 Laura Agnes Ingrid Magerfleisch1
Laura Agnes Ingrid Magerfleisch1 Nertsa Cunoti1Rezart Qorri1Katharina Marilena Weil1Hannah Tröger1Juliane Häring1Lisa Irmscher1
Nertsa Cunoti1Rezart Qorri1Katharina Marilena Weil1Hannah Tröger1Juliane Häring1Lisa Irmscher1 Katja Petrowski2
Katja Petrowski2 Hendrik Berth1*
Hendrik Berth1*
- 1Research Group Medical Psychology and Medical Sociology, Division of Psychological and Social Medicine and Developmental Neurosciences, Medical Faculty Carl Gustav Carus, Technische Universität Dresden, Dresden, Germany
- 2Department of Medical Psychology and Medical Sociology, University Medical Center of the Johannes Gutenberg-University Mainz, Mainz, Germany
Background: Dental anxiety is a prevalent phenomenon with the potential to impact both psychological well-being and oral health outcomes. It may lead to individuals avoiding treatment. This study aims to explore the relationship between psychological anxiety symptoms and physical anxiety symptoms in dental anxiety.
Methods: Between 2019 and 2022, a cross-sectional study was conducted including 1,327 patients from a variety of dental practices in Germany and students (age range: 18–85 years; mean: 39.65 years, 60.7% female). Participants completed validated questionnaires, including the Dental Anxiety Scale (DAS), the Scale Somato-visceral arousal of the Dental Fear Survey (DFS-SVA), the Brief Symptom Inventory 18 (BSI-18 GSI), and the Oral Health Impact Profile (OHIP-5). Data was analysed using Mann–Whitney-U-tests, Spearman correlations, Kruskal–Wallis-tests and linear regression models. The significance level was set at p = 0.05.
Results: The mean value for dental anxiety (DAS) was 9.81 (SD = 4.07) and for physical anxiety symptoms (DFS-SVA) 10.51 (SD = 4.70). Of the participants, 808 (60.9%) reported no dental anxiety, 368 (27.7%) were somewhat anxious and 151 (11.4%) reported severe dental anxiety. A strong correlation was observed between DAS and DFS (r = 0.544), while moderate correlations were found between DAS and BSI-18 (r = 0.300) and between DAS and OHIP-5 (r = 0.371). The application of regression analysis indicated that DFS-SVA was the strongest predictor of DAS scores (β = 0.434, p < 0.001), followed by BSI-18 GSI (β = 0.285, p < 0.001) and age (β = 0.174, p < 0.001). Gender was not found to have a significant influence on results. A significant disparity was observed in the results between male and female scores and on the DAS, DFS-SVA, and BSI-18 GSI compared to men.
Conclusion: The study corroborates substantial correlation between psychological dental anxiety and physical anxiety symptoms. These findings underscore the necessity for early detection and targeted interventions within dental practices with the aim of enhancing both oral health and overall quality of life. It is recommended that future research endeavours focus on the investigation of causal relationships and the identification of effective treatment strategies to further enhance patient care.
1 Introduction
Dental anxiety is a prevalent phenomenon characterized by an apprehension of dental treatment. On a global scale, 15.3% of adults experience any form of dental anxiety, while 12.4% of adults demonstrate high dental fear or anxiety. Severe dental anxiety has been observed in 3.3% of adults (1). Dental anxiety is a recognised mental illness that can range from mild discomfort to extreme phobia. It has both psychological and physical implications for the affected (2). The condition is associated with a variety of symptoms. Consequently, patients exhibit a range of physical, cognitive, emotional and behavioural responses (3). The symptoms experienced by these individuals include sleep disorders, constant nervousness and concentration problems (4). Avoidance is the predominant method of coping with dental anxiety, leading to a vicious cycle (5). Deterioration in oral health has been shown to be a contributing factor to an increase in dental anxiety (6). The relationship between dental anxiety and treatment avoidance has far-reaching consequences. Several studies have demonstrated that anxious or phobic patients are more prone to experiencing untreated caries (7–9) and tooth loss (7, 9). In addition to the consequences regarding oral health, these patients may also exhibit a reduced general sense of well-being and a deteriorated quality of life (2). Dentists can mitigate levels of dental anxiety through the implementation of behavioural interventions (10, 11). It is therefore vital to recognise dental anxiety at the earliest opportunity. The manifestation of symptoms associated with physical dental anxiety may facilitate this process.
There are established instruments for measuring dental anxiety, such as the Dental Anxiety Scale (DAS) (12–14) and the Dental Fear Survey (DFS) (12). The Somato-visceral arousal of the DFS is an instrument that provides additional information on avoidance behaviour and physical reactions (15).
Despite extensive research on the prevalence and general characteristics of dental anxiety, the way anxiety symptoms manifest and interact remains insufficiently understood. In particular, the relationship between psychological components and physical symptoms has received limited empirical attention. While existing studies have identified significant associations between somatisation and dental fear (16), as well as correlations between psychological distress and dental fear (17), few have explored how these symptoms interact. This represents a research gap as a better understanding of the interplay between psychological and physical anxiety symptoms in dental anxiety incorporating the utilisation of instruments such as the DAS and the DFS, could enhance both diagnostic precision and the development of tailored intervention strategies.
Therefore, we aim to ascertain the correlation between psychological and physical anxiety symptoms in dental anxiety in adults. We assume a significant positive correlation. Furthermore, we hypothesise that higher levels of dental anxiety and its associated symptoms are linked to increasing general psychological stress, as measured by BSI-18.
2 Methods
The correlation between psychological anxiety symptoms and physical anxiety symptoms in dental anxiety has been evaluated using a retrospective study. A dataset of earlier studies involving a total of 1,327 adult patients was investigated.
The patients were requested to complete the questionnaires in the waiting room prior to undergoing treatment, following the provision of written informed consent. All respondents, who were required to be at least 18 years of age, were informed in writing about the objectives of the study. Participants were required to demonstrate a good command of the German language and an oriented appearance at the time of the survey, which was assessed by clinic staff. The questionnaires comprised the Dental Anxiety Scale (DAS) and the Scale Somato-visceral arousal of the Dental Fear Survey (DFS-SVA). Perceived oral health was recorded using the Oral Health Impact Profile (OHIP-5). The mental health of the participants was assessed by means of the Brief Symptom Inventory questionnaire (BSI-18).
The study was conducted in full accordance and approved by the Ethical Commission of the Technische Universität Dresden (protocol no. 232062011/29.07.2011).
2.1 Dental anxiety scale (DAS)
The Dental Anxiety Scale (DAS) is an instrument for the assessment of dental anxiety (12, 18). The DAS comprises four questions, which each question having five possible answers (13). The second to fourth question, for example, “When you are waiting in the dentist's office for your turn in the chair, how do you feel?”, relates to the respondent's feelings during various dentist-related situations (19). As the response options are ranked in ascending order from 1 to 5, the severity of dental anxiety can then be categorised within the range of 4–20 (20). The higher the score, the higher the dental anxiety. The patients were then categorised into three groups: little to no anxiety (score ≤10), somewhat anxious (score <10 ≤ 15) and severe dental anxiety (score >15). The reliability of DAS in other German studies was rtt = 0.94 (12), whereas in this survey it is good (McDonald's Omega = 0.925).
2.2 Dental fear survey (DFS)
The Dental Fear Survey (DFS) depicts behavioural and physiological responses to dental anxiety (19). It was also used in German translation, analogous to the original by Kleinknecht et al. from 1973 (15). The content of the 20 questions is divided into three areas: Avoidance of dental treatment, physical reactions to the dental treatment and fear aroused by different dental procedures (15). The DFS responses are measured on a scale from 1 (none) to 5 (great) (21) for questions such as „When having dental work done, I feel nauseated and sick to my stomach” (19). In summary, the scale ranges from 20 to 100 (22). Scores under 51 indicate no dental fear, values between 51 and 75 reflect low anxiety, and scores over 75 display high dental fear (12). In this study only the scale Somato-visceral arousal during dental treatment (physical reactions) of the DFS (DFS-SVA) was used. The scale is comprised of five items including muscle tension, perspiration and nausea (19). The reliability of DFS in German studies was found to be rtt = 0.97 (12) and in this survey the reliability of DFS-SVA is good (McDonald's Omega = 0.9).
2.3 Brief symptom inventory 18 (BSI-18)
The Brief Symptom Inventory 18 (BSI-18) is a tool for measuring psychological stress in patients with various mental and somatic illnesses (23, 24). The questionnaire is divided into three scales of six questions (somatization, anxiety, depression), and is then summarised to the total BSI-18 score (GSI) (25). In this study, only the GSI reflecting the general psychological stress was used (BSI-18 GSI). The items, for example, “feeling lonely” (23), are answered based on the patients’ experiences over the preceding seven days, offering five possible answers ranging from “not at all” (0) to “extremely” (4) (26). The total BSI-18 score ranges from 0 to 72, while each group can score between 0 and 24 (23). The reliability of the GSI of BSI-18 in other German studies was Cronbach's α = 0.93 (23), of BSI-18 GSI in this survey it is good (McDonald's Omega = 0.818).
2.4 Oral health impact profile (OHIP-5)
The Oral Health Impact Profile (OHIP-5) was developed in 1994 by Spade and Spencer (27). An analogous German version was used (28). It is a tool designed to measure oral health-related quality of life, and inquiries into four dimensions: oral function, orofacial pain, orofacial appearance, and psychosocial impact (29). The scale comprises five questions, with one item representing each dimension and an additional item for oral function (30). The questions, for example “Have you experienced difficulty chewing food due to oral problems?”, are answered on a five-point scale ranging from “never” (0) to “very often” (4) (31). The total score ranges from 0 to 20 with higher scores indicating a greater negative impact of oral health issues on an individual's quality of life (32). The reliability of the OHIP-5 in other German studies was found to be Cronbach's alpha = 0.79 (28), in this survey it is good (McDonald's Omega = 0.904).
2.5 Statistical analysis
The data was analysed using the program IBM SPSS 30. The Kolmogorov–Smirnov test was used to determine whether the data was normally distributed. To facilitate the comparison of groups, Mann–Whitney-U-Tests and Kruskal–Wallis-Tests were calculated. The magnitude of the effects was reported using Rosenthal's r or Eta2 respectively. Furthermore, Spearman correlations and a multiple linear regression analysis were conducted. The statistical relevance was determined using the p-value at p = 0.05. The reliability of the scales used was determined using McDonald's omega.
The required sample size for a robust statistical analysis was calculated using the G*Power 3 software program (33). For the implementation of a Mann–Whitney–U test (a comparison of two groups) with a predefined effect size of d = 0.05, a significance level of p = 0.05 and a power of 95% (1−β = 0.95), a minimum of 92 participants per group (total n = 184) are required. For one-way analysis of variance (ANOVA, comparison of three groups), with a predefined effect size of f = 0.25, a significance level of p = 0.05 and a power of 95% (1−β = 0.95) N = 252 individuals are required, as there is no corresponding function for the Kruskal–Wallis-Test. The required sample size for Pearson correlations is N = 115 individuals [predefined effect size of p = 0.30, significance level of p = 0.05 and a power of 95% (1−β = 0.95)] since there is no corresponding function for Spearman correlations. For multiple linear regression analysis with four predictors, the required sample size is N = 129 [predefined effect size of f = 0.15, significance level of p = 0.05, power of 95% (1–β = 0.95)].
3 Results
In the period between 2019 and 2022, a survey was conducted in various dental practices in Germany, encompassing a total of 1,327 students and patients (see overview in Table 1). The age of the respondents varied between 18 and 85 years, with a mean of 39.65 years (SD = 15.94). The proportion of male participants was 38.9% (514), while the proportion of female participants was 60.7% (803). The remaining 0.5% (6) had a different gender. Most respondents stated to have a high school diploma, such as Abitur or acc. university entrance qualification (57.6%, 586). A further 31.7% (323) of participants had an intermediate school-leaving certificate. Of the remaining patients, 8.2% (83) had a lower secondary school-leaving certificate, 1.6% (16) had another school-leaving certificate and 1.0% (10) had no school-leaving certificate.
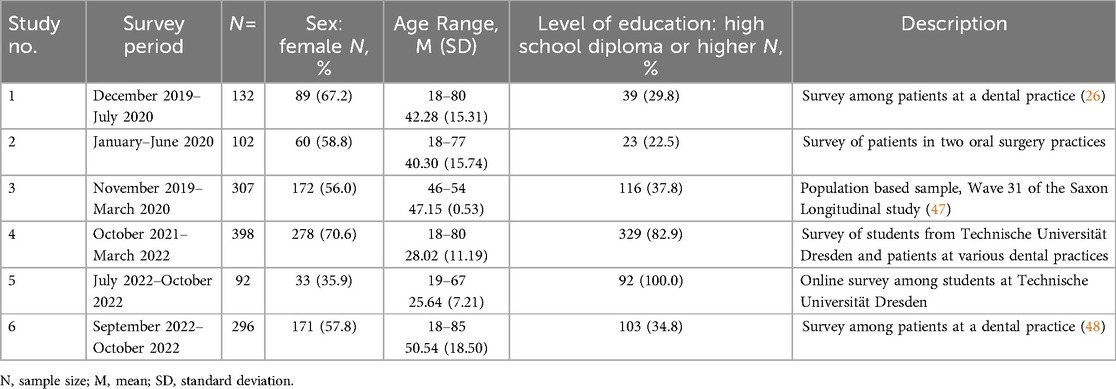
Table 1. Overview of the studies includes in the analyses.
The mean value for dental anxiety (DAS), somatic anxiety symptoms (DFS-SVA), psychological distress (GSI BSI-18), and oral health-related quality of life (OHIP-5) are shown in Table 2. The Kolmogorov–Smirnov test demonstrated that the data is not normally distributed (DAS D = 0.130, p < 0.001; DFS-SVA D = 0.161, p < 0.001; GSI BSI-18 D = 0.169, p < 0.001 and OHIP-5 D = 0.185, p < 0.001). The descriptive analysis revealed gender-specific differences in nearly all the investigated variables (Table 2). A significant disparity in performance was observed between male and female subjects, with female subjects demonstrating higher DAS scores. A similar tendency was also observed in DFS-SVA. Furthermore, psychological distress, measured by the sum-score of BSI-18 (BSI-18 GSI), was found to be significantly higher in women than in men. The values in OHIP-5 did not differ significantly between women and men. The effect sizes are all small (r < 0.30).

Table 2. Descriptive values for DAS, DFS-SVA, BSI-18 GSI and OHIP-5, comparisons between men and women (Mann–Whitney-U-tests, r = effect size rosenthal's r).
There were significant correlations found between all the variables studied (Table 3). The strongest correlation was observed between the somatic symptoms scale of the Dental Fear Survey (DFS-SVA) and the Dental Anxiety Scale (DAS) (r = 0.544). Further moderate correlations were identified between the BSI-18 GSI and the DAS (r = 0.300) as well as between the OHIP-5 and the DAS (r = 0.371). The lowest correlation was between the BSI-18 GSI and the DFS-SVA (r = 0.193).
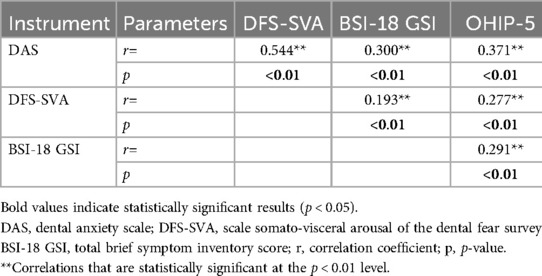
Table 3. Spearman-Correlations between DAS, DFS-SVA, BSI-18 GSI and OHIP-5.
Multiple significant predictors for DAS scores were identified in Table 4. To detect the items influencing the extent of dental anxiety (DAS), a multiple regression analysis was conducted. The dependent variable (DV) was the DAS score. The independent variables (IVs) were age, gender, psychological distress (BSI-18 GSI), and somatic anxiety symptoms (DFS-SVA). The regression analysis demonstrated a significant predictive power (df = 4, F = 130.908, p < 0.001) and explained 34.0% of the variance (R2 = 0.343, adjusted R2 = 0.340). The strongest predictor was DFS-SVA, followed by BSI-18 GSI and age. The impact of the gender found to have no significant influence.
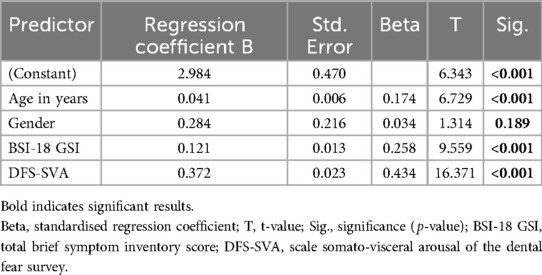
Table 4. Multiple regression analysis for dental anxiety (DAS), predictors: age, gender, BSI-18 GSI, DFS-SVA.
In the total sample, N = 808 (60.9%) participants were not anxious, N = 368 (27.7%) were somewhat anxious and N = 151 (11.4%) had a severe dental anxiety. The analysis of DAS in three groups revealed significant variations in all the parameters examined (Table 5). Individuals experiencing severe dental anxiety demonstrated significantly higher scores on the DFS-SVA, total BSI-18 GSI, and OHIP-5.
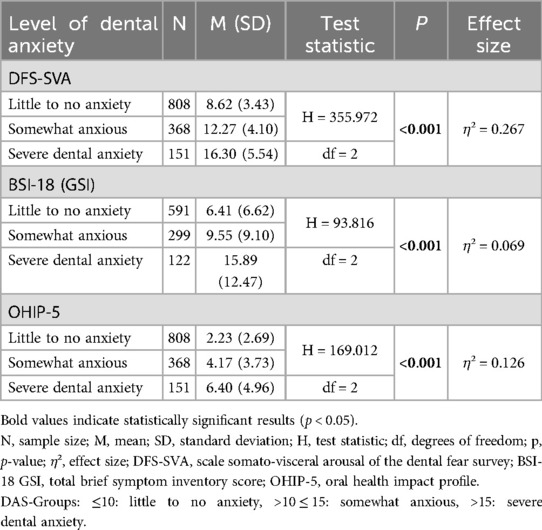
Table 5. Differences in DFS-SVA, BSI-18 GSI, OHIP-5 between groups with different 3 levels of dental anxiety (Kruskal–Wallis-tests).
4 Discussion
The aim of this study was to demonstrate the correlation between psychological and physical anxiety symptoms in dental anxiety. The large and diverse sample size of a general population utilised in this study (see Table 1) makes it particularly pertinent for dental practitioners.
The study demonstrated strong correlations between psychological dental anxiety symptoms (DAS) and physical dental anxiety symptoms (DFS-SVA). Consequently, a significant proportion of patients manifest a range of physical symptoms such as nausea and high heart rate, according to the severity of their dental anxiety. A smaller study in Germany in 2022 yielded comparable results (12).
The moderate correlation between BSI-18 and DAS indicates that patients experiencing elevated levels of general psychological stress also demonstrate a concomitant increase in of dental anxiety. Consequently, it can be hypothesised that mental stress could be a signal for possible dental anxiety. Several studies have demonstrated a strong correlation between dental anxiety and psychological distress, including depression, somatisation and generalised anxiety (17, 34–36). Accordingly, dentists should be vigilant for indications of dental anxiety in patients with documented psychological stress, with the objective of expeditiously identifying those experiencing dental anxiety.
The results also demonstrate a significant correlation between oral health-related quality of life (OHIP-5) and dental anxiety (DAS). Previous studies have shown that individuals experiencing high dental anxiety often perceive a greater negative impact of their oral health on their daily functioning and well-being and consequently have a lower oral health related quality of life (37, 38). As is thoroughly evidenced by the extant literature, the avoidance behaviour due to dental anxiety has a deleterious effect on oral health, reinforcing a vicious cycle in which worsening dental conditions exacerbate anxiety, which in turn results in further delays in treatment. This finding aligns with the conclusions drawn from earlier research (5). Nevertheless, these findings underscore the importance of early intervention and preventive dental care in managing dental anxiety.
Regarding gender differences, the present study found that women consistently reported higher levels of dental anxiety, physiological fear responses, and psychological distress than men. This was also shown in previous studies (17, 35, 39) and is consistent with existing literature suggesting that women are more likely to report anxiety-related disorders (40). The heightened anxiety experienced by woman can be attributed to a combination of emotional and social factors (41). However, the regression analysis revealed that gender was not a significant predictor of DAS scores. This finding suggests that while gender differences exist on a descriptive level, other factors such as psychological distress and avoidance behaviour play a more crucial role in determining the severity of dental anxiety.
This study suggests that dental anxiety increases with age. This contrasts with the results of other studies, which demonstrated a decrease in dental anxiety with increasing age (42–44) or identified middle age as the group with highest levels of dental anxiety (6, 45). The discrepancy may be attributable to sample characteristics. Two of the six surveys were conducted primarily among students, suggesting that the younger participants had a higher educational level compared to participants in the other groups. As dental anxiety has been shown to correlate with educational attainment (46), this difference in education level may have influenced the results.
The utilization of only validated instruments (see method section) is a crucial element in ensuring the reliability of this study. However, it is important to note that there are certain limitations must be considered. All instruments employed in this study were of a subjective nature and only stated by the patients. Despite the anonymity of the responses, the potential for societal pressures to influence the answers remains concern. Objective measures of dental health, such as the periodontal screening index (PSI) or DMF-T, could not be observed. Furthermore, over a period of several years, students and patients from different dental practices throughout Germany with all kinds of dental treatments were invited to participate in this study. Knowing that patients are more afraid of some interventions like extractions than of regular check-ups (41) may have had an influence on the answers to the questionnaires. Patients with high dental anxiety typically refrain from participating in oral-health interventions (5). Consequently, the representation of these patients in this study may be disproportionate. It is important to note that due to missing values for individual questions and/or individual survey waves, the study numbers are somewhat lower in some cases. Moreover, the cross-sectional nature of this study precludes the drawing of causal conclusions. It is recommended that future research should consider longitudinal studies with a view of enhancing our understanding of the causality and long-term development of psychological and physical dental anxiety symptoms.
Overall, the findings of this study demonstrate a close relationship between psychological dental anxiety and physical anxiety symptoms. It is imperative that dentists are cognisant of the psychological and physiological indicators of dental anxiety. In this way, anxious patients can be better recognized earlier, and treatments can be adapted better to individual needs.
5 Conclusion
The present study sought to confirm the correlation between psychological dental anxiety and physical anxiety symptoms. In addition, significant associations shown between dental anxiety (DAS), physical anxiety symptoms (DFS-SVA) and psychological distress (BSI-18 GSI), highlight a broader mental health impact of dental anxiety.
Further studies should be conducted to investigate the long-term development of dental anxiety and to establish detailed correlations between psychological and physical anxiety symptoms.
Data availability statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy issues.
Ethics statement
The studies involving humans were approved by Ethical Commission of the “Technische Universität Dresden” (protocol no. 232062011/29.07.2011). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
LAIM: Methodology, Data curation, Visualization, Formal analysis, Writing – original draft. NC: Writing – review & editing. RQ: Writing – review & editing. KMW: Writing – review & editing. HT: Writing – review & editing. JH: Writing – review & editing. LI: Writing – review & editing. KP: Writing – review & editing. HB: Project administration, Formal analysis, Investigation, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. ChatGPT and DeepL were used to translate parts of the manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
DAS, dental anxiety scale; DFS, dental fear survey; DFS-SVA, scale somato-visceral arousal of the dental fear survey; OHIP-5, oral health impact profile; BSI-18, brief symptom inventory; BSI-18 GSI, total brief symptom inventory score.
References
1. Silveira ER, Cademartori MG, Schuch HS, Armfield JA, Demarco FF. Estimated prevalence of dental fear in adults: a systematic review and meta-analysis. J Dent. (2021) 108:103632. doi: 10.1016/j.jdent.2021.103632
2. Winkler CH, Bjelopavlovic M, Lehmann KM, Petrowski K, Irmscher L, Berth H. Impact of dental anxiety on dental care routine and oral-health-related quality of life in a German adult population-a cross-sectional study. J Clin Med. (2023) 12(16):5291. doi: 10.3390/jcm12165291
3. Appukuttan DP. Strategies to manage patients with dental anxiety and dental phobia: literature review. Clin Cosmet Investig Dent. (2016) 10(8):35–50. doi: 10.2147/CCIDE.S63626
4. de Jongh A, ter Horst G. What do anxious patients think? An exploratory investigation of anxious dental patients’ thoughts. Community Dent Oral Epidemiol. (1993) 21(4):221–3. doi: 10.1111/j.1600-0528.1993.tb00760.x
5. Armfield JM, Stewart JF, Spencer AJ. The vicious cycle of dental fear: exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health. (2007) 14(7):1. doi: 10.1186/1472-6831-7-1
6. Armfield JM, Spencer AJ, Stewart JF. Dental fear in Australia: who’s Afraid of the dentist? Aust Dent J. (2006) 51(1):78–85. doi: 10.1111/j.1834-7819.2006.tb00405.x
7. Kisely S, Sawyer E, Siskind D, Lalloo R. The oral health of people with anxiety and depressive disorders—a systematic review and meta-analysis. J Affect Disord. (2016) 200:119–32. doi: 10.1016/j.jad.2016.04.040
8. Guentsch A, Stier C, Raschke GF, Peisker A, Fahmy MD, Kuepper H, et al. Oral health and dental anxiety in a German practice-based sample. Clin Oral Investig. (2017) 21(5):1675–80. doi: 10.1007/s00784-016-1951-8
9. Armfield JM, Slade GD, Spencer AJ. Dental fear and adult oral health in Australia. Community Dent Oral Epidemiol. (2009) 37(3):220–30. doi: 10.1111/j.1600-0528.2009.00468.x
10. Kvale G, Berggren U, Milgrom P. Dental fear in adults: a meta-analysis of behavioral interventions. Community Dent Oral Epidemiol. (2004) 32(4):250–64. doi: 10.1111/j.1600-0528.2004.00146.x
11. Wide U, Hakeberg M. Treatment of dental anxiety and phobia-diagnostic criteria and conceptual model of behavioural treatment. Dent J. (2021) 9(12):153. doi: 10.3390/dj9120153
12. Tönnies S, Mehrstedt M, Eisentraut I. Die dental anxiety scale (DAS) und das dental fear survey (DFS) – zwei messinstrumente zur erfassung von zahnbehandlungsängsten. Z Med Psychol. (2002) 11:63–72. doi: 10.3233/ZMP-2002-11_2_04
13. Corah NL. Development of a dental anxiety scale. J Dent Res. (1969) 48(4):596. doi: 10.1177/00220345690480041801
14. Corah NL, Gale EN, Illig SJ. Assessment of a dental anxiety scale. J Am Dent Assoc. (1978) 97(5):816–9. doi: 10.14219/jada.archive.1978.0394
15. Kleinknecht RA, Thorndike RM, McGlynn FD, Harkavy J. Factor analysis of the dental fear survey with cross-validation. J Am Dent Assoc. (1984) 108(1):59–61. doi: 10.14219/jada.archive.1984.0193
16. Armfield JM, Pohjola V, Joukamaa M, Mattila AK, Suominen AL, Lahti SM. Exploring the associations between somatization and dental fear and dental visiting. Eur J Oral Sci. (2011) 119(4):288–93. doi: 10.1111/j.1600-0722.2011.00839.x
17. Zinke A, Hannig C, Berth H. Psychological distress and anxiety compared amongst dental patients- results of a cross-sectional study in 1549 adults. BMC Oral Health. (2019) 19(1):27. doi: 10.1186/s12903-019-0719-3
18. Kunzelmann KH, Dünninger P. Dental fear and pain: effect on patient’s perception of the dentist. Community Dent Oral Epidemiol. (1990) 18(5):264–6. doi: 10.1111/j.1600-0528.1990.tb00073.x
19. Chi SI. What is the gold standard of the dental anxiety scale? J Dent Anesth Pain Med. (2023) 23(4):193–212. doi: 10.17245/jdapm.2023.23.4.193
20. Coolidge T, Arapostathis KN, Emmanouil D, Dabarakis N, Patrikiou A, Economides N, et al. Psychometric properties of Greek versions of the modified corah dental anxiety scale (MDAS) and the dental fear survey (DFS). BMC Oral Health. (2008) 8:29. doi: 10.1186/1472-6831-8-29
21. Liu Y, Zhang C, Wu J, Yu H, Xie C. Evaluation of the relationship among dental fear, scaling and root planing and periodontal status using periodontitis stages: a retrospective study. J Dent Sci. (2022) 17(1):293–9. doi: 10.1016/j.jds.2021.04.002
22. Kassem El Hajj H, Fares Y, Abou-Abbas L. Psychometric evaluation of the Lebanese Arabic version of the dental fear survey: a cross-sectional study. BMC Oral Health. (2021) 21(1):651. doi: 10.1186/s12903-021-02015-y
23. Franke GH, Jaeger S, Glaesmer H, Barkmann C, Petrowski K, Braehler E. Psychometric analysis of the brief symptom inventory 18 (BSI-18) in a representative German sample. BMC Med Res Methodol. (2017) 17(1):14. doi: 10.1186/s12874-016-0283-3
24. Derogatis N. BSI 18, Brief Symptom Inventory 18: Administration, Scoring and Procedures Manual. Minneapolis, MN: NSC Pearson (2001). p. 47.
25. Franke G, Jäger S, Morfeld M, Salewski C, Reimer J, Rensing A, et al. Eignet sich das BSI-18 zur Erfassung der psychischen Belastung von nierentransplantierten Patienten? Z Med Psychol. (2010) 19:30–7. doi: 10.3233/ZMP-2010-19_1_05
26. Cunoti N, Qorri R, Irmscher L, Qorri E, Magerfleisch L, Berth H. Dental anxiety and dental care—a comparison between Albania and Germany. BMC Oral Health. (2024) 24(1):1121. doi: 10.1186/s12903-024-04887-2
27. Slade GD, Spencer AJ. Development and evaluation of the oral health impact profile. Community Dent Health. (1994) 11(1):3–11.8193981
28. John MT, Miglioretti DL, LeResche L, Koepsell TD, Hujoel P, Micheelis W. German short forms of the oral health impact profile. Community Dent Oral Epidemiol. (2006) 34(4):277–88. doi: 10.1111/j.1600-0528.2006.00279.x
29. Alhajj MN, Halboub E, Khalifa N, Amran AG, Reissmann DR, Abdullah AG, et al. Translation and validation of the Arabic version of the 5-item oral health impact profile: OHIP5-ar. Health Qual Life Outcomes. (2018) 16(1):218. doi: 10.1186/s12955-018-1046-0
30. John MT, Omara M, Su N, List T, Sekulic S, Häggman-Henrikson B, et al. Recommendations for use and scoring of oral health impact profile versions. J Evid Based Dent Pract. (2022) 22(1):101619. doi: 10.1016/j.jebdp.2021.101619
31. Naik A, John MT, Kohli N, Self K, Flynn P. Validation of the English-language version of 5-item oral health impact profile. J Prosthodont Res. (2016) 60(2):85–91. doi: 10.1016/j.jpor.2015.12.003
32. Simancas-Pallares M, John MT, Enstad C, Lenton P. The Spanish language 5-item oral health impact profile. Int Dent J. (2020) 70(2):127–35. doi: 10.1111/idj.12534
33. Faul F, Erdfelder E, Lang AG, Buchner A. G*power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. (2007) 39(2):175–91. doi: 10.3758/bf03193146
34. Talo Yildirim T, Dundar S, Bozoglan A, Karaman T, Dildes N, Acun Kaya F, et al. Is there a relation between dental anxiety, fear and general psychological status? PeerJ. (2017) 15(5):e2978. doi: 10.7717/peerj.2978
35. Anbari F, Elmi Z, Anbari F, Rezaeifar K. General anxiety and dental fear: is there a relationship? J Dent Mater Tech. (2019) 8(4):190–6. doi: 10.22038/jdmt.2019.14019
36. Halonen H, Nissinen J, Lehtiniemi H, Salo T, Riipinen P, Miettunen J. The association between dental anxiety and psychiatric disorders and symptoms: a systematic review. Clin Pract Epidemiol Ment Health. (2018) 31(14):207–22. doi: 10.2174/1745017901814010207
37. Mehrstedt M, John MT, Tönnies S, Micheelis W. Oral health-related quality of life in patients with dental anxiety. Community Dent Oral Epidemiol. (2007) 35(5):357–63. doi: 10.1111/j.1600-0528.2007.00376.x
38. Hassan BH, Abd El Moniem MM, Dawood SS, Alsultan AA, Abdelhafez AI, Elsakhy NM. Dental anxiety and oral-health-related quality of life among rural community-dwelling older adults. Int J Environ Res Public Health. (2022) 19(13):7643. doi: 10.3390/ijerph19137643
39. Dadalti MT, Cunha AJ, Souza TG, Silva BA, Luiz RR, Risso PA. Anxiety about dental treatment—a gender issue. Acta Odontol Latinoam. (2021) 34(2):195–200. doi: 10.54589/aol.34/2/195
40. McLean CP, Asnaani A, Litz BT, Hofmann SG. Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J Psychiatr Res. (2011) 45(8):1027–35. doi: 10.1016/j.jpsychires.2011.03.006
41. Jeddy N, Nithya S, Radhika T, Jeddy N. Dental anxiety and influencing factors: a cross-sectional questionnaire-based survey. Indian J Dent Res. (2018) 29(1):10–5. doi: 10.4103/ijdr.IJDR_33_17
42. Sukumaran I, Taylor S, Thomson WM. The prevalence and impact of dental anxiety among adult New Zealanders. Int Dent J. (2020) 71(2):122–6. doi: 10.1111/idj.12613
43. Lahti S, Vehkalahti MM, Nordblad A, Hausen H. Dental fear among population aged 30 years and older in Finland. Acta Odontol Scand. (2007) 65(2):97–102. doi: 10.1080/00016350601058085
44. Locker D, Liddell AM. Correlates of dental anxiety among older adults. J Dent Res. (1991) 70(3):198–203. doi: 10.1177/00220345910700030801
45. Hakeberg M, Berggren U, Carlsson SG. Prevalence of dental anxiety in an adult population in a major urban area in Sweden. Community Dent Oral Epidemiol. (1992) 20(2):97–101. doi: 10.1111/j.1600-0528.1992.tb00686.x
46. Bermúdez-Bejarano E, Bermúdez-Sánchez JA, Ruiz-Rey FJ, Baus-Domínguez M, Serrera-Figallo MÁ, Gutiérrez-Pérez JL, et al. Influence of education on dental anxiety and fear in mental disorders after viewing a molar extraction in three types of mental disorder compared to persons with no mental disorder. J Clin Med. (2024) 13(13):3868. doi: 10.3390/jcm13133868
47. Berth H, Brähler E, Zenger M, Stöbel-Richter Y. 30 Jahre Ostdeutsche Transformation: Sozialwissenschaftliche Ergebnisse und Perspektiven der Sächsischen Längsschnittstudie. Gießen: Psychosozial-Verlag (2020).
Keywords: dental anxiety, dental anxiety scale, dental fear survey, oral health, anxiety symptoms, cross-sectional study, Germany
Citation: Magerfleisch LAI, Cunoti N, Qorri R, Weil KM, Tröger H, Häring J, Irmscher L, Petrowski K and Berth H (2025) Correlations between psychological anxiety symptoms and physical anxiety symptoms in dental anxiety—a cross-sectional study with 1327 patients. Front. Oral Health 6:1612982. doi: 10.3389/froh.2025.1612982
Received: 16 April 2025; Accepted: 25 July 2025;
Published: 28 August 2025.
Edited by:
Roberta Gasparro, University of Naples Federico II, ItalyReviewed by:
Satu Lahti, University of Turku, FinlandHatice Yemenoğlu, Recep Tayyip Erdogan University Training and Research Hospital, Türkiye
Copyright: © 2025 Magerfleisch, Cunoti, Qorri, Weil, Tröger, Häring, Irmscher, Petrowski and Berth. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hendrik Berth, aC5iZXJ0aEB1a2RkLmRl