 Burak Dinçer1*†
Burak Dinçer1*† Mehmet Furkan Sağdıç2†
Mehmet Furkan Sağdıç2† Mehmet Olgun3†Ahmet Karayiğit1†Gülay Bilir Dilek4†Serdar Sarıdemir1†
Mehmet Olgun3†Ahmet Karayiğit1†Gülay Bilir Dilek4†Serdar Sarıdemir1† Cihangir Özaslan1†
Cihangir Özaslan1†- 1Department of Surgical Oncology, University of Health Sciences, Gülhane School of Medicine, Ankara Oncology Training and Research Hospital, Ankara, Türkiye
- 2Department of Surgical Oncology, Ankara Etlik City Hospital, Ankara, Türkiye
- 3Department of Surgery, University of Health Sciences, Gülhane School of Medicine, Ankara Oncology Training and Research Hospital, Ankara, Türkiye
- 4Department of Pathology, University of Health Sciences, Gülhane School of Medicine, Ankara Oncology Training and Research Hospital, Ankara, Türkiye
Background: Subtotal gastrectomy is frequently performed for distally located gastric tumors and carries a lower risk of postoperative complications compared to total gastrectomy. However, due to the submucosal spread pattern and worse prognosis of poorly cohesive carcinoma (PCC), some authors advocate for routine total gastrectomy. This study aimed to compare the outcomes of subtotal versus total gastrectomy in patients with mid- and distal-located gastric PCC.
Methods: This single-center retrospective study included patients who underwent resection for gastric PCC between 2012 and 2024. Exclusion criteria were systemic metastasis, palliative surgery, and tumors located in the proximal one-third of the stomach. Patients were analyzed based on demographic, clinical, pathological, and survival data.
Results: A total of 154 patients were included. The median age was 62 years (range: 36–87), and 83 patients (53.9%) were male. Subtotal gastrectomy was performed in 70 patients (45.5%). The median pathological tumor diameter was 60 mm (IQR: 40–90). Over a median follow-up of 79 months, 33 locoregional and 81 systemic recurrences were observed among 146 patients, and 53 patients (36.3%) were alive at the time of last follow-up. Pathological stage was the only independent factor associated with overall survival, while the type of surgery (subtotal vs. total gastrectomy) did not significantly affect survival outcomes.
Conclusion: Our study demonstrated that subtotal gastrectomy yielded oncologic outcomes similar to those achieved with total gastrectomy in mid- and distal gastric poorly cohesive carcinoma cases.
Introduction
In epidemiological studies, a declining trend in the incidence of gastric cancer has been observed over the years (1). However, this trend differs in populations under the age of 50, in whom an increasing incidence has been reported (2). The overall decrease in incidence may be attributed to a reduced prevalence of Laurén’s intestinal-type gastric cancers, which are more common in high-incidence regions and have declined due to improvements in Helicobacter pylori (HP) eradication and changing dietary habits (3). Gastric poorly cohesive carcinoma (PCC), on the other hand, has a lower overall incidence compared to the intestinal type but tends to present at a younger age, follows a more aggressive clinical course, and exhibits a higher propensity for peritoneal metastasis (4, 5). The increased prevalence of gastric PCC (Laurén’s diffuse-type gastric cancer) in younger populations and in regions with lower overall gastric cancer incidence may explain the rising incidence observed in patients under 50 years of age. Although terms such as signet ring cell carcinoma (SRC) or PCC are used for diffuse-type gastric cancers, there is ongoing debate among pathological classification systems. Consequently, consensus efforts have been made to standardize terminology in the literature (6).
Currently, surgical resection remains the only potentially curative treatment option for gastric cancer. In cases of locally advanced disease, subtotal or total gastrectomy combined with D2 lymph node dissection is typically performed (7). Due to the diffuse infiltration pattern of gastric PCC, some guidelines recommend wider macroscopic resection margins, and intraoperative frozen section analysis is advised when necessary. Because of its aggressive nature and higher risk of microscopic margin positivity, total gastrectomy is more frequently performed in this patient group (8, 9). However, total gastrectomy is associated with higher morbidity and mortality rates compared to subtotal gastrectomy, and long-term oncological outcomes appear similar between the two approaches (10, 11). Given that gastric PCC is underrepresented in many of these studies and data in the literature remain limited, the optimal surgical approach for this tumor subtype remains a matter of debate.
In this study, we aimed to compare the outcomes of total versus subtotal gastrectomy in patients undergoing curative surgery for gastric PCC and to evaluate the oncological adequacy of subtotal gastrectomy in this patient population.
Materials and methods
Study population and selection criteria
In this study, archival records of 878 patients diagnosed with gastric cancer at our center were retrospectively reviewed. A total of 154 patients who underwent subtotal or total gastrectomy for histologically confirmed gastric PCC between 2012 and 2024 were included in the analysis. The study was conducted in accordance with the Declaration of Helsinki and approved by the Non-Interventional Clinical Research Ethics Committee of Ankara Oncology Training and Research Hospital (02.01.2025 – No: 2024-12/198).
Patients aged over 18 years who underwent curative surgery for mid- or distal-located gastric cancer and were pathologically diagnosed with PCC were included. Patients with non-PCC gastric cancer, tumors located in the proximal third of the stomach, those who underwent palliative surgery, had distant metastases or an active malignancy other than gastric cancer, or had incomplete follow-up data or missing data were excluded. Due to the limited number of patients who underwent laparoscopic surgery, most of whom had subtotal gastrectomy, laparoscopic cases were not included in the study. Patients were evaluated based on age, sex, family history, American Society of Anesthesiologists (ASA) physical status score (12), tumor localization, neoadjuvant and adjuvant treatments, surgical details, complications, pathological tumor features, recurrence rates, and survival outcomes.
For pathological classification, the 8th edition of the American Joint Committee on Cancer (AJCC) tumor-node-metastasis staging system for gastric cancer, the 2019 World Health Organization (WHO) Classification of Tumours of the Digestive System (5th edition), and the 2019 consensus report by the European Chapter of the International Gastric Cancer Association were used (6, 13, 14).
In survival analyses, the date of surgery was considered the starting point. Locoregional disease-free survival (LDFS) was defined as the time from surgery to locoregional recurrence, systemic disease-free survival (SDFS) as the time to systemic recurrence, and overall survival (OS) as the time to death. In cases without events, the survival time was calculated as the period from surgery to the last follow-up.
Postoperative complications were assessed using the Clavien-Dindo classification (15). Complications classified as Clavien-Dindo grade 3a or higher were considered major complications, while the rest were defined as minor.
Outcome measures
In our study, overall survival (OS) and the factors influencing OS were determined as the primary outcome. Locoregional disease-free survival (LDFS), systemic disease-free survival (SDFS), and the factors affecting these outcomes were determined as the secondary outcomes.
Surgical techniques
At our center, the standard surgical approach for gastric cancer includes either total or distal gastrectomy, determined based on tumor location. For curative lymphadenectomy, a D2 lymph node dissection was performed as described in the Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition) (16). While laparoscopic surgery was used for eligible patients, open surgery was preferred in cases deemed unsuitable for laparoscopy due to factors such as prior abdominal surgeries, locally advanced tumors, or comorbidities.
Adjuvant treatments and follow-up
Gastric cancer cases were discussed in a multidisciplinary tumor board pre- and postoperatively, and decisions regarding neoadjuvant and/or adjuvant chemotherapy (CT) and/or radiotherapy (RT) were made accordingly. Postoperatively, patients were followed every three months for the first five years with physical examinations and tumor markers, and every six months with radiologic imaging. In clinically stable patients, the follow-up intervals were extended. In cases of local recurrence, systemic staging was performed, and re-resection was planned in selected cases with isolated local recurrence. Patients with systemic recurrence received systemic chemotherapy.
Outcome measures
The primary outcome was to evaluate the impact of subtotal versus total gastrectomy on LDFS, SDFS, and OS in patients who underwent curative surgery for mid- or distal-located gastric PCC. Secondary outcomes included complication rates and rates of local or systemic recurrence during follow-up based on surgical approach.
Statistical analysis
Statistical analysis was performed using SPSS® (Statistical Package for the Social Sciences) version 25.0 (IBM Corp., Armonk, NY, USA) and Jamovi (The jamovi project (2025). jamovi (Version 2.6) [Computer Software]. Retrieved from https://www.jamovi.org). Descriptive statistics, including count, percentage, and median, were used to summarize the study data. The normality of continuous variables was assessed using the Shapiro-Wilk test. Normally distributed continuous variables were presented as mean ± standard deviation, while non-normally distributed variables were expressed as median and interquartile range (IQR). Survival data were analyzed using Kaplan-Meier curves, and factors affecting survival were assessed with the log-rank test. Categorical variables were analyzed using Pearson Chi-square test or Fisher’s Exact test, while continuous variables were compared using Student’s t-test or the Mann-Whitney U test. Parameters found to be significant or nearly significant (p<0.1) in the univariate analysis were included in a multivariate Cox proportional hazards regression model. The proportional hazards assumption was assessed using Schoenfeld residuals for each covariate. All p-values were two-sided, and results were considered statistically significant at p<0.05 with a 95% confidence interval.
Results
A total of 154 patients who underwent curative resection with a diagnosis of PCC were included in our study. Subtotal gastrectomy was performed in 70 patients (45.5%), and total gastrectomy was performed in 84 patients (54.5%), with all patients undergoing D2 lymphadenectomy. The median age of the patients was 62 years (range: 36–87), and 83 patients (53.9%) were male. A family history of cancer was present in 29.9% of the patients. The ASA score was 2 in 91 patients. Tumors were located in the gastric corpus in 101 patients. Neoadjuvant CT was administered to 20 patients, while no patients received neoadjuvant RT. In the postoperative period, 75.3% of patients received adjuvant CT and 37% received adjuvant RT. Tumors located in the antrum were significantly more common in patients who underwent subtotal gastrectomy (p<0.001). No significant differences were observed between the groups in other demographic and clinical parameters (Table 1).
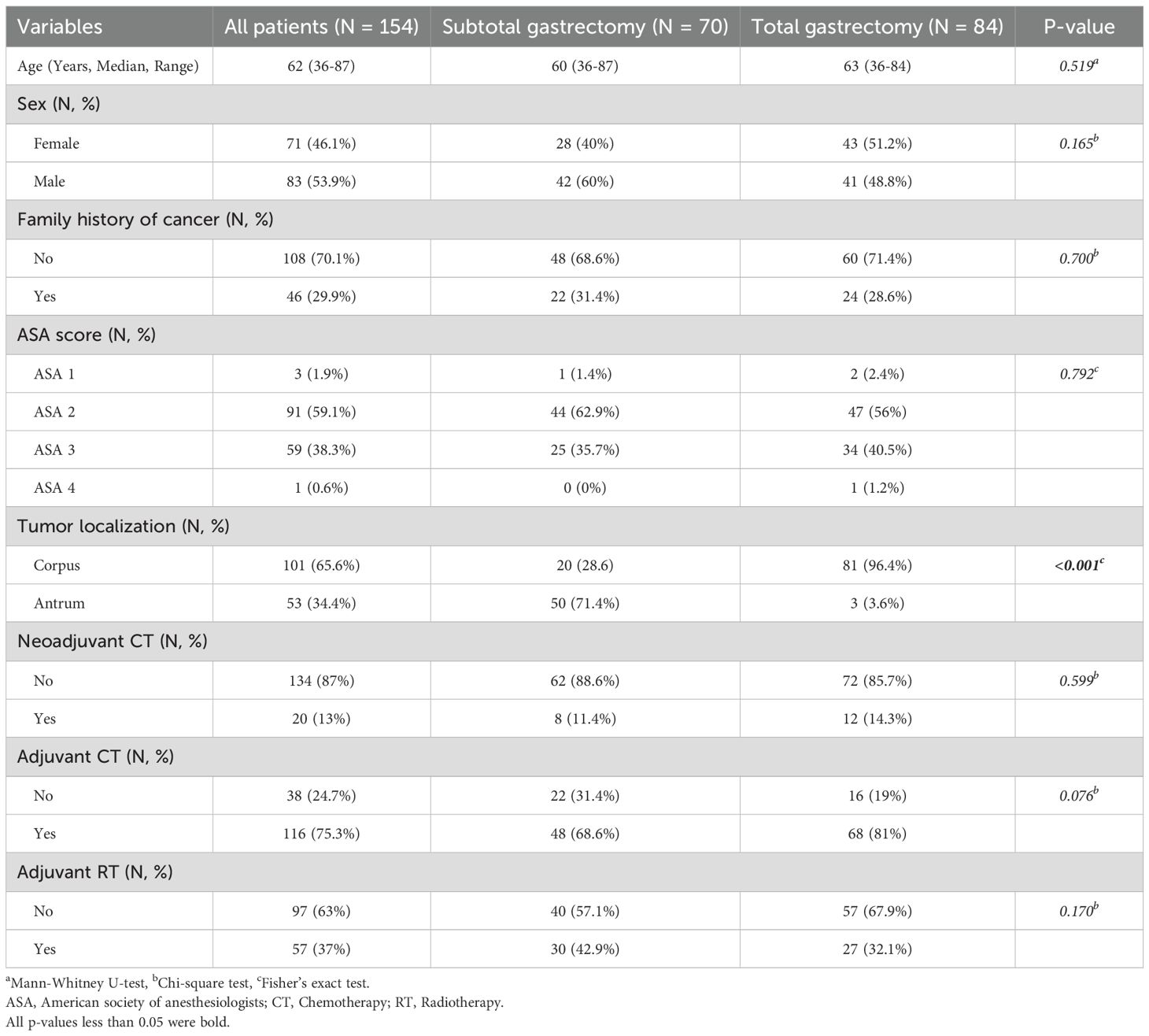
Table 1. Demographic and clinical characteristics.
The median length of hospital stay was 11 days (IQR 9–14). Surgical complications occurred in 37 patients (24%), and major complications (Clavien-Dindo grade 3a or higher) were observed in 22 patients (14.3%). Postoperative 30-day mortality due to surgery-related complications occurred in 8 patients (5.2%). Although the 30-day postoperative mortality was higher in the total gastrectomy group, the difference was not statistically significant (p=0.497) (Table 2).

Table 2. Surgical and pathological parameters.
The median pathological tumor size was 60 mm (IQR 40–90). The most common histological subtype was PCC-not otherwise specified (NOS), accounting for 62.3% of cases. Poor differentiation was observed in 92 patients (59.7%). The most common pathological stage was stage 3C, observed in 42 patients (27.3%). Surgical margin positivity was present in 13 patients (8.4%). No secondary surgery was performed in this R1 resection group; instead, appropriate adjuvant therapies were administered. Tumors in the total gastrectomy group were significantly larger, more poorly differentiated, at a more advanced stage, and showed a higher rate of lymphovascular and perineural invasion (p<0.001, p=0.007, p<0.001, p=0.002, and p<0.001, respectively) (Table 2).
During a median follow-up of 79 months, 33 locoregional and 81 systemic recurrences were observed in 146 patients. At the time of last follow-up, 53 patients (36.3%) were alive (8 patients who died within 30 days postoperatively due to surgical complications were excluded from the survival analysis). Systemic recurrence and mortality rates were significantly higher in the total gastrectomy group (p=0.002 and p=0.021, respectively), whereas locoregional recurrence rates were similar between the groups (p=0.650). LDFS was comparable between the subtotal and total gastrectomy groups (p=0.440). However, both SDFS and OS were significantly lower in the total gastrectomy group (p=0.001 and p=0.009, respectively) (Table 3, Figure 1).

Table 3. Follow-up and survival times (Postoperative mortalities excluded).

Figure 1. Kaplan-Meier curves demonstrating (a) locoregional disease-free survival, (b) systemic disease-free survival, and (c) overall survival in patients who underwent subtotal or total gastrectomy for gastric poorly cohesive carcinoma.
Variables found to be statistically significant or borderline significant (p<0.1) in univariate analysis were further evaluated using multivariate Cox regression analysis. Only pathological stage was identified as an independent factor affecting OS, while surgical approach (subtotal vs. total gastrectomy) was not found to be an independent predictor of survival (Table 4).

Table 4. Factors associated with LDFS, SDFS and OS (multivariate analysis).
Discussion
Surgery plays a central role in the current treatment approach to gastric cancer, with R0 resection offering curative potential in locoregional disease. Given their more aggressive clinical course compared to classical intestinal-type gastric cancers, PCC cases are often considered more suitable for total gastrectomy according to several publications and guidelines (8, 9). However, studies comparing the outcomes of subtotal and total gastrectomy in this specific patient population remain limited. In a multicenter study by M. Boubaddi et al. (17), it was reported that subtotal gastrectomy for distally located PCC cases yields comparable oncologic outcomes with fewer complications. In our study, not only antrum-located tumors but also mid-gastric PCCs that were technically amenable to subtotal gastrectomy were analyzed. Multivariate analysis showed that the type of gastrectomy (subtotal vs. total) had no significant impact on survival.
It has been well documented that complications following gastric cancer resection are associated with poorer prognosis, as they increase the risk of recurrence and may delay adjuvant treatments (18–21). In our study, although major complications were observed more frequently in patients who underwent total gastrectomy, the difference was not statistically significant. Based on both current literature and our findings, subtotal gastrectomy may be associated with fewer complications and may contribute positively to survival in appropriately selected patients.
Tumor stage remains one of the most critical factors guiding treatment in gastric cancer (22, 23). In our study, total gastrectomy were more commonly performed in patients with more advanced stage, poorly differentiated tumors, and those with lymphovascular and perineural invasion. This may reflect a preference for total gastrectomy in order to better adhere to oncologic principles and achieve wider resection margins, potentially improving local control. However, our multivariate analysis demonstrated that the type of gastrectomy is not adversely affect prognosis. The only independent prognostic factor for overall survival was pathological stage, consistent with findings in the literature.
The primary limitations of our study include its retrospective design and single-center setting. Additionally, patients undergoing total gastrectomy tended to have more advanced, poorly differentiated, and biologically aggressive tumors, which could bias comparisons between subtotal and total gastrectomy outcomes. The relatively small number of patients receiving neoadjuvant therapy also limits the generalizability of our findings. Also, the inclusion of only patients who underwent open surgery in our study limits the evaluation of the potential impact of laparoscopy on prognosis in these cases. In addition, due to a lack of data, the impact of surgical margin distance on survival could not be evaluated, and further studies are needed to determine the optimal surgical margin in these patients.
Conclusions
Based on our findings, subtotal gastrectomy may be a feasible option in mid and distal gastric poorly cohesive carcinoma cases, offering comparable oncologic outcomes. Prospective studies comparing subtotal and total gastrectomy and minimal invasive techniques in this patient population are warranted to further enrich the current literature.
Data availability statement
The datasets generated and analyzed during the current study are not publicly available but are available from the corresponding author on reasonable request. Requests to access these datasets should be directed to YnVyYWstZGluY2VyQGhvdG1haWwuY29t.
Ethics statement
The studies involving humans were approved by Non-Interventional Clinical Research Ethics Committee of Ankara Oncology Training and Research Hospital (02.01.2025 – No: 2024-12/198). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
BD: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Visualization, Writing – original draft, Writing – review & editing. MS: Methodology, Validation, Visualization, Writing – review & editing. MO: Methodology, Validation, Visualization, Writing – review & editing. AK: Methodology, Validation, Visualization, Writing – review & editing. GD: Methodology, Validation, Visualization, Writing – review & editing. SS: Methodology, Validation, Visualization, Writing – review & editing. CÖ: Conceptualization, Methodology, Project administration, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660
2. Arnold M, Park JY, Camargo MC, Lunet N, Forman D, and Soerjomataram I. Is gastric cancer becoming a rare disease? A global assessment of predicted incidence trends to 2035. Gut. (2020) 69:823–9. doi: 10.1136/gutjnl-2019-320234
3. Ahn HJ and Lee DS. Helicobacter pylori in gastric carcinogenesis. World J Gastrointest Oncol. (2015) 7:455–65. doi: 10.4251/wjgo.v7.i12.455
4. Assumpção PP, Barra WF, Ishak G, Coelho LGV, Coimbra FJF, Freitas HC, et al. The diffuse-type gastric cancer epidemiology enigma. BMC Gastroenterol. (2020) 20:223. doi: 10.1186/s12876-020-01354-4
5. Koemans WJ, Luijten J, van der Kaaij RT, Grootscholten C, Snaebjornsson P, Verhoeven RHA, et al. The metastatic pattern of intestinal and diffuse type gastric carcinoma - A Dutch national cohort study. Cancer Epidemiol. (2020) 69:101846. doi: 10.1016/j.canep.2020.101846
6. Mariette C, Carneiro F, Grabsch HI, van der Post RS, Allum W, and de Manzoni G. Consensus on the pathological definition and classification of poorly cohesive gastric carcinoma. Gastric Cancer. (2019) 22:1–9. doi: 10.1007/s10120-018-0868-0
7. Smyth EC, Nilsson M, Grabsch HI, van Grieken NC, and Lordick F. Gastric cancer. Lancet. (2020) 396:635–48. doi: 10.1016/s0140-6736(20)31288-5
8. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2018 (5th edition). Gastric Cancer. (2021) 24:1–21. doi: 10.1007/s10120-020-01042-y
9. Smyth EC, Verheij M, Allum W, Cunningham D, Cervantes A, and Arnold D. Gastric cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2016) 27:v38–49. doi: 10.1093/annonc/mdw350
10. Ju T, Rivas L, Kurland K, Chen S, Sparks A, Lin PP, et al. National trends in total vs subtotal gastrectomy for middle and distal third gastric cancer. Am J Surg. (2020) 219:691–5. doi: 10.1016/j.amjsurg.2019.04.012
11. Ji X, Yan Y, Bu ZD, Li ZY, Wu AW, Zhang LH, et al. The optimal extent of gastrectomy for middle-third gastric cancer: distal subtotal gastrectomy is superior to total gastrectomy in short-term effect without sacrificing long-term survival. BMC Cancer. (2017) 17:345. doi: 10.1186/s12885-017-3343-0
12. Rosa F, Tortorelli AP, Quero G, Galiandro F, Fiorillo C, Sollazzi L, et al. The impact of preoperative ASA-physical status on postoperative complications and long-term survival outcomes in gastric cancer patients. Eur Rev Med Pharmacol Sci. (2019) 23:7383–90. doi: 10.26355/eurrev_201909_18846
13. Mranda GM, Xue Y, Zhou XG, Yu W, Wei T, Xiang ZP, et al. Revisiting the 8th AJCC system for gastric cancer: A review on validations, nomograms, lymph nodes impact, and proposed modifications. Ann Med Surg (Lond). (2022) 75:103411. doi: 10.1016/j.amsu.2022.103411
14. Nagtegaal ID, Odze RD, Klimstra D, Paradis V, Rugge M, Schirmacher P, et al. The 2019 WHO classification of tumours of the digestive system. Histopathology. (2020) 76:182–8. doi: 10.1111/his.13975
15. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. (2009) 250:187–96. doi: 10.1097/SLA.0b013e3181b13ca2
16. Japanese Gastric Cancer A. Japanese gastric cancer treatment guidelines 2021 (6th edition). Gastric Cancer. (2023) 26:1–25. doi: 10.1007/s10120-022-01331-8
17. Boubaddi M, Teixeira Farinha H, Lambert C, Pereira B, Piessen G, Gualtierotti M, et al. Total versus subtotal gastrectomy for distal gastric poorly cohesive carcinoma. Ann Surg Oncol. (2024) 31:744–52. doi: 10.1245/s10434-023-14496-y
18. Ohtsuka T, Kitajima Y, Takahashi T, Sato S, Miyoshi A, Kohya N, et al. Infectious complications after gastric cancer surgery accelerate a rapid hepatic recurrence. Hepatogastroenterology. (2009) 56:1277–80.
19. Ebihara Y, Kyogoku N, Murakami Y, Murakawa K, Nakamura F, Morita T, et al. Relationship between laparoscopic total gastrectomy-associated postoperative complications and gastric cancer prognosis. Updates Surg. (2023) 75:149–58. doi: 10.1007/s13304-022-01402-6
20. Obana A, Iwasaki K, and Suwa T. Impact of postoperative complications on gastric cancer survival. Surgery. (2025) 178:108873. doi: 10.1016/j.surg.2024.09.031
21. Saunders JH, Yanni F, Dorrington MS, Bowman CR, Vohra RS, and Parsons SL. Impact of postoperative complications on disease recurrence and long-term survival following oesophagogastric cancer resection. Br J Surg. (2020) 107:103–12. doi: 10.1002/bjs.11318
22. Li W, Zhu H, Dong HZ, Qin ZK, Huang FL, Yu Z, et al. Impact of body composition parameters, age, and tumor staging on gastric cancer prognosis. Eur J Cancer Prev. (2025) 34:267–75. doi: 10.1097/cej.0000000000000917
Keywords: gastric cancer, Lauren’s diffuse gastric cancer, poorly cohesive carcinoma, subtotal gastrectomy, total gastrectomy
Citation: Dinçer B, Sağdıç MF, Olgun M, Karayiğit A, Dilek GB, Sarıdemir S and Özaslan C (2025) Subtotal versus total gastrectomy for mid- and distal gastric poorly cohesive carcinoma: a retrospective controlled study. Front. Oncol. 15:1717678. doi: 10.3389/fonc.2025.1717678
Received: 02 October 2025; Accepted: 07 November 2025; Revised: 02 November 2025;
Published: 24 November 2025.
Edited by:
Xiaojun Liu, Lanzhou University Third Hospital, ChinaReviewed by:
Jorge Gajardo, Universidad de Concepción, ChileCem Ilgin Erol, Medicana Hospital, Türkiye
Copyright © 2025 Dinçer, Sağdıç, Olgun, Karayiğit, Dilek, Sarıdemir and Özaslan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Burak Dinçer, YnVyYWstZGluY2VyQGhvdG1haWwuY29t; YnVyYWsuZGluY2VyQHNidS5lZHUudHI=
†ORCID: Burak Dinçer, orcid.org/0000-0002-3133-9627
Mehmet Furkan Sağdıç, orcid.org/0000-0002-3598-1625
Mehmet Olgun, orcid.org/0009-0000-3398-9546
Ahmet Karayiğit, orcid.org/0000-0003-0380-9190
Gülay Bilir Dilek, orcid.org/0000-0003-2458-578X
Serdar Sarıdemir, orcid.org/0000-0002-9979-9662
Cihangir Özaslan, orcid.org/0000-0002-2611-4837