 Silvia Fernández-García1,2,3*
Silvia Fernández-García1,2,3* Ana Moragas4,5,6
Ana Moragas4,5,6 Maria Giner-Soriano1,3Rosa Morros1,3,5,7Dan Ouchi1,3Ana García-Sangenís1,5,7
Maria Giner-Soriano1,3Rosa Morros1,3,5,7Dan Ouchi1,3Ana García-Sangenís1,5,7 Carl Llor1,5,8
Carl Llor1,5,8- 1Fundació Institut Universitari per a la recerca a l’Atenció Primària de Salut Jordi Gol i Gurina, Barcelona, Spain
- 2Universitat de Girona, Departament de Ciències Mèdiques, Girona, Spain
- 3Universitat Autònoma de Barcelona, Departament de Farmacologia, de Terapèutica i de Toxicologia, Bellaterra, Spain
- 4Institut Català de la Salut, Center d’Atenció Primària Jaume I, Tarragona, Spain
- 5CIBER en Enfermedades Infecciosas Instituto Carlos III, Madrid, Spain
- 6Universitat Rovira i Virgili, Departament de Medicina i Cirurgia, Reus, Spain
- 7Spanish Clinical Research Network, Clinical Research Unit Fundació Institut Universitari per a la Recerca a l’Atenció Primària de Salut Jordi Gol i Gurina, Barcelona, Spain
- 8Research Unit for General Practice, Department of Public Health, University of Southern Denmark, Odense, Denmark
Introduction: Urinary tract infections (UTIs) are a frequent consultation in primary care and are usually treated with empirical antibiotics. Women suffer more from UTIs than men, and are therefore more likely to be treated with antibiotics. The aim of this study was to describe the epidemiology of UTIs in women in Catalonia, Spain.
Methods: We conducted a population-based observational cohort study that included women patients diagnosed with UTI and recurrent UTI within the SIDIAP and CMBD database during the period from 2012 to 2021. UTI diagnoses were grouped into two main groups, cystitis and pyelonephritis, and patients recorded as having 2 or more episodes of UTI within the year following the first recorded UTI were considered to have recurrent UTI.
Results: The study identified 962,998 women with at least one UTI episode. Cystitis was the most frequently reported infection and was primarily treated with fosfomycin, aligning with local clinical guidelines. Pyelonephritis was typically managed with penicillins. Recurrent UTIs accounted for 3.7% of the sample.
Discussion: This large-scale cohort study provides a comprehensive overview of the epidemiology, management, and treatment of urinary tract infections in women in Catalonia. The findings highlight the widespread use of guideline-recommended antibiotics in the routine clinical management of cystitis, but not of pyelonephritis, and underscore the burden of recurrent infections in a small yet clinically significant subgroup of patients.
Introduction
Urinary tract infections (UTIs) are a common infection in primary healthcare (PHC), and most cases are treated with antibiotics (Malmartel and Ghasarossian, 2016; Tandogdu and Wagenlehner, 2016; Kornfält Isberg et al., 2019). UTIs are more common in women than in men, with almost 60% of women experiencing at least one episode during their lifetime (Foxman, 2002; Fihn, 2003). Factors such as parity, history of abortion, sexual behavior, water intake, and urination habits have been identified as key contributors to the increased risk of UTIs (Mavi et al., 2024). In addition, some women will have recurrent UTIs, which are defined as 2 episodes in 6 months or 3 episodes in a year (Bonkat et al., 2024).
The management of UTIs is based on the prescription of empirical antibiotic treatment. The choice of antimicrobial agent is determined by the most frequently implicated pathogen and local resistance patterns. Currently, the treatment of choice in our setting is a single dose of fosfomycin or 5–7 days of nitrofurantoin for cystitis and 7 days of a cephalosporin for pyelonephritis. In addition, in the treatment of recurrent UTIs, non-pharmacological measures or non-antibiotic drugs are recommended (de Cueto et al., 2017; Almirante Gragera et al., 2021; Bonkat et al., 2024; Martín Zurro et al., 2024).
Several studies have suggested that up to 50% of antibiotic prescriptions are inappropriate (Gharbi et al., 2019; Shallcross et al., 2020), leading to the development of antibiotic resistance. Episodes of uncomplicated UTI are attributed to Escherichia coli in approximately 80% of cases, requiring an antibacterial agent that is effective against this pathogen (Palou et al., 2011; de Cueto et al., 2017; Rodriguez-Mañas, 2020). Resistance of uropathogens to common antibiotics has increased significantly in Spain in recent years (European Centre for Disease Prevention and Control, 2020). Resistance rates of Escherichia coli to fosfomycin and nitrofurantoin remain below 5% in Catalonia, according to current resistance data. However, resistance against amoxicillin and clavulanic acid, and quinolones, currently exceeds 20% of strains (Programa VINCat, 2025). To prevent an increase in antibiotic resistance, it is important to evaluate the empirical antibiotic treatment used in our area in clinical practice, and to assess whether it is in line with the observed resistance rates in order to identify areas for improvement.
The aim of our study was to describe the epidemiology of UTIs, as well as their management and treatment, in women in Catalonia, Spain, over a 10-year period. To achieve this, we analysed different local databases that provide information on clinical practice in PHC. This study is part of the project called “Urinary Tract Infections in Catalonia” (Infeccions del tracte urinari a Catalunya -ITUCAT-), which comprises multiple work packages (Moreno et al., 2023). The main project is registered in the HMA-EMA Catalogues of real-world data sources and studies with the code EUPAS49724 (European Medicines Agency (EMA), 2024).
Materials and methods
This was a population-based observational cohort study. The inclusion period was from 1 January 2012, to 31 December 2021. The study population consisted of all women aged ≥18 years with a diagnosis of UTI registered in SIDIAP with at least 1 year of follow-up during the study period. UTI diagnoses were made according to International Statistical Classification of Diseases and Related Health Problems, 10th Revision, Clinical Modification (ICD-10-CM) codes and were grouped into 2 major groups: cystitis (N30, and N39) and pyelonephritis (N10).
The data needed to carry out the project were obtained from the SIDIAP database, and the Minimum Basic Data Sets ([CMBD] of Hospital Discharges and Emergency Departments) registries (Servei Català de la Salut, 2017).
The SIDIAP contains pseudonymised clinical information from the Electronic Health Records in Primary Care (Estació clínica d’atenció primària) program (Information System for Research in Primary Care, 2022), which is the electronic health record program for PHC of the Catalan Health Institute (Institut Català de la Salut [ICS]) in Catalonia. The ICS manages 328 PHC centres, covering a population of 5.8 million people (approximately 80% of the Catalan population) (Recalde et al., 2022). Information is available for more than 3,384 health professionals who care for the adult population.
The data recorded in SIDIAP contains sociodemographic data; health conditions, coded by ICD-10-CM (World Health Organization, 2016); clinical parameters; tobacco and alcohol use; diagnostic procedures; PHC laboratory test results; specialists referrals; and prescriptions of PHC medical staff, with the corresponding pharmacy invoice data, registered as anatomical, therapeutic, chemical (ATC) classification system codes (World Health Organization, 2024). Several reports have shown that SIDIAP data are useful for epidemiological research (Bolíbar et al., 2012; Recalde et al., 2022). SIDIAP is listed in the HMA-EMA Catalogues of real-world data sources and studies (European Medicines Agency (EMA), 2024).
The CMBD is a population-based registry that collects information on conditions treated in the health centers of Catalonia (Servei Català de la Salut, 2017) and includes ICD-10-CM codes (World Health Organization, 2016). This registry contains information provided by all Catalan healthcare centres on healthcare activity and morbidity. The CMBD of Hospital Discharges contains information on acute hospitalizations, with reasons and dates for hospital admission, while the CMBD of Emergency Departments reports activity in emergency departments.
Study variables
The study variables included were sociodemographic information, including the MEDEA index (a socioeconomic deprivation score including five discrete values); clinical variables and health conditions, with ICD-10-CM codes (Supplementary Material S1; Table 1); tobacco and alcohol consumption; PHC laboratory test requests and results; prescriptions, with their corresponding pharmacy invoice data registered as ATC codes; CMBD-HA hospital information and CMBD-UR emergency department referral information.
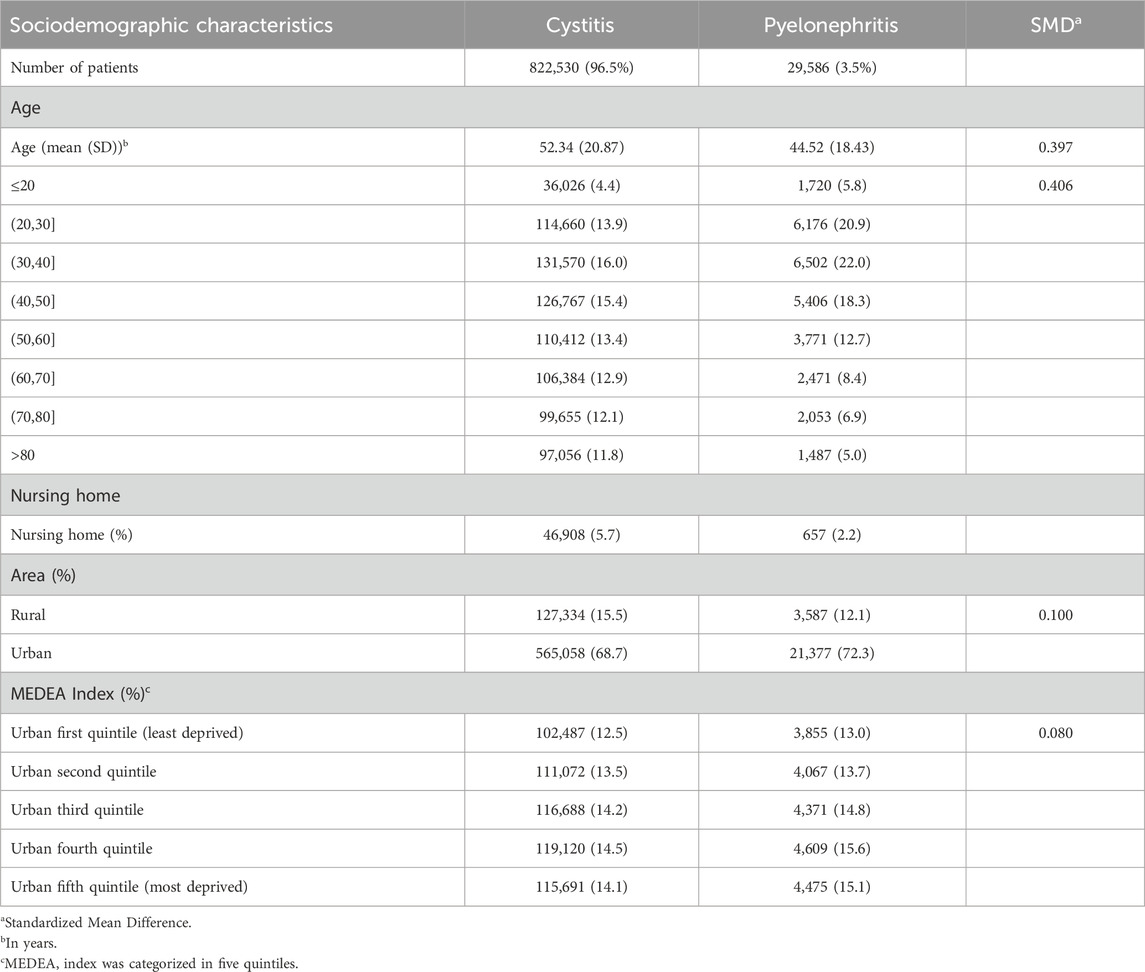
Table 1. Sociodemographic characteristics of patients diagnosed with UTI.
For this study, an episode of UTI was defined as the date of the first diagnosis of UTI within a 14 days interval, regardless of the number of diagnoses recorded during this interval. Outside this interval, a new record of a diagnosis of UTI was considered a new episode of UTI. Furthermore, in order to define the parameters for antibiotic treatment, the request for PHC laboratory tests, referrals to specialized care, or the presence of a urinary catheter were deemed part of the same period of the UTI if they had been registered the 15 days preceding the index date of the UTI and up to 1 month thereafter. For the comparison study between recurrent and non-recurrent infections, recurrent UTI was defined as a patient having 2 or more episodes of UTI in 1 year of follow-up since data index.
To describe antibiotic therapies, a categorization based on ATC groups was perfomed and some modifications were made (Supplementary Material S1; Table 2). For the beta-lactam antibacterial agents, penicillins and other beta-lactam antibacterial agents have been differentiated. Likewise, within the ATC category encompassing macrolides, lincosamides, and streptogramins, only macrolides were considered. Fosfomycin and nitrofurantoin have also been described as a group. ATC groups not shown in Table 4 were included under the ‘other antibiotics’ group. Antibiotic treatment for recurrent UTIs was also described by ATC, with the exception of nitrofurantoin, fosfomycin and trimetropim (guideline-recommended prophylactic antibiotics), which were given continuously during the period of 1 year after the data index, differentiating into two broad groups (less than 3 months, and more than 3 months).
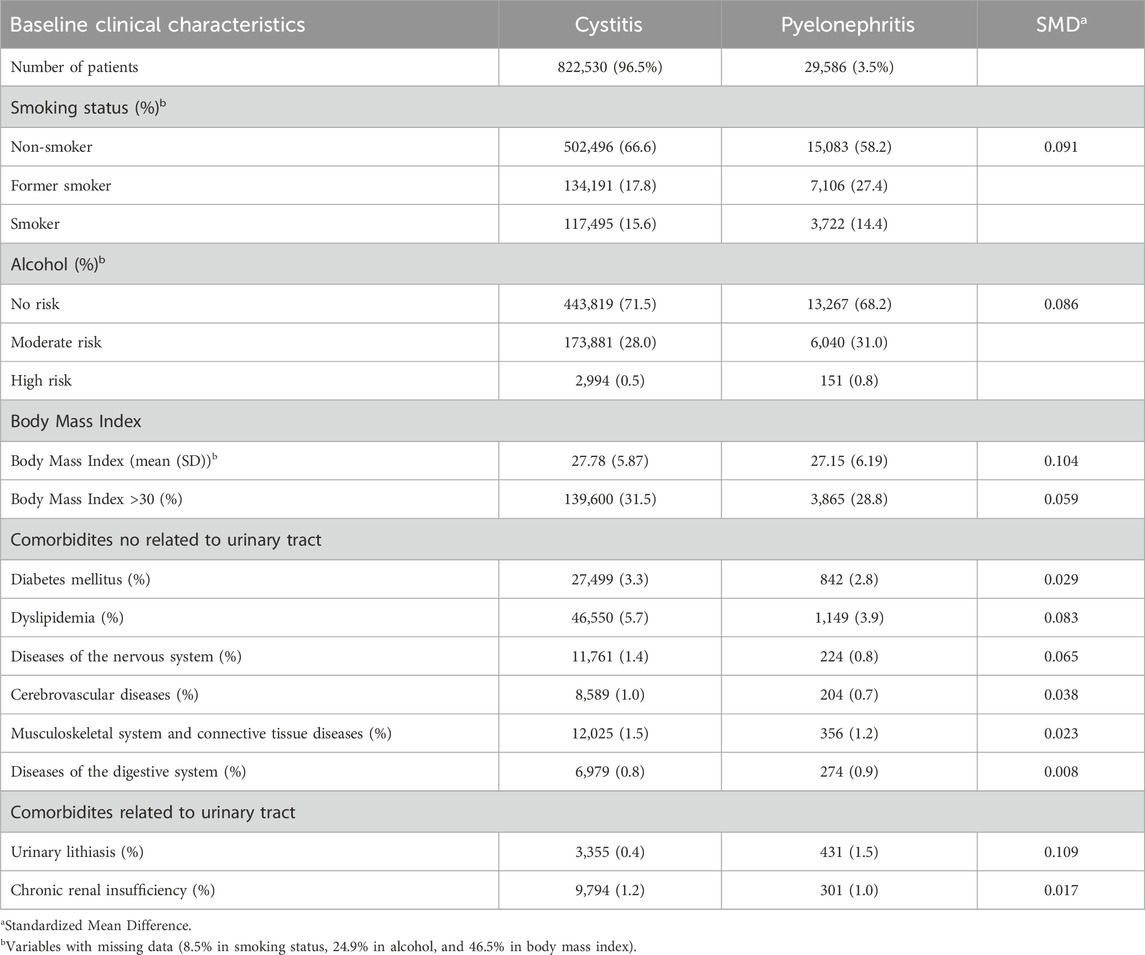
Table 2. Baseline clinical characteristics of patients diagnosed with UTI.
Statistical analysis
The index date was defined as the onset of each UTI episode, from which we retrospectively captured patient demographics, clinical characteristics, medication use, comorbidities, specialist referrals, and laboratory data using standardized data capture protocols with explicit handling of missing data. Specific temporal criteria were applied to each data element: active diagnoses, active medications, while BMI and laboratory values used the most recent measurement within a specific day window surrounding the index date. Our primary analysis included all women with ≥1 UTI episode during the study period, with descriptive statistics presented overall and stratified by UTI diagnosis type. Categorical variables were summarized as frequencies and percentages, with continuous variables reported as either mean (standard deviation) or median (interquartile range) based on distributional characteristics. Between-group balance was assessed using standardized mean differences (SMD), where we considered SMD values ≤0.1 to indicate adequate balance. The distribution of antibiotic treatments among patient groups was ordered by frequency and by single or combination treatments.
Results
Out of 2,396,441 women included in the databases between 2012 and 2021, 962,998 had a record of at least one episode of UTI. After excluding women who did not meet the inclusion criteria (Figure 1), the final sample consisted of 852,116 women.
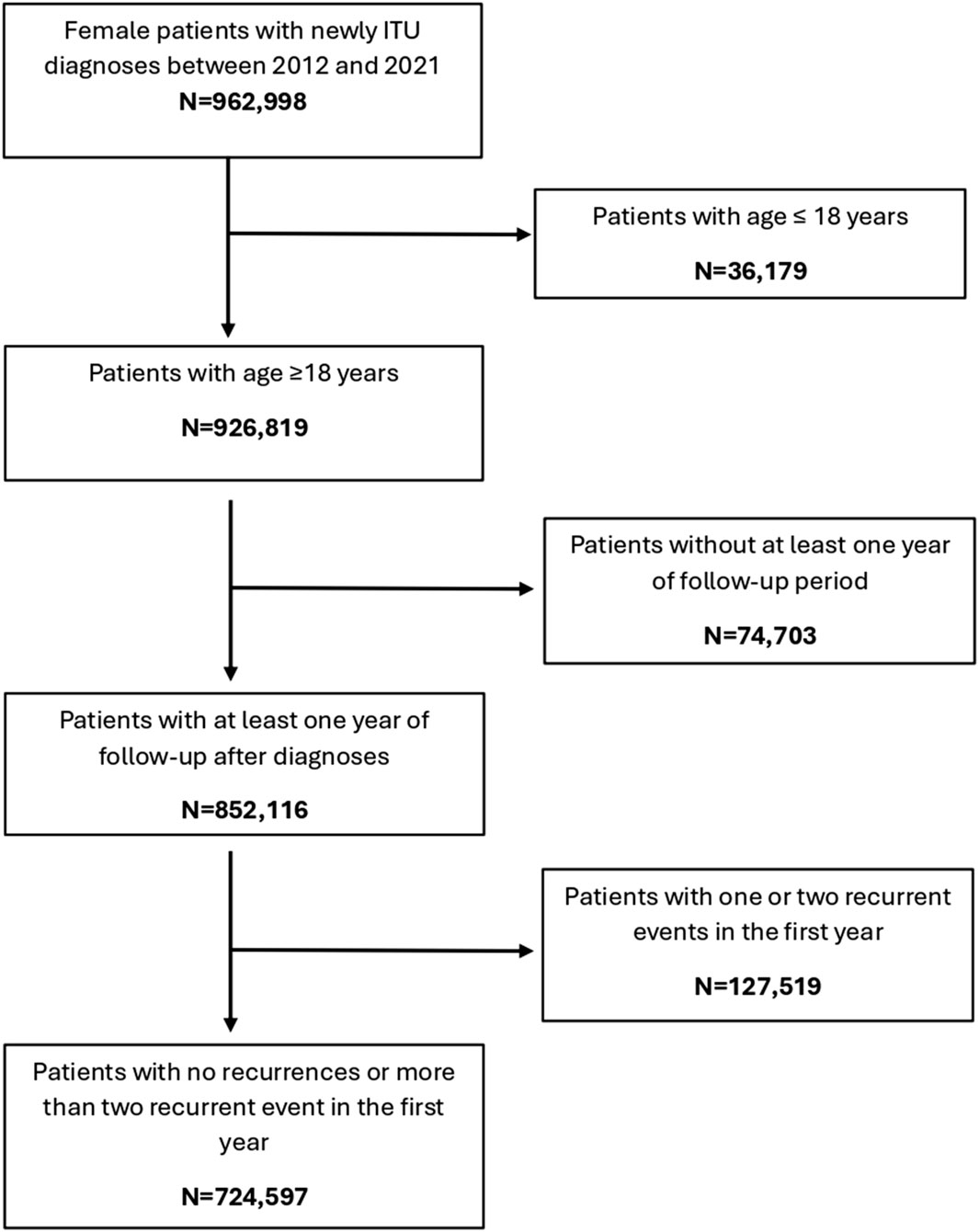
Figure 1. Flowchart of participants in cohort study.
The mean age of women with UTIs was 52 years for those diagnosed with cystitis and 45 years for those diagnosed with pyelonephritis. The highest number in both groups was observed in the 30–40 years age group and decreased with age. No differences were found across the MEDEA Index (Table 1).
Regarding lifestyle factors and comorbidities, non-smokers and non-risk alcohol consumption were found in the majority of patients. It was also observed that about 30% of the patients had a BMI above 30 (Table 2), taking into account the missing data. With regard to non-urinary tract comorbidities, dyslipidemia was the most common, followed by diabetes mellitus. In contrast, urinary tract comorbidities were relatively uncommon (less than 1.5%).
In our setting, the median follow-up from the first episode was 6 years. During this follow-up, about half of the women with UTI had at least one further event. However, when follow-up was limited to the first year after the first event, this percentage of women was reduced by more than half. In both situations, the most common event recorded during this period was a further UTI episode.
Antibiotic treatment was recorded in 82.2% and 61.2% of cases of cystitis and pyelonephritis respectively in the first episode (Table 3). The majority of women were prescribed only one course of antibiotic; fewer than 20% of patients prescribed two or more. About 30% of patients had a urine culture and a small percentage had a record of urinary catheterisation. Although hospital referral rates were low overall, referrals for pyelonephritis were higher than those for cystitis.
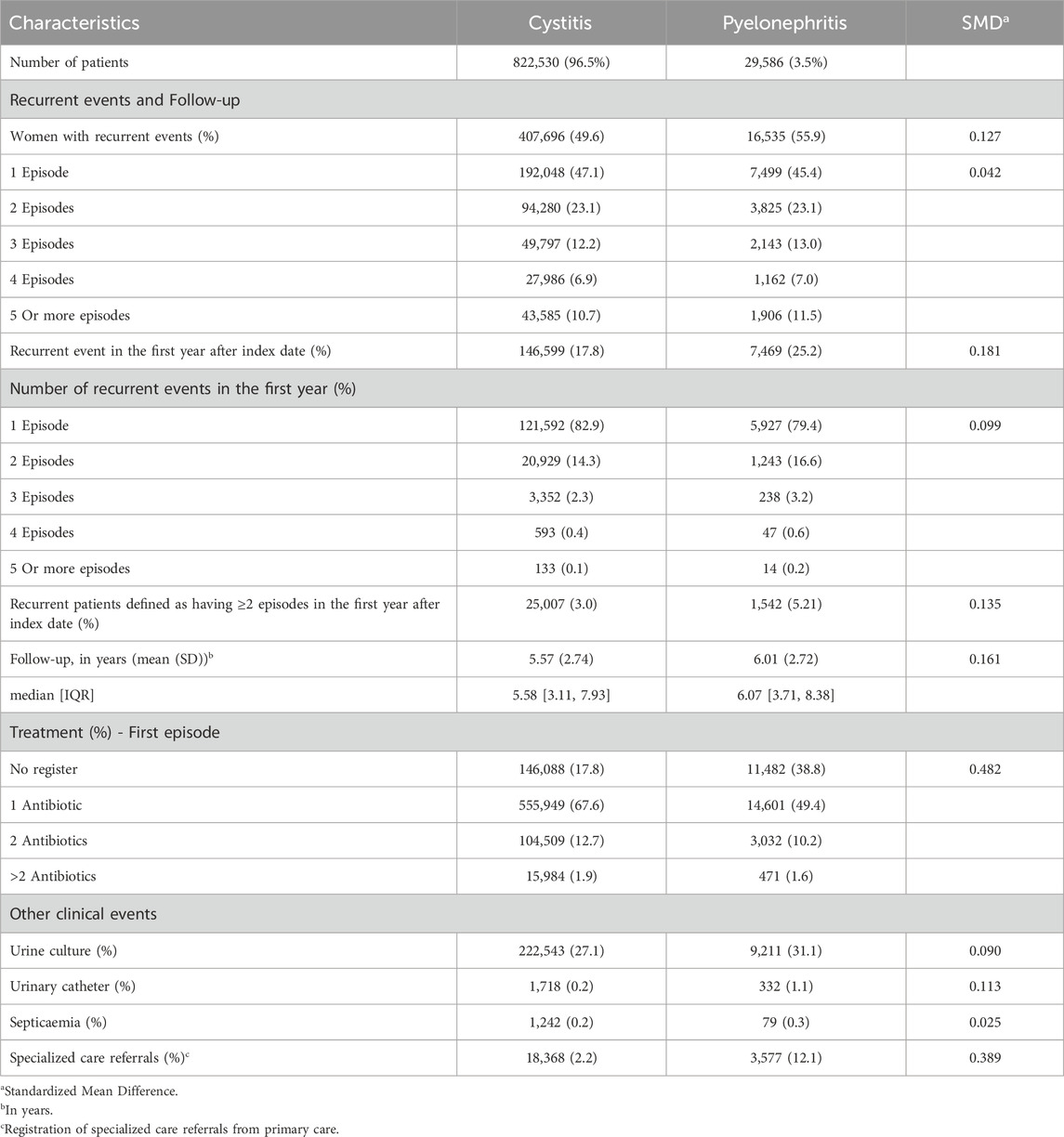
Table 3. Characteristics of UTI episode.
The most prescribed antibiotic treatment in the cystitis group was fosfomycin, followed by treatment with quinolones. In contrast, in the pyelonephritis group, penicillins were the most frequently recorded treatment, followed by treatment with the other beta-lactam antibiotic group. 98.7% of the first-line antibiotics for uncomplicated UTI corresponded to fosfomycin. Table 4; Figures 2–4 describe the antibiotic treatments, including the most frequent drugs of the study.
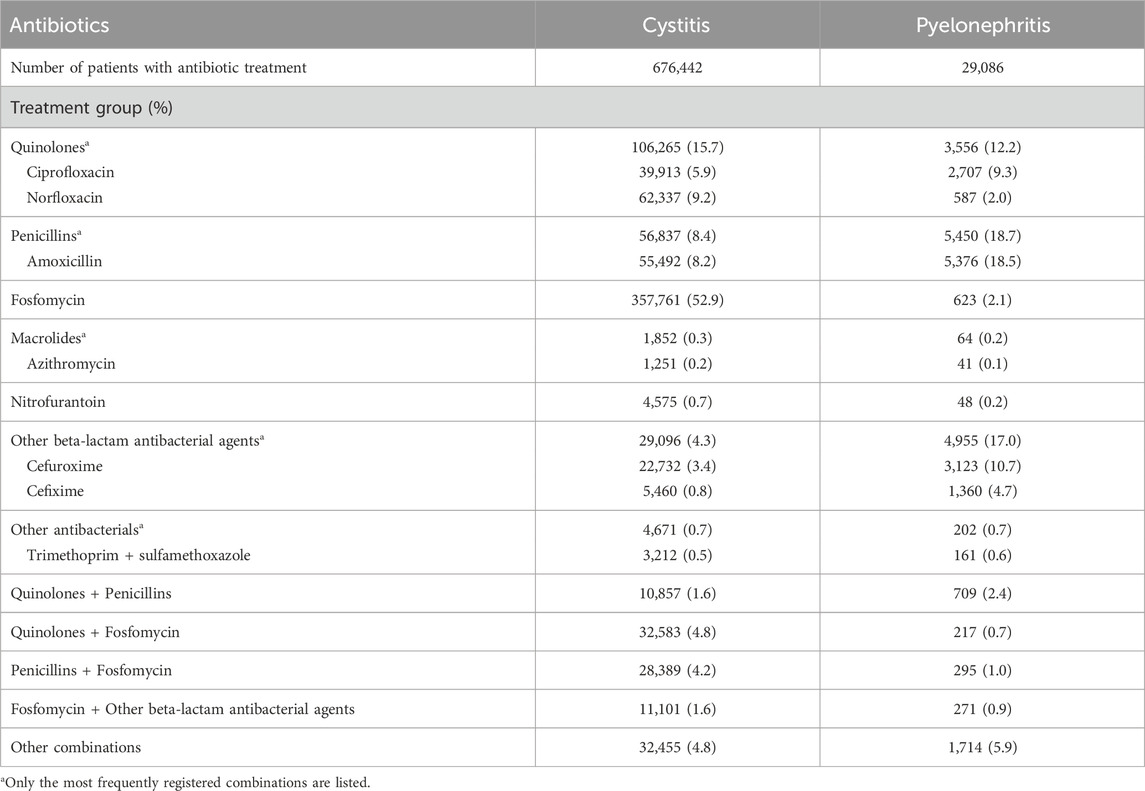
Table 4. Antibiotic treatment of UTI.
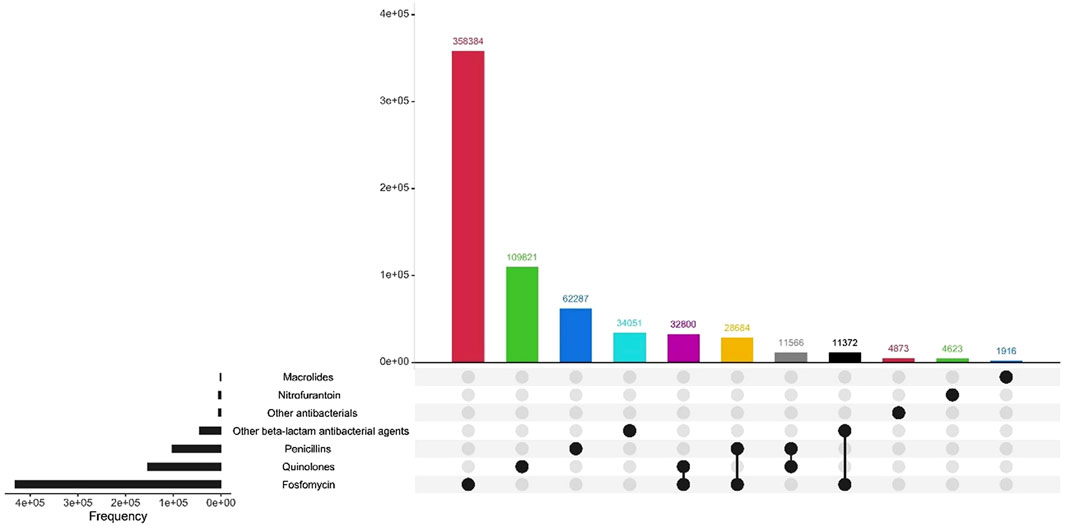
Figure 2. Antibiotic treatment of patients diagnosed with UTI, by treatment group.
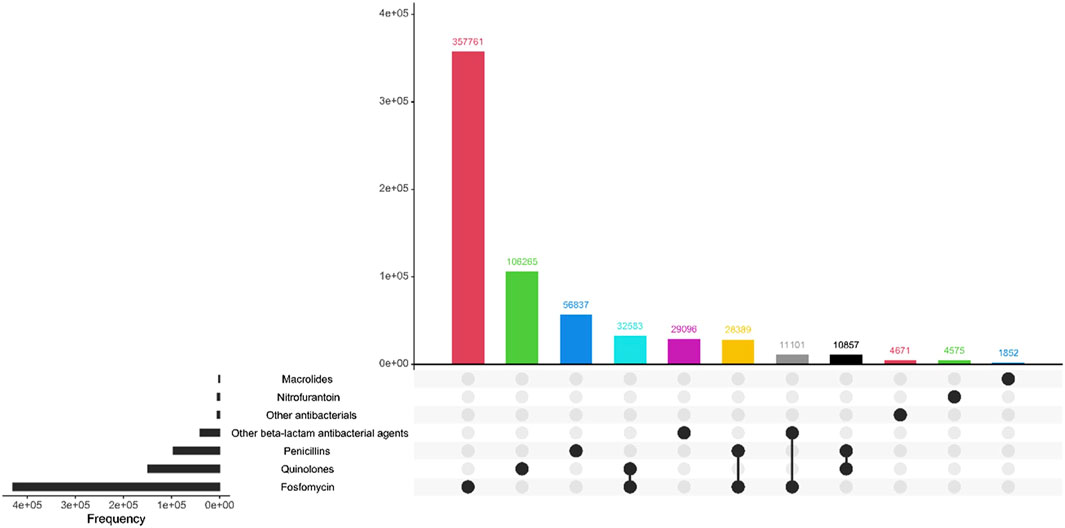
Figure 3. Antibiotic treatment of patients diagnosed with cystitis, by treatment group.
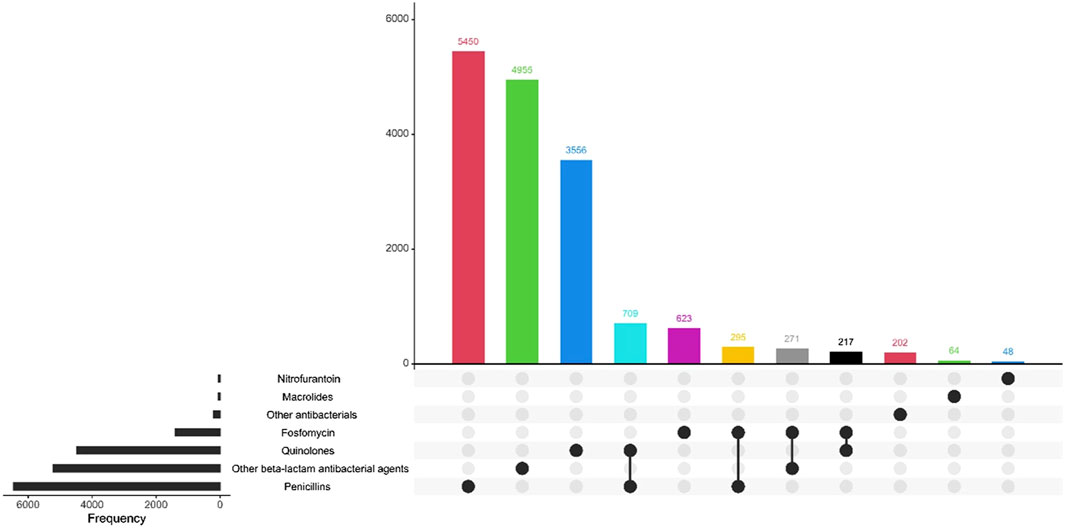
Figure 4. Antibiotic treatment of patients diagnosed with pyelonephritis, by treatment group.
Women who suffered from recurrent UTIs were older, and were more likely to be residents of nursing homes, as well as being more likely to report diabetes mellitus and dyslipidemia (Table 5). In terms of antibiotic dispensing, patients with recurrent UTIs have more antibiotics dispensed (in 3 or more dispensations) than patients with no record of recurrent UTI (Table 6). Fosfomycin was the most commonly reported treatment for recurrent UTI, reaching almost 70%, followed by quinolones, and penicillins.
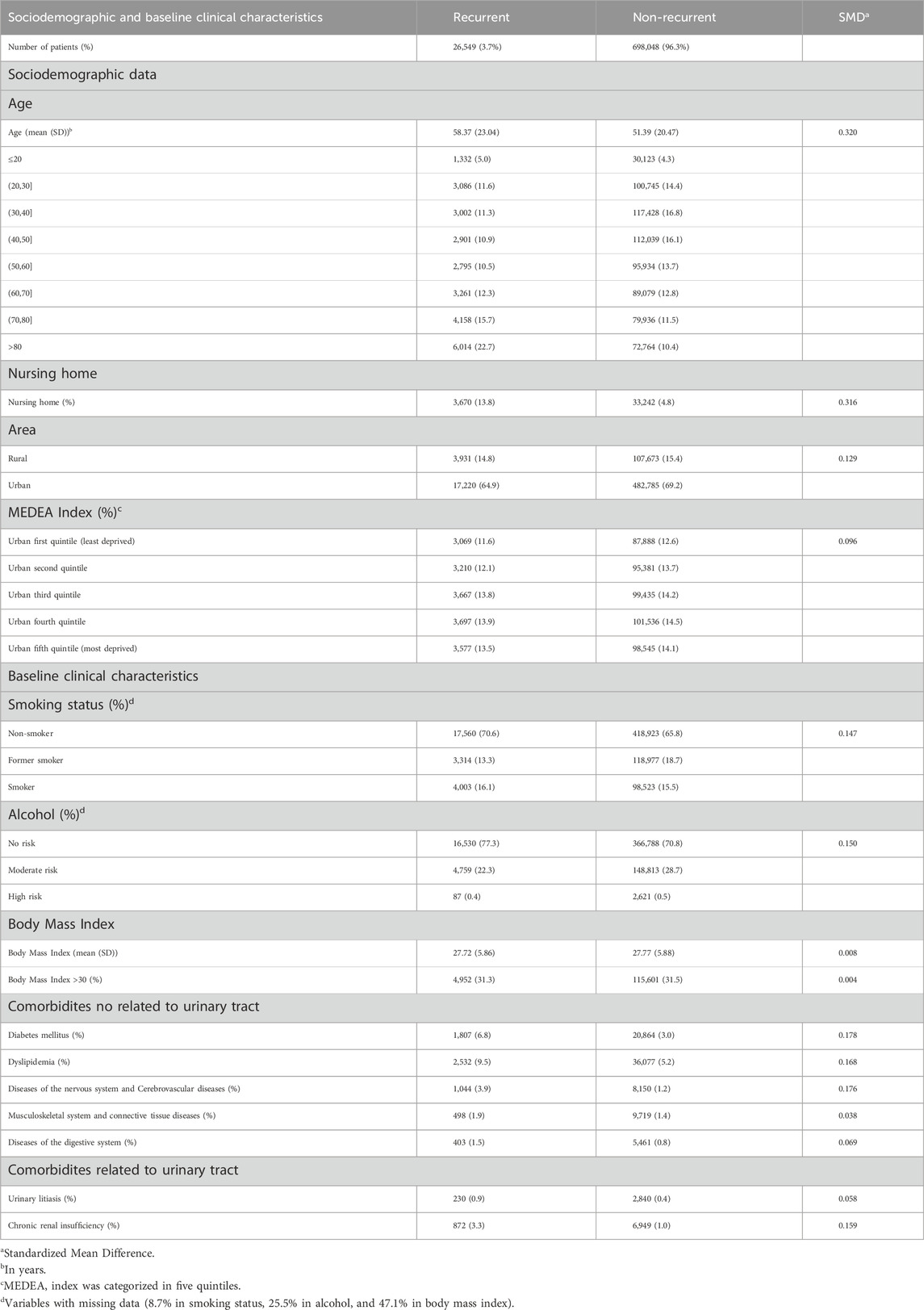
Table 5. Sociodemographic and baseline clinical characteristics of patients diagnosed with recurrent UTI and no recurrent UTI.
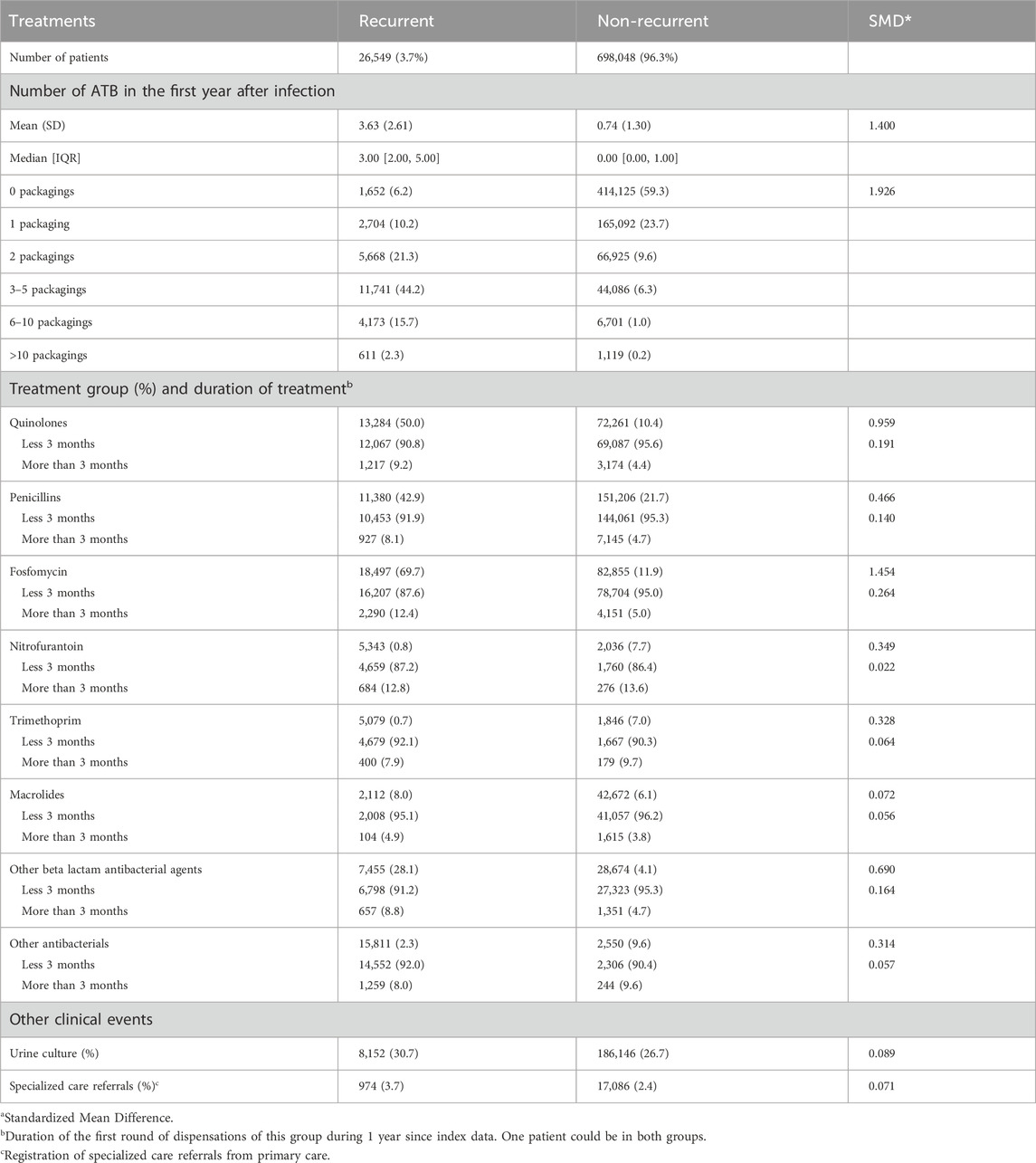
Table 6. Treatment of recurrente UTIs and non-recurrent UTIs.
Discussion
The study aimed to characterise UTIs over a 10-year period in Catalonia using the population-based database, describing the socio-demographic and clinical characteristics, as well as the management of the disease.
Regarding the age at which UTI was recorded in our database, it was similar for cystitis in other populations such as Switzerland (Plate et al., 2019), the Netherlands (Spek et al., 2020), and China (Wong et al., 2017) with ages ranging from 53 to 54 years. However, this was not the case for pyelonephritis, which in our setting was between 30 and 40 years of age, unlike other European country where younger ages were recorded (Isberg et al., 2019).
Diabetes is considered a risk factor for UTI (Bonkat et al., 2024), but it was not the first comorbidity recorded in our study. Nevertheless, the percentage of diabetes mellitus was similar to other countries, such as Sweden with 3.6% (Kornfält Isberg et al., 2019) but not in China, where it is higher (16.4%) (Wong et al., 2017). More women were diagnosed with dyslipidemia, although this is not considered a risk factor.
It should be noted that 17.8% of cystitis and 38.8% of pyelonephritis had no record of antibiotic treatment in the database, which is similar to other studies using databases (Isberg et al., 2019; Kornfält Isberg et al., 2021). However, studies with lower percentages around 7.6% can be found in the literature (Plate et al., 2020). This lack of record could be explained by the use of data from medical records, one of the limitations of observational studies. The percentage of antibiotic treatment recorded in our study was similar to other European studies conducted in Sweden (Kornfält Isberg et al., 2019; Kornfält Isberg et al., 2021), Germany (Gágyor et al., 2020); and Hong Kong (Wong et al., 2017). In the case of pyelonephritis, one of the possible reasons for the higher number of antibiotic non-registrations is referral to a hospital centre as a complicated UTI, as in-hospital antibiotic treatment was not available in our database.
In our setting, cystitis was most commonly treated with fosfomycin, in line with treatment guidelines, whereas pyelonephritis was treated with penicillins as a family of antibacterials. In a study published in 2017 involving a Spanish cohort, fosfomycin was already the most commonly prescribed antibiotic (used in almost 80% of cases), although the overall rate of antibiotic prescriptions related to UTI was higher (95.1%) (Butler et al., 2017).
One of the most significant findings of our study is the high percentage of fosfomycin used among Catalan prescribers. Two antibiotics are recommended by our national guidelines based on their proven efficacy, low rates of resistance, limited ecologial impact, and low propensity to select for resistance (Frimodt-Møller and Bjerrum, 2023; Llor et al., 2023; Bonkat et al., 2024), and our data suggest that healthcare professionals are adhering to these recommendations. Both antibiotics exhibit strong activity against E. coli and are considered first-line treatments in many countries due to their narrow spectrum and favorable safety profiles. However, the use of fosfomycin accounts for more than 98% of the prescriptions for these two recommended antibiotics, while nitrofurantoin is seldom used in our area. This limited use may be attributed to a warning issued in 2016 by the Spanish Agency of Drugs and Medicinal Products, advising against the use of nitrofurantoin for durations longer than 7 days (Martínez-Macías et al., 2018; Almirante Gragera et al., 2021). The use of these antibiotics for uncomplicated UTIs is also recommended in other European countries; however, prescribing patterns are more balanced elsewhere. In some countries, for example, nitrofurantoin is the most used antibiotic remaining the most prescribed agent in the Netherlands and parts of Scandinavia, while fosfomycin is favoured in countries like Germany (Malmros et al., 2019). Interestingly, a systematic review and meta-analysis evaluating the comparative efficacy and safety of fosfomycin and nitrofurantoin in the management of uncomplicated UTIs found a higher incidence of adverse events in the fosfomycin group compared to the nitrofurantoin group (Konwar et al., 2022). Nevertheless, nitrofurantoin is rarely prescribed locally, possibly because regional guidelines recommend it only as an alternative to fosfomycin (Almirante Gragera et al., 2021).
Urine culture was requested for approximately 30% of UTIs, which is in line with other European and Asian countries that report around 30%–40% (Plate et al., 2019; Koh et al., 2023). Due to the nature of the project, the reasons for the request were not available. It should be noted that a descriptive study of the adequacy of urine cultures in our setting has been carried out in one of the work packages of the ITUCAT project. It showed that the percentage of over-requesting urine cultures remains high, with one-fifth of cultures ordered for uncomplicated UTIs (Fernández-García et al., 2025). In addition, a very low percentage of sepsis was recorded, as in a study with database in England, with 0.5% sepsis registered (Gharbi et al., 2019).
In our study, 3.7% of the population reported recurrent UTI. This percentage is similar in different populations, ranging from 2.7% in an English population-based study to 6% in the Welsh population (Ahmed et al., 2019; Sanyaolu et al., 2024) although there are studies with higher percentages, such as a prospective study in Switzerland (Kornfält Isberg et al., 2021) or a study of women in the United States in which 30% of the women surveyed had recurrent UTIs (Gleicher et al., 2023).
The sociodemographic characteristics for recurrent UTIs are similar to other studies in the literature (Samimi et al., 2021; ten Doesschate et al., 2022; Gleicher et al., 2023; Sanyaolu et al., 2024), although the diagnosis of diabetes was reported at higher rates in the literature, reaching 22.1% (Sanyaolu et al., 2024). In studies conducted in Spain, a higher percentage of diagnosed diabetes mellitus and urolithiasis (Lorenzo-Gómez et al., 2015; Carrión-López et al., 2020) was observed than in our database.
Fosfomycin was the most frequently reported antibiotic treatment for recurrent UTIs during the yearly follow-up from the index date, with the lowest frequency in the 3-month period. This antibiotic is one of those used for prophylactic treatment according to clinical guidelines (Patología infecciosa en: Grupo de Trabajo de Enfermedades Infecciosas de la semFYC, 2017; Almirante Gragera et al., 2021; Bonkat et al., 2024). Furthermore, non-antibiotic measures for UTI prophylaxis are not included in the database, although there are several studies in the literature evaluating non-antibiotic treatments (Rui et al., 2022; Hayward et al., 2024; Heltveit-Olsen et al., 2024) to reduce antibiotic overuse and help prevent antimicrobial resistance.
One of the strengths of our study is the large sample size, which allowed us to obtain information from a large proportion of the female population in Catalonia. In addition, the information obtained corresponds to clinical practice in our primary care setting over a period of 10 years, which can be useful for observing the antibiotic stewardship in PHC, as shown in other studies in Europe (Mulder et al., 2019). Understanding how UTIs are treated enables us to determine whether clinical guidelines are being adhered to, ensure that patients are receiving appropriate treatment, and identify areas for improvement in disease management, if necessary, to help prevent antimicrobial resistance. On the other hand, the limitations of our study are those inherent to observational studies using data from electronic health records. Most importantly, causality cannot be established, and there may be bias due to confounding variables and inaccuracies in the records in the health registers. For instance, we acknowledge the potential for selection biases - patients with missing data may represent a healthier population–as well as possible errors arising from incomplete or inaccurate diagnostic records. Another limitation of the study is that our data focused on public primary care settings, so we do not have information from hospitals or private practices.
Our study provides information about the treatment and management of UTI in the women population in our setting, and this information is both important and useful for future research, such as the integration of hospital-based data, assessment of patient adherence to prescribed treatments, and evaluation of the long-term outcomes associated with various management strategies.
Conclusion
We conducted a large-scale study of UTI in women in primary care. Almost the entire female population of Catalonia was included, allowing the description of women with a diagnosis of UTI and obtaining information of great importance for evaluating the management of UTI in our setting.
The sociodemographic characteristics are similar to other studies, both for UTIs and recurrent UTIs. In our study, the use of fosfomycin for the treatment of cystitis is the most commonly reported, in line with local guidelines. In contrast, antibiotic treatment for pyelonephritis does not follow local recommendations according to data from our study, which is based on primary care data. Evaluating the management and treatment of this infection helps us identify areas for improvement in primary care, with the aim of enhancing patient care and preventing antibiotic resistance.
Data availability statement
The datasets generated and/or analyzed during the current study are not publicly available due to patient privacy and data protection concerns, but they are available from the corresponding author on reasonable request.
Ethics statement
The studies involving humans were approved by the Ethics Committee of IDIAP Jordi Gol with ethical approval code 22/089-P (protocol code IJG-ITUCAT-2022 and date of approval: 27/07/2022). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participant’s; legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
SF-G: Investigation, Project administration, Resources, Validation, Visualization, Funding acquisition, Writing – review and editing, Writing – original draft. AM: Conceptualization, Methodology, Supervision, Funding acquisition, Writing – review and editing, Writing – original draft. MG-S: Investigation, Resources, Validation, Visualization, Funding acquisition, Writing – review and editing, Writing – original draft. RM: Conceptualization, Investigation, Methodology, Supervision, Validation, Visualization, Writing – review and editing, Writing – original draft. DO: Data curation, Formal analysis, Investigation, Resources, Software, Validation, Visualization, Funding acquisition, Writing – review and editing, Writing – original draft. AG-S: Project administration, Visualization, Funding acquisition, Writing – review and editing, Writing – original draft. CL: Conceptualization, Methodology, Supervision, Funding acquisition, Writing – review and editing, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by Strategic Research and Innovation Plan for Health, Department of Health (Pla Estratègic de Recerca i Innovació en Salut, Departament de Salut) 2022–2024 grant for the financing of research projects in the field of primary health care, grant number SLT021/21/000022.
Acknowledgments
The authors are grateful to all the sanitary professionals who work at the Institut Català de la Salut, and SIDIAP team for their work in maintaining the database and for their help in carrying out the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2025.1593910/full#supplementary-material.
Abbreviations
ATC, Anatomical, therapeutic, chemical classification system; CMBD, Minimum Basic Data Sets; ICD, International Statistical Classification of Diseases; ICS, Institut Català de la Salut; SIDIAP, Information system for the development of research in Primary Care; UTIs, Urinary tract infections.
References
Ahmed, H., Farewell, D., Jones, H. M., Francis, N. A., Paranjothy, S., and Butler, C. C. (2019). Antibiotic prophylaxis and clinical outcomes among older adults with recurrent urinary tract infection: cohort study. Age Ageing 48, 228–234. doi:10.1093/ageing/afy146
Almirante Gragera, B., Álvarez Martins, M., Ardanuy Tisaire, C., Bonet Monné, S., Canadell Vilarrasa, L., Cano Marron, M., et al. (2021). Programa d’optimització d’antibiòtics: infeccions del tracte urinari en adults. Available online at: https://scientiasalut.gencat.cat/handle/11351/6470 (Accessed September 26, 2024).
Bolíbar, B., Fina Avilés, F., Morros, R., Del Mar Garcia-Gil, M., Hermosilla, E., Ramos, R., et al. (2012). Base de datos SIDIAP: La historia clínica informatizada de Atención Primaria como fuente de información para la investigación epidemiológica. Med. Clin. Barc. 138, 617–621. doi:10.1016/j.medcli.2012.01.020
Bonkat, G., Bartoletti, R., Bruyère, F., Cai, T., Geerlings, S. E., Köves, B., et al. (2024). Urological infections EAU guidelines on. Available online at: http://uroweb.org/guidelines/compilations-of-all-guidelines/ (Accessed June 26, 2025).
Butler, C. C., Francis, N., Thomas-Jones, E., Llor, C., Bongard, E., Moore, M., et al. (2017). Variations in presentation, management, and patient outcomes of urinary tract infection: a prospective four-country primary care observational cohort study. Br. J. General Pract. 67, e830–e841. doi:10.3399/bjgp17X693641
Carrión-López, P., Martínez-Ruiz, J., Librán-García, L., Giménez-Bachs, J. M., Pastor-Navarro, H., and Salinas-Sánchez, A. S. (2020). Analysis of the efficacy of a sublingual bacterial vaccine in the prophylaxis of recurrent urinary tract infection. Urol. Int. 104, 293–300. doi:10.1159/000505162
de Cueto, M., Aliaga, L., Alós, J. I., Canut, A., Los-Arcos, I., Martínez, J. A., et al. (2017). Executive summary of the diagnosis and treatment of urinary tract infection: guidelines of the Spanish society of clinical microbiology and infectious diseases (SEIMC). Enferm. Infecc. Microbiol. Clin. 35, 314–320. doi:10.1016/j.eimc.2016.11.005
European Centre for Disease Prevention and Control (2020). Antimicrobial resistance in the Eu/EEA (EARS-Net) - annual epidemiological report 2020. Available online at: https://www.ecdc.europa.eu/en/publications-data/antimicrobial-resistance-eueea-ears-net-annual-epidemiological-report-2020 (Accessed October 7, 2024).
European Medicines Agency (EMA) (2024). HMA - EMA catalogues of real-world data sources and studies. Available online at: https://catalogues.ema.europa.eu/catalogue-rwd-studies (Accessed March 14, 2025).
Fernández-García, S., Monfà, R., Jiménez, C. M., Giner-Soriano, M., Gómez, F., and Moragas, A. (2025). Appropriateness of urine culture requests in primary care in Spain: a cross-sectional descriptive study. Aten. Primaria 57, 103208. doi:10.1016/j.aprim.2024.103208
Fihn, S. D. (2003). Clinical practice. Acute uncomplicated urinary tract infection in women. N. Engl. J. Med. 349, 259–266. doi:10.1056/NEJMcp030027
Foxman, B. (2002). Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Am. J. Med. 113, 5–13. doi:10.1016/s0002-9343(02)01054-9
Frimodt-Møller, N., and Bjerrum, L. (2023). Treating urinary tract infections in the era of antibiotic resistance. Expert Rev. Anti Infect. Ther. 21, 1301–1308. doi:10.1080/14787210.2023.2279104
Gágyor, I., Strube-Plaschke, S., Rentzsch, K., and Himmel, W. (2020). Management of urinary tract infections: what do doctors recommend and patients do? An observational study in German primary care. BMC Infect. Dis. 20, 813. doi:10.1186/s12879-020-05377-w
Gharbi, M., Drysdale, J. H., Lishman, H., Goudie, R., Molokhia, M., Johnson, A. P., et al. (2019). Antibiotic management of urinary tract infection in elderly patients in primary care and its association with bloodstream infections and all cause mortality: population based cohort study. BMJ (Online) 364, l525. doi:10.1136/bmj.l525
Gleicher, S., Sebesta, E. M., Kaufman, M. R., Dmochowski, R. R., and Reynolds, W. S. (2023). Recurrent urinary tract infection management and prevention techniques among a population-based cohort of women. Neurourol. Urodyn. 42, 1676–1685. doi:10.1002/nau.25281
Hayward, G., Mort, S., Hay, A. D., Moore, M., Thomas, N. P. B., Cook, J., et al. (2024). D-Mannose for prevention of recurrent urinary tract infection among women: a randomized clinical trial. JAMA Intern Med. 184, 619–628. doi:10.1001/jamainternmed.2024.0264
Heltveit-Olsen, S. R., Gopinathan, U., Blix, H. S., Elstrøm, P., and Høye, S. (2024). Effect of methenamine hippurate shortage on antibiotic prescribing for urinary tract infections in Norway - an interrupted time series analysis. J. Antimicrob. Chemother. 79, 1109–1117. doi:10.1093/jac/dkae078
Information System for Research in Primary Care (2022). Information system for research in primary care. Available online at: https://www.sidiap.org/index.php/en/(Accessed March 14, 2025).
Isberg, H. K., Hedin, K., Melander, E., Mölstad, S., and Beckman, A. (2019). Increased adherence to treatment guidelines in patients with urinary tract infection in primary care: a retrospective study. PLoS One 14, e0214572. doi:10.1371/journal.pone.0214572
Koh, S. W. C., Ng, T. S. M., Loh, V. W. K., Goh, J. C., Low, S. H., Tan, W. Z., et al. (2023). Antibiotic treatment failure of uncomplicated urinary tract infections in primary care. Antimicrob. Resist Infect. Control 12, 73. doi:10.1186/s13756-023-01282-4
Konwar, M., Gogtay, N. J., Ravi, R., Thatte, U. M., and Bose, D. (2022). Evaluation of efficacy and safety of fosfomycin versus nitrofurantoin for the treatment of uncomplicated lower urinary tract infection (UTI) in women–A systematic review and meta-analysis. J. Chemother. 34, 139–148. doi:10.1080/1120009X.2021.1938949
Kornfält Isberg, H., Hedin, K., Melander, E., Mölstad, S., and Beckman, A. (2021). Uncomplicated urinary tract infection in primary health care: presentation and clinical outcome. Infect. Dis. 53, 94–101. doi:10.1080/23744235.2020.1834138
Kornfält Isberg, H., Melander, E., Hedin, K., Mölstad, S., and Beckman, A. (2019). Uncomplicated urinary tract infections in Swedish primary care; etiology, resistance and treatment. BMC Infect. Dis. 19, 155. doi:10.1186/s12879-019-3785-x
Llor, C., Hoyos Mallecot, Y., Moragas, A., Troncoso-Mariño, A., Bjerrum, L., and Villmones, H. C. (2023). New paradigms on antibiotic recommendations for community-acquired infections in Spain. Aten. Primaria 55, 102648. doi:10.1016/j.aprim.2023.102648
Lorenzo-Gómez, M. F., Padilla-Fernández, B., García-Cenador, M. B., Virseda-Rodríguez, Á. J., Martín-García, I., Sánchez-Escudero, A., et al. (2015). Comparison of sublingual therapeutic vaccine with antibiotics for the prophylaxis of recurrent urinary tract infections. Front. Cell Infect. Microbiol. 5, 50. doi:10.3389/fcimb.2015.00050
Malmartel, A., and Ghasarossian, C. (2016). Epidemiology of urinary tract infections, bacterial species and resistances in primary care in France. Eur. J. Clin. Microbiol. Infect. Dis. 35, 447–451. doi:10.1007/s10096-015-2560-1
Malmros, K., Huttner, B. D., McNulty, C., Rodríguez-Baño, J., Pulcini, C., Tängdén, T., et al. (2019). Comparison of antibiotic treatment guidelines for urinary tract infections in 15 European countries: results of an online survey. Int. J. Antimicrob. Agents 54, 478–486. doi:10.1016/j.ijantimicag.2019.06.015
Martínez-Macías, O., Pérez-Doñate, V., and Murcia-Soler, M. (2018). Restrictions of nitrofurantoin: lights and shadows. Med. Clin. Barc. 151, 422–423. doi:10.1016/j.medcli.2018.02.018
Martín Zurro, A., Cano Pérez, J., and Gené Badia, J. (2024). Atención Primaria, Principios, organización y métodos en Medicina de Familia., 9 edición. Elsevier.
Mavi, A., Rathi, I., Shannawaz, M., Saeed, S., and Hasan, S. (2024). Correlates of urinary tract infections among women of reproductive age in India: a systematic review. Cureus 16, e58681. doi:10.7759/cureus.58681
Moreno, A. M., Fernández-García, S., Llor, C., Ouchi, D., García-Sangenís, A., Monteagudo, M., et al. (2023). Diagnostic and therapeutic management of urinary tract infections in Catalonia, Spain: protocol for an observational cohort study. JMIR Res. Protoc. 12, e44244. doi:10.2196/44244
Mulder, M., Baan, E., Verbon, A., Stricker, B., and Verhamme, K. (2019). Trends of prescribing antimicrobial drugs for urinary tract infections in primary care in the Netherlands: a population-based cohort study. BMJ Open 9, e027221. doi:10.1136/bmjopen-2018-027221
Palou, J., Pigrau, C., Molina, I., Ledesma, J. M., and Angulo, J.Grupo Colaborador Español del Estudio ARESC (2011). Etiología y sensibilidad de los uropatógenos identificados en infecciones urinarias bajas no complicadas de la mujer (Estudio ARESC): implicaciones en la terapia empírica. Med. Clin. Barc. 136, 1–7. doi:10.1016/j.medcli.2010.02.042
Patología infecciosa en: Grupo de Trabajo de Enfermedades Infecciosas de la semFYC (2017). Manual de enfermedades infecciosas en Atención Primaria. Available online at: www.semfyc.es.
Plate, A., Kronenberg, A., Risch, M., Mueller, Y., Di Gangi, S., Rosemann, T., et al. (2019). Active surveillance of antibiotic resistance patterns in urinary tract infections in primary care in Switzerland. Infection 47, 1027–1035. doi:10.1007/s15010-019-01361-y
Plate, A., Kronenberg, A., Risch, M., Mueller, Y., Di Gangi, S., Rosemann, T., et al. (2020). Treatment of urinary tract infections in Swiss primary care: quality and determinants of antibiotic prescribing. BMC Fam. Pract. 21, 125. doi:10.1186/s12875-020-01201-1
Programa VINCat (2025). Vigilància de les Infeccions Relacionades amb l’Atenció Sanitària de Catalunya. Available online at: https://hdl.handle.net/11351/12530 (Accessed March 13, 2025).
Recalde, M., Rodríguez, C., Burn, E., Far, M., García, D., Carrere-Molina, J., et al. (2022). Data resource profile: the information system for research in primary care (SIDIAP). Int. J. Epidemiol. 51, e324–e336. doi:10.1093/ije/dyac068
Rodriguez-Mañas, L. (2020). Urinary tract infections in the elderly: a review of disease characteristics and current treatment options. Drugs Context 9, 1–8. doi:10.7573/DIC.2020-4-13
Rui, L., Lindbaek, M., and Gjelstad, S. (2022). Preventive effect of methenamine in women with recurrent urinary tract Infections–a case–control study. Scand. J. Prim. Health Care 40, 331–338. doi:10.1080/02813432.2022.2139363
Samimi, P., Ackerman, A. L., Handler, S., Eilber, K. S., and Anger, J. (2021). Recurrent urinary tract infection in women: primary care referral patterns in a tertiary care center. Female Pelvic Med. Reconstr. Surg. 27, 118–120. doi:10.1097/SPV.0000000000000752
Sanyaolu, L., Best, V., Cannings-John, R., Wood, F., Edwards, A., Akbari, A., et al. (2024). Recurrent urinary tract infections and prophylactic antibiotic use in women: cross-sectional study. Br. J. General Pract. 2024, 0015. doi:10.3399/bjgp.2024.0015
Servei Català de la Salut (2017). Conjunt mínim bàsic de dades (CMBD). Available online at: https://catsalut.gencat.cat/ca/proveidors-professionals/registres-catalegs/registres/cmbd/(Accessed October 7, 2024).
Shallcross, L., Rockenschaub, P., Blackburn, R., Nazareth, I., Freemantle, N., and Hayward, A. (2020). Antibiotic prescribing for lower UTI in elderly patients in primary care and risk of bloodstream infection: a cohort study using electronic health records in England. PLoS Med. 17, e1003336. doi:10.1371/journal.pmed.1003336
Spek, M., Cals, J. W. L., Oudhuis, G. J., Savelkoul, P. H. M., and de Bont, E. G. P. M. (2020). Workload, diagnostic work-up and treatment of urinary tract infections in adults during out-of-hours primary care: a retrospective cohort study. BMC Fam. Pract. 21, 231. doi:10.1186/s12875-020-01305-8
Tandogdu, Z., and Wagenlehner, F. M. E. (2016). Global epidemiology of urinary tract infections. Curr. Opin. Infect. Dis. 29, 73–79. doi:10.1097/QCO.0000000000000228
ten Doesschate, T., Hendriks, K., van Werkhoven, C. H., van der Hout, E. C., Platteel, T. N., Groenewegen, I. A. M., et al. (2022). Nitrofurantoin 100 mg versus 50 mg prophylaxis for urinary tract infections, a cohort study. Clin. Microbiol. Infect. 28, 248–254. doi:10.1016/j.cmi.2021.05.048
Wong, C. K. M., Kung, K., Au-Doung, P. L. W., Ip, M., Lee, N., Fung, A., et al. (2017). Antibiotic resistance rates and physician antibiotic prescription patterns of uncomplicated urinary tract infections in southern Chinese primary care. PLoS One 12, e0177266. doi:10.1371/journal.pone.0177266
World Health Organization (2016). International statistical classification of diseases and related health problems 10th revision. Available online at: https://apps.who.int/iris/handle/10665/246208 (Accessed March 14, 2025).
World Health Organization (2024). ATC/DDD index 2023. Available online at: https://www.whocc.no/atc_ddd_index/ (Accessed March 1, 2025).
Keywords: anti-bacterial agents, diagnosis, electronic health records, primary health care, urinary tract infections, women
Citation: Fernández-García S, Moragas A, Giner-Soriano M, Morros R, Ouchi D, García-Sangenís A and Llor C (2025) Urinary tract infections in women in Catalonia, Spain: a population-based observational cohort study in primary care. Front. Pharmacol. 16:1593910. doi: 10.3389/fphar.2025.1593910
Received: 14 March 2025; Accepted: 03 July 2025;
Published: 09 September 2025.
Edited by:
Paola Scavone, Instituto de Investigaciones Biológicas Clemente Estable (IIBCE), UruguayReviewed by:
Shamimul Hasan, Jamia Millia Islamia, IndiaFrancisco Rodrigues, Polytechnic Institute of Castelo Branco, Portugal
Copyright © 2025 Fernández-García, Moragas, Giner-Soriano, Morros, Ouchi, García-Sangenís and Llor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Silvia Fernández-García, c2Zlcm5hbmRlemdAaWRpYXBqZ29sLmluZm8=