 Ying-Jie Su
Ying-Jie Su Zheng Wu2†
Zheng Wu2† Xiu-Mei Ma
Xiu-Mei Ma- 1Department of Pharmacy, Shanghai Jiao Tong University School of Medicine Affiliated Renji Hospital, Shanghai, China
- 2Department of Radiation Oncology, Shanghai Jiao Tong University School of Medicine Affiliated Renji Hospital, Shanghai, China
- 3Department of Pharmacy, Ningbo Hangzhou Bay Hospital, Ningbo, Zhejiang, China
Background: It has been reported that immunotherapy with programmed cell death protein 1 (PD-1) inhibitors (pembrolizumab or nivolumab) can induce multiple eruptive keratoacanthomas (KAs), representing an immune-related cutaneous adverse event (ircAE).
Methods: This case report describes a 63-year-old female with recurrent cervical adenocarcinoma who developed multiple eruptive KAs and a concurrent fungal infection following treatment with the PD-1 inhibitor zimberelimab. We analyzed the etiology, diagnosis, and treatment by integrating clinical manifestations, pathological examinations, previous treatment history, and a review of the literature.
Results: Despite an initial misdiagnosis as a fungal infection, multidisciplinary review identified KA as an ircAE. Topical corticosteroids led to resolution, and another PD-1 inhibitor was reintroduced without recurrence of cutaneous toxicity.
Conclusion: This is the first documented case of eruptive KA linked to zimberelimab, expanding the spectrum of PD-1 inhibitor-associated ircAEs. A concurrent fungal infection obscured the diagnosis, delaying appropriate treatment and highlighting the importance of recognizing rare ircAEs and multidisciplinary collaboration.
1 Introduction
Adverse events (AEs) associated with immune checkpoint inhibitor (ICI) therapy are termed immune-related adverse events (irAEs), arising from dysregulated immune activation. Among these, immune-related cutaneous adverse events (ircAEs) represent the most frequently observed toxicities, with epidemiologic studies indicating an incidence exceeding 50% across all grades (Haanen et al., 2022; Schneider et al., 2021). The clinical spectrum of ircAEs demonstrates significant variability, predominantly characterized by non-specific maculopapular eruptions, inflammatory dermatitis, or vitiligo (Haanen et al., 2022; Schneider et al., 2021). Keratoacanthoma (KA) is common and somewhat cryptic tumor in humans, with controversial epidemiology, histopathological diagnostic criteria, prognosis, and treatment guidelines (Kwiek and Schwartz, 2016). It has been reported that immunotherapy with programmed cell death protein 1 (PD-1) inhibitors (pembrolizumab or nivolumab) can induce multiple eruptive KAs, representing a rare ircAE (Freites-Martinez et al., 2017; Crow et al., 2020; Bandino et al., 2017). We present the particularly unique concurrence of multiple eruptive KAs with a fungal infection in a cervical adenocarcinoma patient receiving another PD-1 inhibitor (zimberelimab), emphasizing diagnostic challenges and management.
2 Case presentation
A 63-year-old female diagnosed with second recurrence cervical adenocarcinoma was admitted to a tertiary teaching hospital in Shanghai and was treated with chemotherapy and zimberelimab immunotherapy for second-line therapy from 7 February 2024, achieving a partial response (PR) after four cycles. Maintenance therapy with zimberelimab was subsequently initiated after return to the local hospital.
The patient presented on May 20 with scattered pruritic nodules measuring approximately 2–5 mm, surrounded by erythema, on her lips, oral mucosa, and extremities. By July, the lip lesions had progressed to ulceration and scab formation (Figure 1A), and new multiple pruritic papules appeared on the dorsal aspect of the right hand (Figure 1B). By August 8, the lesions on the right dorsal hand had worsened, and a large violaceous nodule with hard papules and areas of ulceration was observed (Figure 1C). A biopsy of the lesion from the right dorsal hand performed at a provincial dermatology hospital led to a diagnosis of superficial fungal infection, and she was prescribed antifungal medicines. However, by late August, new papules developed on her lower legs, soles of the feet, and palms during antifungal treatment (Figures 1D–F). She was switched to other antifungal medicines, but there was still no improvement.
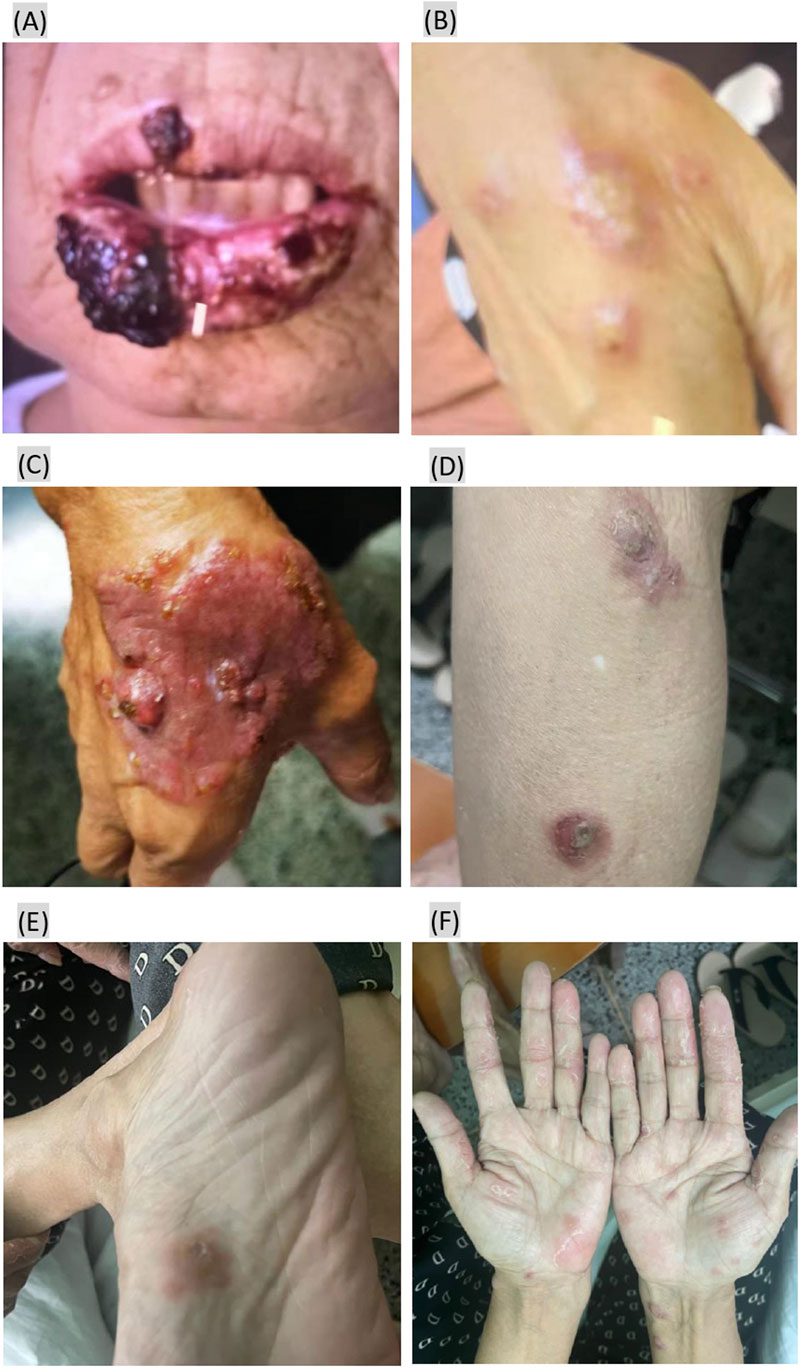
Figure 1. Eruptive keratoacanthoma papules presenting after starting zimberelimab treatment. (A,B) Papules on the lips and right dorsal hand 5 months after zimberelimab treatment. (C) The lesions on right dorsal hand had worsened 6 months after zimberelimab treatment. (D–F) New papules appeared on her lower legs, soles of the feet, and palms nearly 7 months after zimberelimab treatment.
3 Diagnosis and treatment
In September, the patient returned to the tertiary teaching hospital in Shanghai for further treatment, where the original antifungal therapy was continued following a dermatology consultation. An oncology clinical pharmacist conducted a detailed review of the patient’s pathological report in detail: 1. Microscopic pathological findings (Figure 2A) showed excessive keratosis, epidermal hyperplasia and hypertrophy, acanthosis, and irregular extension of dermal processes, along with pseudoepitheliomatous hyperplasia. A neutrophilic abscess, edema of the dermal papillae, small vessel hyperplasia, inflammatory cell infiltration—primarily lamellar lymphocytes and neutrophils—were observed in the epidermis; no granulomas were identified. 2. PAS staining (Figure 2B) presented fungal spores, and mycelia were found in the corneum and epidermal granular layers. Except for fungal infection, the pathological findings were similar to the appearance of “multiple eruptive KAs,” a rare ircAE by ICIs reported in previous papers (Schwartz et al., 2022; Bandino et al., 2017; Freites-Martinez et al., 2017; Crow et al., 2020; Feldstein et al., 2018). The association between the eruptive KAs and zimberelimab was determined using the Naranjo scores, with scores of 5 implying a “probable” relationship. The pharmacist recommended topical halomethasone cream (twice daily) alongside antifungal agents, and zimberelimab was discontinued due to stable tumor status. Most of the skin lesions improved after 10 days of topical halomethasone treatment, and all showed significant remission after 1 month (Figures 3A,B). No new skin lesions were found. Halomethasone cream was subsequently discontinued, and only antifungal therapy was maintained. Another PD-1 inhibitor (sintilimab) was re-administered in the local hospital from December 2024. As of 10 February 2025, the patient had received five infusions of sintilimab, during which time her primary disease remained stable and the skin lesions had completely regressed (Figures 3C,D).
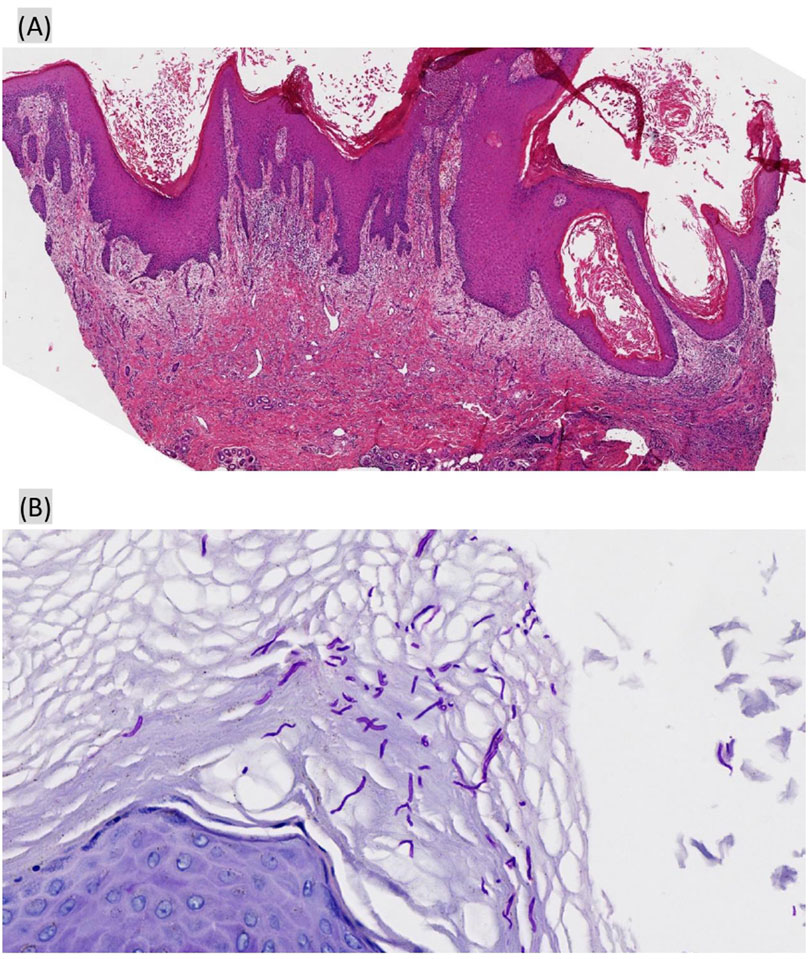
Figure 2. Biopsy of the right dorsal hand papules. (A) Hematoxylin–eosin (HE), original magnification ×40: excessive keratosis, epidermal hyperplasia and hypertrophy, acanthosis, and pseudoepitheliomatous hyperplasia; (B) periodic acid-Schiff (PAS) ×400: fungal spores and mycelia were found in the corneum and epidermal granular layers.

Figure 3. The skin lesions improved after treatment with a topical halomethasone cream. (A,B) All papules improved 1 month after treatment with a topical halomethasone cream; (C,D) skin lesions had completely regressed after 5 months after topical halomethasone treatment.
4 Discussion
To our knowledge, this is the first published report of eruptive KA after treatment with zimberelimab, a PD-1 inhibitor, occurring concurrently with a skin fungal infection. This case expands the spectrum of PD-1 inhibitor-associated ircAEs. While it has been reported that PD-1 inhibitors (pembrolizumab or nivolumab) can induce multiple eruptive KAs, this is the first such association documented with zimberelimab.
Eruptive KA is a rare ircAE induced by immunotherapy, with pathological manifestations ranging from atypical pseudoepitheliomatous hyperplasia (Lee and Wang, 2020; Chaudhari et al., 2017) to typical keratoacanthomas (Schwartz et al., 2022; Olsen et al., 2024; Bednarek et al., 2018) and, in some cases, even resembling squamous cell carcinoma (SCC) (Marsh et al., 2020; Antonov et al., 2019). According to the data from the FAERS database, the current incidence rates of KA and cutaneous squamous cell carcinoma (cSCC) caused by ICIs are 0.027% (43/158000) and 0.053% (83/158000), respectively (Aggarwal et al., 2024). Most cases of eruptive KAs in patients receiving immunotherapy have been reported in the context of lichenoid dermatitis (Schwartz et al., 2022; Feldstein et al., 2018), and eruptive KAs have also been associated with bullous eruptions (Bandino et al., 2017; Schwartz et al., 2022), vitiliginous patches (Bandino et al., 2017), and spongiotic dermatitis (Crow et al., 2020). The patient described in this study exhibited atypical hyperkeratosis, pseudoepitheliomatous hyperplasia, and fungal infection in the context of extensive inflammatory cell infiltration, making the ircAE more complex and difficult to differentiate. This led to the use of antifungal therapy alone during the initial months, delaying appropriate treatment for eruptive KA. As a result, the patient’s quality of life reduced and treatment costs increased. To date, we were the only group to have identified a case of ICI-induced KA occurring concurrently with a skin infection, which contributed to the delayed diagnosis. This case was of great significance in reminding oncologists and dermatologists to highlight a differential diagnosis for rare ircAEs, reinforcing the need for simultaneous biopsy and culture in new lesions. Similarly, there have been analogous reports of such patients being misdiagnosed with SCC and receiving unnecessary radiotherapy, chemotherapy, and/or targeted therapy (Crow et al., 2020; Lee and Wang, 2020). In view of this, rare irAEs particularly require a detailed differential diagnosis that takes into account both pathological methods (Wang and Chen, 2025) and the entire course of diagnosis and treatment.
Multiple eruptive KAs pose a great treatment challenge due to the large number of lesions and the morbidity associated with both surgical and medical management. As a result, controversies remain regarding the optimal approach. In some fortunate patients, the lesions resolved spontaneously, even when immunotherapy was not discontinued (Haraszti et al., 2019) or after the largest lesion was treated with complete curettage, with other lesions resolving thereafter (Antonov et al., 2019). Some patients, like the one we reported in this study, achieved complete regression with only the topical application of a potent corticosteroid cream (Fradet et al., 2019; Marsh et al., 2020); others received combinations of oral corticosteroids (Bandino et al., 2017), acitretin (Schwartz et al., 2022; Haraszti et al., 2019) or hydroxychloroquine (Crow et al., 2020), or intralesional injections of triamcinolone (Lee and Wang, 2020; Freites-Martinez et al., 2017; Bednarek et al., 2018) or 5-fluorouracil (Olsen et al., 2024). In addition, surgical resection or cryosurgery has been used to treat KA lesions in some cases (Marsh et al., 2020; Freites-Martinez et al., 2017; Feldstein et al., 2018; Chaudhari et al., 2017). According to previous literature and this case, eruptive KAs represent inflammation-related, reactive, reversible hyperplasia, rather than true neoplasia, supporting the use of nonsurgical anti-inflammatory therapies (Crow et al., 2020).
5 Conclusion
This case underscores the need for heightened suspicion of ircAEs, like eruptive KAs in patients on ICIs, even in the presence of concurrent infections. Multidisciplinary teamwork (MDT) facilitates timely diagnosis, and topical corticosteroids offer a non-invasive treatment option. Successful rechallenge with a different PD-1 inhibitor suggests appropriate treatment and careful monitoring may enable continued immunotherapy.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material; further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were approved by the Ethics Committee of Renji Hospital, affiliated with Shanghai Jiao Tong University School of Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
Y-JS: writing – original draft, conceptualization. ZW: writing – original draft. Y-LH: writing – original draft, data curation. M-XY: data curation, writing – original draft. X-MM: project administration, writing – review and editing. H-WL: project administration, writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by Bethune Public Welfare Foundation of China (grant no. Z04JKM2023E040).
Acknowledgments
The patient in this manuscript provided written informed consent for the publication of her case details.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Aggarwal, P., Clark, D., Shah, A., Rismiller, K., and Neltner, S. A. (2024). Keratoacanthoma and cutaneous squamous cell carcinoma with PD-1 and PD-L1 inhibitor use. JAMA Dermatol 160, 573–575. doi:10.1001/jamadermatol.2024.0390
Antonov, N. K., Nair, K. G., and Halasz, C. L. (2019). Transient eruptive keratoacanthomas associated with nivolumab. JAAD Case Rep. 5, 342–345. doi:10.1016/j.jdcr.2019.01.025
Bandino, J. P., Perry, D. M., Clarke, C. E., Marchell, R. M., and Elston, D. M. (2017). Two cases of anti-programmed cell death 1-associated bullous pemphigoid-like disease and eruptive keratoacanthomas featuring combined histopathology. J. Eur. Acad. Dermatol Venereol. 31, e378–e380. doi:10.1111/jdv.14179
Bednarek, R., Marks, K., and Lin, G. (2018). Eruptive keratoacanthomas secondary to nivolumab immunotherapy. Int. J. Dermatol 57, e28–e29. doi:10.1111/ijd.13893
Chaudhari, S., Leon, A., Levin, E., Neuhaus, I., and Liao, W. (2017). Case report of multiple keratoacanthomas and squamous cell carcinomas in a patient receiving pembrolizumab. J. Drugs Dermatol 16, 513–515.
Crow, L. D., Perkins, I., Twigg, A. R., Fassett, M. S., Leboit, P. E., Berger, T. G., et al. (2020). Treatment of PD-1/PD-L1 inhibitor-induced dermatitis resolves concomitant eruptive keratoacanthomas. JAMA Dermatol 156, 598–600. doi:10.1001/jamadermatol.2020.0176
Feldstein, S. I., Patel, F., Larsen, L., Kim, E., Hwang, S., and Fung, M. A. (2018). Eruptive keratoacanthomas arising in the setting of lichenoid toxicity after programmed cell death 1 inhibition with nivolumab. J. Eur. Acad. Dermatol Venereol. 32, e58–e59. doi:10.1111/jdv.14503
Fradet, M., Sibaud, V., Tournier, E., Lamant, L., Boulinguez, S., Brun, A., et al. (2019). Multiple keratoacanthoma-like lesions in a patient treated with pembrolizumab. Acta Derm. Venereol. 99, 1301–1302. doi:10.2340/00015555-3301
Freites-Martinez, A., Kwong, B. Y., Rieger, K. E., Coit, D. G., Colevas, A. D., and Lacouture, M. E. (2017). Eruptive keratoacanthomas associated with pembrolizumab therapy. JAMA Dermatol 153, 694–697. doi:10.1001/jamadermatol.2017.0989
Haanen, J., Obeid, M., Spain, L., Carbonnel, F., Wang, Y., Robert, C., et al. (2022). Management of toxicities from immunotherapy: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 33, 1217–1238. doi:10.1016/j.annonc.2022.10.001
Haraszti, S., Polly, S., Ezaldein, H. H., Rothbaum, R., Delost, G. R., and Beveridge, M. (2019). Eruptive squamous cell carcinomas in metastatic melanoma: an unintended consequence of immunotherapy. JAAD Case Rep. 5, 514–517. doi:10.1016/j.jdcr.2019.03.014
Kwiek, B., and Schwartz, R. A. (2016). Keratoacanthoma (KA): an update and review. J. Am. Acad. Dermatol 74, 1220–1233. doi:10.1016/j.jaad.2015.11.033
Lee, M. P., Wang, A. R., and Wang, A. R. (2020). Pembrolizumab-induced pseudoepitheliomatous eruption consistent with hypertrophic lichen planus. J. Cutan. Pathol. 47, 275–279. doi:10.1111/cup.13587
Marsh, R. L., Kolodney, J. A., Iyengar, S., Yousaf, A., Louden, B. A., Al-Bouri, A., et al. (2020). Formation of eruptive cutaneous squamous cell carcinomas after programmed cell death protein-1 blockade. JAAD Case Rep. 6, 390–393. doi:10.1016/j.jdcr.2020.02.024
Olsen, E., Svoboda, S. A., Montanez-Wiscovich, M., and Saikaly, S. K. (2024). Multiple eruptive keratoacanthomas secondary to nivolumab immunotherapy. J. Immunother. 47, 98–100. doi:10.1097/cji.0000000000000498
Schneider, B. J., Naidoo, J., Santomasso, B. D., Lacchetti, C., Adkins, S., Anadkat, M., et al. (2021). Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J. Clin. Oncol. 39, 4073–4126. doi:10.1200/jco.21.01440
Schwartz, R. J., Ho, G., Smith, A., Collgros, H., Regio Pereira, A., Gouveia, B., et al. (2022). Successful treatment of eruptive keratoacanthomas with actitretin for patients on checkpoint inhibitor immunotherapy. J. Eur. Acad. Dermatol Venereol. 36, e445–e448. doi:10.1111/jdv.17940
Keywords: immune checkpoint inhibitors, programmed cell death protein 1, immune-related adverse event, immune-related cutaneous adverse event, eruptive keratoacanthomas
Citation: Su Y-J, Wu Z, Hou Y-L, Yan M-X, Ma X-M and Lin H-W (2025) Case Report: Immune-related eruptive keratoacanthoma with fungal coinfection under PD-1 inhibitor therapy: a diagnostic and therapeutic challenge. Front. Pharmacol. 16:1619450. doi: 10.3389/fphar.2025.1619450
Received: 28 April 2025; Accepted: 25 July 2025;
Published: 13 August 2025.
Edited by:
Zhijie Xu, Central South University, ChinaReviewed by:
Sebastian Yu, Kaohsiung Medical University, TaiwanEmmanouil Karampinis, University of Thessaly, Greece
Copyright © 2025 Su, Wu, Hou, Yan, Ma and Lin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiu-Mei Ma, c2FsbHltYTEyMDFAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship