 Moréniké Oluwátóyìn Foláyan
Moréniké Oluwátóyìn Foláyan Nicaise Ndembi
Nicaise Ndembi Olunike Rebecca Abodunrin
Olunike Rebecca Abodunrin Bridget Haire
Bridget Haire- 1The Africa Oral Health Network (AFRONE), Alexandria University, Alexandria, Egypt
- 2Department of Child Dental Health, Obafemi Awolowo University, Ile Ife, Nigeria
- 3Director General's Office, International Vaccine Institute (IVI), Africa Regional Office, Kigali, Rwanda
- 4Division of Epidemiology and Prevention, Institute of Human Virology, University of Maryland School of Medicine, Baltimore, MD, United States
- 5Department of Epidemiology and Biostatistics, Nanjing Medical University, Nanjing, Jiangsu, China
- 6School of Population Health and Kirby Institute, University of New South Wales, Sydney, NSW, Australia
Current, globally accepted definitions of oral health emphasize pain-free functionality, expressive capacity, and specific psychosocial dimensions that contribute to self-confidence, well-being, and societal participation. However, these definitions inadvertently exclude diverse lived experiences by framing oral health solely through a lens of “normal” functionality and absence of discomfort, failing to consider the ways in which oral health can be experienced uniquely by different individuals and communities. The narrow focus on “pain-free” oral health excludes valid aspects of sexual expression, which may involve consensual oral activities that some find pleasurable even if associated with discomfort. This manuscript examines the limitations of the WHO and FDI definitions of oral health, critiques their exclusion of minority perspectives, and advocates for a more inclusive, holistic approach. Such an approach recognizes the complex and varied ways oral health intersects with identity, intimacy, and societal norms. Normalizing discussions on oral sexual health are essential to advancing a comprehensive understanding of well-being and reducing stigma around sexual minority experiences. Expanding oral health definitions to accommodate broader conceptions of intimacy and pleasure can enhance public health policy, clinical practice, and education, fostering a comprehensive understanding of well-being that reduces stigma around sexual minority experiences and further marginalization of sexual minorities in accessing inclusive care.
Introduction
The concept of oral health as pain-free functionality is enshrined in two prominent, globally accepted definitions of oral health. These two definitions differ somewhat in their emphasis: the FDI World Dental Federation's definition centers on the absence of pain, disease, and discomfort (1) and aims to ensure functional and expressive well-being. The definition by the World Health Organization describes oral health as a state enabling essential functions—eating, breathing, speaking—and encompassing dimensions such as self-confidence, societal participation, and freedom from discomfort or embarrassment (2). These concepts of oral health align with traditional views of health as freedom from suffering, allowing individuals to eat, speak, smile, and communicate with ease.
Together, the definitions emphasize the biopsychosocial model of health, including (3) the connection between oral health and general well-being, and this perspective supports vital aspects of well-being (4). The model is celebrated because it offers a holistic approach to understanding health and illness, integrating biological, psychological, and social dimensions into the understanding of health (5). This broader perspective acknowledges the significant role that mental health, social environments, and personal behaviors play in influencing health outcomes (6). It contrasts with the traditional biomedical model, which primarily focuses on the biological aspects of health (7). The biopsychosocial model promotes personalized care by encouraging healthcare providers to create treatment plans that address not only physical symptoms but also psychological issues, such as stress, and social factors, such as family dynamics or socioeconomic conditions (8).
Further, the biopsychosocial model emphasizes the importance of prevention. Recognizing the interconnectedness of mental and social well-being, it encourages patients to actively manage their health, adopt behavioral changes, and develop coping strategies (9). This focus on prevention extends to promoting better doctor-patient relationships, where understanding a patient's psychological and social contexts can enhance communication, trust, and the overall effectiveness of care (10). The model is particularly beneficial in managing chronic illnesses, where psychological stress and social conditions often exacerbate physical symptoms (11).
However, the biopsychosocial model of oral health has its limitations. Its broad and integrated approach can be challenging to implement in busy clinical settings due to time constraints, limited resources, and a lack of training in non-medical areas like psychology and social work (9). In addition, psychological and social factors can be subjective and difficult to measure, leading to inconsistencies in care. While there is substantial evidence supporting the role of biological factors in health, there is less research on the effectiveness of interventions targeting psychological and social aspects, making it harder to standardize treatment protocols (12). The inclusivity of the model can also lead to overgeneralization, as it may be difficult to determine the relative contribution of each factor to a patient's health, potentially complicating accurate diagnoses (13). Furthermore, the effective application of the model requires a wide range of healthcare professionals and resources, which may not be readily available, particularly in low-resource settings, including many African countries (8).
Moreover, as a key determinant of overall health and well-being, oral health encompasses various social and cultural dimensions. For some, oral health experiences involve nuanced dynamics of pleasure and pain, which are valid elements of their lived realities (14). The narrow view of oral health where wellness and well-being are defined as the absence of pain and discomfort overlooks the experiences of a minority of people, for whom pain and discomfort may not preclude wellness and well-being. In effect, discomfort and pain are not universally perceived as negative, and their absence does not always reflect or contribute to wellness and well-being.
The current definition and its limitations
The current concept of oral health is framed in a somewhat binary way—defined by the presence or absence of disease or discomfort. However, this narrow understanding of health as simply the absence of disease fails to capture the full complexity of oral wellness and well-being. Discomfort and pain, often seen as negative indicators of oral health, are not universally perceived in the same way across cultures or even within individuals. The absence of discomfort or pain does not necessarily correlate with the complete absence of underlying health issues, nor does it always imply that an individual is in a state of well-being (15, 16). For example, individuals who have oral diseases, such as gingivitis or incipient cavities that are not causing pain or discomfort, may still experience lasting effects from the diseases on their well-being.
In addition, cultural perceptions of pain and discomfort can vary significantly (17). In some cultures, pain might be viewed as a normal part of life or a minor inconvenience, while in others, it might be considered a more significant marker of poor health. This subjectivity means that the absence of pain or discomfort is not a universally reliable measure of oral health, and it is possible for someone to feel physically well while experiencing significant psychological or social distress related to their oral health (18). For instance, an individual with cosmetic dental issues that do not cause pain may still feel socially isolated or experience a reduction in quality of life due to low self-esteem or social stigma.
Of concern also is the failure of the framing of oral health to take account of the experiences of those who associate oral experiences, such as certain forms of intimacy, with positive sensations, regardless of discomfort. Individuals may have positive experiences associated with consensual oral activities that may not always be pain-free but are nevertheless consensually pleasurable.
This restrictive understanding may contribute to an environment where oral health professionals lack the language or frameworks to engage with patients on diverse oral health experiences, perpetuating silence and stigma around topics such as oral sexual health. While a pain-free life may be ideal, for some, certain types of controlled pain or discomfort may be integral and acceptable aspects of life that, when related to sexual satisfaction, may be closely linked to well-being. Consequently, framing oral health solely through an absence of pain may inadvertently negate the diversity of intimate practices. This oversight becomes particularly critical in the context of public health, where definitions and frameworks influence clinical practices, health education, and policies. A limited understanding of oral health may encourage judgment or silence in clinical settings, limiting opportunities to discuss, normalize, and support diverse oral health behaviors.
Pain, pleasure, and oral health: reframing definitions
Oral health can encompass varied expressions of identity and intimacy that may involve consensual discomfort or pain, challenging conventional definitions of health. For some, experiences like oral sexual health are integral to their well-being and identity (19). A more inclusive oral health framework that recognizes these realities could enable health policies that validate diverse expressions of intimacy and selfhood. By normalizing discussions around oral sexual health, health systems can better support individuals’ psychosocial well-being, contributing to a holistic understanding of health that respects personal experiences and preferences.
Oral sex is a sexual activity with genital stimulation using the mouth, tongue, teeth, or throat, including oral-vaginal/clitoral contact (cunnilingus), oral-penile contact (fellatio), and oral-anal contact (anilingus). It can be practiced by sex partners of all sexualities (20). Performing oral sex may cause discomfort for some, but this does not necessarily reduce sexual satisfaction, and there is evidence that oral sex enhances well-being and sex life, especially in older adults (21, 22).
Prevalence of oral sex
When definitions of oral health are framed narrowly or without consideration of the full range of oral behaviors, such as oral sex, they can overlook key aspects of oral health and wellness that affect a large proportion of the population. We conducted a rapid review of the literature to identify publications on the prevalence of oral sex. The search was conducted in PubMed and the Web of Science database without any restrictions on the publication year. The search terms used were: Prevalence AND [oral (sex OR “sexual behavior” OR “sexual practices”)] OR cunnilingus, “oral vaginal contact” OR fellatio OR “oral penile contact”. Studies included in the rapid review were cross-sectional, cohort, and systematic reviews. Case-control, randomized controlled trials, quasi-experimental studies, policy analyses, opinion pieces, and editorials were excluded. The references of the included studies were also studied for additional publications.
We identified 13 studies that met the eligibility criteria (23–35). The summary of the publications is highlighted in Table 1. The practice of oral sex varies widely across populations and contexts. Among young adults in the U.S., 66% of women and 65% of men aged 15–24 reported having engaged in oral sex (28). Prevalence among adolescents globally ranges from 1.7% to 26.6%, with university students reporting higher rates (5% to 46.4%) (31). In Kinshasa, 59% of sexually active individuals reported oral sex, in Singapore, prevalence among female sex workers rose from 27.1% to 81.1% between 1992 and 1997 (23, 32), while in Nigeria, 69% of men who have sex with men and transgender women reported oral sex (34).
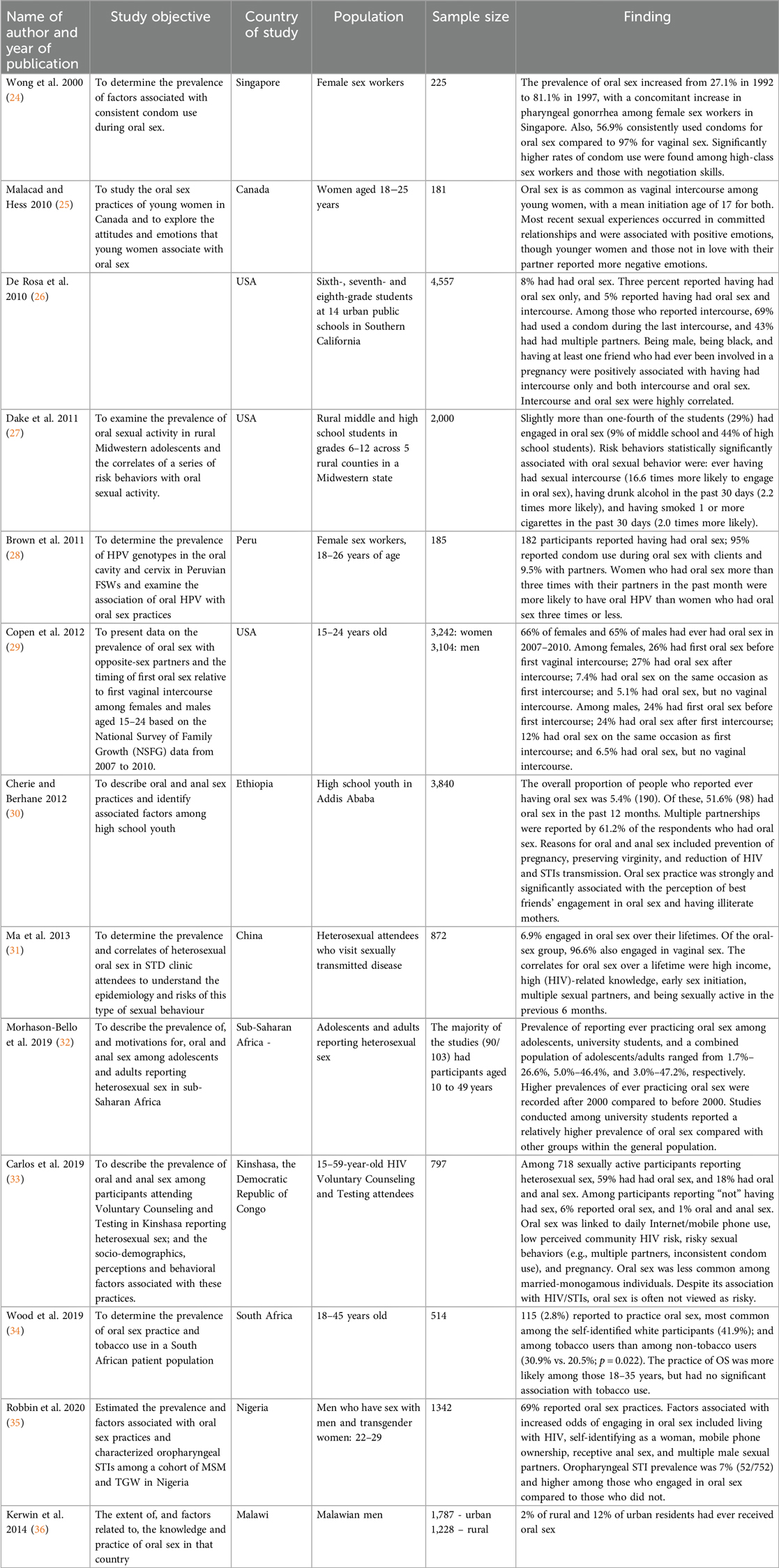
Table 1. Summary of the publications on the prevalence of oral sex.
Variations also exist across demographics, with 41.9% of self-identified white individuals in South Africa reporting oral sex compared to 2.8% overall (33), 5.4% of Ethiopian high school youth associating the practice with peer norms and maternal education (33), and urban populations in Malawi (12%) reported higher prevalence compared to rural counterparts (2%) (36).
Oral sex is often linked in the literature to risky behaviors, including multiple sexual partners, early initiation, and substance use (26, 30). The inconsistent use of condoms during oral sex was a recurring theme, as seen in Singapore and Peru (23, 27), although oral sex is far less risky than penetrative sex. This inconsistency contrasts with higher condom use rates for vaginal sex (23). Sociocultural factors, such as peer influence and education, significantly shape practices and attitudes (29). Despite its association with sexually transmitted infections like human papilloma virus and gonorrhea (27, 34), it is frequently perceived as low risk and a safer alternative to vaginal intercourse (29, 32).
Oral sex is practiced by adults of all genders, ages, and races (36). Among older adults born after 1942, 80% of men and 70% of women report giving or receiving oral sex (21, 22). The proportion of people who engage in oral sex has increased over the years (21), with younger individuals more likely to report engaging in oral sex (24, 33), and initiation often occurring during adolescence or early adulthood (30). Oral health is linked to intimacy, identity, and well-being. These findings underscore the complexity of addressing oral sex practices in public health strategies. Recognizing the sexual dimensions of oral health can reduce stigma, particularly for marginalized groups like sexual and gender minority individuals and sex workers, and foster more comprehensive public health strategies built on the importance of sexual health for the attainment of oral health.
One of the fundamental challenges with the exclusion of oral sex from discussions about oral health is the associated multiple risks, both in terms of health outcomes and societal perceptions. The risks of this exclusion are compounded by the fact that oral sex has become increasingly common and socially accepted as part of sexual expression (37). Failing to incorporate this into health frameworks can result in misinformed or under-informed public health messaging, stigmatization, and neglect in oral health care. It is associated with the transmission of sexually transmitted infections although this risk is lower than that of vaginal or anal sex (38). In addition, oral cancer (linked to HPV) can be associated with oral sex (39). The absence of discussions about oral sex during oral health education can lead to a lack of preventive measures, such as appropriate vaccinations (e.g., the HPV vaccine), and consideration of barriers like dental dams or condoms during oral sex should an infection be present (40). In addition, people who engage in oral sex may feel a sense of shame or guilt if they perceive their behavior as being unmentionable in healthcare contexts. This may impact their willingness to seek advice or treatment, particularly if they are experiencing oral health issues such as sores, lesions, or other symptoms that could be linked to an orally transmitted sexual infection.
The current definitions of oral health contribute to systemic erasure—the institutional exclusion of marginalized experiences that do not conform to biomedical norms (41). This omission has significant consequences. It pathologizes experiences, renders invisible cultural contexts such as Indigenous oral rituals or African dental modifications, and ignores oral sexual health. The consequences of this erasure are far-reaching, resulting in gaps in public health messaging, limited research on oral health's intersection with sexuality and cultural practices, and policy frameworks that prioritize disease-free metrics over holistic well-being. Systemic erasure in oral health definitions is not a passive oversight—it is a structural barrier to equity. By equating health with biological ‘normalcy, current frameworks exclude the very populations most vulnerable to oral health disparities. Redefining oral health requires dismantling these hierarchies to ensure that no individual's well-being is invalidated by the narrowness of existing definitions.
To avoid the risks associated with systemic erasure, it is essential to frame oral health more inclusively and comprehensively—one that recognizes the full range of behaviors that contribute to both physical and psychosocial well-being. A more holistic definition would address oral health in the context of sexual health, acknowledging that oral sex is a common and significant practice for many individuals. By doing so, we can ensure that individuals receive comprehensive health education that encompasses not only the prevention of disease but also the acknowledgment of various sexual practices and their impact on health.
A more inclusive definition of oral health and the policy implications
A more inclusive definition of oral health would allow for more open dialogue and reduce the stigma surrounding sexual health discussions. A more inclusive definition of oral health could be:
Oral health is a state of well-being that includes the absence of disease in the oral cavity, its ability to function in ways that allow individuals to speak, eat, smile, taste, touch, chew, swallow, and convey a range of emotions through facial expressions comfortably with consideration of the psychological, social, and sexual factors that influence oral well-being.
This definition incorporates both the traditional aspects of oral health (e.g., the physical condition of the mouth and teeth) and the modern realities of sexual health, recognizing the need for preventive education and care. By including sexual factors (i.e., oral sex) in the discussion of oral health, healthcare systems can better address the full spectrum of behaviors that influence health outcomes and provide individuals with the tools they need to protect themselves and maintain their overall well-being.
Oral sex is a widespread practice across diverse populations, spanning countries, races, ages, and genders. However, this paper moves beyond prevalence statistics to argue that current oral health definitions fail to recognize minority experiences as valid aspects of well-being. The paradox is clear: while oral sex is practiced globally, its omission from oral health definitions reflects systemic biases that privilege particular norms. Our proposed inclusive definition integrates psychosocial and sexual dimensions, challenging dominant hierarchies that position minority experiences as peripheral rather than integral to oral health. Silence perpetuates disparities. Expanding definitions to reflect lived realities is essential in dismantling stigma and ensuring equitable care.
Moving from evidence to action requires structural change. Medical education must equip oral health providers to discuss oral sexual health without judgment, addressing gaps in promoting oral health that is not based exclusively on the experience of the majority. Public health campaigns should adopt inclusive messaging, recognizing the influence of education on sexual health behaviours. In addition, research funding must prioritize marginalized voices, ensuring that oral health frameworks reflect the realities of diverse communities. Without such shifts, the biopsychosocial model remains theoretical, failing those whose well-being is shaped by more than biomedical factors alone. By prioritizing inclusivity, oral health can move from a tool of exclusion to one of empowerment, ensuring no individual's well-being is rendered invisible by narrow definitions.
A truly inclusive oral health policy acknowledges and respects the diversity of individual experiences and identities. Expanding current definitions of oral health to encompass aspects of consensual sexual pleasure, psychosocial well-being, and cultural nuances would allow health systems to foster environments where all individuals feel respected. By doing so, policy frameworks can better address the needs of all people who engage in oral sexual practices, including minority populations.
One critical step toward inclusivity is re-evaluating educational content for health professionals. Incorporating culturally competent approaches in the dental and public health educational curriculum, especially regarding oral sexual health, can reduce stigma and promote discussions on oral health in the context of intimacy and pleasure, which would support this shift. These educational advancements would not only increase provider competency but also empower healthcare workers to engage respectfully and openly with patients, regardless of their backgrounds or sexual practices. By normalizing discussions around oral sexual health, providers can ensure that patients are comfortable discussing their full health histories, which is essential for comprehensive care. This shift in policy would require collaborative efforts among dental associations, policymakers, and healthcare professionals.
Conclusion
The current definitions of oral health by the FDI and WHO, while foundational, are fundamentally limited by their narrow focus on pain-free functionality. These frameworks fail to acknowledge a critical truth: oral health is a dynamic interplay of biological, psychological, and sociocultural factors—including practices like oral sex that hold diverse meanings across populations and communities. By equating health solely with the absence of disease, these definitions invalidate the lived realities of individuals for whom oral health encompasses pleasure, intimacy, or culturally specific practices. This exclusion is not merely an oversight; it is a form of systemic erasure that perpetuates stigma, particularly for sexual and gender minorities, older adults, and marginalized populations whose sexual practices and health needs are rendered invisible.
To truly advance equity in oral health, we must reject definitions that prioritize biomedical norms over human diversity. An inclusive framework must recognize that well-being is not universally defined by comfort—for many, it involves consensual practices that may challenge traditional health paradigms. Such a shift would transform clinical practice: dismantling taboos, empowering providers to deliver culturally competent care, and validating patients who have long been marginalized by rigid health standards. Policymakers must act urgently to expand these definitions, ensuring they reflect the full spectrum of human experience. The evidence is clear: when practices vary so widely across ages, cultures, and identities, our definitions must be equally expansive. Anything less perpetuates harm under the guise of neutrality.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here.
Author contributions
MF: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. NN: Funding acquisition, Writing – review & editing. OA: Data curation, Writing – review & editing. BH: Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. IHVN is funding the publication of this paper. NN is supported by the US NIH/ NIAID R01 AI147331-04.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. Chat GPT was used to generate the outline and to edit the grammar.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Glick M, Williams DM, Kleinman DV, Vujicic M, Watt RG, Weyant RJ. A new definition for oral health developed by the FDI world dental federation opens the door to a universal definition of oral health. J Am Dent Assoc. (2016) 147(12):915–17. doi: 10.1016/j.adaj.2016.10.001
2. World Health Organisation. Oral Health. Available at: https://www.who.int/health-topics/oral-health#tab=tab_1 (Accessed December 14, 2024).
3. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. (1977) 196(4286):129–36. doi: 10.1126/science.847460
4. Mills A, Berlin-Broner Y, Levin L. Improving patient well-being as a broader perspective in dentistry. Int Dent J. (2023) 73(6):785–92. doi: 10.1016/j.identj.2023.05.005
5. Borrell-Carrió F, Suchman AL, Epstein RM. The biopsychosocial model 25 years later: principles, practice, and scientific inquiry. Ann Fam Med. (2004) 2(6):576–82. doi: 10.1370/afm.245
6. Roberts A. The biopsychosocial model: its use and abuse. Med Health Care and Philos. (2023) 26:367–84. doi: 10.1007/s11019-023-10150-2
7. Rocca E, Anjum RL. Complexity, reductionism and the biomedical model. In: Anjum RL, Copeland S, Rocca E, editors. Rethinking Causality, Complexity and Evidence for the Unique Patient. Cham.: Springer (2020). p. 75–94. doi: 10.1007/978-3-030-41239-5_5
8. Bolton D, Gillett G. Chapter 1 the biopsychosocial model 40 years on. In: Bolton D, Gillett G, editors. The Biopsychosocial Model of Health and Disease: New Philosophical and Scientific Developments. Cham (CH): Palgrave Pivot (2019).
9. Kusnanto H, Agustian D, Hilmanto D. Biopsychosocial model of illnesses in primary care: a hermeneutic literature review. J Family Med Prim Care. (2018) 7(3):497–500. doi: 10.4103/jfmpc.jfmpc_145_17
10. Persaud-Sharma D, Govea M, Hernandez R. Medical ethics and the biopsychosocial model for patient care: a case analysis for improved communication, clinical time, and error avoidance. Cureus. (2020) 12(6):e8535. doi: 10.7759/cureus.8535
11. Meints SM, Edwards RR. Evaluating psychosocial contributions to chronic pain outcomes. Prog Neuropsychopharmacol Biol Psychiatry. (2018) 87(Pt B)):168–82. doi: 10.1016/j.pnpbp.2018.01.017
12. Committee on Developing Evidence-Based Standards for Psychosocial Interventions for Mental Disorders, Board on Health Sciences Policy; Institute of Medicine. Psychosocial Interventions for Mental and Substance Use Disorders: A Framework for Establishing Evidence-Based Standards. England MJ, Butler AS, Gonzalez ML, editors. Washington, DC: National Academies Press (US) (2015).
13. Syed S, Syed S, Bhardwaj K. The role of the bio-psychosocial model in public health. JMR. (2020) 6(5):252–4. doi: 10.31254/jmr.2020.6517
14. Uziel N, Bronner G, Elran E, Eli I. Sexual correlates of gagging and dental anxiety. Community Dent Health. (2012) 29(3):243–7.23038943
15. Miller ET, Abu-Alhaija DM. Cultural influences on pain perception and management. Pain Manag Nurs. (2019) 20:183–4. doi: 10.1016/j.pmn.2019.04.006
16. Rogger R, Bello C, Romero CS, Urman RD, Luedi MM, Filipovic MG. Cultural framing and the impact on acute pain and pain services. Curr Pain Headache Rep. (2023) 27(9):429–36. doi: 10.1007/s11916-023-01125-2
17. Peacock S, Patel S. Cultural influences on pain. Rev Pain. (2008) 1(2):6–9. doi: 10.1177/204946370800100203
18. Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, et al. The revised international association for the study of pain definition of pain: concepts, challenges, and compromises. Pain. (2020) 161(9):1976–82. doi: 10.1097/j.pain.0000000000001939
19. Sladden T, Philpott A, Braeken D, Castellanos-Usigli A, Yadav V, Christie E, et al. Sexual health and wellbeing through the life course: ensuring sexual health, rights and pleasure for all. Int J Sex Health. (2021) 33(4):565–71. doi: 10.1080/19317611.2021.1991071
20. Saini R, Saini S, Sharma S. Oral sex, oral health and orogenital infections. J Glob Infect Dis. (2010) 2(1):57–62. doi: 10.4103/0974-777X.59252
21. Pakpahan C, Darmadi D, Agustinus A, Rezano A. Framing and understanding the whole aspect of oral sex from social and health perspectives: a narrative review. F1000Res. (2022) 11:177. doi: 10.12688/f1000research.108675.3
22. Liu H, Shen S, Hsieh N. A national dyadic study of oral sex, relationship quality, and well-being among older couples. J Gerontol B Psychol Sci Soc Sci. (2019) 74(2):298–308. doi: 10.1093/geronb/gby089
23. Wong ML, Chan RK, Koh D, Wee S. Factors associated with condom use for oral sex among female brothel-based sex workers in Singapore. Sex Transm Dis. (2000) 27(1):39–45. doi: 10.1097/00007435-200001000-00008
24. Malacad BL, Hess GC. Oral sex: behaviours and feelings of Canadian young women and implications for sex education. Eur J Contracept Reprod Health Care. (2010) 15(3):177–85. doi: 10.3109/13625181003797298
25. De Rosa CJ, Ethier KA, Kim DH, Cumberland WG, Afifi AA, Kotlerman J, et al. Sexual intercourse and oral sex among public middle school students: prevalence and correlates. Perspect Sex Reprod Health. (2010 Sep) 42(3):197–205. doi: 10.1363/4219710
26. Dake JA, Price JH, Ward BL, Welch PJ. Midwestern rural adolescents’ oral sex experience. J Sch Health. (2011 Mar) 81(3):159–65. doi: 10.1111/j.1746-1561.2010.00575.x
27. Brown B, Blas MM, Cabral A, Carcamo C, Gravitt PE, Halsey N. Oral sex practices, oral human papillomavirus and correlations between oral and cervical human papillomavirus prevalence among female sex workers in Lima, Peru. Int J STD AIDS. (2011) 22(11):655–8. doi: 10.1258/ijsa.2011.010541
28. Copen CE, Chandra A, Martinez G. Prevalence and timing of oral sex with opposite-sex partners among females and males aged 15−24 years: United States, 2007−2010. Natl Health Stat Report. (2012) (56):1–14.
29. Cherie A, Berhane Y. Oral and anal sex practices among high school youth in Addis Ababa, Ethiopia. BMC Public Health. (2012) 12:5. doi: 10.1186/1471-2458-12-5
30. Ma Q, Pan X, Cai G, Yan J, Xu Y, Ono-Kihara M, et al. The characteristics of heterosexual STD clinic attendees who practice oral sex in Zhejiang province, China. PLoS One. (2013) 8(6):e67092. doi: 10.1371/journal.pone.0067092
31. Morhason-Bello IO, Kabakama S, Baisley K, Francis SC, Watson-Jones D. Reported oral and anal sex among adolescents and adults reporting heterosexual sex in Sub-Saharan Africa: a systematic review. Reprod Health. (2019) 16(1):48. doi: 10.1186/s12978-019-0722-9
32. Carlos S, López-Del Burgo C, Ndarabu A, Osorio A, Rico-Campà A, Reina G, et al. Heterosexual oral and anal sex in Kinshasa (D.R.Congo): data from OKAPI prospective cohort. PLoS One. (2019) 14(1):e0210398. doi: 10.1371/journal.pone.0210398
33. Wood NH, Ayo-Yusuf OA, Gugushe TS, Bogers JP. Tobacco use and oral sex practice among dental clinic attendees. PLoS One. (2019) 14(3):e0213729. doi: 10.1371/journal.pone.0213729
34. Robbins SJ, Dauda W, Kokogho A, Ndembi N, Mitchell A, Adebajo S, et al. Oral sex practices among men who have sex with men and transgender women at risk for and living with HIV in Nigeria. PLoS One. (2020) 15(9):e0238745. doi: 10.1371/journal.pone.0238745
35. Kerwin JT, Thornton RL, Foley SM. Prevalence of and factors associated with oral sex among rural and urban Malawian men. Int J Sex Health. (2014) 26(1):66–77. doi: 10.1080/19317611.2013.830671
36. D'Souza G, Cullen K, Bowie J, Thorpe R, Fakhry C. Differences in oral sexual behaviors by gender, age, and race explain observed differences in prevalence of oral human papillomavirus infection. PLoS One. (2014) 9(1):e86023. doi: 10.1371/journal.pone.0086023
37. Sovetkina E, Weiss M, Verplanken B, Hackett J. Perception of vulnerability in young females’ experiences of oral sex: findings from the focus group discussions. Cogent Psychology. (2017) 4(1). doi: 10.1080/23311908.2017.1418643
38. CDC. Oral Sex and HIV Risk. Available at: https://www.cdc.gov/hiv/pdf/risk/cdc-hiv-oral-sex-fact-sheet.pdf (Accessed 7 November 2024).
39. Martín-Hernán F, Sánchez-Hernández JG, Cano J, Campo J, del Romero J. Oral cancer, HPV infection and evidence of sexual transmission. Med Oral Patol Oral Cir Bucal. (2013) 18(3):e439–44. doi: 10.4317/medoral.18419
40. Richters J, Clayton S. The practical and symbolic purpose of dental dams in lesbian safer sex promotion. Sex Health. (2010) 7(2):103. doi: 10.1071/SH09073
41. Fiveable. Intro to ethnic studies review: key term—erasure. (2025). Available at: https://fiveable.me/key-terms/introduction-to-ethnic-studies/erasure (Accessed 26 March 2025).
Keywords: sexual behavior, psychosocial factors, self-concept, health equity, health policy, health disparities, sexual and gender minorities, quality of life
Citation: Foláyan MO, Ndembi N, Abodunrin OR and Haire B (2025) Redefine oral health: a call for inclusivity in the concept of oral health. Front. Oral Health 6:1543770. doi: 10.3389/froh.2025.1543770
Received: 11 December 2024; Accepted: 14 April 2025;
Published: 7 May 2025.
Edited by:
Praveen S. Jodalli, Manipal College of Dental Sciences, IndiaReviewed by:
Tania Romo-Gonzalez, Universidad Veracruzana, MexicoAntonia Barranca-Enríquez, Universidad Veracruzana, Mexico
Copyright: © 2025 Foláyan, Ndembi, Abodunrin and Haire. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Moréniké Oluwátóyìn Foláyan, dG95aW51a3BvbmdAeWFob28uY28udWs=