 Luis Chauca-Bajaña1,2,†,‡
Luis Chauca-Bajaña1,2,†,‡ Alba Pérez-Jardón2,3,†,‡Carlos Carpio-Cevallos1,‡Andrea Ordoñez Balladares1,4*‡Patricio Proaño-Yela1,‡
Alba Pérez-Jardón2,3,†,‡Carlos Carpio-Cevallos1,‡Andrea Ordoñez Balladares1,4*‡Patricio Proaño-Yela1,‡ Byron Velásquez Ron5,6,‡Leonardo Javier Siguencia Suarez1,‡Carla Verenice Romo Olvera1,‡Diana Orellana Guerrero1,‡
Byron Velásquez Ron5,6,‡Leonardo Javier Siguencia Suarez1,‡Carla Verenice Romo Olvera1,‡Diana Orellana Guerrero1,‡ Mario Pérez-Sayáns2,3,7,‡
Mario Pérez-Sayáns2,3,7,‡
- 1College of Dentistry, University of Guayaquil, Guayas, Ecuador
- 2Oral Medicine, Oral Surgery and Implantology Unit (MedOralRes), Faculty of Medicine and Dentistry, Universidade de Santiago de Compostela, Santiago de Compostela, Spain
- 3ORALRES GROUP, Health Research Institute of Santiago de Compostela (IDIS), Santiago de Compostela, A Coruna, Spain
- 4College Dentistry, University Bolivariana del Ecuador, Durán, Ecuador
- 5Carrera de Odontología, Facultad de Odontología, Universidad de Las Américas (UDLA), Quito, Ecuador
- 6Department Prosthesis Research, Universidad de las Américas (UDLA), Quito, Ecuador
- 7Instituto de los Materiales de Santiago de Compostela (iMATUS), Santiago de Compostela, A Coruna, Spain
Background: Dental anxiety is a widespread issue that significantly impacts oral health behaviors, often leading individuals to postpone or avoid dental care. This avoidance can result in more complex and invasive treatments. This study aimed to evaluate the levels of dental anxiety and associated factors among patients attending the dental clinic at the University of Guayaquil, Ecuador.
Materials and methods: A total of 389 patients were assessed using three validated instruments: the Modified Dental Anxiety Scale (MDAS), the Dental Anxiety Short Scale (SDAI), and the Dental Anxiety and Fear Diagnosis (DAYMO). Statistical analyses included bivariate tests and correlation analyses using Spearman's rho and Pearson's chi-square tests.
Results: Among the participants, 63.8% were female and 36.3% were male. Women reported significantly higher levels of anxiety across all assessment tools (p < 0.05). Based on the SDAI, 47% of patients exhibited moderate to severe anxiety, whereas 19% reported high anxiety levels on the MDAS. The DAYMO instrument revealed that 51.2% of participants experienced mild anxiety, and 27.8% had moderate anxiety. Common anxiety triggers included fear of pain, past negative dental experiences, and concerns about needles or oral hygiene practices.
Conclusions: Dental anxiety was prevalent among patients, particularly among women, with most experiencing mild to moderate levels. These findings underscore the importance of addressing psychological factors in dental care settings to improve patient experience and outcomes.
1 Introduction
Dental anxiety affects many people and is perceived as extreme insecurity related to visits to the dentist or dental treatments (1). Dental anxiety can be caused by fear of pain, previous negative experiences, the feeling of lack of control or simply fear of the unknown (2, 3). This anxiety can trigger a response in the autonomic nervous system, thus leading to increases in involuntary bodily functions, such as blood pressure, heart rate, respiratory rate, gastrointestinal motility and cardiac output (4). The stress that arises in response to dental treatment can be triggered by a variety of factors, ranging from a clearly identifiable cause to more vague stimuli, or it may even occur without any apparent reason (5). Dental anxiety is a complex response that activates multiple systems within the body in reaction to a perceived threat or danger, significantly impacting daily life and acting as a barrier to seeking and receiving dental care (6). This anxiety manifests in three main spheres: the cognitive, characterized by negative thoughts and worries; the psychophysiological, involving physical responses such as increased heart rate; and the behavioral, marked by avoidance of dental appointments (7). Recent evidence indicates that dental anxiety is not only related to previous negative experiences or fear of pain but also to a combination of cognitive and non-cognitive factors. Cognitive aspects, such as catastrophic thinking, negative beliefs, and perceived lack of control, have been shown to significantly intensify anticipatory fear before treatment (8, 9). In contrast, non-cognitive factors, including traumatic dental events, family influence, cultural background, and personality traits such as neuroticism or introversion, also play a relevant role in shaping the patient's anxiety response (10, 11). The interplay of these factors highlights the multidimensional nature of dental anxiety and underlines the importance of considering both psychological and contextual determinants when assessing and managing this condition.
Dental phobia, on the other hand, represents a more intense form of anxiety, characterized by persistent concern regarding specific objects or situations, such as injections or dental procedures in general, which can trigger panic episodes accompanied by sweating and trembling (12). A meta-analysis showed that the prevalence of dental anxiety in Chinese adults was 35.4% (13). A systematic review and meta-analysis reported that the estimated overall prevalence of high and severe dental fear and anxiety (DFA) in adults was 15.3%, 12.4%, and 3.3%, respectively (14). People with severe dental anxiety tend to avoid dental appointments, thereby compromising their oral health, increasing the risk of dental pain, and leading to more invasive treatments (15). A study by Thomson et al. in 2009 (16) revealed that DFA usually occurs in childhood, adolescence or even later in life; hence, it is important to use a reliable and valid assessment tool to properly diagnose dental anxiety before a patient visits a dentist (17). There are several scales designed to measure dental anxiety, among the most commonly used being the DASS-21, which was not included in this study as it also assesses depression (18–21). Among these, the Modified Dental Anxiety Scale (MDAS) is one of the most widely used questionnaires to assess dental anxiety in patients seeking dental care, regardless of the type of procedure they are facing (16, 22). In 1969, Norman Corah (15) created the Dental Anxiety Scale (DAS) to measure pre-procedure anxiety in patients; subsequently, in 1995, this questionnaire evolved into the Modified Dental Anxiety Scale (MDAS), leading to improvements in patient care and experience in the dental environment (23). In 1995, Stouthard, Groen and Mellenbergh developed the nine-item Simplified Dental Anxiety Inventory (SDAI); the SDAI was created based on an analysis of the Dental Anxiety Inventory and has been proven to be a reliable and valid tool (24). Additionally, the SDAI has been shown to be strongly correlated with other dental anxiety scales, such as the Dental Anxiety Scale (DAS), thereby indicating its efficacy for assessing anxiety in patients before they undergo dental procedures (25).
The SDAI, MDAS and DAYMO assess dental anxiety from distinct yet complementary perspectives. MDAS focuses on anticipatory anxiety in specific dental treatment scenarios, while the SDAI evaluates a broader range of emotional and behavioral responses to dental procedures. Additionally, the Dental Anxiety and Your Memory of the Dentist (DAYMO) scale, used as a complementary measure, identifies specific triggers of dental anxiety, such as fear of pain or needles.
This study aimed to better understand dental anxiety and its contributing factors among patients at a comprehensive dental clinic in Guayaquil, Ecuador. To do so, we considered it essential to assess dental anxiety from different complementary perspectives provided by the three selected questionnaires (MDAS, SDAI, and DAYMO) each of which offers a slightly different focus.
The null hypothesis was that there are no significant differences in dental anxiety levels among the different questionnaires used nor in relation to associated factors, such as gender and anxiety-triggering factors, among patients attending the comprehensive dental clinic in Guayaquil, Ecuador.
2 Materials and methods
2.1 Study design and study setting
This cross-sectional observational study was conducted among patients who received care at the comprehensive dental clinic of the Faculty of Dentistry at the University of Guayaquil. Specifically, participants were treated by students in the eighth, ninth, and tenth semesters during academic Cycle II of the 2024–2025 period. The STROBE reporting guidelines were followed.
2.1.1 Inclusion criteria
• Patients aged ≥18 years who attended the comprehensive dental clinic of the Faculty of Dentistry, University of Guayaquil, during academic Cycle II (2024–2025).
• Patients who provided written informed consent and voluntarily agreed to participate.
• Patients who fully completed the three questionnaires (MDAS, SDAI, and DAYMO).
2.1.2 Exclusion criteria
• Patients with cognitive impairments or psychiatric diagnoses that could interfere with the reliable completion of the questionnaires.
• Patients undergoing emergency dental treatment (e.g., acute pain, infection, trauma), as their clinical condition could bias the assessment of dental anxiety.
• Patients who declined participation or submitted incomplete questionnaires.
2.2 Ethical consideration and informed consent
Ethical approval was obtained from both the Dean of the Faculty and the Bioethics Committee of the USC (Reference: USC01/2024), in accordance with the ethical principles outlined in the Declaration of Helsinki. All participants were informed of the study objectives and procedures and provided written informed consent prior to their inclusion in the study.
2.3 Sample size and sampling technique
Two statistical approaches were considered for the sample size estimation. First, based on previously published data regarding differences in mean anxiety levels measured using the Modified Dental Anxiety Scale (MDAS), an a priori power analysis was performed. To detect a mean difference of 0.8 with a standard deviation of 1.5 between men and women, assuming equal variances, a 95% confidence level, and a power of 90%, a minimum of 75 individuals per group was required. This calculation was conducted using Epidat 4.2, resulting in a total required sample size of 150 participants.
Additionally, for the correlational analysis, a proper priori power calculation was performed using G Power 3.1 software. Considering an expected correlation coefficient of r = 0.192, a two-tailed test, an alpha level of 0.05, and a desired power of 0.95, the minimum required sample size was estimated to be 389 participants. The actual sample included in the study matched this requirement, ensuring adequate statistical power for the analyses conducted.
2.4 Research instrument
The participants answered three questionnaires anonymously in the waiting room of the comprehensive clinic. The first questionnaire was the Modified Dental Anxiety Scale (MDAS), which was validated in Spanish by Coolidge et al. (26). In addition, this scale has also been validated in several languages (27–31). The MDAS consists of five items that assess anticipatory anxiety in common dental situations, including waiting for a check-up, sitting in the dentist's chair, anticipating drilling, undergoing scaling, and receiving an anesthetic injection. Each item is rated on a 5-point scale (1 = not anxious, 2 = slightly anxious, 3 = fairly anxious, 4 = very anxious, 5 = extremely anxious). The scores are summed to obtain a global index of dental anxiety, widely validated as a reliable screening tool in different languages and populations. Total scores <9 indicate mild or no anxiety, 9–12 indicate moderate anxiety, 13–14 indicate high anxiety, and ≥15 suggest severe anxiety or dental phobia (16).
The SDAI was originally developed in English by Irene Aartman in 1998 (32) and we have used a version translated into Spanish. The SDAI comprises nine items designed to evaluate both emotional and behavioral reactions to dental stimuli, including nervousness before treatment, avoidance behaviors, and physiological symptoms (e.g., sweating, trembling). Each item is scored on a 5-point Likert scale (33). Total scores range from 9 to 10 (minimal anxiety), 11 to 19 (mild anxiety in specific situations), 20 to 27 (moderate anxiety with some self-control), and 28 to 36 (severe dental anxiety) (34, 35).
The DAYMO questionnaire was developed in Spanish by the authors and previously tested in a pilot study, showing good internal consistency (Cronbach's alpha = 0.817). It consists of items addressing specific anxiety-triggering factors such as fear of pain, needles, noises, or the dentist's judgment of oral hygiene. Each item is scored on a 5-point Likert scale (33), with total scores categorized as follows: < 9 = mild or no anxiety, 9–12 = moderate anxiety, 13–15 = high anxiety, and >15 = severe anxiety. Unlike the MDAS and SDAI, which primarily measure general anticipatory or situational anxiety, the DAYMO provides a more detailed assessment of contextual triggers relevant to dental settings.
The following independent variables were studied: Gender, Marital Status, Socioeconomic status, Level of Education, Number of Children. Socioeconomic status and level of education were determined based on participants' self-reported categorization. As dependent variables, the results of the SDAI, MDAS, and DAYMO Tests.
2.5 Statistical analysis
A multivariate analysis was conducted to evaluate the association between qualitative variables from questionnaires and dental fear and anxiety. Relative frequencies and measures of central tendency (mean, median, standard deviation and variance) were calculated. Spearman's correlation tests were used to assess the relationship between demographic characteristics and dental anxiety. The normality of data distributions was verified using the Kolmogorov–Smirnov test. The associations between sociodemographic variables and the classification of fear and anxiety were determined using Pearson's chi-square test. Bivariate analysis was applied to evaluate the simultaneous effect of the associated factors that would explain the fear and anxiety scores by means of multiple linear regression analysis after verifying that the data met the necessary assumptions (i.e., randomness of the dependent variable and linearity). Results were presented through tables and graphs using SPSS Statistical Software version 27 (36). In addition, the Cronbach alpha coefficient of each scale was calculated, and sociodemographic data such as sex, marital status, socioeconomic level and level of education were also recorded. In all analyses, a p-value less than 0.05 was considered statistically significant.
3 Results
A total of 389 patients were included in this study, of which 63.8% were women and 36.3% were men. A descriptive analysis of the sociodemographic data of the sample is shown in Table 1.
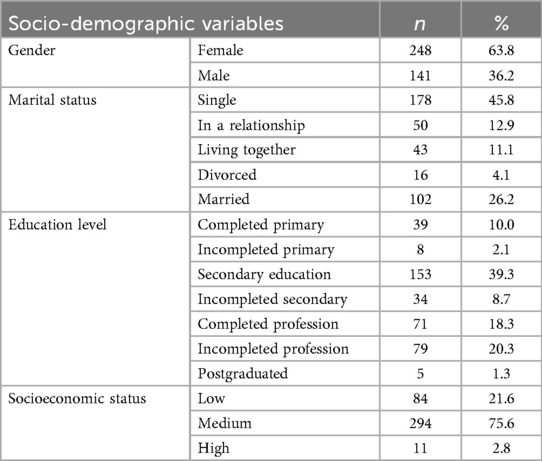
Table 1. Descriptive data.
The anxiety-inducing factors related to dental visits are presented in Table 2, which shows the questions for the different tests and the participants' responses.

Table 2. Questionnaires from the different tests analyzed.
Association analyses using the Chi-square test between socio-demographic variables and anxiety assessments (SDAI, MDAS, and DAYMO) revealed significant differences related to gender, with p-values of 0.025 for SDAI, 0.01 for MDAS, and <0.001 for DAYMO. However, no statistically significant associations were observed for other variables, such as marital status, education level, socioeconomic status, and number of children (Table 3).

Table 3. Analysis of sociodemographic variables in relation to the SDAI, MDAS, and DAYMO tests.
Both the SDAI and MDAS demonstrated high reliability, with Cronbach's alpha coefficients of 0.905 and 0.875, respectively. The DAYMO showed good but slightly lower reliability, with Cronbach's alpha coefficient of 0.817. 47% of patients who completed the SDAI reported moderate or severe levels of anxiety during their visit to the dentist. However, MDAS results indicated that 54% of patients experimented with mild or no anxiety, while 19% reported high or severe anxiety. The DAYMO findings revealed that 51.2% of patients experienced mild anxiety and 27.8% experienced moderate anxiety during dental consultations. Only 5.1% of patients reported severe anxiety. A deeper analysis of the DAYMO results shows that men were more likely to report mild anxiety (58.2%) compared to women (47.2%), while women were more likely to report moderate anxiety (35.1%) compared to men (14.9%). Regardless of the assessment tool (SDAI, MDAS or DAYMO), women exhibited higher anxiety levels than males (Table 4).
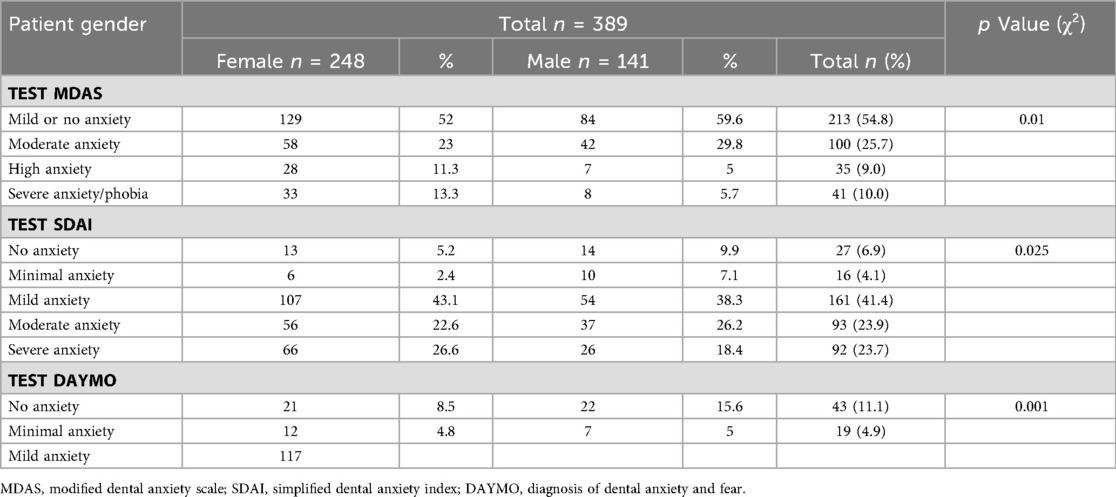
Table 4. Anxiety rating according to each scale.
The results indicate that women exhibit higher levels of dental anxiety compared to men, with a predominance of both mild and severe anxiety. Additionally, while both men and women reported anxiety levels approaching the threshold of severe anxiety on the SDAI, this pattern was not observed on the MDAS or DAYMO (Figure 1). Graphical analyses of perimeter distances between axes in relation to MDAS anxiety levels suggested that both genders reported anxiety levels nearing severe or phobic thresholds (Figure 2). This finding was further supported by the DAYMO results, which showed that both men and women reported anxiety levels very close to severe anxiety (Figure 3).
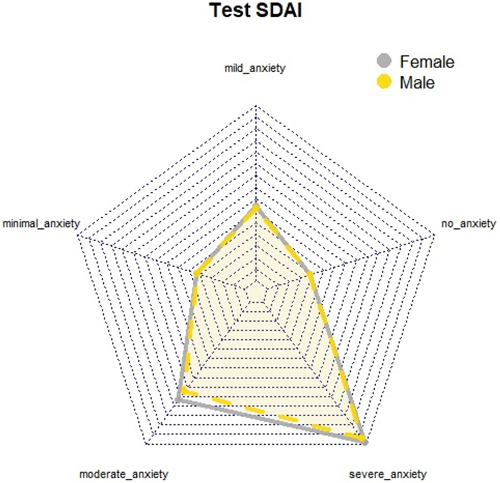
Figure 1. Radial graph SDAI test.
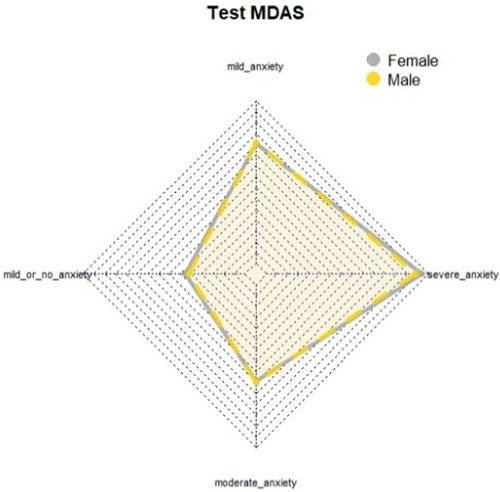
Figure 2. Radial graph MDAS test.
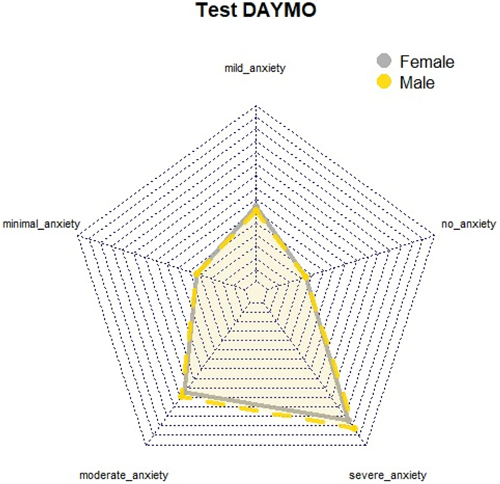
Figure 3. Radial graph DAYMO test.
The variety of anxiety-triggering factors during dental visits was remarkable. Fear of treatment pain, previous negative dental experiences, and apprehension about needles or injections emerged as prominent concerns. In the SDAI test, 11% of patients felt high anxiety when thinking about the use of the dental drill and the preparation of the syringe with anesthesia. In the MDAS test, 53% felt relaxed during dental check-ups and 51% in the waiting room, although 40% experienced mild anxiety in the dentist's chair and 37% when anticipating an injection. According to the DAYMO test, 31% had occasional fear of dental pain and 29% felt some apprehension about needles, but the majority did not have negative dental experiences or fear of sounds or odors from the dental office.
All three tests (SDAI, MDAs, and DAYMO) show positive and significant correlations with each other, suggesting that they are measuring similar aspects of anxiety. The correlations are statistically significant at a confidence level of 0.01, indicating that it is highly unlikely these correlations are due to chance.
Statistically significant correlations were observed between the total scores of the SDAI, MDAS and DAYMO. A strong positive association between these scores was observed, supported by strong and consistently high correlations (Table 5).
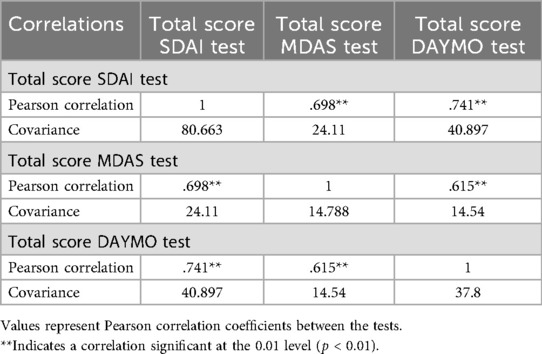
Table 5. Pearson correlation between tests.
By using binary linear regression, the analysis examines whether gender significantly predicts anxiety scores across these different assessment tools. The results in Table 6 further clarify these associations. While the MDAS shows a statistically significant difference between genders (p = 0.02), indicating that gender has a meaningful impact on anxiety levels measured by this scale, the associations for SDAI (p = 0.13) and DAYMO (p = 0.07) did not reach statistical significance. The regression coefficients (B values) indicate the direction of these relationships, with negative values suggesting that females (coded as the reference group) exhibited higher anxiety scores than males (Table 6).

Table 6. Binary linear regression of tests vs. gender.
In addition, a network analysis was performed showing how different levels of anxiety are related, from “No anxiety” and “Mild anxiety” to more intense states such as “Severe anxiety” and “Phobia”. The green nodes represent these levels, while the red ones indicate associated factors that influence them. The arrows suggest how some levels can lead to more severe ones. This approach allows a better understanding of the connections and pathways that can cause anxiety to increase, providing a clearer perspective on how these states develop and worsen (Figure 4).
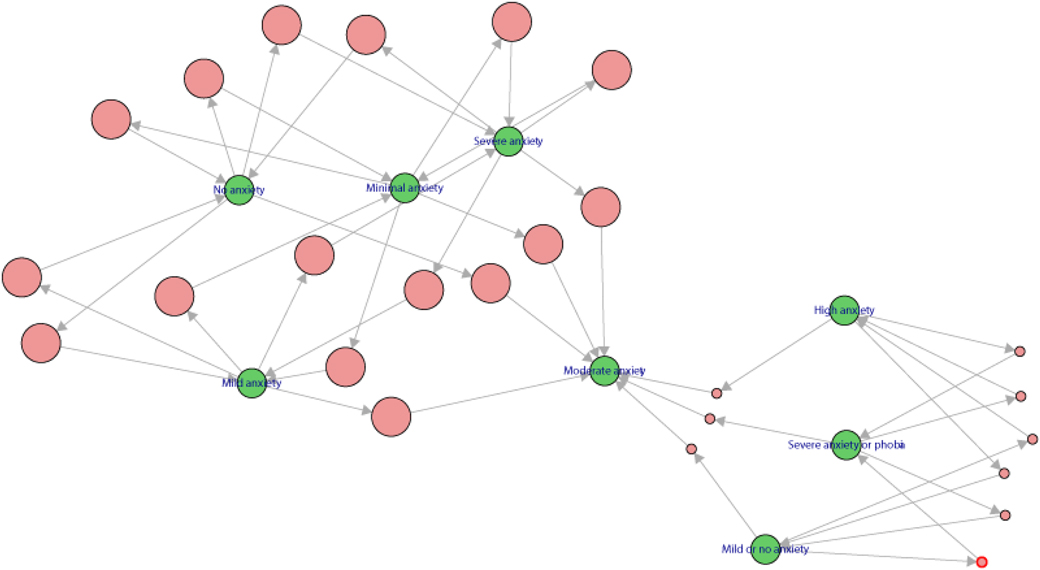
Figure 4. Network of interactions between anxiety levels and associated factors.
4 Discussion
Dental anxiety, characterized by apprehension, nervousness, or fear related to dental care, remains a prevalent concern in dental practice (37). This study aimed to evaluate anxiety levels and associated factors among patients treated at a comprehensive dental clinic using 3 questionnaires, i.e., the MDAS, SDAI and DAYMO. Our findings revealed significant levels of anxiety among participants, with 19% experiencing high or moderate anxiety according to MDAS, 47% reporting moderate anxiety according to SDAI, and 33% exhibiting moderate to severe anxiety according to DAYMO. These results align with previous research, such as Gil-Abando et al. (38), who studied 200 patients and found that 10% had moderate anxiety and 3.5% had severe anxiety according to the MDAS Scale. Similarly, Metin-Gürsoy et al. (39), reported severe anxiety in 34.1% and moderate anxiety in 27.6% of participants. These findings highlight the constant presence of moderate to severe anxiety, thus emphasizing the importance of addressing this concern in dental care to improve patient experiences. Sivaramakrishnan et al. (40) concluded that 23.7% of the participants experienced moderate anxiety, 11.4% felt very anxious, and 4.6% suffered from dental phobia. In contrast, White et al. (41) found that 19% of the total study population exhibited moderate to high dental anxiety, while 6.8% had high levels of dental anxiety. Muneer MU et al. (37) determined that 75% reported having dental anxiety. Other studies, such as those by Alemany-Martínez et al. (42) and Caltabiano et al. (43), showed that women had higher levels of dental anxiety. Saatchi et al. (44) found that women exhibited significantly higher levels of anxiety (p < 0.001) and fear (p = 0.003) compared to men in a study of 473 patients. Similarly, Erten et al. (45) reported that women tended to experience greater anxiety, with a mean score of 9.5 ± 4.1 vs. 7.9 ± 3.3 in men. Furthermore, do Nascimento et al. (46) concluded that anxiety was more prevalent in women, (20.7% vs. 11.3%) in men (p = 0.995). These findings indicate a consistent trend in the literature, highlighting that women tend to experience higher levels of anxiety in dental contexts.
This study highlights a notable disparity in the levels of high and severe anxiety, evidencing a significant prevalence in women in contrast to men. While educational attainment could play an important role, as shown in other studies (47–49), our current study did not find a significant association between educational level and anxiety related to dental care. Other scales, such as the SDAI, were used. Liu Y et al. (50), found that individuals with periodontal disease had an average dental anxiety score of 23.4 ± 8.5, while those without the disease had a score of 22.6 ± 8.6. On the other hand, in the study by Murillo-Benítez et al. (51), the mean SDAI anxiety score was 27.2 ± 12.5, highlighting that 70% of the women presented moderate or high levels of anxiety. In Nepal, research at the BP Koirala Institute of Health Sciences found that 2% of patients exhibited extreme anxiety (MDAS ≥ 19), 20.67% experienced high anxiety, and 51.33% had moderate anxiety, indicating that more than half of the patients experienced some degree of anxiety (52). Similarly, in Lebanon, a study conducted in 29 private dental clinics revealed that 31.5% of patients suffered from dental anxiety, while 22.4% had dental phobia, suggesting that fear of dental procedures is a common concern across different populations (53). In Saudi Arabia, a study at Al-Jouf University found that 51.6% of patients experienced dental anxiety, with 22.1% at a moderate level, 17.1% at a high level, and 12.4% at an extreme level (54). In line with these findings, another study conducted at the Faculty of Dentistry Hospital in Jeddah reported that 48.3% of patients experienced dental anxiety (score >15), while 2.5% had dental phobia (score >16), further confirming the significance of this issue in the region (55).
The results of the research highlight that 47.6% of people had moderate to severe anxiety, with a higher prevalence of anxiety in women. This finding highlights a statistically relevant connection between the levels of anxiety assessed through the SDAI and the gender characteristics of the patients. In addition, the relationships between the questionnaires provide valuable insights into anxiety assessment. The association between the SDAI score and MDAS score suggested a connection between mild and severe anxiety levels. However, when contrasting the SDAI and DAYMO, discrepancies are observed in the identification of mild anxiety. Despite this, the high concordance between MDAS and DAYMO in the absence of anxiety, as well as in the detection of moderate and high levels, highlights the consistency in those specific ranges. These findings underscore the complexity of measuring and understanding anxiety in the dental context, highlighting the need to consider multiple assessment tools to capture diverse aspects of patients' experience of anxiety.
The clinical relevance of this study lies in its ability to provide dental professionals with valuable information regarding the prevalence and associated factors of dental anxiety. Identifying that a significant proportion of patients experience moderate to severe levels of anxiety, along with triggering factors such as fear of pain and negative past experiences, enables dentists to adjust their treatment approaches. Furthermore, the observed gender differences in anxiety levels underscore the need to implement personalized strategies that enhance the patient experience, promoting greater adherence to preventive care and reducing treatment avoidance.
Furthermore, our findings are consistent with international evidence on dental anxiety. In a Chinese implant surgery context, moderate and high preoperative dental anxiety were found in 66.6% and 11.9%, respectively (56). In the Netherlands, a representative adult sample showed dental fear in 24.3% of respondents, with dental phobia present in 3.7%, and women reporting more severe fear (57). These comparisons confirm that dental anxiety is a widespread phenomenon, often more pronounced among women and younger populations. This underscores the importance of broad strategies—like clear communication, pain control, and relaxation techniques—while adapting them to sociocultural contexts.
5 Strengths and limitations
This study has several strengths. First, it included a relatively large sample size (n = 389), which provided adequate statistical power for the analyses and enhanced the reliability of the findings. Second, we employed three validated and complementary instruments (MDAS, SDAI, and DAYMO), allowing for a more comprehensive assessment of dental anxiety than studies relying on a single measure. Third, to our knowledge, this is one of the few investigations exploring dental anxiety in an Ecuadorian population, thereby contributing novel data from a Latin American context where evidence is still limited. Finally, the rigorous application of statistical analyses, including correlation and regression, ensured a robust evaluation of associations between anxiety and demographic variables.
Nevertheless, some limitations should be acknowledged. The cross-sectional design prevents establishing causal relationships between anxiety and associated factors. The use of self-reported questionnaires may introduce response or recall bias, as participants might underreport or overreport their true levels of anxiety. In addition, because the sample was recruited from a single university dental clinic, the findings may not be fully generalizable to other populations or clinical settings. Lastly, the simultaneous use of different anxiety scales, while enriching the analysis, may lead to variability in the reported prevalence across instruments, which should be interpreted with caution.
Despite these limitations, the results highlight the importance of understanding and addressing dental anxiety in daily practice. For many patients, fear of pain, previous negative experiences, and needle apprehension can turn a simple dental visit into a highly stressful experience. In response, dentists can make a meaningful difference by implementing effective strategies, such as explaining each procedure clearly, using distraction techniques such as music or virtual reality, and ensuring a more relaxed atmosphere in the office. Moreover, the fact that women presented higher levels of anxiety reinforces the need for an empathetic and personalized approach, providing a space where patients feel heard and understood. Incorporating tools such as the MDAS or SDAI in the initial assessment would allow early identification of individuals who require special anxiety management, thereby optimizing the patient experience and promoting better adherence to dental treatments. In the long term, this approach not only improves the relationship between dental professionals and patients but also contributes to better oral health outcomes in the population. Finally, our findings emphasize the importance of continuing education in patient psychology for dental professionals to improve treatment adherence and reduce avoidance of dental visits due to fear or anxiety.
Future research should include longitudinal and multicenter studies to evaluate changes in dental anxiety over time, as well as randomized controlled trials to assess the effectiveness of targeted interventions. These approaches would provide more precise and evidence-based guidelines for dental professionals in managing dental anxiety and enhancing the quality of patient care.
6 Conclusions
6.1 Prevalence of anxiety
A significant proportion of patients experienced varying levels of dental anxiety.
Gender Differences: Women exhibited higher levels of moderate and severe anxiety compared to men, according to all anxiety assessment tools (MDAS, SDAI, DAYMO).
6.2 Reliability of assessment tools
The MDAS and SDAI demonstrated high reliability (Cronbach's alpha coefficients of 0.905 and 0.875, respectively), while the DAYMO showed slightly lower reliability (Cronbach's alpha of 0.817).
6.3 Factors influencing anxiety
Fear of pain, previous negative dental experiences, and fear of needles were identified as the primary triggers of dental anxiety.
6.4 Correlation Among scales
A strong correlation was observed between the total scores of the SDAI, MDAS, and DAYMO scales, indicating consistency in measuring anxiety across different tools.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Universidade Santiago De Compostela. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
LC-B: Conceptualization, Data curation, Investigation, Project administration, Resources, Writing – original draft, Writing – review & editing. AP-J: Methodology, Validation, Writing – original draft, Writing – review & editing. CC-C: Methodology, Writing – original draft, Writing – review & editing. AO: Methodology, Writing – original draft, Writing – review & editing. PP-Y: Formal analysis, Writing – original draft, Writing – review & editing. BV: Formal analysis, Software, Visualization, Writing – original draft, Writing – review & editing. LS: Investigation, Writing – original draft, Writing – review & editing. CR: Data curation, Writing – original draft, Writing – review & editing. DO: Visualization, Writing – original draft, Writing – review & editing. MP-S: Conceptualization, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
The authors would like to thank the University of Guayaquil for the opportunity to conduct this research and the University of Santiago of Compostela.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Skaret E, Kvale G, Raadal M. General self-efficacy, dental anxiety and multiple fears among 20-year-olds in Norway. Scand J Psychol. (2003) 44(4):331–7. doi: 10.1111/1467-9450.00352
2. Tickle M, Milsom K, Crawford FIJ, Aggarwal VR. Predictors of pain associated with routine procedures performed in general dental practice. Community Dent Oral Epidemiol. (2012) 40(4):343–50. doi: 10.1111/j.1600-0528.2012.00673.x
3. John MT. Dental anxiety is considerably associated with pain experience during dental procedures. J Evid Based Dent Pract. (2013) 13(1):29–30. doi: 10.1016/j.jebdp.2013.01.002
4. Thoma MV, Zemp M, Kreienbühl L, Hofer D, Schmidlin PR, Attin T, et al. Effects of music listening on pre-treatment anxiety and stress levels in a dental hygiene recall population. Int J Behav Med. (2015) 22(4):498–505. doi: 10.1007/s12529-014-9439-x
5. Jeddy N, Nithya S, Radhika T, Jeddy N. Dental anxiety and influencing factors: a cross-sectional questionnaire-based survey. Indian J Dent Res. (2018) 29(1):10–5. doi: 10.4103/ijdr.IJDR_33_17
6. Al-Namankany A, de Souza M, Ashley P. Evidence-based dentistry: analysis of dental anxiety scales for children. Br Dent J. (2012) 212(5):219–22. doi: 10.1038/sj.bdj.2012.174
7. Ayer WA. Psychology and Dentistry: Mental Health Aspects of Patient Care. New York, NY: Psychology Press (2005). p. 174.
8. de Jongh A, Muris P, ter Horst G, van Zuuren F, Schoenmakers N, Makkes P. One-session cognitive treatment of dental phobia: preparing dental phobics for treatment by restructuring negative cognitions. Behav Res Ther. (1995) 33(8):947–54. doi: 10.1016/0005-7967(95)00027-U
9. Carrillo-Diaz M, Crego A, Armfield JM, Romero-Maroto M. Assessing the relative efficacy of cognitive and non-cognitive factors as predictors of dental anxiety. Eur J Oral Sci. (2012) 120(1):82–8. doi: 10.1111/j.1600-0722.2011.00924.x
10. Scandurra C, Gasparro R, Dolce P, Bochicchio V, Muzii B, Sammartino G, et al. The role of cognitive and non-cognitive factors in dental anxiety: a mediation model. Eur J Oral Sci. (2021) 129(4):e12793. doi: 10.1111/eos.12793
11. Farzanegan P, Ghasempour M, Massoodi A, Shirafkan H. Correlation between child’s dental fear and anxiety symptoms and evaluating factors associated with dental fear. Health Sci Rep. (2025) 8(5):e70879. doi: 10.1002/hsr2.70879
12. Klingberg G, Broberg AG. Dental fear/anxiety and dental behaviour management problems in children and adolescents: a review of prevalence and concomitant psychological factors. Int J Paediatr Dent. (2007) 17(6):391–406. doi: 10.1111/j.1365-263X.2007.00872.x
13. Hong F, Chen P, Yu X, Zeng J. Prevalence of dental anxiety among adults in China: a meta-analysis. Hua Xi Kou Qiang Yi Xue Za Zhi. (2023) 41(1):88–98. doi: 10.7518/hxkq.2023.01.012
14. Silveira ER, Cademartori MG, Schuch HS, Armfield JA, Demarco FF. Estimated prevalence of dental fear in adults: a systematic review and meta-analysis. J Dent. (2021) 108:103632. doi: 10.1016/j.jdent.2021.103632
15. Winkler CH, Bjelopavlovic M, Lehmann KM, Petrowski K, Irmscher L, Berth H. Impact of dental anxiety on dental care routine and oral-health-related quality of life in a German adult population-A cross-sectional study. J Clin Med. (2023) 12(16):5291. doi: 10.3390/jcm12165291
16. Thomson WM, Broadbent JM, Locker D, Poulton R. Trajectories of dental anxiety in a birth cohort. Community Dent Oral Epidemiol. (2009) 37(3):2019. doi: 10.1111/j.1600-0528.2009.00473.x
17. Alsakr A, Gufran K, Alqahtani AS, Alkharaan H, Abushanan A, Alnufaiy B, et al. Pre-treatment and post-treatment dental anxiety in patients visiting intern dental clinic. Medicina (B Aires). (2023) 59(7):1284. doi: 10.3390/medicina59071284
18. Corah NL. Development of a dental anxiety scale. J Dent Res. (1969) 48(4):596. doi: 10.1177/00220345690480041801
19. Humphris GM, Morrison T, Lindsay SJ. The modified dental anxiety scale: validation and United Kingdom norms. Community Dent Health. (1995) 12(3):143–50.7584581
20. Freeman R, Clarke HMM, Humphris GM. Conversion tables for the MDAS and modified dental anxiety scales. Community Dent Health. (2007) 24(1):49–54.17405471
21. Gale EN. Fears of the dental situation. J Dent Res. (1972) 51(4):964–6. doi: 10.1177/00220345720510044001
22. Carter AE, Carter G, Boschen M, AlShwaimi E, George R. Pathways of fear and anxiety in dentistry: a review. World J Clin Cases. (2014) 2(11):642–53. doi: 10.12998/wjcc.v2.i11.642
23. Porritt J, Buchanan H, Hall M, Gilchrist F, Marshman Z. Assessing children’s dental anxiety: a systematic review of current measures. Community Dent Oral Epidemiol. (2013) 41(2):130–42. doi: 10.1111/j.1600-0528.2012.00740.x
24. Khan SDAA, Alqannass NM, Alwadei MM, Alnajrani MD, Alshahrani ZM, Al Alhareth AY, et al. Assessment of the relationship between dental anxiety and oral health-related quality of life. J Pharm Bioallied Sci. (2021) 13(Suppl 1):S359–62. doi: 10.4103/jpbs.JPBS_742_20
25. Corah NL, Gale EN, Illig SJ. Assessment of a dental anxiety scale. J Am Dent Assoc. (1978) 97(5):816–9. doi: 10.14219/jada.archive.1978.0394
26. Coolidge T, Chambers MA, Garcia LJ, Heaton LJ, Coldwell SE. Psychometric properties of Spanish-language adult dental fear measures. BMC Oral Health. (2008) 8(1):15. doi: 10.1186/1472-6831-8-15
27. Ogawa M, Sago T, Furukawa H. The reliability and validity of the Japanese version of the modified dental anxiety scale among dental outpatients. ScientificWorldJournal. (2020) 2020:8734946. doi: 10.1155/2020/8734946
28. Nicolas E, Collado V, Faulks D, Bullier B, Hennequin M. A national cross-sectional survey of dental anxiety in the French adult population. BMC Oral Health. (2007) 7(1):12. doi: 10.1186/1472-6831-7-12
29. Yuan S, Freeman R, Lahti S, Lloyd-Williams F, Humphris G. Some psychometric properties of the Chinese version of the modified dental anxiety scale with cross validation. Health Qual Life Outcomes. (2008) 6:22. doi: 10.1186/1477-7525-6-22
30. Facco E, Gumirato E, Humphris G, Stellini E, Bacci C, Sivolella S, et al. Modified dental anxiety scale: validation of the Italian version. Minerva Stomatol. (2015) 64(6):295–307.26486204
31. Coolidge T, Arapostathis KN, Emmanouil D, Dabarakis N, Patrikiou A, Economides N, et al. Psychometric properties of Greek versions of the modified MDASDental anxiety scale [MDAS] and the dental fear survey [DFS]. BMC Oral Health. (2008) 8:29. doi: 10.1186/1472-6831-8-29
32. Aartman IHA. Reliability and validity of the short version of the dental anxiety inventory. Community Dent Oral Epidemiol. (1998) 26(5):350–4. doi: 10.1111/j.1600-0528.1998.tb01972.x
33. Supriya , Singh R, Ahsan A. Relevance of emotion of anxiety and fear of dentistry as motivational conflict in oral health behaviors. J Contemp Dent Pract. (2024) 25(3):280–8. doi: 10.5005/jp-journals-10024-3643
34. Yeung AWK, Lee JCM, Tanabe HC, Ng SKS, Khong PL, Leung WK, et al. Short version dental anxiety inventory score may predict the response in the insular Cortex to stimuli mimicking dental treatment. Front hum Neurosci. (2019) 13:204. doi: 10.3389/fnhum.2019.00204
35. Chi SI. What is the gold standard of the dental anxiety scale? J Dent Anesth Pain Med. (2023) 23(4):193–212. doi: 10.17245/jdapm.2023.23.4.193
36. Rahman A, Muktadir MG. SPSS: an imperative quantitative data analysis tool for social science research. Int J Res Innov Soc Sci. (2021) 5(10):300–2.
37. Muneer MU, Ismail F, Munir N, Shakoor A, Das G, Ahmed AR, et al. Dental anxiety and influencing factors in adults. Healthcare. (2022) 10(12):2352. doi: 10.3390/healthcare10122352
38. Gil-Abando G, Medina P, Signorini C, Casañas E, Navarrete N, Muñoz-Corcuera M. Assessment of clinical parameters of dental anxiety during noninvasive treatments in dentistry. Int J Environ Res Public Health. (2022) 19(17):11141. doi: 10.3390/ijerph191711141
39. Metin-Gürsoy G, Haciomeroglu AB, Kale-Varlık S, Tortop T. Evaluation of the relationship between anxiety levels and dental appearance. J Clin Pediatr Dent. (2023) 47(4):40–5. doi: 10.22514/jocpd.2023.018
40. Sivaramakrishnan G, Makki H, AlDallal S, Alaswad Z, Sultan E, Ahmed S, et al. The variables associated with dental anxiety and their management in primary care dental clinics in Bahrain: a cross-sectional study. BMC Oral Health. (2022) 22(1):137. doi: 10.1186/s12903-022-02173-7
41. White AM, Giblin L, Boyd LD. The prevalence of dental anxiety in dental practice settings. J Dent Hyg. (2017) 91(1):30–4.29118148
42. Alemany-Martínez A, Valmaseda-Castellón E, Berini-Aytés L, Gay-Escoda C. Hemodynamic changes during the surgical removal of lower third molars. J Oral Maxillofac Surg. (2008) 66(3):453–61. doi: 10.1016/j.joms.2007.06.634
43. Caltabiano ML, Croker F, Page L, Sklavos A, Spiteri J, Hanrahan L, et al. Dental anxiety in patients attending a student dental clinic. BMC Oral Health. (2018) 18(1):48. doi: 10.1186/s12903-018-0507-5
44. Saatchi M, Abtahi M, Mohammadi G, Mirdamadi M, Binandeh ES. The prevalence of dental anxiety and fear in patients referred to isfahan dental school, Iran. Dent Res J (Isfahan). (2015) 12(3):248–53.26005465
45. Erten H, Akarslan ZZ, Bodrumlu E. Dental fear and anxiety levels of patients attending a dental clinic. Quintessence Int. (2006) 37(4):304–10.16594362
46. do Nascimento DL, da Silva Araújo AC, Gusmão ES, Cimões R. Anxiety and fear of dental treatment among users of public health services. Oral Health Prev Dent. (2011) 9(4):329–37.22238731
47. Deogade SC, Suresan V. Psychometric assessment of anxiety with the modified dental anxiety scale among central Indian adults seeking oral health care to a dental school. Ind Psychiatry J. (2016) 25(2):202–9. doi: 10.4103/ipj.ipj_16_16
48. Appukuttan D, Subramanian S, Tadepalli A, Damodaran LK. Dental anxiety among adults: an epidemiological study in south India. N Am J Med Sci. (2015) 7(1):13–8. doi: 10.4103/1947-2714.150082
49. Appukuttan DP, Tadepalli A, Cholan PK, Subramanian S, Vinayagavel M. Prevalence of dental anxiety among patients attending a dental educational institution in Chennai, India–a questionnaire-based study. Oral Health Dent Manag. (2013) 12(4):289–94.24390031
50. Liu Y, Huang X, Yan Y, Lin H, Zhang J, Xuan D. Dental fear and its possible relationship with periodontal status in Chinese adults: a preliminary study. BMC Oral Health. (2015) 15:18. doi: 10.1186/1472-6831-15-18
51. Murillo-Benítez M, Martín-González J, Jiménez-Sánchez MC, Cabanillas-Balsera D, Velasco-Ortega E, Segura-Egea JJ. Association between dental anxiety and intraoperative pain during root canal treatment: a cross-sectional study. Int Endod J. (2020) 53(4):447–54. doi: 10.1111/iej.13245
52. Giri J, Pokharel PR, Gyawali R, Bhattarai B. Translation and validation of modified dental anxiety scale: the Nepali version. Int Sch Res Notices. (2017) 2017:5495643. doi: 10.1155/2017/5495643
53. Kassem El Hajj H, Fares Y, Abou-Abbas L. Assessment of dental anxiety and dental phobia among adults in Lebanon. BMC Oral Health. (2021) 21(1):48. doi: 10.1186/s12903-021-01409-2
54. Fayad MI, Elbieh A, Baig MN, Alruwaili SA. Prevalence of dental anxiety among dental patients in Saudi Arabia. J Int Soc Prev Community Dent. (2017) 7(2):100–4. doi: 10.4103/jispcd.JISPCD_19_17
55. Bahammam MA, Hassan MH. Validity and reliability of an Arabic version of the modified dental anxiety scale in Saudi adults. Saudi Med J. (2014) 35(11):1384–9.25399217
56. Zhang X, Wang B, Qiao SC, Gu YX, Shi JY, Lai HC. A study on the prevalence of dental anxiety, pain perception, and their interrelationship in Chinese patients with oral implant surgery. Clin Implant Dent Relat Res. (2019) 21(3):428–35. doi: 10.1111/cid.12779
Keywords: dental anxiety, anxiety factors, prevalence, oral health, psychological factors
Citation: Chauca-Bajaña L, Pérez-Jardón A, Carpio-Cevallos C, Ordoñez Balladares A, Proaño-Yela P, Velásquez Ron B, Siguencia Suarez LJ, Romo Olvera CV, Orellana Guerrero D and Pérez-Sayáns M (2025) Factors associated with dental anxiety in patients treated at an integrated dental clinic: a cross-sectional study. Front. Oral Health 6:1689805. doi: 10.3389/froh.2025.1689805
Received: 20 August 2025; Accepted: 5 September 2025;
Published: 25 September 2025.
Edited by:
Luis Proença, Instituto Universitário Egas Moniz, PortugalReviewed by:
Roberta Gasparro, University of Naples Federico II, ItalyTinela Panaite, Grigore T. Popa University of Medicine and Pharmacy, Romania
Copyright: © 2025 Chauca-Bajaña, Pérez-Jardón, Carpio-Cevallos, Ordoñez Balladares, Proaño-Yela, Velásquez Ron, Siguencia Suarez, Romo Olvera, Orellana Guerrero and Pérez-Sayáns. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Ordoñez Balladares, YWRvcmRvbmV6YkB1YmUuZWR1LmVj
†These authors have contributed equally to this work
‡ORCID:
Luis Chauca-Bajaña
orcid.org/0000-0002-8713-951X
Alba Pérez-Jardón
orcid.org/0000-0001-5174-8922
Carlos Carpio-Cevallos
orcid.org/0000-0002-4315-7230
Andrea Ordoñez Balladares
orcid.org/0000-0002-6559-4597
Patricio Proaño-Yela
orcid.org/0000-0002-7137-2050
Byron Velásquez Ron
orcid.org/0000-0001-5660-3941
Leonardo Javier Siguencia Suarez
orcid.org/0000-0001-7528-8502
Carla Verenice Romo Olvera
orcid.org/0000-0003-4654-8875
Diana Orellana Guerrero
orcid.org/0000-0003-4826-7655
Mario Pérez-Sayáns
orcid.org/0000-0003-2196-9868