 Moréniké Oluwátóyìn Foláyan1,2
Moréniké Oluwátóyìn Foláyan1,2 Adeyinka Ganiyat Ishola3
Adeyinka Ganiyat Ishola3 Olunike Rebecca Abodunrin4
Olunike Rebecca Abodunrin4 Nicaise Ndembi5,6
Nicaise Ndembi5,6 Maha El Tantawi1,7*
Maha El Tantawi1,7*
- 1The Africa Oral Health Network (AFRONE), Alexandria University, Alexandria, Egypt
- 2Department of Child Dental Health, Obafemi Awolowo University, Ile Ife, Nigeria
- 3Department of Nursing, University of Ibadan, Ibadan, Nigeria
- 4Department of Epidemiology and Biostatistics, Nanjing Medical University, Jiangsu, China
- 5Director General's Office, International Vaccine Institute (IVI), Africa Regional Office, Kigali, Rwanda
- 6Division of Epidemiology and Prevention, Institute of Human Virology, University of Maryland School of Medicine, Baltimore, MD, United States
- 7Department of Pediatric Dentistry and Dental Public Health, Alexandria University, Alexandria, Egypt
Early Childhood Caries (ECC) is a significant oral health condition that impacts children globally. This manuscript's main objective is to explore ECC's impact on children's oral health-related quality of life (OHRQoL) in Africa, and to highlight the policy and programme recommendations to eliminate untreated ECC as a public health threat in Africa. In Africa, ECC poses a significant public health challenge and has the potential to result in functional disabilities in children. A rapid review of the literature focusing on studies from Africa explored the impact of ECC on children's oral health-related quality of life. The three studies that met the eligibility criteria revealed that ECC negatively impacts multiple dimensions of life, including physical health (pain, malnutrition, chewing difficulties), psychological well-being (low self-esteem, stigma), and social functioning (peer relationships, school attendance). Advanced ECC had more pronounced effects, particularly in the symptom and psychological domains. The paper highlights the urgent need to recognise untreated ECC as a disability within public health frameworks in Africa. Policy recommendations include integrating oral health into primary healthcare systems, expanding community-based prevention programmes, incentivising the production of affordable oral health products, and developing school-based education initiatives. Strengthening oral health workforce capacity and enhancing data collection on ECC prevalence is critical for effective policy formulation and resource allocation. Recognising ECC as a potential disability underscores the need for a multi-sectoral approach to address this neglected public health priority and for prioritising actions to eliminate untreated ECC as the International Day of Persons with Disabilities (December 3) is marked.
Introduction
Early Childhood Caries (ECC) is a debilitating disease. It is defined as one or more decayed, missing (due to caries), or filled tooth surfaces in any primary tooth in a child aged 71 months or younger (1). It is also a widespread oral disease that affects infants, toddlers, and preschoolers. The global prevalence ranges from 46.2% (2) to 48% (3). The prevalence increases with age (4) from 17% in one-year-olds to 36%, 43%, 55%, and 63% for 2, 3, 4- and 5-year-olds, respectively (5). More than 530 million children worldwide have ECC, and most ECC cases remain untreated (6). Although the disease is decreasing globally, it is increasing in Africa (7).
ECC is a disability because it is a complex and multifaceted disease that encompasses physical, mental, and social impairments (8). Traditionally, disability has been associated with visible physical limitations or chronic illnesses. However, the World Health Organization (WHO) recognises that disability can also stem from impairments in various domains. Disability is defined as a “dynamic interaction between health conditions and contextual factors.” (8) This definition highlights that a person's health condition does not solely determine disability but is also influenced by social, environmental, and personal factors (8).
This untreated burden not only compromises oral health but also has far-reaching consequences on the physical, psychological, and social development of the child, particularly in low-resource settings like Africa. Against this backdrop, the main objective of this manuscript is to explore the impact of ECC on children's oral health-related quality of life (OHRQoL) in Africa and to highlight policy and programme recommendations aimed at eliminating untreated ECC as a public health threat across the continent.
Untreated early childhood caries and disability
Untreated ECC is associated with conditions that can cause disability. It can lead to infection, pain, abscesses (8), difficulty eating and chewing, malnutrition (9), and difficulty in sleeping (10, 11). The cumulative effect of untreated ECC on the health and well-being of the child impacts physical growth and psychological development (12). This results from the impaired masticatory function of the hippocampus, chronic inflammation, and sleep disturbances that negatively affect cognitive functioning (13). These gut microbiome disruptions due to frequent antibiotics and analgesics to treat ECC-related infections, and the elevated nutritional risk from untreated ECC, can undermine optimal brain and cognitive development in young children (13). Children with untreated ECC have higher risks of developing dental caries in adolescence (14).
Physical development in early childhood is vital for an individual's long-term health and functional ability. Poor physical development can hinder the development of essential motor skills and functional capacity, thereby increasing susceptibility to disability. Physical development encompasses gross and fine motor skills, essential for daily self-care (15). Children experiencing delays in motor skills may face challenges in mobility and coordination, limiting their ability to participate fully in age-appropriate activities (16). Poor physical development often results in increased vulnerability to infections, chronic illnesses (17), functional impairments, and developing disabilities later in life. Lack of early intervention in physical development can lead to irreversible health conditions and impairments that restrict physical independence (18, 19). These impairments may qualify as a disability when they prevent individuals from performing daily activities and meeting social expectations.
In addition, psychological development is integral to a child's ability to function and engage with their surroundings. For example, children with a positive self-image and healthy self-concept are likelier to take on challenges and persevere through difficulties (20). ECC, however, increases the risk of low self-esteem (21) and poor social interaction (12, 22). Social exclusion can also result from stigma (23). In addition, premature tooth loss caused by untreated ECC can impede speech clarity and fluency (8, 12, 24, 25), resulting in communication barriers that limit interaction with peers and engagement in educational activities, ultimately leading to social isolation (26).
Furthermore, poor psychological development poses significant risks for disability when cognitive development is compromised or communication, comprehension, and learning are affected. Cognitive impairments due to untreated ECC (27) can also negatively impact educational attainment and the development of adaptive skills, which are critical for independent living.
Children with ECC frequently report experiencing pain, difficulty with eating, and psychological distress, all of which disrupt their daily activities and overall well-being (28–30). The oral health-related disabilities resulting from ECC affect the OHRQoL and negatively impact an individual's physical, social, and psychological well-being (31). Untreated ECC consistently negatively impacts the OHRQoL of children and their families (32). The most significant impacts are observed in the symptom and psychological domains (32, 33). In addition, ECC predicts reduced OHRQoL as children age (28, 34).
Untreated early childhood caries and disability in children in Africa
The prevalence of ECC in Africa is high, estimated to be 30% (2), with wide variations among countries on the continent (35). The burden of untreated ECC is likely to increase in Africa largely due to population growth, increasing survival rates in early ages, and a high proportion of young populations (36). Whereas the population is expected to decrease somewhat until 2,100 in Asia, Europe, and South America, it is predicted to grow significantly in Africa (37).
There are high concerns about the high risk of functional disability from untreated ECC in Africa. This is related to social, environmental, and personal factors, including access to healthcare and poor supportive family and community environments. Access to oral healthcare facilities is notably limited by several barriers and challenges, including a shortage of trained oral health professionals on the continent (38), uneven distribution of healthcare resources with a concentration in urban areas (39), and limited public funding for oral health services (40). In addition, these issues exacerbate the low prioritisation of oral health in public health policies (41, 42) and poor access to and uptake of preventive dental care.
ECC is not only a dental health issue but also a social concern. It is linked to poverty (43, 44), lower socioeconomic status (45–47), living in low- and middle-income countries (48, 49), and living in poor households that cannot afford dental care, healthy foods, or oral hygiene products (50). Thus, ECC is a social justice issue (51), and the risk of ECC progressing to a disabling condition increases when families lack the resources, knowledge, or access to support systems.
The burden of ECC is also higher in communities where caregivers are not educated on prevention or access to services like fluoride treatment or affordable dental check-ups (52, 53) and in areas where dental care is less prioritised (54). There is limited focus on community programmes that improve access to oral care in Africa (55, 56). The risk factors associated with a higher risk of ECC are also associated with the risk of worse OHRQoL outcomes for ECC in Africa (57).
We conducted a rapid scoping review of the literature for studies on the associations between ECC and the OHRQoL of children in Africa. A search for relevant literature was conducted on the Web of Science, PubMed, and CINAHL databases. Studies were included if they included information about dental caries and OHRQoL, if the target group was children younger than 6 years of age, or if information about them could be extracted, and if they lived in the 54 African Union member states. Studies were included if they were cross-sectional, cohort, case-control, randomised controlled trials, quasi-experimental studies, systematic reviews, or policy analyses. Opinion pieces, editorials, studies lacking primary data on the association between ECC and OHRQoL, and studies not published in English were excluded.
Our search strategy incorporated the following terms: [“early childhood caries” OR ECC OR “dental caries” OR “dental decay” OR “dental cavity” OR “dental cavities” OR “tooth decay” OR (Infant AND “Dental Cavity”) OR (child* AND caries)] AND [“Oral health-related quality of life” OR OHRQL OR (“oral health” AND quality of life) OR (“dental health” AND quality of life) OR OHRQoL] AND Africa.
The review was conducted by two independent reviewers (AGI and ORA) with conflict resolution by a third reviewer (MOF). Rayyan was utilized to manage and screen articles. Standardized forms captured details on study location, study objective, study design, sample size, and study findings.
We identified 75 studies—PubMed (31), Web of Science (36), and CINALH (8)—of which 22 were excluded for duplication. Of the 53 titles/abstracts screened, 40 were excluded for reasons ranging from study participants were not children (21), to study location was outside the scope (8), and study did not report OHRQoL (11). Of the 13 articles sought, 10 were excluded for reasons ranging from the study not focused on Africa (2), to review articles (2), study focused on older ages (4), and ECC not reported (2). Three studies met the eligibility criteria.
The summary of the publications is highlighted in Table 1. The three studies were cross-sectional, conducted in East Africa, enrolled 1,723 children, and were conducted between 2013 and 2020. Like other studies, they indicated that untreated ECC affects multiple dimensions of life, including physical health (pain, discomfort, and dietary restrictions) (58), psychological well-being (stigma and self-esteem) (59), and social functioning (peer relationships and school attendance) (58, 59), in addition to family impacts (60). Although there are few studies, these regional findings may be generalisable to the rest of Africa because the risk factors for ECC and its non-treatment in East Africa are similar to those in most of the other regions of the continent (61), thereby supporting the applicability of these findings to a continental scale although contextual differences are acknowledged.
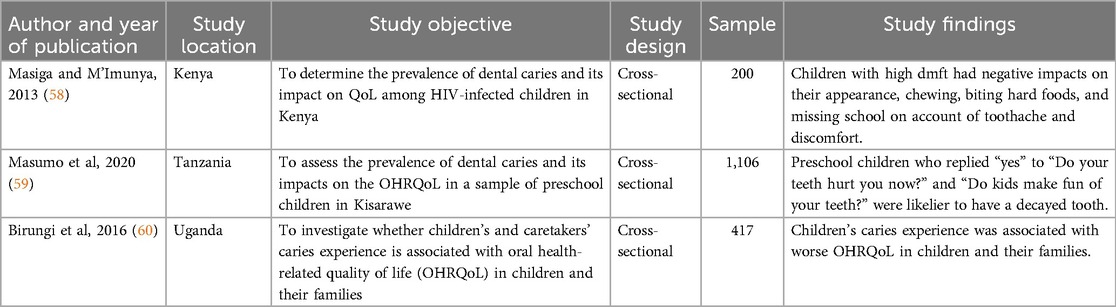
Table 1. Studies reporting on early childhood caries and oral health quality of life.
The findings of the rapid review indicate that children with high dmft experience significant challenges, including negative impacts on appearance, chewing difficulties, and school absenteeism due to toothache and discomfort. These limitations interfere with essential daily activities such as eating and learning (58), contributing to malnutrition, weight loss, and impaired physical development—hallmarks of functional disability (62). Dental pain further exacerbates nutritional deficiencies, potentially delaying both physical and cognitive growth (63), while missed school days hinder educational attainment, reinforcing long-term disadvantages (64). Beyond physical effects, untreated ECC leads to low self-esteem, social anxiety, and psychological distress (65). Visible decay, pain, and tooth loss from ECC can result in peer stigma and bullying (66) and isolation (67), negatively affecting mental health and social interactions. This aligns with the WHO's definition of disability, which includes impairments in social participation and psychological well-being (7).
In addition, ECC's negative impact on children and their families reflects the broader interaction between health conditions and environmental barriers, worsening OHRQoL. Chronic pain and malnutrition can disrupt sleep, impair cognitive function, and weaken immune responses, increasing susceptibility to illness (68). These cumulative effects restrict a child's ability to function and participate fully in society, reinforcing ECC's classification as a disabling condition.
Policy and programme implications to reduce the risk of disability from ECC in Africa
Policy development is a crucial function of public health to enhance population health (69). Health policies guide governments to desired health outcomes and outline the resources needed to achieve these outcomes (70). Recognising ECC as a potential disability for children in Africa calls for comprehensive health policy reform. Such reform includes expanding access to oral healthcare, enhancing public education and awareness, and increasing funding and resources for children's oral health programmes. Policy modifiable factors can address the inequity driving ECC (71). The policies should use a multi-sectoral approach by embedding oral health into existing healthcare and community systems and creating supportive environments to address systemic barriers and enhance community engagement.
Integrate Oral Health into Primary Healthcare Systems: The call to integrate oral health into primary healthcare (PHC) was made in the 1,978 Declaration of Alma-Ata, which emphasised the importance of PHC in achieving “Health for All.” (72). The declaration underscored the need for accessible, community-based preventive and curative services. Since then, the integration is still an important healthcare pathway (73).
In many parts of Africa, PHC is often the first—and sometimes only—point of contact for healthcare (74), making it an effective approach to address ECC. This entails the inclusion of basic oral health screenings in routine pediatric visits at PHC centres, establishing guidelines for ECC risk assessment and preventive counselling, and fluoride application. It also requires training PHC personnel, including community health workers, to detect ECC, educate parents on preventive practices, and apply simple and effective interventions, such as fluoride varnish.
The concept of PHC, however, has to expand beyond Western orthodox practices because child care often occurs through diverse, culturally rooted pathways (75). Traditional healers, family networks, and community leaders play significant roles in children's health in many African communities. Expanding PHC to embrace these local systems can enhance access to child oral health services, promote preventive practices, improve outcomes, reach underserved populations, and increase healthcare utilisation, thus providing a comprehensive care model for ECC.
Expand community-based oral health programmes
Community-based programmes help reach populations with limited access to formal dental services. These programmes leverage community members to promote oral health awareness, prevention, and early intervention. It is important to support the development of community health programmes dedicated to ECC prevention by establishing partnerships with local NGOs, religious institutions, and schools. Mobile dental clinics can also provide preventive and basic curative services by visiting remote areas and offering screenings, fluoride treatments, and referrals.
Most community-based health programmes are in South Asian and Sub-Saharan African countries (76) and are run by community health workers (CHWs). However, there is scarce evidence about using CHWs for oral health programmes (77). Evidence is needed on the effectiveness and cost-effectiveness of engaging CHWs in implementing oral health programmes in rural and underserved African areas with a workforce shortage to deliver oral health care.
Local production and distribution of affordable oral health products
Access to affordable toothbrushes, fluoride toothpaste, and other oral hygiene products remains limited in many African countries. The affordability and availability of oral health products may be improved by policies that promote local production through tax breaks and subsidies for local manufacturers, public-private partnerships, and the use of corporate social responsibility for communities that host the business.
The African Union (AU) and Africa Centres for Disease Control and Prevention (Africa CDC) have rightly prioritised the local production of vaccines and therapies to bolster continental resilience in times of health crises, where rapid access to treatments and vaccines can save lives (78). However, this prioritisation often overlooks non-crisis health issues like oral health, which, although not immediately life-threatening, lead to long-term disability, economic burdens, and reduced quality of life across the continent. The absence of local production of oral hygiene products perpetuates disparities, as many communities face limited access to basic dental care, which has implications for overall health (79). Failing to address oral health thus represents a missed opportunity for holistic disease prevention across Africa, limiting progress towards comprehensive public health. Policies should support the local production of essential oral health products to reduce the prevalence of ECC and other oral diseases and enhance overall health equity across Africa.
Implement school-based oral health education and preventive programmes
Schools provide a powerful platform for reaching young children by fostering early positive habits (80). Developing national oral health programmes focusing on daily oral hygiene, healthy eating, ECC risk assessment, and prevention can reduce ECC prevalence (81). In addition, establishing regular dental screenings in schools, especially for early childhood, like the “Toothbrushing with Fluoride” programme in Thailand (82), can make a difference. This programme provided fluoride toothpaste and toothbrushes for children to use at school daily, reinforcing healthy habits and reducing decay rates over time.
School-based oral health education and preventive programmes in Africa would, however, face challenges due to insufficient funding, shortage of skilled workforce, limited parental involvement (83), poor oral health literacy, and priority given to the primary dentition (84) and the large number of preschool children who are not in school. Currently, 19.7% of children in Africa are not attending school, and 30% of the 250 million out-of-school children globally are in Sub-Saharan Africa (85). Addressing these factors using a multi-sectoral approach to community development would enable the implementation of these programmes.
Develop public awareness campaigns
Awareness of ECC and its impact is limited in many African communities. Public campaigns can increase awareness, shift social norms about oral health, and motivate families to seek early care. Mass media, including radio, television, and social media, can reach a broad audience. However, the messages must be tailored to local cultural beliefs and practices around oral health.
Strengthen oral health workforce capacity
Addressing ECC requires increasing the number and distribution of trained oral health professionals across the continent. Currently, most countries in the WHO African Region do not have enough oral health workforce to address their population's oral health needs, and they will still not have enough by 2030. Task shifting and training other healthcare professionals to provide oral health and ECC-specific services can help address this shortage (86). This includes general health practitioners, paediatricians, nurses, and mid-level providers. By empowering a broader range of healthcare providers with ECC prevention and management skills, early intervention and preventative care at the community level may be possible, especially in underserved and remote areas where dentists are scarce.
Utilise data to inform policies and programmes
Data on ECC prevalence, risk factors, and impact across Africa is limited. Expanding surveillance systems and conducting regular oral health assessments can inform targeted interventions and help allocate resources where they are most needed. Few African countries, like Egypt, Namibia, and South Africa, have been reported to have collected routine surveillance data on ECC (87). Monitoring ECC requires funding research to understand ECC trends and establishing a national ECC registry to monitor intervention responsiveness. Routine ECC surveillance can also be integrated into global surveys such as the Demographic Health Survey, conducted every four to five years in over 45 African countries (88). The data can help policymakers identify high-risk populations and create tailored programmes to address specific needs.
Advocate for ECC inclusion in universal health coverage
In many low- and middle-income countries, oral health services are excluded from universal health coverage (UHC) (89). Advocating for ECC treatment and prevention under UHC would expand access for all, regardless of income, and reduce the economic burden on families. An ecological study, however, suggested that the impact of health expenditure on the prevalence of global ECC was stronger than that of UHC coverage (90). The study suggests that while UHC may provide access to services, the expected reduction in ECC prevalence may not happen if the quality of dental care or preventive services is inadequate, as access does not guarantee effective care. African governments must enhance the quality of dental services within the UHC frameworks and invest in preventive care and dental health education as part of public health initiatives by allocating resources to improve health systems.
Table 2 summarises the key policies and programmes aimed at integrating ECC prevention into the broader healthcare systems. It includes details on possible sources of financial support for the initiatives, including expectations from governments, international organizations, non-governmental organizations, and private sector partnerships. Implementing these policies and programmes is expected to increase early detection of ECC, improve access to oral health services, improve hygiene practices, and reduce ECC prevalence. Challenges to implementing these proposed programmes range from infrastructure limitations and workforce shortages to funding constraints and cultural resistance.
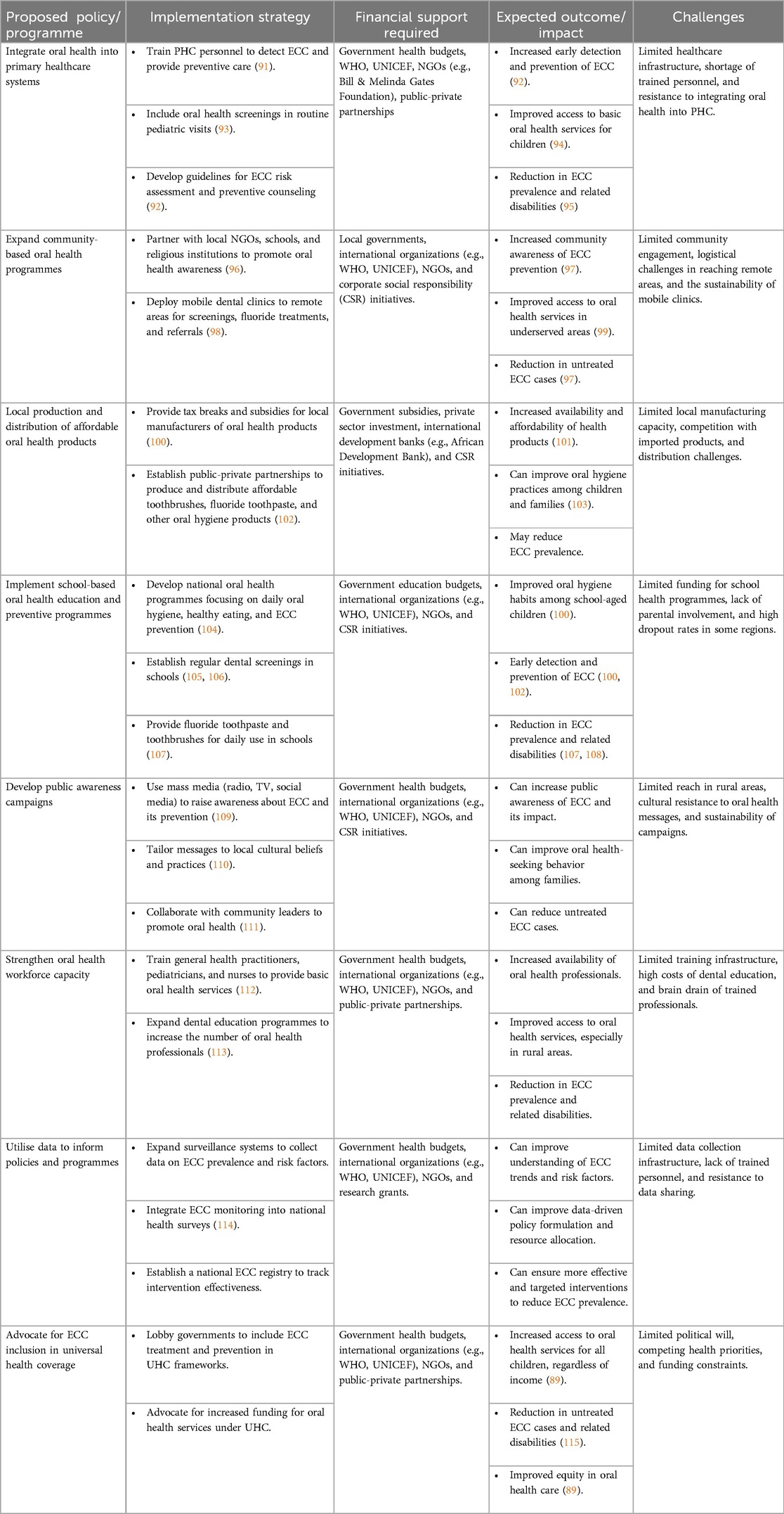
Table 2. Key policies and programmes for integrating ECC prevention into the broader healthcare systems.
The recognition of untreated ECC as a disability provides an opportunity to leverage events like the International Day of Persons with Disabilities on December 3 to raise awareness, drive advocacy, and promote actionable interventions to eliminate untreated ECC (116–118). Framing ECC as a disabling condition highlights its profound impact on children's physical, psychological, and social well-being and positions it as a public health and social justice issue.
Conclusion
Untreated ECC is a major public health and social justice issue in Africa, requiring urgent policy action to prevent its disabling consequences. It has an impact on the physical and psychological well-being of children in Africa, causing disability, and requiring urgent policy reforms. Successful country models demonstrate that integrating oral health into PHC, school-based programmes, and community outreach can significantly reduce ECC prevalence. Financial backing from governments, donors, partners, and private sector partnerships is critical to implementing these policies, including local production of affordable oral health products and workforce expansion. Strengthening data-driven policies through surveillance systems and advocating for ECC inclusion in the UHC can further ensure equitable access to care. By adopting these strategies, African nations can take decisive steps toward eliminating untreated ECC, improving children's well-being, and positioning oral health within broader health equity frameworks.
Author contributions
MF: Conceptualization, Data curation, Formal analysis, Writing – original draft, Writing – review & editing. AI: Data curation, Writing – review & editing. OA: Data curation, Writing – review & editing. NN: Funding acquisition, Writing – review & editing. ME: Formal analysis, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. IHVN is funding the publication of this paper. NN is supported by the US NIH/ NIAID R01 AI147331-04.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. Chat GPT was used to develop the outline for the manuscript and to edit the manuscript
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Drury TF, Horowitz AM, Ismail AI, Maertens MP, Rozier RG, Selwitz RH. Diagnosing and reporting early childhood caries for research purposes. A report of a workshop sponsored by the national institute of dental and craniofacial research, the health resources and services administration, and the health care financing administration. J Public Health Dent. (1999) 59(3):192–7. doi: 10.1111/j.1752-7325.1999.tb03268.x
2. Uribe SE, Innes N, Maldupa I. The global prevalence of early childhood caries: a systematic review with meta-analysis using the WHO diagnostic criteria. Int J Paediatr Dent. (2021) 31(6):817–30. doi: 10.1111/ipd.12783
3. Tinanoff N, Baez RJ, Diaz Guillory C, Donly KJ, Feldens CA, McGrath C, et al. Early childhood caries epidemiology, aetiology, risk assessment, societal burden, management, education, and policy: global perspective. Int J Paediatr Dent. (2019) 29(3):238–48. doi: 10.1111/ipd.12484
4. Kazeminia M, Abdi A, Shohaimi S, Jalali R, Vaisi-Raygani A, Salari N, et al. Dental caries in primary and permanent teeth in children’s worldwide, 1995 to 2019: a systematic review and meta-analysis. Head Face Med. (2020) 16(1):22. doi: 10.1186/s13005-020-00237-z
5. James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. (2018) 392:1789–858. doi: 10.1016/S0140-6736(18)32279-7
6. World Health Organization. World Report on Disability (2011). Available at: https://www.who.int/teams/noncommunicable-diseases/sensory-functions-disability-and-rehabilitation/world-report-on-disability (Accessed December 5, 2024).
7. GBD 2021 Oral Disorders Collaborators. Trends in the global, regional, and national burden of oral conditions from 1990 to 2021: a systematic analysis for the global burden of disease study 2021. Lancet. (2025) 405(10482):897–910. doi: 10.1016/S0140-6736(24)02811-3
8. Finlayson TL, Siefert K, Ismail AI, Sohn W. Psychosocial factors and early childhood caries among low-income African-American children in Detroit. Community Dent Oral Epidemiol. (2007) 35(6):439–48. doi: 10.1111/j.1600-0528.2006.00352.x
9. So M, Ellenikiotis YA, Husby HM, Paz CL, Seymour B, Sokal-Gutierrez K. Early childhood dental caries, mouth pain, and malnutrition in the Ecuadorian Amazon region. Int J Environ Res Public Health. (2017) 14(5):550. doi: 10.3390/ijerph14050550
10. Colak H, Dülgergil CT, Dalli M, Hamidi MM. Early childhood caries update: a review of causes, diagnoses, and treatments. J Nat Sci Biol Med. (2013) 4:29–38. doi: 10.4103/0976-9668.107257
11. Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. (2013) 14:1539–52. doi: 10.1016/j.jpain.2013.08.007
12. Sheiham A. Dental caries affects body weight, growth, and quality of life in preschool children. Br Dent J. (2006) 201:625–6. doi: 10.1038/sj.bdj.4814259
13. Foláyan MO, Femi-Akinlosotu OM, Adeoti B, Olorunmoteni OE. Untreated early childhood caries and possible links with brain development. BioMed. (2023) 3(4):431–9. doi: 10.3390/biomed3040035
14. Lam PPY, Chua H, Ekambaram M, Lo ECM, Yiu CKY. Does early childhood caries increase caries development among school children and adolescents? A systematic review and meta-analysis. Int J Environ Res Public Health. (2022) 19(20):13459. doi: 10.3390/ijerph192013459
15. Welsh Assembly Government. Physical Development. Available at: https://www.gov.wales/sites/default/files/publications/2018-02/physical-development.pdf?e=5305098/62475902 (Accessed December 5, 2024).
16. Waber DP, Bryce CP, Girard JM, Zichlin M, Fitzmaurice GM, Galler JR. Impaired IQ and academic skills in adults who experienced moderate to severe infantile malnutrition: a 40-year study. Nutr Neurosci. (2014) 17:58–64. doi: 10.1179/1476830513Y.0000000061
17. Gwela A, Mupere E, Berkley JA, Lancioni C. Undernutrition, host immunity and vulnerability to infection among young children. Pediatr Infect Dis J. (2019) 38(8):e175–7. doi: 10.1097/INF.0000000000002363
18. Galler JR, Bryce CP, Waber DP, Hock RS, Harrison R, Eaglesfield GD, et al. Infant malnutrition predicts conduct problems in adolescents. Nutr Neurosci. (2012) 15:186–92. doi: 10.1179/1476830512Y.0000000012
19. De Sanctis V, Soliman A, Alaaraj N, Ahmed S, Alyafei F, Hamed N. Early and long-term consequences of nutritional stunting: from childhood to adulthood. Acta Biomed. (2021) 92(1):e2021168. doi: 10.23750/abm.v92i1.11346
20. Bonyan Organization. Factors that Affect Children’s Psychosocial and Social Well-being. Available at: https://bonyan.ngo/child-protection/childrens-psychosocial-and-social-well-being/#:∼:text=Perception%20and%20Beliefs,opportunities%20for%20learning%20and%20growth (Accessed December 5, 2024).
21. Zafar S, Harnekar SY, Siddiqi A. Early childhood caries: etiology, clinical considerations, consequences, and management. Available at: https://www.moderndentistrymedia.com/july_aug2009/zafar.pdf (Accessed December 5 2024).
22. Peres MA, Macpherson LMD, Weyant RJ, Daly B, Venturelli R, Mathur MR, et al. Oral diseases: a global public health challenge. Lancet. (2019) 394(10194):249–60. doi: 10.1016/S0140-6736(19)31146-8
23. Tschammler C, Zimmermann D, Batschkus S, Wiegand A, Folta-Schoofs K. Perception of children with visible untreated and treated caries. J Dent. (2018) 74:37–42. doi: 10.1016/j.jdent.2018.05.006
24. Feitosa S, Colares V, Pinkham J. The psychosocial effects of severe caries in 4-year-old children in recife, pernambuco, Brazil. Cad Saude Publica. (2005) 21:1550–6. doi: 10.1590/S0102-311X2005000500028
25. Low W, Tan S, Schwartz S. The effect of severe caries on the quality of life in young children. Pediatr Dent. (1999) 21:325–6.10509332
26. Hitchcock ER, Harel D, Byun TM. Social, emotional, and academic impact of residual speech errors in school-aged children: a survey study. Semin Speech Lang. (2015) 36(4):283–94. doi: 10.1055/s-0035-1562911
27. Bramantoro T, Mardiyantoro F, Irmalia WR, Kristanti RA, Nugraha AP, Noor TEBTA, et al. Early childhood caries, masticatory function, child early cognitive, and psychomotor development: a narrative review. Eur J Dent. (2024) 18(2):441–7. doi: 10.1055/s-0043-1774326
28. Kragt L, van der Tas JT, Moll HA, Elfrink ME, Jaddoe VW, Wolvius EB, et al. Early caries predicts low oral health-related quality of life at a later age. Caries Res. (2016) 50(5):471–9. doi: 10.1159/000448599
29. Kramer PF, Feldens CA, Ferreira SH, Bervian J, Rodrigues PH, Peres MA. Exploring the impact of oral diseases and disorders on quality of life of preschool children. Community Dent Oral Epidemiol. (2013) 41(4):327–35. doi: 10.1111/cdoe.12035
30. Mathew MG, Jeevanandan G, Maganur PC, Medabesh AA, Juraybi AKM, Abuzawah LHA, et al. Evaluation of factors influencing the oral health-related quality of life among children with early childhood caries: a cross-sectional study. J Contemp Dent Pract. (2022) 23(9):936–43. doi: 10.5005/jp-journals-10024-3405
31. Gift HC, Atchison KA. Oral health, health, and health-related quality of life. Med Care. (1995) 33(11 Suppl):NS57–77. doi: 10.1097/00005650-199511001-00008
32. Zaror C, Matamala-Santander A, Ferrer M, Rivera-Mendoza F, Espinoza-Espinoza G, Martínez-Zapata MJ. Impact of early childhood caries on oral health-related quality of life: a systematic review and meta-analysis. Int J Dent Hyg. (2022) 20(1):120–35. doi: 10.1111/idh.12494
33. Sischo L, Broder HL. Oral health-related quality of life: what, why, how, and future implications. J Dent Res. (2011) 90:1264–70. doi: 10.1177/0022034511399918
34. Benelli KDRG, Chaffee BW, Kramer PF, Knorst JK, Ardenghi TM, Feldens CA. Pattern of caries lesions and oral health-related quality of life throughout early childhood: a birth cohort study. Eur J Oral Sci. (2022) 130(5):e12889. doi: 10.1111/eos.12889
35. Folayan MO, Ramos-Gomez F, Sabbah W, El Tantawi M. Editorial: country profile of the epidemiology and clinical management of early childhood caries, volume II. Front. Public Health. (2023) 11:1201899. doi: 10.3389/fpubh.2023.1201899
36. Dyvik EH. World population by age and region 2023. (2024). Available at: https://www.statista.com/statistics/265759/world-population-by-age-and-region/ (Accessed November 5, 2024).
37. Dyvik EH. Forecast: world population, by continent 2100 (2024). Available at: https://www.statista.com/statistics/272789/world-population-by-continent/ (Accessed November 5, 2024).
38. Gallagher JE, Mattos Savage GC, Crummey SC, Sabbah W, Varenne B, Makino Y. Oral health workforce in Africa: a scarce resource. Int J Environ Res Public Health. (2023) 20(3):2328. doi: 10.3390/ijerph20032328
39. Ogunbodede EO, Kida IA, Madjapa HS, Amedari M, Ehizele A, Mutave R, et al. Oral health inequalities between rural and urban populations of the African and Middle East region. Adv Dent Res. (2015) 27(1):18–25. doi: 10.1177/0022034515575538
40. El Tantawi M, Folayan MO, Ayo-Yusuf O. Editorial: dentistry and oral health in Africa. Front Oral Health. (2023) 4:1160976. doi: 10.3389/froh.2023.1160976
41. World Health Organization. Global Oral Health status Report. Towards Universal Health Coverage for Oral Health by 2030: Regional Summary of the African Region. Geneva: World Health Organization. License: CC BY-NC-SA 3.0 IGO (2023). Available at: https://www.who.int/publications/i/item/978 (Accessed November 05, 2024).
42. Benzian H, Hobdell M, Holmgren C, Yee R, Monse B, Barnard JT, et al. Political priority of global oral health: an analysis of reasons for international neglect. Int Dent J. (2011) 61(3):124–30. doi: 10.1111/j.1875-595X.2011.00028.x
43. El Tantawi M, Attia D, Virtanen JI, Feldens CA, Schroth RJ, Al-Batayneh OB, et al. A scoping review of early childhood caries, poverty and the first sustainable development goal. BMC Oral Health. (2024) 24:1029. doi: 10.1186/s12903-024-04790-w
44. Folayan MO, El Tantawi M, Aly NM, Al-Batayneh OB, Schroth RJ, Castillo JL, et al. Association between early childhood caries and poverty in low and middle income countries. BMC Oral Health. (2020) 6(1):8. doi: 10.1186/s12903-019-0997-9
45. Vasireddy D, Sathiyakumar T, Mondal S, Sur S. Socioeconomic factors associated with the risk and prevalence of dental caries and dental treatment trends in children: a cross-sectional analysis of national survey of Children’s Health (NSCH) data, 2016–2019. Cureus. (2021) 13(11):e19184. doi: 10.7759/cureus.19184
46. Chi DL, Masterson EE, Carle AC, Mancl LA, Coldwell SE. Socioeconomic status, food security, and dental caries in US children: mediation analyses of data from the national health and nutrition examination survey, 2007–2008. Am J Public Health. (2014) 104(5):860–4. doi: 10.2105/AJPH.2013.301699
47. Edelstein BL. The dental caries pandemic and disparities problem. BMC Oral Health. (2006) 6(Suppl 1):S2. doi: 10.1186/1472-6831-6-s1-s2
48. Phantumvanit P, Makino Y, Ogawa H, Rugg-Gunn A, Moynihan P, Petersen PE, et al. WHO global consultation on public health intervention against early childhood caries. Community Dent Oral Epidemiol. (2018) 46:280–7. doi: 10.1111/cdoe.12362
49. Kassebaum NJ, Bernabé E, Dahiya M, Bhandari B, Murray CJ, Marcenes W. Global burden of untreated caries: a systematic review and metaregression. J Dent Res. (2015) 94(5):650–8. doi: 10.1177/0022034515573272
50. Zou J, Du Q, Ge L, Wang J, Wang X, Li Y, et al. Expert consensus on early childhood caries management. Int J Oral Sci. (2022) 14:35. doi: 10.1038/s41368-022-00186-0
51. Ramos-Gomez F. Understanding oral health disparities in the context of social justice, health equity, and children’s Human rights. J Am Dent Assoc. (2019) 150(11):898–900. doi: 10.1016/j.adaj.2019.09.004
52. Schroth RJ, Edwards JM, Brothwell DJ, Yakiwchuk CA, Bertone MF, Mellon B, et al. Evaluating the impact of a community-developed collaborative project for the prevention of early childhood caries: the healthy smile happy child project. Rural Remote Health. (2015) 15(4):3566.26530126
53. Fernando S, Kanthi RD, Bakr M, Johnson NW. Promoting oral health of preschool children using non-dental personnel in rural Sri Lanka. Int J Dent Clin. (2015) 7(4):a–g.
54. de Silva AM, Hegde S, Akudo Nwagbara B, Calache H, Gussy MG, Nasser M, et al. Community-based population-level interventions for promoting child oral health. Cochrane Database Syst Rev. (2016) 9(9):CD009837. doi: 10.1002/14651858.CD009837.pub2
55. Idriss-Wheeler D, Ormel I, Assefa M, Rab F, Angelakis C, Yaya S, et al. Engaging community health workers (CHWs) in Africa: lessons from the Canadian red cross supported programs. PLOS Glob Public Health. (2024) 4(1):e0002799. doi: 10.1371/journal.pgph.0002799
56. Africa CDC. Africa’s opportunity to grow Community Health Workers (2024). Available at: https://africacdc.org/news-item/africas-opportunity-to-grow-community-health-workers/ (Accessed November 5, 2024).
57. Malele-Kolisa Y, Yengopal V, Igumbor J, Nqcobo CB, Ralephenya TRD. Systematic review of factors influencing oral health-related quality of life in children in Africa. Afr J Prim Health Care Fam Med. (2019) 11(1):e1–e12. doi: 10.4102/phcfm.v11i1.1943
58. Masiga MA, M'Imunya JM. Prevalence of dental caries and its impact on quality of life (QoL) among HIV-infected children in Kenya. J Clin Pediatr Dent. (2013) 38(1):83–7. doi: 10.17796/jcpd.38.1.62l1q94650j5l815
59. Masumo RM, Ndekero TS, Carneiro LC. Prevalence of dental caries in deciduous teeth and oral health related quality of life among preschool children aged 4–6 years in Kisarawe, Tanzania. BMC Oral Health. (2020) 20(1):46. doi: 10.1186/s12903-020-1032-x
60. Birungi N, Fadnes LT, Nankabirwa V, Tumwine JK, Åstrøm AN, PROMISE-EBF Study Group. Caretaker’s caries experience and its association with early childhood caries and children’s Oral health-related quality of life: a prospective two-generation study. Acta Odontol Scand. (2016) 74(8):605–12. doi: 10.1080/00016357.2016.1225981
61. Teshome A, Muche A, Girma B. Prevalence of dental caries and associated factors in east Africa, 2000–2020: systematic review and meta-analysis. Front Public Health. (2021) 9:645091. doi: 10.3389/fpubh.2021.645091
62. Groce N, Challenger E, Berman-Bieler R, Farkas A, Yilmaz N, Schultink W, et al. Malnutrition and disability: unexplored opportunities for collaboration. Paediatr Int Child Health. (2014) 34(4):308–14. doi: 10.1179/2046905514Y.0000000156
63. Watt S, Dyer TA, Marshman Z, Jones K. Does poor oral health impact on young children’s Development? A rapid review. Br Dent J. (2024) 237:255–60. doi: 10.1038/s41415-024-7738-4
64. Klein M, Sosu EM, Dare S. School absenteeism and academic achievement: does the reason for absence matter? AERA Open. (2022) 8. doi: 10.1177/23328584211071115
65. Federation FWD. FDI policy statement on oral health and quality of life: adopted by the FDI general assembly: 24 September 2015, Bangkok, Thailand. Int Dent J. (2016) 66:11–2. doi: 10.1111/idj.12233
66. Nadelman P, Bedran N, Magno MB, Masterson D, de Castro ACR, Maia LC. Premature loss of primary anterior teeth and its consequences to primary dental arch and speech pattern: a systematic review and meta-analysis. Int J Paediatr Dent. (2020) 30:687–712. doi: 10.1111/ipd.12644
67. Gomes MC, Perazzo MF, Neves ÉTB, Siqueira MBLD, Paiva SM, Granville-Garcia AF. Premature primary tooth loss and oral health-related quality of life in preschool children. Int J Environ Res Public Health. (2022) 19(19):12163. doi: 10.3390/ijerph191912163
68. Morales F, Montserrat-de la Paz S, Leon MJ, Rivero-Pino F. Effects of malnutrition on the immune system and infection and the role of nutritional strategies regarding improvements in Children's Health Status: a literature review. Nutrients. (2023) 16(1):1. doi: 10.3390/nu16010001
69. CDC. Health policy analysis and evidence. Centers of disease control (2019). Available at: https://www.cdc.gov/policy/analysis/index.html (Accessed November 05, 2024).
70. Mukhari-Baloyi NA, Bhayat A, Madiba TK, Nkambule NR. A review of the South African national oral health policy. S Afr Dent J. (2021) 76(09):551–7. doi: 10.17159/2519-0105/2021/v76no9a6
71. Goldfeld S, Francis KL, Hoq M, Do L, O'Connor E, Mensah F. The impact of policy modifiable factors on inequalities in rates of child dental caries in Australia. Int J Environ Res Public Health. (2019) 16(11):1970. doi: 10.3390/ijerph16111970
72. World Health Organization. 1978: Declaration of Alma-Ata, International Conference on PHC, Alma-Ata, 6-12 September. (1978). Available at: http://www.who.int/hpr/NPH/docs/declaration_almaata.pdf (Accessed November 05, 2024).
73. Emami E, Harnagea H, Girard F, Charbonneau A, Voyer R, Bedos CP, et al. Integration of oral health into primary care: a scoping review protocol. BMJ Open. (2016) 6(10):e013807. doi: 10.1136/bmjopen-2016-013807
74. Azevedo MJ. The State of Health System(s) in Africa: challenges and opportunities. Historical perspectives on the State of Health and Health Systems in Africa, volume II. (2017) 1–73. doi: 10.1007/978-3-319-32564-4_1
75. National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on Community-Based Solutions to Promote Health Equity in the United States. Baciu A, Negussie Y, Geller A, Weinstein JN, editors. Communities in Action: Pathways to Health Equity. Washington, DC: National Academies Press (US) (2017).
76. Black RE, Laxminarayan R, Temmerman M, editors. Reproductive, Maternal, Newborn, and Child Health: Disease Control Priorities, Third Edition (Volume 2). Washington, DC: The International Bank for Reconstruction and Development/The World Bank (2016).
77. Smit D, Barrie R, Louw A. The burden of dental caries in the western cape and a recommended turn-around strategy. South African Dent J. (2017) 72(8):360–5. doi: 10.17159/2519-0105/2017/v72no8a3
78. Africa CDC. Africa CDC Spearheads Bold Move to Secure Africa’s Health Future by Creating a 50 billion Dollar Medical Market (2024). Available at: https://africacdc.org/news-item/africa-cdc-spearheads-bold-move-to-secure-africas-health-future-by-creating-a-50-billion-dollar-medical-market/ (Accessed November 5, 2024).
79. Sabbah W, Folayan MO, El Tantawi M. The link between oral and general health. Int J Dent. (2019) 2019:7862923. doi: 10.1155/2019/7862923
80. Saccomanno S, De Luca M, Saran S, Petricca MT, Caramaschi E, Mastrapasqua RF, et al. The importance of promoting oral health in schools: a pilot study. Eur J Transl Myol. (2023) 33(1):11158. doi: 10.4081/ejtm.2023.11158
81. Nakre PD, Harikiran AG. Effectiveness of oral health education programs: a systematic review. J Int Soc Prev Community Dent. (2013) 3(2):103–15. doi: 10.4103/2231-0762.127810
82. Petersen PE, Hunsrisakhun J, Thearmontree A, Pithpornchaiyakul S, Hintao J, Jürgensen N, et al. School-based intervention for improving the oral health of children in southern Thailand. Community Dent Health. (2015) 32(1):44–50.26263592
83. Akera P, Kennedy SE, Schutte AE, Richmond R, Hodgins M, Lingam R. Perceptions of oral health promotion in primary schools among health and education officials, community leaders, policy makers, teachers, and parents in Gulu district, Northern Uganda: a qualitative study. PLoS One. (2023) 18(11):e0293761. doi: 10.1371/journal.pone.0293761
84. Rughani R, Ondhia A. They're not “just baby teeth”. BDJ Team. (2023) 10:10–3. doi: 10.1038/s41407-023-1709-5
85. UNESCO. 250 million children out-of-school: What you need to know about UNESCO’s latest education data. Available at: https://www.unesco.org/en/articles/250-million-children-out-school-what-you-need-know-about-unescos-latest-education-data#:∼:text=Globally%2C%2016%20%25%20of%20children%20and,Loading%2C%20please%20wait (Accessed December 5, 2024).
86. Braun PA, Widmer-Racich K, Sevick C, Starzyk EJ, Mauritson K, Hambidge SJ. Effectiveness on early childhood caries of an oral health promotion program for medical providers. Am J Public Health. (2017) 107(S1):S97–S103. doi: 10.2105/AJPH.2017.303817
87. Gaffar B, Schroth RJ, Foláyan MO, Ramos-Gomez F, Virtanen JI. A global survey of national oral health policies and its coverage for young children. Front Oral Health. (2024) 5:1362647. doi: 10.3389/froh.2024.1362647
88. The DHS Program. Available at: https://www.dhsprogram.com/Countries/ (Accessed December 5, 2024).
89. Wang TT, Mathur MR, Schmidt H. Universal health coverage, oral health, equity and personal responsibility. Bull World Health Organ. (2020) 98(10):719–21. doi: 10.2471/BLT.19.247288
90. Folayan MO, Tantawi ME, Virtanen JI, Feldens CA, Rashwan M, Kemoli AM, et al. Early childhood caries advocacy group. An ecological study on the association between universal health service coverage index, health expenditures, and early childhood caries. BMC Oral Health. (2021) 21(1):126. doi: 10.1186/s12903-021-01500-8 Erratum in: BMC Oral Health. 2021 May 26;21(1):278. doi: 10.1186/s12903-021-01624-x.33731081
92. Douglass JM, Clark MB. Integrating oral health into overall health care to prevent early childhood caries: need, evidence, and solutions. Pediatr Dent. (2015) 37(3):266–74.26063555
93. Betts KJ, Moravec L. Integration of oral health screening, intervention, and referral into the pediatric well-child visit. J Pediatr Health Care. (2023) 37(6):609–15. doi: 10.1016/j.pedhc.2023.05.007
94. IOM and NRC. Improving Access to Oral Health Care for Vulnerable and Underserved Populations. Washington DC: The National Academies Press (2011).
95. Muhoozi GKM, Atukunda P, Skaare AB, et al. Effects of nutrition and hygiene education on oral health and growth among toddlers in rural Uganda: follow-up of a cluster-randomised controlled trial. Trop Med Int Health. (2018) 23(4):391–404. doi: 10.1111/tmi.13036
96. Fisher J, Berman R, Buse K, Doll B, Glick M, Metzl J, et al. Achieving oral health for all through public health approaches, interprofessional, and transdisciplinary education. NAM Perspect. (2023) 2023:10.31478/202302b. doi: 10.31478/202302b
97. Tiwari T, Sharma T, Harper M, Zacher T, Roan R, George C, et al. Community based participatory research to reduce oral health disparities in American Indian children. J Fam Med. (2015) 2(3):1028.26090520
98. Gao SS, Yon MJY, Chen KJ, Duangthip D, Lo ECM, Chu CH. Utilization of a mobile dental vehicle for oral healthcare in rural areas. Int J Environ Res Public Health. (2019) 16(7):1234. doi: 10.3390/ijerph16071234
99. Nghayo HA, Palanyandi CE, Ramphoma KJ, Maart R. Oral health community engagement programs for rural communities: a scoping review. PLoS One. (2024) 19(2):e0297546. doi: 10.1371/journal.pone.0297546
100. WHO. Global Strategy and Action Plan on Oral Health 2023–2030. Geneva: World Health Organization (2024). Licence: CC BY-NC-SA 3.0 IGO.
101. Mohammed A, Idris-Dantata H, Okwor T, Tanui P, Paintsil E, Kabwe PC, et al. Supporting the manufacturing of medical supplies in Africa: collaboration between Africa CDC, partners, and member states. Glob Health Sci Pract. (2023) 11:e2300121. doi: 10.9745/GHSP-D-23-00121
102. Pine CM, Dugdill L. Analysis of a unique global public-private partnership to promote oral health. Int Dent J. (2011) 61(Suppl 2):11–21. doi: 10.1111/j.1875-595X.2011.00036.x
103. Patrick DL, Lee RS, Nucci M, Grembowski D, Jolles CZ, Milgrom P. Reducing oral health disparities: a focus on social and cultural determinants. BMC Oral Health. (2006) 6(Suppl 1):S4. doi: 10.1186/1472-6831-6-S1-S4
104. Benzian H, Garg R, Monse B, Stauf N, Varenne B, et al. Promoting oral health through programs in middle childhood and adolescence. In: Bundy DAP, Silva N, Horton S, editors. Washington, DC: The International Bank for Reconstruction and Development/The World Bank (2017).
105. Hebbal M, Nagarajappa R. Does school-based dental screening for children increase follow-up treatment at dental school clinics? J Dent Educ. (2005) 69(3):382–6. doi: 10.1002/j.0022-0337.2005.69.3.tb03926.x
106. Arora A, Kumbargere Nagraj S, Khattri S, Ismail NM, Eachempati P. School dental screening programmes for oral health. Cochrane Database Syst Rev. (2022) 7(7):CD012595. doi: 10.1002/14651858
107. Rong WS, Bian JY, Wang WJ, Wang JD. Effectiveness of an oral health education and caries prevention program in kindergartens in China. Community Dent Oral Epidemiol. (2003) 31:412–6. doi: 10.1046/j.1600-0528.2003.00040.x
108. You BJ, Jian WW, Sheng RW, Jun Q, Wa WC, Bartizek RD, et al. Caries prevention in Chinese children with sodium fluoride dentifrice delivered through a kindergarten-based oral health program in China. J Clin Dent. (2002) 13:179–84.12116728
109. Tolvanen M, Lahti S, Poutanen R, Seppa L, Pohjola V, Hausen H. Changes in children’s Oral health-related behavior, knowledge and attitudes during a 3.4-yr randomized clinical trial and oral health-promotion program. Eur J Oral Sci. (2009) 117:390–7. doi: 10.1111/j.1600-0722.2009.00640.x
110. Tabatabaei-Moghaddam H, Sano Y, Mammen S. A case study in creating oral health messages for rural low-income families: a comparison to the cultural appropriateness framework. Health Promot Pract. (2014) 15(5):646–53. doi: 10.1177/1524839914533567
111. Faisal MR, Mishu MP, Jahangir F, Younes S, Dogar O, Siddiqi K, et al. The effectiveness of behaviour change interventions delivered by non-dental health workers in promoting Children’s Oral health: a systematic review and meta-analysis. PLoS One. (2022) 17(1). doi: 10.1371/journal.pone.0262118
112. Golinveaux J, Gerbert B, Cheng J, Duderstadt K, Alkon A, Mullen S, et al. Oral health education for pediatric nurse practitioner students. J Dent Educ. (2013) 77(5):581–90. doi: 10.1002/j.0022-0337.2013.77.5.tb05506.x
113. Foláyan MO, Ishola AG, Bhayat A, El Tantawi M, Ndembi N. Strengthening health systems to tackle oral diseases in Africa: Africa centers for disease control and prevention’s Role. Front Public Health. (2025) 13:1539805. doi: 10.3389/fpubh.2025.1539805
114. Chen J, Duangthip D, Gao SS, Huang F, Anthonappa R, Oliveira BH, et al. Oral health policies to tackle the burden of early childhood caries: a review of 14 countries/regions. Front Oral Health. (2021) 2:670154. doi: 10.3389/froh.2021.670154
115. Folayan MO, Tantawi ME, Virtanen JI, Feldens CA, Rashwan M, Kemoli AM, et al. An ecological study on the association between universal health service coverage index, health expenditures, and early childhood caries. BMC Oral Health. (2021) 21(1):126. doi: 10.1186/s12903-021-01500-8. Erratum in: BMC Oral Health. 2021 May 26;21(1):278. doi: 10.1186/s12903-021-01624-x.33731081
116. Foláyan MO, Amalia R, Kemoli A, Sun IG, Duangthip D, Abodunrin O, et al. Can the sustainable development goal 9 support an untreated early childhood caries elimination agenda? BMC Oral Health. (2024) 24(1):776. doi: 10.1186/s12903-024-04552-8
117. Stevens C. Eliminating early childhood caries. Br Dent J. (2019) 226:548. doi: 10.1038/s41415-019-0289-4
Keywords: oral health, public health, primary health care, health policy, preschool child, health care integration, dental products
Citation: Foláyan MO, Ishola AG, Abodunrin OR, Ndembi N and El Tantawi M (2025) Untreated early childhood caries is a potential disability: policy and programme implications for Africa. Front. Oral Health 6:1546747. doi: 10.3389/froh.2025.1546747
Received: 17 December 2024; Accepted: 7 May 2025;
Published: 21 May 2025.
Edited by:
Praveen S. Jodalli, Manipal College of Dental Sciences, IndiaReviewed by:
Afolabi Oyapero, Lagos State University, NigeriaSeverine N. Anthony, Copperbelt University, Zambia
Jai Ganesh R., K.Ramakrishnan College of Technology, India
Copyright: © 2025 Foláyan, Ishola, Abodunrin, Ndembi and El Tantawi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maha El Tantawi, bWFoYV90YW50YXd5QGhvdG1haWwuY29t