 Shreya Raj1
Shreya Raj1 Ankita Singh2*
Ankita Singh2*
- 1Department of Conservative Dentistry and Endodontics, DA Pandu Memorial RV Dental College, Affiliated with the Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka, India
- 2Department of Conservative Dentistry and Endodontics, Manipal College of Dental Sciences Mangalore, Manipal Academy of Higher Education, Manipal, Karnataka, India
Background: Cracked tooth syndrome is one of the five types of longitudinal fracture. It has been described as an incomplete fracture progressing from the vital tooth crown and progressing subgingivally, usually in a mesio-distal direction, involving dentin and often the dental pulp. Though termed as a syndrome it doesn't present with a set of classical symptoms. Hence, its diagnosis has always been arduous. This review paper summarises the current strategies in diagnosing a cracked tooth. This paper is an attempt to draw standardized protocols for diagnosing cracked tooth.
Objective: The objective of this paper is to delve deeper into cracked tooth syndrome, thereby examining and simplifying each method to elucidate better its representation in clinics, such as history, examination, imaging etc. for an easier diagnosis.
Clinical significance and relevance: Cracked tooth syndrome is a prevalent problem in dental practice. However, its ambiguous symptoms make a definitive diagnosis difficult, leading to a delay or failure to give appropriate therapy. Thus, it is imperative for a clinician to know about the various methods to correctly diagnose and provide apt and early treatment for cracked teeth.
1 Introduction
According to Dorland's Medical Dictionary, a syndrome presents as “a set of symptoms which occur together” (1). The term “cracked tooth syndrome” (CTS) was first described by Cameron (2, 3). It is one of the five types of Longitudinal fractures, described as an incomplete fracture initiated from the vital tooth crown and extending subgingivally, usually directed in a mesiodistal direction, involving dentin and often the dental pulp (Figure 1) (2–5).
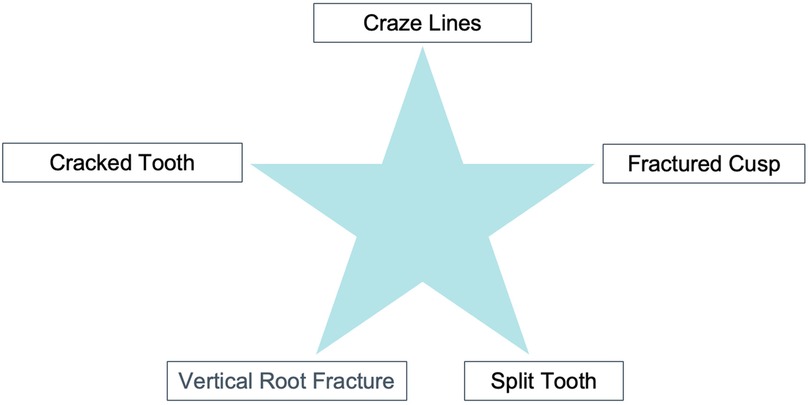
Figure 1. American association of endodontists classification of cracked teeth..
A cracked tooth generally includes one or both of the marginal ridges. This fracture line is usually restricted to the crown of the tooth, although it can extend into the proximal surface of the root. These teeth could be at a higher risk of cuspal fracture, leading to more devastating consequences.
Various terminologies have been proposed for describing cracks in the teeth (Figure 2) (6–11).
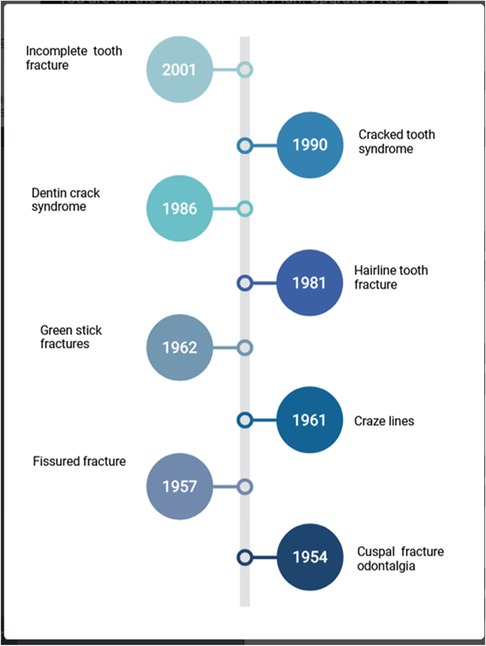
Figure 2. Changing terms over the years for cracked tooth syndrome.
This has led to certain dubiety while attempting to describe clinicians' clinical presentation of cracked teeth (12).
Various factors, including excessive teeth grinding, trauma, and aging, cause the condition. Signs and symptoms vary depending on the severity of the fracture but usually include pain and sensitivity to cold or hot foods and liquids (Figure 3). Diagnosis of CTS is often challenging due to its subtle nature and requires a multidisciplinary approach. This literature review will discuss the signs and symptoms of CTS and the diagnostic methods used to identify the condition accurately.
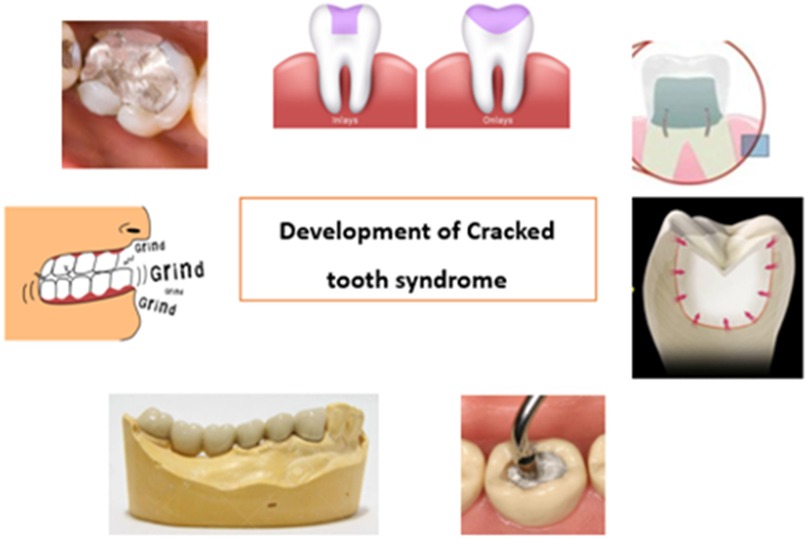
Figure 3. Causes of cracked tooth: (1) heavily restored teeth, (2) inlay/onlay (3) Complex amalgam restorations like pin restorations (4) large forces during restorative procedures like condensation (5) presence of long span bridges (6) parafunctional habits.
2 Methodology
A literature search was carried out on PubMed, MEDLINE (via Ovid), Embase (via Ovid), Scopus, and Web of Science databases for studies published up to March 25th 2025 using a combination of pre-specified “free-text” terms (keywords) and “subject headings”. The Google Scholar search engine was also used to ensure the comprehensiveness of the search and to identify any gray literature. The search process was also supplemented by manual searching in relevant dental journals and reference lists to identify studies missed by our electronic search.
2.1 Signs and symptoms
The cracked tooth syndrome is characterized by a plethora of symptoms that do not follow a clear or consistent pattern. Symptoms differ depending on whether the pulp is healthy, inflammatory, necrotic, or root canal treated (13).
The signs and symptoms of CTS are highly variable, depending on the severity of the fracture. The most common symptoms include:
• Location: Mandibular first molar is the most commonly affected teeth, followed by maxillary premolar, maxillary molar, and mandibular premolar. Mandibular first molars, being the first permanent teeth to erupt, are highly prone to dental caries and restorative treatments, making them more vulnerable to fractures. Additionally, the “wedging effect” from the prominent mesio-palatal cusp of maxillary first molars may further contribute to their susceptibility to fractures (14).
• Pain: Dull vague pain to characteristic “Rebound pain”. Rebound pain is pain experienced on release of pressure upon intake of fibrous food. This is caused by the fractured cusp flexing and repositioning (or “recoiling”), which activates the nerve fibers in dentine tubules from the odontoblastic layer, as well as from the hydrodynamic fluid movement inside the tubules (15).
• Sensitivity to cold or hot foods and beverages.
• Feeling something stuck in the mouth.
Other signs may include a decrease in masticatory function, sensitivity when biting down, and swelling of the gums.
3 Diagnostic methods
Various diagnostic methods for CTS are used in dentistry, including visual inspection of the fractured tooth, palpation and percussion tests, radiography, endodontic probes, and transillumination (Figure 4) (16–18).
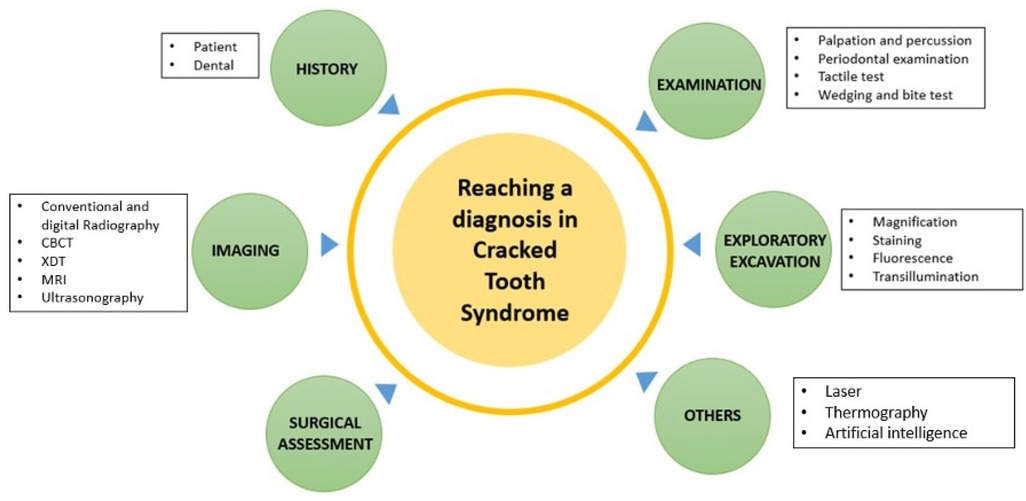
Figure 4. Tools in diagnosing cracked tooth.
Visual inspection is the most common diagnostic tool for determining whether a tooth has been fractured. The clinician should inspect the tooth for discoloration, roughness, and sensitivity to percussion. Palpation and percussion tests also detect tenderness or pain in the fractured area.
Radiography is important for diagnosing CTS and differentiating between a cracked tooth and other conditions such as caries or periodontal disease (18). The radiograph should show a fracture line with a visible crown, root, and enamel-dentin junction.
Endodontic probes can also be used to diagnose CTS. The probe should be inserted into the gingival sulcus and then moved in a mesiodistal direction. If there is an obstruction, this indicates the presence of a crack. Transillumination is another technique used to diagnose CTS, which involves shining a light onto the fractured tooth. If a fracture line is visible, then this is an indication of CTS.
3.1 Subjective examination
3.1.1 Patient history
Patients may fail to localize the problematic tooth and may complain of sensitivity (2, 4, 15). Discomfort while chewing is also one of the common complaints, which is characterized by acute pain on mastication (pressure or release) and sharp, brief pain with cold (14). Pain may range from mild in early stages to very severe spontaneous pain consistent with irreversible pulpitis, necrosis, or apical periodontitis (17). Patient gives a history of accidentally biting a hard object corresponding to the sudden onset of pain. History of damaging habits, such as clenching or grinding the teeth or chewing on ice, pens, hard candy, or other objects, may be reported. A history of a previous incident of a cracked tooth can help reach a diagnosis.
3.1.2 Dental history
The patient may report the underlying cause of the pain and discomfort to have been misdiagnosed. A history of multiple occlusal modifications, with only temporarily relieved symptoms, or screening by several practitioners without a definitive diagnosis, all of which repeatedly indicated no cause for the pain or discomfort.
3.2 Objective visual examination
An additional oral examination reveals enlarged jaw muscles, which might indicate that the person grinds their teeth excessively hard regularly. By carefully analyzing the teeth in a dry condition, craze lines or darker fissures can be observed. The deeper the stains in the crack, the longer the fracture has been there. Other signs of a broken tooth include cracked restorations or unusual gaps between restorations and tooth structure. Wear facets, Cusp-fossae relationships, and a history of teeth clenching or grinding may enhance the probability of fractures.
3.3 Clinical examination
3.3.1 Tactile examination
The tactile examination is done with the aid of an explorer. On the tooth's surface, a sharp explorer's tip would “catch” in a fracture when the explorer is moved (19).
3.3.2 Palpation
Palpation may be ineffective in determining the presence of a crack. Palpating the gingiva surrounding the tooth, on the other hand, may indicate probable dehiscence or fenestration.
3.3.3 Percussion
Percussion helps in determining whether a crack originating from the crown exists. Angular percussion (as opposed to straight vertical percussion) is very advantageous in diagnosis because it can split the fracture line, stimulate the periodontal ligament fibers, or cause fluid to move into the dentinal tubules, which can cause discomfort. Normally, opposite-direction percussion causes no symptoms.
3.3.4 Wedging forces
When wedging forces are applied to a tooth suspected of having crack tooth syndrome, the tooth splits iatrogenically or causes discomfort. It may exacerbate the fracture line, which makes the tooth more prone to a later split. Pressure is applied on the opposing wall to separate the segments, and if no movement is noticed, the tooth is classified as a cracked tooth. A split tooth occurs when the segments separate.
3.3.5 Bite tests
The bite test is intended to imitate the pathognomonic discomfort associated with cracked tooth syndrome that is felt during biting or shortly after the biting pressure is released. Also called “rebound pain” (2, 20). It can be replicated and this pain helps in the identification of a cracked tooth (21). This is caused by the fractured cusp flexing and repositioning (or “recoiling”), which activates the nerve fibers in dentine tubules from the odontoblastic layer, as well as from the hydrodynamic fluid movement inside the tubules (15). However, it is not a confirmatory test.
The bite test can be performed using a wooden toothpick, orange wood sticks, cotton wool rolls, abrasive rubber wheels such as Burlew wheels, or the head of a number 10 round bur in the handle of a cellophane tape (22). Two commercially available instruments are Fractfinder (Denbur, Oak Brook, IL, USA) and Tooth Slooth II (Professional Results Inc., Laguna Niguel, CA, USA). Tooth Slooth is composed of a little plastic biting block in the shape of a pyramid (20 × 10 mm) attached to a handle. We can put the pyramid's tip on each tooth's cusp suspected of having a fracture. The patient is instructed to bite with selective pressure on one cusp. Ehrman et al. suggested adopting this approach since it is more sensitive than wood sticks (20).
3.3.6 Vitality testing
Establishing pulp vitality is critical in diagnosing the pulpal status, but more is needed to aid in crack identification. On the other hand, a crack that continues into the pulp may enable bacterial contamination, affecting the pulp's condition. Periapical and pulp testing findings are similarly varied. The pulp is normally responsive (vital) but can also be non-responsive (necrosis).
3.3.7 Periodontal examination
Periodontal probing may reveal the approximate depth and severity of the fracture. Probing the full perimeter of the tooth in small increments may reveal a narrow, isolated periodontal probing defect, which is indicative of a crack. Subgingival fractures, on the other hand, do not always result in a probing defect. As a result, the absence of thorough probing does not rule out a broken tooth. The presence of deep probing is concerning and implies a worse prognosis. Yang et al. assessed the pulp status in cracked teeth based on periodontal probing depth (PPD) and discovered that cracked teeth with a PPD greater than 4 mm were more likely to have pulp necrosis (21, 23).
3.4 Imaging
3.4.1 Radiographic examination
Seldom are cracks diagnosed through radiographs. However, at later stages, when radiographic evidence of bone defects develops, a crack can be suspected. Taking periapical radiographs from many angles and bitewing radiographs enhances the likelihood of detecting a crack-induced defect early in its development (Figure 5). Thus, newer approaches, such as cone-beam micro-computerized tomography, are more useful in confirming a diagnosis.
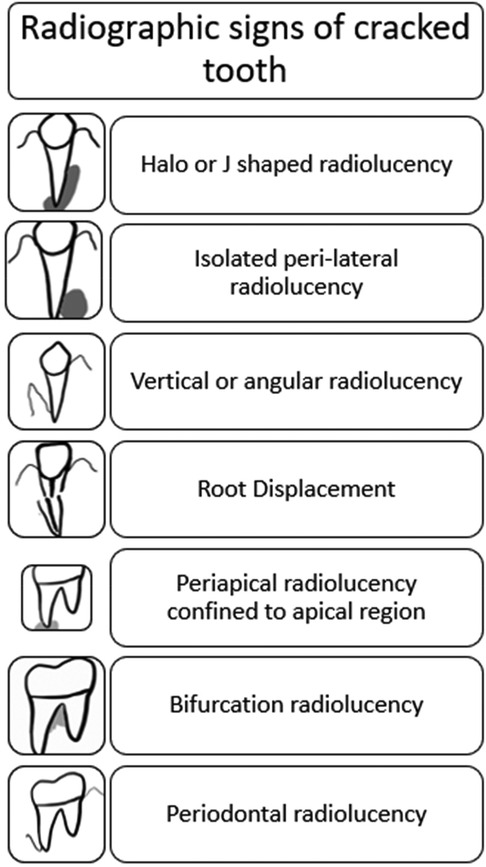
Figure 5. Radiographic signs of cracks and fractures in tooth.
Christoph Jud et al. recently proposed another 3-D imaging method in which they employed x-ray dark-field tomography (XDT) to identify dental microcracks (24, 25).
3.4.2 Optical coherence tomography (OCT)
Optical coherence tomography (OCT) is an optical diagnostic tool based on interferometry. It can offer extensive information on tooth cracks, such as micro-fractures. It is a non-invasive method of diagnosing cracked-tooth syndrome. Sang-Hee Lee et al. effectively showed OCT as an additional approach for broken tooth diagnosis (24).
Sweep source OCT (SS-OCT) is a more sensitive method than previous OCT systems. It obtains subsurface cross-sectional images with the micron-level resolution, which aids in diagnosing cracks.
3.4.3 MRI
The non-invasive and non-ionizing viewing of soft tissues using MRI has shown to be an optimal choice. In their study, Djaudat Idiyatullin et al. demonstrated the ability of SWIFT (Sweep Imaging with Fourier Transformation) MRI to detect cracks as small as 20 micrometers (µm), which is ten times smaller than the imaging voxel size (26).
3.4.4 Ultrasonography
Without the associated risks with ionizing radiation, ultrasound can penetrate hard tissue, including radiopaque restorations (27). In vitro and in vivo Cracked tooth syndrome were successfully identified via ultrasonic systems by Culjat et al. and Sun et al., respectively (28).
3.5 Exploratory excavation
3.5.1 Restoration removal exploratory excavation
Restorations often obscure the cracked tooth. Removal of restorations aids in the visual inspection of the cavity. Special attention is given to weaker areas like mesial and distal marginal ridges. Magnification, staining, transillumination, and application of wedging forces are useful aids in this process.
3.5.2 Staining
To highlight fracture lines on the external tooth surface, in the cavity following restoration removal, or on a surgically exposed root, Iodine, Gentian Violet, or methylene blue dyes can be employed (29).
3.5.3 Magnification
A level magnification of 14×–18× is recommended for the best assessment of enamel fractures. Additionally, it enables us to capture photographs for documentation and record keeping.
3.5.4 Transillumination
Transillumination directly applies a fibreoptic transilluminator or other analogous light sources to the tooth surface (such as a fiber optic handpiece without water or a curing lamp). Transillumination illuminates the fracture from the area of the tooth where the light first penetrates. The fracture line reflects or blocks the light while it passes through structurally sound teeth. Clinically it is the cracked tooth's “night vs. day” appearance (30). Transillumination is particularly beneficial when performed after restorations are removed and are better when used with magnification (22).
3.5.5 Fluorescence
Quantitative light-induced fluorescence (QLF) devices can diagnose tooth fractures. Crack lines get contaminated over time by oral biofilms and metabolites such as porphyrin and are seen as red fluorescent lines on QLF images (28, 29). Using QLF on extracted teeth, Jun et al. tried to determine the depth of enamel cracks non-destructively (22). Studies revealed that QLF images are more successful than radiographic and traditional visual examinations in identifying dental caries (Occlusal) and cracked teeth (31). Sung-Ae Son et al. showed the potential utility of QLF in detecting and characterizing tooth cracks, including their position and depth (32).
3.6 Surgical assessment
Surgical exploration can only be used to visually evaluate the root surface for the existence of a fracture if a crack is highly suspected and cannot be verified by any other method. As neighbouring teeth limit visibility in buccolingual cracks, they are easily identified after surgery.
3.6.1 Others
3.6.1.1 Laser
Lasers are used in dentistry for various purposes, especially as diagnostic and therapeutic aids. In a recent study, Ashita Sapra et al. demonstrated the ability of an 810-nm diode laser at 1W continuous wave to detect early signs of tooth crack (33).
3.6.1.2 Thermography
This non-invasive imaging and visual inspection approach employ bio-thermal patterns. Matsushita-Tokugawa et al. discovered that Vibrothermography (VibroIR) might be a viable approach for identifying dentinal root microcracks by using friction heat generated by ultrasonic vibration (34).
3.6.1.3 Artificial intelligence (AI)
Computers imitate intelligent behavior with minimum human interaction, referred to as artificial intelligence (AI). Treatments or image-based detection algorithms have been created to provide an error-free diagnosis. Fukuda et al. demonstrated that the CNN learning model could recognize VRFs (Vertical Root Fractures) on panoramic photos and operate as a CAD tool (35).
Three approaches to AI have been listed. The first is the CNN-based crack detection (Convolutional neural network) approach, where image classification, object detection, and semantic segmentation are thoroughly discussed. To be more specific, image classification-based algorithms (Alexnet) handle the crack detection issue as if it were a binary classification problem. However, its efficiency is slightly limited. Another technique is Object detection-based methods (YOLO, Faster R-CNN), where they immediately give information about the position and size of the targets of interest with a tagged bounding box in the picture. And finally, the third one is Pixel-level crack segmentation algorithms (Unet, Segnet, CrackSeg), a promising technique for fracture identification since they extract accurate information and more specific properties such as crack route, position, length, width, and density. However, technical challenges with AI-based detection may persist, such as high computing costs, issues selecting appropriate parameters, and the generation or pre-processing of training data sets (36–38).
3.6.1.4 Management and prognosis
Formulating treatment plan for cracked tooth depends upon the extent of fracture line and the pulpal status (34, 39, 40).
The management of a cracked tooth largely depends on factors such as the location, orientation, extent, and severity of the crack. Cracks that are superficial are typically identified early, making them easier to treat. These minor fractures are commonly addressed with simple restorative procedures, like fillings or crowns.
However, when the crack extends deeper and involves the dental pulp, more extensive treatment such as root canal therapy followed by crown placement is necessary to preserve the tooth.
In severe cases, where the crack reaches below the gum line and into the tooth root, repair becomes unfeasible. Such situations usually necessitate tooth extraction, followed by replacement options like dental implants or bridges.
Clark and Caughman categorized the prognosis of cracked teeth into four levels: excellent, good, poor, and hopeless (41, 42).
• Excellent prognosis: Involves fractures within the dentin that angle from the cusp line angles toward the cemento-enamel junction, or slight subgingival extensions, or horizontal fractures of a cusp that do not affect the pulp.
• Good prognosis: Applies to vertical fractures confined to the crown that run mesiodistally into the dentin without reaching the pulp.
• Poor prognosis: Describes cracks that penetrate both the dentin and pulp but remain restricted to the crown.
• Hopeless prognosis: Indicates fractures that travel through the pulp and extend into the root structure, making tooth preservation unlikely.
4 Conclusion
Oral radiographs and cross-sectional images are the most useful methods for diagnosing cracked teeth. While MRI and ultrasonography have been used to identify the crack, they do not show the lesion's exact location. Laser, thermography, and surgical assessment are viable options, but they may need to provide more information to diagnose CTS accurately. AI-based techniques are a promising approach for crack detection, and they have the potential to provide more precise results than more traditional methods. However, AI-based approaches are still in development and will require further research before they can be applied to clinical practice. A combination of diagnostic tools is needed to diagnose CTS and provide effective treatment accurately.
Author contributions
SR: Conceptualization, Data curation, Methodology, Resources, Writing – original draft, Writing – review & editing. AS: Data curation, Formal analysis, Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to acknowledge the support of our institution and all our colleagues and senior faculty who have helped us in formulating this manuscript. We shall be forever indebted for their invaluable contributions and guidance.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Newman Dorland WA. Dorland’s Illustrated Medical Dictionary. 32nd ed. Philadelphia, Pa: Saunders/Elsevier (1925).
2. Cameron CE. The cracked tooth syndrome: additional findings. J Am Dent Assoc. (1976) 93(5):971–5. doi: 10.14219/jada.archive.1964.0108
3. Ehrmann EH, Tyas MJ. Cracked tooth syndrome. Aust Dent J. (1990) 35(4):390–1. doi: 10.1111/j.1834-7819.1990.tb05413.x
4. Rivera EM, Walton RE. Cracking the cracked tooth code: detection and treatment of various longitudinal tooth fractures. Am Assoc Endo Coll Excell News Lett. (2008) 2:1–9. https://winnetkaendodontics.com/wp-content/uploads/2022/07/Cracked-Teeth-Detection.pdf
5. Rivera EM, Walton RE. Longitudinal tooth fractures: findings that contribute to complex endodontic diagnoses. Endod Topics. (2009) 16(1):82–111. doi: 10.1111/j.1601-1546.2009.00243.x
6. Kahler W. The cracked tooth conundrum: terminology, classification, diagnosis, and management. Am J Dent. (2008) 21(5):275–8.19024251
9. Caufield JB. Hairline tooth fracture: a clinical case report. J Am Dent Assoc. (1981) 102(4):501–2. doi: 10.14219/jada.archive.1981.0145
10. Down CH. The treatment of permanent incisor teeth of children following traumatic injury. Aust Dent J. (1957) 2(1):9–24. doi: 10.1111/j.1834-7819.1957.tb01717.x
11. Ellis SG. Incomplete tooth fracture–proposal for a new definition. Br Dent J. (2001) 190(8):424–8. doi: 10.1038/sj.bdj.4800992
12. Lin F, Yue L. Analysis of difficulties in diagnosis and treatment of cracked tooth and research progress. Zhonghua Kou Qiang Yi Xue Za Zhi. (2025) 60(1):8–16. doi: 10.3760/cma.j.cn112144-20241031-00411
13. Hasan S, Singh K, Salati N. Cracked tooth syndrome: overview of literature. Int J Appl Basic Med Res. (2015) 5(3):164–8. doi: 10.4103/2229-516X.165376
14. Nuamwisudhi P, Jearanaiphaisarn T. Oral functional behaviors and tooth factors associated with cracked teeth in asymptomatic patients. J Endod. (2021) 47(9):1383–90. doi: 10.1016/j.joen.2021.05.012
15. Brännström M. The hydrodynamic theory of dentinal pain: sensation in preparations, caries, and the dentinal crack syndrome. J Endod. (1986) 12(10):453–7. doi: 10.1016/S0099-2399(86)80198-4
16. Homewood CI. Cracked tooth syndrome: incidence, clinical findings, and treatment. Aust Dent J. (1998) 43(4):217–22. doi: 10.1111/j.1834-7819.1998.tb00167.x
17. Brynjulfsen A, Fristad I, Grevstad T, Hals-Kvinnsland I. Incompletely fractured teeth associated with diffuse longstanding orofacial pain: diagnosis and treatment outcome. Int Endod J. (2002) 35(5):461–6. doi: 10.1046/j.1365-2591.2002.00501.x
18. Patel S, Teng PH, Liao WC, Davis MC, Fidler A, Haupt F, et al. Position statement on longitudinal cracks and fractures of teeth. Int Endod J. (2025) 58(3):379–90. doi: 10.1111/iej.14186
19. Mathew S, Thangavel B, Mathew CA, Kailasam S, Kumaravadivel K, Das A. Diagnosis of cracked tooth syndrome. J Pharm Bioall Sci. (2012) 4(Suppl 2):S242–4. doi: doi: 10.4103/0975-7406.100219
20. Ehrmann EH, Tyas MJ. Cracked tooth syndrome: diagnosis, treatment and correlation between symptoms and post-extraction findings. Aust Dent J. (1990) 35(2):105–12. doi: 10.1111/j.1834-7819.1990.tb05872.x
21. Yang Y, Chen G, Hua F, Yu Q, Yang W. Biting pain reproduced by the tooth slooth: an aid for early diagnosis of cracked tooth. Quintessence Int. (2019) 50(1):82–7. doi: 10.3290/j.qi.a41498
22. American Association of Endodontists. Transillumination: The 31 “Light Detector”. Chicago, IL: AAE (2008). p. 1–2.
23. Rivera EM, Walton RE. Longitudinal tooth cracks and fractures: an update and review. Endod Topics. (2015) 33(1):14–42. doi: 10.111/etp.12085
24. Lee SH, Lee JJ, Chung HJ, Park JT, Kim HJ. Dental optical coherence tomography: new potential diagnostic system for cracked-tooth syndrome. Surg Radiol Anat. (2016) 38:49–54. doi: 10.1007/s00276-015-1514-8
25. Jud C, Sharma Y, Günther B, Weitz J, Pfeiffer F, Pfeiffer D, et al. X-ray dark-field tomography reveals tooth cracks. Sci Rep. (2021) 11(1):14017. doi: 10.1038/s41598-021-93393-4
26. Idiyatullin D, Garwood M, Gaalaas L, Nixdorf DR. Role of MRI for detecting micro cracks in teeth. Dentomaxillofac Radiol. (2016) 45(7):20160150. doi: 10.1259/dmfr.20160150
27. Li F, Diao Y, Wang J, Hou X, Qiao S, Kong J, et al. Review of cracked tooth syndrome: etiology, diagnosis, management, and prevention. Pain Res Manag. (2021) 2021(1):3788660. doi: 10.1155/2021/3788660
28. Culjat MO, Singh RS, Brown ER, Neurgaonkar RR, Yoon DC, White SN. Ultrasound crack detection in a simulated human tooth. Dentomaxillofac Radiol. (2005) 34(2):80–5. doi: 10.1259/dmfr/12901010
29. Yang S, Jeon MJ, Kim BI, Shin SJ, Park JW. Assessing endodontic treatment feasibility for cracked teeth using quantitative light-induced fluorescence: a retrospective clinical study. J Endod. (2025) 51(5):577–84. doi: 10.1016/j.joen.2025.01.013
30. Son SA, Kim JH, Park JK. The effectiveness of a quantitative light-induced fluorescent device for the diagnosis of a cracked tooth: a case report. J Endod. (2021) 47(11):1796–800. doi: 10.1016/j.joen.2021.08.007
31. Sun K, Yuan L, Shen Z, Xu Z, Zhu Q, Ni X, et al. Scanning laser-line source technique for nondestructive evaluation of cracks in human teeth. Appl Opt. (2014) 53(11):2366–74. doi: 10.1364/AO.53.002366
32. Jun MK, Ku HM, Kim E, Kim HE, Kwon HK, Kim BI. Detection and analysis of enamel cracks by quantitative light-induced fluorescence technology. J Endod. (2016) 42(3):500–4. doi: 10.1016/j.joen.2015.12.008
33. Sapra A, Darbar A, George R. Laser-assisted diagnosis of symptomatic cracks in teeth with cracked tooth: a 4-year in-vivo follow-up study. Aust Endod J. (2020) 46(2):197–203. doi: 10.1111/aej.12391
34. Matsushita-Tokugawa M, Miura J, Iwami Y, Sakagami T, Izumi Y, Mori N, et al. Detection of dentinal microcracks using infrared thermography. J Endod. (2013) 39(1):88–91. doi: 10.1016/j.joen.2012.06.033
35. Fukuda M, Inamoto K, Shibata N, Ariji Y, Yanashita Y, Kutsuna S, et al. Evaluation of an artificial intelligence system for detecting vertical root fracture on panoramic radiography. Oral Radiol. (2020) 36:337–43. doi: 10.1007/s11282-019-00409-x
36. Sun J, Jiang J, Xue Z, Pan J, Qiao D. Layered preparation method for cracked tooth preparation robot based on iso-MRR algorithm. IEEE/ASME Trans Mechatron. (2024):1–12. doi: 10.1109/TMECH.2024.3502779
37. Xie Z, Lu Q, Guo J, Lin W, Ge G, Tang Y, et al. Semantic segmentation for tooth cracks using improved DeepLabv3+ model. Heliyon. (2024) 10(4):e25892. doi: 10.1016/j.heliyon.2024.e25892
38. Aminoshariae A, Kulild J, Nagendrababu V. Artificial intelligence in endodontics: current applications and future directions. J Endod. (2021) 47(9):1352–7. doi: 10.1016/j.joen.2021.06.003
39. Zhang S, Xu Y, Ma Y, Zhao W, Jin X, Fu B. The treatment outcomes of cracked teeth: a systematic review and meta-analysis. J Dent. (2024) 142:104843. doi: 10.1016/j.jdent.2024.104843
40. Kwak Y. Endodontic treatment in the management of cracked tooth. J Korean Dent Assoc. (2024) 62(1):54–9. doi: 10.22974/jkda.2024.62.1.005
41. Mathew VB, Shamsuddin S, Langaliya A, Rathod PT, Gupta B, Ronsivalle V, et al. Survivability of endodontically treated cracked tooth: a systematic review. Technol Health Care. (2024) 32(4):2023–37. doi: 10.3233/THC-231993
Keywords: cracked tooth, diagnosis, fracture, treatment plan, cracked tooth syndrome (CTS)
Citation: Raj S and Singh A (2025) Cracked tooth syndrome: a diagnostic dilemma- a mini review. Front. Oral Health 6:1572665. doi: 10.3389/froh.2025.1572665
Received: 17 February 2025; Accepted: 9 June 2025;
Published: 24 June 2025.
Edited by:
Reisha Rafeek, The University of the West Indies St. Augustine, Trinidad and TobagoReviewed by:
Shamimul Hasan, Jamia Millia Islamia, IndiaCopyright: © 2025 Raj and Singh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ankita Singh, c2luZ2guYW5raXRhQG1hbmlwYWwuZWR1