 Kerui Gan1†
Kerui Gan1† Xiaobo Luo
Xiaobo Luo- 1State Key Laboratory of Oral Diseases, National Clinical Research Center for Oral Diseases, Chinese Academy of Medical Sciences, Research Unit of Oral Carcinogenesis and Management, West China Hospital of Stomatology, Sichuan University, Chengdu, Sichuan, China
- 2Department of Pathology, West China Hospital, Sichuan University, Chengdu, China
Common digestive precancerous lesions, including oral potentially malignant disorders (OPMDs), gastric ulcers and colorectal adenoma, harbor high risk of cancerous transformation. Early intervention of these lesions is significant to prevent carcinogenesis and improve patients’ prognosis. Lycopene, a carotenoid predominantly accumulated in tomatoes, is clinically recommended with its cis structure; as lycopene harbors the most potent antioxidative effects among carotenoids, its chemopreventive effects on the premalignant lesions is noted. Despite several reviews have assessed lycopene’s efficacy for OPMDs, emerging studies have reported varying efficacy for digestive precancerous lesion with no comprehensive summary. Therefore, this review initially evaluates the efficacy and underlying mechanisms of lycopene for management of digestive precancerous lesions. According to the included studies, lycopene may show high promise in the management of digestive precancerous lesions, such as relieving mouth opening and burning sensation of oral submucous fibrosis (OSF), presenting potentially equivalent efficacy on managing oral lichen planus (OLP) as steroids and alleviating gastrointestinal precancers’ symptoms, meanwhile lowering colon cancer risk. Moreover, its mechanisms for managing digestive precancerous lesions are concretely summarized, including anti-oxidative stress effects, anti-inflammatory response and regulation of cell proliferation and apoptosis, especially its modifications on TLR4/TRIF/NF-κB signaling pathway and p53-dependent cell cycle control and apoptosis. More studies are warranted to confirm its long-term efficacy and preventive role against malignant transformation of digestive precancerous lesions as evidence is insufficient.
1 Introduction
Digestive cancers pose a significant threat to patients’ life, usually along with poor prognosis. According to Global Cancer Observatory (GCO), colorectal cancer ranked as the fourth most prevalent malignancy worldwide in 2022, while stomach cancer and oral cancer ranks sixth and 17th respectively. Moreover, the estimated mortality rates of 2.4% and 5.7% for cancers of the lip and oral cavity and the esophagus respectively, and 8.4% along with 11.5% individually for stomach and colorectum cancers, indicated that digestive cancers serve as huge burden for human health (Global Cancer Observatory, 2022). Notably, early intervention in the precancerous stage of digestive cancers could significantly reduce the risk of malignant transformation and improve the life quality of patients (Kumari et al., 2022; Kizhakkoottu and Ramani, 2024; Choi et al., 2024). As for oral potentially malignant disorders (OPMDs) which has an overall malignant transformation rate of 7.9%, early prevention and intervention of OPMDs is of great importance to minimize the risk of malignant transformation (Kumari et al., 2022).
Precancerous lesions, also known as premalignant lesions, are epithelial aberrant alterations that possess the potential to progress into cancers if left untreated. Oral precancerous lesions are usually referred to as OPMDs, which refer to a spectrum of oral mucosal disorders that carry an increased risk of malignant transformation into oral squamous cell carcinoma (OSCC), including oral leukoplakia (OLK), oral submucous fibrosis (OSF), oral lichen planus (OLP), etc. (Warnakulasuriya et al., 2021). OPMDs severely impact the quality of life for patients and can even be life-threatening. For example, the main clinical manifestation of OSF is a burning sensation and intolerance to spices, and as the disease progresses, patients experience reduction in mouth opening, which not only causes pain, poor oral hygiene and impaired chewing and swallowing, but also affects patients’ speaking and appearance, causing psychological issues and limitations in social activities (Peng et al., 2020). Similarly, common types of gastric premalignant lesions are comprised of gastric ulcers, gastric polyps, atrophic gastritis, intestinal metaplasia, etc. (Wang et al., 2022). As for colorectum, aberrant crypt foci (ACF) are the earliest precursor to colorectal cancer (CRC), and colorectal adenoma is the most frequent precancerous lesion; besides, other less-frequent colorectal premalignant lesions cover inflammatory bowel disease (IBD) and some hereditary syndromes (Alrawi et al., 2006; Conteduca et al., 2013; Orlando et al., 2008).
Lycopene is one sort of non-provitamin A and liposoluble carotenoid, acting as a vital part of the human diet. As it could not been synthesized by human body, the primary intake of which is from dietary sources such as ripe tomatoes, pink guavas and several other red fruits and vegetables (Bramley, 2000), with at least 85% of the lycopene in the human diet deriving from tomatoes and tomato products (Bramley, 2000). The red carotenoid is a straight-chain unsaturated alkene with the chemical formula C40H56 that can exist in both cis and trans isomers. While predominantly serving as all-trans isomer in natural plants, the majority of lycopene in human plasma and tissues is cis-isomer, which has superior polarity and water solubility than all-trans isomer (Gärtner et al., 1997; Cooperstone et al., 2015). As a result, compared to the all-trans isomer, the cis form may be better absorbed through the digestive tracts. In vitro, the configuration transformation from trans-isomer to cis-isomer can be accomplished through light, heat and specific chemical processes; in vivo, gastrointestinal and liver enzymes are the main agents responsible for isomerization (Ross et al., 2011). Owing to its liposoluble and isomeric characters, lycopene is more bioavailable in processed tomato products such as ketchup than in raw tomatoes, especially when the carotenoid is processed with oil (Fielding et al., 2005; Tan et al., 2010). Therefore, cis-isomerized lycopene is recommended for clinical use. Lycopene has been utilized as a plant pigment due to its characteristic of red color, however, its potent antioxidant activity and chemopreventive effect have gained increasing attention in recent years.
So far, accumulating evidences have indicated the positive effects of lycopene in preventing cervical and prostate cancers (Mirahmadi et al., 2020). For instance, an umbrella meta-analysis published in 2024 revealed that dietary lycopene is reversely associated with the risk of prostate cancer, digestive cancer and head and neck cancer (Sui et al., 2024). The therapeutic effects of lycopene for head and neck and digestive cancers have also been recognized in the literatures (Al-Ishaq et al., 2020; Zanoni et al., 2019). Besides, as mentioned above, early detection or intervention is crucial in minimizing the possibility of the malignant tumor formation (Kumari et al., 2022; Kizhakkoottu and Ramani, 2024; Choi et al., 2024). Hence, it is important to explore various modalities and mechanisms of preventing and treating digestive precancerous lesions. Notably, emerging researches have suggested the efficacy and mechanisms of lycopene in managing precancerous lesions of the digestive tract including OPMDs, ulcerative colitis, etc. (Kumar et al., 2007; Patil et al., 2014; Singh et al., 2014; Subramaniam et al., 2014; Goel and Ahmed, 2015; Nayak, 2015; Patil et al., 2015; Kopuri et al., 2016; Saran et al., 2018; Piyush et al., 2019; Johny et al., 2019; Arakeri et al., 2020; Gupta et al., 2021; Singh et al., 2004; Singh and Bagewadi, 2017; Kushwaha, 2017; Eita et al., 2021; Hazzaa et al., 2021; Jain and Katti, 2015; Głąbska et al., 2016; Głąbska et al., 2019; Tekeli et al., 2019; Yin et al., 2023; Jung et al., 2013), with rare side effects, which may correlate with its antioxidative mechanisms (Eita et al., 2021; Tekeli et al., 2019; Yin et al., 2023; Boyacioglu et al., 2016; Jain et al., 1999; Aljawad et al., 2014; Li et al., 2021; Sengupta et al., 2006; Liu et al., 2006; Vrieling et al., 2007); one study of meta-analysis in 2020 incorporating 7 RCTs of OSF reported that lycopene is only effective in refining maximum mouth opening without improving other symptoms (Guo et al., 2020); while another study including relevant studies up to April of 2022 indicated that lycopene was capable of relieving symptoms of mouth opening and tongue protrusion of patients with OSF, which meanwhile reducing pain and promoting resolution of OLP, exhibiting comparable efficacy as steroids (Al-Maweri et al., 2023); therefore, conflicting efficacy of lycopene for managing OPMDs was implied. Meanwhile, as digestive cancers pose heavy health burden globally, no relevant review assessing the efficacy of lycopene for digestive precancers has been proposed. Therefore, it is warranted for us to update the previous reviews of OPMDs and gastrointestinal premalignant lesions, and comprehensively assess and explore the potential role of lycopene in managing these digestive precancerous lesions.
2 Efficacy of lycopene in digestive precancerous lesions
In recent years, numerous studies have evaluated the efficacy of lycopene in managing precancerous lesions of the digestive tract, and relevant clinical or animal studies over the last 10 years have been summarized and shown in Table 1.
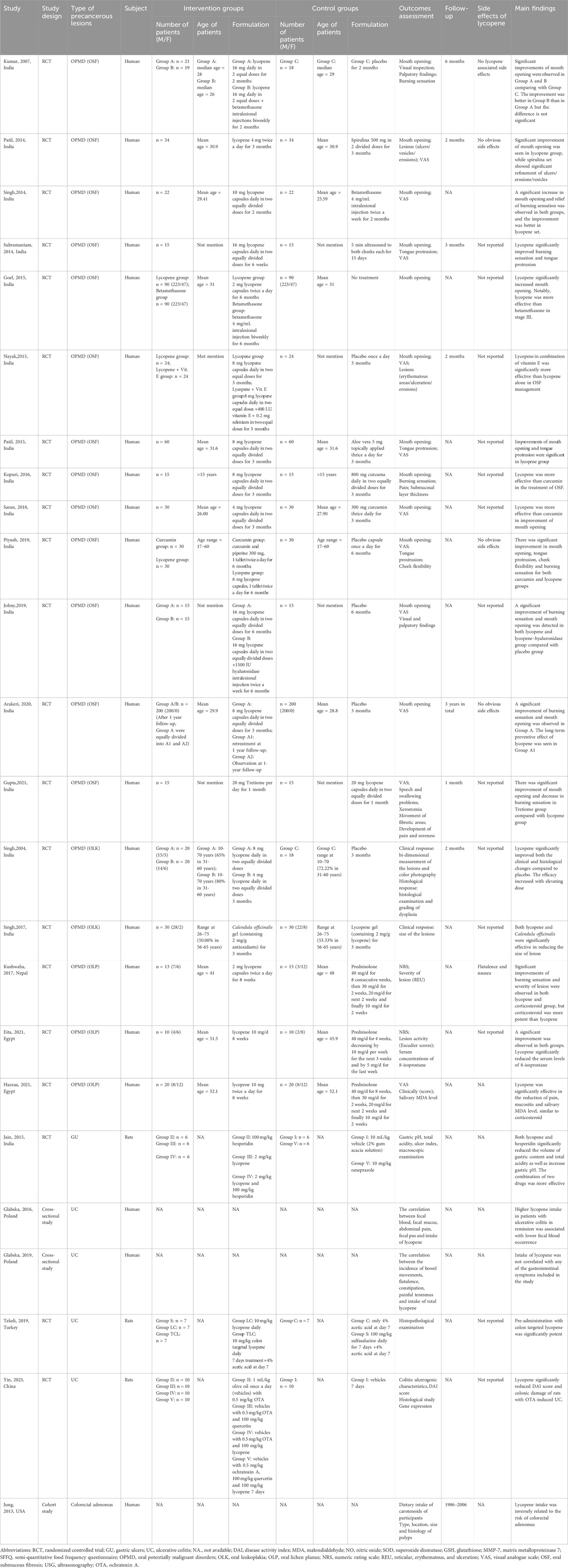
Table 1. General characteristics of included literatures evaluating efficacy of lycopene on digestive precancerous lesions.
2.1 Lycopene for the management of oral potentially malignant disorders
OSF is one of the most common OPMDs closely related to the consumption of betel nuts (Warnakulasuriya and Chen, 2022). After reviewing these relevant studies, 13 studies demonstrated that lycopene could significantly refine the clinical manifestations of OSF patients, among which 12 randomized controlled trial (RCT) studies have compared the potential efficacy between lycopene and other treatment modalities or the combinational effectiveness of lycopene with other drugs, apart from one study by Arakeri et al. which focused on the long-term efficacy of lycopene rather than its comparison with other therapeutic reagents (Kumar et al., 2007; Patil et al., 2014; Singh et al., 2014; Subramaniam et al., 2014; Goel and Ahmed, 2015; Nayak, 2015; Patil et al., 2015; Kopuri et al., 2016; Saran et al., 2018; Piyush et al., 2019; Johny et al., 2019; Arakeri et al., 2020; Gupta et al., 2021).
Glucocorticoids, either topical or oral administration, has long been utilized for treating OSF due to its anti-inflammatory effects. Two studies have explored the various efficacy between lycopene and betamethasone for the treatment of OSF(23,25). Singh’s study including 44 patients demonstrated that lycopene was superior than intralesional injection of betamethasone in improving mouth opening and burning sensation (Singh et al., 2014). However, another study dividing 270 OSF patients into 3 different clinical stages and the effectiveness was assessed in various stages; specifically, lycopene capsules and intralesional injected betamethasone were comparatively effective in increasing the mouth opening in patients at stage I, while betamethasone was more effective than lycopene in stage II, by contrast, lycopene was more potent than betamethasone in stage III. The distinct results may be correlated with varied accessibility of betamethasone for patients at different clinical stages with various degree of mouth opening (Goel and Ahmed, 2015). Apart from the above comparative studies, the RCT study of Kumar and colleagues investigated the efficacy about the combination of lycopene and betamethasone contrasted to the single application of lycopene. The results suggest that although the improvement of mouth opening was better in combination group, the difference was insignificant (Kumar et al., 2007). More RCTs with larger population exploring the combination of lycopene with steroids are required for further evidence of the combined application, thus lowering the side effects of steroids with less needed dose.
Besides, three studies have analyzed and compared the therapeutic effects between lycopene and curcumin (Kopuri et al., 2016; Saran et al., 2018; Piyush et al., 2019). Kopuri’s study revealed that lycopene possessed better performance in improving mouth opening and fibrous bands whereas curcumin mainly contributed to better refining in burning sensation and blanching, concluding that lycopene was more effective than curcumin on the treatment of OSF(28). Similarly, another study indicated that lycopene was more efficacious in increasing mouth opening than curcumin, while none significant relief of burning sensation was indicated between these two drugs (Saran et al., 2018). Besides, Piyush and colleagues have reported the equivalent therapeutic efficacy between lycopene and curcumin for OSF(30).
Additionally, in comparison to aloe vera which is another antioxidant, lycopene exhibited better therapeutic effects in treating OSF (Patil et al., 2015; Sudarshan et al., 2012). Patil et al. discovered that lycopene exhibited a greater effect regarding the enhancement of mouth opening, while spirulina was more advantageous in reducing ulcers (Patil et al., 2014). In a single-blinded RCT, the researchers revealed that Tretiome was superior to lycopene as for the refinement of mouth opening and burning sensation (Gupta et al., 2021). Moreover, several studies have examined the combinatorial efficacy of lycopene with other drugs for OSF. One study suggested that the combination of lycopene and vitamin E may remarkably improve the clinical symptoms of OSF patients than lycopene alone (Nayak, 2015). However, when lycopene was used in combination with hyaluronidase, the effect was comparative as that of lycopene alone (Johny et al., 2019).
While the above studies assessed the efficacy of lycopene in comparison to other drugs or their combination for OSF, the study by Subramaniam et al. investigated the various effectiveness between lycopene and a non-pharmacological approach, therapeutic ultrasound, for managing OSF, suggesting that lycopene has better performance in improving burning sensation and tongue protrusion (Subramaniam et al., 2014). Notably, Arakeri et al. have evaluated the long-term efficacy of lycopene in OSF. Specifically, part of the participants received a second intervention 1 year after the initial treatment of 3 consecutive months. After 1 year of follow-up post re-treatment, recurrence of symptoms was observed among the participants without re-treatment, whereas the clinical manifestations of retreated patients were as that in the initial treatment. Besides, no lycopene related-side effects were observed during the whole trial. Therefore, re-treatment with lycopene at 1 year after the onset of its initial therapy was beneficial in preventing the recurrence of the symptoms (Arakeri et al., 2020).
Hence, based on findings from several RCTs, Lycopene is efficacious in improving mouth opening, tongue protrusion, and burning sensation of OSF compared with placebo; besides, the combination of lycopene with vitamin E might achieve better outcome, so the combined application of lycopene with other strategies are warranted to be confirmed in more well-designed RCTs. Moreover, re-treatment with lycopene is recommended to prevent the symptoms from recurring.
OLK is one common type of OPMDs whose overall malignant transformation rate is estimated to be 3.5% (Aguirre-Urizar et al., 2021). Singh et al. examined the therapeutic effects of lycopene on OLK, concluding that it could significantly refine both clinical signs and histological progression of OLK lesions compared to placebo; and positive correlation was observed between the efficacy and the dosage of drug (Singh et al., 2004). Another study comparing the efficacy between lycopene gel and Calendula officinalis gel for OLK showed that lycopene had similar effectiveness as the other gel, both of which significantly reduced the size of OLK (35). In all, more well-designed RCT is required to validate the efficacy of lycopene for preventing malignant transformation and reducing lesion size of OLK.
OLP is typically treated with topical steroids, with systemic corticosteroids being a common recommendation for resistant patients; however, the application of steroids carry multiple risks, such as adrenal suppression, Cushing’s syndrome and immunosuppression (Liu et al., 2013; K et al., 2011). Three studies examined the therapeutic effects of lycopene on OLP and compared the efficacy between lycopene and prednisolone (Kushwaha, 2017; Eita et al., 2021; Hazzaa et al., 2021). One study showed that, although lycopene significantly reduced clinical symptoms such as burning sensation and severity of lesion in patients with OLP, prednisolone was more effective than lycopene; besides, the lycopene group experienced side effects such as flatulence and nausea, while the prednisolone group reported side effects such as facial puffiness and dizziness (Kushwaha, 2017). However, in two other RCTs, the lycopene group exhibited a statistically significant decrease in pain and lesion severity, and lycopene showed comparable efficacy to that of prednisolone (Eita et al., 2021; Hazzaa et al., 2021). As no lycopene-related side effects were reported in either study, Eita et al. reported occurrence of facial puffiness, gastrointestinal disorders and weakness associated with prednisolone (Eita et al., 2021; Hazzaa et al., 2021). Thus, lycopene serves as a potent alternative when steroids is unsuitable.
As the study on OLP or OLK are still too limited to support the therapeutic role of lycopene, more well-designed studies with long-term observation are required to further uncover the potential.
2.2 Lycopene for the management of gastrointestinal precancerous lesions
Up till now, a few studies have confirmed the potential of lycopene in the treatment of certain gastrointestinal precancerous lesions (Jain and Katti, 2015; Głąbska et al., 2016; Głąbska et al., 2019; Tekeli et al., 2019; Yin et al., 2023; Jung et al., 2013). Jain et al. have performed one RCT exploring the effectiveness of lycopene and hesperidin on pyloric ligation-induced gastric ulcer in rats (Jain and Katti, 2015). The results implied that, although the combination of lycopene and hesperidin exhibited better efficacy, lycopene alone could already markedly reduce the volume of gastric contents, total acidity, and elevate the gastric pH (39).
Ulcerative colitis (UC), one of the dominant forms of inflammatory bowel disease, is associated with an increased risk of developing CRC (9). A cross-sectional study by Glabska et al. analyzed the correlation between the diet of UC patients in remission and their gastrointestinal symptoms, indicating that a higher consumption of lycopene was correlated with a lower incidence of fecal blood in these patients, whereas another similar study by the same research group reported no significant association between lycopene intake and the decreased occurrence of constipation in UC patients (Głąbska et al., 2016; Głąbska et al., 2019). The results of these two trials suggest that increasing the intake of lycopene may alleviate certain gastrointestinal symptoms and improve the overall wellbeing of UC patients, although further prospective studies with large samples are required to confirm this conclusion. The protective effect of lycopene against UC has also been confirmed in animal studies. One, conducted by Yin et al., revealed that lycopene significantly decreased the colonic damage caused by ochratoxin A (OTA)-induced UC(43). Another study that examined the comparative protective effects of conventional and colon-targeted lycopene on acetic acid-induced UC revealed that UC colonic damage, such as ulceration and hemorrhage, was significantly improved in the colon-targeted lycopene group compared with the acetic acid-induced UC group, while no significant changes were observed in conventional lycopene, although there were signs of improvement (Tekeli et al., 2019).
Colorectal adenomas are precancerous lesions of nearly all sporadic CRC (9). In a cohort study with a total of 29,363 patients, out of whom 3,997 were diagnosed with colorectal adenoma, the association between risk of colorectal adenomas and intake of specific carotenoids was analyzed, showing that lycopene intake was negatively correlated with adenoma risk (Jung et al., 2013).
Thus, unlike these studies performed in OPMDs, the studies investing the efficacy of lycopene on managing gastrointestinal precancerous lesions were predominantly limited to animal studies, observational studies, or cohort studies, RCTs evaluating on its efficacy are needed in the future.
3 Possible mechanisms of lycopene in managing premalignant lesions of digestive tract
3.1 Antioxidative mechanisms
Lycopene is a potent antioxidant and has strong capacity to protect against oxidative damage, therefore playing a crucial role in treating selected disorders associated with oxidative stress, including some of the precancerous lesions (Figure 1).

Figure 1. An overview of antioxidative mechanism of lycopene in managing premalignant lesions of digestive tract. Abbreviations: MDA: malondialdehyde; GSH: glutathione; SOD: superoxide dismutase; CAT: catalase; GU: gastric ulcers; ACF: aberrant crypt foci; UC: ulcerative colitis; OLP: oral lichen planus.
As immune system is reported to play primary role in the pathogenesis and carcinogenesis of OLP, free radicals and ROS may intensify the dysfunction of the immune system (Fu et al., 2000). 8-isoprostane serves as a reliable biomarker of oxidative stress (Amirchaghmaghi et al., 2016). The result of one RCT showed significant decrease of serous 8-isoprostane following 8 weeks of lycopene administration, suggesting that lycopene’s effects on OLP might be associated with its ability to reduce oxidative stress (Eita et al., 2021).
Gastric ulcers can be triggered by a variety of factors, including nonsteroidal anti-inflammatory drugs (NSAIDs) and alcohol. Boyacioglu et al. conducted an RCT to investigate the prophylactic effects of lycopene against indomethacin-induced gastric ulcer in rats (Boyacioglu et al., 2016).The results showed that pre-administration of lycopene could protect against DNA damage induced by indomethacin, possibly by improving the superoxide dismutase (SOD) activity, glutathione (GSH) level and decreasing catalse (CAT) activity, malondialdehyde (MDA) level and myeloperoxidase (MPO) activity, thus exerting its antioxidative effects. Another study also confirmed the anti-lipid peroxidation capacity of lycopene on azoxymethymethane (AOM) induced- ACF which is one of the preneoplastic lesions of colorectal carcinoma (Jain et al., 1999).Aljawad et al. investigated the preventive effect of both Vanadyl sulfate and lycopene in comparison to Lansoprazole in ethanol–induced gastric ulcer and concluded that these two drugs exert a positive effect through antioxidative stress (Aljawad et al., 2014).
Studies have indicated a strong correlation between oxidative stress and the progression of UC (Zhou et al., 2018). Li et al. investigated the prophylactic effect and mechanism of lycopene in dextran sulfate sodium (DSS)-induced UC, and they revealed that compared to DSS group, the clinical symptoms of mice in lycopene pre-administrated group were much better controlled and the level of the antioxidant enzymes and lipid peroxidation were significantly decreased (Li et al., 2021). Another study found that lycopene significantly reduced levels of MDA, nitric oxide (NO), MPO and hydroxyproline and increase levels of SOD and GSH, thereby inhibiting oxidative stress and lipid peroxidation and exerting therapeutic effect in ochratoxin A (OTA)-induced UC rats (Yin et al., 2023). Moreover, regarding that GSH is critical in DNA synthesis, while DNA damage is correlated with UC, we can conclude that lycopene exerts its beneficial effect on UC by preventing oxidative-related DNA damage (Yin et al., 2023; Zhang et al., 2024).
3.2 Anti-inflammatory response
3.2.1 TLR4/TRIF/NF-κB signaling pathway
It is reported that the progression of UC is closely associated with the TLR4/NF-κB signaling pathway which has emerged as a vital target for therapeutic interventions aimed at preventing of UC development. Once toll-like receptor 4 (TLR-4) is activated, Tir domain-containing adaptor inducing interferon-beta (TRIF) can bind to TRAF6, then activate a series of kinases, promote entry of activated nuclear factor-kappa B (NF-κB) into nucleus and activate the transcription factor, ultimately leading to the expression and release of inflammatory cytokines. Li et al. found that lycopene pre-administration could modulate the TLR4/TRIF/NF-κB pathway by significantly downregulating the expressions of TLR-4, TRIF, phosphorylated p65 proteins, which in turn suppresses the production of inflammatory cytokines IFN-γ, TNF-α, IL-6, and IL-1β in colonic tissue, thereby reducing inflammation response in the context of UC(48). Additionally, the expression of tight junction-associated proteins in colonic tissues was significantly upregulated after the intervention, suggesting that the intervention may attenuate damage to intercellular tight junctions triggered by inflammatory factors, thereby protecting the intestinal mucosal barrier integrity.
3.2.2 Downregulate expressions of cyclooxygenase-2 and inducible nitric oxide synthase
Overexpression of cyclooxygenase-2 (COX-2) and inducible nitric oxide synthase (iNOS) are correlated to colorectal carcinogenesis, and inhibition of their activities leads to cancer prevention (Sheehan et al., 1999; Rao et al., 1999; de Oliveira et al., 2017). Sengupta et al. discovered that lycopene significantly decreased the incidence of AOM-induced ACF, the earliest precursor of CRC, by inhibiting of COX-2 and iNOS, which were overexpressed in the process of colorectal carcinogenesis, thereby preventing the development of CRC (49).
3.2.3 Downregulate expression of NF-κB and upregulate expression of Nrf-2
NF-κB regulated inflammatory responses and its activation lead to increased expression of pro-inflammatory cytokines, while nuclear factor-erythroid 2–related factor 2 (Nrf-2) reduced the synthesis of inflammatory mediators by inhibiting the NF-κB (Hegazy and El-Bedewy, 2010; Thimmulappa et al., 2016). The study conducted by Tekeli et al. revealed that lycopene significantly decreased levels of NF-κB, IL-1β and IL-6 while increasing the level of Nrf-2, implying that lycopene acts as an anti-inflammatory agent in UC by suppressing the expression of NF-κB and promoting the expression of Nrf-2 (42) (Figure 2).
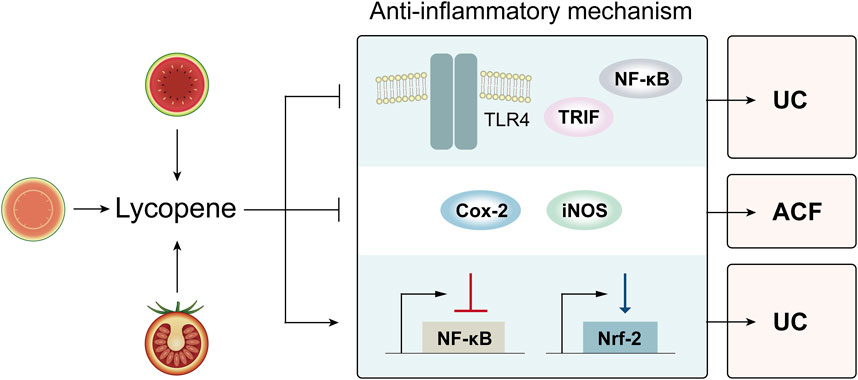
Figure 2. Various anti-inflammatory effects of lycopene in controlling digestive premalignant lesions. Abbreviations: TLR4: toll-like receptor 4; TRIF: Tir domain-containing adaptor inducing interferon-beta; NF-κB: nuclear factor-kappa B; Cox-2: cyclooxygenase-2; iNOS: inducible nitric oxide synthase; Nrf-2: nuclear factor-erythroid 2–related factor 2; UC: ulcerative colitis; ACF: aberrant crypt foci.
3.3 Anti-cell proliferation and pro-apoptosis effects
3.3.1 p53-dependent cell cycle control and apoptosis
p53 is a crucial gene that regulates the balance between cell proliferation and apoptosis through a variety of routes by activating its target genes p21Waf1/Cip1 and BCL2-associated X protein (Bax)-1. Studies have shown that malfunction and mutation of p53 gene may lead to an escalation in cell proliferation and a reduction in apoptosis, ultimately carcinogenesis, including gastric carcinogenesis (Moss, 1998; Xie et al., 2004). Specifically, under the stimulation of DNA damage, p53 is activated and its target genes p21Waf1/Cip1 and Bax-1 are inhibited, and suppression of p21Waf1/Cip1 towards cyclin-CDK and proliferating cellular nuclear antigen (PCNA) is diminished, thereby activating the cell cycle. Similarly, when Bax-1 is inhibited, caspase-3 is inactivated. As a result, the balance between cell proliferation and apoptosis is disrupted, contributing to gastric carcinogenesis (El-Deiry, 1998; Isobe et al., 2004; Aoyagi et al., 2003). Study by Liu et al. revealed that lycopene could re-establish this disturbed balance. They showed that smoking increased the expressions of total p53 and phosphorylated p53 in the gastric mucosa, while lycopene supplementation could significantly reversed the aberrant changes; furthermore, lycopene not only prevented the smoking-induced decrease in p21waf1/cip1, proapoptotic protein Bax-1 and cleaved caspase 3 but also reversed the increase in the cell proliferation markers including cyclin D1 and PCNA, suggesting that lycopene protects the gastric mucosa from smoking-induced damage through p53-dependent cell cycle control and apoptosis, and may counteract the development of gastric cancer associated with smoking (Liu et al., 2006) (Figure 3).
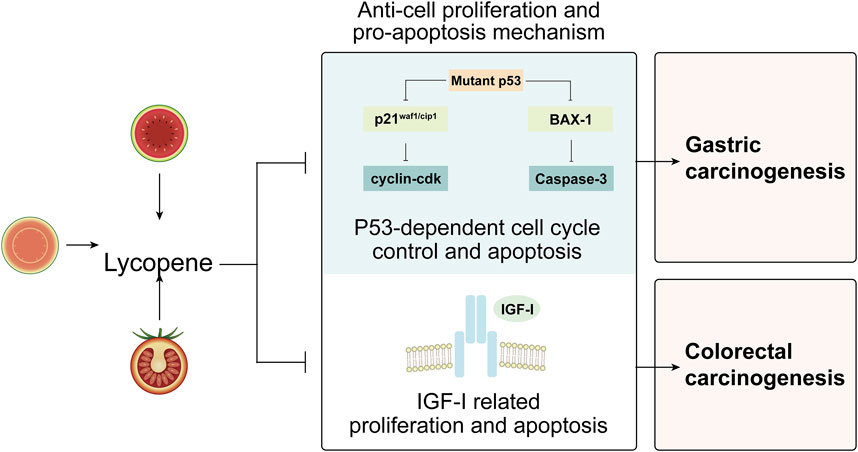
Figure 3. Potential anti-proliferation and pro-apoptosis machinery of lycopene in the management of precancerous lesions of digestive tract. Abbreviations: BAX: BCL2-associated X protein; IGF-I: insulin-like growth factor I.
3.3.2 Insulin-like growth factor I-related proliferation and apoptosis
Higher serum level of insulin-like growth factor I (IGF-I) has been associated with an increased risk of cancer by stimulating proliferation and suppressing apoptosis (Giovannucci et al., 2000; Liu et al., 2003). In a crossover study by Vrieling et al., lycopene was observed to increase the concentrations of circulating insulin-like growth factor binding proteins (IGFBP)-1 and −2, thereby reducing the binding of IGF-I to its receptor, which may indirectly result in decreased bioavailability of IGF-I, potentially playing a preventive role in the development of colorectal cancer (Vrieling et al., 2007) (Figure 3).
4 Discussion
In this review, we briefly introduced the natural sources, biosafety and bioactivity of lycopene and summarized its potential efficacy as well as mechanisms underlying its preventive effects on digestive premalignant lesions.
Lycopene is recognized as a safe and potent antioxidant, playing a significant role in the management of precancerous lesions through several mechanisms, including anti-oxidative stress, anti-inflammatory response and regulation of cell proliferation and apoptosis. Lycopene is vital in treating certain digestive precancerous lesions associated with oxidative stress. It exerts anti-inflammatory effects by modulating TLR4/NF-κB signalling pathway and regulation of molecules such as COX-2, iNOS, NF-κB and Nrf-2. Additionally, lycopene corrects the imbalance between cell proliferation and apoptosis by influencing p53 and IGF-I related proliferation and apoptosis.
Most of the RCT studies regarding OSF indicate that lycopene could relieving mouth opening and burning sensation of patients, thereby improving the life quality. However, given the small sample sizes of these RCTs, the generalizability of the findings is limited. In addition, demographic diversity is not mentioned in most of the studies, which may affect the applicability of the findings to various populations. Besides, lycopene might be regarded as a potent alternative strategy for managing OLP when steroids is not appropriate, offering comparative and safer therapeutic effect with less side effects. Although the underlying mechanisms are unclear, Haque et al. revealed that IFN-γ, an anti-fibrotic cytokine, could significantly reverse clinical signs of OSF patients; while in another study, lycopene was observed to suppress hepatic fibrogenesis, suggesting that lycopene may exert its positive effect on OSF by inhibiting fibrosis (Haque et al., 2001; Heber and Lu, 2002). Moreover, lycopene might exhibit preventive potential for managing other digestive precancers including gastric ulcer, UC and colorectal adenomas, suggesting its broad application in digestive premalignant lesions (Figure 4).

Figure 4. Summary regarding the efficacy of lycopene against digestive premalignant lesions. Abbreviations: OPMDs: oral potentially malignant disorders; OSF: oral submucous fibrosis; OLP: oral lichen planus; OLK: oral leukoplakia.
For the current research, we offered an exhaustive synthesis of the evidence regarding lycopene’s role in managing digestive precancerous lesions and recommendations are made for the clinical use of lycopene. However, insufficient research is currently available to support the role of lycopene in preventing malignant transformation of digestive lesions, thus, larger sample sizes of human clinical trials are warranted to further uncover the potential role of lycopene in preventing the malignant transformation of digestive lesions. we suggest that the long-term effects of lycopene and its combination with other therapies for digestive premalignant lesions are worth investigating. And studies on the bioavailability of lycopene in different dosage forms may contribute to improve the red carotenoid’s efficacy.
In all, based on our research, it is promising to exploit lycopene as a convenient and efficacious approach for alleviating symptoms and preventing malignant transformation of digestive precancerous lesions as well as improving patients’ life quality and prognosis. We call for more research on the role of lycopene in preventing the malignant transformation of digestive precancerous lesions.
Author contributions
KG: Data curation, Investigation, Visualization, Writing–original draft, Writing–review and editing. WS: Data curation, Visualization, Writing–original draft, Writing–review and editing. XLi: Investigation, Visualization, Writing–review and editing. WD: Investigation, Writing–review and editing. YQ: Funding acquisition, Supervision, Writing–review and editing. XLu: Conceptualization, Funding acquisition, Supervision, Writing–review and editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work is supported by National Natural Science Foundation of China (82272899, 81902782, 81730030, 82203180), Research Funding from West China School/Hospital of Stomatology Sichuan University (No. RCDWJS 2022-16), Postdoctoral Research Funding of Sichuan University (2022SCU12132), Research and Develop Program, West China Hospital of Stomatology, Sichuan University (No. RD-02-202204), Key Research Program of Sichuan Provincial Science and Technology Agency (2023YFS0127), Youth Fund Projects of Sichuan Provincial Science and Technology Agency (24NSFSC7843) and the CAMS Innovation Fund for Medical Sciences (CIFMS, 2019-I2M-5-004).
Acknowledgments
We would like to thank the authors of these original studies on this topic included in our review.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Aguirre-Urizar, J. M., Lafuente-Ibáñez de Mendoza, I., and Warnakulasuriya, S. (2021). Malignant transformation of oral leukoplakia: systematic review and meta-analysis of the last 5 years. Oral Dis. 27 (8), 1881–1895. doi:10.1111/odi.13810
Al-Ishaq, R. K., Overy, A. J., and Büsselberg, D. (2020). Phytochemicals and gastrointestinal cancer: cellular mechanisms and effects to change cancer progression. Biomolecules 10 (1), 105. doi:10.3390/biom10010105
Aljawad, F. H., Jawad, M. J., and FadhiL, O. K. (2014). Vanadyl sulfate and Lycopene in prevention of Ethanol induced gastric ulcer. AL-yarmouk J. (1), 1–11.
Al-Maweri, S. A., Halboub, E., Al-Qadhi, G., Al-Wesabi, M., Al-Sharani, H. M., Parveen, S., et al. (2023). Efficacy of lycopene for management of oral potentially malignant disorders: a systematic review and meta-analysis. Oral Surg. Oral Med. Oral Pathology Oral Radiology 135 (1), 79–95. doi:10.1016/j.oooo.2022.08.004
Alrawi, S. J., Schiff, M., Carroll, R. E., Dayton, M., Gibbs, J. F., Kulavlat, M., et al. (2006). Aberrant crypt foci. Anticancer Res. 26 (1A), 107–119.
Amirchaghmaghi, M., Hashemy, S. I., Alirezaei, B., Jahed Keyhani, F., Kargozar, S., Vasigh, S., et al. (2016). Evaluation of plasma isoprostane in patients with oral lichen planus. J. Dent. (Shiraz) 17 (1), 21–25.
Aoyagi, K., Koufuji, K., Yano, S., Murakami, N., Miyagi, M., Koga, A., et al. (2003). The expression of p53, p21 and TGF beta 1 in gastric carcinoma. Kurume Med. J. 50 (1–2), 1–7. doi:10.2739/kurumemedj.50.1
Arakeri, G., Patil, S., Maddur, N., Rao Us, V., Subash, A., Patil, S., et al. (2020). Long-term effectiveness of lycopene in the management of oral submucous fibrosis (OSMF): a 3-years follow-up study. J. Oral Pathol. Med. 49 (8), 803–808. doi:10.1111/jop.13085
Boyacioglu, M., Kum, C., Sekkin, S., Yalinkilinc, H. S., Avci, H., Epikmen, E. T., et al. (2016). The effects of lycopene on DNA damage and oxidative stress on indomethacin-induced gastric ulcer in rats. Clin. Nutr. 35 (2), 428–435. doi:10.1016/j.clnu.2015.03.006
Bramley, P. M. (2000). Is lycopene beneficial to human health? Phytochemistry 54 (3), 233–236. doi:10.1016/s0031-9422(00)00103-5
Choi, S. J., Choi, H. S., Kim, H., Lee, J. M., Kim, S. H., Yoon, J. H., et al. (2024). Gastric cancer and intestinal metaplasia: differential metabolic landscapes and new pathways to diagnosis. Int. J. Mol. Sci. 25 (17), 9509. doi:10.3390/ijms25179509
Conteduca, V., Sansonno, D., Russi, S., and Dammacco, F. (2013). Precancerous colorectal lesions (Review). Int. J. Oncol. 43 (4), 973–984. doi:10.3892/ijo.2013.2041
Cooperstone, J. L., Ralston, R. A., Riedl, K. M., Haufe, T. C., Schweiggert, R. M., King, S. A., et al. (2015). Enhanced bioavailability of lycopene when consumed as cis-isomers from tangerine compared to red tomato juice, a randomized, cross-over clinical trial. Mol. Nutr. and Food Res. 59 (4), 658–669. doi:10.1002/mnfr.201400658
de Oliveira, G. A., Cheng, R. Y. S., Ridnour, L. A., Basudhar, D., Somasundaram, V., McVicar, D. W., et al. (2017). Inducible nitric oxide synthase in the carcinogenesis of gastrointestinal cancers. Antioxid. Redox Signal 26 (18), 1059–1077. doi:10.1089/ars.2016.6850
Eita, A. A. B., Zaki, A. M., and Mahmoud, S. A. (2021). Serum 8-isoprostane levels in patients with resistant oral lichen planus before and after treatment with lycopene: a randomized clinical trial. BMC Oral Health 21 (1), 343. doi:10.1186/s12903-021-01711-z
El-Deiry, W. S. (1998). Regulation ofp53downstream genes. Seminars Cancer Biol. 8 (5), 345–357. doi:10.1006/scbi.1998.0097
Fielding, J. M., Rowley, K. G., Cooper, P., and O’ Dea, K. (2005). Increases in plasma lycopene concentration after consumption of tomatoes cooked with olive oil. Asia Pac J. Clin. Nutr. 14 (2), 131–136.
Fu, Y. C., Jin, X. P., Wei, S. M., Lin, H. F., and Kacew, S. (2000). Ultraviolet radiation and reactive oxygen generation as inducers of keratinocyte apoptosis: protective role of tea polyphenols. J. Toxicol. Environ. Health A 61 (3), 177–188. doi:10.1080/00984100050131323
Gärtner, C., Stahl, W., and Sies, H. (1997). Lycopene is more bioavailable from tomato paste than from fresh tomatoes. Am. J. Clin. Nutr. 66 (1), 116–122. doi:10.1093/ajcn/66.1.116
Giovannucci, E., Pollak, M. N., Platz, E. A., Willett, W. C., Stampfer, M. J., Majeed, N., et al. (2000). A prospective study of plasma insulin-like growth factor-1 and binding protein-3 and risk of colorectal neoplasia in women. Cancer Epidemiol. Biomarkers Prev. 9 (4), 345–349.
Głąbska, D., Guzek, D., Zakrzewska, P., and Lech, G. (2019). Intake of lutein and zeaxanthin as a possible factor influencing gastrointestinal symptoms in caucasian individuals with ulcerative colitis in remission phase. J. Clin. Med. 8 (1), 77. doi:10.3390/jcm8010077
Głąbska, D., Guzek, D., Zakrzewska, P., Włodarek, D., and Lech, G. (2016). Lycopene, lutein and zeaxanthin may reduce faecal blood, mucus and pus but not abdominal pain in individuals with ulcerative colitis. Nutrients 8 (10), 613. doi:10.3390/nu8100613
Global Cancer Observatory (2022). Cancer Today. Available at: https://gco.iarc.fr/en (Accessed: 19 September 2024).
Goel, S., and Ahmed, J. (2015). A comparative study on efficacy of different treatment modalities of oral submucous fibrosis evaluated by clinical staging in population of Southern Rajasthan. J. Can. Res. Ther. 11 (1), 113–118. doi:10.4103/0973-1482.139263
Guo, J., Xie, H., Wu, H., and Liang, M. (2020). Efficacy of lycopene in the treatment of oral submucous fibrosis: a meta-analysis of randomized controlled trials. J. Evid. Based Dent. Pract. 20 (4), 101471. doi:10.1016/j.jebdp.2020.101471
Gupta, A., Kumar, S., Srivastava, P., Rathi, V. C., Saxena, S., and Aggarwal, A. (2021). Effect of trans retinoic acid on patients with oral submucous fibrosis-randomized single-blind monocentric study. J. Oral Maxillofac. Pathol. 25 (3), 411–416. doi:10.4103/jomfp.JOMFP_192_20
Haque, M. F., Meghji, S., Nazir, R., and Harris, M. (2001). Interferon gamma (IFN-γ) may reverse oral submucous fibrosis. J. Oral Pathology and Med. 30 (1), 12–21. doi:10.1034/j.1600-0714.2001.300103.x
Hazzaa, H. H., Elsaadany, B., Abdulhady, E. M., and Ahmed, E. M. (2021). Lycopene versus corticosteroid in the treatment of symptomatic oral lichen planus patients: a randomized double blinded clinical trial. Oral Biol. Craniofacial Res. 6 (4), 6059.
Heber, D., and Lu, Q. Y. (2002). Overview of mechanisms of action of lycopene. Exp. Biol. Med. (Maywood) 227 (10), 920–923. doi:10.1177/153537020222701013
Hegazy, S. K., and El-Bedewy, M. M. (2010). Effect of probiotics on pro-inflammatory cytokines and NF-kappaB activation in ulcerative colitis. World J. Gastroenterol. 16 (33), 4145–4151. doi:10.3748/wjg.v16.i33.4145
Isobe, N., Onodera, H., Mori, A., Shimada, Y., Yang, W., Yasuda, S., et al. (2004). Caspase-3 expression in human gastric carcinoma and its clinical significance. Oncology 66 (3), 201–209. doi:10.1159/000077996
Jain, C. K., Agarwal, S., and Rao, A. V. (1999). The effect of dietary lycopene on bioavailability, tissue distribution, in vivo antioxidant properties and colonic preneoplasia in rats. Nutr. Res. 19 (9), 1383–1391. doi:10.1016/s0271-5317(99)00095-0
Jain, D., and Katti, N. (2015). Combination treatment of lycopene and hesperidin protect experimentally induced ulcer in laboratory rats. J. Intercult. Ethnopharmacol. 4 (2), 143–146. doi:10.5455/jice.20150314061404
Johny, J., Bhagvandas, S. C., Mohan, S. P., Punathil, S., Moyin, S., and Bhaskaran, M. K. (2019). Comparison of efficacy of lycopene and lycopene–hyaluronidase combination in the treatment of oral submucous fibrosis. J. Pharm. Bioallied Sci. 11 (Suppl. 2), S260-S264–4. doi:10.4103/JPBS.JPBS_6_19
Jung, S., Wu, K., Giovannucci, E., Spiegelman, D., Willett, W. C., and Smith-Warner, S. A. (2013). Carotenoid intake and risk of colorectal adenomas in a cohort of male health professionals. Cancer Causes Control 24 (4), 705–717. doi:10.1007/s10552-013-0151-y
Kizhakkoottu, S., and Ramani, P. (2024). Knowledge about the importance of early diagnosis and treatment of oral potentially malignant disorders among the south Indian population: an institutional retrospective study. Cureus 16 (4), e57740. doi:10.7759/cureus.57740
Kopuri, R. K. C., Chakravarthy, C., Sunder, S., Patil, R. S., Shivaraj, W., and Arakeri, G. (2016). A comparative study of the clinical efficacy of lycopene and curcumin in the treatment of oral submucous fibrosis using ultrasonography. J. Int. Oral Health 8 (6), 687–691. doi:10.2047/jioh-08-06-09
K, T., M, C., S, F., and G, L. (2011). Interventions for treating oral lichen planus. Cochrane database Syst. Rev. (7), CD001168. doi:10.1002/14651858.CD001168.pub2
Kumar, A., Bagewadi, A., Keluskar, V., and Singh, M. (2007). Efficacy of lycopene in the management of oral submucous fibrosis. Oral Radiology, Endodontology 103 (2), 207–213. doi:10.1016/j.tripleo.2006.07.011
Kumari, P., Debta, P., and Dixit, A. (2022). Oral potentially malignant disorders: etiology, pathogenesis, and transformation into oral cancer. Front. Pharmacol. 13, 825266. doi:10.3389/fphar.2022.825266
Kushwaha, R. (2017). Comparative study of the efficacy of lycopene versus prednisolone in the management of oral lichen planus- a randomized, double blind clinical trial. World J. Pharm. Pharm. Sci. 6 (5), 1103–1115. doi:10.20959/wjpps20175-9144
Li, Y., Pan, X., Yin, M., Li, C., and Han, L. (2021). Preventive effect of lycopene in dextran sulfate sodium-induced ulcerative colitis mice through the regulation of TLR4/TRIF/NF-κB signaling pathway and tight junctions. J. Agric. Food Chem. 69 (45), 13500–13509. doi:10.1021/acs.jafc.1c05128
Liu, C., Lian, F., Smith, D. E., Russell, R. M., and Wang, X. D. (2003). Lycopene supplementation inhibits lung squamous metaplasia and induces apoptosis via up-regulating insulin-like growth factor-binding protein 3 in cigarette smoke-exposed ferrets. Cancer Res. 63 (12), 3138–3144.
Liu, C., Russell, R. M., and Wang, X. D. (2006). Lycopene supplementation prevents smoke-induced changes in p53, p53 phosphorylation, cell proliferation, and apoptosis in the gastric mucosa of ferrets. J. Nutr. 136 (1), 106–111. doi:10.1093/jn/136.1.106
Liu, D., Ahmet, A., Ward, L., Krishnamoorthy, P., Mandelcorn, E. D., Leigh, R., et al. (2013). A practical guide to the monitoring and management of the complications of systemic corticosteroid therapy. All Asth Clin. Immun. 9 (1), 30. doi:10.1186/1710-1492-9-30
Mirahmadi, M., Azimi-Hashemi, S., Saburi, E., Kamali, H., Pishbin, M., and Hadizadeh, F. (2020). Potential inhibitory effect of lycopene on prostate cancer. Biomed. Pharmacother. 129, 110459. doi:10.1016/j.biopha.2020.110459
Moss, S. F. (1998). Review article: cellular markers in the gastric precancerous process. Aliment. Pharmacol. Ther. 12 (Suppl. 1), 91–109. doi:10.1111/j.1365-2036.1998.00002.x
Nayak, A. (2015). Efficacy of lycopene in combination with vitamin e in management of oral submucous fibrosis - a clinical prospective study. J. Adv. Med. Dent. Sci. Res. 3 (3), 21–25.
Orlando, F. A., Tan, D., Baltodano, J. D., Khoury, T., Gibbs, J. F., Hassid, V. J., et al. (2008). Aberrant crypt foci as precursors in colorectal cancer progression. J. Surg. Oncol. 98 (3), 207–213. doi:10.1002/jso.21106
Patil, S., Khandelwal, S., and Maheshwari, S. (2014). Comparative efficacy of newer antioxidants spirulina and lycopene for the treatment of oral submucous fibrosis. Clin. Cancer Investig. J. 3 (6), 482. doi:10.4103/2278-0513.142618
Patil, S., Sahu, R., Sghaireen, M., Kunsi, S., and Maheshwari, S. (2015). Comparative study of the efficacy of lycopene and aloe vera in the treatment of oral submucous fibrosis. Int. J. Health Allied Sci. 4 (1), 13. doi:10.4103/2278-344x.149216
Peng, Q., Li, H., Chen, J., Wang, Y., and Tang, Z. (2020). Oral submucous fibrosis in Asian countries. J. Oral Pathology and Med. 49 (4), 294–304. doi:10.1111/jop.12924
Piyush, P., Mahajan, A., Singh, K., Ghosh, S., and Gupta, S. (2019). Comparison of therapeutic response of lycopene and curcumin in oral submucous fibrosis: a randomized controlled trial. Oral Dis. 25 (1), 73–79. doi:10.1111/odi.12947
Rao, C. V., Kawamori, T., Hamid, R., and Reddy, B. S. (1999). Chemoprevention of colonic aberrant crypt foci by an inducible nitric oxide synthase-selective inhibitor. Carcinogenesis 20 (4), 641–644. doi:10.1093/carcin/20.4.641
Ross, A. B., Vuong, L. T., Ruckle, J., Synal, H. A., Schulze-König, T., Wertz, K., et al. (2011). Lycopene bioavailability and metabolism in humans: an accelerator mass spectrometry study. Am. J. Clin. Nutr. 93 (6), 1263–1273. doi:10.3945/ajcn.110.008375
Saran, G., Umapathy, D., Misra, N., Channaiah, S., Singh, P., Srivastava, S., et al. (2018). A comparative study to evaluate the efficacy of lycopene and curcumin in oral submucous fibrosis patients: a randomized clinical trial. Indian J. Dent. Res. 29 (3), 303–312. doi:10.4103/ijdr.IJDR_551_16
Sengupta, A., Ghosh, S., Das, R. K., Bhattacharjee, S., and Bhattacharya, S. (2006). Chemopreventive potential of diallylsulfide, lycopene and theaflavin during chemically induced colon carcinogenesis in rat colon through modulation of cyclooxygenase-2 and inducible nitric oxide synthase pathways. Eur. J. Cancer Prev. 15 (4), 301–305. doi:10.1097/00008469-200608000-00005
Sheehan, K. M., Sheahan, K., O’Donoghue, D. P., MacSweeney, F., Conroy, R. M., Fitzgerald, D. J., et al. (1999). The relationship between cyclooxygenase-2 expression and colorectal cancer. JAMA 282 (13), 1254–1257. doi:10.1001/jama.282.13.1254
Singh, D., Shashikanth, M., Misra, N., and Agrawal, S. (2014). Lycopene and intralesional betamethasone injections in the management of oral submucous fibrosis. J. Indian Acad. Oral Med. Radiol. 26 (3), 264. doi:10.4103/0972-1363.145000
Singh, M., and Bagewadi, A. (2017). Comparison of effectiveness of Calendula officinalis extract gel with lycopene gel for treatment of tobacco-induced homogeneous leukoplakia: a randomized clinical trial. Int. J. Pharm. Investig. 7 (2), 88–93. doi:10.4103/jphi.JPHI_19_17
Singh, M., Krishanappa, R., Bagewadi, A., and Keluskar, V. (2004). Efficacy of oral lycopene in the treatment of oral leukoplakia. Oral Oncol. 40 (6), 591–596. doi:10.1016/j.oraloncology.2003.12.011
Subramaniam, A. V., Subramaniam, T., and Agarwal, N. (2014). Assessment of the effectiveness of antioxidant therapy (lycopene) and therapeutic ultrasound in the treatment of oral submucous fibrosis. Int. J. Pharm. and Ther. 5 (5), 344–350.
Sudarshan, R., Annigeri, R. G., and Sree Vijayabala, G. (2012). Aloe vera in the treatment for oral submucous fibrosis - a preliminary study. J. Oral Pathol. Med. 41 (10), 755–761. doi:10.1111/j.1600-0714.2012.01168.x
Sui, J., Guo, J., Pan, D., Wang, Y., Xu, Y., Sun, G., et al. (2024). The efficacy of dietary intake, supplementation, and blood concentrations of carotenoids in cancer prevention: insights from an umbrella meta-analysis. Foods 13 (9), 1321. doi:10.3390/foods13091321
Tan, H. L., Thomas-Ahner, J. M., Grainger, E. M., Wan, L., Francis, D. M., Schwartz, S. J., et al. (2010). Tomato-based food products for prostate cancer prevention: what have we learned? Cancer Metastasis Rev. 29 (3), 553–568. doi:10.1007/s10555-010-9246-z
Tekeli, İ. O., Ateşşahin, A., Sakin, F., Aslan, A., Çeribaşı, S., and Yipel, M. (2019). Protective effects of conventional and colon-targeted lycopene and linalool on ulcerative colitis induced by acetic acid in rats. Inflammopharmacol. 27 (2), 313–322. doi:10.1007/s10787-018-0485-x
Thimmulappa, R. K., Lee, H., Rangasamy, T., Reddy, S. P., Yamamoto, M., Kensler, T. W., et al. (2016). Nrf2 is a critical regulator of the innate immune response and survival during experimental sepsis. J. Clin. Invest 116 (4), 984–995. doi:10.1172/JCI25790
Vrieling, A., Voskuil, D. W., Bonfrer, J. M., Korse, C. M., van Doorn, J., Cats, A., et al. (2007). Lycopene supplementation elevates circulating insulin-like growth factor binding protein-1 and -2 concentrations in persons at greater risk of colorectal cancer. Am. J. Clin. Nutr. 86 (5), 1456–1462. doi:10.1093/ajcn/86.5.1456
Wang, P., Li, P., Chen, Y., Li, L., Lu, Y., Zhou, W., et al. (2022). Chinese integrated guideline on the management of gastric precancerous conditions and lesions. Chin. Med. 17, 138. doi:10.1186/s13020-022-00677-6
Warnakulasuriya, S., and Chen, T. H. H. (2022). Areca nut and oral cancer: evidence from studies conducted in humans. J. Dent. Res. 101 (10), 1139–1146. doi:10.1177/00220345221092751
Warnakulasuriya, S., Kujan, O., Aguirre-Urizar, J. M., Bagan, J. V., González-Moles, M. Á., Kerr, A. R., et al. (2021). Oral potentially malignant disorders: a consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis. 27 (8), 1862–1880. doi:10.1111/odi.13704
Xie, H. L., Su, Q., He, X. S., Liang, X. Q., Zhou, J. G., Song, Y., et al. (2004). Expression of p21WAF1 and p53 and polymorphism of p21WAF1 gene in gastric carcinoma. World J. Gastroenterol. 10 (8), 1125–1131. doi:10.3748/wjg.v10.i8.1125
Yin, Z., Wang, Q., and Cheng, H. (2023). Synergistic protective effect of interactions of quercetin with lycopene against ochratoxin A-induced ulcerative colitis. Appl. Biochem. Biotechnol. 195 (9), 5253–5266. doi:10.1007/s12010-022-04287-8
Zanoni, D. K., Montero, P. H., Migliacci, J. C., Shah, J. P., Wong, R. J., Ganly, I., et al. (2019). Survival outcomes after treatment of cancer of the oral cavity (1985-2015). Oral Oncol. 90, 115–121. doi:10.1016/j.oraloncology.2019.02.001
Zhang, J., Yu, M., Zhang, T., Song, X., Ying, S., Shen, Z., et al. (2024). Deficiency in epithelium RAD50 aggravates UC via IL-6-mediated JAK1/2-STAT3 signaling and promotes development of colitis-associated cancer in mice. J. Crohns Colitis 29, jjae134. doi:10.1093/ecco-jcc/jjae134
Keywords: Lycopene, digestive precancerous lesions, oxidative stress, inflammatory response, chemoprevention
Citation: Gan K, Shi W, Liu X, Ding W, Qiu Y and Luo X (2024) Emerging functions of lycopene in the management of digestive premalignant lesions. Front. Pharmacol. 15:1478170. doi: 10.3389/fphar.2024.1478170
Received: 09 August 2024; Accepted: 07 October 2024;
Published: 17 October 2024.
Edited by:
Nageswaran Sivalingam, RM Institute of Science and Technology, IndiaReviewed by:
Kusmardi Kusmardi, University of Indonesia, IndonesiaArumugam Suriyam Nagappan, University of Madras, India
Copyright © 2024 Gan, Shi, Liu, Ding, Qiu and Luo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaobo Luo, eGlhb2JvbEBzY3UuZWR1LmNu; Yan Qiu, cWl1eWFuMjI3QDEyNi5jb20=
†These authors have contributed equally to this work and share first authorship