larissa Barbosa Oliveira1,2
Shirley das Graças Ferreira1,2†Larissa Barbosa Oliveira1,2 Romana Giordani Ribeiro Saliba1,2†Paula Cristina Martins Soares1,2Thais Paiva Moraes1,2,11Ana Carolina Guglielmelli Mendonça1,2Amanda Cristina Braga de Oliveira1,2†Daniela Rodrigues Siqueira1,2Jane Sanglard de Oliveira1,2,9†Charles Andreé Joseph de Padua12†Geraldo Felício Cunha Jr12Marcus Simões Castilho13Bárbara Pace Silva Assis Carvalho2,14,15Gabriel de Almeida Silva Jr2,16†Waldeir José de Almeida Júnior2,6,11†
Romana Giordani Ribeiro Saliba1,2†Paula Cristina Martins Soares1,2Thais Paiva Moraes1,2,11Ana Carolina Guglielmelli Mendonça1,2Amanda Cristina Braga de Oliveira1,2†Daniela Rodrigues Siqueira1,2Jane Sanglard de Oliveira1,2,9†Charles Andreé Joseph de Padua12†Geraldo Felício Cunha Jr12Marcus Simões Castilho13Bárbara Pace Silva Assis Carvalho2,14,15Gabriel de Almeida Silva Jr2,16†Waldeir José de Almeida Júnior2,6,11† Clecio Ênio Murta de Lucena2,16,17†Eduardo Carvalho Pessoa18Annamaria Massahud Rodrigues dos Santos16,19†Heverton Leal Ernesto de Amorim20†
Clecio Ênio Murta de Lucena2,16,17†Eduardo Carvalho Pessoa18Annamaria Massahud Rodrigues dos Santos16,19†Heverton Leal Ernesto de Amorim20† Ruffo Freitas-Junior21†Marcus Nascimento Borges21
Ruffo Freitas-Junior21†Marcus Nascimento Borges21 Andre Mattar22
Andre Mattar22 Marcelo Antonini23Daniel de Araújo Brito Buttros18,24†Lorena Lima Coto Dominguez1
Marcelo Antonini23Daniel de Araújo Brito Buttros18,24†Lorena Lima Coto Dominguez1 Bruna Pires1
Bruna Pires1 Carolina Nazareth Valadares25†Fernando Marcos dos Reis17†
Carolina Nazareth Valadares25†Fernando Marcos dos Reis17†- 1Redimama-Redimasto, Belo Horizonte, Brazil
- 2Brazilian Society of Mastology, Belo Horizonte, Brazil
- 3UNIFIPMOC University Center, Montes Claros, Brazil
- 4MaterMOC Breast Unit, Montes Claros, Brazil
- 5Anatomia Laboratory, Belo Horizonte, Brazil
- 6Faculty of Medical Sciences of Minas Gerais, Belo Horizonte, Brazil
- 7Analysis Laboratory, Belo Horizonte, Brazil
- 8Santa Casa College BH, Belo Horizonte, Brazil
- 9Santa Casa de Misericordia de Belo Horizonte, Belo Horizonte, Brazil
- 10Military Hospital (ISPM), Belo Horizonte, Brazil
- 11Mater Dei Hospital, Belo Horizonte, Brazil
- 12Cetus Oncology Belo Horizonte, Belo Horizonte, Brazil
- 13Radiocare, Belo Horizonte, Brazil
- 14Oncoclinicas, Belo Horizonte, Brazil
- 15Diagnostic Imaging Sonar, Belo Horizonte, Brazil
- 16Orizonti Institute, Belo Horizonte, Brazil
- 17Federal University of Minas Gerais, Belo Horizonte, Brazil
- 18São Paulo State University Júlio de Mesquita Filho, School of Medicine, Botucatu, Brazil
- 19Minas Gerais State Servants Welfare Institute, Belo Horizonte, Brazil
- 20UD Diagnosis, João Pessoa, Brazil
- 21Federal University of Goiás, Goiânia, Brazil
- 22Women Hospital, São Paulo, Brazil
- 23Hospital of the State Public Servant of São Paulo, São Paulo, Brazil
- 24Claretian University Center, Rio Claro, Brazil
- 25Hospital Paulistano, São Paulo, Brazil
Introduction: Vacuum-assisted excision (VAE) of breast lesions is a technique used for diagnostic and therapeutic purposes and is performed on an outpatient basis, with local anesthesia and image guidance. Currently, VAE is used in the management of benign lesions and lesions of uncertain malignant potential (B3 lesions). More recently, there has been interest in VAE for the percutaneous treatment of small breast cancers, the aim of which was to reduce morbidity and aggressive surgical treatment. Due to how conventional VAE is performed, histopathological assessment of the resection margins is not possible. Obtaining free margins after a breast cancer resection is a primary objective in the surgical treatment of this disease. If VAE could ensure free margins and the absence of residual tumor in the surgical excision, it would represent a safe method for a minimally invasive treatment, providing an effective percutaneous treatment of small early breast cancers.
Methods: The prospective VAE-BREAST 01 study explores the role of VAE associated with cavity margin sample shaving (CMSH) as a one-step approach in the diagnosis and complete excision of small breast tumors, ensuring the absence of residual disease in surgical pathology. Women with lesions smaller than 1.5 cm, ACR BI-RADS™ (American College of Radiology Breast Imaging Reporting and Data System) category 4 or 5, and identified by screening or clinical alteration are included. Multifocal, multicentric breast cancers and breast cancers associated with diffuse and extensive calcifications are excluded. The sensitivity, specificity, accuracy, positive predictive value, negative predictive value, and the false-negative and false-positive rates of VAE+CMSH for the complete excision of breast cancers will be calculated. The collected data also will include patients’ demographics, image characteristics of the lesions, information regarding the VAE+CMSH and surgical procedure, biopsy and surgical pathology, and data on side effects, patient acceptance, cosmetic results, and patients’ experiences during VAE.
Ethics and dissemination: Ethics approval was obtained from the Brazilian National Research Ethics Commission (CONEP). Participants will provide written informed consent, and researchers will follow institutional guidelines for data collection and management.
Clinical Trial Registration: https://ensaiosclinicos.gov.br/, identifier U1111-1301-4235
Highlights
● Our prospective study will provide valuable information on the potential role of VAE+CMSH in the percutaneous treatment of small breast cancers.
Introduction
Breast cancer is an extremely heterogeneous and multifactorial disease. With the establishment of systematic population screening, the majority of diagnosed tumors by screening are small and non-palpable. Screening mammography has been associated with a moderate reduction in mortality from breast cancer in women aged 40–70 years (1–3). Benchmarks reported by the Breast Cancer Surveillance Consortium for mammography screening include a median tumor size of 14 mm, 77.3% node-negative cancers, 52.6% minimal cancers (<1 cm invasive cancers or in situ), and 74.8% stage 0 and 1 cancers (4).
Breast cancer treatment has undergone numerous changes and advances, leading to the current era of personalized and precision treatment (5). The establishment of mammographic screening programs has increased the diagnosis of small breast cancers, many of which have favorable biological characteristics. Some of these tumors have excellent long-term outcomes, with the 10-year breast cancer-specific survival approaching 100% (1). Such tumors may never become symptomatic within a patient’s lifetime due to their indolent nature may thus represent overdiagnosis (3, 6, 7). It is estimated that, for every breast cancer death prevented by screening, three cancers were overdiagnosed and consequently overtreated (3, 4, 6, 7). There still remains no method to identify which cancers are likely to be overtreated. Thus, there is increasing interest in the de-escalation of locoregional therapies for small screen-detected breast cancers.
It is crucial to find a balance between early detection and the treatments offered, promoting a more personalized and balanced approach to the management of breast lesions. Recently, the omission of sentinel node biopsy (SNB) has been recognized as a standard approach for early T1N0(us) breast cancers with good prognosis in women over 50 years, with important reduction of the harms of surgical treatment (8–13). It is of utmost importance to note that the majority of cancers detected in screening programs are small, node-negative, and hormone receptor-positive cancers eligible for SNB omission (4, 11).
Diagnostic imaging and percutaneous interventions are increasingly playing a key role in the management of patients with breast abnormalities, from fibroadenoma to lesions of uncertain malignant potential (B3 lesions) in core needle biopsy (14–20). Vacuum-assisted excision (VAE) can completely excise small breast cancers. However, until now, it is not possible to ensure complete excision with free margins without conventional surgery (21).
SMALL is a prospective, multicenter, randomized phase III trial of VAE versus surgery in patients with small, biologically favorable, screen-detected invasive breast cancer. VAE could potentially reduce the morbidity and surgical overtreatment of screen-detected estrogen cancers with good prognosis (22). However, with conventional VAE, it is currently not possible to assess the margin status. This new trial aimed to evaluate the efficiency of VAE combined with percutaneous cavity margin sample shaving (CMSH) in predicting complete excision of breast cancers smaller than 1.5 cm using a one-step diagnostic–treatment approach for ACR BI-RADS™ (American College of Radiology Breast Imaging Reporting and Data System) category 4 or 5 lesions (23).
Methods
Study design
This is a phase 2, prospective, non-randomized clinical trial recruiting patients with ACR BI-RADS™ category 4 or 5 mammographic or sonographic breast lesions smaller than 1.5 cm (Figure 1). The aim was to evaluate the efficiency of VAE+CMSH in predicting complete excision of breast cancers [invasive cancers (IC) and ductal carcinoma in situ (DCIS)] smaller than 1.5 cm in a one-step diagnostic–treatment approach for ACR BI-RADS™ category 4 or 5 lesions. The CMSH immediately after VAE is a diagnostic test to predict complete percutaneous excision and will be evaluated based on the sensitivity, specificity, accuracy, positive predictive value (PPV), negative predictive value (NPV), false-negative rate (FNR), and false-positive rate (FPR). The CMSH will be considered the diagnostic test in the evaluation and the surgery the gold standard. CMSH negative (no tumor cells in the samples) or positive (with tumor cells in the samples) results will be compared with the gold standard excision/surgery negative (no residual tumor cells) or positive (presence of residual tumor cells) results.
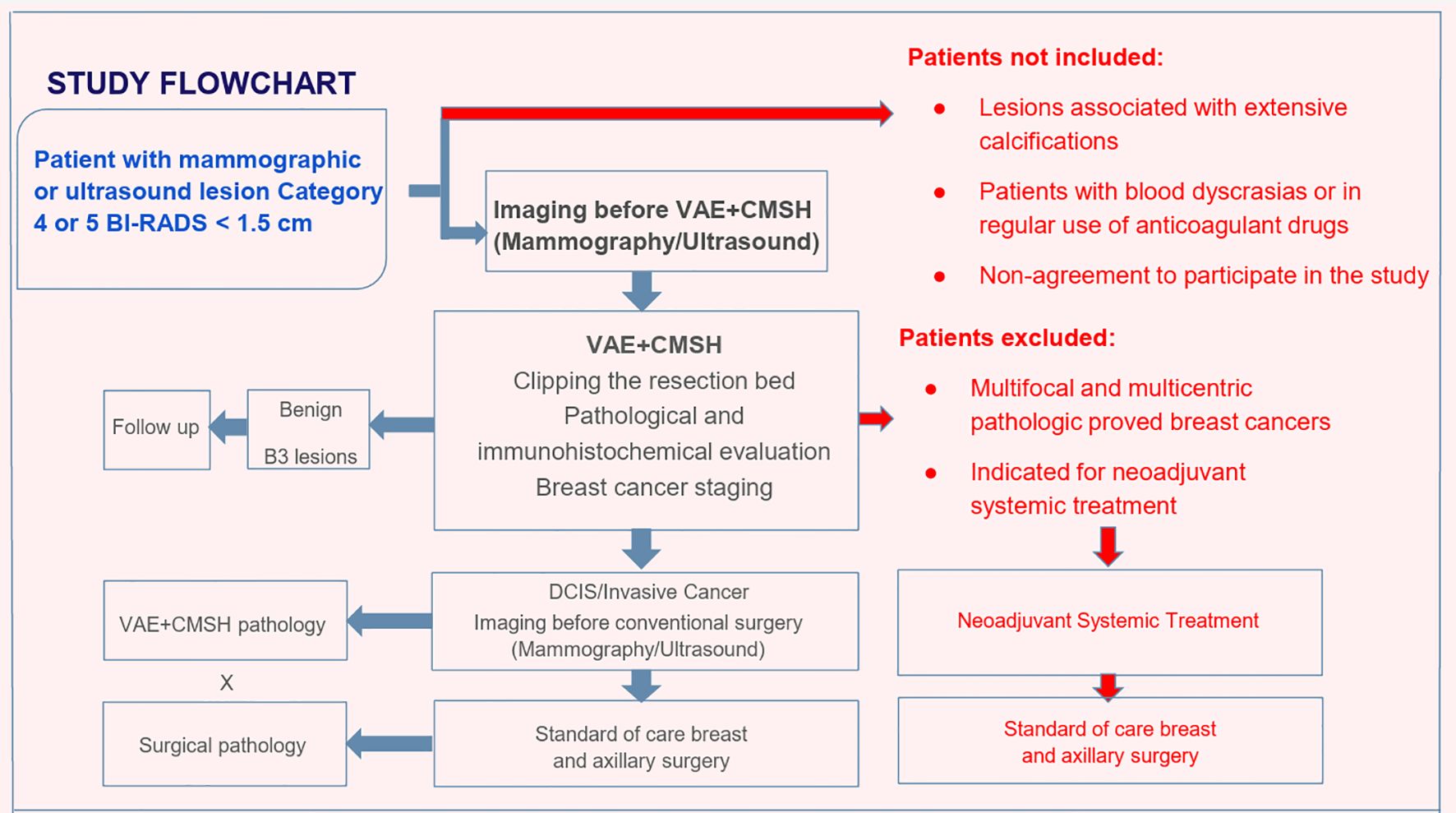
Figure 1. Study flowchart. VAE, vacuum-assisted excision; CMSH, cavity margin sample shaving; B3 lesions, lesions of uncertain malignant potential in core needle biopsy; DCIS, ductal carcinoma in situ.
Study setting
The procedures are realized in an outpatient basis at two Breast Units in the state of Minas Gerais, Brazil.
Study duration
The first patient was recruited on November 29, 2023. Recruitment is estimated to end in December 2026.
Eligibility criteria
Women with ACR BI-RADS™ category 4 or 5 lesions smaller than 1.5 cm identified by screening or clinical alteration, who are literate, and are aged over 18 years are included. The exclusion criteria were: multifocal and multicentric pathologically proven breast cancers, lesions associated with diffuse and extensive calcifications, patients with blood dyscrasias or in regular use of anticoagulant drugs, and non-agreement to participation in the study. Patients indicated for neoadjuvant systemic treatment after VAE+CMSH are also excluded (Figure 1).
Interventions and patient pathways
Patients with mammographic or sonographic lesions (≤1.5 cm) classified as ACR BI-RADS categories 4–5 will undergo VAE+CMSH (Figure 1).
If the pathological diagnosis reveals a benign lesion, the patient is discharged and returned to routine screening. If the pathological diagnosis indicates a B3 lesion, the case is discussed by a multidisciplinary team, and the patient is preferably monitored or undergoes surgical excision, in case of imaging–pathology discordance. All types of B3 lesions are allowed to be followed without surgical excision. The final multidisciplinary decision is absolute.
If malignancy is diagnosed (DCIS or IC), the patient is staged and submitted to standard primary surgical treatment, regardless of the CMSH result, according to the Brazilian Guideline for Breast Cancer Diagnosis and Treatment from the Brazilian Health Department (24), and the surgical pathology is compared with the VAE+CMSH pathology.
Patients with pathologically confirmed multifocal or multicentric disease in the preoperative stage are excluded. Patients indicated for neoadjuvant systemic treatment, according to the Brazilian Guideline for Breast Cancer Diagnosis and Treatment from the Brazilian Health Department (24), after VAE+CMSH are also excluded.
Imaging
All patients are submitted to mammography and breast ultrasound before VAE+CMSH. Only those with ≤1.5-cm lesions classified as ACR BI-RADS categories 4–5 in both methods will undergo VAE+CMSH. If two lesions are detected in a patient, these are recorded as individual lesions, unless they proven to be multifocal or multicentric breast cancer, in which case they are excluded (Figure 1). Magnetic resonance imaging (MRI) of the breast or contrast-enhanced mammography (CEM) is not considered in the inclusion or exclusion criteria and is allowed at the discretion of the multidisciplinary team in charge. If requested at any time, the lesion measurement in the MRI or CEM is not applied as an inclusion or an exclusion criterion.
VAE+CMSH standard procedure
All procedures are performed by mastologists or breast-dedicated radiologists experienced in VAE by ultrasound or stereotactically. In Brazil, mastology is a specialty. Brazilian mastologists are trained and qualified physicians in the specialty of mastology with the skills to study, prevent, diagnose, and treat diseases, congenital and/or acquired conditions of the breasts, promoting and executing the necessary therapeutic means, whether clinical, surgical, reparative, and/or palliative. Mastologists master the execution of fine needle aspiration (FNA) biopsy, core needle biopsy (CNB), vacuum-assisted biopsy (VAB), and/or VAE, guided or unguided by imaging methods (25).
The VAE+CMSH procedure is always performed on an outpatient basis with local anesthesia. A 7-G or a 10-G needle is used at the discretion of the performing physician according to each case and patient features, such as distance from the skin and the pectoralis muscle and implants, among others (Figure 2).
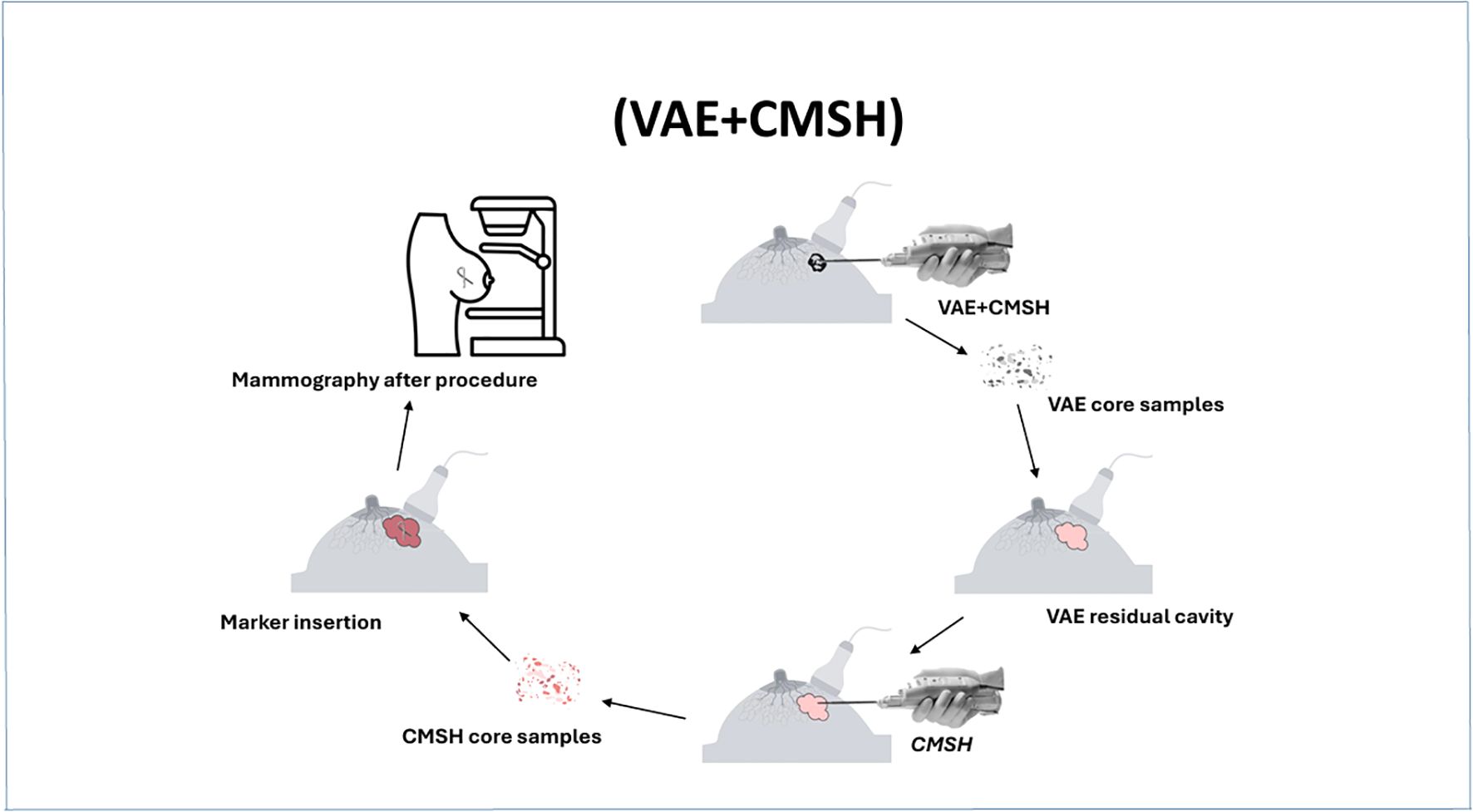
Figure 2. Standard protocol of vacuum-assisted excision (VAE) and cavity margin sample shaving (CMSH).
The VAE step of the procedure consists in carrying out the number of core samples necessary for the complete excision of the lesion. The excision is always performed in round circles of 12 samples, and so on, with the Encore Inspire™ device. The VAE step ends with the last round circle after removal of the lesion. The number of VAE samples is recorded in the report and then sent to the pathologist in a special bottle labeled VAE.
CMSH consists of, after documenting the complete excision of the lesion, rinsing the needle (when guided by ultrasound), performing another round of 12 core samples, and sending these to the pathologist in a separate bottle as CMSH evaluation (Figure 3). Evidently, when performed stereotactically, the step of rinsing the needle is not required. The biopsy site is then clipped, followed by immediate mammographic confirmation of clip placement and recording any complications and the procedure time.
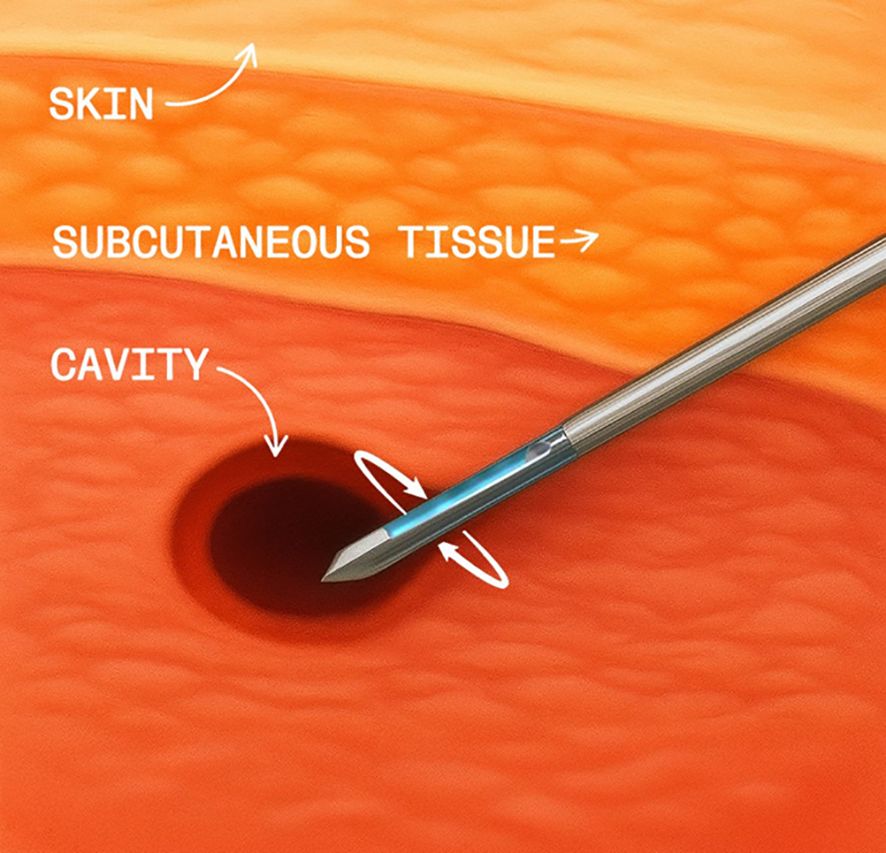
Figure 3. Cavity margin sample shaving (CMSH).
Surgical procedure
Surgical excision is mandatory and is performed for all cases of malignancy (DCIS/IC) in VAE+CMSH. After surgery, the surgical specimen is radiographed to confirm the presence of the marker placed during VAE+CMSH. Surgical treatment, breast conservation or mastectomy, and axillary surgery are performed according to clinical practice and standard of surgical care. Patients are submitted to no axillary surgery (omission of SNB), SNB, or axillary clearance according to standard of care (11, 24).
VAE+CMSH pathology
Gross specimens are separated from the clots, measured, weighed, and inked. Total inclusion of the fragments is performed, and slices are cut every 4 μm. Tests range from the usual hematoxylin–eosin (HE) analysis on slides, with or without immunohistochemistry and at the discretion of the case by the pathologist, to follow-up with fluorescence in situ hybridization (FISH) and genetic analyses (e.g., oncotype), if indicated. All tissue samples are submitted for histopathological evaluation. The maximum pathological tumor size following VAE+CMSH is defined as the measure of the maximum size of the tumor in the slide of the greatest core sample compromised by the tumor. Following assessment, the VAE+CMSH pathology diagnosis (i.e., benign, B3 lesion, and DCIS or IC), the presence of DCIS with comedonecrosis, the biomarker status (e.g., ER/PR/HER2/Ki67), the morphological tumor type, and the nuclear and histological grades are all recorded.
Surgical pathology
Gross surgical specimens are measured, weighed, and inked. All surgically excised tissue is submitted for histopathological evaluation, and slices are cut every 4 μm. Tests range from the usual HE analysis on slides, with or without immunohistochemistry and at the discretion of the case by the pathologist, to follow-up with FISH and genetic analyses (e.g., oncotype), if indicated. Following assessment, the margins status, the maximum pathological residual tumor size, the diagnosis (i.e., benign, B3 lesion, and DCIS or IC), the presence of DCIS with comedonecrosis, multifocality, the biomarker status (e.g., ER/PR/HER2/Ki67), the morphological tumor type, and the nuclear and histological grades are all recorded.
Staging
All malignancies (DCIS/IC) are staged following the AJCC Cancer Staging Manual (26). Following the AJCC recommendation, the pathological tumor size (pT) based on gross measurement may be somewhat inaccurate. Microscopic assessment is preferred as it can distinguish fibrosis and noninvasive or invasive carcinoma. The microscopically determined pT is based on measurement of only the invasive component. For small invasive tumors that can be submitted in one section or paraffin block, microscopic measurement is the most accurate way to determine the pT. In some situations, systematic pathology evaluation allows microscopic reconstruction of the tumor; however, reconstruction measurements are correlated with the gross and imaging size before assignment of the pT (26). The AJCC emphasizes that, in patients who have undergone diagnostic vacuum-assisted core needle biopsy (VAB) sampling prior to surgical excision, measuring only the residual tumor may result in the underclassification of the T category and the understaging of the tumor, particularly with smaller tumors. In such cases, the original invasive cancer size is estimated and verified based on the best combination of the imaging, gross, and microscopic histological findings. Adding the maximum invasive cancer dimension on the VAB to the residual invasive tumor in the excision is not recommended as this method often overestimates the maximum tumor dimension. In general, the maximum dimension in either the VAB or the excisional biopsy is used for T categorization, unless the imaging dimensions suggest a larger invasive cancer (26). In the VAE BREAST 01 trial, the above AJCC recommendations for small tumors and tumors submitted to VAB prior to surgery are applied.
Adjuvant treatment and follow-up
All patients receive adjuvant systemic therapy and radiotherapy according to the Brazilian Guideline for Breast Cancer Diagnosis and Treatment from the Brazilian Health Department (24).
Outcomes
Primary outcome measures
The sensitivity, specificity, accuracy, PPV, NPV, FNR, and FPR of VAE+CMSH in predicting complete excision of breast cancers smaller than 1.5 cm in a one-step diagnostic–treatment approach will be calculated.
Secondary outcome measures
1. Evaluate the VAE+CMSH protocol defined complications and their management: bruises, skin lacerations, and unsuccessful procedures. Specifically for bruises, a scale was developed for quantification and classification (Table 1). The need for surgical drainage of VAE hematomas is also recorded.
2. Evaluate acceptance, cosmetic results, and satisfaction using The Breast-Q Questionnaire ICHOM Pre- and Postoperative Scales (27) in patients who have undergone VAE+CMSH and therapeutic breast surgery. Patients will be interviewed after VAE+CMSH and after therapeutic breast surgery and the results compared.
3. Evaluate the incidence of benign lesions, B3 lesions, and breast cancers (DCIS/IC) in ACR BI-RADS category 4–5 lesions ≤1.5 cm in mammography or ultrasound in the recent era.
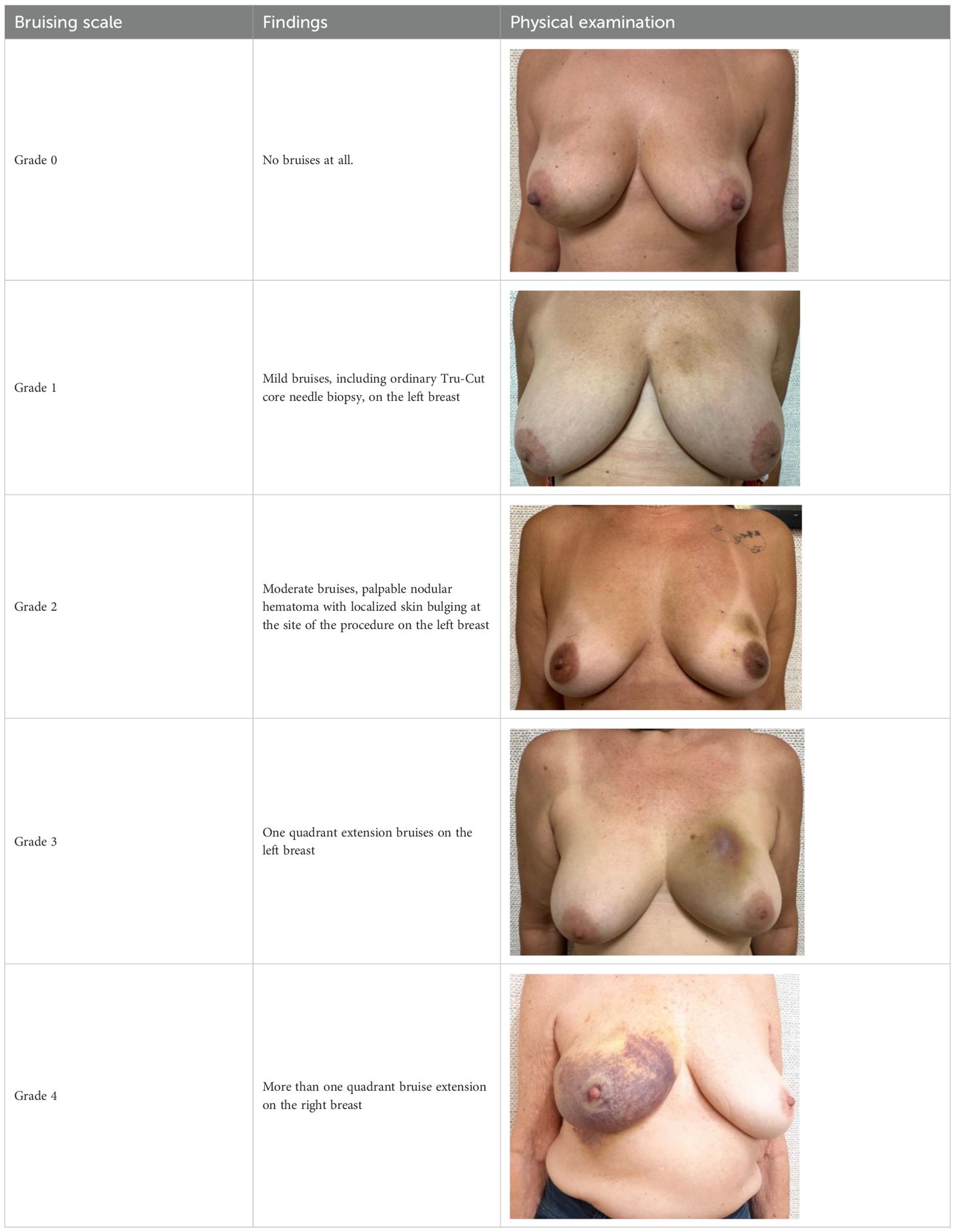
Table 1. Bruising scale after vacuum-assisted excision (VAE).
Sample size calculation
The total sample size to be recruited is 353 patients based on a PPV3 of 35.9% (range = 20%–40%) for cancer in biopsies of ACR BI-RADS category 4–5 lesions (23), a margin of error of 5%, a 95% confidence interval, a FNR of the diagnostic test below 10%, and the availability of 100 positive cases. The 10% FNR refers to the minimum standard threshold at which all breast cancer de-escalation strategies have been proven effective (28).
Healthy economic outcomes
If VAE+CMSH is proven to be an effective approach, the cost-effectiveness of upfront VAE+CMSH for the one-step diagnosis and excision of ≤1.5-cm ACR BI-RADS category 4–5 lesions versus the traditional CNB and subsequent surgery approach, when indicated, will be estimated based on the Brazilian Data on Breast Cancer (29), the Brazilian Methodological Guidelines for Economic Evaluation Studies of Health Technologies (30), and the recommendations from the National Commission for the Incorporation of Technologies into Unified Health System (CONITEC) (31), the Brazilian Public Health System (SUS).
Mammographic and ultrasonographic image library
VAE BREAST-01 will generate a library of de-identified mammographic and sonographic breast images, with the aim being for future studies to identify potential image features that could determine cases where VAE+CMSH is associated with early breast cancer complete excision.
Ethics and dissemination
Ethics approval was obtained from the Brazilian National Research Ethics Commission (CONEP). Participants will provide written informed consent, and researchers will follow institutional guidelines for data collection and management (Clinical Trial Registration: https://ensaiosclinicos.gov.br/; identifier: U1111-1301-4235). Data will be available at reasonable request to the chief investigator on completion of the trial and after publication of the results. The study results will be published in a peer-reviewed journal and presented at relevant specialty conferences. The findings will be shared with the relevant professional organizations to inform future guideline development.
Discussion
Currently, there are several scenarios in which breast surgery can be omitted when lesions are treated using VAE: fibroadenomas and lesions of uncertain malignant potential are some examples (14–20). Active surveillance of DCIS with a low risk of progression to invasive cancer (32), percutaneous treatment of DCIS (33, 34), and small invasive breast tumors (21, 22, 35) are also under investigation.
The median breast cancer tumor size has decreased over the years due to mammographic screening. Breast cancers diagnosed in mammographic screening programs tend to be less aggressive luminal cancers, and some of them may represent overdiagnosis (3, 6, 7). Quality indicator goals for screening include a median tumor size of 14 mm, 77.3% node-negative cancers, 52.6% minimal cancers (<1 cm invasive cancers or in situ), and 74.8% stage 0 and 1 cancers (4, 23). The current guideline for axillary surgery recommends the omission of SNB in select patients who are postmenopausal and ≥50 years of age and in those with negative findings on preoperative axillary ultrasound for grade 1–2 small (≤2 cm), hormone receptor-positive, human epidermal growth factor receptor 2 (HER2)-negative breast cancers and who underwent breast-conserving therapy (11). A large portion of screen-detected breast cancer would be potentially excised using VAE, reducing the aggressiveness of surgical treatment and the impact of overtreatment.
Our group first study published evaluating the role of VAB (not VAE) in the excision of small malignant tumors reported 25% complete resection. However, in this series, CMSH was not obtained (21). Other studies have demonstrated that the use of VAB complete excision was possible in 18%–48.9% of cases (36–38), although none of these evaluated CMSH. Thus, the addition of the CMSH step could increase the chance and predict complete excision of a malignant tumor (35).
Free surgical margins are a determining factor in minimizing the local recurrence of breast cancer (39–42). However, the pursuit of wide margins must be balanced with the preservation of healthy tissue and the patient’s quality of life (43–46). Wider margins are unlikely to have additional benefits for the long-term local control of disease, and no ink on the tumor is sufficient for invasive disease, with a margin of 2 mm recommended for DCIS (39, 40). Analyzing this scenario, VAE+CMSH could be an approach for the complete excision of small breast cancers (DCIS/IC), minimizing the unnecessary excision of healthy tissue and reducing overtreatment.
It is a goal to reduce the healthcare interval of breast cancer. Delays in initiating breast cancer treatment are associated with significantly worse survival, particularly for cancer-specific mortality (47). Treatment interval (TI) is the time between the pathological diagnosis and the initiation of treatment (48). A recent meta-analysis has demonstrated that each additional 4-week delay in initiating treatment increases the risk of death by over 10%, underscoring the urgency of minimizing delays in diagnosis-to-treatment pathways (47). In Brazil, 21.5% of women with breast cancer take 31–60 days between diagnosis and treatment initiation, and 56.3% take more than 60 days (29). VAE+CMSH, as a one-step diagnosis and excision approach, could be useful in reducing the TI, particularly in countries where access to surgical treatment is difficult.
The incidence of B3 lesions varies between 3% and 21%, with higher rates in screening populations (49, 50). B3 lesions on CNB are currently mostly managed by second-line VAE (16–20). The estimated PPV3 of diagnostic imaging is 35.9% for cancer in biopsies of ACR BI-RADS category 4–5 lesions (23). There are no reliable data on the incidence of B3 lesions in VAEs of ≤15-mm ACR BI-RADS category 4–5 lesions. It is quite possible that more than 50% of these biopsies will present a B3 lesion diagnosis or small breast cancer. If upfront VAE+CMSH is successful in excising these lesions with free margins, this benefit could outweigh the adverse effects of, eventually, a more extensive procedure compared with ordinary Tru-Cut CNB for benign lesions.
There is great concern among surgeons whether VAE hematoma could lead to wider breast procedures or increase the mastectomy rate or compromised margins in breast cancer excisions after VAE-CMSH. In fact, the hematoma is confined to a cavity that contains the clip. The appropriate management of breast surgical excision after VAE-CMSH is excision of the cavity containing the clip. This excision can be performed at any time following VAE-CMSH, depending on the decision of the attending surgeon. Typically, even grade 3 or 4 hematomas are resolved within 30–60 days (51). The study will record the interval between VAE and surgery, the type of surgery performed (either breast-conserving surgery or mastectomy), the indication for each procedure, and the incidence of compromised surgical margins on breast surgery after VAE-CMSH.
There is the concern about completely excising an invasive triple-negative (TNBC) or HER2-positive breast cancer, which should be submitted to neoadjuvant chemotherapy (NAC) instead of upfront surgery. The majority of screen-detected small breast cancers are hormone receptor-positive cancers with good prognosis. TNBC or HER2-positive breast cancer is not generally diagnosed by mammographic screening or is ≤15 mm (6, 52). Early breast cancer guidelines recommend NAC for HER2-positive stage II or III breast cancer (>20 mm or N1) (8, 53).
HER2-positive breast cancers ≤15 mm associated with metastatic axillary nodes are candidates for NAC (8, 53). After VAE-CMSH diagnosing IC, the patient is staged, including axillary ultrasound evaluation and immunohistochemistry. In the case of pT1N1 HER2-positive IC, the patient is excluded and indicated for NAC. After NAC, the clipped breast tumor bed and axillary nodes are evaluated for residual disease according to standard of care (8, 53).
Early breast cancer guidelines recommend upfront surgery for ≤10-mm TNBC. In general, for T1c TNBC, the usual recommendation is NAC (8, 53). Nevertheless, no prospective double-blind randomized clinical trial has evaluated upfront surgery followed by NAC versus NAC followed by surgery for T1cN0 TNBC. Retrospective data showed that T1N0 TNBC submitted to upfront surgery followed by adjuvant chemotherapy did not have inferior outcomes compared with those who received NAC followed by surgery. However, patients with T1c tumors who achieved complete pathologic response to NAC had the best outcomes, suggesting that NAC provides important prognostic information that can guide adjuvant treatments (54). However, based on the results of CREATE-X, adjuvant capecitabine leads to improvements in overall survival (OS) and invasive disease-free survival (DFS) in patients with early TNBC and evidence of residual disease following NAC, with the population of T1 patients being poorly represented (14.7%) (55). Specifically, in relation to T1c (11–15 mm) TNBC, the data are scarcer. On the other hand, there is good evidence that delaying the initiation of adjuvant chemotherapy is critical for TNBC, particularly for stage IA (T1N0) (56). The diagnosis and treatment of ≤15-mm TNBC with a one-step procedure could reduce the time to adjuvant chemotherapy and improve prognosis.
Conclusion
This trial design will provide an opportunity to standardize VAE associated with the CMSH procedure, as well as will evaluate its efficacy in achieving complete excision with clear margins in small breast cancers and other breast lesions ≤1.5 cm. The results of this trial will be crucial for advancing the de-escalation of breast cancer treatment.
Ethics statement
The study was approved by Brazilian National Research Ethics Comission. The study was conducted in accordance with local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
HC: Methodology, Formal analysis, Writing – review & editing, Software, Supervision, Investigation, Writing – original draft, Visualization, Conceptualization, Validation, Funding acquisition, Data curation, Project administration, Resources. BC: Investigation, Writing – original draft, Resources, Funding acquisition, Visualization, Software, Formal analysis, Validation, Conceptualization, Data curation, Project administration, Supervision, Writing – review & editing, Methodology. BR: Writing – review & editing, Investigation, Data curation, Validation. PT: Writing – review & editing, Validation, Data curation, Investigation. ANS: Methodology, Investigation, Formal analysis, Writing – review & editing. BS: Methodology, Formal analysis, Investigation, Writing – review & editing. DP: Data curation, Writing – review & editing, Investigation. TO: Data curation, Writing – review & editing, Investigation. PC: Methodology, Writing – review & editing, Investigation. SF: Writing – review & editing, Investigation, Data curation. LO: Investigation, Data curation, Writing – review & editing. RS: Data curation, Investigation, Writing – review & editing. PS: Investigation, Writing – review & editing, Data curation. TM: Investigation, Writing – review & editing. AM: Writing – review & editing, Investigation. AO: Investigation, Writing – review & editing. DS: Investigation, Writing – review & editing, Data curation. JO: Writing – review & editing, Data curation. CP: Validation, Methodology, Investigation, Writing – review & editing. GC: Methodology, Validation, Writing – review & editing. MC: Data curation, Methodology, Validation, Writing – review & editing, Investigation. BAC: Investigation, Writing – review & editing. GS: Investigation, Writing – review & editing. WS: Investigation, Writing – review & editing. CL: Writing – review & editing, Investigation. EP: Writing – review & editing, Investigation, Methodology. ARS: Investigation, Writing – review & editing. HA: Methodology, Writing – review & editing. RF: Writing – review & editing, Investigation. MB: Investigation, Writing – review & editing. AM: Investigation, Writing – review & editing. MA: Methodology, Writing – review & editing. DB: Methodology, Writing – review & editing. LD: Investigation, Writing – review & editing. BP: Writing – review & editing, Data curation. CV: Writing – review & editing, Methodology. FR: Writing – review & editing, Validation.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. This research is partially funded by the BD.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Fuller MS, Lee CI, and Elmore JG. Breast cancer screening: an evidence-based update. Med Clin North Am. (2015) 99:451–68. doi: 10.1016/j.mcna.2015.01.002
2. Gøtzsche PC and Jørgensen KJ. Screening for breast cancer with mammography. Cochrane Database Syst Rev. (2013) 2013:CD001877. doi: 10.1002/14651858.CD001877.pub5
3. Welch HG, Prorok PC, O’Malley AJ, and Kramer BS. Breast-cancer tumor size, overdiagnosis, and mammography screening effectiveness. N Engl J Med. (2016) 375:1438–47. doi: 10.1056/NEJMoa1600249
4. Breast Cancer Surveillance Consortium. Screening performance benchmarks. Available online at: https://www.bcsc-research.org/statistics/screening-performance-benchmarks (Accessed October 5, 2025).
5. Sarhangi N, Hajjari S, Heydari SF, Ganjizadeh M, Rouhollah F, and Hasanzad M. Breast cancer in the era of precision medicine. Mol Biol Rep. (2022) 49:10023–37. doi: 10.1007/s11033-022-07571-2
6. Wallis MG. How do we manage overdiagnosis/overtreatment in breast screening? Clin Radiol. (2018) 73:372–80. doi: 10.1016/j.crad.2017.09.016
7. Nelson HD, Pappas M, Cantor A, Griffin J, Daeges M, and Humphrey L. Ann harms of breast cancer screening: systematic review to update the 2009 U.S. Prev Serv Task Force Recommendation Intern Med. (2016) 164:256–67. doi: 10.7326/M15-0970
8. Loibl S, André F, Bachelot T, Barrios CH, Bergh J, Burstein HJ, et al. ESMO Guidelines Committee. Electronic address:Y2xpbmljYWxndWlkZWxpbmVzQGVzbW8ub3Jn. Early breast cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. (2024) 35:159–82. doi: 10.1016/j.annonc.2023.11.016
9. Gentilini OD, Botteri E, Sangalli C, Galimberti V, Porpiglia M, Agresti R, et al. SOUND trial group. Sentinel lymph node biopsy vs no axillary surgery in patients with small breast cancer and negative results on ultrasonography of axillary lymph nodes: the SOUND randomized clinical trial. JAMA Oncol. (2023) 9:1557–64. doi: 10.1001/jamaoncol.2023.3759
10. Reimer T, Stachs A, Veselinovic K, Kühn T, Heil J, Polata S, et al. Axillary surgery in breast cancer - primary results of the INSEMA trial. N Engl J Med. (2025) 392:1051–64. doi: 10.1056/NEJMoa2412063
11. Park KU, Somerfield MR, Anne N, Brackstone M, Conlin AK, Couto HL, et al. Sentinel lymph node biopsy in early-stage breast cancer: ASCO guideline update. J Clin Oncol. (2025) 43:1720–41. doi: 10.1200/JCO-25-00099
12. Reimer T, Stachs A, Veselinovic K, Polata S, Müller T, Kühn T, et al. INSEMA investigators. Patient-reported outcomes for the Intergroup Sentinel Mamma study (INSEMA): A randomised trial with persistent impact of axillary surgery on arm and breast symptoms in patients with early breast cancer. EClinicalMedicine. (2022) 55:101756. doi: 10.1016/j.eclinm.2022.101756
13. Gentilini O, Botteri E, Dadda P, Sangalli C, Boccardo C, Peradze N, et al. Physical function of the upper limb after breast cancer surgery. Results from the SOUND (Sentinel node vs. Observation after axillary Ultra-souND) trial. Eur J Surg Oncol. (2016) 42:685–9. doi: 10.1016/j.ejso.2016.01.020
14. Image-guided vacuum-assisted excision biopsy of benign breast lesions Interventional procedures guidance (2006). Available online at: www.nice.org.uk/guidance/ipg156 (Accessed October 5, 2025).
15. The Use of Transcutaneous and Percutaneous Ablation for the Treatment of Benign and Malignant Tumors of the Breast. Available online at: https://www.breastsurgeons.org/docs/statements/Consensus-Guideline-on-the-Use-of-Transcutaneous-and-Percutaneous-Methods-for-the-Treatment-of-Benign-and-Malignant-Tumors-of-the-Breast.pdf (Accessed October 5, 2025).
16. Pinder SE, Shaaban A, Deb R, Desai A, Gandhi A, Lee AHS, et al. NHS Breast Screening multidisciplinary working group guidelines for the diagnosis and management of breast lesions of uncertain Malignant potential on core biopsy (B3 lesions). Clin Radiol. (2018) 73:682–92. doi: 10.1016/j.crad.2018.04.004
17. NHS Breast Screening Programme Clinical guidance for breast cancer screening assessment. Available online at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/567600/Clinical_guidance_for_breast:cancer_screening:assessment_Nov_2016.pdf:~:text=This%20document%20is%20a%20refresh%20of%20the%20third,guidance%20following%20consultation%20with%20national%20groups%20and%20organisations (Accessed October 5, 2025).
18. Rubio IT, Wyld L, Marotti L, Athanasiou A, Regitnig P, Catanuto G, et al. European guidelines for the diagnosis, treatment and follow-up of breast lesions with uncertain Malignant potential (B3 lesions) developed jointly by EUSOMA, EUSOBI, ESP (BWG) and ESSO. Eur J Surg Oncol. (2024) 50:107292. doi: 10.1016/j.ejso.2023.107292
19. Elfgen C, Leo C, Kubik-Huch RA, Muenst S, Schmidt N, Quinn C, et al. Third International Consensus Conference on lesions of uncertain Malignant potential in the breast (B3 lesions). Virchows Arch. (2023) 483:5–20. doi: 10.1007/s00428-023-03566-x
20. Gil MLBV, Coelho BA, Couto HL, Silva HMS, Pessoa EC, Sharma N, et al. Vacuum-assisted excision: a safe minimally invasive option for benign phyllodes tumor diagnosis and treatment-a systematic review and meta-analysis. Front Oncol. (2024) 14:1394116. doi: 10.3389/fonc.2024.1394116
21. Valadares CN, Couto HL, Soares AN, Toppa PH, Ricardo BP, McIntosh SA, et al. Potential role of vacuum-assisted procedures in resecting breast cancers and highlighting selection criteria to support future trials. Front Oncol. (2023) 13:1239574. doi: 10.3389/fonc.2023.1239574
22. Elder K, Coles C, Dodwell D, Elsberger B, Foster J, Gaunt C, et al. SMALL: open surgery versus minimally invasive vacuum-assisted excision for small screen-detected breast cancer-protocol for a phase III randomised multicentre trial. BMJ Open. (2025) 15:e099702. doi: 10.1136/bmjopen-2025-099702
23. Sickles EA, D’Orsi CJ, Bassett LW, et al. ACR BI-RADS® Mam mography. In: ACR BI-RADS® Atlas, Breast Imaging Reporting and Data System. American College of Radiology, Reston (2013).
24. Brazilian’s guideline for breast cancer diagnose and treatment. Available online at: http://conitec.gov.br/images/Relatorios/2018/Recomendacao/Relatorio_DDT_CarcinomaDeMama_2018.pdf (Accessed October 5, 2025).
25. Education M.d. Competency Matrix in Mastology. Brazilian Education Ministry (2022). Available online at: http://www.gov.br/mec/pt-br/residencia-medica/pdf/matriz-mastologia.pdf (Accessed October 5, 2025).
26. Hortobagyi GN, Connolly JL, D´Orsi CJ, Edge SB, Mittendorf EA, Hugo HS, et al. AJCC Cancer Staging Manual, Breast, Eight Edition. Cham, Switzerland: Springer International Publishing (2017). doi: 10.1007/978-3-319-40618-3_48.
27. BREAST-Q Version 2.0. Available online at: http://qportfolio.org/wp-content/uploads/2018/12/BREAST-Q-USERS-GUIDE.pdf (Accessed October 5, 2025).
28. Heil J, Pfob A, and Kuerer HM. De-escalation towards omission is the tipping point of individualizing breast cancer surgery. Eur J Surg Oncol. (2020) 46:1543–5. doi: 10.1016/j.ejso.2020.03.208
29. . DATA AND FIGURES ON BREAST CANCER Annual Report 2023, relatorio_dados-e-numeros-ca-mama-2023.pdf.
30. Antonini Ribeiro R, Lavanholi Neyeloff J, Itria A, Cristina Canuto Santos V, Manso de Mello Vianna C, Nunes da Silva E, et al. Diretriz metodológica para estudos de avaliação econômica de tecnologias em saúde no Brasil. J Bras Econ da Saúde. (2016) 8:174–84. Available online at: http://www.jbes.com.br/images/v8n3/174.pdf (Accessed October 5, 2025).
31. Brazil. Ministry of Health. Secretariat of Science, Technology and Innovation. The use of cost-effectiveness thresholds in health decisions: Recommendations from the National Commission for the Incorporation of Technologies into SUS (2023). Available online at: https://www.gov.br/conitec/pt-br/midias/pdf/2022/20221106_relatorio-uso-de-limiares-de-custo-efetividade-nas-decisoes-em-saude.pdf (Accessed October 5, 2025).
32. Hwang ES, Hyslop T, Lynch T, Frank E, Pinto D, Basila D, et al. The COMET (Comparison of Operative versus Monitoring and Endocrine Therapy) trial: a phase III randomised controlled clinical trial for low-risk ductal carcinoma in situ (DCIS). BMJ Open. (2019) 9:e026797. doi: 10.1136/bmjopen-2018-026797
33. Nicosia L, Mariano L, Latronico A, Bozzini AC, Bellerba F, Gaeta A, et al. Exploring non-surgical alternatives for low to intermediate-grade in situ ductal carcinoma of the breast using vacuum-assisted excision: the VACIS protocol. Front Med (Lausanne). (2024) 11:1467738. doi: 10.3389/fmed.2024.1467738
34. Rella R, Romanucci G, Belli P, Ramunno M, Nunnari J, Russo G, et al. Improved evaluation of patients with small clusters of microcalcifications on mammograms: Implementation of vacuum assisted excision with “cavity margins shaving” technique. Eur J Radiol. (2025) 188:112138. doi: 10.1016/j.ejrad.2025.112138
35. Björnström M, Niinikoski L, Arlan K, Meretoja TJ, Ståhls A, and Hukkinen K. Vacuum-assisted excision of small breast cancers under ultrasound guidance. Eur J Radiol. (2023) 167:111049. doi: 10.1016/j.ejrad.2023.111049
36. He XF, Ye F, Wen JH, Li SJ, Huang XJ, Xiao XS, et al. High residual tumor rate for early breast cancer patients receiving vacuum-assisted breast biopsy. J Cancer. (2017) 8:490–6. doi: 10.7150/jca.17305
37. Park JH, Ahn SE, Kim S, Kwon MJ, Suh YJ, and Kim D. Complete surgical excision is necessary following vacuum-assisted biopsy for breast cancer. Curr Oncol. (2022) 29:9357–64. doi: 10.3390/curroncol29120734
38. Wei Q, Zheng Q, Gu Y, Teng R, and Zhao W. Occurrence of Residual Breast Tumors and Efficacy of MRI in their Detection after Vacuum-assisted Excisional Biopsy. Curr Med Imaging. (2024) 20:e15734056289252. doi: 10.2174/0115734056289252240304113622
39. Morrow M, Van Zee KJ, Solin LJ, Houssami N, Chavez-MacGregor M, Harris JR, et al. Society of surgical oncology-american society for radiation oncology-american society of clinical oncology consensus guideline on margins for breast-conserving surgery with whole-breast irradiation in ductal carcinoma in situ. J Clin Oncol. (2016) 34:4040–6. doi: 10.1200/JCO.2016.68.3573
40. Moran MS, Schnitt SJ, Giuliano AE, Harris JR, Khan SA, Horton J, et al. Society of Surgical Oncology-American Society for Radiation Oncology consensus guideline on margins for breast-conserving surgery with whole-breast irradiation in stages I and II invasive breast cancer. Ann Surg Oncol. (2014) 21:704–16. doi: 10.1245/s10434-014-3481-4
41. Co M, Fung MWY, and Kwong A. Surgical margin and local recurrence of ductal carcinoma in situ. Cancer Treat Res Commun. (2024) 39:100793. doi: 10.1016/j.ctarc.2024.100793
42. Bundred JR, Michael S, Stuart B, Cutress RI, Beckmann K, Holleczek B, et al. Margin status and survival outcomes after breast cancer conservation surgery: prospectively registered systematic review and meta-analysis. BMJ. (2022) 378:e070346. doi: 10.1136/bmj-2022-070346
43. Vos EL, Siesling S, Baaijens MHA, Verhoef C, Jager A, Voogd AC, et al. Omitting re-excision for focally positive margins after breast-conserving surgery does not impair disease-free and overall survival. Breast Cancer Res Treat. (2017) 164:157 67. doi: 10.1007/s10549-017-4232-621
44. Sorrentino L, Agozzino M, Albasini S, Bossi D, Mazzucchelli S, Vanna R, et al. Involved margins after lumpectomy for breast cancer: Always to be re-excised? Surg Oncol. (2019) 30:141–6. doi: 10.1016/j.suronc.2019.08.00222
45. Vos EL, Gaal J, Verhoef C, Brouwer K, van Deurzen CHM, and Koppert LB. Focally positive margins in breast conserving surgery: Predictors, residual disease, and local recurrence. Eur J Surg Oncol. (2017) 43:1846–54. doi: 10.1016/j.ejso.2017.06.00723
46. Fitzgerald S, ROmanoff A, Cohen A, Schmidt H, Weltz C, IJ B, et al. Close and positive lumpectomy margins are associated with similar rates of residual disease with additional surgery. Ann Surg Oncol. (2016) 23:4270–6. doi: 10.1245/s10434-0165490-y
47. Ungvari Z, Fekete M, Buda A, Lehoczki A, Munkácsy G, Scaffidi P, et al. Quantifying the impact of treatment delays on breast cancer survival outcomes: a comprehensive meta-analysis. Geroscience. (2025). doi: 10.1007/s11357-025-01719-1
48. Helsper CCW, van Erp NNF, Peeters PPHM, and de Wit NNJ. Time to diagnosis and treatment for cancer patients in the Netherlands: Room for improvement? Eur J Cancer. (2017) 87:113–21. doi: 10.1016/j.ejca.2017.10.003
49. Rakha EA, Lee AH, Jenkins JA, Murphy AE, Hamilton LJ, and Ellis IO. Characterization and outcome of breast needle core biopsy diagnoses of lesions of uncertain Malignant potential (B3) in abnormalities detected by mammographic screening. Int J Cancer. (2011) 129:1417–24. doi: 10.1002/ijc.25801
50. Rageth CJ, O’Flynn EAM, Pinker K, Kubik-Huch RA, Mundinger A, Decker T, et al. Second International Consensus Conference on lesions of uncertain Malignant potential in the breast (B3 lesions). Breast Cancer Res Treat. (2019) 174:279–96. doi: 10.1007/s10549-018-05071-1
51. Zheng J, Cai S, Song H, Wang Y, Han X, Han G, et al. Prediction of postoperative hematoma occurrence after ultrasound-guided vacuum-assisted breast biopsy in minimally invasive surgery for percutaneous removal of benign breast lesions. Gland Surg. (2020) 9:1346–53. doi: 10.21037/gs-20-344
52. Hewitt K, Son J, Glencer A, Borowsky AD, Cooperberg MR, and Esserman LJ. The evolution of our understanding of the biology of cancer is the key to avoiding overdiagnosis and overtreatment. Cancer Epidemiol Biomarkers Prev. (2020) 29:2463–74. doi: 10.1158/1055-9965.EPI-20-0110
53. Korde LA, Somerfield MR, Carey LA, Crews JR, Denduluri N, Hwang ES, et al. Neoadjuvant chemotherapy, endocrine therapy, and targeted therapy for breast cancer: ASCO guideline. J Clin Oncol. (2021) 39:1485–505. doi: 10.1200/JCO.20.03399
54. Huang K, Jakub J, Gabriel E, Moreno-Aspitia A, and McLaughlin S. Overall survival following neoadjuvant chemotherapy versus adjuvant chemotherapy in clinically node negative T1 triple negative breast cancer. Ann Surg Oncol. (2023) 30:7026–35. doi: 10.1245/s10434-023-13977-4
55. Masuda N, Lee SJ, Ohtani S, Im YH, Lee ES, Yokota I, et al. Adjuvant capecitabine for breast cancer after preoperative chemotherapy. N Engl J Med. (2017) 376:2147–59. doi: 10.1056/NEJMoa161264526
Keywords: vacuum assisted excision, minimally invasive treatment, early breast cancer, de-escalation, precision oncology
Citation: Couto HL, Coelho BA, Ricardo BFP, Toppa PH, Soares AN, Silvestre da Silva BT, Pires DM, Ferreira TCO, Clarke P, Ferreira SG, Oliveira LB, Saliba RGR, Soares PCM, Moraes TP, Mendonça ACG, de Oliveira ACB, Siqueira DR, de Oliveira JS, de Padua CAJ, Cunha Jr GF, Castilho MS, Carvalho BPSA, Silva Jr GA, de Almeida Júnior WA, de Lucena CÊM, Pessoa EC, dos Santos AMR, de Amorim HLE, Freitas-Junior R, Borges MN, Mattar A, Antonini M, Buttros DAB, Dominguez LLC, Pires B, Valadares CN and dos Reis FM (2025) Vacuum-assisted excision: one-step approach to the diagnosis and percutaneous treatment of small early breast cancer (the VAE-BREAST 01 study protocol). Front. Oncol. 15:1687634. doi: 10.3389/fonc.2025.1687634
Received: 18 August 2025; Accepted: 22 September 2025;
Published: 24 October 2025.
Edited by:
Lorenzo Scardina, Fondazione Policlinico Universitario A. Gemelli - IRCCS, ItalyReviewed by:
Omar Hamdy, Mansoura University, EgyptNikolay Amirov, N.N. Petrov National Medical Research Center of Oncology, Russia
Copyright © 2025 Couto, Coelho, Ricardo, Toppa, Soares, Silvestre da Silva, Pires, Ferreira, Clarke, Ferreira, Oliveira, Saliba, Soares, Moraes, Mendonça, de Oliveira, Siqueira, de Oliveira, de Padua, Cunha, Castilho, Carvalho, Silva, de Almeida Júnior, de Lucena, Pessoa, dos Santos, de Amorim, Freitas-Junior, Borges, Mattar, Antonini, Buttros, Dominguez, Pires, Valadares and dos Reis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Henrique Lima Couto, ZW5yaXF1ZWNvdXRvQGhvdG1haWwuY29t
†ORCID: Bertha Andrade Coelho, orcid.org/0000-0001-9803-1427
Bernardo Ferreira de Paula Ricardo, orcid.org/0000-0002-1891-1457
Bruna Torres Silvestre da Silva, orcid.org/0000-0002-1192-2938
Douglas de Miranda Pires, orcid.org/0000-0003-4264-9820
Tereza Cristina de Oliveira Ferreira, orcid.org/0000-0003-2907-9464
Shirley das Grac¸ as Ferreira, orcid.org/0000-0003-3235-6805
Romana Giordani Ribeiro Saliba, orcid.org/0009-0004-6181-5059
Amanda Cristina Braga de Oliveira, orcid.org/0009-0005-4524-8856
Jane Sanglard de Oliveira, orcid.org/0009-0004-1325-2917
Charles Andree´ Joseph de Padua, orcid.org/0000-0002-2664-7959
Gabriel de Almeida Silva Jr, orcid.org/0009-0007-3777-595X
Waldeir José de Almeida Júnior, orcid.org/0000-0002-1791-8315
Clecio Eˆ nio Murta de Lucena, orcid.org/0000-0002-5841-1828
Annamaria Massahud Rodrigues dos Santos, orcid.org/0000-0002-2393-2447
Heverton Leal Ernesto de Amorim, orcid.org/0009-0005-8912-4134
Ruffo Freitas-Junior, orcid.org/0000-0003-4145-8598
Daniel de Arau´ jo Brito Buttros, orcid.org/0000-0002-7309-1287
Nazareth Valadares, orcid.org/0000-0002-3513-6763
Fernando Marcos dos Reis, orcid.org/0000-0002-9258-7472