 Víctor Beltrán1,2,3,4*
Víctor Beltrán1,2,3,4* Leonardo López5
Leonardo López5 Pablo Acuña-Mardones1,2,4,6Roberto Silva7Claudia Acevedo1Jaime Bustos8Claudio Alarcón8
Pablo Acuña-Mardones1,2,4,6Roberto Silva7Claudia Acevedo1Jaime Bustos8Claudio Alarcón8 Randal von Marttens9
Randal von Marttens9 Iris Espinoza10
Iris Espinoza10 Rodrigo Mariño11,12,13*
Rodrigo Mariño11,12,13*
- 1Universidad de La Frontera, Centro de Investigación e Innovación en Odontología Clínica (CIDIC), Facultad de Odontología, Temuco, Chile
- 2Universidad de La Frontera, Centro de Excelencia en Medicina Traslacional (CEMT), Temuco, Chile
- 3Universidad de La Frontera, Núcleo Científico y Tecnológico en Biorecursos (BIOREN), Temuco, Chile
- 4Universidad de La Frontera, Centro de Excelencia en Física e Ingeniería en Salud (CFIS), Facultad de Ingeniería y Ciencias, Temuco, Chile
- 5Universidad de La Frontera, Instituto de Informática Educativa, Temuco, Chile
- 6Universidad de La Frontera, Doctorado en Ciencias Morfológicas, Facultad de Medicina, Temuco, Chile
- 7Fuerza Aérea de Chile, Santiago, Chile
- 8Universidad de La Frontera, Departamento de Ingeniería Industrial y de Sistemas, Facultad de Ingeniería y Ciencias, Temuco, Chile
- 9Universidad de La Frontera, Programa de Magíster en Odontología, Facultad de Odontología, Temuco, Chile
- 10Departamento de Patología y Medicina Oral, Facultad de Odontología, Universidad de Chile, Santiago, Chile
- 11Monash Health, Monash Health Dental Services, Dandenong, VIC, Australia
- 12Melbourne Dental School, The University of Melbourne, Parkville, VIC, Australia
- 13Department of Conservative Dentistry and Oral Health, Riga Stradiņš University, Riga, Latvia
Objectives: The aim of this study is to provide initial evidence of the impact of teledentistry, using satellite communication technology to improve access to oral healthcare in underserved populations in rural and remote areas.
Methods: A pilot model of teledentistry care for older adults, incorporating technological and clinical components with a satellite solution for areas without connectivity, was evaluated in the Los Lagos Region, Chile. This was classified in terms of the sequential industrial modernization framework and technology types.
Results: Thirty-one older adults participated in this evaluation, with a mean age of 66.3 years. The majority (56%) had not visited a dentist in over five years. The average DMFT index was 24.2 teeth, with almost half of the participants (45.4%) presenting unmet restorative needs, and 83.3% required prosthetic appliances. A large proportion of the sample requiring a referral for emergency treatment. Most consultations (84%) were for emergency care, predominantly due to dental pain. The strategy was classified as part of the Industry 4.0 trend of modernization, with elements of the Industry 3.0.
Conclusion: This piloted model of care can enhance care access and improve health outcomes for isolated populations. This innovative model of care ensured that all participants received oral health assessments, addressing the need for the systematic identification of older adults at risk of oral health emergencies. Future directions could include the integration of contextual artificial intelligence and expansion into other underserved areas, reinforcing the role of digital ecosystems in enhancing access to care and reducing health disparities.
1 Introduction
Around the world, significant disparities in health outcomes between urban and rural populations persist, particularly in relation to oral healthcare (1–4). Access to oral healthcare in rural areas is often constrained by geographical and transportation barriers, local shortages of oral health professionals, and inadequate healthcare infrastructure (5–8). Addressing these challenges, along with broader socioeconomic inequities and social determinants of health, is essential to improving access and reducing inequalities in oral health services. In particular, the geographic isolation of rural communities presents unique and persistent obstacles to equitable oral healthcare delivery.
In recent years, the landscape of healthcare delivery has undergone profound transformation. The rise of digital health and telehealth platforms offers several advantages for health promotion and serves as an effective point of entry for patients into the public oral healthcare system (9, 10). This also facilitates the identification of at-risk individuals, overcoming traditional geographic and logistical barriers (11–13), and provides valuable opportunities for teaching and research. This approach was previously implemented in two studies that applied teledentistry models for older adults living in remote areas of Chile. The first implemented an asynchronous (store-and-forward) teledentistry network during the COVID-19 pandemic (14), in which general dentists collected clinical data and digital images in mobile units and referred cases remotely to specialists. This model effectively maintained access to oral care for older adults with urgent or priority needs. The subsequent study extended the model to rural Mapuche communities (15), reporting a high burden of oral disease and demonstrating the usefulness of remote specialist input in reducing travel barriers.
However, despite the potential of telehealth to bridge gaps in access to oral healthcare, many rural and remote communities continue to face significant challenges that hinder the effective implementation of these solutions. A major barrier to the successful deployment of telemedicine in such regions is the lack of reliable internet connectivity. Rural and remote areas are often characterized by sparse populations and vast distances, which can make it economically unfeasible for investment in the necessary infrastructure to provide internet services. As a result, residents in these communities are left without access to essential telehealth services, thereby exacerbating existing health disparities. Furthermore, the limitations in connectivity not only affect telehealth but also hinder the overall socioeconomic development of these areas, as access to information and communication technologies (ICT) is increasingly recognized as a critical determinant of health and well-being (16).
Satellite communication offers a practical solution to providing internet access where traditional networks fail. The integration of satellite technology in teledentistry can serve as an essential element of reducing the isolation experienced in rural areas. This study aims to generate preliminary evidence for using satellite communication technology to support the expansion of digital oral health models, improving access to care for rural and remote populations in Chile, particularly for older adults with limited internet connectivity. Additionally, to highlight the digital transformation and its relation to industrial revolutions, the study will examine the technologies developed for the system within the framework of Industry 4.0 and the Sequential Industrial Modernisation Framework to evaluate its potential contribution to the professional practice of dentistry.
2 Materials and methods
This section is organized into three parts. The first details a teledentistry care model developed for older adults in remote areas, technological architecture and security and the satellite solution aimed at providing connectivity. The second part outlines the clinical assessment methods. The last part describes the classification in terms of the Industry 4.0, the sequential industrial modernization framework and technology types, used to analyse how innovative digital oral health applications can improve access to care using.
2.1 Part 1 integrated teledentistry ecosystem for older adults
The teledentistry care model developed for older adults integrates technological, organisational, and clinical components to address the specific challenges faced by this vulnerable population, particularly in remote areas with limited access to oral health care. The structure of the model is based on a protocolised sequence of steps, starting with the identification and recruitment of older adult patients. Recruitment of participants was conducted in collaboration with institutional and community organizations representative of the rural population in Chile. Primarily, the National Service for Older Adults (SENAMA: In Spanish: Servicio Nacional del Adulto Mayor). SENAMA's regional database provides up-to-date, comprehensive information about older adults. Identification of potential participants was based on the inclusion criteria applied to these records and data from local community organizations that periodically assess health needs, including oral health needs. These organizations generate lists for priority healthcare, which were supplemented by interviews with local older adults' associations, community leaders, and local teams, confirming eligibility and willingness to participate. Thus, recruitment was systematic, with institutional support and active community participation, ensuring a representative and contextualized sample.
Patient admission included collecting sociodemographic and medical information via remote or in-person interviews. This stage was limited to registration and scheduling of visits. Clinical care was provided in mobile units, community centers, or in the patient's homes, tailored to patients' mobility levels. Dentists performed examinations using digital tools, enabling synchronous or asynchronous referrals to specialists (e.g., oral pathologist, periodontologist, radiologist, geriatrics, etc.).
The Teleplatform for Geriatric and Dental Specialties (In Spanish: Teleplataforma de Especialidades Geriátricas y Odontológicas (TEGO) formed the core infrastructure of the model, facilitating the management of clinical information, teleconsultations, and logistical aspects such as appointment scheduling and monitoring patient follow-ups, enhancing decision-making and continuity of care for older adults. The model prioritises connectivity within the care network by allowing general dentists to share information with specialists and remote support teams. Through virtual meetings, screen sharing, and secure messaging, it facilitated case registration, follow-up, and the export of clinical reports for effective oral health management.
2.2 Operational flow and structure of the TEGO platform
The TEGO platform operated as a web-based system that facilitates the management and implementation of dental care for older adults through digital modules that allow the storage of anamnesis records for patients treated in mobile units (14). The operational process begun with the enrolment of older adults in the TEGO platform by trained staff, who registered and scheduled mobile care appointments in their areas of residence. The platform recognises user profiles with specific functionalities according to their responsibilities.
During the face-to-face consultations, a digital anamnesis was prepared, which was organised in a clinical file composed of a general anamnesis, medical-geriatric anamnesis, and dental-geriatric anamnesis. The dental-geriatric anamnesis was supported by a virtual 3D phantom, allowing the integration of observations, images, or photographic records at specific anatomical sites, simulating the standardised orofacial structure of an adult. This record facilitated communication between the general dentist and specialists from various dental and medical-geriatric fields.
The workflow concluded in the clinical records module, where all generated information converged and allowed interaction between the general dental practitioner and the assigned specialists, who may supplement the information with medical examinations and monitor the patient's progress. The TEGO platform has an associated mobile app focused on oral health education interventions for older adults.
2.3 Technological architecture and security
The TEGO platform utilized a classical three-layer web architecture, ensuring a secure and scalable technological environment for managing clinical information. The Presentation Layer (FrontEnd), developed with React.js, featured user-friendly interface and integrates 3D models, enhancing visualization and communication between dentists and specialists through interactive representations of anatomical structures. The Business Logic Layer, built on Node.js, managed application logic, data interchange, and security, using Express for efficient communication, MySQL for secure database interaction, bcrypt for password encryption, and jsonwebtoken for access control. Only authorised general dentists and specialists can view or modify patient records. Authentication is role-based and managed through encrypted credentials using bcrypt and jsonwebtoken protocols; no external or public users can access clinical data.
The Data Layer stored clinical and administrative information in a MariaDB database on a cloud-based server, ensuring data confidentiality and integrity with robust security measures, including encryption and regular updates. Additionally, the TEGO mobile application, created with Flutter, supports oral health education and preventative interventions, allowing patients access to appointment information and educational resources while promoting adherence to treatment (17). Overall, the platform emphasizes security and compliance with health information protection regulations.
The TEGO platform was designed for modular expansion and scalability, facilitating the addition of new clinical modules and integration with external health information systems, such as national health registries. Its technological stack ensures that future needs, including increased user capacity and artificial intelligence algorithms for clinical decision support, could be accommodated without affecting performance or security.
2.4 Satellite connectivity for remote areas
To ensure access in areas without terrestrial connectivity, a portable satellite ground station was available to support real-time tele-dentistry. This system included a 1.8 m Ku-band parabolic antenna, Block Up Converter (BUC), Low Noise Block downconverter (LNB), SCPC modem, Cisco switch, two IP phones, coaxial/RF cabling, and tactical transport cases. The system operated on a 15 MHz channel within a 36 MHz transponder, delivering an effective throughput of approximately 10 Mbps and a latency of 550 ms (See Table 1).
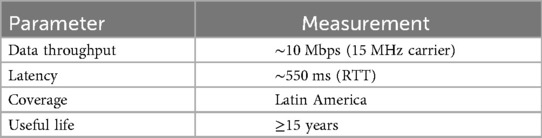
Table 1. Performance metrics of the satellite system.
Communications were provided via the geostationary satellite Eutelsat 117 West B, positioned at 117° W and operating in the Ku band. Launched in 2016 on the Boeing BSS 702SP platform, with a useful life of over 15 years, it features 48 transponders and coverage across Mexico, Central America, the Caribbean, the Andean region, and the Southern Cone. The system provides robust, reliable, and continuous coverage for the operation of TEGO in remote locations. The Eutelsat 117 West B satellite provides complete coverage of continental Chile, including the municipality of Cochamó where data were collected; therefore, the entire study area was within the operational footprint of the portable ground station.
2.5 Part 2 clinical assessments
This assessment employed a cross-sectional design. With the ethics' approval granted by the Ethics Committee of the Universidad de La Frontera (UFRO) (ID: 169/23, approved on 18 March 2024), residents of the municipality of Cochamó in the Los Lagos Region of Chile were invited to participate in this assessment. This location was selected due to the area's limited access to the internet and for reasons of convenience and the working relationship established with the municipality. Data was collected between September and October 2024.
The inclusion criteria consisted of individuals aged 60 years or older, able to provide informed consent and follow instructions. Participants were dentate, defined as having one or more natural teeth. By focusing on dentate participants, the study aimed to explore how environmental factors, such as access to oral healthcare, and individual contextual factors, like socioeconomic status, influenced current oral health status. Informed consent was obtained from all participants prior to their inclusion in the study.
Oral examinations were carried out by one trained and calibrated dental examiner (RvM). The examiner received training and an online calibration exercise involving the review of 20 cases. The Intra-examiner reliability, measured using Cohen's Kappa statistics, exceeded 0.90, indicating an almost perfect level of agreement, as per Landis and Koch criteria (18).
Oral examinations were conducted in an approved by the regional Health Authority mobile dental clinic. Standardization of conditions during evaluations and treatments was ensured, including appropriate lighting, infection control protocols were followed in accordance with current health regulations to provide a safe environment for the evaluations.
Data collection comprised assessments of the following domains:
1. Sociodemographic characteristics: Participants’ age, sex, and educational level were recorded, categorized as “No formal education or complete primary education or less,” “Incomplete or complete secondary education,” and “Post-secondary education.”
2. Use of Oral Healthcare Services: Dental service utilization was assessed by participants indicating the time since their last dental visit, with response options: “12 months or less”, “12 months to 2 years”, “2 to 4 years”, “more than 4 years.” For this analysis, dental attendance was categorized as having visited a dentist within the last 12 months (Yes/No).
3. Clinical Data and Oral Health Status: Clinical data included:
a. Dental status: the number of decayed teeth (DT), filled teeth (FT), and the number of natural teeth present were assessed according to the World Health Organization criteria for Oral Health Surveys (19). To further explore dental health status, the dental caries assessment included the proportion of unmet restorative needs. A restorative unmet normative needs index was calculated by dividing the number of decayed surfaces by the total number of decayed and filled surfaces: [DS/(DS + FS)] (20).
b. Prosthetic Status: Evaluated normative need for dental prostheses, categorized as “Not needed or in good condition,” “Needs repairs,” “Needs one” or “Replacement needed.”
c. Periodontal status was assessed using three indicators: 0 = sound; 1 = visual presence of gingivitis; 2 visual and tactile presence of periodontitis, using the CPI Probe (19).
d. Urgency of Treatment: Recorded in four urgency levels: 1 = No urgency; 2 = Low urgency; 3 = Advanced urgency; and 4 = High urgency (19).
During clinical examinations, patients experiencing pain were treated without delays to in order to relieve their discomfort, including palliative care when needed. Cases requiring further treatment were referred to the oral health specialty clinic at the University of La Frontera, to ensure timely and appropriate follow-up. Moreover, participants had access to treatment and prosthetic rehabilitation at no cost to them. These services were provided under the comprehensive care program, ensuring that all diagnosed patients received necessary attention, including prosthetics, through institutional and public resources.
The costs of these referrals were either waived or covered by the project. Treatments were provided at the UFRO dental specialties clinics, thus ensuring timely and appropriate follow-ups.
The Statistical Analysis presents basic descriptive statistics for selected sociodemographic factors, dental status, unmet restorative and prosthetics needs, and periodontal status. Descriptive statistics included sociodemographic and oral health data, including means, standard deviations, frequency distributions. All statistical analyses were performed using SPSS Statistics (Version 30.0).
2.6 Part 3 classification in terms of the industry 4.0, the sequential industrial modernization framework and technology types
Industry 4.0, initiated in Germany in 2011 as a governmental program for industrial modernization, represents the integration of emerging technologies across various sectors, including, healthcare (21), education (22), and the pharmaceuticals (23, 24), emphasizing the digital transformation of traditional professional practices. The concept has led to terms like Industry 3.0 and Industry 5.0, associated with the Third and Fifth Industrial Revolutions. These terms have been used to classify developments and practices in the Sequential Industrial Modernisation Framework (25–27).
The classification in the study categorized technologies into five types based on their inputs and outputs: T1.0 (non-electrical), T2.0 (analogue electric), T3.0 (digital data), T4.0 (digital information), and T5.0 (digital contextual intelligence). Each technology was analysed according to its characteristics and classified across different industry levels. For example, “electronics” applies to both Industry 2.0 and Industry 3.0. The system's classification is determined by scoring, identifying its association with one or more Industry levels and Technology Types (25–27).
In this work the developed platform was analysed in terms of the Industry 4.0 concept in the Sequential Industrial Modernization Framework, and by a system-theory-based approach that considers the characteristics of its inputs and outputs (25–27).
3 Results
3.1 Clinical assessments
A total of 31 older adults agreed to participate in the study. Of these, 7 were excluded due to incomplete data. The remaining 24 participants were clinically examined and interviewed. Mean age was 66.3 (SD 4.7) years, with 61.4% women. According to the time interval since the last dental visit: 28% reported having been to the dentist in the previous 12 months. Another 16.0% reported their last visit to the dentist being more than 12 months and less than two years ago. More importantly, more than half of the sample (56.0%) reported not having been to the dentist within the last five years (20.0%), or longer (36.0%).
The mean number of teeth with dental caries history (i.e., DMFT index) was 24.2 (SD 4.0) teeth. Unmet restorative needs were high. A significant portion of the participants (45.4%) reported unmet restorative needs. Additionally, the majority of participants (83.3%) required a prosthetic appliance; of these, 85% indicated needs for repairs, replacements, or that one to be made, highlighting a continuous cycle of unmet needs that could lead to further complications in oral health.
Regarding the periodontal status, two of participants were found to have no periodontal needs (8.3%). Gingivitis was observed in 16 participants (66.7%%), and six (25.0%) of the sample had periodontitis.
Data show that a large majority (84%) of consultations were for emergency care, with two-thirds of these emergencies due to dental pain. Consequently, by level of emergency, the majority had some level of emergency, although the majority was low level (83.9). Additionally, 9.7% of the participants showed no emergency. Three participants, (9.7%) were able to receive an online referral and consultation with an oral pathologist for potentially life-threatening conditions. All conditions were documented and indexed in a standardized 3D model of oral soft tissues and mucosa (Figure 1).
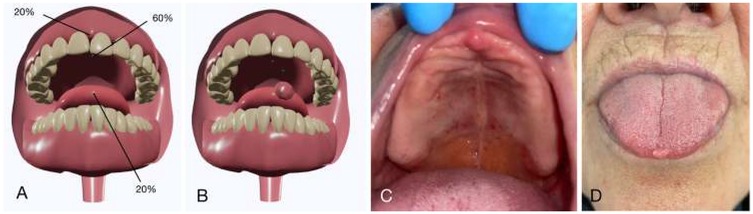
Figure 1. Localisation of intraoral lesions identified during examination. (A,B) 3D models showing lesion sites and frequencies. (C,D) Clinical records illustrating lesions at each location.
3.2 Satellite connection
As previously stated, the direct outcome concerning satellite coverage within the study area demonstrated enhanced access to oral healthcare services reliant on this technology. In Chile, the area encompassed by the satellite signal corresponds to 100% of the continental territory, including the Cochamó municipality. While there are some attenuation effects towards the extreme southern regions, these phenomena do not occur at the latitude of our area of interest.
Furthermore, there were no reported service failures during the period of data collection under analysis. Although some reports of intense solar events were recorded, resulting in G3-level geomagnetic storms, which may induce temporary disturbances in communications and minor disruptions in links, no critical failures were reported for the Eutelsat 117° West satellite. The system's resilience and redundancy allowed normal operations during data collection.
3.3 Classification in terms of the industry 4.0 concept
The technologies that are part of the developed system were identified and then classified (Table 2). The results show that most of the identified elements are part of Industry 4.0 (7/17), followed by Industry 3.0 (3/10). This allows classification of the presented system as part of the Industry 4.0 trend of modernization, with elements of the Industry 3.0.

Table 2. Identification of technologies and industry level associated.
The input-output signals of the platform were identified from the point of view of the professional dentist interacting with the system. From these inputs and outputs, only digital technology was considered, as the platform requires interaction through the web-based platform. From this perspective, the system could also be considered as part of the Industry 4.0 levels.
4 Discussion
The clinical data presented several noteworthy insights regarding the oral health needs of participants. They suggest variability in the levels of access to oral healthcare, for example, only 28% had visited a dentist in the last 12 months, which is considered an optimal dental visits frequency (28). More alarmingly, 56.0% had not visited a dentist in at least five years. Nonetheless, with the implementation of this model of care, even those with less-than-optimal dental visits frequency received a dental examination and an assessment of their oral health needs.
A critical unmet need was the lack of systematic identification for older adults “at risk” of dental emergencies due to dental pain. The findings highlight persistent inequities in access to dental care. Although these emergencies may not be life-threatening, they can greatly affect an individual's quality of life, nutrition, and overall well-being. The emergency data does not exclude those with more advanced periodontal disease (25%), whose conditions could trigger acute episodes, suggesting many seek care reactively, potentially worsening their dental health over time. In addition to emergency referrals, a large portion of participants required referrals to general practitioners for preventive, restorative, periodontal, oral surgery, and prosthodontic care.
Treating dental emergencies poses significant costs for both individuals and society, particularly affecting older adults in rural and remote areas who are less likely to receive regular oral examinations. This leads to missed opportunities for early identification and for addressing their needs under conventional care models, even where teledentistry is available. It was only when the model was enhanced to include the alternative of satellite connectivity that these challenges were overcame, enhancing equitable access to oral healthcare services in underserved regions. This integration ensures that patients receive necessary care through real-time consultations, remote diagnoses, and ongoing monitoring, effectively meeting the oral health needs of those with limited access to traditional healthcare services.
Although Chile leads Latin America in internet connectivity (29), a significant proportion of the population, especially in rural and remote areas, remains uncovered, mainly due to the lack of broadband infrastructure rather than cost alone. According to national reports, in some rural regions, broadband coverage does not exceed 50%, and the challenge of deploying infrastructure in isolated areas is a major barrier to universal connectivity (30).
The present initiative was successfully applied in a study aimed at evaluating teledentistry for older adults residing in remote regions of Chile. The initiative builds on previous experiences (31) by establishing a model in which the initial contact with the healthcare system occurs in areas with limited or no connectivity. The study also included the provision of oral health care information and emergency dental services for those requiring immediate attention.
Developing or enhancing digital models could benefit those living in rural areas, with no permanent access to oral health services. Additionally, it is envisaged that, based on the results of this pilot model, dental public health strategies and oral health professional training programs could be developed. Accordingly, this study constitutes an initial yet significant contribution to research into oral health promotion. It complements existing data on oral health among older adults and offers implications for policy, research, and practice regarding the promotion of oral health and the delivery of care for this population. Furthermore, it is anticipated that the results of this pilot model will inform the development of public dental health strategies and training programmes for oral health professionals.
The present study also highlights the potential of targeted and tailored interventions for the reduction of discrimination and inequalities under the Leave No One Behind principle, a central component of the 2030 Sustainable Development and its Sustainable Development Goals (SDGs) agenda (32, 33). In fact, digital health is related to several United Nations SDG goals, including education (Goal 4), gender equality (Goal 5), infrastructure (Goal 9—ensuring universal and affordable internet access), and partnerships for implementation and diffusion of information and communications technologies and global interconnectedness (Goal 17) (34).
In the context of Industry 4.0, this work contributes to the emerging concept of Dentistry 4.0 (35, 36) by integrating advanced technologies into its design. The system incorporates key components such as internet-based services accessible via satellite connectivity, cloud computing for remote data management, and cybersecurity embedded within its framework. Additionally, simulation functionalities are included through 3D modelling. While the system represents significant progress towards cyber-physical systems—where physical and digital domains merge—the full integration of these domains is not yet complete. The study aligns with the Sequential Industrial Modernization Framework, highlighting digital information as a critical input-output signal in dental practice. Although the findings demonstrate the potential for digital modernization in dentistry, they also indicate the need for further technological integration and the incorporation of contextual artificial intelligence to achieve the Industry 5.0 level, outlining opportunities for future research and development in the field.
While this study offers valuable insights into the technology proficiency, and potential adoption using these technologies in populations with no or unreliable connectivity, it is not without its limitations. Firstly, although valuable insights have been gained about the oral health of this population, it must be noted that the purpose was not to obtain a definitive oral health profile of the older adult population living in remote geographic areas of Los Lagos Region. The findings offer a preliminary understanding and represent an important step toward providing a foundation for more targeted programmes and future research initiatives aimed at older adults living in those areas. Geographically, the study is confined to only one municipality. Despite these limitations, we believe that the current approach was appropriate given the exploratory nature of the study. The information generated in this study serves as crucial input for the design of health policies and programmes aligned with national and regional priorities for older adults (37).
5 Conclusion
The study provides preliminary yet compelling evidence that the integration of satellite-based internet connectivity in teledentistry improves access to oral healthcare for geographically isolated populations. Combining a digital health platform with real-time remote consultations enables management of urgent and chronic oral health needs in difficult to access regions. The model's classification within the Industry 4.0 framework underscores its technological maturity and foundational role in Dentistry 4.0. Despite limited scope, its successful implementation suggests scalability and relevance. Future directions should include the integration of contextual artificial intelligence and expansion into other underserved areas, reinforcing the role of digital ecosystems in reducing health disparities.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Universidad de La Frontera (ID: 169/23, approved on 18 March 2024). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
VB: Project administration, Data curation, Methodology, Formal analysis, Conceptualization, Funding acquisition, Investigation, Supervision, Writing – review & editing, Writing – original draft. LL: Conceptualization, Writing – original draft, Methodology, Formal analysis, Writing – review & editing. PA: Methodology, Writing – review & editing, Investigation, Software, Funding acquisition, Project administration. RS: Writing – review & editing, Data curation, Methodology. CAce: Formal analysis, Data curation, Supervision, Methodology, Writing – review & editing, Conceptualization, Investigation. JB: Formal analysis, Writing – review & editing, Methodology. CAla: Methodology, Writing – review & editing, Formal analysis. RvM: Formal analysis, Writing – review & editing, Data curation. IE: Writing – original draft, Writing – review & editing. RM: Supervision, Methodology, Formal analysis, Conceptualization, Data curation, Writing – original draft, Writing – review & editing, Investigation.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was partially funded by the Presidential Grant Project, “Clinical Centre for Innovation in Oral Health of Older Adults in the La Araucanía Region, Chile” (Exempt Resolution No. 472), and the FRO2495 project, “Integrated Technological Ecosystem of Tele-Dentistry to Provide General and Specialised Dental Care for Older Adults”.
Acknowledgments
We would like to thank the Chilean Air Force (FACH) and the Institute of Educational Informatics at the Universidad de La Frontera, Chile, for their collaboration and logistical support. We also extend our thanks to the Municipality of Cochamó and the Reloncaví Health Service, Chile.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Alhozgi A, Feine JS, Tanwir F, Shrivastava R, Galarneau C, Emami E. Rural–urban disparities in patient satisfaction with oral health care: a provincial survey. BMC Oral Health. (2021) 21:261. doi: 10.1186/s12903-021-01613-0
2. Chen H-F, Lee H-E, Chen I-T, Huang Y-T, Ho P-S, Karim SA. Rural–urban disparities in the incidence and treatment intensity of periodontal disease among patients with diabetes. Front Public Health. (2023) 11:1241150. doi: 10.3389/fpubh.2023.1241150
3. Oshima K, Miura H, Tano R, Fukuda H. Urban-rural differences in the prevalence of having a family dentist and their association with income inequality among Japanese individuals: a cross-sectional study. BMC Oral Health. (2024) 24:741. doi: 10.1186/s12903-024-04528-8
4. Maganty A, Byrnes M, Hamm M, Wasilko R, Sabik Davies BJ, Jacobs BL. Barriers to rural health care from the provider Perspective. Rural Remote Health. (2023). doi: 10.22605/rrh7769
5. Barry R, Green E, Robson K, Nott M. Factors critical for the successful delivery of telehealth to rural populations: a descriptive qualitative study. BMC Health Serv Res. (2024) 24(1):908. doi: 10.1186/s12913-024-11233-3
6. Cortelyou-Ward K, Atkins DN, Noblin A, Rotarius T, White P, Carey C. Navigating the digital divide: barriers to telehealth in rural areas. J Health Care Poor Underserved. (2020) 31:1546–56. doi: 10.1353/hpu.2020.0116
7. Chueke D. Persisting barriers to the adoption of telemedicine in Latin America after the COVID-19 pandemic. Telehealth Med Today. (2023) 8(5). doi: 10.30953/thmt.v8.423
8. Garcia Saiso S, Marti MC, Malek Pascha V, Pacheco A, Luna D, Plazzotta F, et al. Barreras y facilitadores a la implementación de la telemedicina en las Américas. Rev Panam Salud Pública. (2021) 45:1. doi: 10.26633/rpsp.2021.131
9. Emami E, Harnagea H, Shrivastava R, Ahmadi M, Giraudeau N. Patient satisfaction with e-oral health care in rural and remote settings: a systematic review. Syst Rev. (2022) 11(1):234. doi: 10.1186/s13643-022-02103-2
10. Mariño R, Ghanim A. Definition of teledentistry. In: Giraudeau N, editor. e-Health Care in Dentistry and Oral Medicine. Cham: Springer. (2018). pp. 3–14. doi: 10.1007/978-3-319-69450-4_1
11. Anawade PA, Sharma D, Gahane S. A comprehensive review on exploring the impact of telemedicine on healthcare accessibility. Cureus. (2024) 16(3):e55996. doi: 10.7759/cureus.55996
12. Maita KC, Maniaci MJ, Haider CR, Avila FR, Torres-Guzman RA, Borna S, et al. The impact of digital health solutions on bridging the health care gap in rural areas: a scoping review. Perm J. (2024) 28:130–43. doi: 10.7812/TPP/23.134
13. Phuong J, Ordóñez P, Cao J, Moukheiber M, Moukheiber L, Caspi A, et al. Telehealth and digital health innovations: a mixed landscape of access. PLOS Digit Health. (2023) 2:e0000401. doi: 10.1371/journal.pdig.0000401
14. Beltrán V, von Marttens A, Acuña-Mardones P, Sanzana-Luengo C, Rueda-Velásquez SJ, Alvarado E, et al. Implementation of a teledentistry platform for dental emergencies for the elderly in the context of the COVID-19 pandemic in Chile. BioMed Res Int. (2022) 2022:1–8. doi: 10.1155/2022/6889285
15. Beltrán V, Muñoz-Sepúlveda F, Acevedo C, Navarro P, Venegas B, Salgado C, et al. A rural teledentistry care experience: a geriatric approach to assessing oral health Status and treatment needs in older adults from a Mapuche community in Chile. Front. Public Health. (2024) 12:1356622. doi: 10.3389/fpubh.2024.1356622
16. Benda NC, Veinot TC, Sieck CJ, Ancker JS. Broadband internet access is a social determinant of health!. Am J Public Health. (2020) 110:1123–5. doi: 10.2105/AJPH.2020.305784
17. Morales-Gómez CB, Espinoza-Santander IL, López-Neira L, von Marttens AH, Borgeat MC, Lee XM, et al. Mhealth to enhance oral cancer awareness in older adults in Chile: a preliminary report. Explor Digit Health Technol. (2025) 3:101139. doi: 10.37349/edht.2025.101139
18. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. (1977) 33:159–74. doi: 10.2307/2529310
19. World Health Organization. Oral Health Surveys: Basic Methods. 5th ed. Geneva: World Health Organization (2013). (Accessed October 27, 2025).
20. Diangelis AJ, Rojas AJ. Dental caries and periodontal disease in an Indochinese refugee population. J Dent Res. (1982) 61:1233–5. doi: 10.1177/00220345820610110401
21. Osama M, Ateya AA, Sayed MS, Hammad M, Pławiak P, Abd El-Latif AA, et al. Internet of medical things and healthcare 4.0: trends, requirements, challenges, and research directions. Sensors. (2023) 23:7435. doi: 10.3390/s23177435
22. Mansor NA, Abdullah N, Rahman HA. Towards electronic learning features in education 4.0 environment: literature study. Indones J Electr Eng Comput Sci. (2020) 19:442–50. doi: 10.11591/ijeecs.v19.i1.pp442-450
23. Alarcon C, Shene C. Arduino soft sensor for monitoring schizochytrium Sp. fermentation, a proof of concept for the industrial application of genome-scale metabolic models in the context of pharma 4.0. Processes. (2022) 10:2226. doi: 10.3390/pr10112226
24. Malheiro V, Duarte J, Veiga F, Mascarenhas-Melo F. Exploiting pharma 4.0 technologies in the non-biological complex drugs manufacturing: innovations and implications. Pharmaceutics. (2023) 15:2545. doi: 10.3390/pharmaceutics15112545
25. Alarcón S, Alarcon C. Questioning the concepts of the fourth industrial revolution and industry 4.0 when describing modernization as a sequential framework. Sustainability. (2025) 17:4531. doi: 10.3390/su17104531
26. Alarcon C, Alarcon S, Hoffer A, Pavez B. Hydrogen 5.0: interdisciplinary development of a proof-of-concept smart system for green hydrogen leak detection. Processes. (2025) 13:639. doi: 10.3390/pr13030639
27. Madhavan M, Sharafuddin MA, Wangtueai S. Measuring the industry 5.0-readiness level of SMEs using industry 1.0–5.0 practices: the case of the seafood processing industry. Sustainability. (2024) 16:2205. doi: 10.3390/su16052205
28. Breque M, De Nul L, Petridis A. Industry 5.0: Towards a Sustainable, Human-Centric and Resilient European Industry. Luxembourg: Publications Office of the European Union. (2021). ISBN 978-92-76-25308-2.
29. Council of Australian Governments. Healthy Mouths, Healthy Lives, Australia’s National Oral Health Plan 2015–2024. Canberra, Australia: Australian Government. (2015). Available online at: https://www.health.gov.au/resources/publications/healthy-mouths-healthy-lives-australias-national-oral-health-plan-2015-2024?language=en"https://www.health.gov.au/resources/publications/healthy-mouths-healthy-lives-australias-national-oral-health-plan-2015-2024?language=en
30. Bianchi T. Internet Usage in Chile—Statistics & Facts. New York, NY: Statista. (2024). Available online at: https://www.statista.com/topics/7128/internet-usage-in-chile/#topicOverview
31. Comisión Nacional de Evaluación y Productividad. Informe Anual de Productividad 2024. (2024). Available online at: https://cnep.cl/wp-content/uploads/2025/01/INFORME-ANUAL-2024-FINAL.pdf (Accessed November 11, 2025).
32. Beltrán V, Acuña-Mardones P, Diaz J, Alvarado E, Von Marttens A. TEGO: a new concept of teledentistry for the elderly through a web platform and mobile app in the context of the COVID-19 pandemic. J Oral Res. (2022) (1):1–8. doi: 10.17126/joralres.2022.023
33. United Nations, Sustainable Development Group. Leave No One Behind. (2021). Available online at: https://unsdg.un.org/2030-agenda/universal-values/leave-no-one-behind (Accessed November 11, 2025).
34. Giraudeau N, Varenne B. Advocacy for a digital oral health that leaves no one behind. JDR Clin Trans Res. (2021) 7(1):25–8. doi: 10.1177/23800844211026610
35. International Telecommunication Union (ITU). 2030 Agenda for Sustainable Development. ITU, Geneva. (2025). Available online at: https://www.itu.int/en/ITU-D/Statistics/Pages/intlcoop/sdgs/default.aspx (Accessed November 11, 2025).
36. Haleem A, Javaid M. Industry 4.0 and its applications in dentistry. Indian J Dent Res. (2020) 31:824. doi: 10.4103/ijdr.IJDR_904_18
37. Javaid M, Haleem A, Singh RP, Suman R. Dentistry 4.0 technologies applications for dentistry during COVID-19 pandemic. Sustain Oper Comput. (2021) 2:87–96. doi: 10.1016/j.susoc.2021.05.002
38. Superintendencia de Salud, Gobierno de Chile. Salud Oral Integral de Personas de 60 Años. Santiago, Chile. (2025). Available online at: https://www.superdesalud.gob.cl/orientacion-en-salud/salud-oral-integral-de-personas-de-60-anos/ (Accessed November 11, 2025).
Keywords: telehealth, teledentistry, oral health, satellite connection, rural and remote
Citation: Beltrán V, López L, Acuña-Mardones P, Silva R, Acevedo C, Bustos J, Alarcón C, von Marttens R, Espinoza I and Mariño R (2025) A teledentistry care model for older populations in remote settings in Chile using satellite communication technology. Front. Oral Health 6:1699401. doi: 10.3389/froh.2025.1699401
Received: 5 September 2025; Revised: 2 November 2025;
Accepted: 4 November 2025;
Published: 4 December 2025.
Edited by:
Luis Proença, Instituto Universitário Egas Moniz, PortugalReviewed by:
Mennatollah Sharkawy, New Giza University, EgyptMonira Samaan Kallás, Hospital Sirio Libanes, Brazil
Copyright: © 2025 Beltrán, López, Acuña-Mardones, Silva, Acevedo, Bustos, Alarcón, von Marttens, Espinoza and Mariño. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Víctor Beltrán, dmljdG9yLmJlbHRyYW5AdWZyb250ZXJhLmNs; Rodrigo Mariño, ci5tYXJpbm9AdW5pbWVsYi5lZHUuYXU=