 Prashanti Eachempati
Prashanti Eachempati John Martin
John Martin Sally Hanks4
Sally Hanks4 Mona Nasser
Mona Nasser- 1Peninsula Dental School, University of Plymouth, Plymouth, United Kingdom
- 2Faculty of Dentistry, Manipal University College Malaysia, Melaka, Malaysia
- 3School of Geography, Earth and Environmental Sciences, University of Plymouth, Plymouth, United Kingdom
- 4Faculty of Health, University of Plymouth, Plymouth, United Kingdom
This case study explores the adaptation of the walking method coupled with auto-photography and photo elicitation, a participatory research tool traditionally used in landscape studies, for application in dental research settings. By presenting the UniCDent toolkit, we demonstrate how this immersive method can enhance understanding of patient experiences in dentistry through sensory engagement and spatial exploration. The toolkit comprises four components: Imagery, Gallery Walk, Quadrant Mapping, and Trade-offs, each designed to facilitate active participation and foster in-depth reflections on the dental environment. Participants navigate a simulated dental clinic, documenting their sensory experiences and social interactions, thereby enriching the data collected. This multi-layered approach allows researchers to capture the complexities of patient experiences, providing insights that are applicable across various research projects within dentistry. The commentary highlights the versatility of the walking method, emphasising its role in improving patient-centred care by capturing patient experiences and perspectives. It also demonstrates its value in enhancing the understanding of diverse research enquiries in dental research.
Introduction
Walking methods are well-established in participatory research. They are commonly utilised in landscape place-based research, allowing participants to engage with their environments through sensory exploration. Walking method encompasses different types, such as exploratory walks (1) walking interviews (2), and transect walks (3) each designed to deepen understanding of the space and its inhabitants (4–7). While predominantly used in outdoor settings—like neighbourhoods and public spaces—these methods have also been applied in indoor environments, including grocery stores and schools (8, 9). Notably, this method has recently found its way into health research, offering valuable insights into the relationship between individuals and their healthcare environments (10). The walking method can be used alongside other participatory approaches, such as auto-photography and photo elicitation, where individuals capture images to reflect their experiences.
However, its application in dentistry remains unexplored, presenting an opportunity for innovation in understanding patient experiences. This article seeks to present a case study on adapting this method to provide an innovative approach to participatory research in dentistry, recognising the significance of spatial factors in shaping patient perceptions within the dental environment. In this case study, we explored how participants experienced and navigated the dental environment using the walking method coupled with auto-photography and photo elicitation. Within the different participatory approaches, the walking method aligns with the Exploration and Visioning domain while also intersecting with Engagement and Capacity Building (11). Auto-photography and photo elicitation fit into the Visual and Narrative domains (12).
In participatory research, the “walking method” immerses participants in a setting to engage their senses and explore firsthand experiences (13, 14). We tailored this method specifically for a dental clinic to address a range of research questions. We demonstrate this method in the context of a specific case study which aims to explore what patients perceive as uncertainty in the dental environment and how they respond to the uncertainty. Instead of relying on traditional interview techniques detached from the environment, the participants journeyed in a simulated dental clinic, allowing them to engage with the setting through their senses—sight, sound, smell, and touch—while also observing the social dynamics between patients and the dental team. This multi-layered approach enhanced participant engagement by anchoring their experiences in the real-world environment, offering richer, more nuanced insights into their interactions and perceptions.
While we used this method to explore uncertainty in the dental clinic, its value lies in its versatility. It can be adapted to a broad range of participatory research initiatives within clinical and other applied settings. By enabling participants to interact directly with their environment, the walking method facilitates a deeper understanding of context-specific phenomena, making it a powerful tool for exploring diverse research questions.
The toolkit
The UniCDent toolkit, which stands for “Uncertainty in Clinical Dentistry” toolkit, was developed taking inspiration from cult rural tool kit (15). It comprises of four tools that can be used independently or in conjunction with one another, as demonstrated in our participatory research approach. For ease of explaining how the toolkit works or can be applied in practice, we take the specific example of a case study exploring uncertainty in clinical dentistry. This case study was conducted in a multiethno-linguistic population of Malaysia. The study included 12 participants from each ethnic group: Malay, Indian, and Chinese. Maximum variation sampling was used to ensure that each group included individuals with differing levels of uncertainty tolerance.
Tool one. Imagery: the walking method and auto-photography
The “Imagery” step was central to immersing participants in the dental environment. In this phase, participants journeyed through a simulated dental setup, engaging their senses of sight, smell, touch, and hearing. As they navigated different areas within the clinic, they were encouraged to observe and photograph elements that triggered feelings of uncertainty (Figure 1). They documented not just the visual aspects but also other characteristics of the environment through writing, enhancing their sensory engagement. They were encouraged to select objects and place them in their tote bags as needed to illustrate what triggers uncertainty for them.
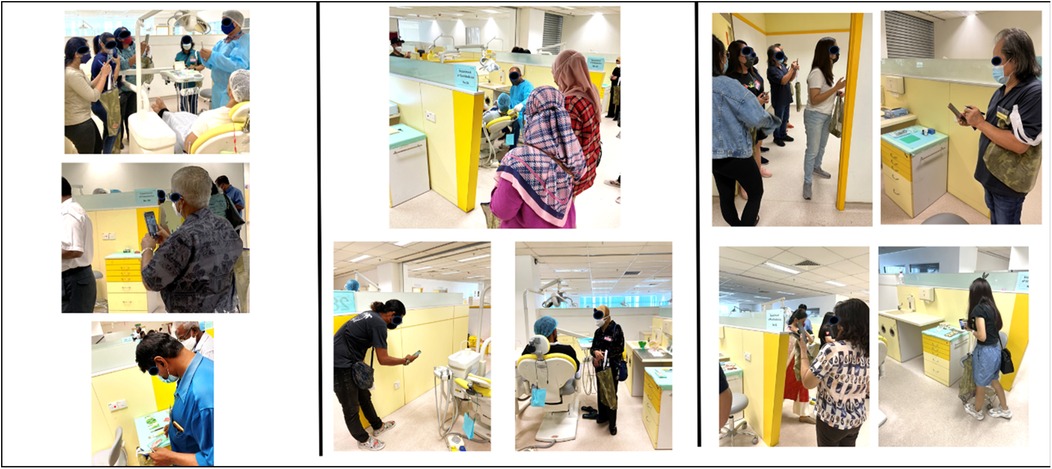
Figure 1. Imagery: participants navigating the dental clinic using auto-photography.
This method offered a more immersive and dynamic way of exploring uncertainty compared to traditional interviews that isolate participants from the environment in which their uncertainty arises. By being part of the dental environment, participants could better articulate the specific triggers that evoke uncertainty, giving us a deeper understanding of how these factors interact in a real-world setting.
Tool two. Gallery walk: exploring photographic interpretations using photo elicitation
Following the sensory journey, participants engaged in a “Gallery Walk”, where they printed and shared the photographs taken during the tour (Figure 2). This phase explored the subjective meanings participants attributed to their images, offering insight into how specific sights, sounds, or objects contributed to their feelings of uncertainty. The open discussion that followed fostered a collective exploration of these interpretations, as each participant guided the group through their thought process.

Figure 2. Gallery walk: participants explaining the uncertainty perceived using photo elicitation method.
Through this activity, we grasped the dynamic and multifaceted nature of uncertainty (16). It became clear that uncertainty is not triggered by isolated factors but by multiple, interacting layers of sensory stimuli and social dynamics. For example, participants noted how the sound of dental burs being used in the handpiece, the smell of dental materials, and the sight of being in a vulnerable position in the dental chair could intensify feelings of anxiety. These sensory elements, coupled with a non-empathetic dentist or an unwelcoming receptionist, further compounded uncertainty, leading participants to question whether they wanted to proceed with treatment, or leave.
This element of the exercise illuminated the significant opportunity to uncover the emotional and psychological complexities that arise in a dental environment. It could be applied to a wide range of research questions, revealing how various elements within a clinical setting influence patient comfort and decision-making. This method enabled us to capture this complexity and provided a platform for patients to articulate how these sensory and social experiences affect their willingness to continue treatment, thus offering deeper insights into the factors that contribute to uncertainty within a dental context.
Tool three. Quadrant mapping: categorising uncertainty
In the “Quadrant Mapping” step, a grid with four quadrants was created (Figure 3), where one axis represented the level of uncertainty (High/Low) and the other indicated the impact on decision-making (High Impact/Low Impact). This framework resulted in four quadrants, each representing different combinations: High Uncertainty/Low Impact, High Uncertainty/High Impact, Low Uncertainty/Low Impact, and Low Uncertainty/High Impact. Participants categorised the images and objects they had captured using this grid, based on the level of uncertainty and its perceived impact on their decision-making (Figure 4).
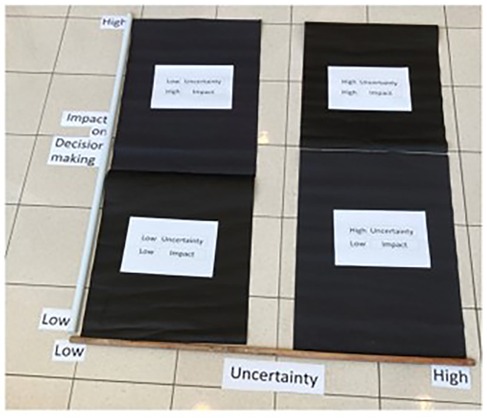
Figure 3. Grid for quadrant mapping.

Figure 4. Quadrant mapping: uncertainty classified based on the impact on decision making.
While this structured approach provided clarity on how patients prioritise and weigh their uncertainty in the context of clinical dentistry, it is by no means limited to this application. The framework is flexible and can be customised to suit different research questions and settings, with grid labels adjusted according to the specific focus of interest. What we present here is a case study example to demonstrate its potential, but the quadrant mapping technique can be tailored to suit various participatory research initiatives, allowing for insights specific to the context being studied.
Tool four. Trade-offs: decision-making when confronted with uncertainty
The final step, “Trade-offs”, explored the factors that influence changes in decision-making when patients experience uncertainty. Participants identified the top three reasons that might prompt them to alter their decisions in a dental setting, particularly in the face of uncertainty. To facilitate this process, participants were given flashcards that listed multiple factors that could influence their decision-making. Empty cards were also provided for them to write in any additional factors they thought of that were not already included in the list (Figure 5). Each participant was instructed to select and rank three flashcards as 1, 2, and 3. Once this ranking was completed, participants were asked to explain their choices.

Figure 5. Trade-offs: patients identifying trade-offs when confronted with uncertainty.
This exercise revealed the trade-offs patients are willing to make when confronted with uncertainty in clinical decision making. It provided valuable insights into how patients rationalise and navigate their choices when confronted with uncertainty. It highlighted the importance of understanding patients' willingness to compromise and the factors influencing their decisions, as well as how uncertainty shapes their overall dental experience.
Once again, this step can be customised based on the specific research question, as every choice or decision that a patient makes is inherently surrounded by trade-offs. Identifying these trade-offs would be relevant to a variety of research inquiries.
Insights from this immersive experiment using UniCDent
By adapting the walking method from landscape research (17) to the dental clinic setting, we have developed an immersive participatory tool that extends beyond the study of uncertainty and can be applied to a wide range of research questions.
In our research, the principles of the walking method were applied to explore participants' interactions with the clinical environment (18).
Place referred to how walking through specific locations, such as a dental clinic, activated relationships between participants, the environment, and the sensory elements of that space. As participants moved through the space, they were able to observe the roles of patients, clinicians, and staff, gaining valuable insights into the clinical environment.
Sensory Inquiry emphasised the role of the senses in engaging with the environment. In the context of the dental clinic, participants were absorbed in the setting through the sounds of drills, the smells of materials, and the tactile sensations of instruments. This sensory engagement offered a deeper understanding of how these elements influenced patient decision-making and clinical interactions.
Embodiment highlighted the importance of physically moving through the space to uncover lived experiences. By walking through the clinic, participants not only observed but also felt and experienced the environment, allowing us to understand how they perceived and responded to their surroundings.
Rhythm reflected the pace of activities within the clinical setting. The rhythm fluctuated depending on patient flow, the nature of procedures, and interactions happening in the clinical environment. This variability provided insights into how the pace of the clinic impacted participants' experiences and interactions.
Auto-photography further empowered participants by allowing them to document aspects of their environment that held personal meaning. Rooted in self-perception (19), this method enabled participants to represent their realities freely, without being constrained by researcher-led frameworks. Photo elicitation added another layer to this inquiry. Photographs taken by participants served as prompts for dialogue, enabling me to explore the meanings, emotions, and memories they associated with their images.
Potential challenges of the walking method and mitigation strategies
Although some authors have noted that the walking method can be lengthy and pose practical and ethical concerns (4), we did not encounter these challenges in our study. We ensured that the method was structured efficiently, balancing engagement with time considerations while maintaining participant comfort. Additionally, some argue that sensitive discussions during the walking method could lead to misunderstandings among participants, potentially affecting data quality (20). However, we minimised power imbalances by employing facilitators from the same ethnic groups to conduct workshops in their mother tongues and by aligning our approach with Hofstede's Cultural Dimensions Theory (21). This helped ensure cultural sensitivity, foster inclusivity, and enhance participant engagement.
Conclusion
While we demonstrated the tool's application for a specific case study, the UniCDent toolkit is versatile and can be customised for various research inquiries that have a spatial dimension to it. By incorporating these immersive techniques, researchers can develop patient-centred care strategies and explore diverse dimensions of clinical environments. This participatory method has allowed us to navigate the complexities of patient experiences, offering valuable insights that can enhance outcomes and advance dental research across various contexts. Indeed, this participatory method with legs has allowed us to walk into the complexities of patient experiences, paving the way for improved outcomes and greater understanding in any healthcare setting.
Data availability statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethics statement
This study has been approved by Research and Ethics board, University of Plymouth, and Institutional ethics committee, Manipal University College, Melaka, Malaysia. This study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
PE: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. JM: Methodology, Supervision, Writing – review & editing. SH: Supervision, Validation, Writing – review & editing. MN: Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. Generative AI, specifically ChatGPT, was utilized solely for grammar checks and sentence structure corrections. No assistance was sought or provided for content creation or intellectual input related to the substance of the document.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Bazuń D, Kwiatkowski M. Exploratory walk and local cohesion—the concept and application. Mobilities. (2021) 17(4):565–84. doi: 10.1080/17450101.2021.1999775
2. Butler M, Derrett S. The walking interview: an ethnographic approach to understanding disability. Internet J Allied Health Sci Pract. (2014) 12(3):6. doi: 10.46743/1540-580X/2014.1491
3. Rojas A, Nomedji K, West CT. Walking the line: conducting transect walks in Burkina Faso. Pract Anthropol. (2021) 43(1):18–21. doi: 10.17730/0888-4552.43.1.18
4. Carpiano RM. Come take a walk with me: the “go-along” interview as a novel method for studying the implications of place for health and well-being. Health Place. (2009) 15(1):263–72. doi: 10.1016/j.healthplace.2008.05.003
5. Clark A, Emmel N. Using walking interviews. ESRC National Centre for Research Methods (2010). Available at: http://hummedia.manchester.ac.uk/schools/soss/morgancentre/toolkits/13-toolkit-walking-interviews.pdf (Accessed November 11, 2024).
6. Evans J, Jones P. The walking interview: methodology, mobility and place. Appl Geogr. (2011) 31(2):849–58. doi: 10.1016/j.apgeog.2010.09.005
7. Holton M, Riley M. Talking on the move: place-based interviewing with undergraduate students. Area. (2014) 46(1):59–65. doi: 10.1111/area.12070
8. Thompson C, Cummins S, Brown T, Kyle R. Understanding interactions with the food environment: an exploration of supermarket food shopping routines in deprived neighbourhoods. Health Place. (2013) 19(1):116–23. doi: 10.1016/j.healthplace.2012.10.003
9. Garcia CM, Eisenberg ME, Frerich EA, Lechner KE, Lust K. Conducting go-along interviews to understand context and promote health. Qual Health Res. (2012) 22(10):1395–403. doi: 10.1177/1049732312452936
10. Marcotte J, Grandisson M, Milot É, Dupéré S. The walking interview: a promising method for promoting the participation of autistic people in research projects. Int J Qual Methods. (2022) 21:1–12. doi: 10.1177/16094069221090065
11. Duea SR, Zimmerman EB, Vaughn LM, Dias S, Harris J. A guide to selecting participatory research methods based on project and partnership goals. J Particip Res Methods. (2022) 3(1). doi: 10.35844/001c.32605
12. Vaughn LM, Jacquez F. Participatory research methods—choice points in the research process. J Particip Res Methods. (2020) 1(1). doi: 10.35844/001c.13244
13. Lenette C. Health on the move: walking interviews in health and wellbeing research. In: Marsden C, Wills J, editors. Creative Approaches to Health Education. London: Routledge (2021). p. 136–59.
14. Lenette C, Gardner J. Short take: walking interviews with refugee-background women. Field Methods. (2021) 33(3):305–12. doi: 10.1177/1525822X20987331
15. Martin J, Williamson D, Łucznik K, Guy JA. Development of the my cult-rural toolkit. Sustainability. (2021) 13(7):7128. doi: 10.3390/su13137128
16. Eachempati P, Büchter RB, Ks KK, Hanks S, Martin J, Nasser M. Developing an integrated multilevel model of uncertainty in health care: a qualitative systematic review and thematic synthesis. BMJ Glob Health. (2022) 7(5):e008113. doi: 10.1136/bmjgh-2021-008113
17. Macpherson H. Walking methods in landscape research: moving bodies, spaces of disclosure and rapport. Landsc Res. (2016) 41(4):425–32. doi: 10.1080/01426397.2016.1156065
18. Springgay S, Truman S. Walking Methodologies in a More-than-human World. London: Routledge (2018).
19. Glaw X, Inder K, Kable A, Hazelton M. Visual methodologies in qualitative research: autophotography and photo elicitation applied to mental health research. Int J Qual Methods. (2017) 16:1–8. doi: 10.1177/1609406917748215
20. Kanyamuna V, Zulu K. Participatory research methods: importance and limitations of participation in development practice. World J Soc Sci Humanit. (2022) 8(1):9–13. Available at: https://pubs.sciepub.com/wjssh/8/1/2/
Keywords: walking method, participatory research, dental environment, patient perceptions, community or stakeholder engagement
Citation: Eachempati P, Martin J, Hanks S and Nasser M (2025) Walking in a dental environment with the “UniCDent” tool kit—part 1: a participatory tool with legs!. Front. Oral Health 6:1545170. doi: 10.3389/froh.2025.1545170
Received: 18 December 2024; Accepted: 6 May 2025;
Published: 23 May 2025.
Edited by:
Lucas Arrais de Campos, Tampere University, FinlandReviewed by:
Irfan Adil Majid, Ibn Sina National College for Medical Studies, Saudi ArabiaOana Almasan, University of Medicine and Pharmacy Iuliu Hatieganu, Romania
Copyright: © 2025 Eachempati, Martin, Hanks and Nasser. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Prashanti Eachempati, cHJhc2hhbnRpLmVhY2hlbXBhdGlAcGx5bW91dGguYWMudWs=