 Ana Isabel Contreras-Madrid1,2
Ana Isabel Contreras-Madrid1,2 Roshan Melwani-Sadhwani1
Roshan Melwani-Sadhwani1 Rocío Trinidad Velázquez-Cayón1
Rocío Trinidad Velázquez-Cayón1 David Pérez-Jorge3
David Pérez-Jorge3 Juliana Cassol Spanemberg1*
Juliana Cassol Spanemberg1*
- 1Department of Dentistry, Faculty of Health Sciences, Fernando Pessoa Canarias University (UFPC), Gran Canaria, Spain
- 2University of La Laguna, Tenerife, Spain
- 3Department of Didactics and Educational Research, University of La Laguna (ULL) and National Distance Education University (UNED), Tenerife, Spain
Background: The mandibular third molars are the most frequently impacted teeth, followed by their maxillary counterparts and the upper canines. Their retention is influenced by several anatomical and developmental factors, including limited retromolar space, unfavorable angulation, and eruption trajectory—each critical for proper emergence.
Objective: This study examines the association between the eruption or impaction of mandibular third molars and variables such as eruption space, transpalatal width, and eruption angulation.
Materials and methods: Seventy-one mandibular third molars were evaluated using 31 jaw models and 31 orthopantomograms (OPGs). Transpalatal width was measured linearly on the models, while angular data concerning eruption space and direction were derived from the OPGs. Statistical analysis was performed using SPSS (v.25).
Results: Retention was observed in 12.9% of cases. Linear assessments indicated that 51% of the molars were at risk of impaction, contingent on their angulation.
Conclusions: Maxillary constriction significantly increases the risk of mandibular third molar retention. Linear measurements proved more reliable than angular metrics in estimating eruption space. Thus, for diagnosing transverse maxillary discrepancies, linear transpalatal width measurements are preferred over non-metric evaluations.
1 Introduction
The third molars (3M), commonly known as “wisdom teeth”, are the last to erupt, typically between 18 and 24. Their retention rate is approximately 98%, with 78% corresponding to the lower third molars (1–3). A recent systematic review and meta-analysis by Pinto et al. (4), covering 98 studies and 183.828 subjects worldwide, reported a pooled prevalence of impacted third molars at 36.9% per subject and 46.4% per tooth. The study also identified demographic predictors, including a higher prevalence in females than males and a greater incidence of mandibular vs. maxillary impactions, underscoring the global clinical importance of this condition.
Retention of the lower 3M is primarily associated with limited space in the mandibular bone (5–7). This retention may occur asymptomatically or be accompanied by discomfort due to complications such as inflammation and infections in the soft tissues of the oral cavity, including pericoronitis and periodontal disease. Complications affecting deeper structures are often related to dental caries adjacent to the retained molars (8–10). Other recognised pathologies linked to lower 3M retention, such as root resorption, cysts, tumours, and mandibular fractures, frequently cause pain, impair masticatory function, and reduce the quality of life of affected individuals (5, 10–12).
Recent studies have investigated the genetic expression changes following surgical extraction of impacted third molars to better understand postoperative complications. Zhou et al. (13) identified 555 differentially expressed genes in gingival tissues, including those involved in immune response and bone mineralization. These findings offer valuable insights for improving postoperative management, personalizing treatments, and developing novel therapies to minimize inflammation and enhance healing after third molar surgery. Furthermore, Motoc et al. (14) highlighted the significant influence of demographic and biological factors such as age, gender, body mass index, diet, and salivary pH on the prevalence of periodontal pathogenic bacteria in children and adolescents, emphasizing the multifactorial nature of oral health and its potential implications for third molar pathology.
Historically, guidelines and recommendations regarding the extraction vs. retention of mandibular third molars have evolved under the influence of institutions such as the Royal College of Surgeons of England and the National Institutes of Health in the United States, as well as regional bodies like the National Institute for Health and Care Excellence (15). Despite these efforts, the surgical removal of third molars remains controversial due to insufficient evidence supporting routine extraction, particularly in asymptomatic and partially erupted cases. Moreover, the increased incidence of distal surface caries (DSC) in second molars adjacent to impacted third molars has been a focal point of clinical concern and guideline formulation over the past two decades.
The size and morphology of the dental arches, along with the dimensions of the mandibular bone, have been studied to predict lower third molar eruption (16). Although various studies have validated the use of linear and angular measurements to assess the likelihood of lower third molar eruption (17–19), the relationship between trans palatal width, available eruption space (ED), and the degree of angular deviation in the eruption direction of the lower third molars remains unclear.
1.1 Conceptualisation and background
The eruption of the lower third molar (3M) begins with its calcification around the age of 9 and typically concludes between the ages of 20 and 24. This eruption process is influenced by various factors, including race, diet, genetics, insufficient retromolar space, and specific patterns in the growth of the mandibular ramus, all of which may affect the possibility of eruption (20–23). A lack of retromolar space in the mandible, combined with a marked degree of angulation (i.e., the inclination of the eruption axis), may result in impaction against the second molar, thereby causing the third molar to be deflected towards the lingual cortex of the mandible (20).
When analysing the aetiological factors contributing to lower 3M retention (24–26), highlight the importance of mandibular bone growth direction—specifically, the spatial relationship between the anterior border of the mandibular ramus and the distal surface of the lower second molar—as a determinant of available space for third molar eruption. Horizontal mandibular growth, as opposed to vertical growth, tends to generate greater space for eruption, thereby reducing the likelihood of lower 3M retention (Figure 1).
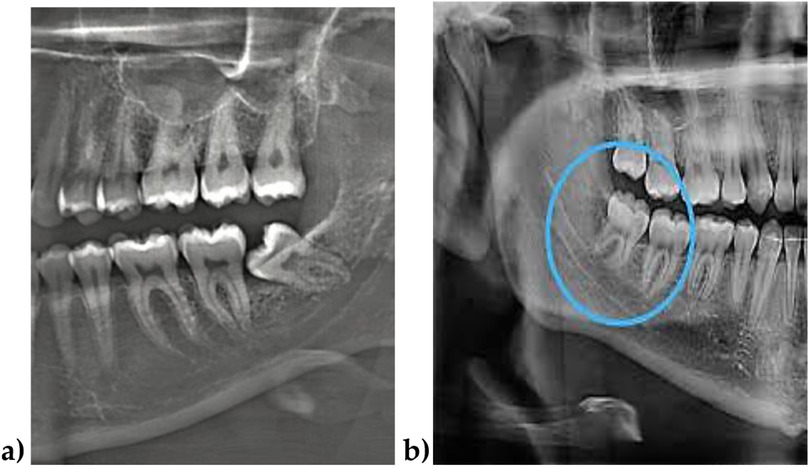
Figure 1. (a) Case with no space for the lower third molar eruption due to a lack of mandibular growth. (b) Case with space available for eruption of the third molar due to mandibular growth. Source: (a): The authors; (b) Dr. Daniel Sepulveda.
Several authors agree that a combination of factors determines the etiology of lower third molar retention. These include bone resorption at the anterior border of the mandibular ramus, increased inclination in the direction of growth, and mesial displacement of the teeth. These factors are crucial in determining the available space and are related to the probability of a successful eruption of the lower third molar. Collante & Lewintre (27), Bareiro & Duarte (24), Puyen (25), and Rodríguez del Toro et al. (26) also maintain that if half of the third molar is within the mandibular bone ramus, the probability of eruption is 50%.
There are several classifications for retained third molars, all of which coincide in evaluating their position and relationship to the ascending ramus of the mandible, the retromolar space available for eruption, the angle of eruption, and the tissue coverage over the retained lower third molar. These classifications are fundamental tools for oral surgeons, as they facilitate an accurate clinical diagnosis and surgical treatment planning, allowing them to predict the extraction difficulty and anticipate possible complications.
Among the most commonly used classifications for third molar (3M) retention are those based on the third molar's position relative to the second molar's longitudinal axis. These classifications consider various factors, such as the depth of 3M impaction, its relationship to the lower second molar, the mesiodistal diameter of the retained 3M crown, and the distance between the lower second molar and the anterior border of the mandibular ramus. They are primarily based on three main factors: the depth and direction of the eruption of the third molar, the number, direction, and morphology of its roots, along with two complementary factors: its relationship to the inferior dental canal and the second molar. All these classifications have proven valuable and reliable tools (6, 7, 28).
Within the clinical assessment and evolution of the 3M retention process, the analysis of radiographic records, such as lateral cephalic radiographs and orthopantomographs (OPG), should consider aspects such as the depth and inclination of the tooth, its relation to the mandibular ramus, root characteristics, and ED (17–19) (Figure 2).

Figure 2. The third molar region will include. Source: The authors.
A recent review study on third molar (3M) eruption prediction highlighted that, among 2,78 patients assessed at a young age, early evaluation reduced the need for invasive treatments, such as surgical extraction in adulthood, and minimised the risk of associated oral diseases, including pericoronitis, infections, and dental caries in the molars adjacent to the retained 3M. This had a positive impact on the long-term oral and general health of children and adolescents (10).
To predict the likelihood of lower 3M eruption, several studies have emphasised the importance of evaluating factors such as the available eruption distance (ED), crown size, and changes in eruption angulation (18, 19). For this purpose, different analytical methods have been developed, involving both linear measurements of the eruption space and angular measurements of the eruption inclination of the lower 3M, using lateral cephalometric radiographs and orthopantomographs (OPG).
Leon (29) and Mummolo et al. (19), conducted studies to predict 3M eruptions based on linear ED measurements. To do this, they traced the occlusal plane. They established two perpendicular lines and two tangents—one to the distal surface of the lower second molar and the other to the anterior edge of the ascending ramus of the mandible. The linear distance between these tangents was termed the available space (AB), while the mesiodistal width of the third molar crown was defined as CD.
These studies agree that when the mesiodistal width of the 3M crown (CD) is less than the available space (AB), the probability of eruption is high. Conversely, when CD exceeds AB, retention becomes more likely. Furthermore, it has been established that eruption is highly probable when the ratio between these two linear measurements (AB/CD) is equal to or greater than 1.
On the other hand, if this ratio is less than 1, the probability of eruption is significantly reduced or even absent (Figure 3).
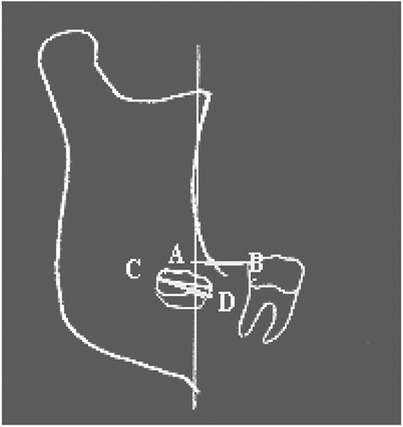
Figure 3. 3M eruption probability. Source: Quiros & Palma (18).
One of the most widely used analytical methods to predict third molar (3M) eruption using linear measurements is the approach proposed by Ganns in 1993. This method determines the available eruption distance (ED). It compares it with the mesiodistal width (MD) of the 3M using the following formula: X = ED/mesiodistal width of the lower 3M, where X represents the probability of eruption and the space available for lower 3M eruption. According to this analysis, when X ≤ 0.7 mm, the eruption of the lower third molar is unlikely; when X is between 0.71 mm and 0.99 mm, the partial eruption is expected; and when X > 1.0 mm, the full eruption is likely.
Other studies have used linear measurements of ED by applying cephalometric landmarks on lateral cephalometric radiographs. Sánchez (30) and Rodríguez et al. (31), employed the cephalometric point Xi, representing the centre of the mandibular ramus, to measure the distance to the distal surface of the second molar, using the occlusal plane as a reference. Their results showed that an ED ranging from 21 mm–29 mm corresponds to partial eruption, whereas distances of 30 mm or more indicate complete eruption of the lower 3M.
In a different approach, Verma et al. (32), Ericsson (33), and Romero et al. (34) combined linear and angular measurements using lateral cephalometric radiographs and orthopantomograms (OPGs) to predict third molar (3M) eruption. Their analysis included linear parameters such as the mesiodistal width of the third molar, the distance between the anterior border of the ascending ramus and the distal surface of the second molar, and the distance from the cephalometric point Xi to the distal surface of the second molar. They also measured the angle of inclination of the third molar relative to its apical base.
In a related study, Kaur et al. (35) indicated that three variables must be considered to reliably predict lower third molar eruption: (a) the linear distance from the distal surface of the second molar to the anterior border of the ascending ramus, which should not be less than 14 mm; (b) the distance from cephalometric point Xi to the distal surface of the second molar, which should be at least 35 mm; and (c) the direction of eruption, measured as the inclination of the third molar relative to the occlusal plane, which should be at least 40°, to ensure a favourable eruption path. These findings are illustrated in Figure 4.

Figure 4. 3M eruption potential. Source: Kaur et al. (35).
Several studies have identified issues related to transpalatal width in the context of maxillary growth and development, which have been described as transverse malocclusions. These are typically classified as unilateral crossbites (UCD) and bilateral crossbites (BCM) (Figures 5, 6).

Figure 5. Unilateral crossbite. Source: The authors.

Figure 6. Bilateral crossbite. Source: The authors.
To determine transpalatal width (36, 37), measured the distance between canines, premolars, and homologous molars on both sides, using as a reference the most vestibular point of the clinical crown of the canines. They established standard measurements of 30.96 ± 1.8 mm between the first premolars, 39.8 ± 2 mm between the second premolars, and 54.36 ± 2.1 mm between the molars. In addition, they measured the cusp-to-cusp distance of the canines, reporting a normative value of 25.3 ± 1.6 mm.
In a complementary study on dental arch development and size, Mayoral & Mayoral (38) and Mosquera (39) proposed one of the most reliable methods for assessing dental arch dimensions and transpalatal width. These authors measured the transpalatal width by recording the distances between the canines, premolars, and molars, using the central fossae of the first and second premolars as reference points, and the homologous first molars on the right and left sides. They established standard values of 35 mm for the distance between the first premolars, 41 mm for the second premolars, and 47 mm for the first molars. More recent studies have adopted these same parameters and measurements in determining transpalatal widths, including the works of Narciandi et al. (40), Rodrígue del Toro et al., (26), and Lozano Villegas (41).
Having reviewed the background of 3M retention and the prediction of its eruption, this study examined the relationship between transpalatal width and the space available for eruption or retention of the lower third molar by analysing linear and angular measurements in 71 molars from 31 patients. The aim was to understand how these variables correlate and to assess their impact on lower 3M retention. The findings of this research, which explore the relationship between jaw dimensions and third molar retention, may be highly relevant for diagnosis, planning, and preventive treatment in dental practice, thereby contributing to improved oral and overall health outcomes for patients.
1.2 Objectives
• Analyse the correlation between lower third molar retention/eruption and predictive variables to determine the relationship between lower third molar retention and/or eruption and various predictive factors, including linear measurements of available mandibular space, maxillary transverse width, and angular parameters influencing eruption direction.
• Assess non-metric indicators of maxillary compression regarding molar retention/eruption: Examine non-metric signs of maxillary compression, such as a narrow or ogival palate, posterior crossbite, protrusion, and dental crowding, to evaluate their potential association with lower third molar retention or eruption.
2 Materials and methods
2.1 Study design
The study was conducted by the Declaration of Helsinki and was approved by the Ethics Committee of CEIBA, University of La Laguna (Protocol code 2,023–3,337). This descriptive study examined the characteristics of lower third molars through linear and angular measurements obtained from OPGs and study models. The analysis integrated radiographic images and plaster models of the jaws to evaluate key anatomical variables associated with third molar retention and eruption.
2.2 Sample
The study comprised thirty-one patients evaluated using thirty-one panoramic radiographs, thirty-one study models, and seventy-one radiographic images of lower third molars.
The sample distribution, categorized by sex and age, is presented in Table 1.

Table 1. Distribution of the sample according to sex and age (n = 31).
2.3 Sample selection criteria
Patients were not randomly selected, but had to meet strict inclusion criteria to ensure the homogeneity of the sample and the validity of the analyses performed. Individuals between 11 and 19 years of age with permanent dentition only, fully developed roots in the lower second molars, and no history of previous dental extractions or orthodontic treatments that could alter the morphology or space available in the mandible were chosen. This selection was justified because the study aimed to analyse the relationship between space available for eruption and retention of lower third molars under representative clinical conditions, minimising the interference of external factors or previous treatments.
In addition, patients with dental anomalies, oral diseases, or radiographs of insufficient quality to ensure the accuracy of linear and angular measurements were excluded. This methodological strategy was necessary so that the results were primarily attributable to the patient's anatomical and functional characteristics, ensuring the reliability and validity of the predictions of lower third molar eruption or retention.
This was a retrospective and exploratory study. Therefore, no formal sample size calculation was conducted. The sample was composed of clinical records, study models, and panoramic radiographs from patients who visited a private dental clinic in Plasencia, Spain, over a four-year period. Participants were selected through non-probabilistic, convenience sampling, and only those who met the inclusion criteria were considered. This approach ensured access to high-quality diagnostic material suitable for evaluating third molar eruption and retention.
2.4 Procedure and data collection
Participants or their legal representatives, in the case of minors under 18 years old, provided informed consent to allow access to medical records, personal and clinical data, panoramic radiographs, and study models. The study was conducted following the guidelines of the Declaration of Helsinki.
The topics were extracted from keywords derived from the research question to ensure rigorous data collection and purification. The most frequent keywords in related studies were initially identified to refine the search for these topics.
The most appropriate search equations were formulated from this stage by combining keywords using Boolean operators (AND, OR). To determine the affinity of studies with the objectives of this research, their relevance and suitability were assessed by reading abstracts and the full texts.
2.4.1 Radiographic procedure
Panoramic radiographs were obtained using a CRANEX OME CEPH radiographic unit (Orion Corporation Sonedex, Finland). According to the manufacturer's specifications, the equipment presents a 30% inherent distortion (expansion) due to the mandible's three-dimensional structure.
2.4.2 Sample classification
Cases were classified by dentition type, including 31 panoramic radiographs from 16 female and 15 male patients. All patients exhibited permanent dentition and met the study selection criteria.
2.4.3 Manual measurements
Measurements were manually taken on study models using a Limit brand digital caliper with automatic shut-off function at 300 mm and 150 mm (manufacturing code 29281201, serial number 001027), compliant with ISO 9001:2000 standards. All measurements adhered to established linear and angular criteria.
To ensure the reliability of the measurements, all linear and angular assessments were conducted by a single trained examiner. To assess intraobserver reliability, 25% of the sample was remeasured after a two-week interval under the same conditions. The intra-class correlation coefficient (ICC) was used to evaluate reproducibility, yielding values above 0.90 for all variables, which indicates excellent reliability.
2.4.4 Maxillary width and palatal morphology analysis
The digital caliper measured the maxillary transpalatal width from the central fossa of the first and second upper premolars to their contralateral counterparts. The intermolar distance between the first upper molars was also evaluated. Standard reference values were:
• First premolars: 35 mm
• Second premolars: 41 mm
• First molars: 47 mm
Measurements below these values indicated maxillary compression.
Palatal morphology was analysed on the models to diagnose maxillary compression or narrowing and to determine the presence or absence of an ogival (V-shaped) palate. Palatal morphology was classified as either ogival (V-shaped) or normal (U-shaped).
2.4.5 Anterior teeth protrusion
The protrusion of the upper anterior teeth was evaluated by measuring the distance (in mm) from the upper incisors' incisal edge to the lower incisors' vestibular surface, with protrusion classified according to the measured distance.
2.4.6 Panoramic radiograph analysis: space and angulation for eruption
All panoramic radiographs were obtained using the same equipment: CRANEX OME CEPH (Orion Corporation Sonedex, Finland). Exposure parameters ranged from 60–90 kV, 4–15 mA, and 10–20 s, depending on individual patient characteristics. The device underwent regular calibration, and geometric accuracy was verified using a phantom model with known dimensions.
Panoramic imaging introduces an estimated 30% horizontal expansion, particularly noticeable in the anterior mandibular region due to its curved anatomy. However, in the posterior (molar) region, this distortion is minimal, thus allowing reliable linear and angular measurements of the third molar.
To assess the available space for eruption or retention of the lower third molar, a line representing the occlusal plane was drawn on the panoramic radiograph. A perpendicular reference line was projected from the most distal point of the crown of the lower second molar. The available space (line AB) was measured from this point to its intersection with the anterior border of the mandibular ramus. Additionally, the mesiodistal width of the third molar crown (line CD) was recorded.
The eruption index (X) was calculated to estimate the probability of lower third molar eruption using the following formula:
where:
• Ed (or AB) is the available space (mm), defined as the linear distance from point A (distal surface of the second molar) to point B (intersection of the occlusal plane with the anterior border of the mandibular ramus).
• MD (or CD) is the mesiodistal crown width of the third molar (mm), measured from point C (distal surface of the third molar crown) to point D (mesial surface of the same crown).
• X represents the eruption index, indicating the probability of eruption.
Interpretation of the index:
• X ≤ 1.0 (0–0.99 mm): No possibility or partial eruption.
• X > 1.0 (≥1 mm): Higher probability of complete eruption.
To summarise these aspects, a summary of the variables considered for the study is presented in Table 2.
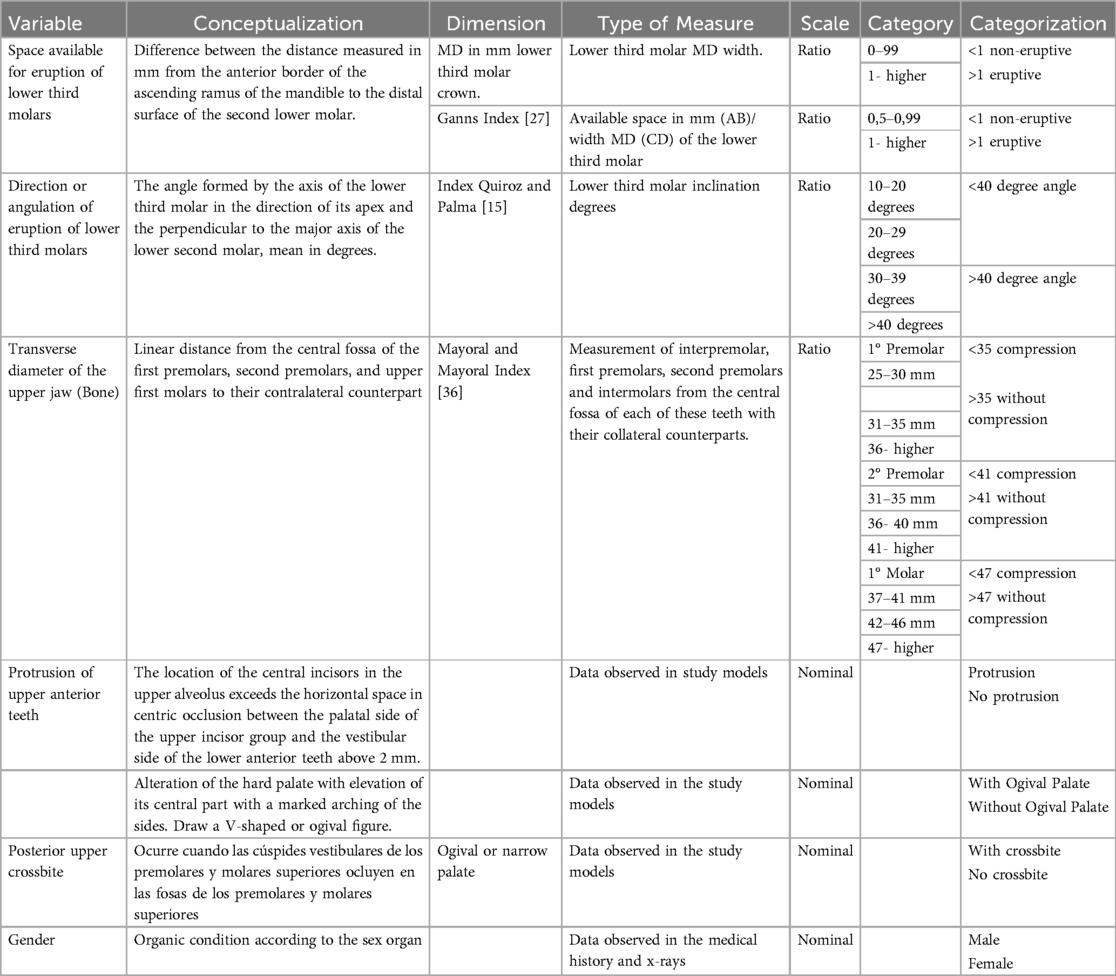
Table 2. Conceptualization and description of the variables of the study.
3 Data processing
3.1 Analysis approach
The data collected from the study models' observations and panoramic radiographs, which were systematically recorded in specially designed tables, underwent comprehensive analysis. This analysis utilised the Statistical Package for the Social Sciences (SPSS), version 25.
3.2 Statistical methods
A range of statistical methods was employed to analyse the data rigorously. Descriptive statistics were used to summarise and interpret the data succinctly. Contingency tables facilitated the exploration of relationships between variables, while the Chi-square test assessed associations and identified potential patterns. This test is instrumental in examining differences in the distributions of categorical variables. Risk estimation techniques were also applied to evaluate the probability of specific outcomes, offering insight into potential risk factors or correlations. Lastly, the COR test was utilized to determine the strength and direction of the relationship between two variables.
4 Results
4.1 Measurements of upper jaw width in plaster models
The initial phase of the analysis focused on determining the transverse width of the upper jaw using plaster models, following established measurements (38).
The results revealed the following average distances: The distance for the upper first premolars averaged 21.8 mm (SD 2.9). The distance for the upper second premolars was 36.7 mm (SD 3). The upper intermolar distance averaged 43.12 mm (SD 3.2).
These measurements offer a comprehensive overview of the transverse dimensions of the upper jaw in the studied sample (Table 3).
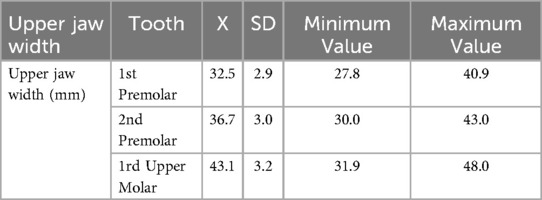
Table 3. Results of upper jaw width measurements (mm).
The results of the upper jaw's transverse skeletal malocclusion were obtained and presented in Table 3. Upon analyzing the variables indicative of maxillary compression (39, 41–43) and considering additional factors such as posterior crossbite, the presence of an ogival palate, and dental protrusion to assess transpalatal and sagittal width, it was found that 83.9% of the upper first premolars exhibited transverse maxillary compression. Moreover, measurements of the second premolars and intermolar distances revealed that 87.1% of the patients displayed maxillary compression. Analysis of the other diagnostic variables for compression revealed that 35.5% of patients had a posterior crossbite, 87.1% exhibited an ogival palate, and 54.8% presented with dental protrusion (Table 4).

Table 4. Diagnosis of maxillary transverse malocclusion by compression or transverse narrowing of the maxilla according to linear measurements of transpalatal width and other non-metric indicators of transverse malocclusion.
A new variable was introduced to assess maxillary compression or narrowing based on the three transpalatal width measurements. If at least one of the three values indicated a positive result, the patient was diagnosed with transpalatal compression or narrowing of the maxilla. Conversely, if all the values were negative, indicating the absence of narrowing, the patient was classified “without compression.” A summary of the measurements regarding the presence of compression or transpalatal narrowing is presented in Table 5. It was found that 90.3% of the cases exhibited compression, while 9.7% did not have compression of the upper jaw.

Table 5. Summary measure of compression or transverse narrowing of the maxilla.
The available space (ED) for the eruption of the third molars was measured using panoramic radiographs. Linear measurements of eruption space (AB) and crown width (CD) were employed to predict molar retention, while angular measurements assessed the direction of eruption of the lower third molars. The AB space measurements averaged 21.8 mm ± 4.3 for the right molars and 21.7 mm ± 3 for the left molars. For the CD measurements, the mean value for the lower right third molar was 15.4 mm ± 3.2, while for the left, it was 13.7 mm ± 9.9. The eruption direction inclination was 38.2° ± 16.8 for the right molars and 31.2° ± 10.8 for the left lower third molars (Table 6).
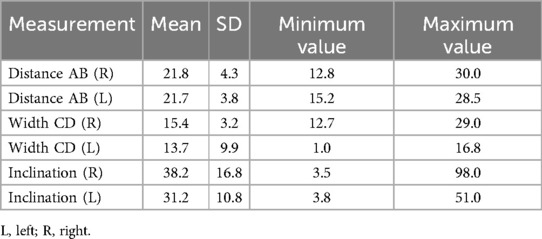
Table 6. The results of the measurements of eruption space (ED), crown width (CD), and eruption inclination of the lower third molar are as follows.
The results also encompassed predictive variables for lower third molar retention, particularly the ratio between available space (AB) and mesiodistal crown width (CD), as well as the eruption angle, which were used to estimate the eruption prognosis. It was observed that, according to eruption space measurements, 13.3% of the patients were likely to retain their lower third molars. Conversely, 50% were expected to retain the molars using molar angulation or inclination measurements, while the remaining 50% were predicted to experience their eruption. These findings suggest that linear measurements of available eruption space may underestimate the diagnosis, whereas angular inclination measurements may overestimate it (Table 7).

Table 7. Prediction of lower third molar eruption with linear and angular method.
Continuing the analysis of retention predictors, linear and angular measurements were employed without distinguishing between right and left molars, yielding the results shown in Table 8.

Table 8. Summary measure of eruption/retention prediction based on linear and angular measurements.
Using the linear measurement method (AB/CD ratio), retention was estimated in 12.9% of patients, whereas the angular method (based on inclination <40°) predicted retention in 51%. These values correspond to different diagnostic indicators, applied independently to the same cohort. The angular method tends to overestimate retention, while the linear approach underestimates it (Table 9).

Table 9. Relationship between the predictive methods of linear space-available and angular measures for retention/eruption of lower third molars as a function of sex.
Regarding the interaction between gender and third molar eruption prognosis, the analysis showed that, based on linear measurements, 12.5% of women were estimated to have a poor prognosis for eruption (i.e., predicted retention), compared to 13.3% of men. Conversely, favorable eruption was projected in 87.5% of women and 86.7% of men, with no significant gender differences (p = 0.72).
The final analysis compared both predictive methods to determine the more accurate predictor of lower third molar retention. The comparison, conducted using the COR (C-statistic) curve, revealed a higher value for the linear measurement method (COR: 0.429) compared to the angular method (COR: 0.399). The area beneath the curve for the linear method was graphically larger, suggesting its superior predictive ability for both retention presence (sensitivity) and absence (specificity) (see Table 9).
Additionally, inter-method comparisons were performed using the Kappa statistical test to assess agreement between the linear and angular measurement methods. The resulting Kappa value of 0.244 indicated a low level of agreement in retention diagnosis. Moreover, a p-value of 0.038 suggested a statistically significant relationship between them (Table 10).
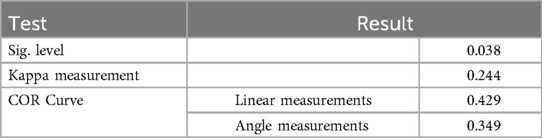
Table 10. Comparison between linear and angular methods. COR and KAPPA curve test.
Based on the compression variable assessed through linear measurements, the predictive values for retention or eruption were not statistically significant. However, in evaluating retention risk, patients with decreased transpalatal width, as measured by the linear method, exhibited a higher risk (RR: 1.13 for narrowing or compression).
Similar results were observed in the angular measurement analysis, where maxillary compression was associated with an increased retention risk (RR: 1.08) compared to RR: 0.46 in non-compressed cases. Additionally, posterior crossbite, assessed using the linear method, was associated with an elevated retention risk (RR: 2.5) (Table 11).
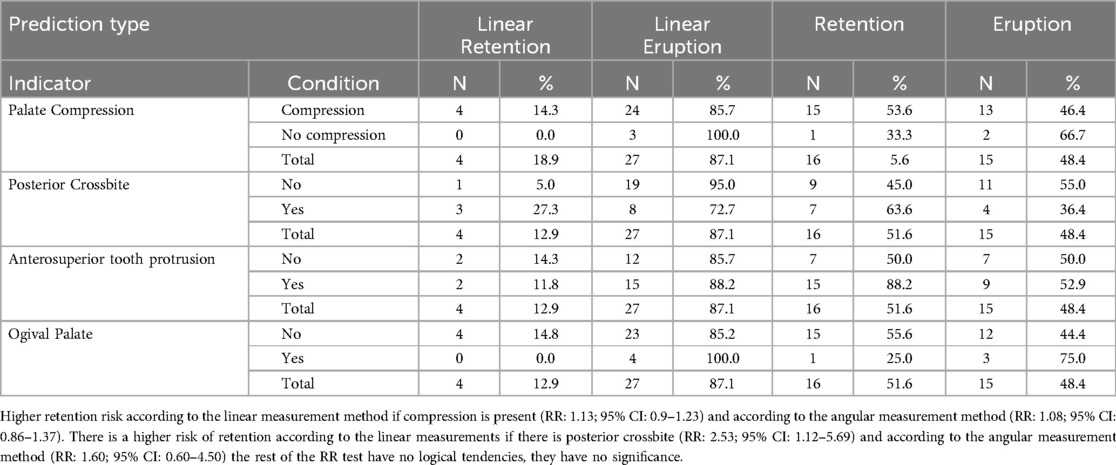
Table 11. Result of the linear indicators of maxillary compression relationship with the retention of the lower third molars.
5 Discussion
The prevalence and management of third molars continue to be a topic of global concern. Meta-analyses report an approximate 37% prevalence of third molars per patient, with higher rates in females and more frequent mandibular impactions (4). These epidemiological insights emphasise the relevance of predictive studies like ours, aimed at identifying factors influencing lower third molar retention and eruption.
Our findings highlight a strong association between reduced transverse maxillary development and the retention of third molars. Specifically, 90.3% of patients presented with maxillary compression and ogival palates, supporting earlier observations by Mayoral & Mayoral (38), González et al. (44), and Rodríguez Del Toro et al. (26). The linear measurements of dental arch width obtained in this study are also consistent with previously reported norms (36, 38), validating the clinical patterns observed.
Early diagnosis has been widely recognized as a cornerstone in the management of third molars, potentially reducing the need for surgical intervention and associated complications (10, 17, 45). Recent molecular advances, such as those by Zhou et al., further enhance our understanding by revealing changes in gene expression in gingival tissues post-extraction, offering novel insights into postoperative care.
Consistent with earlier literature (35, 45), our study confirms that factors such as limited eruption space, molar inclination, and crown size critically affect third molar positioning. The AB/CD ratio proved predictive: values ≥1 indicated a 70% probability of eruption, while ratios <1 significantly lowered this likelihood, mirroring the results of Ganns et al. (46). Eruption inclination angles (average 38.2° and 31.2°) also fell within ranges reported in prior predictive models (19).
A notable finding was the elevated risk of third molar retention in patients with posterior crossbite (RR: 2.5), which aligns with evidence linking vertical growth patterns and the mesial inclination of the third molar crown to an increased retention risk (25–27). These morphological traits are often associated with inadequate mandibular growth and reduced retromolar space, as previously described by Puyen (25), Rodríguez del Toro et al. (26), and Plaza et al. (47). Such anatomical limitations suggest a broader link between third molar retention and skeletal Class II patterns, particularly those with diminished anteroposterior maxillary dimensions (48, 49).
Significantly, while over 80% of our sample showed maxillary compression, this high prevalence limits the generalizability of our findings. The reduced variability in maxillary width may limit the statistical power to detect differences across subgroups. Thus, although a strong correlation was observed, caution should be applied in extending these conclusions to more diverse populations. Future studies should explore these associations in larger and more heterogeneous cohorts.
Lastly, our results support the evolution of clinical approaches to third molar management, advocating for individualized assessment rather than routine extraction. Concerns such as the development of distal surface caries in adjacent second molars remain central to decision-making, reinforcing the importance of early and precise diagnostic evaluation.
6 Limitations
Despite the contributions of this study, several limitations should be considered when interpreting the findings. The sample size may not adequately represent the general population, which constrains the generalizability of the results. Furthermore, the cross-sectional design does not allow for the establishment of causal relationships between predictive variables and third molar retention or eruption. Radiographic evaluations, particularly angular and linear measurements, are susceptible to potential measurement errors, which can impact accuracy. Additionally, the study did not control for relevant confounding variables such as genetic predispositions, environmental influences, or coexisting oral conditions that may affect the eruption process. Another important limitation is the lack of longitudinal follow-up, which restricts insight into the progression of third molar development over time.
Moreover, the assessment of transpalatal width was based exclusively on dental measurements obtained from plaster models. Skeletal parameters, such as those evaluated in Andrews' Element III analysis, were not included due to the retrospective nature of the data and the absence of three-dimensional imaging or articulated models. While dental metrics provide useful clinical information, they may not fully reflect underlying skeletal discrepancies. Future studies should consider integrating skeletal assessments to enhance diagnostic precision.
7 Conclusions
This study presents key findings relevant to the prediction of lower third molar retention and eruption:
• Maxillary compression was observed in 90.3% of patients, with a strong correlation between compressed or ogival palates and molar retention.
• Linear transpalatal measurements proved reliable in identifying transverse maxillary narrowing, in line with previous research.
• The AB/CD ratio emerged as a useful predictor:
○ AB/CD ≥ 1 → ∼70% eruption probability;
○ AB/CD < 1 → increased retention likelihood.
• Angular measurements also supported the prediction of eruption direction or retention.
• Higher retention risk was associated with:
○ Maxillary compression;
○ Posterior crossbite;
○ Upper anterior dental protrusion;
○ Skeletal Class II patterns and insufficient mandibular growth.
• Posterior crossbite, linked with vertical growth and mesial crown inclination, was a particularly strong indicator of retention risk.
Future studies should be designed with larger and more diverse cohorts to improve external validity. Incorporating longitudinal follow-up would provide valuable data on temporal changes in third molar positioning. Moreover, controlling for potential confounding factors and exploring genetic and systemic determinants would enhance the understanding of the multifactorial nature of molar eruption and retention.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by CEIBA/University of La Laguna. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
AC: Supervision, Conceptualization, Writing – review & editing, Funding acquisition, Writing – original draft, Methodology, Project administration, Formal analysis, Investigation, Validation, Data curation. RM: Visualization, Investigation, Validation, Supervision, Writing – original draft, Writing – review & editing, Resources, Data curation. RV: Software, Investigation, Resources, Writing – review & editing, Validation, Formal analysis, Funding acquisition, Methodology. DP: Validation, Writing – review & editing, Data curation, Methodology, Supervision. JC: Funding acquisition, Resources, Formal analysis, Writing – review & editing, Validation, Investigation, Supervision, Data curation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Universidad Fernando Pessoa Canarias (UFPC), which covered the article processing charge (APC).
Acknowledgments
To all study participants and the Fernando Pesssoa Canarias University. This manuscript is part of one of the articles of the doctoral thesis that Ana Isabel Contreras-Madrid is writing at the University of La Laguna, specifically in the Health Sciences program.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. The authors acknowledge using ChatGPT to assist with English translation, enhance coherence, and improve the overall quality of the language, as they are non-native English speakers.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Costa MA, Figueiredo de Oliveira AE, Silva Rd, Ferreira Costa J, Ferreira López F, Lima Rodrigues SA. Prevalencia de terceros molares incluidos en estudiantes de una escuela pública de São Luís - MaranhãoBrasil. Acta Odontol Venez. (2010) 48(4):1–9. Available online at: https://www.actaodontologica.com/ediciones/2010/4/art-17/
2. Hashemipour MA, Tahmasbi-Arashlow M, Fahimi-Hanzaei F. Incidence of impacted mandibular and maxillary third molars: a radiographic study in a Southeast Iran population. Med Oral Patol Oral Cir Bucal. (2013) 18(1):e140. doi: 10.4317/medoral.18028
3. Salcedo Arones N. Posición de terceras molares mandibulares según Winter en pacientes de un centro de salud militar, Ayacucho 2023 [tesis]. Universidad Roosevelt, Ayacucho, Peru (2023). Available online at: http://repositorio.uroosevelt.edu.pe/handle/20.500.14140/1739 (Accessed March 8, 2025).
4. Pinto AC, Francisco H, Marques D, Martins JNR, Caramês J. Worldwide prevalence and demographic predictors of impacted third molars—systematic review with meta-analysis. J Clin Med. (2024) 13(24):7533. doi: 10.3390/jcm13247533
5. Gunst K, Mesotten K, Carbonez A, Willems G. Third molar root development in relation to chronological age: a large sample sized retrospective study. Forensic Sci Int. (2003) 136(1–3):52–7. doi: 10.1016/S0379-0738(03)00263-9
6. Gamarra J, Diaz-Reissner C, Ocampos H, Adorno CG, Fretes V. Frecuencia de la posición, inclinación y grado de dificultad quirúrgica de terceros molares mandibulares en pacientes que acuden a la facultad de odontología de la universidad nacional de Asunción. Mem Inst Investig Ciencias Salud. (2022) 20(1):22–9. doi: 10.18004/mem.iics/1812-9528/2022.020.01.22
7. Guerrero Córdova BR. Estudio radiográfico de terceros molares inferiores retenidos en el cantón quero (Tesis). (2023).
8. Campbell JH. Pathology associated with the third molar. Oral Maxillofac Surg Clin North Am. (2013) 25(1):1–10. doi: 10.1016/j.coms.2012.11.005
9. Cardoso GB, Savegnago GDO, Hirsch WDB, Vizzotto MB, Liedke GS. Pathologic conditions associated with impacted third molars: a retrospective study of panoramic radiographs in a Southern Brazilian population. Imaging Sci Dent. (2023) 53(4):303–12. doi: 10.5624/isd.20230036
10. Contreras-Madrid AI, Sanjuan-Perez AD, Melwuani-Sadhwani R, Mejia-Torrus JL. Derecho a la salud oral de los adolescentes: prevención y detección precoz de la retención de terceros molares. In: Jiménez Hernández-Castillo MI, Catalina S, Silva Rivera L, editors. Educar Para la Felicidad. Madrid: Dykinson (2024). p. 660–72.
12. Contreras-Madrid AI, Sadhwani RNM, Agustín ERA. Promoción y prevención de la salud oral y enfermedades bucodentales en niños y adolescentes. In: Jiménez Hernández AS, Castro Ramírez CJ, Vergara Arboleda M, Chacón Pinilla RS, editors. La escuela promotora de derechos, buen trato y participación: revisiones, estudios y experiencias. Barcelona: Octaedro (2023). p. 383–92.
13. Zhou H, Fu N, Tian Y, Zhang N, Fan Q, Zeng F, et al. Transcriptome sequencing of gingival tissues from impacted third molars patients reveals the alterations of gene expression. Comb Chem High Throughput Screen. (2024) 27(16):2350–65. doi: 10.2174/0113862073256803231114095626
14. Motoc GV, Juncar RI, Moca AE, Motoc O, Vaida LL, Juncar M. The relationship between age, gender, BMI, diet, salivary pH and periodontal pathogenic bacteria in children and adolescents: a cross-sectional study. Biomedicines. (2023) 11(9):2374. doi: 10.3390/biomedicines11092374
15. Toedtling V, Forouzanfar T, Brand HS. Historical aspects about third molar removal versus retention and distal surface caries in the second mandibular molar adjacent to impacted third molars. Br Dent J. (2023) 234(4):268–73. doi: 10.1038/s41415-023-5532-3
16. Cabrera DLP, Alcolea JR, Viltres GP. Longitud normal del cuerpo mandibular y la posible erupción de terceros molares inferiores. Multimed. (2017) 19(3):1–12.
17. Rolseth V, Mosdøl A, Dahlberg PS, Ding Y, Bleka Ø, Skjerven-Martinsen M, et al. Age assessment by Demirjian’s development stages of the third molar: a systematic review. J Forensic Med. (2019) 29(5):2311–21. doi: 10.1016/j.jflm.2019.05.010
18. Quiroz O, Palma A. El tercer molar mandibular, método predictivo de erupción. J Clin Odontol. (1999) 14(1):21–6.
19. Mummolo S, Gallusi G, Strappa EM, Grilli F, Mattei A, Fiasca F, et al. Prediction of mandibular third molar impaction using linear and angular measurements in young adult orthopantomograms. Appl Sci. (2023) 13(7):4637. doi: 10.3390/app13074637
20. Zelic K, Nedeljkovic N. Size of the lower third molar space in relation to age in Serbian population. Vojnosanit Pregl. (2013) 70:923–8. doi: 10.2298/VSP110509017Z
21. Al-Gunaid TH, Bukhari AK, El Khateeb SM, Yamaki M. Relationship of mandibular ramus dimensions to lower third molar impaction. Eur J Dent. (2019) 13(2):213–21. doi: 10.1055/s-0039-1693922
22. Nguyen A, Caplin J, Avenetti D, Durfee S, Kusnoto B, Sciote JJ, et al. A longitudinal assessment of sex differences in the growth of the mandibular retromolar space. Arch Oral Biol. (2022) 143:105547. doi: 10.1016/j.archoralbio.2022.105547
23. Magat G, Akyuz M. Are morphological and morphometric characteristics of maxillary anterior region and nasopalatine canal related to each other? Oral Radiol. (2023) 39(2):372–85. doi: 10.1007/s11282-022-00647-6
24. Bareiro F, Duarte L. Posición más frecuente de inclusión de terceros molares mandibulares y su relación anatómica con el conducto dentario inferior en pacientes del hospital nacional de itauguá hasta el año 2012. Rev Nacional (Itauguá). (2014) 6(1):40–8.
25. Puyen Goicochea EC. Factores asociados a la indicación de exodoncia profiláctica de tercera molar inferior en el tratamiento de ortodoncia, perú-2021 (Tesis). (2023).
26. Rodríguez del Toro M, González Espangler L, Romero García LI, Soto Cantero LA. Validación de un modelo cefalométrico de predicción para el brote de los terceros molares. Rev Cubana Estomatol. (2021) 58(4):e4010. doi: 10.1590/S0034-83762021000400003
27. Collante CI, Lewintre ME. Relación entre terceros molares inferiores retenidos, el apiñamiento dentario tardío anteroinferior con la suma angular del polígono de Björk-Jarabak. Rev Fac Odontol. (2007) 1(1):31–8. Available online at: https://revistas.unne.edu.ar/index.php/rfo/article/view/5142
28. Erdoğdu Ç, Akay G. Relationship between mandibular arch parameters and third molar impaction. Int Dent J. (2024) 74:S64. doi: 10.1016/j.identj.2024.07.763
29. León Ramírez G. Relación entre el espacio del tercer molar inferior y los diferentes patrones esqueléticos en pacientes de 12 a 17 años que acuden al centro odontológico “dental científica”, Lima 2017-2019 (Tesis). (2021).
30. Sánchez Salinas YM. Predicción del espacio para el tercer molar mediante la cefalometría de ricketts [2016 (tesis)]. Huánuco (2017).
31. Rodríguez SG. Normas de medidas e índices odontométricos para el diagnóstico de anomalías dentomaxilofaciales. Universidad de Ciencias Médicas, La Habana (2021).
32. Verma A, Sharma P, Bhatnagar S. Evaluation and prediction of impacted mandibular third molars by panoramic radiography: a retrospective study. Int J Orthod Rehabil. (2017) 8(3):101. doi: 10.4103/ijor.ijor_25_17
33. Ericsson PA. Asociación de las dimensiones anatómicas mandibulares como etiología de la impactación del tercer molar inferior (Tesis). Universidad Nacional de Chimborazo (2021).
34. Jara-Romero CF, Sigcho-Romero CR, Sánchez-Sánchez RJ, Cedeño-Zambrano DA. Relación del biotipo facial y las inclusiones de los terceros molares según la clasificación de Pell y Gregory. Dominio Ciencias. (2023) 9(3):294–320. doi: 10.23857/dc.v9i3.3444
35. Kaur K, Jaiswal A, Shivani , Singh J. Assessment of lower third molar eruption status in different facial growth patterns in adults. J Indian Orthod Soc. (2024) 58(1):47–53. doi: 10.1177/09749098231123456
36. Ricketts RA. A principle of racial growth of the mandible. Angle Orthod. (1972) 42:368–86. doi: 10.1043/0003-3219(1972)042%3C0368:APORGO%3E2.0.CO;2
37. Reyna-Gutierrez J, Aliaga del Castillo A, Marengo-Castillo H, Alvarado-Menacho S. Dimensiones transversales en pacientes con secuela de fisura labio-alveolo-palatina bilateral. Odontol Clín Cient. (2011) 10(2):157–61. doi: 10.1016/j.occ.2011.06.003
38. Mayoral J, Mayoral G. Ortodoncia: Principios Fundamentales y Práctica. Barcelona: Editorial Labor (1969).
39. Mosquera SKZ, Ramos LP, Molina VAN. Dimensión transversal maxilar en adultos clase I esqueletal en tomografía de cráneo completo. Rev Arbitrada Interdiscip Ciencias Salud. (2022) 6(1):614–30. doi: 10.24265/raics.2022.v6n1.03
40. Narciandi OA, Soto Rico A, Cruz Estupiñán D. Expansion orthopedics of maxillary disjunction. Rapid Expansion. Investig Medicoquirúrgicas. (2021) 13(3):1–14. doi: 10.5281/zenodo.5586478
41. Lozano Villegas AG. Cambios radiográficos esqueletales en el maxilar producidos por la Expansión maxilar rápida (Tesis). Universidad Autónoma de Nuevo León (2023).
42. Casma Meneses KA. Concordancia diagnóstica entre el índice vert de ricketts y el índice de proporción facial en la determinación de la tipología facial en pacientes atendidos en la especialidad de ortodoncia y ortopedia maxilar de la universidad privada de Tacna durante los periodos 2012-2014 y 2014-2016 (Tesis). (2017).
43. Ramos Pazos NA, Suazo Galdames IC, Martínez MLM, Reyes L. Relaciones transversales faciales en niños chilenos de la Región del Maule. Int J Morphol. (2007) 25(4):703–7. doi: 10.4067/S0717-95022007000400015
44. González AG, López AF, Fernández ST, Ocampo AM, Valencia JE. Sensibilidad y especificidad de un análisis radiográfico, tomográfico y de modelos digitales en la determinación de discrepancias transversales. Rev Mex Ortod. (2018) 6(1):28–34.
45. Juodzbalys G, Daugela P. Mandibular third molar impaction: review of literature and a proposal of a classification. J Oral Maxillofac Res. (2013) 4(2):e1. doi: 10.5037/jomr.2013.4201
46. Ganns C, Hochban W, Kielbassa AM, Umstadt HE. Prognosis of third molar eruption. Oral Surg Oral Med Oral Pathol. (1993) 76:688–93. doi: 10.1016/0030-4220(93)90384-V
47. Plaza SP, Reimpell A, Silva J, Montoya D. Relationship between skeletal class II and class III malocclusions with vertical skeletal pattern. Dent Press J Orthod. (2019) 24(4):63–72. doi: 10.1590/2177-6709.24.4.063-072.oar
48. Jeevitha J, Thiagarajan A, Sivalingam B. Influence and impact of mandibular ramal dimensions on the incidence of lower third molar impaction: a prospective study. J Pharm Bioallied Sci. (2022) 14(5):364. doi: 10.4103/jpbs.jpbs_232_22
Keywords: retained third molar, transpalatal width, available space, direction of eruption, prediction of third molar retention
Citation: Contreras-Madrid AI, Melwani-Sadhwani R, Velázquez-Cayón RT, Pérez-Jorge D and Cassol Spanemberg J (2025) Influence of linear and angular parameters on lower third molar retention: the role of space allocation and transpalatal width. Front. Oral Health 6:1612527. doi: 10.3389/froh.2025.1612527
Received: 15 April 2025; Accepted: 12 August 2025;
Published: 22 September 2025.
Edited by:
Kitty Jieyi Chen, Sun Yat-sen University, ChinaReviewed by:
Rahela Tabita Moca, University of Oradea, RomaniaMohamed Elkorashie, Suez Canal University, Egypt
Petya Kanazirska, Medical University, Bulgaria
Copyright: © 2025 Contreras-Madrid, Melwani-Sadhwani, Velázquez-Cayón, Pérez-Jorge and Cassol Spanemberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juliana Cassol Spanemberg, amNhc3NvbEB1ZnBjYW5hcmlhcy5lcw==