 Nansi López-Valverde
Nansi López-Valverde Antonio López-Valverde
Antonio López-Valverde José Antonio Blanco Rueda
José Antonio Blanco Rueda
- Department of Surgery, University of Salamanca, Instituto de Investigación Biomédica de Salamanca (IBSAL), Salamanca, Spain
Peri-implantitis is an infectious-inflammatory disease that affects the tissues surrounding implants and is one of the main causes of implant failure. Hyaluronic acid (HA) is a natural polymer with multiple biomedical and cosmetic applications. The aim of this systematic review and meta-analysis was to evaluate its efficacy in the treatment of peri-implant disease.
Methods: In accordance with PRISMA, the question was established: is HA treatment effective as a sole or adjunctive therapy for the treatment of peri-implantitis? PubMed/Medline, Embase, Cochrane Central, Dentistry & Oral Sciences Source and Web of Science were searched until December 2024. Inclusion criteria were interventional studies (RCTs and case series), according to the PICOs strategy in subjects with peri-implant pathology (participants), treated with HA (intervention) compared to conventionally treated or untreated patients (control) and assessing response to treatment (outcomes).
Results: Thirty-two studies were obtained and four were selected. Risk of bias was assessed using the Cochrane Risk of Bias tool and methodological quality using the Joanna Briggs Institute tool. Meta-analysis of parameters was performed for pooled studies and for subgroups. The overall effect was in favour of the experimental group.
Conclusions: The use of HA as background or adjunctive therapy in peri-implantitis may be effective, although well-designed RCTs are warranted to validate the efficacy of the product.
Systematic Review Registration: Identifier (INPLANSY 2024100050).
1 Introduction
Dental implants have become a reliable treatment for the replacement of missing teeth, with successful results approaching 83% of the cases treated after 16 years of follow-up (1); although some of them fail in the short, medium or long term. This failure is the result of multiple factors: age, smoking, certain systemic pathologies, the site of placement in the maxilla, the quantity and quality of available bone, etc. However, the most frequent local cause of failure is infection (2). The term peri-implantitis describes an inflammatory response to an infection induced by the accumulation of bacterial plaque on the surface of the implant biomaterial, which leads to a loss of supporting bone, its progression being influenced not only by bacterial dysbiosis but also by the host's inflammatory response (3, 4).
Surgical and non-surgical interventions have been proposed for their treatment, with the aim of reducing the peri-implant pocket and bleeding on probing and, therefore, radiographic consolidation of the peri-implant bone. Non-surgical methods include the use of teflon instruments, titanium tips, ultrasonic tips or laser, however, the rough surfaces of implants are difficult to decontaminate because they favor bacterial adhesion. Because of this, this type of treatment is often used in combination with adjunctive techniques such as antiseptic agents or antibiotics (5). However, the treatment of peri-implantitis has become a challenge, due to the difficulty of adequately decontaminating the implant surface, which is of vital importance for the successful resolution of bone defects created by the disease (6).
Hyaluronic acid (HA) is a natural polymer belonging to the glycosaminoglycan family, which is abundant in the extracellular matrix of periodontal tissues (7). It has several physiological functions capable of regulating osmotic pressure and tissue lubrication, helping to maintain the homeostatic and structural integrity of tissues, making it an ideal biomaterial for medical applications (8). In addition, it can act as an external cytoskeleton, modifying and controlling cell morphology and regulating tissue repair processes by activating inflammatory cells that initiate a response to injury and regulate the behavior of epithelial cells and fibroblasts, thus, it may play an important role in the inflammatory response, as high molecular weight HA degrades to lower molecular weight molecules in inflamed tissues such as in the postoperative period after implant surgery (9, 10). In recent years, HA formulations have been developed for topical administration as adjuvant treatment in acute and chronic gingival diseases and in tissue healing after oral surgery, generally based on preclinical studies (11, 12). However, despite the existence of studies on the role of HA in the field of dentistry, clinical studies evaluating the role of HA in peri-implant tissues are scarce and a standard treatment for peri-implantitis cannot yet be extracted from the clinical literature, although its properties as a mediator of the inflammatory response and regulator of tissue regeneration processes, in addition to its demonstrated role in angiogenesis and neovascularization, make it a suitable biomaterial for the adjuvant treatment of peri-implant lesions (13).
Studies on the efficacy of HA in peri-implant diseases are scarce and, to our knowledge, no literature review has been performed, so the aim of the present systematic and meta-analytic review of randomized clinical studies was to evaluate the efficacy of HA in the treatment of peri-implant diseases.
2 Materials and methods
2.1 Study presentation and registration
This systematic review and meta-analysis have been prepared according to “The Pre-ferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) (14) and the Cochrane Handbook guidelines (15). The protocol of this meta-analysis has been registered in INPLASY under the number: INPLASY2024100050, doi number: 10.37766/inplasy2024.10.0050.
2.2 Question of interest
The focus of the research question was formulated according to the PICOs format: “Is HA treatment effective as a sole or adjuvant therapy for the treatment of peri-implantitis?”.
Intervention studies in adult patients with peri-implantitis (P) comparing HA treatment (I) with patients receiving conventional treatment or no treatment (C) were included to observe the effects on clinical parameters (O), and only randomized clinical studies were considered (Table 1).
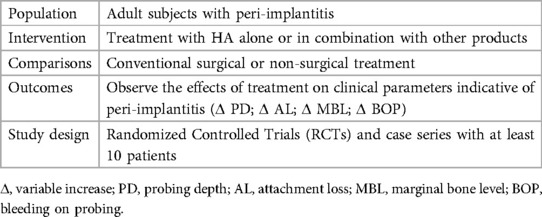
Table 1. PICOs format.
2.3 Studies selection; inclusion and exclusion criteria
The original research studies were selected according to the following inclusion criteria: (i) randomized clinical trials (single or double blind) with more than 10 participants aged 18 years or over; (ii) case series with at least 10 patients; (iii) dealing with peri-implant pathologies; (iv) providing data on clinical parameters indicative of peri-implant disease; (v) that used statistical methods including means and standard deviation, together with the units of measurement of mediator levels; (vi) published in English. Studies that did not meet all the criteria, that lacked data on peri-implant disease, experimental studies in animals or in vitro, clinical cases or case series with fewer than 10 patients, literature reviews and non-relevant studies (editorials, conference contributions, historical reviews, etc.) were excluded.
2.4 Search approach
Two reviewers (NL-V, AL-V) conducted independent searches of the PubMed/Medline, Embase, Cochrane Central, Dentistry & Oral Sciences Source and Web of Science (WOS) databases up to August 2024. They used the Medical Subject Headings (MeSH) terms: Peri-Implantitis*/diagnosis OR Peri-Implantitis*/AND Dental Implants* AND Dental Plaque* AND Hyaluronic Acid/therapeutic use* AND Humans*. In addition, a manual search was carried out and the gray literature was consulted. The bibliographic references of the included studies were also examined to obtain as much information as possible (Table 2).

Table 2. Search strategy.
2.5 Data extraction
Two reviewers (NL-V and AL-V) extracted and tabulated the data from each included study using the standardized JBI-MAStARI data extraction tools. Similarly, the titles and abstracts of the pre-selected studies were reviewed by both reviewers. Those that met the inclusion criteria were read in full and data were extracted. Discrepancies between reviewers were resolved through discussion and the mediation of a third reviewer (JABR). Cohen's kappa index (κ) (16) was used to assess inter-rater agreement. Because all the articles included were randomized studies, the data extraction form “The Joanna Briggs Institute Meta-Analysis of Statistics Assessment and Review Instrument (JBI-MAStARI)” specific for randomized controlled trials was used. The data extracted from the studies included specific details of the interventions, study methods, populations, specific objectives and significant results, in order to formulate the question of interest. The results were subjected to double data entry to minimize errors.
2.6 Methodological rigor of the studies; evaluation of study quality
The methodological quality of the studies included in the meta-analysis was evaluated with the JBI MAStARI tool. This instrument considers the evidence and the specific methods used in RCTs to synthesize different types of evidence. The checklist consists of thirteen items, with possible answers of “yes”, “no”, “unclear”, or “not applicable”. A “yes” answer scores one point. To be included, a study had to obtain a minimum score of seven (17).
2.7 Analysis
The data obtained from the selected RCTs were analyzed with Review Manager software (RevMan Software. Version 5.4.1; The Cochrane Collaboration, Copenhagen, Denmark; 2020). A meta-analysis of the pooled studies and a subgroup analysis were performed for each of the variables that evaluated peri-implantitis. All analyses were based on the mean difference (MD) and standard deviation (SD) to estimate continuous data, and on 95% confidence intervals (CI) to evaluate categorical data. Heterogeneity was considered not important with an I2 of 0%–30%; moderate with an I2 of 40%–50%; substantial with an I2 of 60%–75%; and considerable with an I2 ≥ 75%. The threshold for statistical significance was set at p < 0.05. Due to the homogeneity of the results, a fixed-effect meta-analysis was carried out.
2.8 Risk of bias
Two investigators (NL-V and AL-V) independently assessed the risk of bias of studies using the Cochrane Risk of Bias Tool (RoB2) (18), using 7 domains: Random sequence generation (Selection bias); Allocation concealment (Selection bias); Blinding of participants and personnel (Execution bias); Blinding of outcome assessment (Detection bias); Incomplete outcome data (Attrition bias). Studies were assessed with “high”, “low” and “borderline” risk of bias; “borderline” risk of bias was applied to that lacking information on possible bias. Discrepancies among the evaluators were discussed to reach consensus.
3 Results
The electronic search found a total of 32 results of which 9 full-text publications were evaluated and 5 were excluded based on a priori criteria, resulting in 4 studies included in the meta-analysis (19–22). Inter-reviewer agreement in including studies exceeded 90% (κ >90%) (Figure 1).
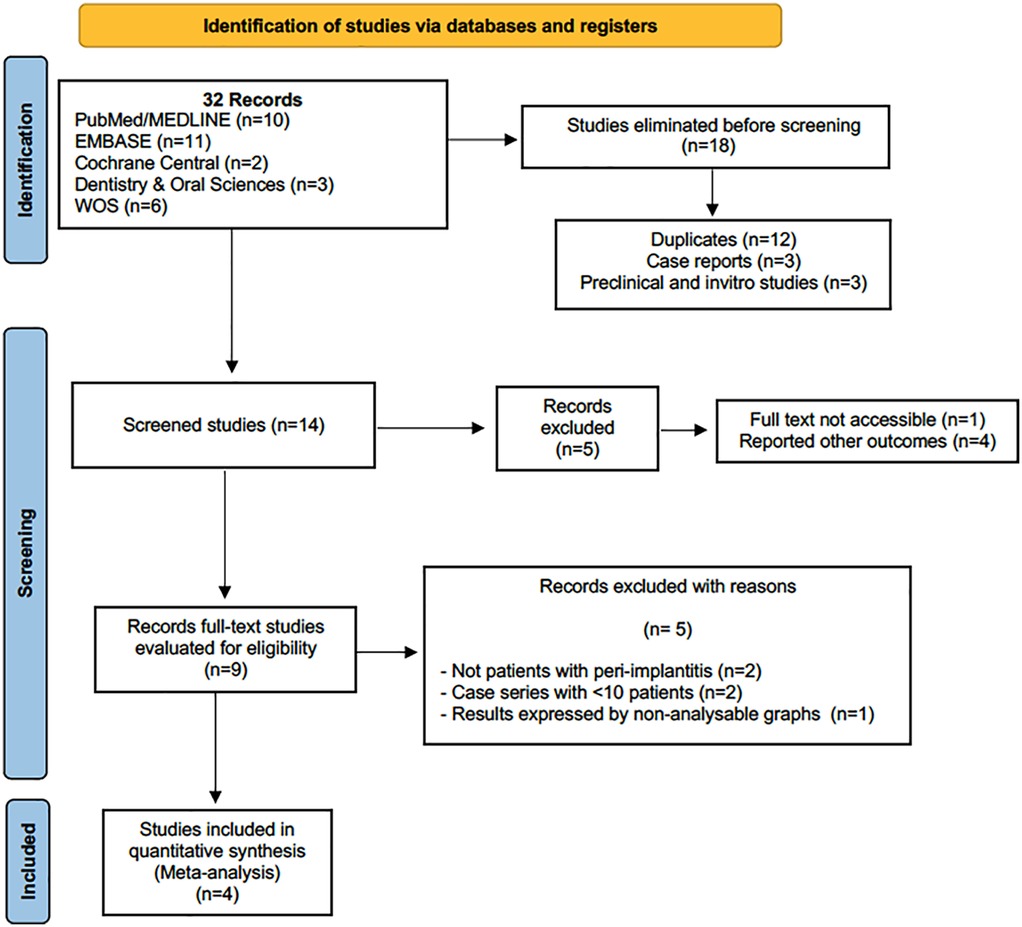
Figure 1. Flowchart.
3.1 Characteristics of the studies
Thirty-two studies were originally identified, 18 of which were eliminated after the first screening. Subsequently, five more studies were eliminated, and then another five, finally leaving four studies for the meta-analysis (19–22), of which three were RCTs (19, 20) and one (22) was a prospective study. A total of 152 patients and 242 implants were studied. The follow-up periods ranged from 1.5 to 12 months.
The study by Soriano-Lerma et al. (19) evaluated the effects of an HA gel on the microbiome of implants with peri-implantitis in 63 patients and 104 implants after 45 days, reporting a decrease in microbial diversity after treatment with HA, compared to the control group.
Sánchez-Fernández et al. (20) investigated the effects of HA on peri-implant clinical variables and the crevicular concentrations of the pro-inflammatory biomarker's interleukin IL-1β and tumor necrosis factor α (TNF-α) in 63 patients and 104 implants in patients with peri-implantitis, finding, after 90 days, a decrease in bleeding on probing, as well as significantly lower PD values in the test group at 45 and 90 days. Similarly, implants with PD ≥5 mm showed higher levels of IL-1β in the control group at 45 days than in the test group.
Rakašević et al. (21) evaluated the clinical and radiographic efficacy of a bovine bone substitute fused with HA in reconstructive surgery of peri-implant bone defects in 13 patients with 19 implants placed and reported a significantly greater vertical gain in minimum crest height at 6 months in the test group compared to the control group.
The prospective study by Friedmann et al. (22) evaluated the efficacy of a cross-linked collagen matrix biofunctionalized with HA as a reconstructive therapy for peri-implantitis, reporting complete pocket closure in the sixth week after surgery. They also found a significant reduction in the number and frequency of bleeding sites, together with a significant reduction in pocket depth and an increase in mineralized tissue (Tables 3 and 4).
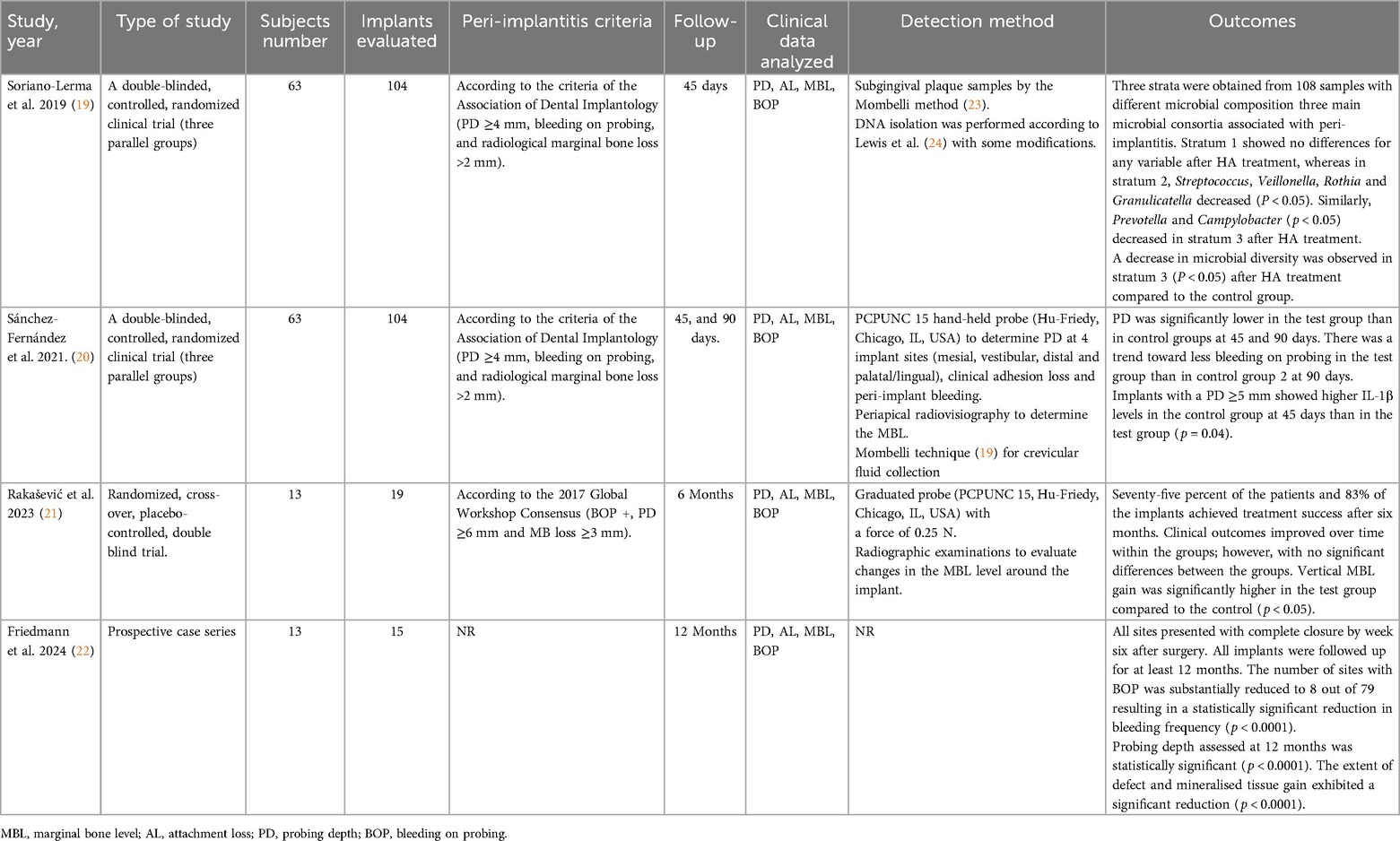
Table 3. Characteristics of studies and participants included in the meta- analysis.
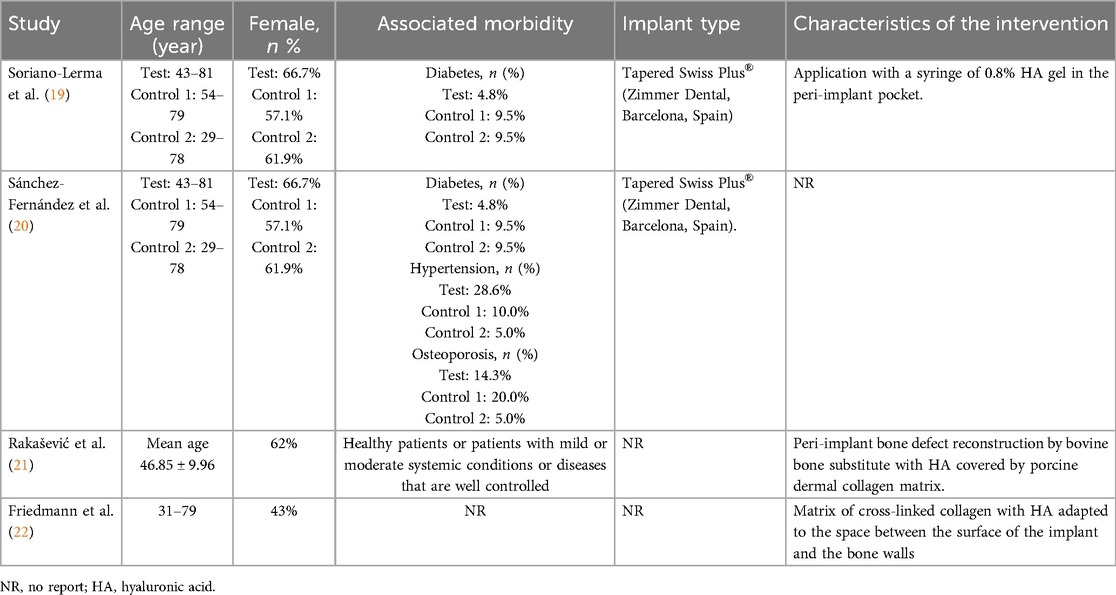
Table 4. Specific and sociodemographic characteristics of the studies.
3.2 Assessment of methodological rigor
The methodological quality of all included studies ranged from very high (>10 points) to high (10 points), as determined by the JBI- MAStARI critical appraisal checklist for RCTs. The study by Friedmann et al. (22) was not evaluated because it was a prospective study (Table 5).
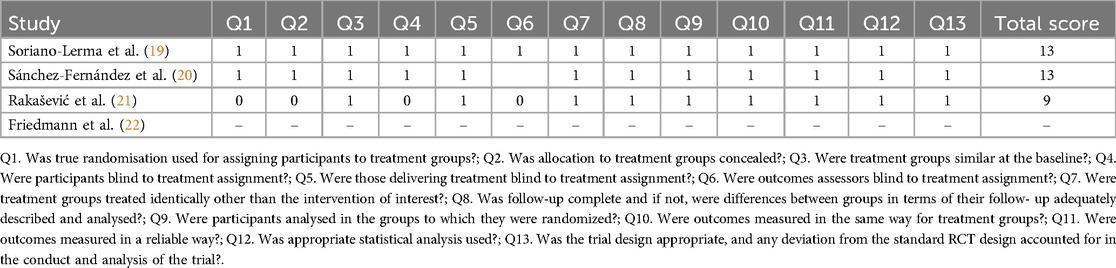
Table 5. Methodological quality of included studies according to JBI-MAStARI.
3.3 Meta-analysis, risk of bias
Separate individual meta-analyses were performed for each of the variables analysed (PD, AL, MBL and BOP). The meta-analysis for the BOP and PD subgroups showed the highest statistical significance (p < 0.00001 and p = 0.0003, respectively), with considerable heterogeneity (I2 = 97% and 84% respectively) and a trend towards significance for the MBL subgroup (p = 0.06), although with moderate heterogeneity (I2 = 59%) (Figures 2–5). Meta-analysis of pooled studies showed statistical significance towards the experimental group (p = 0.007) and substantial heterogeneity (I2 = 79.5%). Not included in this meta-analysis was the LA subgroup, which showed zero heterogeneity (I2 = 0%) and for which a separate fixed-effect meta-analysis was performed (Figure 6). No analysis of adverse effects was performed due to lack of dat.

Figure 2. Forest plot of BOP.

Figure 3. Forest plot of MBL.

Figure 4. Forest plot AL.

Figure 5. Forest plot of PD.
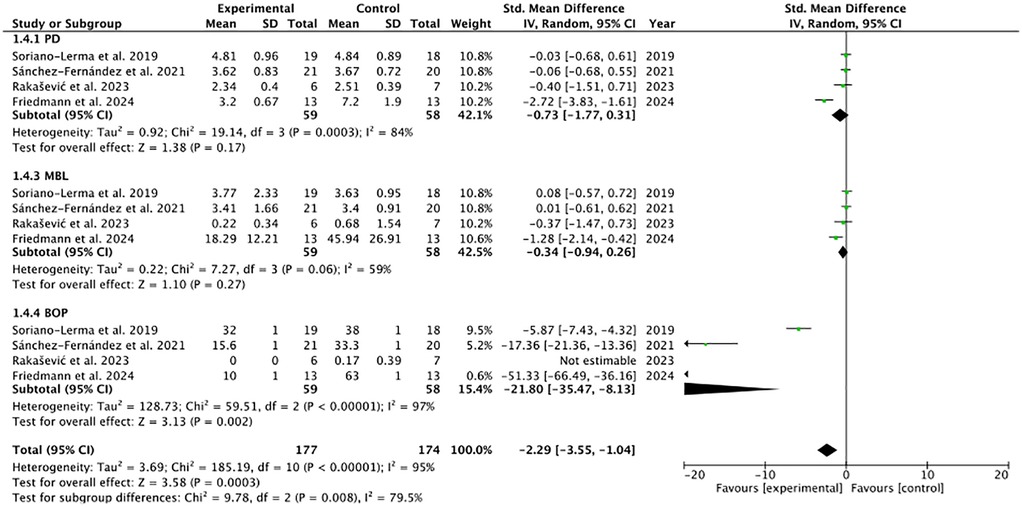
Figure 6. Forest plot of the pooled studies.
Risk of bias assessment is one of the pillars of evidence-based medicine; therefore, two reviewers (NL-V and AL-V) independently analysed the quality of included studies according to the Cochrane Risk of Bias tool. Two of the included studies (19, 20) met the criteria. The study by Rakašević et al. (21) had the highest number of biases, especially in the domains “Allocation concealment”, “Blinding of participants and staff” and “Blinding of outcome data” (Figure 7). The case-control study, for obvious reasons, could not be evaluated.
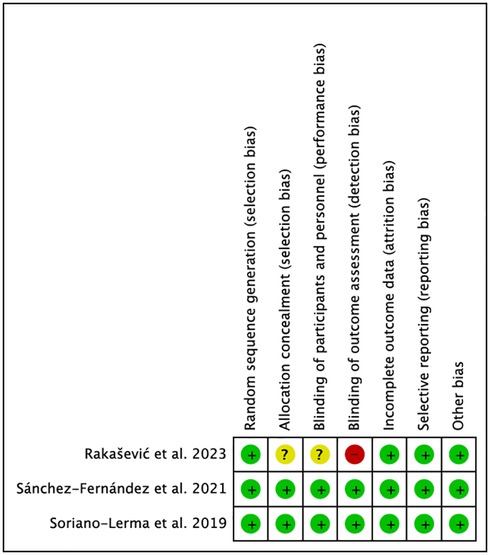
Figure 7. Risk of bias.
3.4 Publication bias
The graphs in Figures 8, 9 (except for AL), where the x-axis represents the observed results and the y-axis the standard error, show a large asymmetry, indicative of publication and reporting bias.
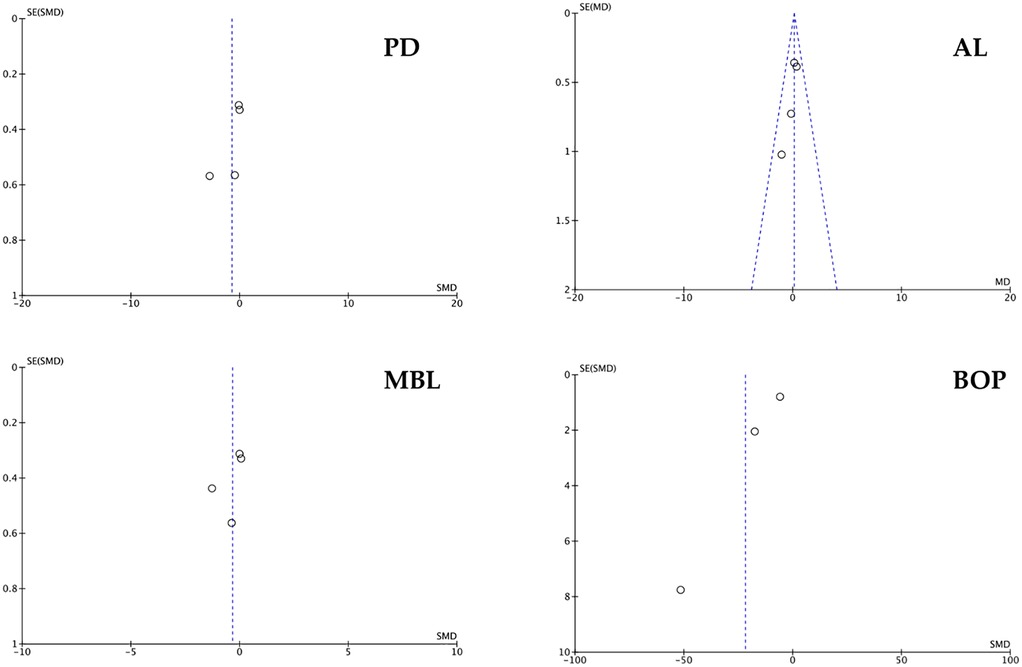
Figure 8. Funnel plot of PD, AL, MBL and BOP. For the AL parameter, a fixed effects funnel plot was performed.
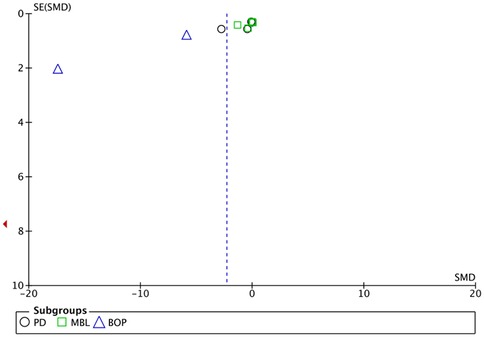
Figure 9. Funnel plot of clustered studies.
4 Discussion
Since so few RCTs have investigated the benefits of HA in peri-implant disease, we set out to prepare this systematic review with meta-analyses that would help to better understand the efficacy of the product in the pathogenesis of inflammatory peri-implant disease. Based on the best available evidence (i.e., three RCTs and one prospective study), we were unable to draw clear conclusions on its clinical efficacy.
Certain studies have highlighted that HA plays an important role in both periodontal repair and regeneration (25). In addition, non-cross-linked HA is considered to enhance tissue lubrication in cartilage, joints, and bones, guiding cell growth and differentiation, as well as accelerating the regeneration process and the healing and repair of chronic wounds (26). Its anti-inflammatory action in the healing process of hard and soft tissues has also been hypothesized (7, 27, 28).
A recent systematic review (29) showed that mechanical debridement alone or with complementary treatment, was not capable of eradicating the predominant pathogens from peri-implantitis sites and in this respect, certain in vitro studies have demonstrated the ability of HA to provoke a bacteriostatic response by reducing pathogenic periodontal bacteria and decreasing bacterial recolonization after mechanical debridement (30, 31). Subsequent to these studies, Soriano-Lerma et al. (19) demonstrated in an RCT on 63 subjects and 104 implants placed, the ability of HA to reduce early biofilm colonising bacteria (Streptococcus, Veillonella and Rothia), as well as a mild action on mid-colonisers (Prevotella and Campylobacter), and its ineffectiveness once late colonisers have established in the peri-implant area. They even reported that the use of HA in advanced stages of peri-implantitis produces a protective action of the peri-implant area against bacterial colonisation, considered the main aetiological cause of complications (32). Early colonisers provide a breeding ground for the colonisation of anaerobic periodontopathogenic bacteria (19), however, mid and late colonisers, with a Gram-negative anaerobic profile, are characteristic of periodontal diseases, although they have also been recognised in peri-implantitis (33, 34).
Inflammation of the peri-implant mucosa and the consequent bone loss are characteristic of peri-implantitis (35), and it has been shown that high molecular weight HA cancels out the immune response and prevents inflammation (36). In preclinical models it has been observed that supplementation with high molecular weight HA is associated with antiapoptotic, antioxidant and anti-inflammatory effects (37) and, in this sense, the study by Soriano-Lerma et al. and Sánchez Fernández et al. (19, 20) used high molecular weight al HA, which could have influenced the treatment results. However, other previous studies had demonstrated the beneficial effects of high molecular weight HA, one in a microbiome analysis (19) and another, a pilot study that evaluated the application of HA as a nebulizer (38). On the other hand, the molecular cross-linking of HA seems to improve its properties by achieving better bioavailability and resistance to degradation (39) and in this respect some research has resorted to cross-linked HA after subgingival instrumentation and has shown gains in clinical attachment levels and reductions in pocket depth levels (40). In our review, only one study (22) resorted to cross-linked HA as adjuvant therapy post-decontamination of the exposed implant surface.
In this context, reconstruction of bone defects caused by peri-implantitis has been proposed with the aim of limiting peri-implant mucosal recession and thus achieving bone regeneration around the implant (41). Since HA is attributed osteoinductive properties that would favor osteogenesis and bone regeneration through osteogenic cell stimulation and differentiation (in addition to influencing angiogenesis and bone neovascularization), it could play a role in this aspect (42). Rakašević et al. (21) in a RCT study on a sample of 13 patients and 19 sites with peri-implantitis, found significant values in terms of vertical bone gain of the marginal bone in the HA-treated group compared to the control (p < 0.05), as well as a significant improvement with respect to the absence of BOP. Friedmann et al. (22) also found a substantial reduction in the number of sites with BOP at 12-month follow-up (p < 0.0001). These results, in agreement with previous preclinical studies (43), could be due to the ability of HA to act as an anti-inflammatory agent by stopping the production of pro-inflammatory cells, however they disagree with the results obtained by Rakašević et al. (21) who only found a complete reduction of BOP in 20% of cases. Sánchez Fernández et al. (20) also observed a greater reduction in bleeding on probing in the experimental group, although without statistical significance (p = 0.07). However, a recent meta-analysis (44) showed that the prevalence of peri-implantitis was around one third in both BOP-positive implants and patients and cautioned that, although this is an indicative clinical factor in the diagnosis of peri-implantitis, clinicians should be aware of the significant false-positive rates of BOP. Other authors (45) have also commented that the value of BOP as a diagnostic tool for peri-implantitis would only fluctuate between 0% and 52% and before establishing a diagnosis of peri-implantitis, this parameter should be evaluated along with other parameters such as visual signs of inflammation, probing depth and progressive bone loss.
During tissue injury, HA is actively produced to regulate inflammatory cell activation and repair of injured tissues. All this results in an innate response that in turn regulates the behavior of epithelial cells and fibroblasts (46). For all these reasons and its anti-inflammatory, immunomodulatory, healing and tissue regenerative properties, HA is an attractive molecule for alternative treatments to conventional ones in pathologies of inflammatory origin (47).
Proinflammatory cytokines (IL-1β, TNF-α, IL-6, IL-17 and IL-12) play an important role in the initiation and progression of inflammatory diseases, and elevated crevicular concentrations of these proinflammatory biomarkers have been associated with peri-implantitis, especially IL-1β, which has been identified as a major contributor to bone loss, and elevated levels of IL-1 β in saliva are considered to reflect a local inflammatory response in peri-implant tissues (48, 49). Similarly, TNF-α is implicated in the destruction of peri-implant tissues by activating immune cells and in-creasing the production of other proinflammatory cytokines (50). Consistently, research has shown that increased levels of TNF-α in saliva are often associated with elevated levels of IL-1 β. These results suggest that the presence of elevated levels of IL-1 β and TNF-α in saliva may serve as a potential biomarker for the diagnosis and follow-up of peri-implantitis (51); however, Sanchez-Fernandez et al. (18) found that only those cases with a PD ≥5 mm showed a significantly greater reduction (p = 0.04) in IL-1β concentrations at 45 days, along with a greater reduction in BOP in the experimental group.
Oral hygiene has a very significant impact on bone stability around osseointegrated implants, and poor oral hygiene is considered to be related to greater bone loss (52). A retrospective cohort study on a predictive model of peri-implantitis that evaluated 254 implants, reported that the most influential factor in predicting survival was the time the implant had been functioning, followed by oral hygiene (53). Various studies have compared different products for the control of peri-implant health (54, 55). An interesting study by de Araujo et al. compared peri-implant health (hard and soft tissue) in 50 edentulous patients and a total of 120 implants, using HA gels or chlorhexidine in the patient maintenance protocol, reporting that both products improved gingival patterns, however, chlorhexidine did so with a constant level of dental plaque index or an increase in supragingival calculus, something that the group treated with HA did not show, and they suggested administering HA in the first 2 months and chlorhexidine between 2 and 6 months. In terms of bacteriology, they highlighted the bacteriostatic effect of HA on microorganisms such as Porphyromonas gingivalis, Aggregatibacter actinomycetemcomitans and Staphylococcus aureus, which leads to a reduction in the risk of postsurgical infection and promotes more predictable regeneration (56). In a similar vein, Soriano-Lerma et al. (19) reported on the ability of HA to reduce the bacteria that colonize the biofilm early on and that the use of HA in advanced stages of peri-implantitis produces a protective action in the peri-implant area against bacterial colonization.
Sánchez-Fernández et al. (20) evaluated the MBL in 104 implants, finding at 45 days a stability of the parameter in the experimental group and increased in the control group, which they attributed to the short duration of the follow-up period or to the fact that the product did not reach the bottom of the peri-implant pocket and, they therefore suggested a longer use, since in a previous study they had reported the opposite, that the application of high molecular weight HA in post-extraction sockets produced an increase in bone formation in the experimental group at 45 days (57). Rakašević et al. (21), after 6 months, also achieved successful treatment of bone defects caused by peri-implantitis, using a bovine bone substitute and HA, without additional MBL loss; however, the best results obtained in reference to this parameter, in the 15 implants analysed, were reported by Friedmann et al. (22) with more than 69% gain of mineralised tissue. Nevertheless, surgical debridement techniques have been used in the past. Used in the latter two studies could bias the excellent results obtained.
It is known that increased PD and AL, due to the loss of supporting bone, decreases the osseointegration of the coronal portion of the implant and, in addition, the rough and threaded surfaces of the implants make their decontamination difficult (58). In this aspect, Sánchez-Fernández et al. (20) used HA gel vs. placebo to reduce peri-implant pockets and increase attachment levels, obtaining values that only approached statistical significance (p = 0.06 for AL and p = 0.08 for PD). Rakašević et al. and Friedmann et al. (21, 22), used bone substitutes in combination with HA gel or HA-functionalised membranes, respectively, obtaining significant reductions in PD (3.9 ± 1.8 mm) compared to surgical treatment alone, which, according to recent meta-analyses, only obtained a mean reduction of 1.27 mm (59, 60).
Our study found in the analysis of pooled studies a strong statistical significance in favour of the intervention group over the control group (p = 0.00001), although heterogeneity was considerable (I2 = 93%). For this reason, we consider it a strength of our meta-analysis that the studies reviewed showed promising results for the use of HA in the treatment of peri-implant pathologies. However, more studies are needed to provide a more detailed understanding of the mechanisms of HA degradation in order to improve its biomedical applications and develop methods that allow for simple administration. It would also be necessary to study its mode of action in inflammatory pathologies, in order to make the most of this powerful molecule.
On the other hand, it should be noted that our systematic review and meta-analysis has a number of limitations and the results obtained should be taken with caution. First, we found significant heterogeneity among the studies that evaluated HA in the treatment of peri-implantitis (except for the AL parameter which yielded an I2 = 0%), due to study design, application of the product (alone or in combination with others), in combination with surgical or non-surgical treatments, doses and outcome assessment. Secondly, three of the included studies were RCTs and one was a prospective case series, and the risk of bias and methodological quality could not be assessed. Therefore, well-designed RCTs with long-term follow-up periods justifying the benefits of HA in the treatment of peri-implantitis are justifiable and necessary. Finally, it would be necessary to test and evaluate HA protocols and formulations suitable for clinical applications.
5 Conclusions
Within these limitations, current data indicate that the application of HA, alone or in combination with other materials in bone defects, may provide additional clinical benefits when used as an adjunct to surgical and non-surgical periodontal treatment. In addition, topical application of HA in peri-implantitis appears to reduce inflammation. However, due to the high risk of bias and heterogeneity, well-designed RCTs evaluating the role of this material in various clinical scenarios are needed.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
NL-V: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. AL-V: Project administration, Writing – original draft, Writing – review & editing. JB: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Smeets R, Henningsen A, Jung O, Heiland M, Hammächer C, Stein JM. Definition, etiology, prevention and treatment of peri-implantitis–a review. Head Face Med. (2014) 10:34. doi: 10.1186/1746-160X-10-34
2. Kochar SP, Reche A, Paul P. The etiology and management of dental implant failure: a review. Cureus. (2022) 14:e30455. doi: 10.7759/cureus.30455
3. Berglundh T, Armitage G, Araujo MG, Avila-Ortiz G, Blanco J, Camargo PM, et al. Peri-implant diseases and conditions: consensus report of workgroup 4 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J Clin Periodontol. (2018) 20:S286–91. doi: 10.1111/jcpe.12957
4. Alves CH, Russi KL, Rocha NC, Bastos F, Darrieux M, Parisotto TM, et al. Host-microbiome interactions regarding peri-implantitis and dental implant loss. J Transl Med. (2022) 20:425. doi: 10.1186/s12967-022-03636-9
5. Ephros H, Kim S, DeFalco R. Peri-implantitis: evaluation and management. Dent Clin North Am. (2020) 64:305–13. doi: 10.1016/j.cden.2019.11.002
6. Almohandes A, Abrahamsson I, Dionigi C, Berglundh T. Surgical treatment of experimental peri-implantitis using mechanical and chemical decontamination procedures: a pre-clinical in vivo study. J Clin Periodontol. (2022) 49:518–25. doi: 10.1111/jcpe.13607
7. Fallacara A, Baldini E, Manfredini S, Vertuani S. Hyaluronic acid in the third millennium. Polymers (Basel). (2018) 10:701. doi: 10.3390/polym10070701
8. Dahiya P, Kamal R. Hyaluronic acid: a boon in periodontal therapy. N Am J Med Sci. (2013) 5:309–15. doi: 10.4103/1947-2714.112473
9. Marcotti S, Maki K, Reilly GC, Lacroix D, Adachi T. Hyaluronic acid selective anchoring to the cytoskeleton: an atomic force microscopy study. PLoS One. (2018) 13:e0206056. doi: 10.1371/journal.pone.0206056
10. Garantziotis S. Modulation of hyaluronan signaling as a therapeutic target in human disease. Pharmacol Ther. (2022) 232:107993. doi: 10.1016/j.pharmthera.2021.107993
11. Mendes RM, Silva GA, Lima MF, Calliari MV, Almeida AP, Alves JB, et al. Sodium hyaluronate accelerates the healing process in tooth sockets of rats. Arch Oral Biol. (2008) 53:1155–62. doi: 10.1016/j.archoralbio.2008.07.001
12. Li L, Lee J, Cho YD, Kim S, Seol YJ, Lee YM, et al. The optimal dosage of hyaluronic acid for bone regeneration in rat calvarial defects. J Periodontal Implant Sci. (2023) 53:259–68. doi: 10.5051/jpis.2203000150
13. Sasaki T, Watanabe C. Stimulation of osteoinduction in bone wound healing by high-molecular hyaluronic acid. Bone. (1995) 16:9–15. doi: 10.1016/s8756-3282(94)00001-8
14. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
15. Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: a new edition of the cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. (2019) 10:ED000142. doi: 10.1002/14651858.ED000142
16. Casagrande A, Fabris F, Girometti R. Beyond kappa: an informational index for diagnostic agreement in dichotomous and multivalue ordered-categorical ratings. Med Biol Eng Comput. (2020) 58:3089–99. doi: 10.1007/s11517-020-02261-2
17. Jordan Z, Lockwood C, Munn Z, Aromataris E. The updated joanna briggs institute model of evidence-based healthcare. Int J Evid Based Healthc. (2019) 17:58–71. doi: 10.1097/XEB.0000000000000155
18. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. Rob 2: a revised tool for assessing risk of bias in randomised trials. Br Med J. (2019) 366:l4898. doi: 10.1136/bmj.l4898
19. Soriano-Lerma A, Magán-Fernández A, Gijón J, Sánchez-Fernández E, Soriano M, García-Salcedo JA, et al. Short-term effects of hyaluronic acid on the subgingival microbiome in peri-implantitis: a randomized controlled clinical trial. J Periodontol. (2020) 91:734–45. doi: 10.1002/JPER.19-0184
20. Sánchez-Fernández E, Magán-Fernández A, O'Valle F, Bravo M, Mesa F. Hyaluronic acid reduces inflammation and crevicular fluid IL-1β concentrations in peri-implantitis: a randomized controlled clinical trial. J Periodontal Implant Sci. (2021) 51:63–74. doi: 10.5051/jpis.1903660183
21. Rakašević D, Šćepanović M, Mijailović I, Mišić T, Janjić B, Soldatović I, et al. Reconstructive peri-implantitis therapy by using bovine bone substitute with or without hyaluronic acid: a randomized clinical controlled pilot study. J Funct Biomater. (2023) 14:149. doi: 10.3390/jfb14030149
22. Friedmann A, Jung R, Bilhan H, Ghawi-Begovic HA, Kauffmann F, Diehl D. Reconstructive surgical therapy of peri-implant defects with ribose cross-linked collagen matrix and crosslinked hyaluronic acid—a prospective case series. Clin Oral Investig. (2024) 28:536. doi: 10.1007/s00784-024-05942-6
23. Mombelli A, McNabb H, Lang NP. Black-pigmenting gram- negative bacteria in periodontal disease. I. Topographic distribution in the human dentition. J Periodontal Res. (1991) 26:301–7. doi: 10.1111/j.1600-0765.1991.tb02067.x
24. Lewis DA, Brown R, Williams J, White P, Jacobson SK, Marchesi JR, et al. The human urinary microbiome; bacterial DNA in voided urine of asymptomatic adults. Front Cell Infect Microbiol. (2013) 3:41. doi: 10.3389/fcimb.2013.00041
25. Donegan GC, Hunt JA, Rhodes N. Investigating the importance of flow when utilizing hyaluronan scaffolds for tissue engineering. J Tissue Eng Regen Med. (2010) 4:83–95. doi: 10.1002/term.208
26. Takeda K, Sakai N, Shiba H, Nagahara T, Fujita T, Kajiya M, et al. Characteristics of high-molecular-weight hyaluronic acid as a brain-derived neurotrophic factor scaffold in periodontal tissue regeneration. Tissue Eng Part A. (2011) 17:955–67. doi: 10.1089/ten.TEA.2010.0070
27. Litwiniuk M, Krejner A, Speyrer MS, Gauto AR, Grzela T. Hyaluronic acid in inflammation and tissue regeneration. Wounds. (2016) 28:78–88.26978861
28. Han W, Lv Y, Sun Y, Wang Y, Zhao Z, Shi C, et al. The anti-inflammatory activity of specific-sized hyaluronic acid oligosaccharides. Carbohydr Polym. (2022) 276:118699. doi: 10.1016/j.carbpol.2021.118699
29. Di Spirito F, Pisano M, Di Palo MP, Salzano F, Rupe A, Fiorino A, et al. Potential impact of microbial variations after peri-implantitis treatment on peri-implant clinical, radiographic, and crevicular parameters: a systematic review. Dent J (Basel). (2024) 12:414. doi: 10.3390/dj12120414
30. Pirnazar P, Wolinsky L, Nachnani S, Haake S, Pilloni A, Bernard GW. Bacteriostatic effects of hyaluronic acid. J Periodontol. (1999) 70:370–4. doi: 10.1902/jop.1999.70.4.370
31. Zamboni F, Okoroafor C, Ryan MP, Pembroke JT, Strozyk M, Culebras M, et al. On the bacteriostatic activity of hyaluronic acid composite films. Carbohydr Polym. (2021) 260:117803. doi: 10.1016/j.carbpol.2021.117803
32. Wadia R. Biofilm as a risk factor in implant treatment. Br Dent J. (2019) 227:1041. doi: 10.1038/s41415-019-1055-3
33. Pokrowiecki R, Mielczarek A, Zaręba T, Tyski S. Oral microbiome and peri-implant diseases: where are we now? Ther Clin Risk Manag. (2017) 13:1529–42. doi: 10.2147/TCRM.S139795
34. Carvalho ÉBS, Romandini M, Sadilina S, Sant'Ana ACP, Sanz M. Microbiota associated with peri-implantitis-A systematic review with meta-analyses. Clin Oral Implants Res. (2023) 34:1176–87. doi: 10.1111/clr.14153
35. Berglundh T, Armitage G, Araujo MG, Avila-Ortiz G, Blanco J, Camargo PM, et al. Peri-implant diseases and conditions. Consensus report of workgroup 4 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J Periodontol. (2018) 89(Suppl 1):S313–8. doi: 10.1002/JPER.17-0739
36. Abbate V, Iaconetta G, Maglitto F, Improta G, Romano A, Bonavolontà P, et al. A comparative study of different administrations of nebulized hyaluronic acid after endoscopic endonasal surgery for chronic rhinosinusitis. Indian J Otolaryngol Head Neck Surg. (2022) 74(Suppl 2):1037–43. doi: 10.1007/s12070-020-02110-6
37. Mohammed AI, Celentano A, Paolini R, Low JT, Silke J, O’ Reilly LA, et al. High molecular weight hyaluronic acid drastically reduces chemotherapy-induced mucositis and apoptotic cell death. Cell Death Dis. (2023) 14:453. doi: 10.1038/s41419-023-05934-6
38. Lopez MA, Manzulli N, D'Angelo A, Lauritano D, Papalia R, Candotto V. The use of hyaluronic acid as an adjuvant in the management of peri-implantitis. J Biol Regul Homeost Agents. (2017) 31:123–7. doi: 10.1002/JPER.19-0184
39. Posarelli C, Passani A, Del Re M, Fogli S, Toro MD, Ferreras A, et al. Cross-linked hyaluronic acid as tear film substitute. J Ocul Pharmacol Ther. (2019) 5:381–7. doi: 10.1089/jop.2018.0151
40. Ramanauskaite E, Machiulskiene V, Shirakata Y, Dvyliene UM, Nedzelskiene I, Sculean A. Clinical evaluation of sodium hypochlorite/amino acids and cross-linked hyaluronic acid adjunctive to non-surgical periodontal treatment: a randomized controlled clinical trial. Clin Oral Investig. (2023) 27:6645–56. doi: 10.1007/s00784-023-05271-0
41. Jepsen S, Schwarz F, Cordaro L, Derks J, Hämmerle CHF, Heitz-Mayfield LJ, et al. Regeneration of alveolar ridge defects. Consensus report of group 4 of the 15th European workshop on periodontology on bone regeneration. J Clin Periodontol. (2019) 46(Suppl 21):277–86. doi: 10.1111/jcpe.13121
42. Arpağ OF, Damlar I, Altan A, Tatli U, Günay A. To what extent does hyaluronic acid affect healing of xenografts? A histomorphometric study in a rabbit model. J Appl Oral Sci. (2018) 26:e20170004. doi: 10.1590/1678-7757-2017-0004
43. Shirakata Y, Imafuji T, Nakamura T, Kawakami Y, Shinohara Y, Noguchi K, et al. Periodontal wound healing/regeneration of two-wall intrabony defects following reconstructive surgery with cross-linked hyaluronic acid-gel with or without a collagen matrix: a preclinical study in dogs. Quintessence Int. (2021) 52:308–16. doi: 10.3290/j.qi.b937003
44. Yu X, Lin X, Wang F, Wu Y. Long-term predictive value of bleeding on probing in peri-implantitis diagnosis: a systematic review and meta-analysis. J Evid Based Dent Pract. (2024) 24:102034. doi: 10.1016/j.jebdp.2024.102034
45. Dukka H, Saleh MHA, Ravidà A, Greenwell H, Wang HL. Is bleeding on probing a reliable clinical indicator of peri-implant diseases? J Periodontol. (2021) 92:1669–74. doi: 10.1002/JPER.20-0890
46. Liang J, Jiang D, Noble PW. Hyaluronan as a therapeutic target in human diseases. Adv Drug Deliv Rev. (2016) 97:186–203. doi: 10.1016/j.addr.2015.10.017
47. Chen LH, Xue JF, Zheng ZY, Shuhaidi M, Thu HE, Hussain Z. Hyaluronic acid, an efficient biomacromolecule for treatment of inflammatory skin and joint diseases: a review of recent developments and critical appraisal of preclinical and clinical investigations. Int J Biol Macromol. (2018) 116:572–84. doi: 10.1016/j.ijbiomac.2018.05.068
48. Liu YC, Lerner UH, Teng YT. Cytokine responses against periodontal infection: protective and destructive roles. Periodontol 2000. (2010) 52:163–206. doi: 10.1111/j.1600-0757.2009.00321.x
49. Gomes AM, Douglas-de-Oliveira DW, Ferreira SD, Silva TAD, Cota LOM, Costa FO. Periodontal disease, peri-implant disease and levels of salivary biomarkers IL-1β, IL-10, RANK, OPG, MMP-2, TGF-β and TNF-α: follow-up over 5 years. J Appl Oral Sci. (2019) 27:e20180316. doi: 10.1590/1678-7757-2018-0316
50. Lumbikananda S, Srithanyarat SS, Mattheos N, Osathanon T. Oral fluid biomarkers for peri-implantitis: a scoping review. Int Dent J. (2024) 74:387–402. doi: 10.1016/j.identj.2023.11.005
51. Gürlek Ö, Gümüş P, Nile CJ, Lappin DF, Buduneli N. Biomarkers and bacteria around implants and natural teeth in the same individuals. J Periodontol. (2017) 88:752–61. doi: 10.1902/jop.2017.160751
52. Serino G, Ström C. Peri-implantitis in partially edentulous patients: association with inadequate plaque control. Clin Oral Implants Res. (2009) 20:169–74. doi: 10.1111/j.1600-0501.2008.01627.x
53. Mameno T, Wada M, Nozaki K, Takahashi T, Tsujioka Y, Akema S, et al. Predictive modeling for peri-implantitis by using machine learning techniques. Sci Rep. (2021) 11:11090. doi: 10.1038/s41598-021-90642-4
54. Butera A, Maiorani C, Gallo S, Pascadopoli M, Venugopal A, Marya A, et al. Evaluation of adjuvant systems in non-surgical peri-implant treatment: a literature review. Healthcare (Basel). (2022) 10:886. doi: 10.3390/healthcare10050886
55. Renvert S, Roos-Jansåker AM, Claffey N. Non-surgical treatment of peri-implant mucositis and peri-implantitis: a literature review. J Clin Periodontol. (2008) 35:305–15. doi: 10.1111/j.1600-051X.2008.01276.x
56. de Araújo Nobre M, Cintra N, Maló P. Peri-implant maintenance of immediate function implants: a pilot study comparing hyaluronic acid and chlorhexidine. Int J Dent Hyg. (2007) 5:87–94. doi: 10.1111/j.1601-5037.2007.00239.x
57. Alcântara CEP, Castro MAA, Noronha MS, Martins-Junior PA, Mendes RM, Caliari MV, et al. Hyaluronic acid accelerates bone repair in human dental sockets: a randomized triple-blind clinical trial. Braz Oral Res. (2018) 32:e84. doi: 10.1590/1807-3107bor-2018.vol32.0084
58. Khammissa RA, Feller L, Meyerov R, Lemmer J. Peri-implant mucositis and peri-implantitis: clinical and histopathological characteristics and treatment. SADJ. (2012) 122:124–6. doi: 10.1038/s41415-024-7402-z
59. Risolo M, Cevik-Aras H, Sayardoust S. The effect of reconstructive techniques as treatment modality for peri-implant osseous defects—a systematic review and meta-analysis. Acta Odontol Scand. (2023) 81:569–77. doi: 10.1080/00016357.2023.2243325
Keywords: hyaluronic acid, dental implants, peri-implantitis, clinical trial, meta-analysis
Citation: López-Valverde N, López-Valverde A and Blanco Rueda JA (2025) Role of hyaluronic acid in the treatment of peri-implant diseases: results of a meta-analysis. Front. Oral Health 6:1564599. doi: 10.3389/froh.2025.1564599
Received: 21 January 2025; Accepted: 24 April 2025;
Published: 1 May 2025.
Edited by:
Federica Di Spirito, University of Salerno, ItalyReviewed by:
Giuseppe Sangiovanni, University of Salerno, ItalyGiuseppina De Benedetto, University of Salerno, Italy
Copyright: © 2025 López-Valverde, López-Valverde and Blanco Rueda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio López-Valverde, YWxvcGV6dmFsdmVyZGVAdXNhbC5lcw==