 Monica L. Quijano-Lievano1,2,3,4
Monica L. Quijano-Lievano1,2,3,4 Oscar Ramirez2,3,4
Oscar Ramirez2,3,4 Yichen Chen5Maricela Robles-Murguia5
Yichen Chen5Maricela Robles-Murguia5 Meenakshi Devidas5
Meenakshi Devidas5 Hilmarie Muñiz-Talavera5
Hilmarie Muñiz-Talavera5 Adolfo Cárdenas-Aguirre5
Adolfo Cárdenas-Aguirre5 Carlos Portilla2,6Diana Castrillon7Diana Rendon7
Carlos Portilla2,6Diana Castrillon7Diana Rendon7 Andreia Ribeiro Pereira Aguiar De Paula8
Andreia Ribeiro Pereira Aguiar De Paula8 Rosdali Diaz-Coronado9
Rosdali Diaz-Coronado9 María Sánchez-Martín10,11
María Sánchez-Martín10,11 Silvio Torres12Verónica Soto Chávez13
Silvio Torres12Verónica Soto Chávez13 Asya Agulnik5*
Asya Agulnik5*- 1Health Doctorate Department, Universidad del Valle, Cali, Colombia
- 2Bone Marrow Transplant Unit, Clínica Imbanaco, Cali, Colombia
- 3Cali Population-Based Cancer Registry, Department of Pathology, Universidad del Valle, Cali, Colombia
- 4Research Unit, Fundación Pediatric Oncologists-Hematologists (POHEMA), Cali, Colombia
- 5St. Jude Children’s Research Hospital, Memphis, TN, United States
- 6Pediatric Department, Medicine School, Universidad del Valle, Cali, Colombia
- 7Pediatric Hemato-Oncology Unit, Clínica Imbanaco, Cali, Colombia
- 8Hospital do Amor/Hospital de Cancer Infanto Juvenil de Barretos, Barretos, Brazil
- 9Instituto Nacional de Enfermedades Neoplásicas (INEN), Lima, Peru
- 10Hospital Universitario La Paz, Madrid, Spain
- 11Doctorate School, Medicine Faculty, Universidad Autónoma de Madrid, Madrid, Spain
- 12Hospital Universitario Austral, Buenos Aires, Argentina
- 13Hospital Civil de Guadalajara, Guadalajara, Mexico
Background/Aim: Escala de Valoración de Alerta Temprana (EVAT) is a Spanish-language Pediatric Early Warning Score (PEWS) validated to predict the need for unplanned intensive care unit (ICU) transfer in hospitalized children with cancer. We assess the effect of PEWS implementation on hospitalized children undergoing hematopoietic stem cell transplantation (HSCT) in variable-resource centers in South America and Europe.
Methods: We analyzed data from a prospective registry of clinical deterioration events (CDE), defined as an unplanned ICU transfer, ICU-level intervention on the ward, ward cardiopulmonary arrest, or deterioration to death, among hospitals implementing PEWS. We included CDE occurring in patients under age 19 hospitalized in an HSCT unit between April 2017 and June 2024. We used the Wilcoxon rank sum test, chi-square test, and Fisher’s exact test to compare CDE occurring before PEWS implementation (pre-PEWS) and during/after PEWS implementation (post-PEWS).
Results: During the study period, we identified 221 CDE among 146 patients from six centers (South America n = 5; Europe n = 1). The median age was 9 years (IQR, 4–14), 68% (n = 150/220) were male, and 20% (n = 44/221) experienced more than one CDE. The overall event mortality rate was 18% (n = 39/221). Of 221 CDE, 71 occurred pre-PEWS implementation and 150 post-PEWS implementation. CDE post-PEWS were less likely due to respiratory distress (38%, n = 27/71 vs. 23% n = 35/150, p = 0.0348), had fewer organ systems with dysfunction at ICU transfer (median 2 [IQR 1–3] vs. 0 [IQR 0–2], p < 0.001), and had lower PIM2, which indicates a lower severity of illness at ICU transfer (median 5.0 [IQR 1.4–7.9] vs. 1.5 [IQR 1.2–3.4], p < 0.001). There was a non-significant decrease in clinical deterioration event mortality post-PEWS implementation (24%, n = 17/71 vs. 15%, n = 22/150, p = 0.1335).
Conclusions: PEWS implementation promoted the early identification of critical illness as well as ICU transfer at a lower severity of illness for children undergoing HSCT. This work further supports the use of PEWS in the care of all children with cancer and blood disorders globally.
1 Introduction
Hospitalized pediatric patients diagnosed with cancer and those undergoing hematopoietic stem cell transplantation (HSCT) are at a high risk for clinical deterioration and death, especially in resource-limited settings. Pediatric early warning score (PEWS) systems aid in the early identification of clinical deterioration in hospitalized children (1–6). The system includes a scoring scale that enables nursing staff to assess hospitalized patients based on vital signs and clinical status as part of routine care. It also includes a response algorithm that guides healthcare team interventions for patients with clinical deterioration (5). Escala de Valoración de Alerta Temprana (EVAT) is a Spanish-language PEWS that has been validated to predict the need for unplanned transfer to the pediatric intensive care unit (PICU) in hospitalized children with cancer (2, 5). However, the study of its use in the care of children undergoing HSCT is limited.
Proyecto EVAT is a quality improvement collaborative initiated by St. Jude Children’s Research Hospital (7) in partnership with regional leaders in Latin America and Europe to improve outcomes for children with cancer who are at risk for deterioration (4, 8). The regional experience with Proyecto EVAT demonstrates a successful strategy for adoption and scale-up of an evidence-based practice in real-world settings (8), with more than 110 pediatric oncology centers implementing and sustaining PEWS. PEWS implementation through Proyecto EVAT has been shown to reduce clinical deterioration mortality in participating centers regardless of their resource level (4).
Prior studies suggest that early transfer to the ICU may lead to better outcomes for patients undergoing HSCT who develop critical illness (1–3, 5). The PEWS informing EVAT was validated in pediatric HSCT patients in the United States (3). However, information about how PEWS implementation affects clinical outcomes in this population in other settings is limited (9–12). This study evaluates the impact of PEWS implementation on hospitalized children and adolescents undergoing HSCT in variable-resource centers in South America and Europe.
2 Methods
2.1 Study design
We performed a secondary analysis of data collected for a prospective, multicenter cohort study of hospitals providing childhood cancer care in patients undergoing HSCT. Each of these hospitals participated in Proyecto EVAT, a Spanish-language PEWS adapted for low-resource settings (13). Registry methods have previously been described and are briefly summarized below.
2.2 Human subjects approval
The St. Jude Institutional Review Board reviewed this secondary registry-based de-identified data analysis as non-human subjects research. Every collaborating center received official local approval to carry out PEWS and take part in Proyecto EVAT. Where required, further institutional approvals were acquired following local regulations.
2.3 Setting
Of 96 centers participating in Proyecto EVAT as of June 2024, 12 centers could perform HSCT. Of these, six centers that had completed PEWS implementation and had both baseline and post-implementation registry data on clinical deterioration events (CDE) were included in this study. These six centers joined Proyecto EVAT after April 1, 2017 and completed PEWS implementation by December 31, 2023, allowing at least 6 months of post-PEWS implementation data collection. We define two periods: the period occurring before PEWS implementation (pre-PEWS) and during/after PEWS implementation (post-PEWS). In addition to facility data routinely collected by Proyecto EVAT (4), we surveyed each participating HSCT center on HSCT infrastructure (number of available pediatric HSCT beds, separation of the HSCT unit from the oncology ward, and ward nursing ratios) and transplant activity during the year of PEWS implementation (annual number and type of HSCT, CAR-T therapy, the underlying diseases transplanted, and intensity of conditioning).
2.4 PEWS
PEWS/EVAT uses a five-component rating system (neurological, cardiovascular, respiratory, and nursing and family concerns) based on vital signs, physical examination results, and treatment needs (Supplementary Figure S1). Hospitalized patients are rated by a bedside nurse after routine vital sign checks. This rating matches a clinical decision algorithm (Supplementary Figure S2) that indicates potential clinical deterioration and guides the clinical team toward appropriate treatment escalation.
2.5 Project PEWS/EVAT procedures
EVAT’s procedures have been described in detail previously (4). Briefly, Proyecto EVAT facilitates the implementation of PEWS in participating hospitals through a mentored implementation strategy (8). Hospitals join Proyecto EVAT through collaboration with St. Jude Global or by learning about the initiative from other collaborating institutions. Local teams who lead the PEWS implementation process consist of at least a ward nurse, ward physician, and critical care physician (4). The hospitals are guided through a three-phase process of planning, pilot implementation, and sustainability. Planning for implementation is the focus of the first phase (pre-PEWS); PEWS pilot and implementation are covered in the second phase (during PEWS); and PEWS sustainability is the focus of the third phase (post-PEWS). St. Jude and regional PEWS mentor center experts train and support local teams, helping them overcome barriers to adoption and ensuring the quality of PEWS implementation. Hospitals have completed implementation when they reach a specified level of PEWS quality, defined as having fewer than 15% PEWS errors for two consecutive months. Once implementation is complete, hospitals receive mentoring to create sustainability plans for the ongoing use of PEWS. Starting at the PEWS pilot and for 18 months post-implementation, participating centers collect data on the quality of PEWS use, including adherence to the PEWS algorithm, accuracy in calculating PEWS scores, and documentation of PEWS alongside vital signs. Weekly reviews of nursing records and monthly summaries are conducted to evaluate the use of PEWS among hospitalized pediatric cancer patients (5, 8).
2.6 Terminology
HSCT is a critical therapeutic intervention for pediatric patients with hematologic malignancies, immune deficiencies, and genetic disorders (8). The procedure involves infusing hematopoietic stem cells (along with hematopoietic progenitor cells) to reestablish the patient’s hematopoietic system. Generally, HSCT is performed after a preparative regimen consisting of agents designed to create marrow space, suppress the patient’s immune system to prevent rejection, and eradicate malignant cells in cancer patients (8).
Proyecto EVAT defines a CDE as any hospitalized patient who requires unplanned ICU transfer, receives an ICU-level intervention on the ward, including mechanical ventilation (invasive and non-invasive), vasoactive infusion, cardiopulmonary resuscitation (CPR), or ward cardiopulmonary arrest, or experiences a non-palliative death. A CDE ends at the moment of death, ICU discharge, or last ward-based ICU-level intervention (2, 4, 8). ICU-level interventions include CPR, vasoactive infusion, and invasive or noninvasive (continuous positive pressure and bi-level positive pressure) mechanical ventilation (4). ICU transfer is defined as the transfer to any hospital unit designed to provide a higher level than ward-based care to deteriorating patients (2). Clinical deterioration event-mortality is defined as a CDE that resulted in death in the ICU or within 24 hours of ICU discharge, or at the end of ward-based ICU interventions (14). The degree of illness severity and resource utilization is recorded at the start of the CDE (4). Deterioration in children with limitations on life-sustaining measures (do not resuscitate order or equivalent) was not considered a CDE and was not included in this study. Severity of illness and resource utilization describe the degree of critical illness at the start of the CDE (4). Sepsis and organ dysfunction are defined by the criteria proposed by Goldstein and colleagues (15). The Pediatric Index of Mortality 2 (PIM2) is calculated with standard criteria (16).
Ward cardiopulmonary arrest is defined as a clinical deterioration event requiring acute invasive mechanical ventilation or CPR or resulting in a non-palliative death on the ward (4). Ward CPR or death is defined as a CDE with cardiac arrest on the ward requiring CPR or resulting in a nonpalliative ward death (4, 15).
2.7 Measurements
Participating centers collected prospective data in a quality improvement registry from the start of participation in Proyecto EVAT through 18 months post-implementation. Variables gathered from clinical records included age, sex, neoplastic diagnosis, induction therapy for acute leukemia, and disease status. For each CDE reported, local site leads completed a de-identified case report form (Supplementary Figure S3) that included the following information: the cause of the CDE, the Pediatric Index of Mortality 2 (PIM2) severity score, physiological variables (neutrophil and platelet counts, lactate levels, and C-reactive protein), infectious variables (type of infection and any positive isolates), critical interventions (use of vasopressors, both invasive and non-invasive ventilation, renal replacement therapy, cardiopulmonary resuscitation), and transfer to a higher-level-of-care facility (ICU, intermediate care unit, emergency room) at the time of the CDE. We used hospital mortality and clinical deterioration events as the primary outcome variables. Additionally, the severity of illness on ICU transfer was described using the PIM-2 severity score and the presence of organ dysfunction at the time of transfer to a higher level of care. For each CDE reported, local site leads sent data to St. Jude for entry into a REDCap database (17). To ensure quality, clinical research associates at St. Jude regularly examined the data for missing or incorrect information.
2.8 Inclusion
The patients included in this study were under age 19 at the time of receiving the HSCT infusion, were hospitalized in the HSCT unit during the center’s quality improvement data collection period, and had data on deterioration events collected from the HSCT unit that had implemented EVAT/PEWS through Proyecto EVAT (Supplementary Table S1).
2.9 Statistical analysis
Descriptive statistics were used to define CDE characteristics among patients undergoing HSCT, pre-PEWS, and post-PEWS implementation at participating centers. The post-PEWS were collapsed in analysis due to the rapid uptake of PEWS use among these units and the similarities of data during these periods. We described hospital characteristics and HSCT services across centers (Supplementary Table S2). To describe the impact of PEWS on CDE, we compared events pre-PEWS and post-PEWS implementation. The CDE was used as the unit of analysis and CDE mortality as the primary outcome. Wilcoxon rank sum test, chi-square test, and Fisher’s exact test were used to assess event-level association between continuous/categorical CDE characteristics pre- and post-PEWS implementation. P-values <0.05 were considered statistically significant. Data were analyzed using R, version 4.4.1.
3 Results
3.1 HSCT characteristics of participating centers
During the study period, six centers from five upper-middle-income countries in Latin America (Mexico, Peru, Colombia, Argentina, and Brazil) and one center from a high-income country (Spain) contributed pre- and post-PEWS implementation registry data for patients admitted to a transplant unit and were included in the analysis (Table 1, Figure 1). These centers reported an annual total of 168 HSCT; of these, 67% (n = 113) were allogeneic and 36% (n = 60) were haploidentical. HSCT was used in 68% (n = 114) of the cases for neoplastic diseases and received myeloablative conditioning in 49% (n = 82) of the procedures.

Table 1. Characteristics of the participating centers.

Figure 1. Map of participating EVAT Project centers by World Bank income level.
3.2 CDE characteristics and outcomes
The centers reported a total of 221 CDE in 146 unique patients (one to six CDE/patient) during the study period. Of these, 71 events occurred among 50 patients pre-PEWS and 150 events occurred among 96 patients post-PEWS implementation; 39% CDE (n = 86/221) experienced more than one CDE. No patient experienced CDE both before and after PEWS implementation. Event characteristics are described in Table 2 and Supplementary Table S3. Most events occurred in patients with hematologic malignancy (n = 153/221, 69%). CDE were attributable most often to sepsis or septic shock (n = 96, 43%) and respiratory distress (n = 62, 28%). The notable resource utilization and outcomes of the overall population included a median ICU length of-stay of 4.8 days [IQR 2.56–12.1 days] and a median duration of mechanical ventilation and vasoactive infusion of 3.2 days [IQR 1.1–10.8 days] and 1.9 days [IQR 0.9-4.3 days], respectively (Supplementary Table S4). Before transfer to a higher-care facility, ICU physicians evaluated the patient in 68% (n = 151/221) of the events, and 14% (n = 30/221) had ICU-level intervention on the ward. Ultimately, 98% (n = 216/221) were transferred to a higher level of care (ICU 97% [n = 210/216] and intermediate care unit 3% [n = 6/216]), with a median delay of 3.6 h [IQR 2.0–6.3 h] after CDE start. The outcomes of patients not transferred to a higher level of care are described in Supplementary Table S5. Overall, there were 39 CDE mortalities, representing an overall mortality rate of 18% (n = 39/221). One death occurred on the floor before transfer to the ICU; the remainder occurred in an ICU. Out of 39 deaths, 97.4% (n = 38/39) were attributable to treatment- or transplant-related mortality; only one was due to cancer progression or relapse.
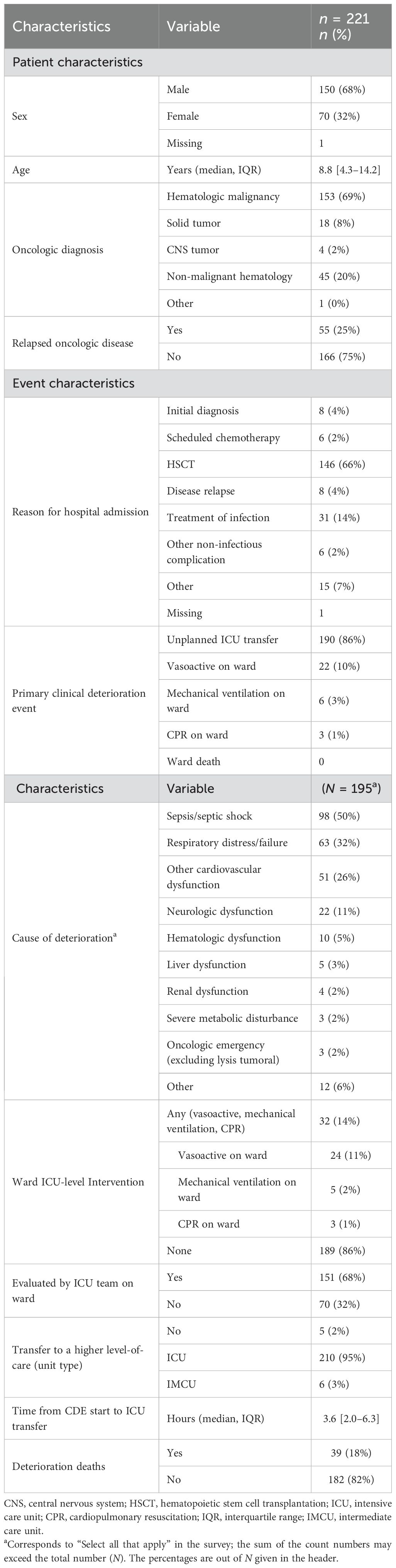
Table 2. Characteristics of clinical deterioration events.
3.3 CDE pre- and post-PEWS implementation
Events pre-PEWS had a similar distribution of age, sex, and status of oncologic disease as those post-PEWS (Table 3), though the distribution of oncologic diagnoses differed between these groups (p = 0.0495). Additionally, events occurring post-PEWS began earlier following hospital admission (median 22 [16–60] vs. 16 [11–28] days, p = 0.0016) and were less often due to respiratory distress or failure (38% [n = 27/71] vs. 23% [n = 35/150], p = 0.035).
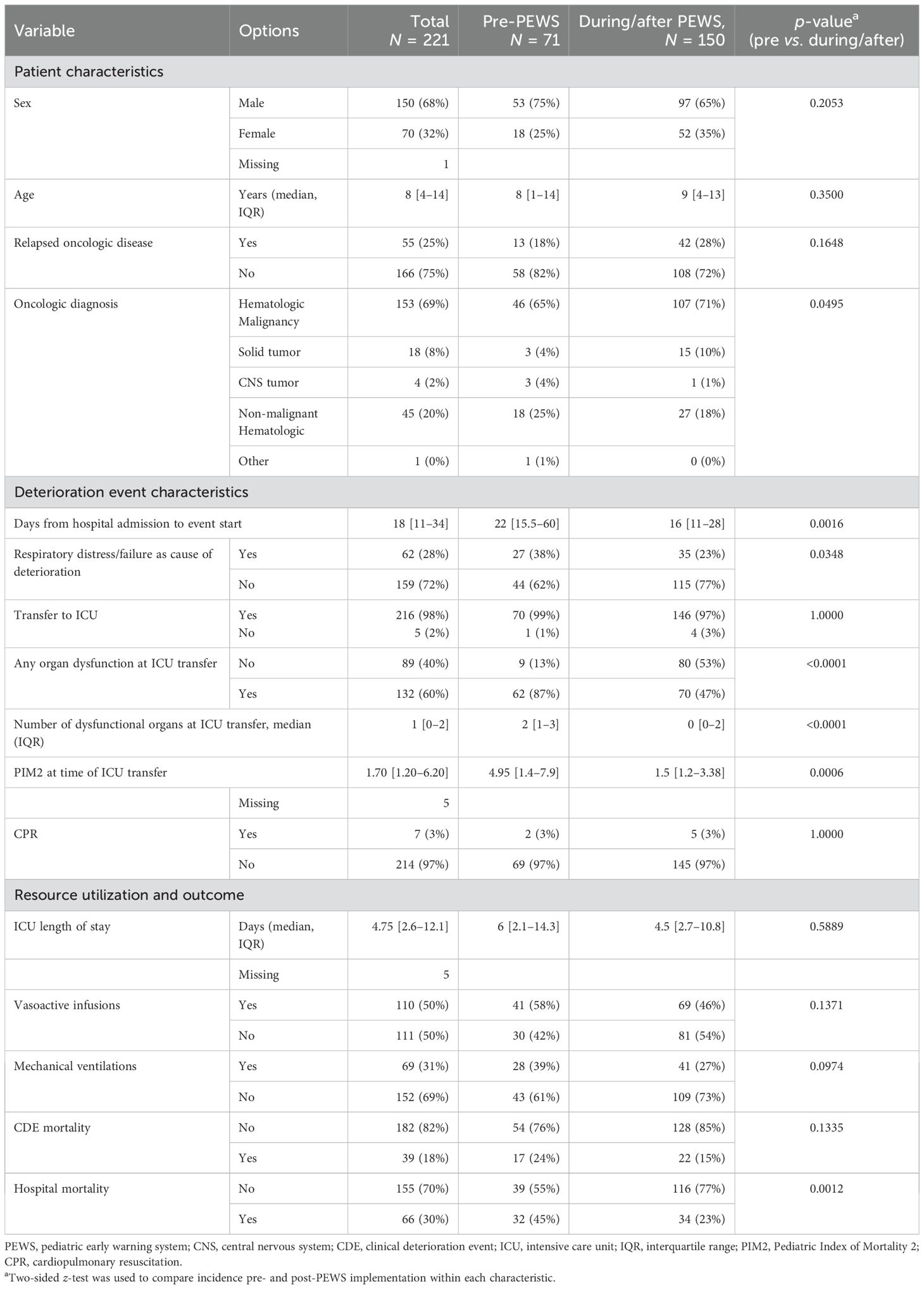
Table 3. Comparisons of clinical deterioration events before and during/after PEWS implementation.
Transfer to the ICU occurred at a lower severity of illness post-PEWS compared to the pre-PEWS period (Table 3). At the time of ICU transfer, events post-PEWS were less likely to have any organ dysfunction (87% [n = 62/71] pre vs. 47% [n = 70/150] post, p < 0.0001). The median number of organs with dysfunction at ICU transfer also decreased (2 [1–3] vs. 0 [0–2], p < 0.0001). Additionally, patients were transferred to the ICU earlier in their illness, with PIM2 scores decreasing post-PEWS implementation (median 5.0 [IQR 1.4–7.9] vs. 1.5 [IQR 1.2–3.4], p < 0.001).
ICU resource utilization, including the use of vasoactive infusions, mechanical ventilation, and ICU length-of-stay, was similar pre-PEWS and post-PEWS implementation (Table 3). There was a non-significant decrease in CDE mortality in the period after PEWS implementation (24% vs. 15%, p = 0.1335) and a significant decrease in hospital mortality (45% vs. 23%, p = 0.0012).
4 Discussion
In children hospitalized in six HSCT units involved in a quality improvement collaborative, we observed improved management of clinical deterioration events following implementation of PEWS, demonstrated by a lower severity of illness at transfer to a higher level of care, including lower median PIM-2 score and less organ dysfunction. This improvement occurred without an increase in ICU resource utilization, representing an overall improvement in the quality and safety of care for hospitalized HSCT patients without additional hospital costs. These findings are similar to data from the impact of PEWS on hospitalized children with cancer not undergoing HSCT (4, 5, 18).
Previously, there was concern about the performance of PEWS in children undergoing HSCT, as these tools were originally developed to identify clinical deterioration in hospitalized general pediatric patients (17). HSCT patients represent a unique and vulnerable group, facing higher mortality rates during critical illness and a greater need for escalated medical care (19). The increased vulnerability of HSCT recipients during critical illness stems from a complex interplay of pre-transplant factors (age, comorbid conditions (20), CMV seropositivity, the underlying disease and disease status), transplant-related factors (graft characteristics and source, intensity of the conditioning regimen, and immunosuppressive therapy), and post-transplant factors (time from HSCT to clinical deterioration, grade III or IV acute graft vs. host disease) (21, 22). Therefore, prompt detection of clinical deterioration is integral to prevent further complications and transplant-related mortality (19). As a result, in many hospitals, children undergoing HSCT are monitored more closely than pediatric oncology patients who are not undergoing HSCT. For example, the International Society of Pediatric Oncology (SIOP) Nursing Standards for Low- and Middle-Income Countries (LMICs) recommend lower nurse–patient ratios for transplant units compared to general oncology (23). Nonetheless, PEWS have been validated to predict deterioration among hospitalized children undergoing HSCT (3). Similarly, in this study, we observed earlier ICU transfer following PEWS implementation in six diverse hospitals providing HSCT care. The decision to transfer a patient to the ICU was based on each center’s customized PEWS response algorithm adapted to the local setting, a key element for successful implementation (24, 25). These findings add to existing evidence that a comprehensive system with standardized assessment and response such as PEWS, paired with a robust implementation strategy, can guide early action and improve hospital outcomes for these vulnerable patients (26).
In this study, we observed a decreased severity of illness on ICU transfer for hospitalized children undergoing HSCT, as measured by organ dysfunction and PIM2 scores at ICU transfers. Severity of illness at the time of initiation of critical care is strongly associated with poor outcomes and a common proxy for ICU mortality (16, 22). PEWS use is intended to detect deterioration promptly, thus expanding the time available to initiate interventions and prevent the development of irreversible organ dysfunction. Concordantly, early ICU evaluation and ICU transfer are recommended by recent international consensus to improve outcomes for hospitalized children undergoing HSCT (26). The observed decrease in organ dysfunction and PIM2 scores after PEWS implementation indicates that patients were transferred to the ICU earlier in the course of illness (13, 14). This suggests PEWS facilitates the identification, management, and triage of children undergoing HSCT, thus improving the quality and safety of care (9, 10, 17, 27, 28). In larger prior studies, this decrease in severity of illness was also shown to result in a reduction in CDE mortality. While we observed this trend in the current study, it did not reach statistical significance, possibly due to the smaller sample size (4).
The majority of deaths during clinical deterioration observed in this study were not due to cancer progression or relapse but rather due to treatment complications such as multi-organ dysfunction. This signifies potentially preventable transplant-related mortality that can be mitigated by improved supportive care. Existing evidence demonstrates that avoiding delays to the timely initiation of appropriate critical care and PICU-level interventions is an important strategy to decrease mortality in these patients (6, 17, 27, 29, 30). This study shows that the implementation of systems like PEWS that support nurses and doctors to perform a structured patient evaluation leads to earlier detection of CDE and earlier ICU transfer. In addition to systems that promote the early identification of clinical deterioration, advances in transplant procedures, the increasing use of immune effector cell therapies, candidate selection, and pediatric intensive care management (including prompt PICU and early critical care management strategies (31–36) are all strategies that improve clinical outcomes for children undergoing HSCT (26). However, support measures differ across centers and countries, highlighting the need for further research to alleviate treatment-related mortality while considering local contexts.
Our study has several limitations. The study design, which compares CDE occurring pre-PEWS and post-PEWS implementation, weakens the causal inference regarding the impact of PEWS implementation on the observed decrease in the severity of CDE. Nevertheless, the general characteristics of the CDE were similar pre-PEWS and post-PEWS implementation, and the PIM2 score is a robust objective predictor of mortality risk and time of initiation of critical care (16). Our sample size was limited due to the number of pediatric HSCTs performed at Proyecto EVAT centers that completed PEWS implementation. This may have restricted our ability to detect smaller effects related to PEWS implementation, including the impact on CDE mortality. Additionally, due to the limited number of events pre- and post-PEWS implementation, the results were reported at the event-level only, and controlling for multiple sampling was not possible statistically. A larger-scale trial will be needed to confirm these results through patient-level analyses, such as using generalized estimating equations. Another limitation was the manner by which children receiving HSCT were identified in the Proyecto EVAT CDE registry used in this study. This registry was initially designed for patients diagnosed with cancer and hospitalized in centers mostly without access to HSCT. Therefore, data on the type of transplant, date of transplant, conditioning intensity, donor match, cell processing, graft versus host, and diagnostic criteria for transplant indication, among other factors, were not collected in the registry. For this reason, patients undergoing HSCT were identified by their unit of hospitalization. It is possible that patients with a history of remote HSCT were thus missed in this analysis. Additionally, the lack of details on transplant-related factors prevents us from controlling for these factors in our analysis. Finally, prior studies have highlighted additional benefits of PEWS implementation in the care of children with cancer, including enhanced staff empowerment, improved interdisciplinary communication, higher perceived quality of care, and cost savings, which were not measured in this research (18, 27, 37). Future work should investigate the impact of PEWS on these multi-level outcomes for children undergoing HSCT.
5 Conclusion
This study suggests that PEWS implementation across six centers with diverse HSCT capabilities in Latin America and Spain improved hospital outcomes for children undergoing HSCT by facilitating the early detection of critical illness and prompt ICU transfer at a lower severity of illness. These data contribute to the current literature supporting the effectiveness of PEWS in improving care for pediatric oncology patients, including those undergoing HSCT.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
MQ: Conceptualization, Formal analysis, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. OR: Investigation, Methodology, Writing – review & editing. YC: Data curation, Formal analysis, Methodology, Validation, Writing – review & editing. MR: Investigation, Writing – review & editing. MD: Formal analysis, Methodology, Writing – review & editing. HM: Writing – review & editing. AC: Writing – review & editing. CP: Writing – review & editing. DC: Writing – review & editing. DR: Writing – review & editing. AD: Writing – review & editing. RD: Writing – review & editing. MS: Writing – review & editing. ST: Writing – review & editing. VS: Writing – review & editing. AA: Conceptualization, Data curation, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declared that financial support was not received for this work and/or its publication.
Acknowledgments
We thank the St. Jude Global team and especially the EVAT study team for their support and dedication to this project. We also recognize the leaders of the HSCT units at the participating centers who made this publication possible (Supplementary Table S6).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2025.1712611/full#supplementary-material
References
1. Brown SR, Garcia DM, and Agulnik A. Scoping review of pediatric Early Warning Systems (PEWS) in resource-limited and humanitarian settings. Front Pediatr. (2019) 6:419215. doi: 10.3389/fped.2018.00410
2. Agulnik A, Méndez Aceituno A, Mora Robles LN, Forbes PW, Soberanis Vasquez DJ, Mack R, et al. Validation of a pediatric early warning system for hospitalized pediatric oncology patients in a resource-limited setting. Cancer. (2017) 123:4903–13. doi: 10.1002/cncr.30951
3. Agulnik A, Forbes PW, Stenquist N, Rodriguez-Galindo C, and Kleinman M. Validation of a pediatric early warning score in hospitalized pediatric oncology and hematopoietic stem cell transplant patients. Pediatr Crit Care Med. (2016) 17:e146–53. Available online at: https://journals.lww.com/pccmjournal/fulltext/2016/04000/validation_of_a_pediatric_early_warning_score_in.26.aspx (Accessed November 21, 2023).
4. Agulnik A, Muniz-Talavera H, Pham LTD, Chen Y, Carrillo AK, Cárdenas-Aguirre A, et al. Effect of paediatric early warning systems (PEWS) implementation on clinical deterioration event mortality among children with cancer in resource-limited hospitals in Latin America: a prospective, multicentre cohort study. Lancet Oncol. (2023) 24:978–88. Available online at: http://www.thelancet.com/article/S1470204523002851/fulltext (Accessed December 10, 2023).
5. Agulnik A, Mora Robles LN, Forbes PW, Soberanis Vasquez DJ, Mack R, Antillon-Klussmann F, et al. Improved outcomes after successful implementation of a pediatric early warning system (PEWS) in a resource-limited pediatric oncology hospital. Cancer. (2017) 123:2965–74. doi: 10.1002/cncr.30664
6. Dean NP, Fenix JB, Spaeder M, and Levin A. Evaluation of a pediatric early warning score across different subspecialty patients. Pediatr Crit Care Med. (2017) 18:655–60. doi: 10.1097/PCC.0000000000001176
7. St. Jude Global. St. Jude Children’s Research Hospital . Available online at: https://www.stjude.org/global.html (Accessed June 3, 2025).
8. Agulnik A, Gonzalez Ruiz A, Muniz-Talavera H, Carrillo AK, Cárdenas A, Puerto-Torres MF, et al. Model for regional collaboration: Successful strategy to implement a pediatric early warning system in 36 pediatric oncology centers in Latin America. Cancer. (2022) 128:4004–16. doi: 10.1002/cncr.34427
9. Soeteman M, Lekkerkerker CW, Kappen TH, Tissing WJ, Nieuwenhuis EE, and Wösten-van Asperen RM. The predictive performance and impact of pediatric early warning systems in hospitalized pediatric oncology patients—A systematic review. Pediatr Blood Cancer. (2022) 69:e29636. doi: 10.1002/pbc.29636
10. Maccarana T, Pillon M, Bertozzi V, Carraro E, Cavallaro E, Bonardi CM, et al. Oncological pediatric early warning score: a dedicated tool to predict patient’s clinical deterioration and need for pediatric intensive care treatment. Pediatr Hematol Oncol. (2024) 41:422–31. doi: 10.1080/08880018.2024.2355543
11. Mills D, Schmid A, Najajreh M, Al Nasser A, Awwad Y, Qattush K, et al. Implementation of a pediatric early warning score tool in a pediatric oncology Ward in Palestine. BMC Health Serv Res. (2021) 21. doi: 10.1186/s12913-021-07157-x
12. Agulnik A, Gossett J, Carrillo AK, Kang G, and Morrison RR. Abnormal vital signs predict critical deterioration in hospitalized pediatric hematology-oncology and post-hematopoietic cell transplant patients. Front Oncol. (2020) 10. doi: 10.3389/fonc.2020.00354
13. Agulnik A, Robles-Murguia M, Chen Y, Muñiz-Talavera H, Pham L, Carrillo A, et al. Multilevel mortality risk factors among pediatric hematology-oncology patients with deterioration. Cancer. (2025) 131. doi: 10.1002/cncr.35818
14. Agulnik A, Cárdenas A, Carrillo AK, Bulsara P, Garza M, Alfonso Carreras Y, et al. Clinical and organizational risk factors for mortality during deterioration events among pediatric oncology patients in Latin America: A multicenter prospective cohort. Cancer. (2021) 127:1668–78. doi: 10.1002/cncr.33411
15. Goldstein B, Giroir B, and Randolph A. International pediatric sepsis consensus conference: Definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med. (2005) 6. doi: 10.1097/00130478-200501000-00033
16. Slater A, Shann F, and Pearson G. PIM2: A revised version of the Paediatric Index of Mortality. Intensive Care Med. (2003) 29:278–85. doi: 10.1007/s00134-002-1601-2
17. Cater DT, Tori AJ, Moser EAS, and Rowan CM. Modification and assessment of the bedside pediatric early warning score in the pediatric allogeneic hematopoietic cell transplant population. Pediatr Crit Care Med. (2018) 19:483–8. doi: 10.1097/PCC.0000000000001521
18. Siječić A, Quesada-Stoner AC, Islam S, Malone S, Puerto-Torres MF, Cardenas Aguirre A, et al. Clinician perspectives on the multilevel impacts of Pediatric early warning systems (PEWS) in resource-variable hospitals. Front Oncol. (2025) 15. doi: 10.3389/fonc.2025.1573360
19. Zinter MS, Logan BR, Fretham C, Sapru A, Abraham A, Aljurf MD, et al. Comprehensive prognostication in critically ill pediatric hematopoietic cell transplant patients: results from merging the center for international blood and marrow transplant research (CIBMTR) and virtual pediatric systems (VPS) registries. Biol Blood Marrow Transplant. (2020) 26:333–42. Available online at: https://www.sciencedirect.com/science/article/pii/S108387911930638X (Accessed June 3, 2025).
20. Smith AR, Majhail NS, MacMillan ML, DeFor TE, Jodele S, Lehmann LE, et al. Hematopoietic cell transplantation comorbidity index predicts transplantation outcomes in pediatric patients. Blood. (2011) 117:2728–34. doi: 10.1182/blood-2010-08-303263
21. Zinter MS, DuBois SG, Spicer A, Matthay K, and Sapru A. Pediatric cancer type predicts infection rate, need for critical care intervention, and mortality in the pediatric intensive care unit. Intensive Care Med. (2014) 40:1536–44. doi: 10.1007/s00134-014-3389-2
22. Saillard C, Darmon M, Bisbal M, Sannini A, Chow-Chine L, Faucher M, et al. Critically ill allogenic HSCT patients in the intensive care unit: a systematic review and meta-analysis of prognostic factors of mortality. Bone Marrow Transplant. (2018) 53:1233–41. doi: 10.1038/s41409-018-0181-x
23. Day S, Hollis R, Challinor J, Bevilacqua G, and Bosomprah E. Baseline standards for paediatric oncology nursing care in low to middle income countries: position statement of the SIOP PODC Nursing Working Group. Lancet Oncol. (2014) 15:681–2. Available online at: https://www.sciencedirect.com/science/article/abs/pii/S147020451470213X?fr=RR-7&ref=pdf_download&rr=966d946b5b3db6f7 (Accessed June 24, 2025).
24. Almblad AC, Siltberg P, Engvall G, and Målqvist M. Implementation of pediatric early warning score; adherence to guidelines and influence of context. J Pediatr Nurs. (2018) 38:33–9. doi: 10.1016/j.pedn.2017.09.002
25. Reuland C, Shi G, Deatras M, Ang M, Evangelista PPG, and Shilkofski N. A qualitative study of barriers and facilitators to pediatric early warning score (PEWS) implementation in a resource-limited setting. Front Pediatr. (2023) 11. doi: 10.3389/fped.2023.1127752
26. Di Nardo M, Ghafoor S, Szmit Z, Elbahlawan L, Rowan CM, Agulnik A, et al. International expert consensus statement on PICU admission and early critical care management for paediatric patients following haematopoietic cell transplant and immune effector cell therapy. Lancet Child Adolesc Health. (2025) 9:426–38. doi: 10.1016/S2352-4642(25)00091-4
27. Garza M, Graetz DE, Kaye EC, Ferrara G, Rodriguez M, Soberanis Vásquez DJ, et al. Impact of PEWS on perceived quality of care during deterioration in children with cancer hospitalized in different resource-settings. Front Oncol. (2021) 11. doi: 10.3389/fonc.2021.660051
28. Cuttini M, Dall’Oglio I, Ruscitto A, Pagaduan Cabillon E, Broccati F, Ciaralli I, et al. Accuracy of bedside paediatric early warning system (BedsidePEWS) in a pediatric stem cell transplant unit. J Pediatr Oncol Nurs. (2016) 33:249–56. doi: 10.1177/1043454215600154
29. Fausser JL, Tavenard A, Rialland F, Le Moine P, Minckes O, Jourdain A, et al. Should we pay attention to the delay before admission to a pediatric intensive care unit for children with cancer? Impact on 1-month mortality. A report from the French children’s oncology study group, GOCE. J Pediatr Hematol Oncol. (2017) 39:e244–8. doi: 10.1097/MPH.0000000000000816
30. Parshuram CS, Duncan HP, Joffe AR, Farrell CA, Lacroix JR, Middaugh KL, et al. Multicentre validation of the bedside paediatric early warning system score: A severity of illness score to detect evolving critical illness in hospitalised children. Crit Care. (2011) 15. doi: 10.1186/cc10337
31. González-Vicent M, Marín C, Madero L, Sevilla J, and Díaz MA. Risk score for pediatric intensive care unit admission in children undergoing hematopoietic stem cell transplantation and analysis of predictive factors for survival. J Pediatr Hematol Oncol. (2005) 27:526–31. doi: 10.1097/01.mph.0000184637.94923.11
32. Warwick AB, Mertens AC, Ou Shu X, Ramsay NKC, and Neglia JP. Outcomes following mechanical ventilation in children undergoing bone marrow transplantation. Bone Marrow Transplant. (1998) 22:787–94. Available online at: https://www.nature.com/articles/1701417 (Accessed June 4, 2025).
33. Lamas A, Otheo E, Ros P, Vázquez JL, Maldonado MS, Muñoz A, et al. Prognosis of child recipients of hematopoietic stem cell transplantation requiring intensive care. Intensive Care Med. (2003) 29:91–6. doi: 10.1007/s00134-002-1549-2
34. Tomaske M, Bosk A, Eyrich M, Bader P, and Niethammer D. Risks of mortality in children admitted to the paediatric intensive care unit after haematopoietic stem cell transplantation. Br J Haematol. (2003) 121:886–91. doi: 10.1046/j.1365-2141.2003.04390.x
35. Rowan CM, Gertz SJ, McArthur J, Fitzgerald JC, Nitu ME, Loomis A, et al. Invasive mechanical ventilation and mortality in pediatric hematopoietic stem cell transplantation: A multicenter study. Pediatr Crit Care Med. (2016) 17:294–302. doi: 10.1097/PCC.0000000000000673
36. Tamburro RF, Barfield RC, Shaffer ML, Rajasekaran S, Woodard P, Morrison RR, et al. Changes in outcomes (1996-2004) for pediatric oncology and hematopoietic stem cell transplant patients requiring invasive mechanical ventilation. Pediatr Crit Care Med. (2008) 9:270–7. doi: 10.1097/PCC.0b013e31816c7260
Keywords: pediatrics, cancer, hematopoietic stem cell transplantation, early warning score, critical illness, pediatric intensive care unit
Citation: Quijano-Lievano ML, Ramirez O, Chen Y, Robles-Murguia M, Devidas M, Muñiz-Talavera H, Cárdenas-Aguirre A, Portilla C, Castrillon D, Rendon D, De Paula ARPA, Diaz-Coronado R, Sánchez-Martín M, Torres S, Soto Chávez V and Agulnik A (2025) Impact of implementing a pediatric early warning system on outcomes in hematopoietic stem cell transplant units in South America and Europe. Front. Oncol. 15:1712611. doi: 10.3389/fonc.2025.1712611
Received: 24 September 2025; Accepted: 14 November 2025; Revised: 01 November 2025;
Published: 09 December 2025.
Edited by:
Luca Giacomelli, Polistudium srl, ItalyReviewed by:
Natacha Mauz, Centre Hospitalier Annecy Genevois (CH Annecy), FranceBeate Winkler, University Medical Center Hamburg-Eppendorf, Germany
Copyright © 2025 Quijano-Lievano, Ramirez, Chen, Robles-Murguia, Devidas, Muñiz-Talavera, Cárdenas-Aguirre, Portilla, Castrillon, Rendon, De Paula, Diaz-Coronado, Sánchez-Martín, Torres, Soto Chávez and Agulnik. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Asya Agulnik, YXN5YS5hZ3VsbmlrQHN0anVkZS5vcmc=