 Paul Thoueille1,2
Paul Thoueille1,2 Susana Alves Saldanha2Fabian Schaller2
Susana Alves Saldanha2Fabian Schaller2 Eva Choong2François Veuve2Aline Munting3Matthias Cavassini3Dominique Braun4,5
Eva Choong2François Veuve2Aline Munting3Matthias Cavassini3Dominique Braun4,5 Huldrych F. Günthard4,5Jessy J. Duran Ramirez4,5Bernard Surial6Hansjakob Furrer6Andri Rauch6Pilar Ustero7Alexandra Calmy7,8Marcel Stöckle9Caroline Di Benedetto10Enos Bernasconi11Patrick Schmid12Catia Marzolini2,9,13
Huldrych F. Günthard4,5Jessy J. Duran Ramirez4,5Bernard Surial6Hansjakob Furrer6Andri Rauch6Pilar Ustero7Alexandra Calmy7,8Marcel Stöckle9Caroline Di Benedetto10Enos Bernasconi11Patrick Schmid12Catia Marzolini2,9,13 François R. Girardin1,2
François R. Girardin1,2 Thierry Buclin1
Thierry Buclin1 Laurent A. Decosterd2
Laurent A. Decosterd2 Monia Guidi1,14,15* for the Swiss HIV Cohort Study
Monia Guidi1,14,15* for the Swiss HIV Cohort Study- 1Service of Clinical Pharmacology, Department of Medicine, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
- 2Laboratory of Clinical Pharmacology, Department of Laboratory Medicine and Pathology, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
- 3Service of Infectious Diseases, Department of Medicine, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
- 4Department of Infectious Diseases and Hospital Epidemiology, University Hospital Zurich, Zurich, Switzerland
- 5Institute of Medical Virology, University of Zurich, Zurich, Switzerland
- 6Department of Infectious Diseases, Inselspital, Bern University Hospital, University of Bern, Bern, Switzerland
- 7Division of Infectious Diseases, Geneva University Hospitals, Faculty of Medicine, Geneva, Switzerland
- 8Department of Medicine, Faculty of Medicine, University of Geneva, Geneva, Switzerland
- 9Division of Infectious Diseases and Hospital Epidemiology, University Hospital Basel, University of Basel, Basel, Switzerland
- 10Division of Infectious Diseases, Ente Ospedaliero Cantonale, Lugano, Switzerland
- 11Division of Infectious diseases, Ente Ospedaliero Cantonale, University of Geneva, and University of Southern Switzerland, Lugano, Switzerland
- 12Division of Infectious Diseases and Hospital Epidemiology, Cantonal Hospital St Gallen, St Gallen, Switzerland
- 13Department of Molecular and Clinical Pharmacology, Institute of Translational Medicine, University of Liverpool, Liverpool, United Kingdom
- 14Centre for Research and Innovation in Clinical Pharmaceutical Sciences, Lausanne University Hospital and University of Lausanne, Lausanne, Switzerland
- 15Institute of Pharmaceutical Sciences of Western Switzerland, University of Geneva, University of Lausanne, Geneva, Switzerland
Background: The pharmacokinetics of long-acting rilpivirine has mostly been studied in clinical trials, which do not fully address the uncertainties that arise in routine clinical situations.
Aims and methods: Our population analysis aims to establish percentile curves for rilpivirine concentrations in people with HIV (PWH) followed-up in a routine clinical setting, while identifying patient-related factors that may influence rilpivirine exposure. A total of 238 PWH enrolled in our nationwide multicenter observational study contributed to 1038 concentrations (186 and 852 concentrations after oral and intramuscular injection, respectively).
Results: Rilpivirine pharmacokinetics were best described by a two-compartment model with an oral to intramuscular relative bioavailability factor. A simple zero-order absorption process was retained for oral administration while a parallel first-order absorption was used for intramuscular administration, with 27.6% of the dose released via a fast absorption pathway and the remaining fraction via a slow absorption pathway. Our model estimated that long-acting rilpivirine reaches steady-state after 2.5 years and has an elimination half-life of 18 weeks, consistent with published estimates. In females, a 45.6% reduction in the proportion of the dose absorbed via the rapid absorption pathway was observed. However, this resulted in no more than 15% difference in trough concentrations (Ctrough) compared to males, which was not considered to be clinically relevant.
Conclusion: Overall, our model-based simulations showed that only approximately 50% of long-acting rilpivirine Ctrough would be above the 50 ng/mL threshold associated with optimal therapeutic response, while approximately 85% of Ctrough would be above the first quartile of concentrations observed in Phase III trials (32 ng/mL).
1 Introduction
Rilpivirine is a non-nucleoside reverse transcriptase inhibitor (NNRTI) prescribed orally in combination with emtricitabine and tenofovir in treatment-naïve patients with a viral load below 100,000 copies at baseline (U.S. Food and Drug Administration, 2011). In addition, rilpivirine, in combination with dolutegravir, is usually prescribed as a complete regimen for people whose viral load has remained below 50 copies/mL for at least 3 months (U.S. Food and Drug Administration, 2021). Recently, rilpivirine was formulated as a nanosuspension for intramuscular (i.m.) injection, which allowed the apparent elimination half-life (t1/2) of rilpivirine to be extended from 45 h to approximately 13–28 weeks (Hodge et al., 2021; U.S. Food and Drug Administration, 2022; European Medicines Agency (EMA), 2021a). Rilpivirine in combination with cabotegravir is the first long-acting regimen for the maintenance treatment of HIV-1 infection in adults (U.S. Food and Drug Administration, 2022; European Medicines Agency (EMA), 2021a; European Medicines Agency (EMA), 2021b). Following an oral initiation period, an i.m. injection of 900 mg of rilpivirine plus 600 mg of cabotegravir is administered into the gluteal muscle. Subsequently, 900 mg of rilpivirine plus 600 mg of cabotegravir is given i.m. every 2 months, or monthly in some regions with 600 mg of rilpivirine plus 400 mg of cabotegravir.
Population pharmacokinetic (popPK) analysis of long-acting rilpivirine based on data from Phase III registrational trials suggested a one-compartmental model with linear elimination and two parallel sequential zero-first-order absorption pathways to describe the drug pharmacokinetics (Neyens et al., 2021; Benaboud et al., 2023). The analysis showed that rilpivirine concentrations following i.m. injection and oral administration were similar. In addition, no demographic or clinical covariates were found to significantly impact rilpivirine pharmacokinetics. Regarding therapeutic plasma exposure, the protein-adjusted concentration required for 90% inhibition of viral replication (PAIC90) with rilpivirine is 12 ng/mL (Margolis et al., 2015). However, the clinical target thresholds are higher based on available drug exposure–response studies. A threshold of 50 ng/mL has been recommended as the minimum concentration to increase the likelihood of a therapeutic response (Aouri et al., 2016; Dickinson et al., 2015). Some authors concluded that even higher plasma levels of rilpivirine of up to 100 ng/mL should be targeted (Néant et al., 2019). Finally, multivariable analyses showed that rilpivirine resistance mutations at baseline, HIV-1 subtype A6/A1, body mass index (BMI) greater than 30 kg/m2, or low rilpivirine and/or cabotegravir trough concentration (Ctrough) 4 weeks after the initial loading dose (i.e., 32 ng/mL and 1,120 ng/mL, respectively, corresponding to the first quartile of concentrations observed in Phase III trials) were associated with an increased risk of virologic failure (European Medicines Agency (EMA), 2021a; European Medicines Agency (EMA), 2021b; Cutrell et al., 2021; Orkin et al., 2023).
This popPK analysis is part of a Swiss observational study designed to monitor drug levels in people with HIV (PWH) who are treated with long-acting injectable cabotegravir plus rilpivirine (Thoueille et al., 2024a). The present study provides the first description of long-acting rilpivirine concentration–time profiles and their variability in PWH in a routine clinical setting and aims to establish percentile curves to help with the interpretation of drug concentration measurements as part of therapeutic drug monitoring (Thoueille et al., 2024b). Cabotegravir reference curves are described in a separate article for clarity (Thoueille et al., 2024c).
2 Methods
2.1 Study population
The Swiss HIV Cohort Study (SHCS) was established in 1988 and is a prospective longitudinal study for the follow-up of PWH (>18 years old) in Switzerland (Scherrer et al., 2022). Written informed consent was obtained from all participants, and the SHCS was approved by Canton Ethics Committees. The majority of drug samples were collected at the discretion of physicians longitudinally (i.e., sparse samples) from March 2022 to June 2023, following the approval of long-acting cabotegravir plus rilpivirine in Switzerland. All PWH enrolled in the nationwide observational study were considered for the popPK analysis (Thoueille et al., 2024a). In addition, a detailed sampling plan within a dosing interval was offered to consenting PWH followed-up in Lausanne and Geneva (Switzerland) receiving long-acting rilpivirine. This substudy consisted of blood sampling taken before the dose injections and at 1 week, 2 weeks, 4 weeks, and 8 weeks (corresponding to the end of the dosing interval, Ctrough) after the i.m. dose (Project-ID 2022-00619, approved by the Canton’s Ethics Committee, Lausanne, Switzerland).
The dose of rilpivirine, timing of the blood sampling and the last dose, bodyweight (BW), height, and body mass index (BMI) were recorded. Additional clinical and demographic information, such as sex at birth, age, viremia, CD4 cell count, and co-medications were extracted from the SHCS database. The criteria for exclusion from our popPK analysis included one undetectable rilpivirine plasma concentration after oral administration, which was due to non-adherence to oral treatment. In addition, observations were excluded if there was unreliable information about the time and/or date of the last drug administration and/or blood collection.
2.2 Analytical method
Samples were analyzed by a previously published validated multiplex high-performance liquid chromatography coupled to tandem mass spectrometry with a lower limit of quantification of 5 ng/mL (Courlet et al., 2020).
2.3 Population pharmacokinetic analysis
The non-linear mixed effects modeling was performed using the software NONMEM® (v7.5.1, ICON Development Solutions, Ellicott City, MD, USA), assisted by PsN (v5.3.1) and Pirana (v2.9.3). Data management, visual exploration, and statistical analyses were performed using R (v4.1.1, R Development Core Team, http://www.r-project.org/). As samples were collected at least 2 weeks after treatment initiation, steady-state levels were assumed for all samples collected during the oral lead-in period (i.e., oral rilpivirine half-life (t1/2) of 45–50 h) (Rilpivirine (oral) PK Fact Sheet, 2021). It should be noted that most PWH contributed to only one sample for oral rilpivirine, as samples were conveniently collected immediately before the i.m. loading dose (i.e., few samples were collected after oral administration). Regarding i.m. injections, steady-state levels were assumed from week 96 in accordance with available information (Overton et al., 2023). Two PWH received long-acting cabotegravir and rilpivirine every 4 weeks (400 mg/600 mg) for compassionate use before Swiss market authorization. This was the only recommended regimen at that time. These PWH were switched to the two-monthly regimen (600 mg/900 mg of cabotegravir/rilpivirine) a few months after the start of the study.
2.4 Model building and selection
A classic stepwise procedure was used to identify the model that best fitted the concentrations of rilpivirine after oral and i.m. administrations. The models were specified through differential equations using the NONMEM® subroutine ADVAN13 to best depict the dynamics of the longitudinal data collected. One- and two-compartment models with different absorption processes and linear elimination were compared. During preliminary model developments, the use of a zero-order absorption (
The absorption process of long-acting rilpivirine was best described by a parallel first-order absorption (
where
The variation of the NONMEM® objective function value (ΔOFV) was used at a 0.05 significance level in the forward model-building step (ΔOFV < −3.84 for one additional parameter) to statistically discriminate hierarchical models. During the backward deletion step, a significance level of 0.01 (ΔOFV >6.63 for the removal of one parameter) was used. Non-nested models were discriminated using Akaike’s information criterion. Model selection relied on diagnostic plots and the accuracy of PK parameter estimates, quantified by the relative standard error (RSE). The reliability of the results was also assessed by characterizing model shrinkage and the normality of the distribution of individual eta estimates.
2.5 Model-based Monte Carlo simulations
The clinical relevance of covariates was evaluated by comparing the PK profiles and Ctrough values of rilpivirine obtained in different groups of interest. Population percentiles for rilpivirine after oral and i.m. administration were generated to help interpret drug concentration measurements as part of therapeutic drug monitoring.
2.6 Model validation
The observed concentrations were compared with the 5th, 50th, and 95th prediction percentiles using prediction-corrected visual predictive checks (pcVPCs) performed on the final popPK model (Lindbom et al., 2005; Bergstrand et al., 2011; Jonsson and Karlsson, 1999). In addition, the original model estimates were examined against the bootstrap median parameter values and their 95% confidence intervals generated using 2000 replicates (Lindbom et al., 2005). Finally, cross-validation was performed using repeated data-splitting (n = 5) to create random subsets of the dataset, with 80% allocated to the modeling dataset and 20% to the validation dataset. Log-transformed individual observed and predicted concentrations were then evaluated using mean prediction error (MPE) and root mean square error (RMSE) as metrics to assess model accuracy and precision, respectively (Sheiner and Beal, 1981).
3 Results
Overall, 238 PWH contributed to 1,038 rilpivirine concentrations (186 concentrations after oral administration and 852 concentrations after i.m. injection collected from 176 PWH and 222 PWH, respectively), with detailed PK investigation performed on 28 PWH. Table 1 summarizes the characteristics of the PWH included in the analysis. Overall, four samples (range: 1–15) were collected per individual, with one (1–3) for oral rilpivirine and three (1–14) for i.m. rilpivirine. The median duration of follow-up was 26 weeks (3–196). Only 10 PWH had rilpivirine concentrations assumed to be at a steady state (i.e., from week 96) after i.m. administration.
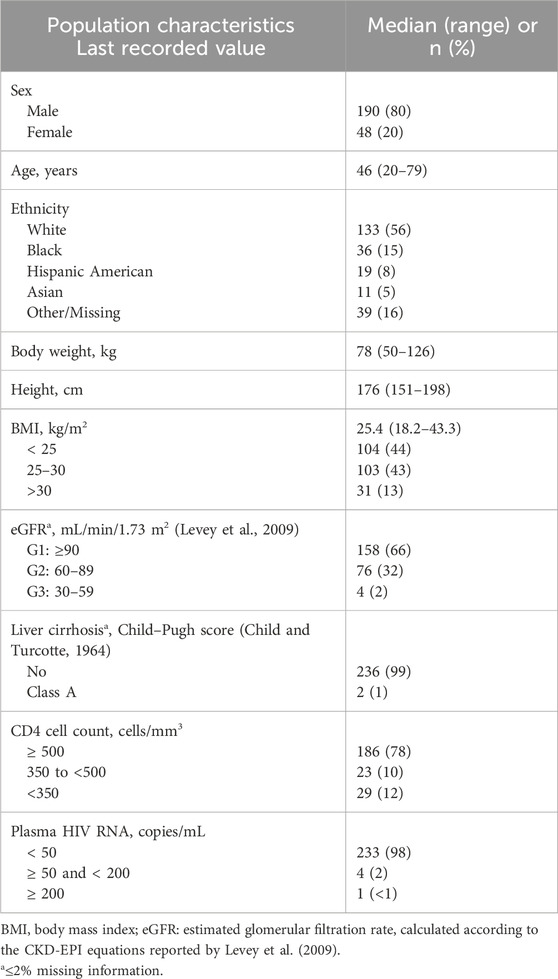
Table 1. Characteristics of the PWH.
3.1 Structural and covariate models
Consistent with available information (Neyens et al., 2021), long-acting rilpivirine was characterized by “flip-flop” kinetics (i.e., absorption rate constants (
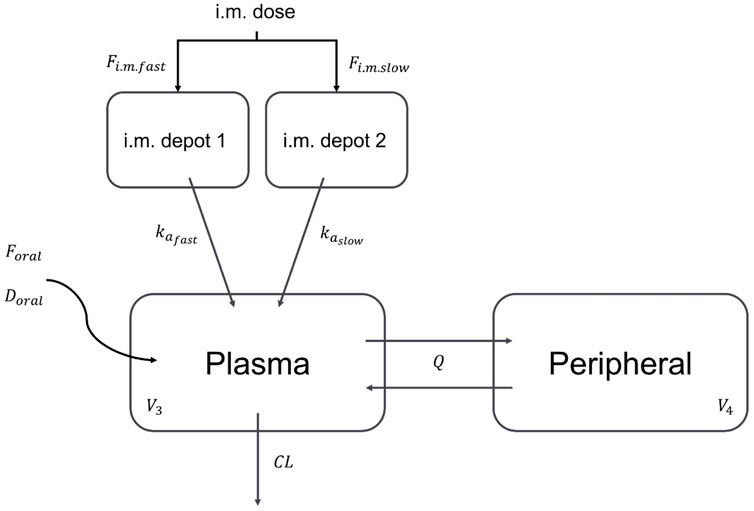
Figure 1. Structural model used to describe rilpivirine concentration-time profile. i.m.: intramuscular;
Univariate analyses revealed the effects of female sex (ΔOFV = −11, p < 0.001), and BMI (ΔOFV = −6, p < 0.05) on
This effect showed that females had an
3.2 Model-based Monte Carlo simulations
Supplementary Figure S2 shows the PK profile with variability obtained for rilpivirine after oral administration. The median Ctrough at a steady state under oral rilpivirine was 80 ng/mL [95% prediction interval (PI95): 32–211]. Our model-based simulations suggest that 85% of PWH receiving oral rilpivirine would have a Ctrough above the target of 50 ng/mL associated with therapeutic response. Regarding long-acting rilpivirine, it was found that females had a 12% lower rilpivirine Ctrough 4 weeks after the loading dose (Supplementary Figures S3, S4; Supplementary Table S2). Then, females had 8%, 12%, 10%, 14%, and 15% higher rilpivirine Ctrough at weeks 16, 24, 32, 40, and 48, respectively. Therefore, although statistically significant, the effect of sex on long-acting rilpivirine Ctrough was not considered clinically relevant, and this model was not validated. Indeed, the base and covariate models showed a maximum difference of 14% in the prediction of i.m. rilpivirine Ctrough (Supplementary Table S2). Figure 2 presents the population PK profile obtained for rilpivirine after i.m. injection (i.e., without any covariate). Overall, our model-based simulations showed that only 50% of rilpvirine Ctrough values were above the 50 ng/mL threshold after i.m. injection at week 8 (i.e., 4 weeks after the loading dose). A median 22% reduction in Ctrough values was observed at week 16. Subsequently, rilpivirine Ctrough values were found to increase through week 48 but remained almost 50% below the 50 ng/mL target at all time points. Finally, model-based simulations suggested that approximately 5% and almost 15% of PWH would have Ctrough values below 2×PAIC90 (i.e., 24 ng/mL) and below the first quartile of concentrations observed in Phase III trials (i.e., 32 ng/mL), respectively.
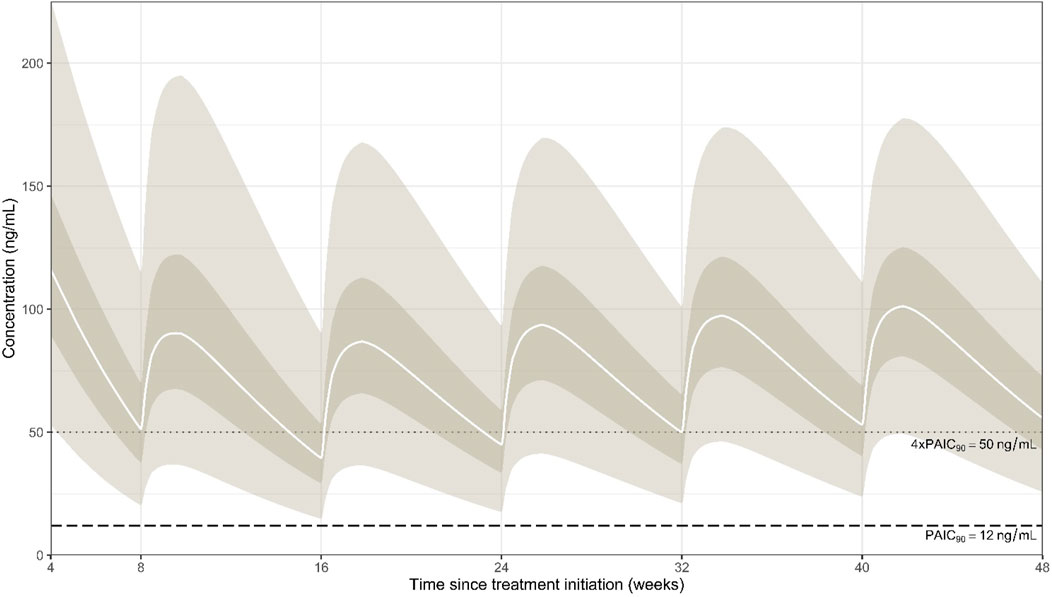
Figure 2. Simulated population percentiles after intramuscular administration of rilpivirine following a 4-week period of oral lead-in. The solid white lines represent the median (50% percentile), while the dark surfaces encompass the 50% prediction intervals, and the light surfaces encompass the 95% prediction intervals. The horizontal dashed line represents the PAIC90 of 12 ng/mL, while the dotted line shows the threshold of 50 ng/mL.
3.3 Model validation
Supplementary Figure S1 shows the goodness-of-fit diagnostic plots of the base model as no covariates were found to be clinically relevant. It should be noted that there was a modest shrinkage of 40% on the BSV of
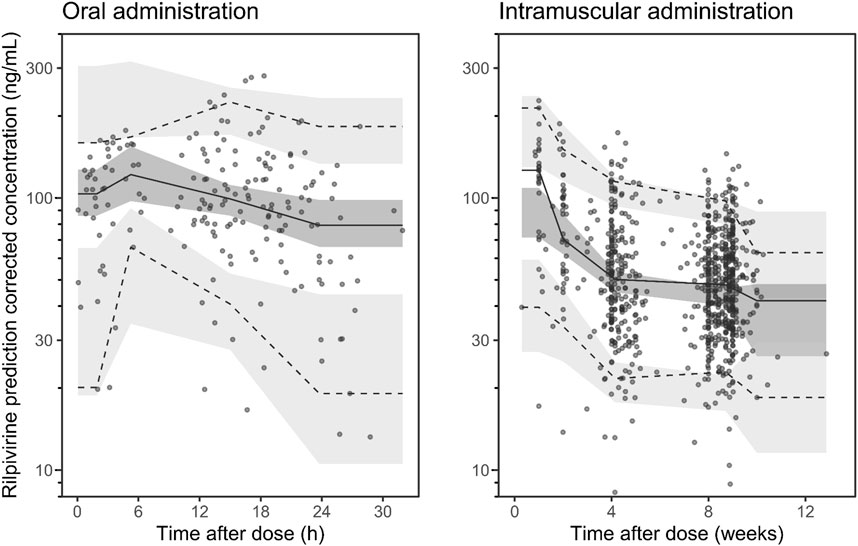
Figure 3. Visual predictive check of the retained rilpivirine popPK model for oral administration (left panel) and for intramuscular administration (right panel) for rilpivirine. Open circles represent the observed plasma concentrations. Solid and dashed lines represent the median and 90% prediction intervals (PI90%) of the observed data, respectively. Dark- and light-shaded surfaces represent the model-predicted 90% confidence intervals of the simulated median and PI90%. Note: one concentration with time beyond 4000 h is not displayed.
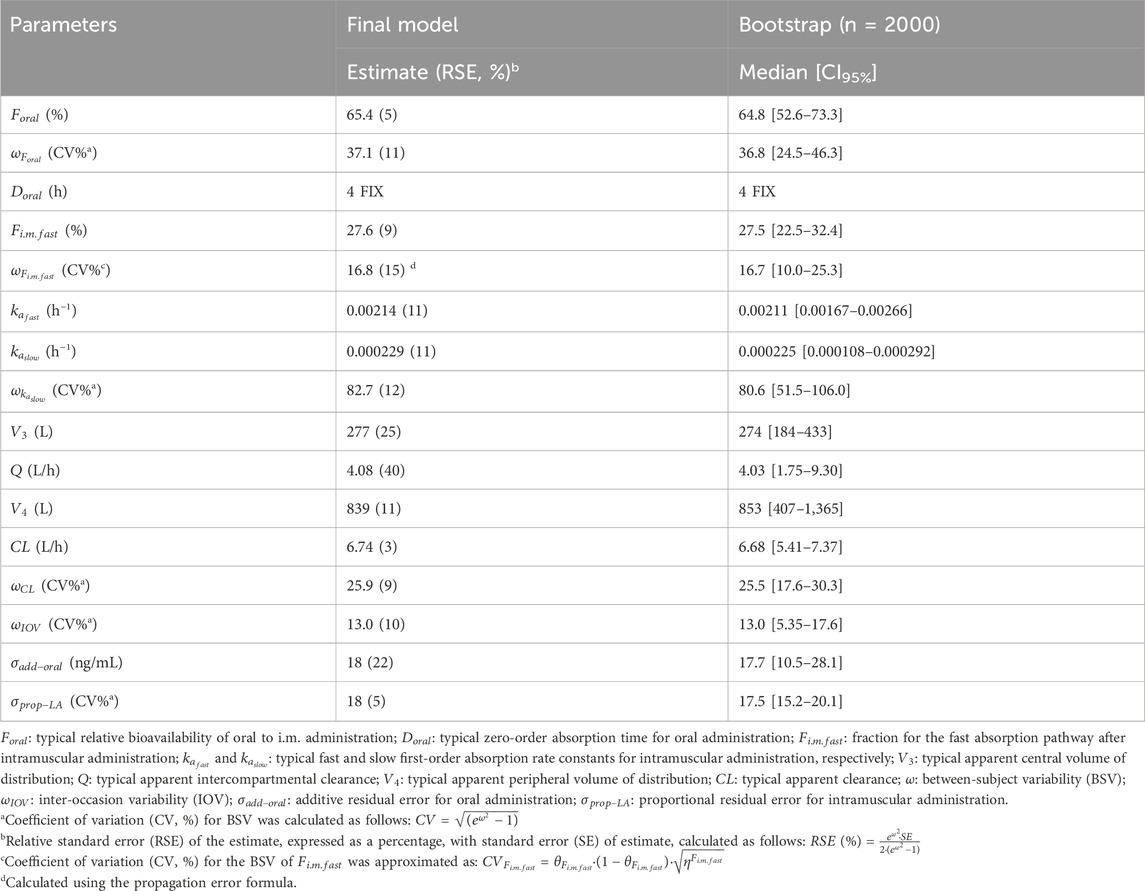
Table 2. Final population PK parameter estimates of rilpivirine with their bootstrap evaluations.
4 Discussion
The present study describes the first popPK model of rilpivirine in PWH followed in a routine clinical setting, including both oral and i.m. routes of administration. The parallel absorption process found in our popPK model for long-acting rilpivirine is consistent with a previously published popPK model based on Phase III registrational studies (Neyens et al., 2021). Our model shows that approximately a quarter (i.e., 27.6%) of the nanosuspension dose is absorbed via a relatively fast absorption pathway, while the remaining (i.e., 72.4%) is absorbed via a ten-time slower absorption pathway. Females were found to have an almost 50% reduction in the fraction of the dose absorbed via the fast absorption pathway, thereby having overall slower drug absorption than males. Because of the “flip-flop” kinetics displayed by long-acting rilpivirine, this slower absorption resulted in lower concentration in females at week 8 (i.e., 4 weeks after the loading dose). Females then exhibited higher concentrations from week 16 and onward. However, as there were no more than a 15% difference in rilpivirine Ctrough levels throughout 48 weeks and the addition of this covariate explained only 11% of the BSV on
On another note, preliminary model developments showed that the clearance of rilpivirine after i.m. injection was 18% lower than the clearance calculated for oral rilpivirine (with distinct BSV). In addition to being statistically significant, an estimation of the relative bioavailability (
Our popPK model allowed the estimation of t1/2 for oral rilpivirine of 17 h and 240 h, corresponding to an initial decrease due to diffusion into the peripheral compartment and the onset of elimination and a final decrease due to elimination after equilibrium is reached, respectively. On the other hand, the time to reach a steady state and the t1/2 of long-acting rilpivirine were estimated using the absorption rate constant of the slowest absorption pathway (
Our model-based simulations showed that 15% of PWH taking oral rilpivirine would have a Ctrough below the target of 50 ng/mL, which is twice lower than that previously reported by Aouri et al. (2016). We hypothesize that, because of the modality of drug administration (i.e., fasting condition because high gastric pH impairs intestinal absorption of rilpivirine (U.S. Food and Drug Administration, 2011) and the relatively short duration of the oral lead-in period, overall adherence in our study may have been better than in the PWH population of Aouri et al. (2016), which received oral rilpivirine in the long term. However, some of the low concentrations observed in PWH on oral rilpivirine might have been caused by impaired adherence. In addition, three PWH enrolled in our study had gastric bypass surgery, and their rilpivirine concentrations were found to be reduced after oral administration, as shown in Supplementary Figure S2 (Piso et al., 2023). This effect was not included in the model because statistical power prevented proper estimation of the PK parameters. Regarding long-acting rilpivirine, our model-based simulations showed that only approximately 50% of rilpivirine Ctrough were above the 50 ng/mL threshold after i.m. injection. This finding is consistent with information from Phase III registrational studies (Cutrell et al., 2021; Overton et al., 2023; Orkin et al., 2021). The results of our analysis indicate that the threshold of 2×PAIC90 (24 ng/mL) may be a more appropriate target for long-acting rilpivirine Ctrough levels than the 4×PAIC90 value (50 ng/mL) (Thoueille et al., 2024b). The latter may be overly alarmist and prompt healthcare providers to discontinue long-acting treatment unnecessarily. Nevertheless, it is important to note that viral failure is still observed in individuals with rilpivirine levels below 50 ng/mL, particularly in PWH who have additional risk factors. Lastly, simulations showed that 5% of PWH would have rilpivirine Ctrough below 2×PAIC90 (24 ng/mL), which may be of concern.
Limitations of the present work should be acknowledged. Because the majority of PWH contributed to one sample and no detailed PK sampling was available for oral rilpivirine, the discrimination between BSV and RUV variabilities was limited for oral rilpivirine PK. In addition, because sex was considered clinically irrelevant, the model including this covariate was not validated. Therefore, the results of model-based simulations including sex should be interpreted with caution. Although our study found that no clinical covariate influenced rilpivirine disposition in our real-world cohort from Switzerland, available evidence derived from physiologically-based pharmacokinetic (PBPK) modeling showed that morbidly obese PWH could be at higher risk of presenting suboptimal Ctrough levels (Bettonte et al., 2024a). Such an effect could not be identified in our study due to the absence of morbidly obese individuals in our population. In addition, another recent PBPK study showed a modest increase in the exposure of long-acting rilpivirine in older compared to younger individuals, which nevertheless does not warrant a dose adjustment (Bettonte et al., 2024b). Similarly, the small number of older people in our study population may have mitigated the effect of age on rilpivirine PK. Further research is warranted to confirm whether our findings are applicable to populations from other settings. In addition, the design of our study provided limited opportunities to collect early concentrations during the first few days after i.m. injection. The detailed PK investigations revealed variable concentration patterns in some individuals, with some having consistently low plasma concentrations as early as 1 week to 2 weeks after the injection. The underlying cause of these unusual PK profiles remains uncertain within the scope of our analysis. At this time, it remains unclear whether low plasma levels associated with identified or unidentified risk factors could compromise the therapeutic success of long-acting cabotegravir and rilpivirine (Orkin et al., 2023).
In conclusion, our study provides the first long-acting rilpivirine concentration-time profiles and their variability in PWH in a routine clinical setting. In accordance with previous results, no covariate was found to clinically influence rilpivirine disposition. A comprehensive discussion of the thresholds to be used in the clinical setting can be found elsewhere (Thoueille et al., 2024a; Thoueille et al., 2024b).
5 Group members of the Swiss HIV Cohort Study
I. Abela, K. Aebi-Popp, A. Anagnostopoulos, M. Battegay, E. Bernasconi, D. L. Braun, H. C. Bucher, A. Calmy, M. Cavassini, A. Ciuffi, G. Dollenmaier, M. Egger, L. Elzi, J. Fehr, J. Fellay, H. Furrer, C. A. Fux, H. F. Günthard (President of the SHCS), A. Hachfeld, D. Haerry (deputy of “Positive Council”), B. Hasse, H. H. Hirsch, M. Hoffmann, I. Hösli, M. Huber, D. Jackson-Perry (patient representatives), C. R. Kahlert (Chairman of the Mother & Child Substudy), L. Kaiser, O. Keiser, T. Klimkait, R. D. Kouyos, H. Kovari, K. Kusejko (Head of Data Centre), N. Labhardt, K. Leuzinger, B. Martinez de Tejada, C. Marzolini, K. J. Metzner, N. Müller, J. Nemeth, D. Nicca, J. Notter, P. Paioni, G. Pantaleo, M. Perreau, A. Rauch (Chairman of the Scientific Board), L. Salazar-Vizcaya, P. Schmid, R. Speck, M. Stöckle (Chairman of the Clinical and Laboratory Committee), P. Tarr, A. Trkola, G. Wandeler, M. Weisser, and S. Yerly.
Data availability statement
The datasets presented in this article are not readily available. A request for data sharing can be sent to the Scientific Board of the Swiss HIV Cohort Study. A detailed explanation of the purpose for the request, as well as a study protocol, if applicable, should be presented. The final decision about data release will be taken by the Scientific Board of the SHCS. Requests to access the datasets should be directed to https://www.shcs.ch/.
Ethics statement
The studies involving humans were approved by the Swiss HIV Cohort Study, Canton’s Ethics Committee, Lausanne, Switzerland. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
PT: Conceptualization, Formal analysis, Methodology, Visualization, writing–original draft and writing–review and editing. SS: writing–review and editing. FS: writing–review and editing. EC: writing–review and editing. FV: Data curation, writing–review and editing. AM: Investigation, writing–review and editing. MC: Investigation, writing–review and editing. DB: Investigation, writing–review and editing. HFG: Investigation, writing–review and editing. JJDR: Data curation, writing–review and editing. BS: Investigation, writing–review and editing. HFG: Investigation, writing–review and editing. AR: Investigation, writing–review and editing. PU: Investigation, writing–review and editing. AC: Investigation, writing–review and editing. MS: Investigation, writing–review and editing. CDB: Investigation, writing–review and editing. EB: Investigation, writing–review and editing. PS: Investigation, writing–review and editing. CM: writing–review and editing. FG: writing–review and editing. TB: Conceptualization, Formal analysis, Methodology, writing–review and editing. LAD: Conceptualization, Methodology, Project administration, Funding acquisition, writing–review and editing. MG: Conceptualization, Formal analysis, Methodology, writing–review and editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This independent work was funded by the Swiss National Science Foundation, grant number N◦ 324730_192449. This study was performed within the framework of the Swiss HIV Cohort Study, supported by the Swiss National Science Foundation (grant #201369), by SHCS project #879, and by the SHCS research foundation. The public funding source of the study had no role in the design of the study, in data collection, analysis, and interpretation, in manuscript writing, or in the decision to submit the article for publication. This study received no support from pharmaceutical industries.
Acknowledgments
The authors would like to thank all people with HIV who participated in the study, as well as the physicians, nurses, and data-collecting staff of the SHCS centers in Switzerland and the data- and coordination center of the SHCS for excellent data management and administration.
Conflict of interest
MC reports grants and payment for expert testimony from Gilead, MSD, and ViiV and support for attending meetings from Gilead, paid to his institution. DB reports honoraria for advisory boards, lectures, and travel grants from the companies Gilead, ViiV, and MSD. HG has received unrestricted research grants from Gilead Sciences and ViiV Healthcare; fees for data and safety monitoring board membership from Merck; consulting/advisory board membership fees from Gilead Sciences, GSK, Johnson and Johnson, Janssen, Novartis, and ViiV Healthcare; and grants from the Yvonne Jacob Foundation, from the National Institutes of Health, and unrestricted research grants from Gilead Sciences. The institution of JD received grants from Gilead Sciences and ViiV. BS reports support for travel grants and advisory boards from Gilead Sciences and ViiV, paid to his institution. The institution of HF received educational grants from ViiV, MSD, AbbVie, Gilead, and Sandoz. MS reports advisory board payments to his institution by Gilead, MSD, ViiV, Moderna, and Pfizer. The institution of AR received grants from Gilead, support for attending meetings from Gilead and Pfizer, and advisory board fees from MSD and Moderna. CM has received speaker honoraria from ViiV, MSD, and Gilead. CD received travel grants for congress participation from Gilead. The institution of EB received grants from the Swiss National Science Foundation; grants from MSD; support for attending meetings from Gilead, MSD, ViiV, and Pfizer; and advisory board fees from Gilead, MSD, ViiV, Pfizer, Moderna, AstraZeneca, Abbvie, and Lilly. The institution of PS received honoraria for advisory board participation and support for attending meetings from ViiV and Gilead. None of those grants and supports was related to the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors, and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2024.1437400/full#supplementary-material
References
Aouri, M., Barcelo, C., Guidi, M., Rotger, M., Cavassini, M., Hizrel, C., et al. (2016). Population Pharmacokinetics and Pharmacogenetics Analysis of Rilpivirine in HIV-1-Infected Individuals. Antimicrob. agents Chemother. 61 (1), e00899-16. doi:10.1128/AAC.00899-16
Benaboud, S., Solas, C., Bouchet, S., Gregoire, M., Lemaitre, F., Venisse, N., et al. (2023). Comment on: population pharmacokinetics of the rilpivirine long-acting formulation after intramuscular dosing in healthy subjects and people living with HIV. J. Antimicrob. Chemother. 78, 853–854. doi:10.1093/jac/dkad009
Bergstrand, M., Hooker, A. C., Wallin, J. E., and Karlsson, M. O. (2011). Prediction-corrected visual predictive checks for diagnosing nonlinear mixed-effects models. AAPS J. 13, 143–151. doi:10.1208/s12248-011-9255-z
Bettonte, S., Berton, M., Stader, F., Battegay, M., and Marzolini, C. (2024a). Effect of obesity on the exposure of long-acting cabotegravir and rilpivirine: a modeling study. Clin. Infect. Dis. 79, 477–486. doi:10.1093/cid/ciae060
Bettonte, S., Berton, M., Stader, F., Battegay, M., and Marzolini, C. (2024b). Drug exposure of long-acting cabotegravir and rilpivirine in older people with human immunodeficiency virus: a pharmacokinetic modeling study. Open forum Infect. Dis. 11, ofae171. doi:10.1093/ofid/ofae171
Bouzom, F., Laveille, C., Merdjan, H., and Jochemsen, R. (2000). Use of nonlinear mixed effect modeling for the meta-analysis of preclinical pharmacokinetic data: application to S 20342 in the rat. J. Pharm. Sci. 89, 603–613. doi:10.1002/(SICI)1520-6017(200005)89:5<603::AID-JPS6>3.0.CO;2-E
Child, C. G., and Turcotte, J. G. (1964). Surgery and portal hypertension. Major Probl. Clin. Surg. 1, 1–85.
Courlet, P., Alves Saldanha, S., Cavassini, M., Marzolini, C., Choong, E., Csajka, C., et al. (2020). Development and validation of a multiplex UHPLC-MS/MS assay with stable isotopic internal standards for the monitoring of the plasma concentrations of the antiretroviral drugs bictegravir, cabotegravir, doravirine, and rilpivirine in people living with HIV. J. mass Spectrom. JMS 55, e4506. doi:10.1002/jms.4506
Cutrell, A. G., Schapiro, J. M., Perno, C. F., Kuritzkes, D. R., Quercia, R., Patel, P., et al. (2021). Exploring predictors of HIV-1 virologic failure to long-acting cabotegravir and rilpivirine: a multivariable analysis. Aids 35, 1333–1342. doi:10.1097/qad.0000000000002883
Dickinson, L., Yapa, H. M., Jackson, A., Moyle, G., Else, L., Amara, A., et al. (2015). Plasma tenofovir, emtricitabine, and rilpivirine and intracellular tenofovir diphosphate and emtricitabine triphosphate pharmacokinetics following drug intake cessation. Antimicrob. agents Chemother. 59, 6080–6086. doi:10.1128/AAC.01441-15
Eke, A. C., Chakhtoura, N., Kashuba, A., Best, B. M., Sykes, C., Wang, J., et al. (2018). Rilpivirine plasma and cervicovaginal concentrations in women during pregnancy and postpartum. J. Acquir Immune Defic. Syndr. 78, 308–313. doi:10.1097/QAI.0000000000001677
European Medicines Agency (EMA) (2021a). Rekambys product information. Available at: https://www.ema.europa.eu/en/documents/product-information/rekambys-epar-product-information_en.pdf (Accessed February, 2023).
European Medicines Agency (EMA) (2021b). Vocabria product information. Available at: https://www.ema.europa.eu/en/documents/product-information/vocabria-epar-product-information_en.pdf (Accessed February, 2023).
Hodge, D., Back, D. J., Gibbons, S., Khoo, S. H., and Marzolini, C. (2021). Pharmacokinetics and drug–drug interactions of long-acting intramuscular cabotegravir and rilpivirine. Clin. Pharmacokinet. 60, 835–853. doi:10.1007/s40262-021-01005-1
Jonsson, E. N., and Karlsson, M. O. (1999). Xpose--an S-PLUS based population pharmacokinetic/pharmacodynamic model building aid for NONMEM. Comput. methods programs Biomed. 58, 51–64. doi:10.1016/s0169-2607(98)00067-4
Jucker, B. M., Fuchs, E. J., Lee, S., Damian, V., Galette, P., Janiczek, R., et al. (2021). Multiparametric magnetic resonance imaging to characterize cabotegravir long-acting formulation depot kinetics in healthy adult volunteers. Br. J. Clin. Pharmacol. 88, 1655–1666. doi:10.1111/bcp.14977
Levey, A. S., Stevens, L. A., Schmid, C. H., Zhang, Y. L., Castro, A. F., Feldman, H. I., et al. (2009). A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 150, 604–612. doi:10.7326/0003-4819-150-9-200905050-00006
Lindbom, L., Pihlgren, P., and Jonsson, E. N. (2005). PsN-Toolkit--a collection of computer intensive statistical methods for non-linear mixed effect modeling using NONMEM. Comput. methods programs Biomed. 79, 241–257. doi:10.1016/j.cmpb.2005.04.005
Margolis, D. A., Brinson, C. C., Smith, G. H. R., de Vente, J., Hagins, D. P., Eron, J. J., et al. (2015). Cabotegravir plus rilpivirine, once a day, after induction with cabotegravir plus nucleoside reverse transcriptase inhibitors in antiretroviral-naive adults with HIV-1 infection (LATTE): a randomised, phase 2b, dose-ranging trial. Lancet Infect. Dis. 15, 1145–1155. doi:10.1016/s1473-3099(15)00152-8
Néant, N., Gattacceca, F., Lê, M. P., Yazdanpanah, Y., Dhiver, C., Bregigeon, S., et al. (2018). Population pharmacokinetics of Rilpivirine in HIV-1-infected patients treated with the single-tablet regimen rilpivirine/tenofovir/emtricitabine. Eur. J. Clin. Pharmacol. 74, 473–481. doi:10.1007/s00228-017-2405-1
Néant, N., Solas, C., Bouazza, N., Lê, M. P., Yazdanpanah, Y., Dhiver, C., et al. (2019). Concentration–response model of rilpivirine in a cohort of HIV-1-infected naive and pre-treated patients. J. Antimicrob. Chemother. 74, 1992–2002. doi:10.1093/jac/dkz141
Neyens, M., Crauwels, H. M., Perez-Ruixo, J. J., and Rossenu, S. (2021). Population pharmacokinetics of the rilpivirine long-acting formulation after intramuscular dosing in healthy subjects and people living with HIV. J. Antimicrob. Chemother. 76, 3255–3262. doi:10.1093/jac/dkab338
Orkin, C., Bernal Morell, E., Tan, D. H. S., Katner, H., Stellbrink, H. J., Belonosova, E., et al. (2021). Initiation of long-acting cabotegravir plus rilpivirine as direct-to-injection or with an oral lead-in in adults with HIV-1 infection: week 124 results of the open-label phase 3 FLAIR study. lancet HIV 8, e668–e678. doi:10.1016/S2352-3018(21)00184-3
Orkin, C., Schapiro, J. M., Perno, C. F., Kuritzkes, D. R., Patel, P., DeMoor, R., et al. (2023). Expanded multivariable models to assist patient selection for long-acting cabotegravir + rilpivirine treatment: clinical utility of a combination of patient, drug concentration, and viral factors associated with virologic failure. Clin. Infect. Dis. 77, 1423–1431. doi:10.1093/cid/ciad370
Overton, E. T., Richmond, G., Rizzardini, G., Thalme, A., Girard, P. M., Wong, A., et al. (2023). Long-acting cabotegravir and rilpivirine dosed every 2 Months in adults with human immunodeficiency virus 1 type 1 infection: 152-week results from ATLAS-2M, a randomized, open-label, phase 3b, noninferiority study. Clin. Infect. Dis. 76, 1646–1654. doi:10.1093/cid/ciad020
Piso, R. J., Thoueille, P., Hoffman, M., and Decosterd, L. A. (2023). Low Rilpivirine plasma levels in lead-in phase for patients with gastric bypass. SSI, SSHH, SSTTM Jt. Annu. Meet.
Savic, R. M., and Karlsson, M. O. (2009). Importance of shrinkage in empirical bayes estimates for diagnostics: problems and solutions. AAPS J. 11, 558–569. doi:10.1208/s12248-009-9133-0
Scherrer, A. U., Traytel, A., Braun, D. L., Calmy, A., Battegay, M., Cavassini, M., et al. (2022). Cohort profile update: the Swiss HIV cohort study (SHCS). Int. J. Epidemiol. 51, 33–34j. doi:10.1093/ije/dyab141
Sheiner, L. B., and Beal, S. L. (1981). Some suggestions for measuring predictive performance. J. Pharmacokinet. Biopharm. 9, 503–512. doi:10.1007/BF01060893
Thoueille, P., Cavassini, M., Guidi, M., Buclin, T., Girardin, F. R., Decosterd, L. A., et al. (2024b). Guidance for the interpretation of long-acting cabotegravir and rilpivirine concentrations based on real-world therapeutic drug monitoring data and documented failures. Open forum Infect. Dis. 11. doi:10.1093/ofid/ofae023
Thoueille, P., Saldanha, S. A., Schaller, F., Choong, E., Munting, A., Cavassini, M., et al. (2024a). Real-world trough concentrations and effectiveness of long-acting cabotegravir and rilpivirine: a multicenter prospective observational study in Switzerland. Lancet Regional Health – Eur. 36, 100793. doi:10.1016/j.lanepe.2023.100793
Thoueille, P., Saldanha, S. A., Schaller, F., Choong, E., Veuve, F., Munting, A., et al. (2024c). Population pharmacokinetics of cabotegravir following oral administration and long-acting intramuscular injection in real-world people with HIV. Clin. Pharmacol. & Ther. 115, 1450–1459. doi:10.1002/cpt.3240
U.S. Food and Drug Administration (2022). Cabenuva product label. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/212888s005s006lbl.pdf (Accessed February, 2023).
U.S. Food and Drug Administration (2011). Edurant product label. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2011/202022s000lbl.pdf (Accessed August, 2023).
U.S. Food and Drug Administration (2021). Juluca product label. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/210192s011lbl.pdf (Accessed August, 2023).
Keywords: rilpivirine, population pharmacokinetics, HIV, NONMEM, long-acting injectable
Citation: Thoueille P, Saldanha SA, Schaller F, Choong E, Veuve F, Munting A, Cavassini M, Braun D, Günthard HF, Duran Ramirez JJ, Surial B, Furrer H, Rauch A, Ustero P, Calmy A, Stöckle M, Di Benedetto C, Bernasconi E, Schmid P, Marzolini C, Girardin FR, Buclin T, Decosterd LA and Guidi M (2024) Population pharmacokinetics of rilpivirine following oral administration and long-acting intramuscular injection in real-world people with HIV. Front. Pharmacol. 15:1437400. doi: 10.3389/fphar.2024.1437400
Received: 23 May 2024; Accepted: 14 October 2024;
Published: 15 November 2024.
Edited by:
Gerardo Garcia-Lerma, Centers for Disease Control and Prevention (CDC), United StatesReviewed by:
Dario Cattaneo, Luigi Sacco Hospital, ItalyKristina Brooks, University of Colorado Anschutz Medical Campus, United States
Copyright © 2024 Thoueille, Saldanha, Schaller, Choong, Veuve, Munting, Cavassini, Braun, Günthard, Duran Ramirez, Surial, Furrer, Rauch, Ustero, Calmy, Stöckle, Di Benedetto, Bernasconi, Schmid, Marzolini, Girardin, Buclin, Decosterd and Guidi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Monia Guidi, bW9uaWEuZ3VpZGlAY2h1di5jaA==