 Pascal Le Corre1,2,3*†
Pascal Le Corre1,2,3*† Gwenolé Loas4,5
Gwenolé Loas4,5- 1Pôle Pharmacie, Service Hospitalo-Universitaire de Pharmacie, CHU de Rennes, Rennes, France
- 2Univ Rennes, CHU Rennes, Inserm, EHESP, Irset (Institut de Recherche en Santé, Environnement et Travail) - UMR_S 1085, Rennes, France
- 3Laboratoire de Biopharmacie et Pharmacie Clinique, Faculté de Pharmacie, Université de Rennes 1, Rennes, France
- 4Department of Psychiatry, Hôpital Erasme, Université Libre de Bruxelles (ULB), Brussels, Belgium
- 5Research Unit (ULB 266), Hôpital Erasme, Université Libre de Bruxelles (ULB), Brussels, Belgium
The rapid spread of COVID-19 has become a health emergency causing an urgent need for drug treatments to control the outbreak, especially in more vulnerable individuals. This is reinforced by the fact that prophylactic vaccines and neutralizing monoclonal antibodies may not be fully effective against emerging variants. Despite all efforts made by the scientific community, efficient therapeutic options currently remain scarce, either in the initial, as well as in the advanced forms of the disease. From retrospective observational studies and prospective clinical trials, selective serotonin reuptake inhibitors (SSRIs), and other antidepressants with functional inhibition of acid sphingomyelinase (FIASMAs), have emerged as potential treatments of COVID-19. This has led to some prematurely optimistic points of view, promoting a large prescription of fluvoxamine in patients with COVID-19, that we think should be reasonably tempered.
Introduction
Many studies have proposed potential therapeutic approaches for treatment of COVID-19, especially for COVID-19 patients who are not hospitalized nor severely ill. Among these therapeutic options, antidepressants—especially selective serotonin reuptake inhibitors (SSRIs) - have emerged, being associated with protection against severe COVID-19.
It should be noted that several scientific journals, as well as mainstream press, have promoted the use of SSRIs, especially of fluvoxamine in patients with COVID-19 (Facente et al., 2021; Sidik 2021; Wroe et al., 2021). However, current evidence available in the literature, as well as some limitations in the studies performed, should invite caution in promoting a large prescription of fluvoxamine as a repurposed drug in the infectious phase in patients with COVID-19. However, as antidepressant drugs, SSRIs may be used in patients who have been infected with COVID-19 and may subsequently develop symptoms of depression.
Current Evidence on Selective Serotonin Reuptake Inhibitors in Patients with COVID-19
Before the COVID-19 pandemic, numerous in vitro studies found that functional inhibitors of ASM (FIASMAs) disrupted infection by intracellular bacterial pathogens (Cockburn et al., 2019), Ebola virus (Johansen et al., 2015), severe acute respiratory syndrome coronavirus (SARS-CoV) (Dyall et al., 2014) or middle east respiratory syndrome coronavirus (MERS-CoV) (Dyall et al., 2014). Among FIASMAs with antiviral activity, SSRIs have been proposed as sertraline in Ebola virus disease (Johansen et al., 2015) or fluoxetine in influenza virus infection (Schloer et al., 2020), in hepatitis C virus (Young et al., 2014), coxsackievirus (Zuo et al., 2012), enterovirus (Bauer et al., 2019) and Ebola virus (Kummer et al., 2022). Beside antiviral properties, SSRIs have anti-inflammatory and immunomodulary properties that should be of value in the management of inflammatory lung disease in COVID-19 (Meikle et al., 2021; Pashaei 2021).
Retrospective observational studies in patients with COVID-19 have suggested that SSRIs (fluoxetine and fluvoxamine) may play a role in COVID-19 management. A retrospective study involving 345 patients with a medication order of antidepressants within 48 h of hospital admission has shown that antidepressant prescription was linked to a reduced likelihood of intubation or death, as a composite study endpoint (Hoertel et al., 2021a). More interestingly, a more powered retrospective observational study involving 3,401 patients with a medication order for a SSRI prescribed within a period ranging from 10 days before to 7 days after COVID-19 diagnosis, showed that SSRIs, and more specifically fluoxetine, have been associated with a reduced severity of COVID-19, as shown by a reduced relative risk of mortality (Oskotsky et al., 2021). Another retrospective study on 269 in hospitalized patients with pneumonia found a lower mortality rate in patients receiving fluoxetine (Németh et al., 2021). Two very recent retrospective observational studies on chronic treatment with antidepressants and notably SSRIs have given contradictory results. In a small size study in psychiatric inpatients, a significant association between antidepressant use and reduced COVID-19 infection was found notably for fluoxetine and trazodone (Clelland et al., 2021). The second study with a much higher number of subjects reported no significant difference in mortality between inpatients with COVID-19 receiving SSRIs and those not taking SSRIs (Rauchman et al., 2022). In the latter study, no patients were taking fluvoxamine.
These favorable effects of SSRIs have been linked to several potential underlying mechanisms of action including anti-inflammatory properties, agonist sigma-1 receptor (S1R) properties, as well as inhibition of acid sphingomyelinase/ceramide system. Within antidepressants with SIR agonist properties, fluvoxamine is the most powerful with a low nanomolar affinity (around 10-times more potent than fluoxetine), and early intervention of fluvoxamine (i.e., in the early infection and pulmonary stage) has been proposed (Hashimoto et al., 2022). Furthermore, taking into account that hypoxia could be a strong factor in COVID-19 progression, the use of fluvoxamine in the early phase of COVID-19 has been suggested in order to counteract some early posthypoxic events (Grieb et al., 2021; Grieb and Rejdak, 2021; Rejdak and Grieb, 2021). Additionally, retrospective observational studies have shown that calcium channel blockers (particularly amlodipine that is a FIASMA) promoting pulmonary vasodilatation, have improved clinical outcomes (Solaimanzadeh 2021).
Furthermore, functional inhibitors of acid sphingomyelinase (FIASMAs)—that include several SSRIs—were also associated to a reduced likelihood of intubation or death (Hoertel et al., 2021b). The role of FIASMAs per se in patients with COVID-19 has been previously highlighted (Schloer et al., 2020; Loas and Le Corre, 2021).
Beyond retrospective observational studies, prospective clinical trials with fluvoxamine - and to a lesser extent fluoxetine - have been set up: 3 trials are completed and the results have been published (Lenze et al., 2020; Reis et al., 2021; Seftel and Boulware, 2021), 5 studies are ongoing, 2 have been suspended, and 1 has been withdrawn. The main features of these studies are summarized in Table 1.
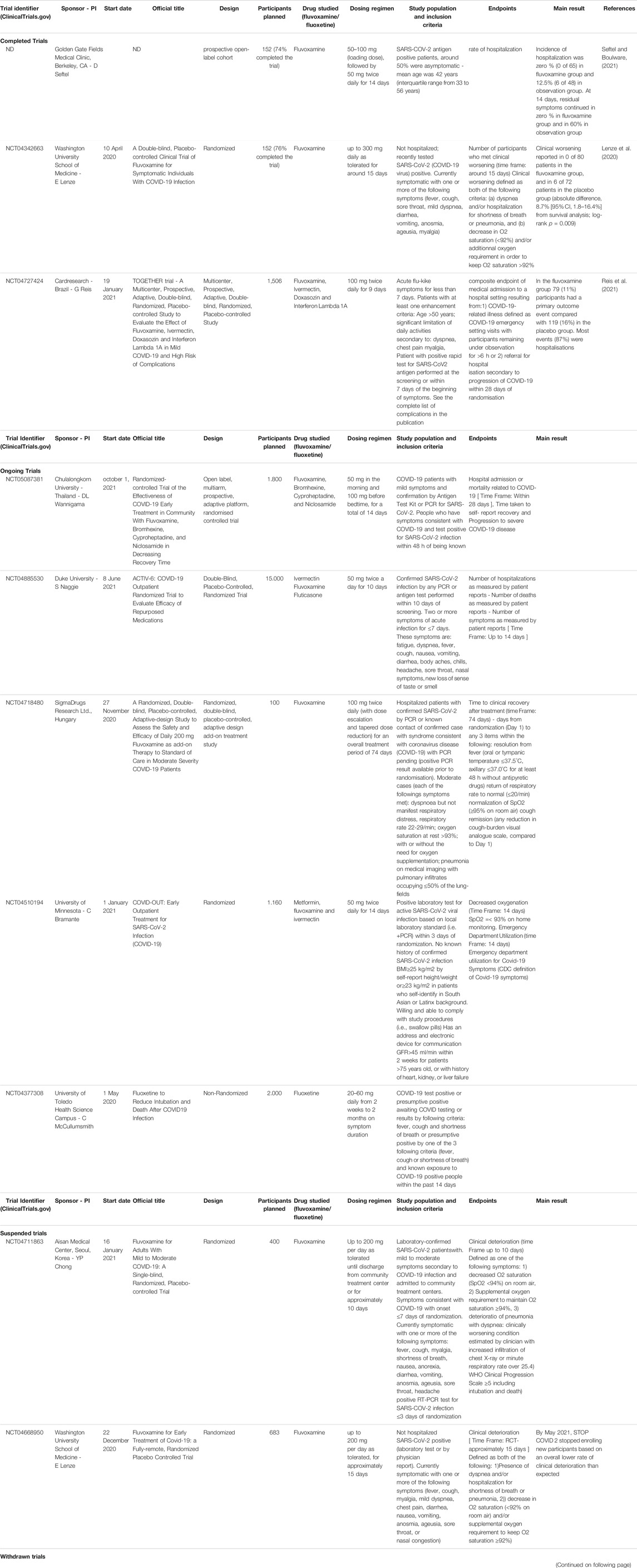
TABLE 1. Main features of completed, ongoing, suspended and withdrawn trial on fluvoxamine and fluoxetine in patients with COVID-19.
Among the currently published studies, the study by Lenze (Lenze et al., 2020) has shown a lower probability of clinical deterioration within 15 days in the fluvoxamine group. In this first study performed in a rather small number of patients (80 in the treatment group), fluvoxamine was dosed 100 mg three-times daily from randomization up to 15 days. The second study by Reis (Reis et al., 2021) has shown a risk reduction of 5% (32% relative risk reduction) on the primary outcome of hospitalization. This outcome was defined as either a retention in a COVID-19 emergency setting or a transfer to tertiary hospital attributable to COVID-19. In this second and larger trial (741 in the treatment group), fluvoxamine was dosed 100 mg twice daily for 9 days.
It should be noted that a larger trial (STOP COVID 2) of fluvoxamine (expected 683 participants given fluvoxamine up to 200 mg per day for 15 days) has stopped enrolling new participants as of May 2021 due to futility and as a result, shows that a lower than expected rate of clinical deterioration may have needed a higher number of participants (Table 1).
Based on the available literature, the the IDSA guideline panel recommendation 24 (IDSA guideline, 2021) panel recommendation 24 indicates that among ambulatory patients with COVID-19, fluvoxamine should be used only within clinical trials to better delineate the effects of fluvoxamine on disease progression, such as need for hospital admission, ICU care, and ultimately mortality (Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19, version V5.5.3 updated 9 November 2021).
Furthermore, there are currently 2 meta-analysis in a preprint state (Kacimi et al., 2021, submitted 2021; Lee et al., 2021, submitted 2021) and it should be noted that they did not include the same studies, only 2 studies in common on the 3 included studies. A meta-analysis has concluded that fluvoxamine has not shown significant efficacy in reducing either the mortality rates or mechanical ventilation while promising results in decreasing the likelihood for hospitalization in patients with COVID-19 (Kacimi et al., 2021, submitted 2021). The second meta-analysis (including unpublished data from the suspended trial STOP COVID 2) has concluded that fluvoxamine showed a high probability of preventing hospitalization in outpatients with COVID-19, and that this drug could be a treatment option for patients providing the lack of contraindication (Lee et al., 2021, submitted 2021).
Discussion
We would like to point out three important methodological limitations of the current larger study by Reis (Reis et al., 2021) related to the primary endpoint, the absence of control in affectivity, and to the fluvoxamine dosing regimen that deserved discussion. These comments might also help to temper the conclusions of the two meta-analysis.
First, the use of a composite criterion constitutes a strong limitation of this study. The reasons for the retention in an emergency setting, and for the transfer to a tertiary hospital are not documented, and the likelihood for implication of non-COVID-19 urgency reasons cannot be ruled out. Moreover, when differences between groups were examined for each component of the criterion, only the retention in emergency setting reached statistical significance (7/741 vs 36/756 in fluvoxamine and placebo groups, respectively). Indeed, the difference in hospitalization, that represented 87% of the total events, was not significant (75/741–10% vs 97/756–13% in fluvoxamine and placebo groups, respectively). Thus, the difference in the composite criterion is mainly explained by the difference in the rate of retention in the emergency setting. The mortality rate was not significantly different between the two groups (fluvoxamine: 17/741, 2% vs placebo: 25/756, 3%, p = 0.24). Considering the rate of mortality reported (2 and 3% in the fluvoxamine and placebo groups, respectively), a number of subjects of 3,788 by group would have been required to reach the 33% difference observed in the study (80% power, α level of 0.05, bilateral test). Hence, the promising or the high probability of preventing hospitalization in outpatients as suggested by the meta-analysis should be reasonably ruled out.
Second, an important confounding factor has not been considered. The level of positive and/or negative effects has not been controlled in the Together trial (Reis et al., 2021) contrary to the previous trial on fluvoxamine by Lenze (Lenze et al., 2020) that reported comparable levels of anxiety in the two groups since anxiety may relate to shortness of breath. Furthermore, fluvoxamine is an antidepressant and anxiolytic drug which will increase pain thresholds (Palmer and Benfield, 1994). Hence, subjects with low negative affect and/or increased pain threshold may be less aware of their symptoms and therefore less prone to go an emergency setting.
Third, the effect of fluvoxamine should occur with some delay as the elimination half-life (T1/2) is 14–22 h, and is increased by 30–50% after multiple dosing (van Harten 1993). Hence, steady-state concentrations are reached within 5–10 days after initiation of therapy, and even beyond 10 days in the elderly since T1/2 is doubled. In the Reis study, time to emergency setting visit and time to hospitalization were 4 and 5 days, respectively. Thus, the duration of treatment in the study may not be suitable to establish a link between fluvoxamine and the primary endpoint. This pharmacokinetic feature also applies to retrospective observational studies. A study has shown that the administration of a low dose (37.5 mg) of amitriptyline in healthy subjects was sufficient to reduce ASM activity in vitro, and to prevent ex vivo the infection of freshly isolated nasal epithelial cell (Carpinteiro et al., 2020). The ex vivo protective effect of amitriptyline against infection appeared within a short delay (1.5 h), and lasted for at least 24 h. The study suggested that low dosage of amitriptyline could prevent infection of freshly isolated nasal epithelial cells with SARS-Cov-2 and with a very short time of action.
Considering that clinical symptoms of COVID-19 affecting notably the lungs, antidepressant concentration in this tissue would be an important factor to consider. A pre-print study (Eugene 2022) simulated the tissue concentrations of fluoxetine and estimated the percentage of patients achieving a trough level for the effective concentration of lungs (based on a 90% inhibition of SARS-CoV-2 as reported in Calu-3 human lung cells). At a median daily dose of 40 mg of fluoxetine, inhibiting concentrations in the lung would be achieved in 60% of patient at day 1, 90% at day 5 and 93% at day 10 of dosing. However, it should be noticed that considering a mean elimination half-life of 3.5 days of fluoxetine reported in the study (quite smaller than that observed in patients, around 4–6 days), the simulated plasma profile is quite unusual since 50% of the steady-state should be reached in 1 half-life (3.5 days). This was not the case in the simulation where around 75% of the steady-state was reached within one half-life suggesting an overestimation of the initial plasma and corresponding tissue concentrations so that the percentage of patients with effective concentration of lungs and day 1 may be overestimated.
Apart from methodological caveats, we think that the promotion for a widespread use of fluvoxamine is currently inappropriate, and that other intrinsic pharmacological properties of the drug should be considered that have been underlined by several authors (Glebov, 2021). Although the adverse events during the clinical trials (Lenze et al., 2020; Reis et al., 2021) on fluvoxamine have been moderate, the incidence of clinically significant drug-drug interactions or of psychiatric adverse reactions of SSRI (e.g., insomnia, anxiety, …) could be a concern on a large-scale use (Blaess et al., 2021). Furthermore, fluvoxamine is a not a drug with smart pharmacokinetics. Fluvoxamine has a high first-pass metabolism and displays a non-linear and sex-dependent pharmacokinetics with a high inter-patient variability (Altamura et al., 2015). Fluvoxamine is metabolized by a CYP2D6 that displays a marked racial/ethnic difference in frequency of functional alleles. Moreover, fluvoxamine is a potent inhibitor of CYP1A2, and a moderate inhibitor of CYP3A4, CYP2C9 and CYP2C19 so it may lead to drug-drug interactions with the numerous drugs prescribed in chronic diseases (17.4% of the case of severe adverse events reported to the FAERS are related to drug interaction, FDA Adverse Event Reporting System, consulted December 31, 2021). Thus, prescription of fluvoxamine to patients with medical comorbidities should be considered with caution.
We do hope that the ongoing trials will help to refineg the place for SSRIs in the treatment of COVID-19 in its initial stages, including their safety. This may come from the results of ACTIV-6 and of COVID-OUT that are enrolling a significant number of patients with different arms exploring not only fluvoxamine but also other drugs (Table 1). However, within these trials, a non-randomized study with fluoxetine will not help to better understand the positioning of this SSRI. This is unfortunate since the retrospective observational study by Oskotsky (Oskotsky et al., 2021) has suggested a positive impact of fluoxetine on the risk of mortality.
However, the role of SSRIs and other antidepressants may better be considered in advanced forms of COVID-19. Indeed, some of these drugs have FIASMAs properties (Loas and Le Corre, 2021); and there is preclinical evidence that ASM has an essential role in the pathogenesis of sepsis/host response, and that its inhibition might have a positive influence on the outcome (Chung and Claus, 2021). Furthermore, activation of the sphingomyelinase-ceramide pathway in response to infection in intensive care patients with severe COVID-19 has shown a potential benefit in the inhibition of ASM (Abusukhun et al., 2021). Additionally, a small-sized open-label study of COVID-19 ICU hospitalized patients (prospective cohort trial with matched controls in patients, n = 51 with a follow up of 15 days), showed that fluvoxamine (100 mg three-times daily) reduced the overall mortality 58.8 vs 76.5%) (Calusic et al., 2021).
Targeting both the host and the virus should also be considered given the synergy of the combination of fluoxetine with direct-antiviral agents (e.g., remdesivir and its metabolite GS-441524) that has been displayed on ex vivo cellular models (Brunotte et al., 2021; Schloer et al., 2021). Moreover, the combination of a host-directed drug (i.e., baricitinib) and of an antiviral (i.e., remdesivir) in patients hospitalized with moderate to severe disease for COVID-19 has been proven beneficial in reducing the recovery time, and in speeding up the improvement in clinical outcomes (Kalil et al., 2021). Hence, a more systematic study of the combination of SSRIs with direct-antiviral agents should be of value. However, a parallel estimation of the potential in vivo drug-drug interactions between these drugs (both as victim drug and as perpetrator) should be carried out given the potential for drug-drug interactions of SSRI’s (e.g., fluoxetine and fluvoxamine) and of some antivirals. Remdesivir and molnupiravir are pro-drugs metabolized by non-CYP450 enzymes with short half-lives and are less prone to drug-drug interactions, and thus the evaluation of DDI should consider their active moiety. However, the recently marketed ritonavir-boosted association with nirmatrelvir (Paxlovid™) should be used with caution with regard to drug-drug interactions in COVID-19 as a result of the well known DDI potential of ritonavir (Heskin et al., 2022).
Conclusion and Future Directions
It is clear that positioning SSRIs in outpatients with COVID-19 is not that simple and that methodological precautions have to be considered. The use of the DREL scale (i.e., drug repositioning evidence level, Oprea and Overington, 2015) may help assess of the quality of the scientific evidence from drug repositioning studies. Given the time-course of COVID-19 symptoms with a rapid deterioration in high-risk patients, the ideal drug should have either a short elimination half-life or should be started with a loading dose to rapidly reach the steady state. Beyond the daily dose, the dosing regimen (i.e., interval between doses) should also be considered since the interval between the doses influences the accumulation ratio as well as the fluctuations in blood and tissue levels that may be of concern. Drug safety profile is also an issue, and non-antidepressants FIASMAs having fewer side effects and already widely prescribed in the population, such as melatonin or antihistamines, may be an option.
However, the benefit-risk balance of SSRIs, and of other antidepressants especially with FIASMA properties, in treating advanced forms COVID-19 in hospitalized patients is much more favorable and should be considered and investigated. In these patients, combined strategies with host-directed drugs and direct-antiviral agents are also an issue to consider. In this perspective, a drug such as amitriptyline that showed improvement in the early pro-inflammatory response associated with sepsis in pre-clinical models (Xia et al., 2019a; Xia et al., 2019b; Chung and Claus, 2021), as well as a potential to prevent infection of isolated human nasal epithelial cells with COVID-19 (Carpinteiro et al., 2020; Loas and Le Corre, 2021) may represent an option for clinical trials in this setting.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author Contributions
PLC and GL conceived the Perspective together, and both have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abusukhun, M., Winkler, M. S., Pöhlmann, S., Moerer, O., Meissner, K., Tampe, B., et al. (2021). Activation of Sphingomyelinase-Ceramide-Pathway in COVID-19 Purposes its Inhibition for Therapeutic Strategies. Front. Immunol. 12, 784989. doi:10.3389/fimmu.2021.784989
Altamura, A. C., Caldiroli, A., and Buoli, M. (2015). Pharmacokinetic Evaluation of Fluvoxamine for the Treatment of Anxiety Disorders. Expert Opin. Drug Metab. Toxicol. 11 (4), 649–660. doi:10.1517/17425255.2015.1021331
Bauer, L., Manganaro, R., Zonsics, B., Strating, J. R. P. M., El Kazzi, P., Lorenzo Lopez, M., et al. (2019). Fluoxetine Inhibits Enterovirus Replication by Targeting the Viral 2C Protein in a Stereospecific Manner. ACS Infect. Dis. 5 (9), 1609–1623. doi:10.1021/acsinfecdis.9b00179
Blaess, M., Kaiser, L., Sommerfeld, O., Csuk, R., and Deigner, H. P. (2021). Drugs, Metabolites, and Lung Accumulating Small Lysosomotropic Molecules: Multiple Targeting Impedes SARS-CoV-2 Infection and Progress to COVID-19. Int. J. Mol. Sci. 22 (4), 1797. doi:10.3390/ijms22041797
Brunotte, L., Zheng, S., Mecate-Zambrano, A., Tang, J., Ludwig, S., Rescher, U., et al. (2021). Combination Therapy with Fluoxetine and the Nucleoside Analog GS-441524 Exerts Synergistic Antiviral Effects against Different SARS-CoV-2 Variants In Vitro. Pharmaceutics 13 (9), 1400. doi:10.3390/pharmaceutics13091400
Calusic, M., Marcec, R., Luksa, L., Jurkovic, I., Kovac, N., Mihaljevic, S., et al. (2021). Safety and Efficacy of Fluvoxamine in COVID‐19 ICU Patients: An Open Label, Prospective Cohort Trial with Matched Controls. Br. J. Clin. Pharmacol. 1, 1. doi:10.1111/bcp.15126
Carpinteiro, A., Edwards, M. J., Hoffmann, M., Kochs, G., Gripp, B., Weigang, S., et al. (2020). Pharmacological Inhibition of Acid Sphingomyelinase Prevents Uptake of SARS-CoV-2 by Epithelial Cells. Cell Rep Med 1 (8), 100142. doi:10.1016/j.xcrm.2020.100142
Chung, H. Y., and Claus, R. A. (2021). Keep Your Friends Close, but Your Enemies Closer: Role of Acid Sphingomyelinase during Infection and Host Response. Front. Med. (Lausanne) 7, 616500. doi:10.3389/fmed.2020.616500
Clelland, C. L., Ramiah, K., Steinberg, L., and Clelland, J. D. (2021). Analysis of the Impact of Antidepressants and Other Medications on COVID-19 Infection Risk in a Chronic Psychiatric In-Patient Cohort. BJPsych Open 8 (1), e6. doi:10.1192/bjo.2021.1053
Cockburn, C. L., Green, R. S., Damle, S. R., Martin, R. K., Ghahrai, N. N., Colonne, P. M., et al. (2019). Functional Inhibition of Acid Sphingomyelinase Disrupts Infection by Intracellular Bacterial Pathogens. Life Sci. Alliance 2 (2), e201800292. doi:10.26508/lsa.201800292
Dyall, J., Coleman, C. M., Hart, B. J., Venkataraman, T., Holbrook, M. R., Kindrachuk, J., et al. (2014). Repurposing of Clinically Developed Drugs for Treatment of Middle East Respiratory Syndrome Coronavirus Infection. Antimicrob. Agents Chemother. 58, 4885–4893. doi:10.1128/AAC.03036-14
Eugene, A. R. (2022). Fluoxetine Pharmacokinetics and Tissue Distribution Suggest a Possible Role in Reducing SARS-CoV-2 Titers. London: F1000 Research.
Facente, S. N., Reiersen, A. M., Lenze, E. J., Boulware, D. R., and Klausner, J. D. (2021). Fluvoxamine for the Early Treatment of SARS-CoV-2 Infection: A Review of Current Evidence. Drugs 81 (18), 2081–2089. doi:10.1007/s40265-021-01636-5
Glebov, O. O. (2021). Low-Dose Fluvoxamine Modulates Endocytic Trafficking of SARS-CoV-2 Spike Protein: A Potential Mechanism for Anti-COVID-19 Protection by Antidepressants. Front. Pharmacol. 12, 787261. doi:10.3389/fphar.2021.787261
Grieb, P., and Rejdak, K. (2021). Are central Nervous System Drugs Displaying Anti-inflammatory Activity Suitable for Early Treatment of COVID-19? Folia Neuropathol. 59 (2), 113–120. doi:10.5114/fn.2021.107572
Grieb, P., Swiatkiewicz, M., Prus, K., and Rejdak, K. (2021). Hypoxia May Be a Determinative Factor in COVID-19 Progression. Curr. Res. Pharmacol. Drug Discov. 2, 100030. doi:10.1016/j.crphar.2021.100030
Hashimoto, Y., Suzuki, T., and Hashimoto, K. (2022). Mechanisms of Action of Fluvoxamine for COVID-19: a Historical Review. Mol. Psychiatry 7, 1–10. doi:10.1038/s41380-021-01432-3
Heskin, J., Pallett, S. J. C., Mughal, N., Davies, G. W., Moore, L. S. P., and Rayment, M. (2022). Caution required with use of ritonavir-boosted PF-07321332 in COVID-19 management. Lancet 399 (10319), 21–22. doi:10.1016/S0140-6736(21)02657-X
Hoertel, N., Sánchez-Rico, M., Gulbins, E., Kornhuber, J., Carpinteiro, A., Lenze, E. J., et al. (2021b). Association between FIASMAs and Reduced Risk of Intubation or Death in Individuals Hospitalized for Severe COVID-19: An Observational Multicenter Study. Clin. Pharmacol. Ther. Dec 110 (6), 1498–1511. doi:10.1002/cpt.2317
Hoertel, N., Sánchez-Rico, M., Vernet, R., Beeker, N., Jannot, A.-S., Neuraz, A., et al. (2021a). Association between Antidepressant Use and Reduced Risk of Intubation or Death in Hospitalized Patients with COVID-19: Results from an Observational Study. Mol. Psychiatry 26 (9), 5199–5212. doi:10.1038/s41380-021-01021-4
IDSA guideline (2021). Infectious Diseases Society of America Guidelines on the Treatment and Management of Patients with COVID-19, Version V5.5.3 Updated 9 Nov 2021. posted online at www.idsociety.org/COVID19guidelines.
Johansen, L. M., DeWaldShoemakerHoffstrom, L. E. C. J. B. G., Shoemaker, C. J., Hoffstrom, B. G., Lear-Rooney, C. M., Stossel, A., et al. (2015). A Screen of Approved Drugs and Molecular Probes Identifies Therapeutics with Anti-ebola Virus Activity. Sci. Transl Med. 7 (290), 290ra89. doi:10.1126/scitranslmed.aaa5597
Kacimi, O., Greca, E., Haireche, M. A., ElHawary, A. S., Setti, M. O., Caruana, R., et al. (2021). The Place of Fluvoxamine in the Treatment of Non-critically Ill Patients with COVID-19: A Living Systematic Review and Meta-Analysis. MedRxiv preprint 1, 1. doi:10.1101/2021.12.19.21268044
Kalil, A. C., Patterson, T. F., Mehta, A. K., Tomashek, K. M., Wolfe, C. R., Ghazaryan, V., et al. (2021). Baricitinib Plus Remdesivir for Hospitalized Adults with Covid-19. N. Engl. J. Med. 384 (9), 795–807. doi:10.1056/NEJMoa2031994
Kummer, S., Lander, A., Goretzko, J., Kirchoff, N., Rescher, U., and Schloer, S. (2022). Pharmacologically Induced Endolysosomal Cholesterol Imbalance through Clinically Licensed Drugs Itraconazole and Fluoxetine Impairs Ebola Virus Infection In Vitro. Emerging Microbes & Infections 11 (1), 195–207. doi:10.1080/22221751.2021.2020598
Lee, T. C., Vigod, S., Bortolussi-Courval, É., Hanula, R., Boulware, D. R., Lenze, E. J., et al. (2021). Fluvoxamine for Outpatient COVID-19 to Prevent Hospitalization: A Systematic Review and Meta-Analysis. MedRxiv Preprint 1, 1. doi:10.1101/2021.12.17.21268008
Lenze, E. J., Mattar, C., Zorumski, C. F., Stevens, A., Schweiger, J., Nicol, G. E., et al. (2020). Fluvoxamine vs Placebo and Clinical Deterioration in Outpatients with Symptomatic COVID-19: A Randomized Clinical Trial. JAMA 324 (22), 2292–2300. doi:10.1001/jama.2020.22760
Loas, G., and Le Corre, P. (2021). Update on Functional Inhibitors of Acid Sphingomyelinase (FIASMAs) in SARS-CoV-2 Infection. Pharmaceuticals (Basel) 14 (7), 691. doi:10.3390/ph14070691
Meikle, C. K. S., Creeden, J. F., McCullumsmith, C., and Worth, R. G. (2021). SSRIs: Applications in Inflammatory Lung Disease and Implications for COVID‐19. Neuropsychopharmacol. Rep. 41 (3), 325–335. doi:10.1002/npr2.12194
Németh, Z. K., Szűcs, A., Vitrai, J., Juhász, D., Németh, J. P., and Holló, A. (2021). Fluoxetine Use Is Associated with Improved Survival of Patients with COVID-19 Pneumonia : A Retrospective Case-Control Study. Ideggyogy Sz 74 (11-12), 389–396. doi:10.18071/isz.74.0389
Oprea, T. I., and Overington, J. P. (2015). Computational and Practical Aspects of Drug Repositioning. Assay Drug Dev. Technol. 13 (6), 299–306. doi:10.1089/adt.2015.29011.tiodrrr
Oskotsky, T., Marić, I., Tang, A., Oskotsky, B., Wong, R. J., Aghaeepour, N., et al. (2021). Mortality Risk Among Patients with COVID-19 Prescribed Selective Serotonin Reuptake Inhibitor Antidepressants. JAMA Netw. Open 4 (11), e2133090. doi:10.1001/jamanetworkopen.2021.33090
Palmer, K. J., and Benfield, P. (1994). Fluvoxamine. CNS Drugs 1, 57–87. doi:10.2165/00023210-199401010-00006
Pashaei, Y. (2021). Drug Repurposing of Selective Serotonin Reuptake Inhibitors: Could These Drugs Help Fight COVID-19 and Save Lives? J. Clin. Neurosci. 88, 163–172. doi:10.1016/j.jocn.2021.03.010
Rauchman, S. H., Mendelson, S. G., Rauchman, C., Kasselman, L. J., Pinkhasov, A., and Reiss, A. B. (2022). Ongoing Use of SSRIs Does Not Alter Outcome in Hospitalized COVID-19 Patients: A Retrospective Analysis. Jcm 11 (1), 70. doi:10.3390/jcm11010070
Reis, G., Dos Santos Moreira-Silva, E. A., Silva, D. C. M., Thabane, L., Milagres, A. C., Ferreira, T. S., et al. (2021). Effect of Early Treatment with Fluvoxamine on Risk of Emergency Care and Hospitalisation Among Patients with COVID-19: the TOGETHER Randomised, Platform Clinical Trial. Lancet Glob. Health S2214-109X (21), e42–e51. doi:10.1016/S2214-109X(21)00448-4
Rejdak, K., and Grieb, P. (2021). Fluvoxamine and Amantadine: central Nervous System Acting Drugs Repositioned for COVID-19 as Early Intervention. Curr. Neuropharmacol. 19, 1. doi:10.2174/1570159X19666210729123734
Schloer, S., Brunotte, L., Goretzko, J., Mecate-Zambrano, A., Korthals, N., Gerke, V., et al. (2020). Targeting the Endolysosomal Host-SARS-CoV-2 Interface by Clinically Licensed Functional Inhibitors of Acid Sphingomyelinase (FIASMA) Including the Antidepressant Fluoxetine. Emerg. Microbes Infect. 9 (1), 2245–2255. doi:10.1080/22221751.2020.1829082
Schloer, S., Brunotte, L., Mecate‐Zambrano, A., Zheng, S., Tang, J., Ludwig, S., et al. (2021). Drug Synergy of Combinatory Treatment with Remdesivir and the Repurposed Drugs Fluoxetine and Itraconazole Effectively Impairs SARS‐CoV‐2 Infection In Vitro. Br. J. Pharmacol. 178 (11), 2339–2350. doi:10.1111/bph.15418
Seftel, D., and Boulware, D. R. (2021). Prospective Cohort of Fluvoxamine for Early Treatment of Coronavirus Disease 19. Open Forum Infect. Dis. 8 (2), ofab050. doi:10.1093/ofid/ofab050
Sidik, S. M. (2021). Common Antidepressant Slashes Risk of COVID Death, Study Says. Nature 29, 1. doi:10.1038/d41586-021-02988-4
Solaimanzadeh, I. (2021). Why Pulmonary Vasodilation May Be Part of a Key Strategy to Improve Survival in COVID-19. Cureus 13 (12), e20746. doi:10.7759/cureus.20746
van Harten, J. (1993). Clinical Pharmacokinetics of Selective Serotonin Reuptake Inhibitors. Clin. Pharmacokinet. 24 (3), 203–220. doi:10.2165/00003088-199324030-00003
Wroe, E. B., Seung, K. J., Baker, B. K., and Farmer, P. E. (2021). Test and Treat: a Missing Link in the Global Fight against COVID-19. Lancet Glob. Health S2214-109X (21), e181–e182. doi:10.1016/S2214-109X(21)00568-4
Xia, B. T., Beckmann, N., Winer, L. K., Kim, Y., Goetzman, H. S., Veile, R. E., et al. (2019b). Amitriptyline Treatment Mitigates Sepsis-Induced Tumor Necrosis Factor Expression and Coagulopathy. Shock 51 (3), 356–363. doi:10.1097/SHK.0000000000001146
Xia, B. T., Beckmann, N., Winer, L. K., Pugh, A. M., Pritts, T. A., Nomellini, V., et al. (2019a). Amitriptyline Reduces Inflammation and Mortality in a Murine Model of Sepsis. Cell Physiol Biochem 52 (3), 565–579. doi:10.33594/000000040
Young, K. C., Bai, C. H., Su, H. C., Tsai, P. J., Pu, C. Y., Liao, C. S., et al. (2014). Fluoxetine a Novel Anti-hepatitis C Virus Agent via ROS-, JNK-, and PPARβ/γ-dependent Pathways. Antivir. Res 110, 158–167. doi:10.1016/j.antiviral.2014.08.002
Keywords: selective serotonin reuptake inhibitors (SSRIs), functional inhibitors of acid sphingomyelinase (FIASMAs), COVID-19, fluvoxamine, repurposed drugs. (Min.5-Max. 8)
Citation: Le Corre P and Loas G (2022) Difficulty in Repurposing Selective Serotonin Reuptake Inhibitors and Other Antidepressants with Functional Inhibition of Acid Sphingomyelinase in COVID-19 Infection. Front. Pharmacol. 13:849095. doi: 10.3389/fphar.2022.849095
Received: 05 January 2022; Accepted: 25 January 2022;
Published: 03 March 2022.
Edited by:
Francisco Lopez-Munoz, Camilo José Cela University, SpainReviewed by:
Sebastian Schloer, University of Münster, GermanyPawel Grieb, Mossakowski Medical Research Centre, Polish Academy of Sciences, Poland
Jesús García-Colunga, Universidad Nacional Autónoma de México, Mexico
Elyse M. Cornett, Louisiana State University Health Shreveport, United States
Copyright © 2022 Le Corre and Loas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pascal Le Corre, cGFzY2FsLmxlLWNvcnJlQHVuaXYtcmVubmVzMS5mcg==
†ORCID:Pascal Le Corre, orcid.org/0000-0003-4483-0957