 Omorinola Adekemi Afolabi1*
Omorinola Adekemi Afolabi1* Abel Nnamdi Chukwuemeka2
Abel Nnamdi Chukwuemeka2 Anita Mofiyinfolu Dabar2
Anita Mofiyinfolu Dabar2 Richard Omoefe Oveh3Saheed Ademola Ibraheem4
Richard Omoefe Oveh3Saheed Ademola Ibraheem4 Nadia Adjoa Sam-Agudu5,6,7
Nadia Adjoa Sam-Agudu5,6,7 Maha El Tantawi8,9,10,11
Maha El Tantawi8,9,10,11 Abideen Olurotimi Salako9George Uchenna Eleje10,12Joanne Lusher13
Abideen Olurotimi Salako9George Uchenna Eleje10,12Joanne Lusher13 Oliver Ezechi9
Oliver Ezechi9 Moréniké Oluwátóyìn Foláyan9,10,14
Moréniké Oluwátóyìn Foláyan9,10,14
- 1Department of Social Development, Moshood Abiola Polytechnic, Abeokuta, Ogun, Nigeria
- 2Department of Public Health, Lead City University, Ibadan, Oyo, Nigeria
- 3Department of Information and Communication Technology, University of Delta, Agbor, Delta, Nigeria
- 4Scientific and Industrial Research Department, National Research Institute for Chemical Technology, Zaira, Nigeria
- 5International Research Center of Excellence, Institute of Human Virology, Abuja, Nigeria
- 6Department of Paediatrics and Child Health, University of Cape Coast School of Medical Sciences, Cape Coast, Ghana
- 7Department of Pediatrics, University of Minnesota Medical School, Minneapolis, MN, United States
- 8Faculty of Dentistry, Alexandria University, Alexandria, Egypt
- 9Oral Health Initiative, Nigerian Institute of Medical Research, Yaba, Lagos, Nigeria
- 10Africa Oral Health Network, Alexandria University, Alexandria, Egypt
- 11Faculty of Dental Medicine, Alamein International University, New Alamein City, Egypt
- 12Department of Obstetrics and Gynaecology, Nnamdi Azikiwe University, Awka, Nigeria
- 13Provost’s Group, Regent’s University London, London, United Kingdom
- 14Department of Child Dental Health, Obafemi Awolowo University, Ile-Ife, Nigeria
Background: Adolescence is a critical developmental stage where oral, mental, and sexual and reproductive health are closely interconnected. However, these domains are often assessed in isolation, creating a gap in holistic adolescent health understanding and intervention. This study aimed to develop an integrated tool for assessing oral, mental, and sexual and reproductive health.
Methods: A systematic literature review framework guided the study. Three dimensions—oral health, mental health, and sexual and reproductive health—were defined a priori. A structured search of PubMed and ScienceDirect identified relevant English-language articles and tools validated for use with adolescents in Nigeria. Deductive analysis was used for logical partitioning to identify items for domains and subscales. A preliminary questionnaire was drafted, organized into five sections: socio-demographics, oral health, mental health, sexual and reproductive health, and health service utilization. Items were matched with appropriate response scales.
Results: Seventy-eight articles were identified, and 43 met the inclusion criteria. From these, domains and subscales were adopted to construct an 81-item tool. Section one contains 21 socio-demographic items. Section two covers mental health with five constructs: psychological distress (12 items), depression (nine), generalized anxiety (eight), suicide ideation (four), and risk factors (alcohol, tobacco, psychoactive substance use, and self-esteem). Section three measures sexual and reproductive health with 11 items on sexual debut and activity status. Section four assesses oral health with eight items on oral hygiene, self-reported oral problems, and oral habits. Section five includes two questions on health service utilization, covering general, dental, and psychiatric services.
Conclusion: This integrated 81-item tool captures three interconnected aspects of adolescent health, offering potential to strengthen service integration for this population. Beyond practice, it provides a foundation for empirical research to advance multisectoral adolescent health approaches. Future work should focus on validating the tool across diverse adolescent populations.
Introduction
Adolescents, defined as young people between 10 and 19 years of age (1), are at a critical stage of psychological, social, cognitive, and physical development (2). This is also a stage in life when habits are formed and health practices are developed, which can influence health outcomes at later stages of life (3–6). As such, adolescence is a distinctive stage of human development and a crucial time for establishing the foundations of good health. A strategic and integrated focus on the health and well-being of adolescents is therefore vital for optimal development in future health outcomes (7, 8).
Health-related habits that are formed during adolescence include oral health habits. Poor oral health can affect overall health, school performance, and social interactions (9). For adolescents in Nigeria, the high prevalence of oral diseases is a public health issue. Severe periodontal disease affects 25.1% of people 15 years and older (10), and dental caries affects about 22.9% (11). The large population of adolescents in Nigeria—more than one in four Nigerians are adolescents (12, 13) and 50% of the population is younger than 19 years (14)—suggests that the burden of oral diseases in this population is likely to be significant.
Also, of concern is the high burden of poor mental and sexual, and reproductive health among adolescents in the country. The prevalence of mental health disorders among adolescents ranges between about 10% and 37% (15–17), mainly in the form of depression, anxiety disorders, attention-deficit/hyperactivity disorder, and substance use disorder (18, 19). The high rates of unintended pregnancies, unsafe abortions, and sexually transmitted infections, including HIV, are also a concern, with reports of HIV prevalence being 14%–17%, and the prevalence of other sexually transmissible infections ranging from 29% to 48.8% (20–22).
The high prevalence of oral diseases, mental health challenges, and adverse sexual and reproductive health (SRH) outcomes among Nigerian adolescents is compounded by the significant interconnections between these domains. About 10%–37% of adolescents in Nigeria experience peculiar mental health challenges such as stress, depression, and anxiety (23–26). Poor access to sexual and reproductive health education increases the risks of early initiation of sex, teenage pregnancies, and sexually transmitted infections (27). About 11%—20.2% of adolescents initiate sex by 13 years (28, 29), 18.7%–22.9% of 15–19-year-olds are pregnant (30), and 13% to 95.1% experience sexual abuse (31). Poor oral health increases the risk for poor mental health (32) and vice versa (33). Poor oral health can also mediate poor sexual and reproductive health (34, 35).
These vulnerabilities converge because they share common social, economic, and behavioral determinants, such as family socioeconomic status, stigma, and health-seeking behaviors. This deep interrelatedness necessitates an integrated assessment tool to holistically capture these overlapping risks, which isolated evaluations inevitably miss. The current practice of using separate, siloed tools is clinically inadequate. Adolescents are often averse to referrals; when directed from one specialist to another (e.g., from oral to mental health services), many disengage due to stigma, cost, or mistrust, leading to fragmented care and missed intervention opportunities (36, 37). A unified OMSRH tool streamlines this process by enabling a “one-stop shop” assessment. This adolescent-friendly approach minimizes referral attrition, maximizes healthcare utilization, and is especially vital in resource-limited settings like Nigeria. By identifying co-occurring risks early, it facilitates the design of holistic interventions that address shared root causes, ultimately improving health outcomes and aligning with global strategies for integrated, adolescent-centered care (37).
There is currently no integrated instrument that measures these three areas of adolescents’ health despite their interconnectedness. The aim of this study was, therefore, to develop an integrated oral, mental, sexual, and reproductive health assessment tool for adolescents that will facilitate an inclusive and dynamic understanding of adolescent health in Nigeria.
Methods
Study design
A three-phased, nine-step mixed-methods approach proposed by Boateng et al. (36) was adopted for this study. This current study reports on the first of the three phases: conceptualization and item generation. The summary of the tool development process is presented in Figure 1.
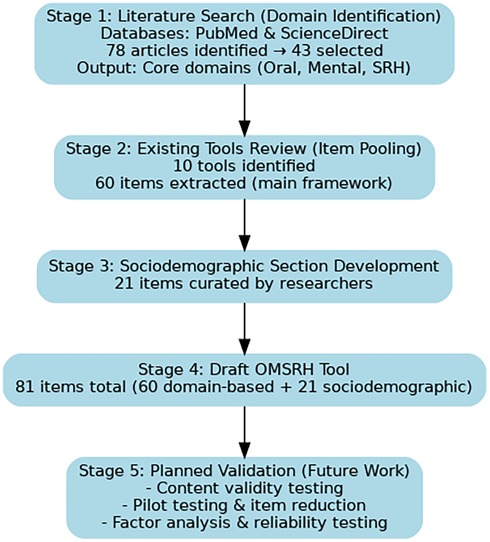
Figure 1. Flowchart summarizing the OMSRH tool development process.
Domain identification
The study employed a systematic literature review framework, using a pre-defined and structured approach to identify and analyze relevant articles. The three key dimensions to be measured—oral health, mental health, and sexual and reproductive health—were defined a priori. A literature search was then conducted in PubMed and ScienceDirect to systematically identify articles or tools that conceptualized the measurement of these domains in English. There were no date restrictions. The identified articles were examined through thematic analysis to extract information on domains and subscales.
Articles were included if they addressed the conceptualization or measurement of at least one of the three dimensions and were designed for general health assessment in apparently healthy populations rather than for specific illnesses or unique contexts. Articles were excluded if they did not address any of the three dimensions or if they were highly specific to particular diseases or specialized populations.
A total of 78 articles were retrieved, with their full texts downloaded and reviewed for relevance. Of these, 12 articles were excluded for not addressing any of the three health dimensions, while 23 articles were excluded for being non-generic, as they were designed for specific illnesses or contexts. These were deemed unsuitable because the proposed tool aims to assess health among an apparently healthy adolescent population. Ultimately, 43 articles (38–80) were included in the study, and the domains and subscales statistically associated with any of the three key health dimensions were adopted for further development of the health assessment tool.
Item generation
Next, the deductive method, also known as logical partitioning (81, 82), was used to identify items for the domains and subscales for the assessment tool. This approach to item generation in instrument design involves developing items based on existing theories, frameworks, or established concepts. Researchers first define the constructs they intend to measure and then generate items that align with these predefined concepts (81, 82). This method ensures theoretical consistency and validity, as items are directly linked to well-established literature and models. It is commonly used in structured assessments, ensuring that the instrument accurately reflects the intended constructs. However, it may limit the discovery of new dimensions not covered by prior theories (83).
Item compilation
The measurement items were derived from validated tools and empirical studies, with most maintaining their original response scales, while a few were adjusted. The selected tools were those validated for use with adolescents in Nigeria, enhancing the likelihood that the measurement meets the five essential characteristics for ensuring the quality of construct measurement: consistent understanding, consistent administration or communication to respondents, clear communication of what constitutes an adequate answer, access to the information necessary for accurate responses, and respondents’ willingness to provide the correct answers required by the question at all times (83–87). Additional socio-demographic questions were formulated for the background section.
The preliminary questionnaire was then drafted, organizing pooled and formulated items into five sections: socio-demographics, oral health, mental health, sexual and reproductive health, and health service utilization.
Results
These 43 included articles were only used to identify appropriate domains through which the dimensions of interest would be measured. Existing validated and unvalidated tools relevant to the domains identified from these articles were then reviewed, and items for the tool were generated from these. The existing tools identified at this stage include both globally recognized and validated ones, like GHQ-12, the Rosenberg self-esteem scale, PHQ-9, GAD-7, as well as unvalidated ones used in empirical studies among adolescents in Nigeria (23–25, 34, 43). Most items were retained verbatim, while some were rephrased. For clarity and cultural appropriateness to the Nigerian adolescent context. A summary of findings is presented in Table 1. The findings from the literature review are divided into oral health, mental health, and sexual and reproductive health.
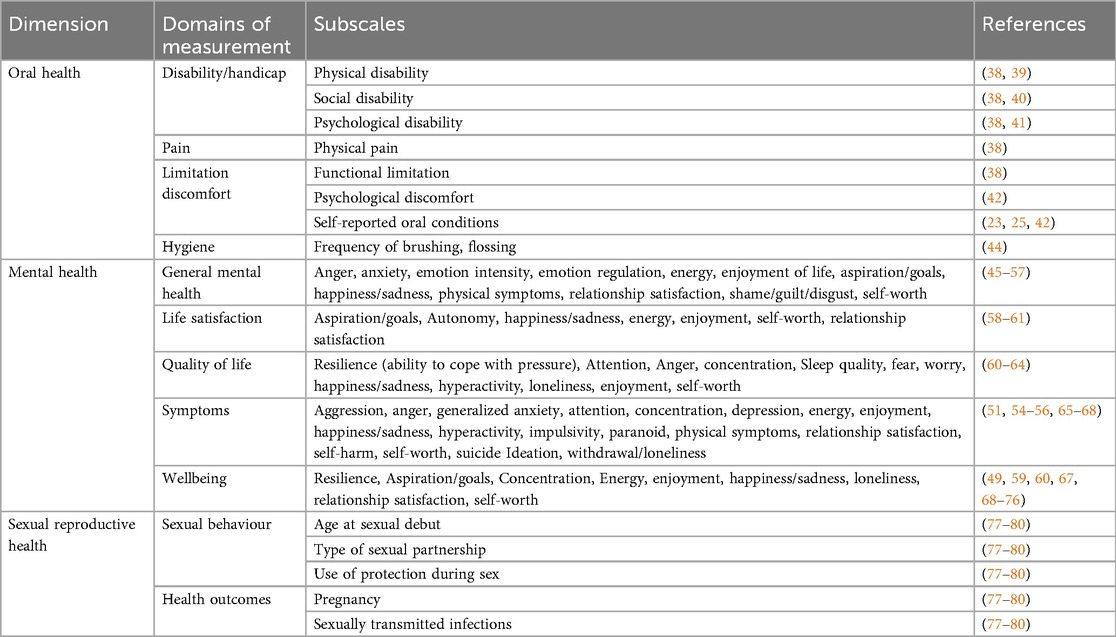
Table 1. Summary of literature on domains for measuring oral, mental, and sexual reproductive health.
Oral health
The literature review identified four key measurement domains (disability/handicap, pain, limitations/discomfort, and hygiene) and eight subscales. Physical, social, and psychological disabilities were recognized as essential subscales for understanding the broader impact of oral health conditions (38–41). Pain was primarily measured as physical pain (38), while functional limitations (38), psychological discomfort (42), and personal experiences of oral health problems (23, 25, 43) were measures of limitations/discomfort. In addition, providing insight into oral hygiene behaviours, such as frequency of brushing and flossing (44), was highlighted as a preventive indicator.
The oral health domain was structured around self-reported oral conditions, functional limitations, hygiene practices, diet, and self-reported health status, as identified in the review. The literature emphasized disability (physical, social, psychological), pain, and hygiene behaviours such as tooth brushing and flossing (38–41, 43, 44). In addition, dietary habits, particularly the frequency of refined sugar consumption, were recognized as significant factors influencing oral health (42, 43).
Mental health
The review identified five measurement domains, emphasizing a multi-faceted approach to measuring mental health: general mental health, life satisfaction, quality of life, symptoms, and overall well-being. General mental health assessment includes emotional regulation, anxiety, anger, energy levels, self-worth, and relationship satisfaction (45–58). Life satisfaction was associated with autonomy, aspirations, and happiness (58–60), while quality of life incorporated resilience, attention, concentration, and sleep quality (59–61). Mental health symptoms, such as aggression, depression, anxiety, hyperactivity, impulsivity, and suicidal ideation, were identified as critical factors influencing adolescent health (51, 54–70). In addition, well-being was linked to resilience, aspirations, self-worth, and social relationships, aligning with broader mental health and quality of life frameworks. These frameworks include the Physical, Mental and Social Well-being Scale (PMSW-21) (50), the Life Orientation Test for optimism (60), the WHOQOL-SRPB BREF for spiritual and personal beliefs within quality of life (71), the Resilience Scale for Adolescents (READ) (72), the Well-Being Picture Scale (73), the Subjective Vitality Scale (74), the SPF-IL scale of social production functions (75), and the Questionnaire for Eudaimonic Well-Being (QEWB) (76).
For mental health, the literature highlighted general mental health indicators, including anger, anxiety, self-worth, and energy levels, which formed the basis for subscales such as ability to concentrate, worry, and confidence (45–58). Mental health symptoms, particularly depression, anxiety, and suicidal ideation, were cited as critical indicators of adolescent well-being (50, 54–58). Furthermore, mental health risk factors, such as tobacco use, alcohol consumption, psychoactive substance use, and self-esteem, were integrated based on their strong association with adolescent mental health outcomes (51, 60, 73–76).
Sexual and reproductive health
The literature review categorized sexual and reproductive health into sexual behaviour and health outcomes. Sexual behaviour includes key indicators such as age at sexual debut, type of sexual partnerships, and use of protection during sex, which are essential for assessing risk behaviors and preventive practices (77–80). Health outcomes focus on pregnancy and sexually transmitted infections (STIs), reflecting critical consequences of sexual behaviors among adolescents (77–80).
The sexual and reproductive health domain was guided by studies focusing on sexual behaviour and health outcomes. The review emphasized age at sexual debut, type of sexual partnerships (including multiple and transactional partnerships), and condom use, which were included as essential subscales (78, 79). In addition, sexually transmitted infections (STIs) were identified as a critical health outcome, reflecting the risks associated with adolescent sexual behaviours (78, 80).
Item measures
Based on the findings from the literature review, Table 2 outlines the final domains and subscales selected for the OMSHR Assessment Tool. The measurement items were derived from validated tools and empirical studies, with most maintaining their original response scales, while a few were adjusted. The selected tools were those validated for use with adolescents in Nigeria, enhancing the likelihood that the measurement meets the five essential characteristics for ensuring the quality of construct measurement: consistent understanding, consistent administration or communication to respondents, clear communication of what constitutes an adequate answer, access to the information necessary for accurate responses, and respondents’ willingness to provide the correct answers required by the question at all times (80–87). Additional socio-demographic questions were formulated for the background section. The preliminary questionnaire was then drafted, organizing pooled and formulated items into five sections: socio-demographics, oral health, mental health, sexual and reproductive health, and health service utilization.
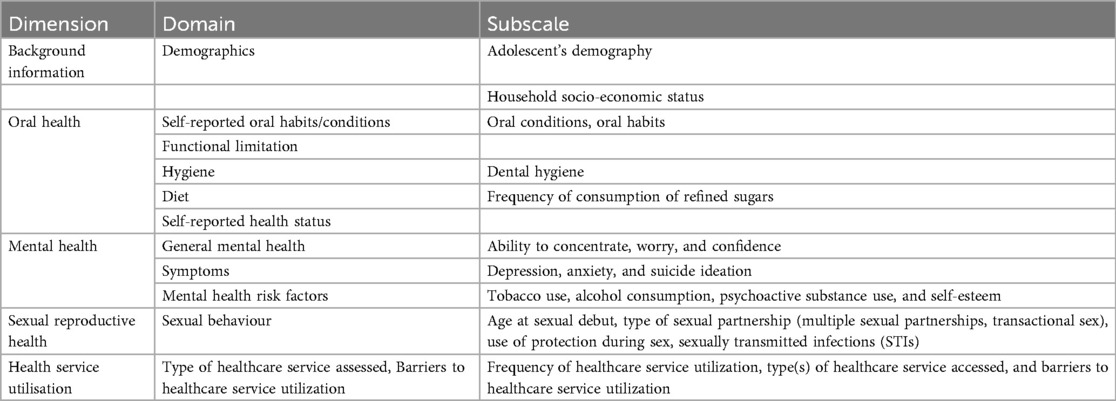
Table 2. Selected domains and subscales for the oral, mental, sexual, and reproductive health assessment tool.
Socio-demographics
This section aims to gather background information and family structure details. It includes personal data such as age, date of birth, gender identity, height, weight, school enrollment status, type of school, class (for in-school adolescents), education level, and occupation (for out-of-school adolescents). Most questions are open-ended, except for the secondary school type, which uses a four-point scale (Public Day, Public Boarding, Private Day, Private Boarding) to assess family socio-economic status. The second part focuses on family structure and socio-economic background.
Oral health
Oral health was evaluated across five domains: self-reported oral health habits, functional limitation, oral hygiene, diet, and self-reported oral health status. Oral habits are indicators of physical oral health status and indicators of potential manifestations of co-occurring mental health issues; thus, they can capture overlapping vulnerabilities and provide a more holistic assessment of adolescent well-being. Self-reported oral health habits were assessed by asking whether participants engaged in any of eight behaviours that could impact oral health or overall well-being—digit or finger sucking, tongue sucking, tongue thrusting, lip sucking, lip biting, nail biting, object biting, and bruxism, with responses recorded on a dichotomous (yes/no) scale (25). Responses are on a dichotomous (yes/no) scale.
Functional limitation was evaluated with three items. The first item asked whether participants faced challenges performing any of the five mouth functions, with responses on a dichotomous (yes/no) scale. The second item asked respondents to rate the health status of their teeth, lips, tongue, oral mucosa, and jaws using a 5-point Likert scale, ranging from “excellent” to “poor.” The third item asked how much their overall life had been negatively affected by conditions of these oral parts, with responses on a 5-point Likert scale from “not at all” to “very much” (25).
Oral hygiene was assessed with one item that asked how often participants brushed their teeth. Item response is on a 5-response continuum ranging from “never or irregular” to “more than once a day” (23–25).
Diet was also assessed with an item that inquired about the frequency of consumption of sugar-containing snacks or drinks between main meals. Item response is also on a 5-response continuum ranging from “about 3or more times a day” to “occasionally, not every day” (23–25).
Self-reported oral health status involved asking about ten common oral health problems –tooth holes, tooth sensitivity, bleeding gums, bad breath, fractured or discoloured teeth, painful teeth, mouth ulcers, missing teeth, and no tooth problems, also rated on a dichotomous scale (yes/no), with the item and scale modified from (25).
Mental health
Mental health was assessed through four domains: psychological distress, depression, generalized anxiety, and suicide ideation, chosen for their relevance to adolescents’ experiences.
Psychological distress was measured using the 12-Item General Health Questionnaire (GHQ-12), which includes items about recent experiences such as concentration, sleep, decision-making, and overall emotional well-being (55). The GHQ-12 is widely used to screen for mental health issues among different populations, both people with underlying medical conditions and in apparently healthy people (86–88), and is recognized for its unidimensional measure of psychological distress (89–91). The tool has been validated for use in Nigeria (92, 93), both in clinical and community settings. Studies in Nigeria (88, 94) have reported high internal consistency for the GHQ-12, with Cronbach's alpha values ranging from 0.78 to 0.92, indicating strong reliability. The optimal cutoff score for detecting psychological distress varies but commonly falls between 3 and 4 (92, 93). To assess its concurrent validity, the GHQ-12 was validated against structured clinical interviews such as the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders (DSM) Disorders (SCID), showing good sensitivity and specificity in detecting psychological distress (92). Its sensitivity rates are above 85% (92) and specificity around 80%–90% (92, 93), indicating that the GHQ-12 is a reliable screening tool in Nigerian settings.
Depression was measured with items from the Patient Health Questionnaire (PHQ-9) (95), which assesses symptoms like lack of interest, sleep disturbances, low energy, and feelings of worthlessness. Responses are rated on a four-point scale, ranging from “not at all” to “nearly every day.” The PHQ has been validated for use in Nigeria in both clinical (among stroke patients (93) and community settings among university students (96). Studies have reported high Cronbach's alpha values (≥ 0.80) (96, 97), indicating strong internal consistency and reliability. This suggests that the PHQ-9 items are measuring the same construct (depression) consistently across respondents. Its test-retest reliability also demonstrated good stability over time in Nigerian samples, with high correlation coefficients (r = 0.80) in repeated measures (97). Factor analysis to assess its construct validity also confirmed a one-factor structure, aligning with the core concept of depression (96).
Generalized anxiety was measured with the GAD-7 scale, which includes items on nervousness, excessive worry, difficulty relaxing, and irritability, also rated on a four-point scale (98). Studies that assessed the psychometric properties of the GAD in Nigerian populations were not found.
Suicide ideation was assessed using the Suicide Behaviours Questionnaire—Revised (SBQ-R), which includes questions on lifetime and past-year suicidal thoughts, attempts, and the likelihood of future attempts (99, 100). The psychometric properties of the SBQ-R were tested among a population of students in tertiary institutions (101). The SBQ-R has shown strong construct validity among Nigerian respondents, through significant positive correlations with the HADS-Anxiety and Depression subscales, and the GHQ-12 (101). Cronbach's alpha for the SBQ-R items was 0.80. Receiver Operating Characteristics curve evaluation suggests that the best cut-off total score with the optimal sensitivity (0.882), specificity (0.875), and highest accuracy (0.879) was 8 in terms of identifying the students at high risk of suicide (101).
In addition, the tool evaluated mental health risk factors, including alcohol consumption, smoking, and psychoactive substance use, as well as self-esteem. Self-esteem was measured using the Rosenberg Self-Esteem Scale, which consists of ten statements about self-worth, with responses on a 4-point Likert scale to minimize response bias (56, 102).
Sexual reproductive health
The tool assesses sexual reproductive health in two domains: sexual behaviour and health outcomes. Sexual behaviour is evaluated through lifetime experience of sexual intercourse, age at sexual debut, circumstances surrounding it, forms of intercourse (anal, vaginal, oral), and types of sexual engagement (transactional, multiple partnerships) in the past 12 months. It also measures the frequency of condom use during consensual sex and the protection used against sexually transmitted infections (STIs) in the last sexual encounter. The health outcome domain includes the incidence of STIs in the past six months and self-rated sexual health status, assessed on a six-point scale: Excellent, Good, Fair, Poor, Very Poor, and Don’t Know. The part of the tool was derived from the National HIV and AIDS and Reproductive Health Survey (NARHS) (103).
Health service utilisation
The tool assessed health service utilization with two domains—types of healthcare service accessed and the barriers to utilization of healthcare service. The type of healthcare service assessed was measured with two items. The first item asked participants when they visited any of the healthcare professionals listed last time. Healthcare professionals listed in the item response are dentists, general practitioners, psychiatrists, and psychologists (25). Barriers to healthcare service utilization were measured with one item that asked participants for reasons why they have not visited any of the identified healthcare professionals in the past 6 months (25).
An 81-item tool was developed to assess adolescents’ oral, mental, and sexual reproductive health, comprising five sections. Section one includes 21 questions on socio-demographic variables. Section two evaluates mental health through four constructs: psychological distress (12 questions), depression (9 questions), generalized anxiety (8 questions), and suicide ideation (4 questions), along with six questions on mental health risk factors—alcohol, tobacco, and psychoactive substance use, and self-esteem. Section three addresses sexual and reproductive health with 11 questions covering sexual activity, age at sexual debut, types of sexual intercourse (oral, vaginal, or anal), sexual partnerships (multiple, transactional, heterogenous, gay/lesbian, others), condom use, sexual outcomes (STI incidence), and self-rated sexual health status. Section four assesses oral health through eight questions on oral hygiene, self-reported oral problems, oral habits, and functional limitations. Section five contains two questions on health service utilization, including general, dental, and psychiatric care. The instrument, which is currently at the conceptualization stage and has not been validated, can be found in Supplementary File 1.
Table 3 discusses the suggested scoring criteria for the instrument. The tool assesses adolescent well-being across mental health, sexual and reproductive health, and oral health, with sociodemographic and service utilization sections used only for descriptive stratification and not scored. Overall scores range from about 55 to 247, but interpretation relies on the profile of scores within domains rather than the composite number. The Mental Health Domain (44–180) is the most detailed, covering psychological distress (10–40), depressive symptoms (9–36), anxiety (7–28), suicidal ideation (4–16), risk behaviors (5–20), and self-esteem (10–40). Severity is graded, with high scores indicating greater problems, except for self-esteem, where higher is better. Notably, a score ≥3 on any suicidal ideation item requires urgent referral. The Sexual and Reproductive Health Domain uses risk indices rather than clinical cut-offs. Key measures include the Composite Sexual Risk Index, contraception/condom use (0–5, higher = riskier), and transactional sex/multiple partners (0–12, higher = greater vulnerability). Scores reflect relative levels of risk across behaviors. The Oral Health Domain (0–33) balances protective and risk factors: oral conditions (0–9, higher = more problems), hygiene habits (0–12, higher = better practices), diet/sugary snacks (0–4, higher = more risk), self-rated oral health (0–4, higher = poorer perception), and functional limitation (0–4, higher = more impairment). By synthesizing across domains, adolescents can be classified as low risk (normal scores throughout), moderate risk (mild to moderate severity in at least one domain), or high risk (severe findings in any domain, such as high suicidal ideation, severe depression/anxiety, extreme sexual health risk, or very poor oral health). High-risk profiles indicate the need for urgent and comprehensive intervention.
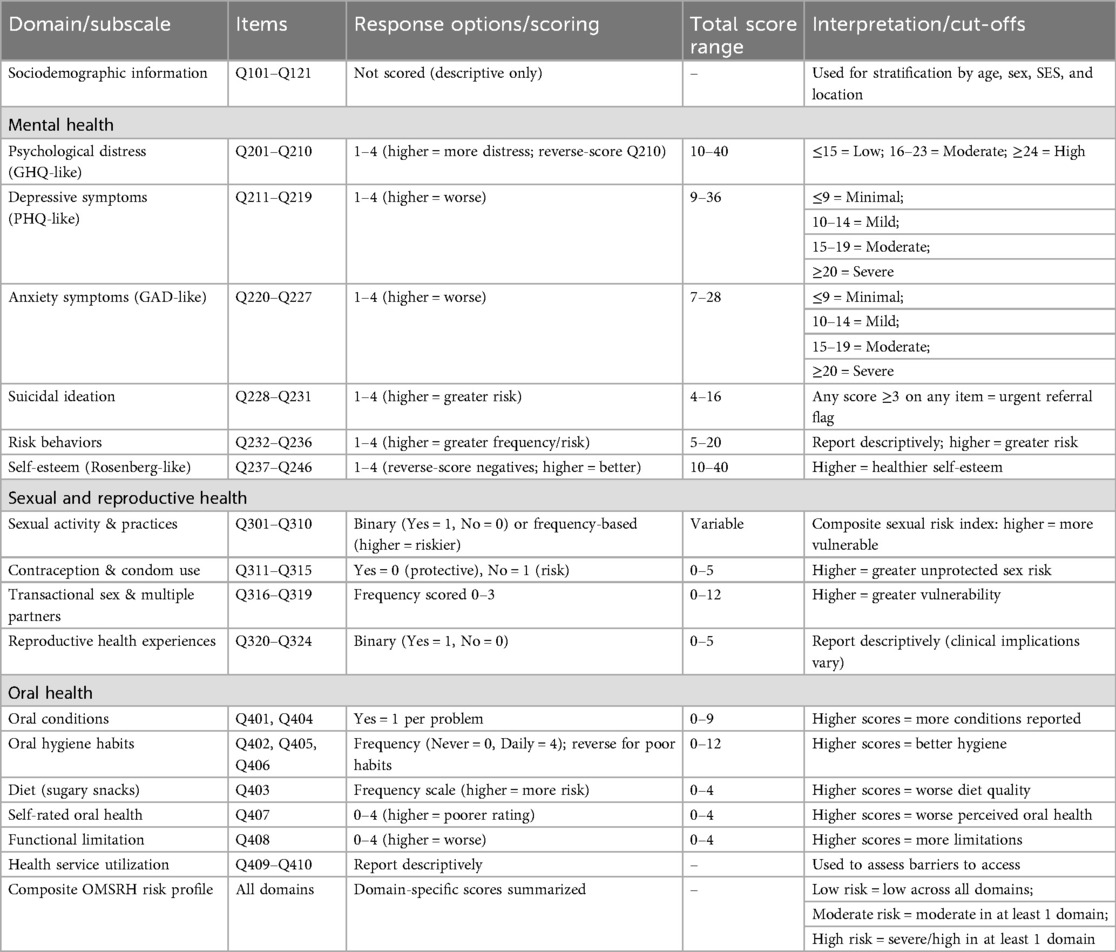
Table 3. Scoring framework for the OMSRH tool.
Discussion
The study aimed to develop an integrated tool to assess oral, mental, and sexual reproductive health (OMSRH) among adolescents, addressing the interconnectedness of these health domains. The outcome was the creation of an 81-item tool divided into five sections, capturing a comprehensive picture of adolescent health by incorporating validated items from existing instruments and newly formulated questions. This tool represents a significant step toward integrating health assessments for adolescents, which could facilitate better service delivery and research in this population.
One of the strengths of the current study is that the tool measures multiple related dimensions of adolescent health, including socio-demographics, mental health, sexual and reproductive health, oral health, and health service utilization. This holistic approach ensures that the interconnectedness of these health domains is captured, which is crucial for understanding adolescent well-being. In addition. many items in the tool were adapted from well-established instruments, reducing the risk of construct underrepresentation (104) and construct-irrelevant variance (105) that can lead to the invalidation of the tool (106, 107). This enhances the tool's credibility and ensures that the constructs being measured are grounded in prior research. The tool also includes both dichotomous and Likert-scale response options, allowing for flexibility in measuring different constructs. The Likert-type response scales with five points have higher reliability, and are appropriate for use with the unipolar items measured in the instrument (108). This adaptability makes it suitable for diverse adolescent populations and various research settings. Furthermore, by combining oral, mental, and sexual reproductive health into a single tool, the instrument has the potential to streamline health assessments and promote integrated service delivery for adolescents, particularly in resource-limited settings like Nigeria.
Despite the study limitations, the development of this tool opens up multiple potential for improving adolescent health outcomes. The tool is still in the first phase of development. While the items have been generated and organized, the tool has not yet undergone content validation, cognitive interviews, or pilot testing. This means that its reliability and validity have not been established for any context or any population. Future steps for validation are discussed, enabling the tool to serve as a foundation for integrated health interventions that address the interconnected health needs of adolescents. The tool could also facilitate empirical research that explores the relationships between these health domains, providing valuable insights into the factors that influence adolescent well-being. Although the 81-item tool is also currently long, it is anticipated that the validation of this comprehensive item pool would lead to a shorter, more parsimonious, yet psychometrically sound instrument.
To realize this potential, the next steps should involve refining and validating the tool. This will include conducting a content validity and logical validity assessment, where an expert panel reviews the tool to confirm that the items are relevant, clear, and comprehensive. This process helps identify any gaps or redundancies in the tool, ensuring it accurately measures the intended constructs (106–111), while also providing preliminary evidence of the instrument's construct validity (112–116). In addition, conducting cognitive interviews with adolescents about the tool will help refine the tool's clarity, ensure that the questions are easily understood by the target population, improve the tool's usability, and reduce response bias (117, 118).
Furthermore, the developed tool needs to be pilot tested with a small sample of adolescents to evaluate its reliability using statistical measures such as Cronbach's alpha and Intraclass Correlation Coefficient (119, 120). This will provide initial insights into the tool's internal consistency and stability (110, 111, 114, 116). The tool's construct validity still needs to be determined through factor analysis and criterion analysis. Factor analysis will help confirm the tool's underlying structure, while criterion analysis will assess how well the tool correlates with other established measures of adolescent health (113–115).
Based on the findings from the pilot test and validity assessments, revisions should be made to refine the tool (113, 120). Following this, a large-scale validation study would be conducted to confirm the tool's reliability and accuracy across diverse adolescent populations. A minimum of 300–450 is recommended (121–123). Efforts would be made to reduce the number of items without compromising the tool's comprehensiveness—only parsimonious, functional, and internally consistent items would be ultimately included (116). This will enhance its practicality and ease of administration in real-world settings (124).
Finally, the tool needs to be evaluated through dimensionality testing (125–128) and confirmatory factor analysis (122, 126, 128) on a new sample. The finalized items from these tests can be used to generate scale scores for substantive analysis (82, 90). In addition, reliability (112, 114, 129) and tool validity (113–115, 130) assessments must be conducted. If the tool is to be applied in different cultural contexts, further adaptation may be required to ensure its relevance and appropriateness. This could involve modifying certain items or response options to better align with the cultural norms and health perceptions of the target population (131). This first version of the OMSRH tool has been intentionally designed as a health status, self-report instrument, suitable for use across diverse adolescent settings (schools, community centers, hospitals, and youth programs).
Conclusion
The OMSRH is a newly designed tool that marks the first step in systematically measuring the oral, mental, sexual, and reproductive health needs of adolescents, thereby promoting an integrated approach for managing the critical health needs of adolescents. Its holistic approach, use of validated items, and potential for integrated service delivery make it a valuable resource for assisting in improving adolescent health outcomes. However, further development and validation are necessary to confirm its reliability and validity. Following further validation testing, this tool can serve as a powerful instrument for research, policy, and practice, ultimately contributing to better health and well-being for adolescents in Nigeria and beyond.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
OA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. AC: Validation, Writing – review & editing. AD: Validation, Writing – review & editing. RO: Validation, Writing – review & editing. SI: Validation, Writing – review & editing. NS-A: Project administration, Validation, Writing – review & editing. ME: Project administration, Validation, Writing – review & editing. AS: Validation, Writing – review & editing. GE: Validation, Writing – review & editing. JL: Validation, Writing – review & editing. OE: Project administration, Resources, Supervision, Validation, Writing – review & editing. MF: Conceptualization, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by the Oral Health Initiative, Centre for Reproduction and Population Health Studies, Nigeria Institute of Medical Research, grant number NM-ADJGT-22-0082-OHI/COH2024/0004.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. ChatGPT for used for grammar check.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issue please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/froh.2025.1592482/full#supplementary-material
References
1. UNICEF (2024). Adolescents. Available online at: https://data.unicef.org/topic/adolescents/overview/ (Accessed December 16, 2024).
2. Agarwal S, Maheshwari AK, Jindal M, Rastogi P. Study of Adolescent Stage and Its Impacts on Adolescents. (n.d.). Available online at: https://www.researchgate.net/publication/362646945 (Accessed September 17, 2025).
3. Kim ES, Wilkinson R, Okuzono SS, Chen Y, Shiba K, Cowden RG. Positive affect during adolescence and health and well-being in adulthood: an outcome-wide longitudinal approach. PLoS Med. (2024) 21(4):e1004365. doi: 10.1371/journal.pmed.1004365
4. Kankaanpää A, Tolvanen A, Heikkinen A, Kaprio J, Ollikainen M, Sillanpää E. The role of adolescent lifestyle habits in biological aging: a prospective twin study. Elife. (2022) 11:e80729. doi: 10.7554/eLife.80729
5. Wiium N, Breivik K, Wold B. Growth trajectories of health behaviors from adolescence through young adulthood. Int J Environ Res Public Health. (2015) 12(11):13711–29. doi: 10.3390/ijerph121113711
6. McDade TW, Chyu L, Duncan GJ, Hoyt LT, Doane LD, Adam EK. Adolescents’ expectations for the future predict health behaviors in early adulthood. Soc Sci Med. (2011) 73(3):391–8. doi: 10.1016/j.socscimed.2011.06.005
7. Folayan MO, Adeniyi AA, Oziegbe EO, Fatusi AO, Harrison A. Integrated oral, mental, and sexual health management for adolescents: a call for professional collaboration. Int J Adolesc Med Health. (2018) 30(3). doi: 10.1515/ijamh-2016-0060
8. Folayan MO, Sam-Agudu NA, Adeniyi A, Oziegbe E, Chukwumah NM, Mapayi B. A proposed one-stop-shop approach for the delivery of integrated oral, mental, sexual, and reproductive healthcare to adolescents in Nigeria. Pan Afr Med J. (2020) 37:1–12. doi: 10.11604/pamj.2020.37.172.22824
9. Rebelo MAB, Rebelo Vieira JM, Pereira JV, Quadros LN, Vettore MV. Does oral health influence school performance and school attendance? A systematic review and meta-analysis. Int J Paediatr Dent. (2019) 29(2):138–48. doi: 10.1111/ipd.12441
10. WHO (2022), Oral Health Nigeria 2022 country profile available at downloaded 15 December 2024. Available online at: https://www.who.int/publications/m/item/oral-health-nga-2022-country-profile (Accessed September 17, 2025).
11. Okolo CC, Oredugba FA, Denloye OO, Adeyemo YI. Dental caries prevalence, severity, and pattern among male adolescents in Kano, Nigeria. J West Afr Coll Surg. (2022) 12:88–93. doi: 10.4103/jwas.jwas_101_22
12. Centre for Research, Evaluation Resources and Development (CRERD), Bayero University Kano (BUK), The Bill & Melinda Gates Institute for Population and Reproductive Health at The Johns Hopkins Bloomberg School of Public Health. Performance Monitoring and Accountability 2020 (PMA2020) Survey Round 4, PMA2017/Nigeria-R4 (National). Nigeria, Baltimore, MD: The Bill & Melinda Gates Institute for Population and Reproductive Health at The Johns Hopkins Bloomberg School of Public Health (2017).
13. Abiodun MT, Omoigberale AI, Ibadin MO. Current practice of adolescent preventive services among paediatric residents in Nigeria. South Afr J Child Health. (2016) 10(2):108. doi: 10.7196/SAJCH.2016.v10i2.717
14. National Bureau of Statistics (NBS). Nigeria Multiple Indicator Cluster Survey 2011 Main Report. Abuja: National Bureau of Statistics (NBS) (2011).
15. Ogbonna PN, Iheanacho PN, Ogbonnaya NP. Prevalence of mental illness among adolescents (15–18 years) treated at federal neuropsychiatric hospital, Enugu, Nigeria, from 2004 to 2013. Arch Psychiatr Nurs. (2020) 34:7–13. doi: 10.1016/j.apnu.2019.12.008
16. Babasola KM, Okhiria A, Bale SI, Srounke TA, Alli U. Prevalence of mental illness among youths in Ogun state, south west Nigeria. UMYU Scientifica J. (2024) 3:63–70. doi: 10.56919/usci.2431.007
17. Abubakar-Abdullateef A, Adedokun B, Omigbodun O. A comparative study of the prevalence and correlates of psychiatric disorders in almajiris and public primary school pupils in Zaria, northwest Nigeria. Child Adolesc Psychiatry Ment Health. (2017) 11:29. doi: 10.1186/s13034-017-0166-3
18. Stanley N, Chinwe ES. Prevalence of mental disorders in Abakaliki, Ebonyi state, southeastern Nigeria. J Am Psychiatr Nurses Assoc. (2022) 28:306–18. doi: 10.1177/1078390320951910
19. Kumbet SJ, Oseni TIA, Mensah-Bonsu M, Damagum FM, Opare-Lokko EBA, Namisango E, et al. Common adolescent mental health disorders seen in Family Medicine Clinics in Ghana and Nigeria. PLoS One. (2023) 18(11):e0285911. doi: 10.1371/journal.pone.0285911
20. Onyeka IN, Miettola J, Ilika AL, Vaskilampi T. Unintended pregnancy and termination of studies among students in Anambra state, Nigeria: are secondary schools playing their part? Afr J Reprod Health. (2011) 15l:109. PMID: 22590897
21. Aboki H, Folayan MO, Daniel'and U, Ogunlayi M. Changes in sexual risk behavior among adolescents: is the HIV prevention programme in Nigeria yielding results? Afr J Reprod Health. (2014) 18(3 Spec No):109–17. PMID: 26050383
22. Nwabueze SA, Azuike EC, Ezenyeaku CA, Aniagboso CC, Azuike ED, Iloghalu IC, et al. Perception of sexually transmitted infection-preventive measures among senior secondary school students in Nnewi-north local government area, Anambra state, Nigeria. Open J Prev Med. (2014) 4:708–16. doi: 10.4236/ojpm.2014.49080
23. El Tantawi M, Folayan MO, Oginni O, Adeniyi AA, Mapayi B, Yassin R, et al. Association between mental health, caries experience, and gingival health of adolescents in suburban Nigeria. BMC Oral Health. (2021) 21(1):223. doi: 10.1186/s12903-021-01589-x
24. Folayan MO, Arowolo O, Mapayi B, Chukwumah NM, Alade MA, Yassin RH, et al. Associations between mental health problems and risky oral and sexual behaviour in adolescents in a sub-urban community in southwest Nigeria. BMC Oral Health. (2021) 21(1):401. doi: 10.1186/s12903-021-01768-w
25. Folayan MO, El Tantawi M, Oginni O, Oziegbe E, Mapayi B, Arowolo O, et al. Oral health practices and oral hygiene status as indicators of suicidal ideation among adolescents in southwest Nigeria. PLoS One. (2021) 16(2):e0247073. doi: 10.1371/journal.pone.0247073
26. Akinrinde D, Ayeni S, Akande D, Adegbite A. Exploring Common Mental Health Problems among Nigerian Adolescents: Identified Challenges and Recommendations for the Future. Durham, NC: The Center for Policy Impact in Global Health (2024). Available online at: https://centerforpolicyimpact.org/2024/09/03/exploring-common-mental-health-problems-among-nigerian-adolescents-identified-challenges-and-recommendations-for-the-future/ (Accessed September 17, 2025).
27. Fatusi A, Wang W. Multiple sexual partnership mediates the association between early sexual debut and sexually transmitted infection among adolescent and young adult males in Nigeria. Eur J Contracept Reprod Health Care. (2009) 14(2):134–43. doi: 10.1080/13625180802601110
28. Fehintola FO, Fehintola AO, Ogunlaja OA, Akinola SE, Awotunde TO, Ogunlaja IP, et al. Prevalence and predictors of early sexual debut among adolescents in Ogbomoso, Nigeria. Am J Public Health Res. (2018) 6(3):148–54. doi: 10.12691/ajphr-6-3-4
29. Durowade KA, Babatunde OA, Omokanye LO, Elegbede OE, Ayodele LM, Adewoye KR, et al. Early sexual debut: prevalence and risk factors among secondary school students in Ido-ekiti, Ekiti state, south-west Nigeria. Afr Health Sci. (2017) 17(3):614–22. doi: 10.4314/ahs.v17i3.3
30. Akombi-Inyang BJ, Woolley E, Iheanacho CO, Bayaraa K, Ghimire PR. Regional trends and socioeconomic predictors of adolescent pregnancy in Nigeria: a nationwide study. Int J Environ Res Public Health. (2022) 19(13):8222. doi: 10.3390/ijerph19138222
31. Gesinde AM, Nwabueze AC, Angela Okojide OBO. Review of child and adolescent sexual abuse in Nigeria: implications for 21st century counsellors. Cov Int J Psychol. (2020) 5(1):71–86. Available online at: https://journals.covenantuniversity.edu.ng/index.php/cijp/article/view/2102 (Accessed December 16, 2024).
32. Palomer T, Ramírez V, Ortuño D. Relationship between oral health and depression: data from the national health survey 2016–2017. BMC Oral Health. (2024) 24:188. doi: 10.1186/s12903-024-03950-2
33. Tiwari T, Kelly A, Randall CL, Tranby E, Franstve-Hawley J. Association between mental health and oral health status and care utilization. Front Oral Health. (2022) 2:732882. doi: 10.3389/froh.2021.732882
34. Folayan MO, El Tantawi M, Yassin R, Arowolo O, Sam-Agudu NA. Sexual health risk indicators and their associations with caries status and gingival health of adolescents resident in sub-urban south-west Nigeria [version 2; peer review: 1 approved, 2 approved with reservations]. AAS Open Research. (2024) 5:7. doi: 10.12688/aasopenres.13301.2
35. Hill B, Mugayar LRF, da Fonseca MA. Oral health implications of risky behaviors in adolescence. Dent Clin North Am. (2021) 65(4):669–87. doi: 10.1016/j.cden.2021.06
36. Coyle RM, Lampe FC, Miltz AR, Sewell J, Anderson J FRCP, Apea V, et al. Associations of depression and anxiety symptoms with sexual behaviour in women and heterosexual men attending sexual health clinics: a cross-sectional study. Sex Transm Infect. (2019) 95(4):254–61. doi: 10.1136/sextrans-2018-053689
37. Duby Z, McClinton Appollis T, Jonas K, Maruping K, Dietrich J, LoVette A, et al. “As a young pregnant girl… the challenges you face”: exploring the intersection between mental health and sexual and reproductive health amongst adolescent girls and young women in South Africa. AIDS Behav. (2021) 25(2):344–53. doi: 10.1007/s10461-020-02974-3
38. Brennan DS, Spencer AJ. Dimensions of oral health related quality of life measured by EQ-5D+ and OHIP-14. Health Qual Life Outcomes. (2004) 2:35. doi: 10.1186/1477-7525-2-35
39. Gift HC, Atchison KA, Dayton CM. Conceptualizing oral health and oral health-related quality of life. Soc Sci Med. (1997) 44(5):601–8. doi: 10.1016/s0277-9536(96)00211-0
40. Moreno SF, Tsakos G, Brealey D, Boniface D, Needleman I. Development of a tool to assess oral health-related quality of life in patients hospitalised in critical care. Qual Life Res. (2020) 29(2):559–68. doi: 10.1007/s11136-019-02335-1
41. Aranza D, Nota A, Galić T, Kozina S, Tecco S, Peričić TP, et al. Development and initial validation of the oral health activities questionnaire. Int J Environ Res Public Health. (2022) 19(9):5556. doi: 10.3390/ijerph19095556
42. Linton MJ, Dieppe P, Medina-Lara A. Review of 99 self-report measures for assessing well-being in adults: exploring dimensions of well-being and developments over time. BMJ Open. (2016) 6:e010641. 10.113627388349
43. El Tantawi M, Folayan MO, Bhayat A. Oral health Status and practices, and anthropometric measurements of preschool children: protocol for a multi-African country survey. JMIR Res Protoc. (2022) 11(4):e33552. doi: 10.2196/33552
44. Sbricoli L, Bernardi L, Ezeddine F, Bacci C, Di Fiore A. Oral hygiene in adolescence: a questionnaire-based study. Int J Environ Res Public Health. (2022) 19(12):7381. doi: 10.3390/ijerph19127381
45. Lin PI, Srivastava G, Beckman L, Kim Y, Hallerbäck M, Barzman D, et al. A framework-based approach to assessing mental health impacts of the COVID-19 pandemic on children and adolescents. Front Psychiatry. (2021) 12:655481. doi: 10.3389/fpsyt.2021.655481
46. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. (1965) 12:63–70. doi: 10.1001/archpsyc.1965.01720310065008
47. Ryff CD, Keyes CLM. The structure of psychological well-being revisited. J Pers Soc Psychol. (1995) 69:719–27. doi: 10.1037//0022-3514.69.4.719
48. Grossi E, Groth N, Mosconi P. Development and validation of the short version of the psychological general well-being index (PGWB-S). Health Qual Life Outcomes. (2006) 4:88. doi: 10.1186/1477-7525-4-88
49. Vaingankar JA, Subramaniam M, Chong SA. The positive mental health instrument: development and validation of a culturally relevant scale in a multi-ethnic Asian population. Health Qual Life Outcomes. (2011) 9:92–92. doi: 10.1186/1477-7525-9-92
50. Supranowicz P, Paz M. Holistic measurement of well-being: psychometric properties of the physical, mental, and social well-being scale (PMSW-21) for adults. Rocz Panstw Zakl Hig. (2014) 65:251–8. PMID: 25247806
51. Wardenaar KJ, van Veen T, Giltay EJ, de Beurs E, Penninx BWJH, Zitman FG. Development and validation of a 30-item short adaptation of the mood and anxiety symptoms questionnaire (MASQ). Psychiatry Res. (2010) 179:101–6. doi: 10.1016/j.psychres.2009.03.005
52. Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, et al. The Warwick-Edinburgh mental well-being scale (WEMWBS): development and UK validation. Health Qual Life Outcomes. (2007) 5:63. doi: 10.1186/1477-7525-5-63
53. Vella-Brodrick DA, Allen FC. Development and psychometric validation of the mental, physical, and spiritual well-being scale. Psychol Rep. (1995) 77:659–74. doi: 10.2466/pr0.1995.77.2.659
55. Goldberg D, Williams P. Users’ guide to the general health questionnaire. Tidsskrift for Den Norske Legeforening. (1989) 109(13):1391–4. PMID: 3597327
56. Schiaffino KM. Other measures of psychological well-being: the affect balance scale (ABS), general health questionnaire (GHQ-12), life satisfaction index-A (LSI-A), Rosenberg self-esteem scale, satisfaction with life scale (SWLS), and state-trait anxiety Index (STAI). Arthritis Care Res. (2003) 49:S165–S74. doi: 10.1002/art.11408
57. Black L, Panayiotou M, Humphrey N. Measuring general mental health in early-mid adolescence: a systematic meta-review of content and psychometrics. JCPP Adv. (2022) 3(1):e12125. doi: 10.1002/jcv2.12125
58. Pavot W, Diener E, Suh E. The temporal satisfaction with life scale. J Pers Assess. (1998) 70(2):340–54. doi: 10.1207/s15327752jpa7002_11
59. Kahneman D, Krueger AB. Developments in the measurement of subjective well-being. J Econ Perspect. (2006) 20:3–24. doi: 10.1257/089533006776526030
60. Scheier MF, Carver CS, Bridges MW. Distinguishing optimism from neuroticism (and trait anxiety, self-mastery, and self-esteem): a reevaluation of the life orientation test. J Pers Soc Psychol. (1994) 67:1063–78. doi: 10.1037//0022-3514.67.6.1063
61. Orth Z, Moosajee F, Van Wyk B. Measuring mental wellness of adolescents: a systematic review of instruments. Front Psychol. (2022) 13(1):835601. doi: 10.3389/fpsyg.2022.835601
62. Ventegodt S, Merrick J, Andersen NJ. Measurement of quality of life III. From the IQOL theory to the global, generic SEQOL questionnaire. SciWorld J. (2003) 3:972–91. doi: 10.1100/tsw.2003.77
63. Henrich G, Herschbach P. Questions on life satisfaction (FLZ M): a short questionnaire for assessing subjective quality of life. Eur J Psychol Assess. (2000) 16:150–9. doi: 10.1027/1015-5759.16.3.150
64. Frisch MB, Cornell J, Villanueva M, Retzlaff PJ. Clinical validation of the quality of life inventory. A measure of life satisfaction for use in treatment planning and outcome assessment. Psychol Assess. (1992) 4(1):92–101. doi: 10.1037/1040-3590.4.1.92
65. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
66. Joseph S, Linley PA, Harwood J. Rapid assessment of well-being: the short depression-happiness scale (SDHS). Psychol Psychother. (2004) 77:463–78. doi: 10.1348/1476083042555406
67. Van Dam NT, Earleywine M. Validation of the center for epidemiologic studies depression scale—revised (CESD-R):pragmatic depression assessment in the general population. Psychiatry Res. (2011) 186:128–32. doi: 10.1016/j.psychres.2010.08.018
68. World Health Organisation (WHO). Wellbeing Measures in Primary Health Care: The DEPCARE Project. Copenhagen: WHO Regional Office for Europe (1998). Available online at: https://iris.who.int/bitstream/handle/10665/349766/WHO-EURO-1998-4234-43993-62027-eng.pdf (Accessed September 17, 2025).
69. Keyes CLM. Subjective well-being in mental health and human development research worldwide: an introduction. Soc Indic Res. (2006) 77(1):1–10. doi: 10.1007/s11205-005-5550-3
70. Clarke A, Friede T, Putz R, Ashdown J, Martin S, Blake A. Warwick-Edinburgh mental well-being scale (WEMWBS): validated for teenage school students in England and Scotland. A mixed methods assessment. BMC Public Health. (2011) 11:487. doi: 10.1186/1471-2458-11-48
71. Skevington SM, Gunson KS, Connell O, A K. Introducing the WHOQOL-SRPB BREF: developing a short-form instrument for assessing spiritual, religious, and personal beliefs within quality of life. Qual Life Res. (2013) 22:1073–83. doi: 10.1007/s11136-012-0237-0
72. Kelly Y, Fitzgerald A, Dooley B. Validation of the resilience scale for adolescents (READ) in Ireland: a multi-group analysis. Int J Methods Psychiatr Res. (2017) 26:e1506. doi: 10.1002/mpr.1506
73. Gueldner SH, Michel Y, Bramlett MH. The well-being picture scale: a revision of the index of field energy. Nurs Sci Q. (2005) 18:42–50. doi: 10.1177/0894318404272107
74. Ryan RM, Frederick C. On energy, personality, and health: subjective vitality as a dynamic reflection of well-being. J Pers. (1997) 65:529–65. doi: 10.1111/j.1467-6494.1997.tb00326.x
75. Nieboer A, Lindenberg S, Boomsma A, Van Bruggen AC. Dimensions of well-being and their measurement: the SPF-IL scale. Soc Indicators Res. (2005) 73:313–53. doi: 10.1007/s11205-004-0988-2
76. Waterman AS, Schwartz SJ, Zamboanga BL. The questionnaire for eudaimonic well-being: psychometric properties, demographic comparisons, and evidence of validity. J Posi Psychol. (2010) 5:41–61. doi: 10.1080/17439760903435208
77. Runtz M. Development of a Measure of Women’s Reproductive and Sexual Health: The Reproductive Health Scale (RHQ). Ottawa: University of Victoria (2007). Available online at: https://www.researchgate.net/publication/237227026
78. Cleland J, Ingham R, Stone N. Asking Young People About Sexual and Reproductive Behaviours: Illustrative Core Instruments. Geneva: WHO (2001). Available online at: https://cdn.who.int/media/docs/default-source/hrp/adolescents/sample-core-instruments.pdf (Accessed: 17 September 2025).
79. Danaux J, Hart J, Desai S, Green X, Nyame-Mireku A, Rutledge J, et al. Sexual and Reproductive Wellbeing (SRWB) Measure Development Strategy. Washington, DC: Coalition to Expand Contraceptive Access (CECA), New Orleans, LA: National Birth Equity Collaborative (NBEC), San Francisco, CA: Person-Centered Reproductive Health Program (2023). p. 1–12.
80. Ahmed F, Ahmad G, Brand T, Zeeb H. Key indicators for appraising adolescent sexual and reproductive health in south Asia: international expert consensus exercise using the Delphi technique. Glob Health Action. (2020) 13(1):1830555. doi: 10.1080/16549716.2020.1830555
81. Boateng GO, Neilands TB, Frongillo EA, Melgar-Quiñonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health. (2018) 6:149. doi: 10.3389/fpubh.2018.00149
82. Hinkin TR. A brief tutorial on the development of measures for use in survey questionnaires. (1998). Available online at: http://scholarship.sha.cornell.edu/articles/521 (Accessed September 17, 2025).
83. Sinclair S, Jaggi P, Hack TF, McClement SE, Cuthbertson L. A practical guide for item generation in measure development: insights from the development of a patient-reported experience measure of compassion. J Nurs Meas. (2020) 28(1):138–56. doi: 10.1891/JNM-D-19-00020
84. Fowler FJ Jr. Improving Survey Questions: Design and Evaluation. Thousand Oaks, CA: Sage Publications (1995).
85. Hinkin TR. A review of scale development practices in the study of organizations. J Manage. (1995) 21(5):967–88. doi: 10.1016/0149-2063(95)90050-0
86. Bejar II. Recent development and prospects in item generation. In: Embretson SE, editor. Measuring Psychological Constructs: Advances in Model-based approaches. Washington, DC: American Psychological Association (2010). p. 201–26. doi: 10.1037/12074-009
87. Kalkbrenner MT. A practical guide to instrument development and score validation in the social sciences: the MEASURE approach. Pract Assess Res Eval. (2021) 26(1). doi: 10.7275/svg4-e671
88. Anjara SG, Bonetto C, Van Bortel T, Brayne C. Using the GHQ-12 to screen for mental health problems among primary care patients: psychometrics and practical considerations. Int J Ment Health Syst. (2020) 14:62. doi: 10.1186/s13033-020-00397-0
89. Wojujutari AK, Idemudia ES, Ugwu LE. The evaluation of the general health questionnaire (GHQ-12) reliability generalization: a meta-analysis. PLoS One. (2024) 19(7):e0304182. doi: 10.1371/journal.pone.0304182
90. Mayhew E, Stuttard L, Beresford B. An assessment of the psychometric properties of the GHQ-12 in an English population of autistic adults without learning difficulties. J Autism Dev Disord. (2021) 51(4):1093–106. doi: 10.1007/s10803-020-04604-2
91. Lee B, Kim YE. Factor structure of the 12-item general health questionnaire (GHQ-12) among Korean university students. Psychiatry Clin Psychopharmacol. (2020) 30(3):248–53. doi: 10.5455/PCP.20200518112914
92. Makanjuola VA, Onyeama M, Nuhu FT, Kola L, Gureje O. Validation of short screening tools for common mental disorders in Nigerian general practices. Gen Hosp Psychiatry. (2014) 36(3):325–9. doi: 10.1016/j.genhosppsych.2013.12.010
93. Audu AI, Sheikh TL, Olisah TO, Amedu MA. Validity of the use of GHQ-12 in primary health care settings in northern Nigeria. J Med Basic Sci Res. (2021) 2(2):51–5. doi: 10.5281/zenodo.5810816
94. Comotti A, Fattori A, Greselin F, Bordini L, Brambilla P, Bonzini M. Psychometric evaluation of GHQ-12 as a screening tool for psychological impairment of healthcare workers facing COVID-19 pandemic. Med Lav. (2023) 114(1):e2023009. doi: 10.23749/mdl.v114i1.13918
95. Spitzer RL, Kroenke K, Williams JBW. Brief Patient Health Questionnaire. Washington, DC: American Psychological Association (1999). doi: 10.1037/t06166-000
96. Adewuya AO, Ola BA, Afolabi OO. Validity of the patient health questionnaire (PHQ-9) as a screening tool for depression amongst Nigerian university students. J Affect Disord. (2006) 96(1-2):89–93. doi: 10.1016/j.jad.2006.05.021
97. Okeafor IN, Okeafor CU. PHQ-9 diagnostic accuracy and optimal cut-off for depression among patients with stroke in Nigeria. Ann Ib Postgrad Med. (2023) 21(1):11–6. PMID: 37528812
98. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166(10):1092–7. doi: 10.1001/archinte.166.10.1092
99. Aprigio I, Gauer G. Suicidal behaviors questionnaire-revised: adaptation and psychometric properties of the Brazilian version. Death Stud. (2024):1–10. doi: 10.1080/07481187.2024.2421963
100. Rueda-Jaimes GE, Castro-Rueda VA, Rangel-Martínez-Villalba AM, Corzo-Casasadiego JD, Moreno-Quijano C, Camacho PA. Validity of the suicide behaviors questionnaire-revised in patients with short-term suicide risk. Eur J Psychiatry. (2017) 31(4):145–50. doi: 10.1016/j.ejpsy.2017.09.002
101. Aloba O, Ojeleye O, Aloba T. The psychometric characteristics of the 4-item suicidal behaviors questionnaire-revised (SBQ-R) as a screening tool in a non-clinical sample of Nigerian university students. Asian J Psychiatr. (2017) 26:46–51. doi: 10.1016/j.ajp.2017.01.017
102. Rosenberg M. Rosenberg Self-Esteem Scale (RSES). Washington, DC: American Psychological Association (1965). doi: 10.1037/t01038-000
103. Federal Ministry of Health [Nigeria]. National HIV & AIDS and Reproductive Health Survey, 2012 (NARHS Plus). Abuja, Nigeria: Federal Ministry of Health (2013).
104. Spurgeon SL. Evaluating the unintended consequences of assessment practices: construct irrelevance and construct underrepresentation. Meas Eval Couns Dev. (2017) 50(4):275–81. doi: 10.1080/07481756.2017.1339563
105. Downing SM. Threats to the validity of locally developed multiple-choice tests in medical education: construct-irrelevant variance and construct underrepresentation. Adv Health Sci Educ Theory Pract. (2002) 7(3):235–41. doi: 10.1023/a:1021112514626
106. Stuhlsatz M. A framework of construct-irrelevant variance for contextualized constructed response assessment. Front Educ. (2021) 6:751283. doi: 10.3389/feduc.2021.751283
107. Strauss ME, Smith GT. Construct validity: advances in theory and methodology. Annu Rev Clin Psychol. (2009) 5:1–25. doi: 10.1146/annurev.clinpsy.032408.153639
108. Joshi A, Kale S, Chandel S, Pal DK. Likert scale: explored and explained. Br J Appl Sci Technol. (2015) 7(4):396–403. doi: 10.9734/BJAST/2015/14975
109. Almanasreh E, Moles R, Chen TF. Evaluation of methods used for estimating content validity. Res Social Adm Pharm. (2019) 15(2):214–21. doi: 10.1016/j.sapharm.2018.03.066
110. Zamanzadeh V, Rassouli M, Abbaszadeh A, Majd HA, Nikanfar A, Ghahramanian A. Details of content validity and objectifying it in instrument development. Nurs Pract Today. (2014) 1(3):163–71. Available online at: https://scispace.com/pdf/details-of-content-validity-and-objectifying-it-in-16hjw67bum.pdf
111. Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Improving the content validity of the mixed methods appraisal tool: a modified e-delphi study. J Clin Epidemiol. (2019) 111:49–59.e1. doi: 10.1016/j.jclinepi.2019.03.008
112. Sürücü L, Maslakçı A. Validity and reliability in quantitative research. BMIJ. (2020) 8(3):2694–726. doi: 10.15295/bmij.v8i3.1540
113. McCrae RR, Kurtz JE, Yamagata S, Terracciano A. Internal consistency, retest reliability, and their implications for personality scale validity. Pers Soc Psychol Rev. (2011) 15(1):28–50. doi: 10.1177/1088868310366253
114. Bolarinwa OA. Principles and methods of validity and reliability testing of questionnaires used in social and health science research. Niger Postgrad Med J. (2015) 22(4):195–201. doi: 10.4103/1117-1936.173959
115. Taherdoost H. Validity and reliability of the research instrument: how to test the validation of a questionnaire/survey in a research. Int J Acad Res Manag. (2016) 5. doi: 10.2139/ssrn.3205040
116. Kimberlin CL, Winterstein AG. Validity and reliability of measurement instruments used in research. Am J Health-Syst Pharm. (2008) 65(23):2276–84. doi: 10.2146/ajhp070364
117. Bogner K, Landrock U. Response biases in standardised surveys. GESIS Survey Guidelines. Mannheim, Germany: GESIS – Leibniz Institute for the Social Sciences (2016). doi: 10.15465/gesis-sg_en_016
118. Balza JS, Cusatis R, McDonnell SM, Basir MA, Flynn KE. Effective questionnaire design: how to use cognitive interviews to refine questionnaire items. J Neonatal Perinatal Med. (2022) 15(2):345–9. doi: 10.3233/NPM-210848
119. Brooks J, Reed DM, Savage B. Taking off with a pilot: the importance of testing research instruments. InECRM2016-Proceedings of the 15th European Conference on Research Methodology for Business Management: ECRM2016 (2016). p. 51–9. Available online at: http://www.academic-bookshop.com/ourshop/prod_4937625-ECRM-2016-15th-European-Conference-on-Research-Methodology-for-Business-and-Management-Studies-London-UK-Print-ISSN-20490968-Print-ISBN.html
120. Hazzi O, Maldaon I. A pilot study: vital methodological issues. Business Theory Prac. (2015) 16(1):53–62. doi: 10.3846/btp.2015.437
121. Gunawan J, Marzilli C, Aungsuroch Y. Establishing appropriate sample size for developing and validating a questionnaire in nursing research. Belitung Nurs J. (2021) 7(5):356–60. doi: 10.33546/bnj.1927
122. Goetz C, Coste J, Lemetayer F, Rat AC, Montel S, Recchia S, et al. Item reduction based on rigorous methodological guidelines is necessary to maintain validity when shortening composite measurement scales. J Clin Epidemiol. (2013) 66(7):710–8. doi: 10.1016/j.jclinepi.2012.12.015
123. Guadagnoli E, Velicer WF. Relation of sample size to the stability of component patterns. Am Psychol Assoc. (1988) 103:265–75. doi: 10.1037/0033-2909.103.2.265
124. Kersting NB, Stevenson PA, Chen M-K. Chapter 6: examining and understanding dimensionality in the context of instrument development: considerations from the classroom video analysis instrument measuring usable teaching knowledge in mathematics. J Res Math Educ. (2016) 15:119–38.
125. Calderón Garrido C, Navarro González D, Lorenzo Seva U, Ferrando Piera PJ. Multidimensional or essentially unidimensional? A multi-faceted factor-analytic approach for assessing the dimensionality of tests and items. Psicothema. (2019) 31(4):450–7. doi: 10.7334/psicothema2019.153
126. Ghiyasvandian S, Matourypour P. Dimensioning the instrumentation: exploratory or confirmatory factor analysis? Rev Bras Enferm. (2017) 70:233–4. doi: 10.1590/0034-7167-2016-0183
127. Morin AJS, Arens AK, Marsh HW. A bifactor exploratory structural equation modeling framework for the identification of distinct sources of construct-relevant psychometric multidimensionality. Struct Equ Model Multidiscip J. (2016) 23:116–39. doi: 10.1080/10705511.2014.961800
128. Tavakol M, Wetzel A. Factor analysis: a means for theory and instrument development in support of construct validity. Int J Med Educ. (2020) 11:245–7. doi: 10.5116/ijme.5f96.0f4a
129. Ögel K, Karadayı G, Şenyuva G, Kanoğlu H. Ergenler için ruhsal sorunlar tarama Ölçeği’nin (ERST) geçerlilik ve güvenilirlik çalışması/the reliability and validity study of psychological screening test for adolescents (PSTA). Dusunen Adam J Psychiatry Neurol Sci. (2012) 25:8–16. doi: 10.5350/dajpn2012250101
130. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16(9):606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
Keywords: adolescents, health screening, assessment tool, oral health, mental health, sexual and reproductive health
Citation: Afolabi OA, Chukwuemeka AN, Dabar AM, Oveh RO, Ibraheem SA, Sam-Agudu NA, El Tantawi M, Salako AO, Eleje GU, Lusher J, Ezechi O and Foláyan MO (2025) Development of the oral, mental, and sexual reproductive health assessment tool for adolescents in Nigeria. Front. Oral Health 6:1592482. doi: 10.3389/froh.2025.1592482
Received: 8 April 2025; Accepted: 26 September 2025;
Published: 30 October 2025.
Edited by:
Temitope Omolehinwa, University of Pennsylvania, United StatesReviewed by:
Pauliana Valéria Machado Galvão, Universidade de Pernambuco, BrazilBruno Špiljak, University of Zagreb, Croatia
Copyright: © 2025 Afolabi, Chukwuemeka, Dabar, Oveh, Ibraheem, Sam-Agudu, El Tantawi, Salako, Eleje, Lusher, Ezechi and Foláyan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Omorinola Adekemi Afolabi, bW9yaW5zb2xhMjAwMUB5YWhvby5jb20=