 Mirella Llamosí1,2†Covadonga Pérez-García1†Aída Úbeda1,2
Mirella Llamosí1,2†Covadonga Pérez-García1†Aída Úbeda1,2 Erick J. Vidal-Alcántara1
Erick J. Vidal-Alcántara1 Inés Pareja-Cerbán1,2Elena Gómez-Rubio3Pilar Coronel3
Inés Pareja-Cerbán1,2Elena Gómez-Rubio3Pilar Coronel3 Juan Carlos Sanz4,5Mirian Domenech1,2
Juan Carlos Sanz4,5Mirian Domenech1,2 Julio Sempere1,2*
Julio Sempere1,2* Jose Yuste1,2*
Jose Yuste1,2*- 1Spanish Pneumococcal Reference Laboratory, National Center for Microbiology, Instituto de Salud Carlos III, Madrid, Spain
- 2CIBER de Enfermedades Respiratorias (CIBERES), Instituto de Salud Carlos III, Madrid, Spain
- 3Scientific Department, Meiji Pharma Spain, Alcala de Henares, Spain
- 4Regional Public Health Laboratory, Comunidad de Madrid, Madrid, Spain
- 5CIBER de Epidemiología y Salud Pública (CIBERESP), Instituto de Salud Carlos III, Madrid, Spain
Background: Streptococcus pneumoniae remains a major respiratory pathogen. Although pneumococcal conjugate vaccines (PCVs) have reduced the burden of resistant vaccine-covered serotypes, serotype replacement has led to the emergence of non-vaccine types.
Methods: This study assessed the activity of β-lactam antibiotics against 1,018 clinical isolates of S. pneumoniae with reduced penicillin susceptibility collected across Spain in 2019–2020. Minimum inhibitory concentrations (MICs) were determined for oral cephalosporins (cefditoren, cefuroxime, cefixime, cefpodoxime), intravenous cephalosporins (cefotaxime, cefuroxime), and penicillins (penicillin, amoxicillin). MIC50 and MIC90 values were analyzed by year, serotype (PCV20- vs. PCV21-specific), and clinical presentation.
Results: Cefditoren showed the lowest MIC50/90 values among oral β-lactams, and cefotaxime was the most active intravenous cephalosporin. Most isolates were resistant to cefuroxime (oral and intravenous) based on EUCAST breakpoints. While penicillin derivatives showed susceptibility with increased exposure at MIC50, MIC90 values indicated resistance to oral amoxicillin. A rise in antibiotic use during the COVID-19 pandemic’s first year was associated with an increased proportion of resistant isolates, particularly among non-invasive respiratory infections. Serotype analysis revealed that PCV20-specific types (9V, 14 and 19A) and shared PCV20 and PCV21 serotypes (11A and 19A) had higher MIC90 values and bigger proportion of resistant strains to β-lactams than PCV21-unique ones (15A, 23B and 24F).
Conclusion: Despite the overall increase in resistance, cefditoren and cefotaxime retained favorable in vitro activity, while cefuroxime, cefixime, and cefpodoxime exhibited poor efficacy. Newer PCVs may broaden protection against emerging resistant serotypes, yet continued antimicrobial resistance surveillance is essential, especially regarding non-vaccine serotypes. These findings support cefditoren and cefotaxime as viable therapeutic options against non-susceptible S. pneumoniae isolates.
1 Introduction
The use of pneumococcal conjugate vaccines (PCVs) in children and adults has proven to be an effective intervention for controlling the burden of both invasive and non-invasive pneumococcal disease (Bertran et al., 2024; Pérez-García et al., 2024; Sempere et al., 2024; Pérez-García et al., 2025), in addition to being a key measure in reducing the impact of antimicrobial resistance (AMR). In Spain, the effectiveness of PCVs (PCV7 and PCV13) in controlling the spread of resistant pneumococcal isolates has been demonstrated, and it is suggested that incorporating these vaccines into national immunization schedules is a cost-effective strategy to counteract antibiotic resistance (Sempere et al., 2022; Calvo-Silveria et al., 2025). Before the introduction of PCVs in Spain, most cases of invasive pneumococcal disease (IPD) associated with antimicrobial resistance were caused by serotypes included in conjugate vaccines (Fenoll et al., 2015). Following the implementation of PCV7 for a brief period and later PCV13, there was a drastic decline in IPD cases caused by vaccine serotypes associated with resistance (Sempere et al., 2022). However, the emergence of non-vaccine serotypes harboring antibiotic resistance has also been observed. These serotypes have been increasing in recent years, and some are associated with hypervirulence, such as the ST6521 clone in serotype 11A (Aguinagalde et al., 2015; González-Díaz et al., 2020) and the GPSC10 genetic lineage in serotype 24F (Lo et al., 2022), which is linked to severe meningitis episodes.
In the United States, PCVs have also shown an impact in reducing the burden of IPD caused by antibiotic-resistant serotypes (Bajema et al., 2022). Among children under 5 years old, the incidence of resistance-associated IPD decreased across all antibiotic classes from 2009 to 2018, dropping from 8.8 to 2.3 per 100,000 inhabitants for macrolides, from 5.9 to 0.4 per 100,000 for cephalosporins, and from 5.2 to 0.4 per 100,000 for penicillins (Bajema et al., 2022). Among adults over 65 years old during the same period, the incidence decreased from 10.4 to 7.3 per 100,000 for macrolides, from 6.2 to 2.4 per 100,000 for cephalosporins, and from 3.6 to 1.6 per 100,000 for penicillins (Bajema et al., 2022). Nearly two decades after the introduction of PCVs in the U.S., their impact on reducing IPD by AMR resistant isolates remains significant.
However, recently approved and implemented vaccines, such as PCV15 and PCV20, along with PCV21—an adult-targeted vaccine already approved by the FDA and EMA—are expected to expand coverage against non-vaccine serotypes associated with antibiotic resistance. To ensure their effectiveness, these vaccines must be administered with high coverage rates. Another problem with AMR and IPD is the possibility of increased resistant rates during the first pandemic year due to the extensive use of azithromycin and other antibiotics to prevent complications related to bacterial coinfections in patients with COVID-19 (Meschiari et al., 2022). Several authors have warned that antibiotic resistance has expanded because of the careless use of antibiotics in the medical field, the food industry, agriculture, and other industries (Singh, 2024). In addition, other studies have stated that antimicrobial resistance has emerged as a hidden pandemic following COVID-19 (Singh and Sodhi, 2023). A recent report from United States confirmed that multidrug resistant infections in hospitals increased during the pandemic due to antibiotic exposure (Yek et al., 2025).
In this study, we show the evolution of antimicrobial resistance to different β-lactam antibiotics including oral cephalosporins, intravenous cephalosporins, and penicillins, in pneumococcal isolates causing disease in adults. We compared data from 2019 to 2020, coinciding with the years before and after the COVID-19 pandemic, to assess the impact of the pandemic in the antibiotic susceptibility of Streptococcus pneumoniae.
2 Materials and methods
2.1 Study design
All pneumococcal isolates tested were received at the Spanish Pneumococcal Reference Laboratory (SPRL) as part of the daily routine surveillance conducted in the laboratory. The study period covers the years 2019, a late PCV13 vaccine period prior to COVID-19 pandemic and 2020, the first year of COVID-19 pandemic when non-pharmacological measures were implemented since February.
We randomly selected a minimum of 500 clinical isolates from 2019 to 2020 that were non-susceptible to penicillin with a minimum inhibitory concentration (MIC) ≥ 0.12 mg/L. In this case, we selected 500 of 586 non-susceptible isolates from 2019 (85.3%), and all 518 non-susceptible isolates from the year 2020 (100%). The 2019 isolates were randomly chosen from our nationwide collection, which already ensures representative sampling across Spanish regions. As our study focused on characterizing the overall population of penicillin non-susceptible isolates rather than regional differences, random selection was considered sufficient to maintain representativeness, while ensuring that the final selection still included isolates from all regions. All clinical isolates were obtained from adult patients, with an average age of 57 years in 2019, and 61 years in 2020. Isolates were categorized into three clinical groups: invasive pneumonia (blood isolates from hospitalized pneumonia patients), non-invasive pneumonia (bronchoaspirate isolates from pneumonia cases), and non-respiratory invasive infections (blood isolates from non-pneumonia cases). Meningitis isolates were excluded from the study. Pneumonia was diagnosed by clinicians based on clinical criteria and recorded using the International Classification of Diseases (ICD) codes. Cases were reported to the pneumococcal reference laboratory when strains were submitted for characterization from the different Spanish hospitals. All respiratory invasive pneumonia strains were isolated from hemocultures, whereas non-invasive pneumonia strains were obtained from bronchoaspirates. For non-respiratory invasive infections, all strains were isolated from patients without respiratory disease and were also obtained from hemocultures.
The SPRL annually reports all IPD cases in Spain to the European Center for Disease Control (ECDC), covering up to 80%–85% of the national cases according to estimates from the National Center for Epidemiology. Since 2018, it has also reported cases to the Invasive Respiratory Infection Surveillance Network (IRIS). Pneumococcal identification was confirmed using the Optochin-susceptibility test and bile solubility test. Serotyping was conducted using the Quellung reaction, dot blot assay with specific antisera, and/or PCR-capsular sequence analysis as previously described (de Miguel et al., 2021; Pérez-García et al., 2024). Optochin disk and blood agar plates were purchased from Becton Dickison Spain. Antipneumococcal sera for serotyping were purchased from Statem Serum Institute (Denmark).
2.2 Antimicrobial susceptibility testing
We included and compared antimicrobial susceptibility testing of oral cephalosporins (cefixime, CFX; cefditoren, CDN; cefpodoxime, CPD; and cefuroxime, CXM), intravenous cephalosporins (cefotaxime, CTX; cefuroxime, CXM) and other β-lactams (penicillin, PEN; amoxicillin, AMX). MICs were determined by agar dilution technique following EUCAST clinical breakpoints from 2023 (Table 1).
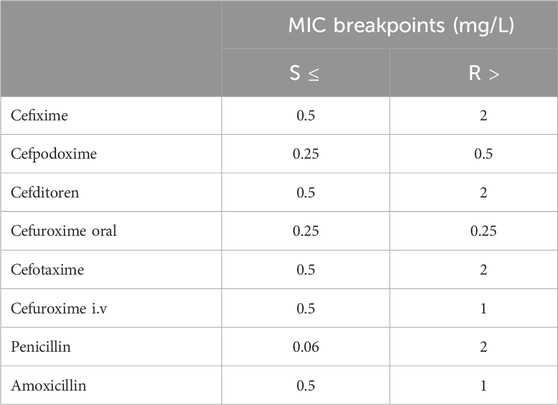
Table 1. MIC breakpoints for Streptococcus pneumoniae considered in the study following EUCAST criteria.
Streptococcus pneumoniae ATCC 49619 standard strain was used as control. Antimicrobials were purchased from Sigma Aldrich (Merck, United States). Cefditoren was obtained from Meiji Pharma Spain.
2.3 Statistical analysis
Data of antimicrobial susceptibility to each antibiotic are representative of results obtained from all the isolates analyzed of each year (500 isolates from 2019 and 518 from 2020). Statistical analysis was performed by using two-tailed Student’s t-test (for two groups’ comparisons). GraphPad InStat version 8.2 (GraphPad Software, San Diego, CA, United States) was used for data analysis. Differences were considered statistically significant with P < 0.05 (*) and highly significant with P < 0.01 (**) and P < 0.001 (***). MIC50 represents the minimum concentration of an antimicrobial that inhibits 50% of the tested isolates, while MIC90 represents the concentration that inhibits 90% of the isolates, and they were calculated as the 50th and 90th percentiles respectively.
3 Results
3.1 Cefditoren and cefotaxime are the cephalosporins with lower MIC values during the study period
Analysis of antimicrobial susceptibility of oral cephalosporins confirmed that cefixime exhibited the highest MIC90 and MIC50 values in 2019 and 2020, with values of 32 mg/L and 8 mg/L, respectively, in both years (Figure 1). These non-susceptibility levels corresponded to resistance according to EUCAST breakpoints. Cefuroxime was the second oral cephalosporin, with the highest MIC90 and MIC50 values in 2019–2020. Its MIC50 value increased from 2 mg/L in 2019 to 4 mg/L in 2020, while its MIC90 remained at 8 mg/L in both years (Figure 1). All MIC values for cefuroxime classified the studied isolates as resistant according to both oral and intravenous EUCAST breakpoints (Table 1). Cefpodoxime presented MIC90 and MIC50 values of 4 mg/L and 0.5–1 mg/L, respectively being classified as resistant with EUCAST breakpoints. Cefditoren had MIC90 and MIC50 values of 1 mg/L and 0.25 mg/L, respectively, in both years (Figure 1). This is interesting because cefditoren showed the lowest MIC values among all oral cephalosporins studied.
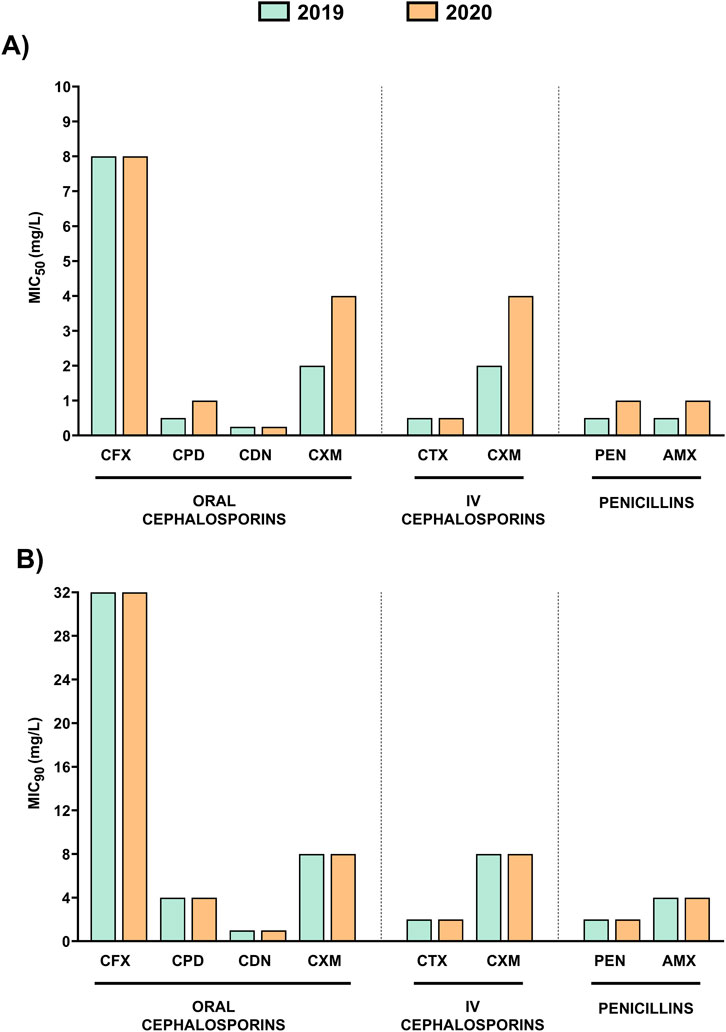
Figure 1. Comparison of MIC50 and MIC90 values for oral cephalosporins, intravenous cephalosporins, and penicillins in 2019 and 2020. (A) MIC50 values (mg/L) for all isolates tested in the study in 2019 (green) and 2020 (orange). (B) MIC90 values (mg/L) for all isolates tested in the study in 2019 (green) and 2020 (orange).
Among intravenous cephalosporins, cefotaxime presented lowest MIC values than cefuroxime, with MIC90 of 2 mg/L and MIC50 of 0.5 mg/L in 2019–2020 (Figure 1). Antibiotic interpretation according to EUCAST criteria, showed that pneumococcal isolates may be considered susceptible with increased exposure to cefotaxime and resistant to cefuroxime (Table 1). Statistical analysis confirmed significant differences for cefditoren as the antibiotic with the lowest MIC in comparison to the rest of β-lactam antibiotics including cefotaxime (***P < 0.001, two-tailed Student’s t-test).
In most cases, general MIC values were similar between 2019 and 2020 but for cefuroxime, cefpodoxime, penicillin and amoxicillin, we observed an increase in the MIC50 value from 2019 to 2020 (Figure 1A). In the case of amoxicillin, this represents a shift from “susceptible with increased exposure” to “resistant” (Table 1). Moreover, to evaluate the impact of higher antibiotic consumption at the early stages of COVID-19 pandemic, we evaluated the proportion of pneumococcal resistant isolates in 2019 and 2020 (Figure 2). Our results showed an increased pattern of antibiotic resistance to most antibiotics evaluated from 2019 to 2020 (Figure 2). The increase was remarkable for all antibiotics but for cefditoren and cefotaxime, where we only observed a slight increase in the proportion of resistant isolates of 0.2% or a diminish in the proportion of resistance isolates to 1.2% respectively (Figure 2).
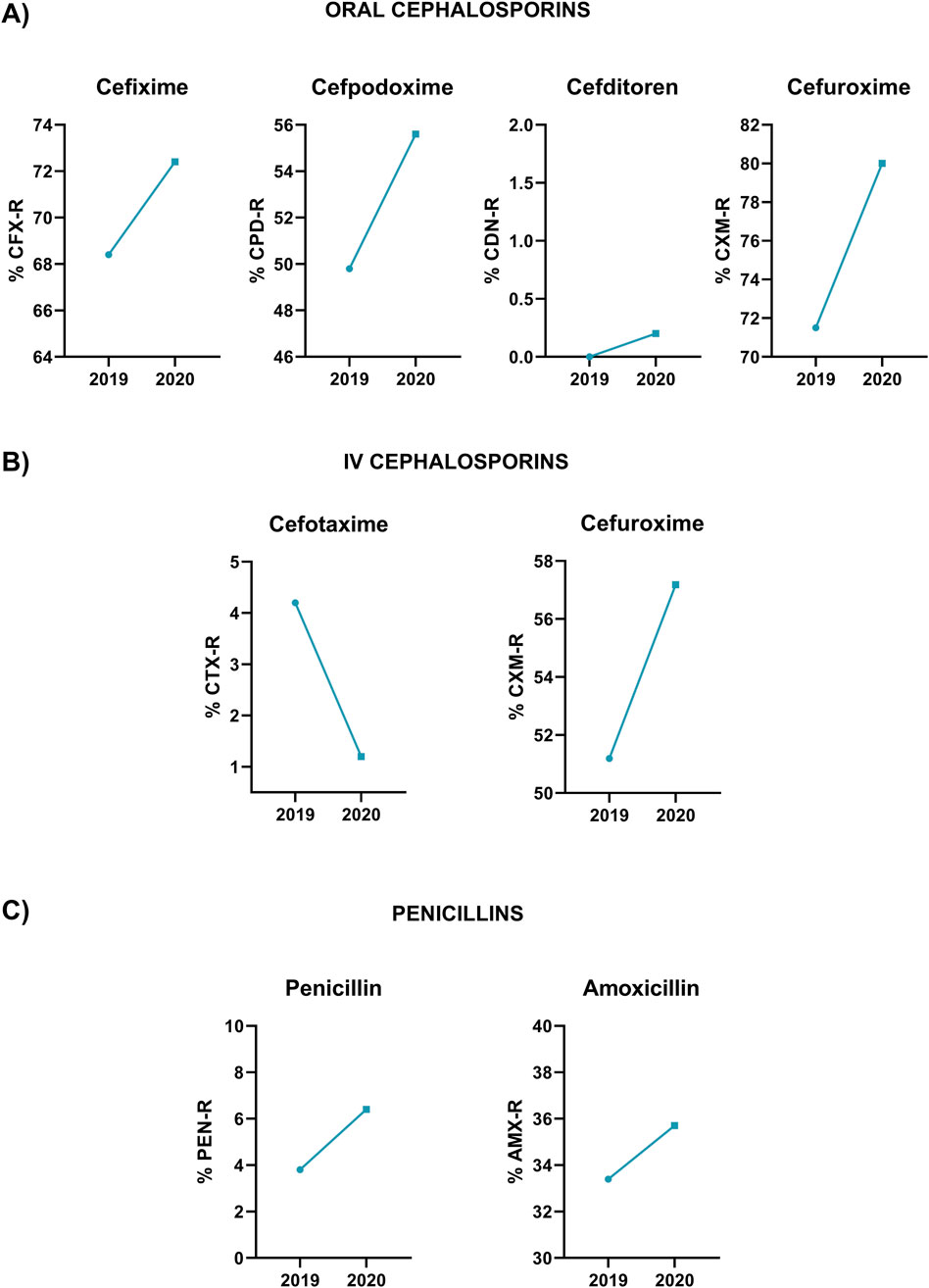
Figure 2. Proportion of resistant isolates in 2019 and 2020 following EUCAST clinical breakpoints to the different antibiotics tested in the study. (A) Oral cephalosporins. (B) Intravenous cephalosporins. (C) Penicillins.
3.2 Cefditoren and cefotaxime maintain low MIC values regardless of the source of the infection
The outcome of the infection based on the antibiotic treatment choice may be affected by the localization of the infectious process. Infections of the respiratory tract that may be caused in many cases by bacteria forming biofilms such as patients with chronic obstructive pulmonary disease (COPD) might be more difficult to eradicate than bacteria from other origins that are not associated with biofilms (Kyd et al., 2011; Domenech et al., 2012). Invasive isolates (regardless of the origin) had lower MIC values for intravenous cephalosporins (cefotaxime and cefuroxime) and penicillins (penicillin and amoxicillin) in comparison to non-invasive isolates from respiratory origin (Table 2). Another interesting finding was that cefditoren and cefotaxime as oral and intravenous options respectively showed the lowest MIC90 values (0.5–1 mg/L) of all antibiotics tested (Table 2).
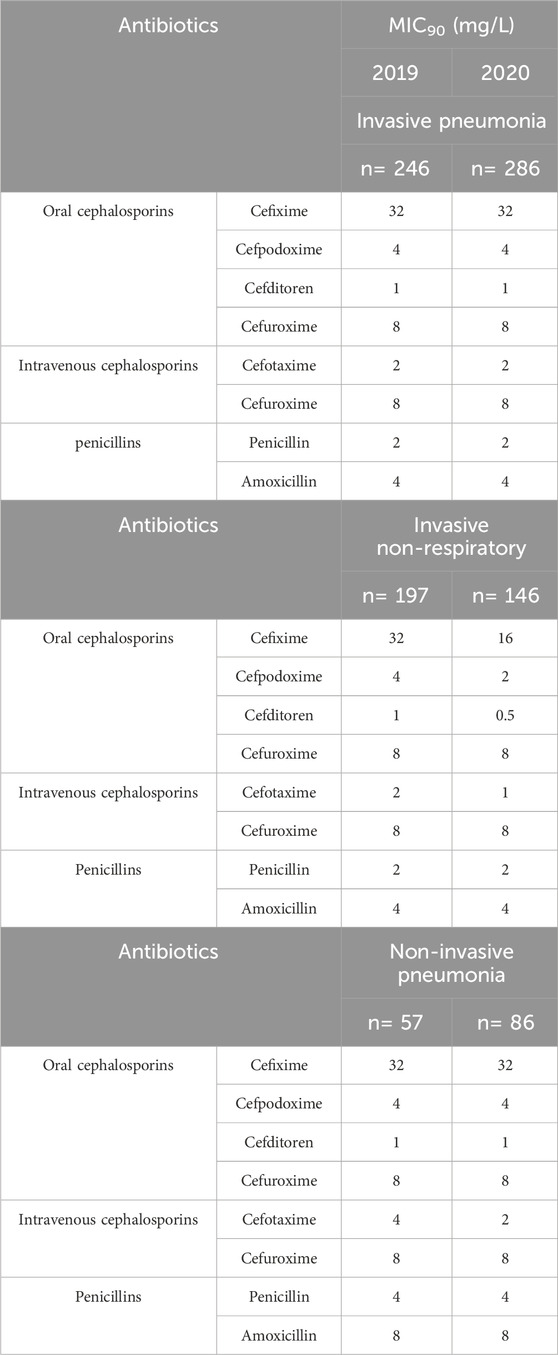
Table 2. In vitro activity of oral cephalosporins, intravenous cephalosporins, and penicillins in clinical isolates from different sources. Number of isolates from each clinical group are indicated in the table.
3.3 Evolution of antibiotic resistance in prevalent unique serotypes of PCV20 and PCV21 causing IPD in adults
Characterization of the resistance levels of serotypes included in the recent approved vaccines PCV20 and PCV21 is essential to evaluate their impact to prevent pneumococcal disease caused by resistant isolates of these serotypes. Hence, we analyzed the MIC90 values for the different β-lactams of the most prevalent unique PCV20 serotypes that are not included in PCV21 (9V, 14 and 19F), unique PCV21 serotypes not included in PCV20 (15A, 23B and 24F) and common PCV20/PCV21 serotypes that are present in both vaccines (11A and 19A) (Figures 3–5).
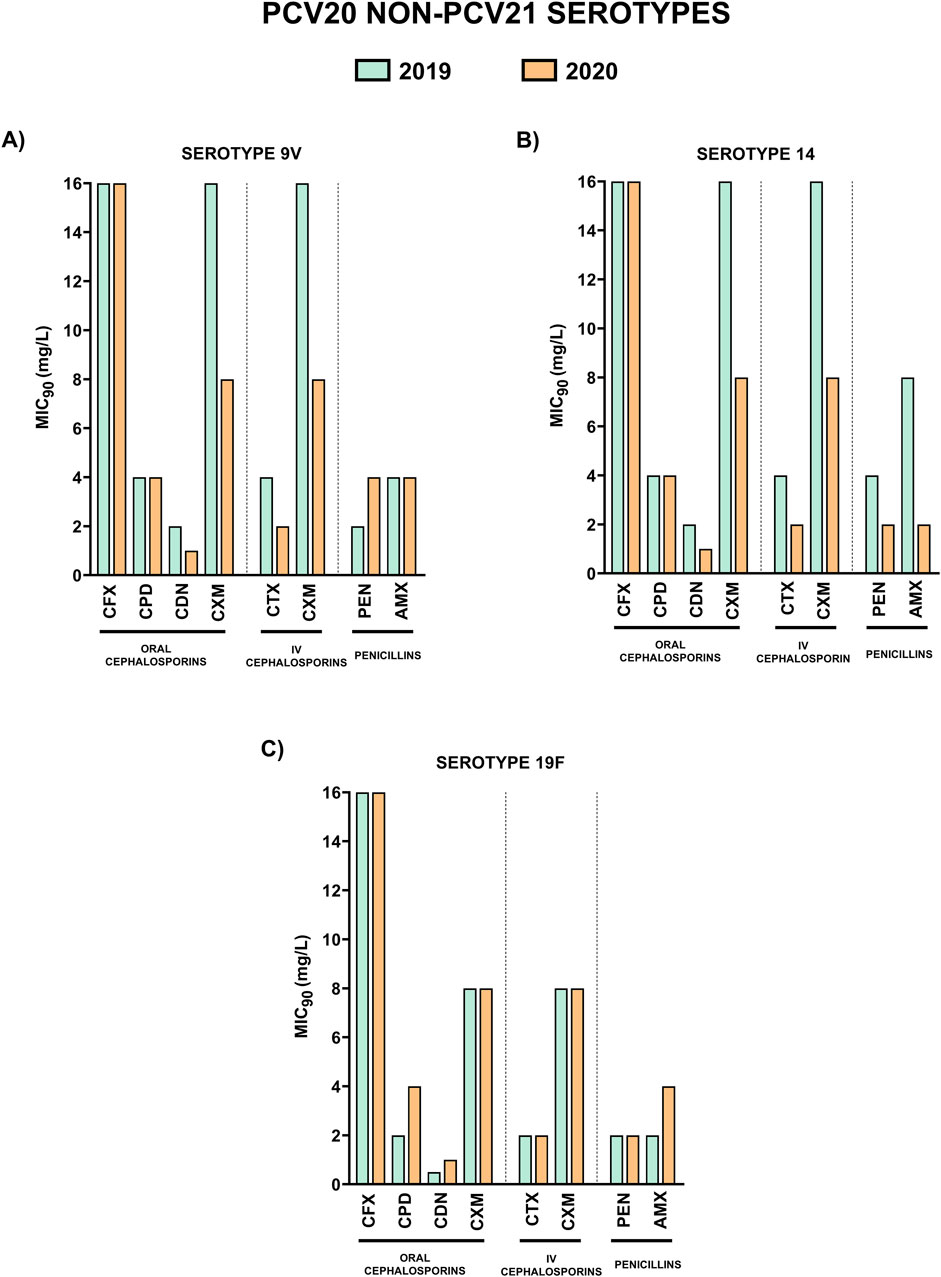
Figure 3. Comparison of MIC90 values of oral cephalosporins, intravenous cephalosporins and penicillins for the most prevalent serotypes associated with non-susceptibility to penicillin included in PCV20 and not in PCV21. 2019 is shown in green and 2020 in orange. (A) MIC90 values (mg/L) for serotype 9V. (B) MIC90 values (mg/L) for serotype 14. (C) MIC90 values (mg/L) for serotype 19F.
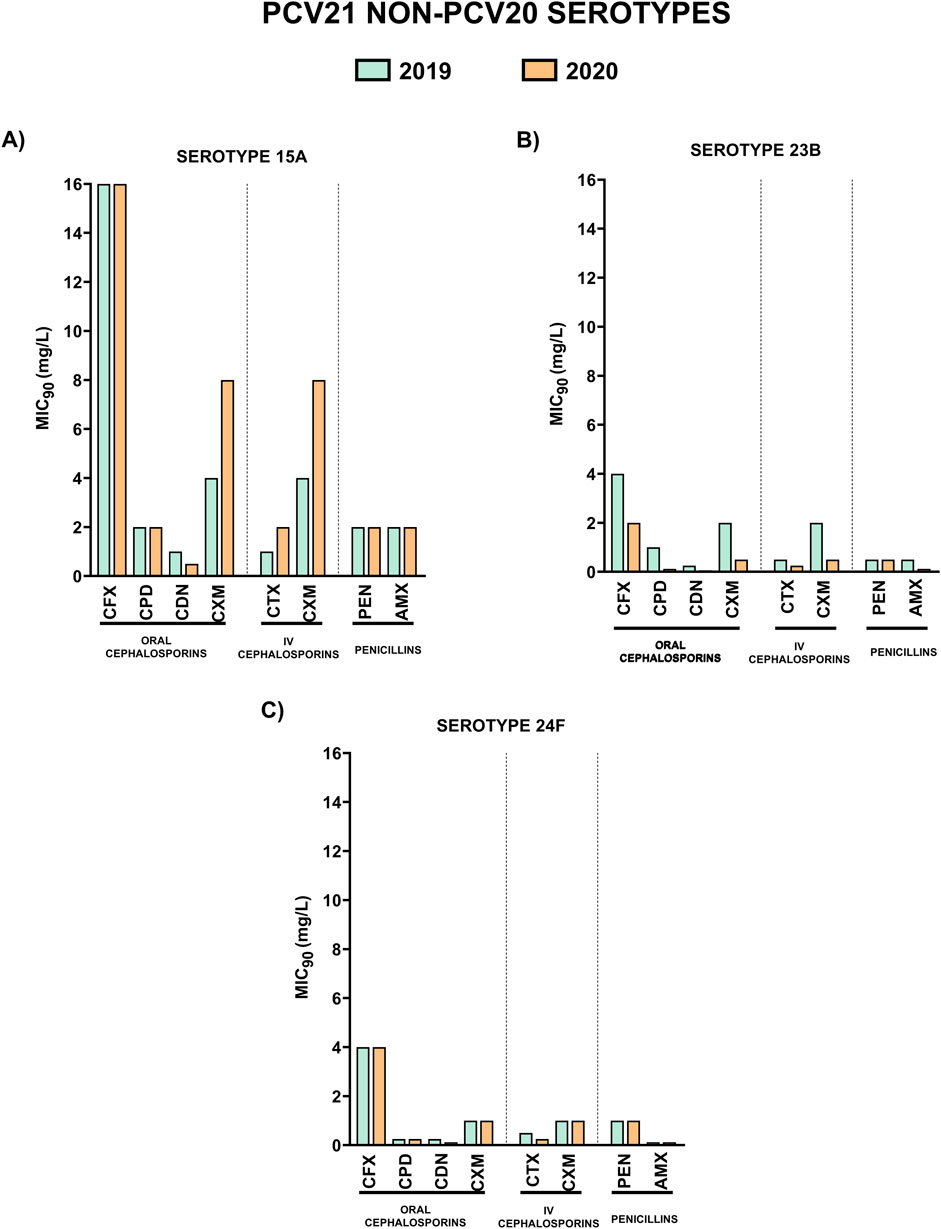
Figure 4. Comparison of MIC90 values of oral cephalosporins, intravenous cephalosporins and penicillins for the most prevalent serotypes associated with non-susceptibility to penicillin included in PCV21 and not in PCV20. 2019 is shown in green and 2020 in orange. (A) MIC90 values (mg/L) for serotype 15A. (B) MIC90 values (mg/L) for serotype 23B. (C) MIC90 values (mg/L) for serotype 24F.
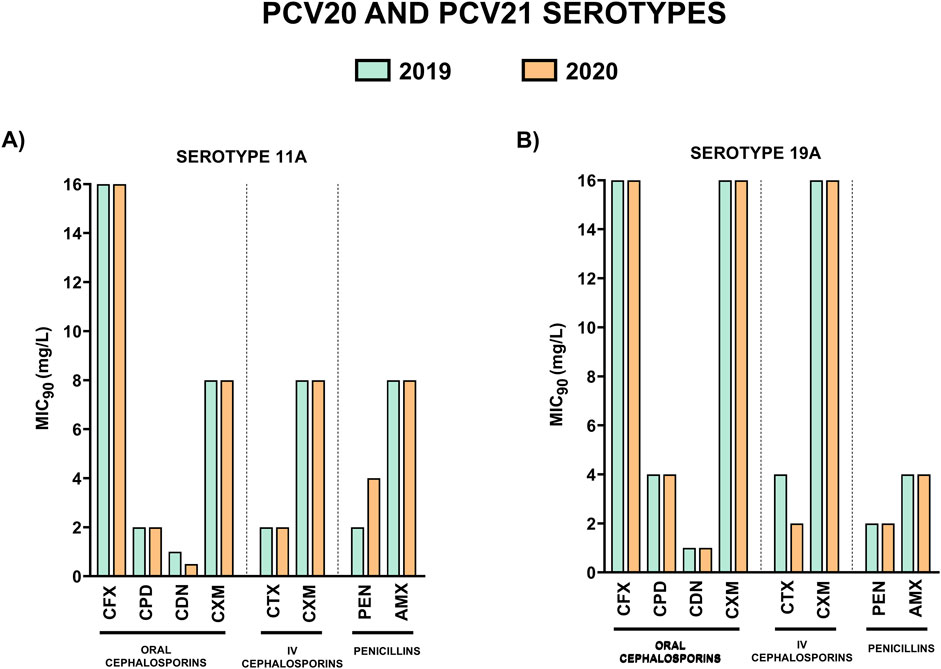
Figure 5. Comparison of MIC90 values of oral cephalosporins, intravenous cephalosporins and penicillins for the most prevalent serotypes associated with non-susceptibility to penicillin included in both PCV20 and PCV21. 2019 is shown in green and 2020 in orange. (A) MIC90 values (mg/L) for serotype 11A. (B) MIC90 values (mg/L) for serotype 19A.
Unique PCV20 serotypes and those that are shared by both vaccines, presented higher MIC90 values to the different antibiotics in comparison to unique PCV21 serotypes (Figures 3, 4). Among oral cephalosporins, cefixime exhibited the highest MIC90 values in all the serotypes studied followed by cefuroxime and cefpodoxime. In contrast, cefditoren demonstrated the greatest activity across all serotypes, with the lowest MIC90 values, even considering the intravenous cephalosporin cefotaxime (Figures 3–5). When studying the activity against penicillins, unique PCV20 serotypes and common PCV20/PCV21 serotypes presented higher MIC90 levels to both penicillin and amoxicillin (Figures 3, 5). Our study confirmed that serotype 11A that is present in PCV20 and PCV21 had the higher MIC90 levels to penicillin and amoxicillin (Figure 5). Moreover, we also observed that unique PCV20 serotypes, especially serotypes 9V and 14, and common PCV20/PCV21 serotypes (11A and 19A) presented a higher proportion of resistant strains to the different β-lactams than unique PCV21 serotypes (Table 3). None of the unique PCV21 non-PCV20 serotypes presented resistant strains to penicillin or cefotaxime, and only serotype 15A presented strains resistant to amoxicillin (Table 3). Cefditoren was the only β-lactam without resistant strains in the most prevalent serotypes associated with non-susceptibility to penicillin in Spain.
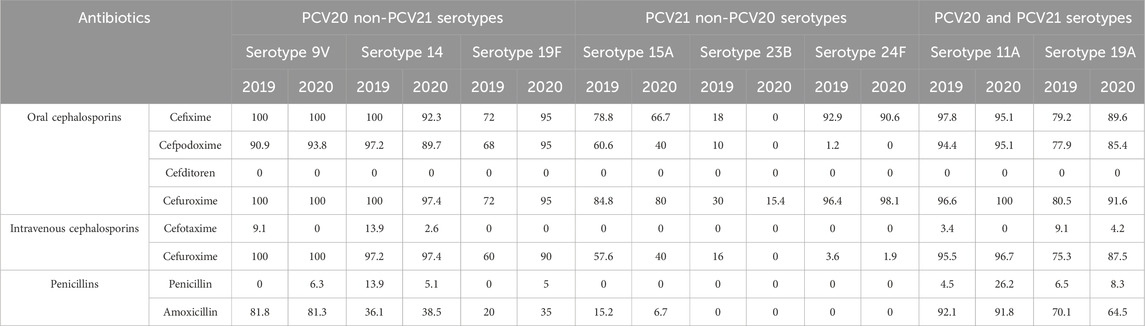
Table 3. Percentage of resistant isolates to β-lactams for the different serotypes analyzed in the study. Serotypes associated with non-susceptibility to penicillin included in PCV20 and not in PCV21 (9V, 14 and 19F). Serotypes associated with non-susceptibility to penicillin included in PCV21 and not in PCV20 (15A, 23B and 24F). Serotypes associated with non-susceptibility to penicillin included in both PCV20 and PCV21 (11A and 19A).
When studying the specific impact of higher antibiotic consumption during the early stages of the COVID-19 pandemic on resistance patterns in serotypes, we observed changes in some of them between 2019 and 2020. This was of special relevance for certain serotypes such as 9V (unique to PCV20) and 11A (PCV20/PCV21) changing the consideration to penicillin by EUCAST from ‘susceptible with increased exposure’ in 2019 (MIC90; 2 mg/mL) to ‘resistant’ in 2020 (MIC90; 4 mg/mL) (Figure 6). This was also highlighted in the rise of the proportion of resistant strains to penicillin in 2020 for serotypes 9V and 11A, from 0% to 6.3% and from 4.5% to 26.2% respectively (Table 3).
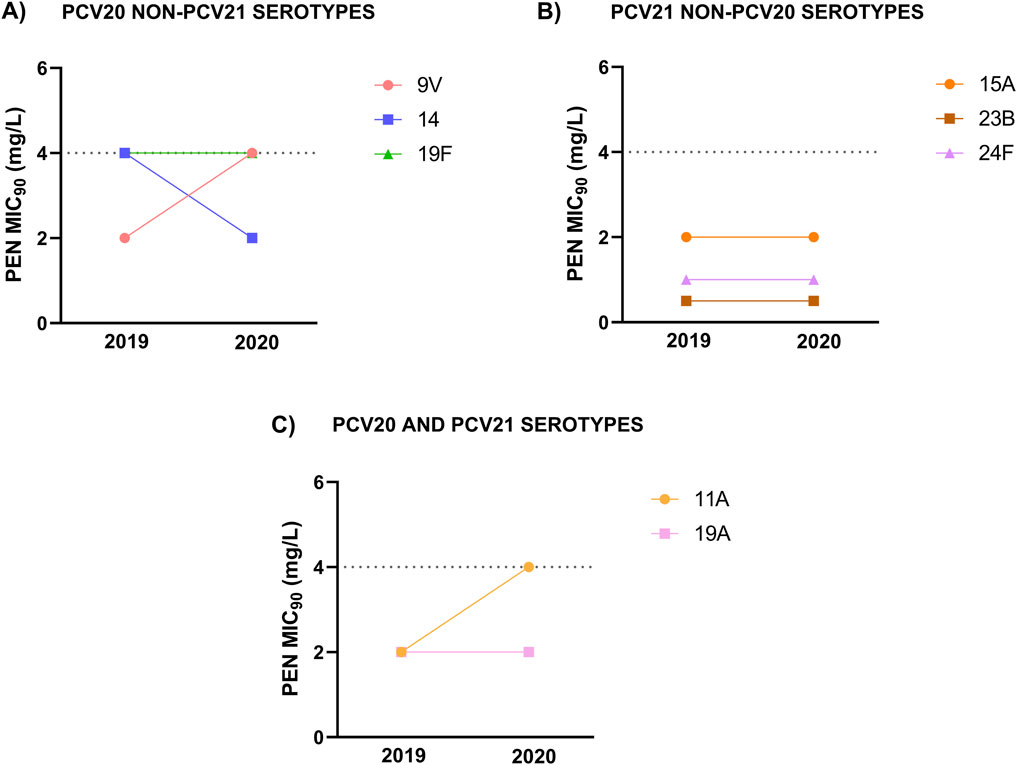
Figure 6. Penicillin MIC90 values in 2019 and 2020 for the different serotypes analyzed in the study. (A) Serotypes associated with non-susceptibility to penicillin included in PCV20 and not in PCV21. (B) Serotypes associated with non-susceptibility to penicillin included in PCV21 and not in PCV20. (C) Serotypes associated with non-susceptibility to penicillin included in both PCV20 and PCV21.
4 Discussion
A key breakthrough in combating pneumococcal disease was the development of antibiotic chemotherapy, which emerged in the 1930s and led to the discontinuation of serum therapy. Nevertheless, the effectiveness of antibiotic chemotherapy was soon threatened by the emergence of resistant clinical isolates, which appeared shortly after the widespread use of antibiotics (Spagnolo et al., 2021). The prevalence of antibiotic resistance in pneumococcus increased globally in the pre-PCV era, and despite the current use of vaccines with high coverage rates in pediatric population, the rise of serotypes associated with antibiotic resistance remains as a concerning phenomenon (Cassiolato et al., 2018; Sempere et al., 2022). Resistance patterns vary depending on serotype and geographic region, as several factors contribute to the emergence and spread of resistant isolates, including low vaccination rates specially in adult population, serotype replacement by non-vaccine serotypes, and inappropriate antibiotic use (Reinert, 2009; Song et al., 2012; Chávez et al., 2021). However, prophylactic strategies based on immunization appear to be the best approach for controlling the development of IPD and pneumonia, as well as reducing the impact of antibiotic resistance (Atkins et al., 2018).
Our results showed a rise in antibiotic resistance during the first year of the COVID-19 pandemic. During 2020, the generic use of antibiotics to avoid co-infections with bacterial pathogens was extended (Langford et al., 2021) and antibiotic sales correlated positively with COVID-19 cases globally (Nandi et al., 2023). Moreover, a recent United States study confirmed that AMR infections in hospitalized patients during the pandemic increased due to antibiotic exposure (Yek et al., 2025), which is in line with our observations. This makes antimicrobial stewardship essential, even in the context of a global health crisis (Langford et al., 2021), as inadequate use of antibiotics may exacerbate the antimicrobial resistance problem (Group, 2021).
In this study we showed that cefditoren was the β-lactam antibiotic with the highest proportion of susceptible isolates, achieving the lowest MIC50 and MIC90 values among all antibiotics tested, including other oral and intravenous cephalosporins. Since its introduction in 2004 and despite its widespread use in clinical practice, the emergence of non-susceptible isolates to this antibiotic has remained very low. In contrast, cefixime, cefpodoxime and cefuroxime, two third-generation and one second-generation oral cephalosporins, had the lowest proportion of susceptible isolates throughout the study period. It had already been demonstrated that cefditoren maintains good activity against penicillin-non-susceptible isolates due to its high affinity for PBP2x, enhancing its antimicrobial activity, which explains the consistently low and stable MIC50 and MIC90 values (0.5 and 1 μg/mL in most of the clinical isolates analyzed) (Yamada et al., 2007; Yang et al., 2012).
Lower respiratory tract infections (LRTIs) are associated with high morbidity and mortality rates worldwide. Before the COVID-19 pandemic, nearly 2.4 million deaths were caused by infections affecting the LRT being S. pneumoniae the major etiologic agent of these cases, affecting largely to high-risk groups such as the pediatric and elderly population (children under 5 years old and adults over 65 years old) (GBD, 2018). In this sense, our findings demonstrated that cefditoren as oral option and cefotaxime as iv choice, exhibited the highest antimicrobial activities regardless of the serotype or source of the clinical isolate. This is important from the LRTIs perspective as both cephalosporins are indicated for the treatment of community-acquired pneumonia (Granizo et al., 2006; Di Marco et al., 2014). We observed higher MIC values for iv cephalosporins and penicillins in non-invasive isolates than in invasive isolates (both with or without respiratory origin). Other studies have also described a higher proportion of resistance in non-invasive isolates compared with IPD isolates (Mohanty et al., 2023). Our results demonstrated that cefditoren maintained the same antimicrobial activity regardless of the source of the clinical isolate. Cefditoren can be used as oral treatment following parenteral administration of third-generation cephalosporins such as cefotaxime or ceftriaxone (Monmaturapoj et al., 2012). This is particularly relevant because early switching from intravenous to oral antibiotic therapy in patients with severe community-acquired pneumonia has been shown to be safe and to reduce hospitalization time (Mandell et al., 2007). It is also recommended by various organizations, including the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS). In this context, cefditoren has been recommended as the most suitable option for the early switch from intravenous third-generation cephalosporins to oral therapy, as it has a similar spectrum of activity but greater intrinsic efficacy (Blasi et al., 2016). This transition benefits not only patients but also healthcare systems by reducing hospitalization time and costs, as well as the risk of hospital-acquired infections—one of the major healthcare challenges today. This concept agrees with a recent study evaluating the hospital burden of pneumococcal disease in Spain showing that the annual cost of pneumococcal hospitalizations for the national health system exceeded EUR 383 million (Gil-Prieto et al., 2025).
Although the introduction of conjugate vaccines significantly reduced IPD cases caused by vaccine serotypes and helped control the spread of multidrug-resistant isolates, many countries have reported serotype replacement, including the emergence of multidrug-resistant serotypes (Cassiolato et al., 2018; Ladhani et al., 2018; de Miguel et al., 2021; Ouldali et al., 2021). Especially, serotypes associated with hypervirulent lineages, such as 11A and 24F, are of great concern (Aguinagalde et al., 2015; Lo et al., 2022). Recently, new conjugate vaccines PCV15 and PCV20 have been approved and introduced in Spain and PCV21 has been recently approved by FDA and EMA. This will be very useful from the public health perspective because the use of broader vaccines would increase the potential coverage against resistant isolates. For instance, PCV20 and PCV21 include serotype 11A, that showed high MIC90 values for most antibiotics tested, although cefditoren and cefotaxime still maintained a good antimicrobial activity profile against this serotype. Moreover, PCV21, a vaccine targeting specifically the adult population, has been just approved by FDA and EMA, and includes non-PCV20 serotypes such as 15A, 23B and 24F, and could be a potential candidate to ameliorate the emergence of these multidrug-resistant serotypes (Sempere et al., 2022). However, PCV21 excluded PCV20 serotypes such as 14, 19F and 9V that diminished after PCV13 introduction but are still an important cause of IPD in Spain (Pérez-García et al., 2024).
To summarize, we evaluated the evolution of antimicrobial resistance to different β-lactam antibiotics by comparing the years before and after the COVID-19 pandemic, in order to assess its impact on the antibiotic susceptibility of S. pneumoniae. The main limitations of the manuscript are the lack of results covering recent years although this will be address in future studies, and the lack of information on patients’ clinical characteristics.
Overall, we found that cefditoren as oral cephalosporin, and cefotaxime as iv option, are good candidates for the treatment of pneumococcal disease in Spain, even when it is associated with reduced susceptibility to β-lactams. Moreover, the high antimicrobial activity of cefditoren might reinforce its use as an oral option after pneumococcal hospitalization. From the prevention perspective, the use of higher valency conjugate vaccines in Spain might tackle the emergence of non-PCV13 serotypes associated with antibiotic resistance.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
Author contributions
ML: Writing – original draft, Methodology, Investigation, Writing – review and editing. CP-G: Writing – review and editing, Writing – original draft, Investigation, Methodology, Software. AÚ: Writing – review and editing, Investigation, Writing – original draft. EV: Writing – review and editing, Writing – original draft, Investigation. IP-C: Investigation, Writing – original draft, Writing – review and editing. EG-R: Writing – original draft, Writing – review and editing, Methodology, Conceptualization. PC: Methodology, Conceptualization, Writing – original draft, Writing – review and editing. JS: Investigation, Conceptualization, Writing – review and editing, Writing – original draft. MD: Methodology, Writing – original draft, Writing – review and editing, Supervision, Investigation. JS: Conceptualization, Writing – review and editing, Supervision, Formal Analysis, Writing – original draft, Data curation, Methodology. JY: Supervision, Conceptualization, Data curation, Writing – review and editing, Funding acquisition, Formal Analysis, Writing – original draft, Methodology.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This work was supported by the Spanish Ministry of Science and Innovation (grant PID 2020–119298RB-I00 and PID2024-161570OB-I00), by Instituto de Salud Carlos III (grant PI24CIII/00045), Meiji Pharma Spain (grant ES24PE03), and internal funding from Instituto de Salud Carlos III.
Conflict of interest
JY has received research grants from Merck Sharp & Dohme, Pfizer, and Meiji Pharma Spain. JY has received honoraria from Merck Sharp & Dohme, GSK and Pfizer for meeting presentations and financial support from Merck Sharp & Dohme and Pfizer to attend scientific meetings. JS has received honoraria from Merck Sharp & Dohme in advisory boards. MD has received financial support from Merck Sharp & Dohme to attend scientific meetings. EG-R and PC are members of staff of the Scientific Department of Meiji Pharma Spain.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Aguinagalde, L., Corsini, B., Domenech, A., Domenech, M., Camara, J., Ardanuy, C., et al. (2015). Emergence of amoxicillin-resistant variants of Spain9V-ST156 pneumococci expressing serotype 11A correlates with their ability to evade the host immune response. PLoS One 10 (9), e0137565. doi:10.1371/journal.pone.0137565
Atkins, K. E., Lafferty, E. I., Deeny, S. R., Davies, N. G., Robotham, J. V., and Jit, M. (2018). Use of mathematical modelling to assess the impact of vaccines on antibiotic resistance. Lancet Infect. Dis. 18 (6), e204–e213. doi:10.1016/s1473-3099(17)30478-4
Bajema, K. L., Gierke, R., Farley, M. M., Schaffner, W., Thomas, A., Reingold, A. L., et al. (2022). Impact of pneumococcal conjugate vaccines on antibiotic-nonsusceptible invasive pneumococcal disease in the United States. J. Infect. Dis. 226 (2), 342–351. doi:10.1093/infdis/jiac154
Bertran, M., D'Aeth, J. C., Abdullahi, F., Eletu, S., Andrews, N. J., Ramsay, M. E., et al. (2024). Invasive pneumococcal disease 3 years after introduction of a reduced 1 + 1 infant 13-valent pneumococcal conjugate vaccine immunisation schedule in England: a prospective national observational surveillance study. Lancet Infect. Dis. 24 (5), 546–556. doi:10.1016/s1473-3099(23)00706-5
Blasi, F., Page, C., Rossolini, G. M., Pallecchi, L., Matera, M. G., Rogliani, P., et al. (2016). The effect of N-acetylcysteine on biofilms: implications for the treatment of respiratory tract infections. Respir. Med. 117, 190–197. doi:10.1016/j.rmed.2016.06.015
Calvo-Silveria, S., Gonzalez-Diaz, A., Marimon, J. M., Cercenado, E., Quesada, M. D., Casabella, A., et al. (2025). Resilience and emergence of pneumococcal serotypes and lineages in adults post-PCV13 in Spain: a multicentre study. J. Infect. Public Health 18 (1), 102619. doi:10.1016/j.jiph.2024.102619
Cassiolato, A. P., Almeida, S. C. G., Andrade, A. L., Minamisava, R., and Brandileone, M. C. C. (2018). Expansion of the multidrug-resistant clonal complex 320 among invasive Streptococcus pneumoniae serotype 19A after the introduction of a ten-valent pneumococcal conjugate vaccine in Brazil. PLoS One 13 (11), e0208211. doi:10.1371/journal.pone.0208211
Chávez, A. F., Comas, L. G., Moreno, J. C. S., Moreno, R. C., de Provens, O. C. P., and Andrés, J. M. A. (2021). Effect of childhood pneumococcal vaccination and beta-lactam antibiotic use on the incidence of invasive pneumococcal disease in the adult population. Eur. J. Clin. Microbiol. Infect. Dis. 40 (7), 1529–1538. doi:10.1007/s10096-021-04196-4
de Miguel, S., Domenech, M., González-Camacho, F., Sempere, J., Vicioso, D., Sanz, J. C., et al. (2021). Nationwide Trends of invasive pneumococcal disease in Spain from 2009 through 2019 in Children and adults during the pneumococcal conjugate vaccine era. Clin. Infect. Dis. 73 (11), e3778–e3787. doi:10.1093/cid/ciaa1483
Di Marco, F., Braido, F., Santus, P., Scichilone, N., and Blasi, F. (2014). The role of cefditoren in the treatment of lower community-acquired respiratory tract infections (LRTIs): from bacterial eradication to reduced lung inflammation and epithelial damage. Eur. Rev. Med. Pharmacol. Sci. 18 (3), 321–332.
Domenech, M., García, E., and Moscoso, M. (2012). Biofilm formation in Streptococcus pneumoniae. Microb. Biotechnol. 5 (4), 455–465. doi:10.1111/j.1751-7915.2011.00294.x
Fenoll, A., Granizo, J. J., Giménez, M. J., Yuste, J., and Aguilar, L. (2015). Secular trends (1990-2013) in serotypes and associated non-susceptibility of S. pneumoniae isolates causing invasive disease in the pre-/post-era of pneumococcal conjugate vaccines in Spanish regions without universal paediatric pneumococcal vaccination. Vaccine 33 (42), 5691–5699. doi:10.1016/j.vaccine.2015.08.009
GBD (2018). Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect. Dis. 18 (11), 1191–1210. doi:10.1016/s1473-3099(18)30310-4
Gil-Prieto, R., Hernandez-Barrera, V., Marín-García, P., González-Escalada, A., and Gil-de-Miguel, Á. (2025). Hospital burden of pneumococcal disease in Spain (2016-2022): a retrospective study. Hum. Vaccin Immunother. 21 (1), 2437915. doi:10.1080/21645515.2024.2437915
González-Díaz, A., Machado, M. P., Càmara, J., Yuste, J., Varon, E., Domenech, M., et al. (2020). Two multi-fragment recombination events resulted in the β-lactam-resistant serotype 11A-ST6521 related to Spain9V-ST156 pneumococcal clone spreading in south-western Europe, 2008 to 2016. Eurosurveillance 25 (16), 1900457. doi:10.2807/1560-7917.Es.2020.25.16.1900457
Granizo, J. J., Giménez, M. J., Barberán, J., Coronel, P., Gimeno, M., and Aguilar, L. (2006). The efficacy of cefditoren pivoxil in the treatment of lower respiratory tract infections, with a focus on the per-pathogen bacteriologic response in infections caused by Streptococcus pneumoniae and Haemophilus influenzae: a pooled analysis of seven clinical trials. Clin. Ther. 28 (12), 2061–2069. doi:10.1016/j.clinthera.2006.12.010
Group, P. T. C. (2021). Azithromycin for community treatment of suspected COVID-19 in people at increased risk of an adverse clinical course in the UK (PRINCIPLE): a randomised, controlled, open-label, adaptive platform trial. Lancet 397 (10279), 1063–1074. doi:10.1016/S0140-6736(21)00461-X
Kyd, J. M., McGrath, J., and Krishnamurthy, A. (2011). Mechanisms of bacterial resistance to antibiotics in infections of COPD patients. Curr. Drug Targets 12 (4), 521–530. doi:10.2174/138945011794751519
Ladhani, S. N., Collins, S., Djennad, A., Sheppard, C. L., Borrow, R., Fry, N. K., et al. (2018). Rapid increase in non-vaccine serotypes causing invasive pneumococcal disease in England and Wales, 2000-17: a prospective national observational cohort study. Lancet Infect. Dis. 18 (4), 441–451. doi:10.1016/s1473-3099(18)30052-5
Langford, B. J., So, M., Raybardhan, S., Leung, V., Soucy, J. R., Westwood, D., et al. (2021). Antibiotic prescribing in patients with COVID-19: rapid review and meta-analysis. Clin. Microbiol. Infect. 27 (4), 520–531. doi:10.1016/j.cmi.2020.12.018
Lo, S. W., Mellor, K., Cohen, R., Alonso, A. R., Belman, S., Kumar, N., et al. (2022). Emergence of a multidrug-resistant and virulent Streptococcus pneumoniae lineage mediates serotype replacement after PCV13: an international whole-genome sequencing study. Lancet Microb. 3 (10), e735–e743. doi:10.1016/s2666-5247(22)00158-6
Mandell, L. A., Wunderink, R. G., Anzueto, A., Bartlett, J. G., Campbell, G. D., Dean, N. C., et al. (2007). Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 44 Suppl 2 (Suppl. 2), S27–S72. doi:10.1086/511159
Meschiari, M., Onorato, L., Bacca, E., Orlando, G., Menozzi, M., Franceschini, E., et al. (2022). Long-term impact of the COVID-19 pandemic on in-hospital antibiotic consumption and antibiotic resistance: a time series analysis (2015-2021). Antibiotics 11 (6), 826. doi:10.3390/antibiotics11060826
Mohanty, S., Feemster, K., Yu, K. C., Watts, J. A., and Gupta, V. (2023). Trends in Streptococcus pneumoniae antimicrobial resistance in US children: a multicenter evaluation. Open Forum Infect. Dis. 10 (3), ofad098. doi:10.1093/ofid/ofad098
Monmaturapoj, T., Montakantikul, P., Mootsikapun, P., and Tragulpiankit, P. (2012). A prospective, randomized, double dummy, placebo-controlled trial of oral cefditoren pivoxil 400mg once daily as switch therapy after intravenous ceftriaxone in the treatment of acute pyelonephritis. Int. J. Infect. Dis. 16 (12), e843–e849. doi:10.1016/j.ijid.2012.07.009
Nandi, A., Pecetta, S., and Bloom, D. E. (2023). Global antibiotic use during the COVID-19 pandemic: analysis of pharmaceutical sales data from 71 countries, 2020-2022. EClinicalMedicine 57, 101848. doi:10.1016/j.eclinm.2023.101848
Ouldali, N., Varon, E., Levy, C., Angoulvant, F., Georges, S., Ploy, M. C., et al. (2021). Invasive pneumococcal disease incidence in children and adults in France during the pneumococcal conjugate vaccine era: an interrupted time-series analysis of data from a 17-year national prospective surveillance study. Lancet Infect. Dis. 21 (1), 137–147. doi:10.1016/s1473-3099(20)30165-1
Pérez-García, C., Sempere, J., de Miguel, S., Hita, S., Úbeda, A., Vidal, E. J., et al. (2024). Surveillance of invasive pneumococcal disease in Spain exploring the impact of the COVID-19 pandemic (2019-2023). J. Infect. 89, 106204. doi:10.1016/j.jinf.2024.106204
Pérez-García, C., González-Díaz, A., Domenech, M., Llamosí, M., Úbeda, A., Sanz, J. C., et al. (2025). The rise of serotype 8 is associated with lineages and mutations in the capsular operon with different potential to produce invasive pneumococcal disease. Emerg. Microbes Infect. 14, 2521845. doi:10.1080/22221751.2025.2521845
Reinert, R. R. (2009). The antimicrobial resistance profile of Streptococcus pneumoniae. Clin. Microbiol. Infect. 15 (Suppl. 3), 7–11. doi:10.1111/j.1469-0691.2009.02724.x
Sempere, J., Llamosí, M., López Ruiz, B., Del Río, I., Pérez-García, C., Lago, D., et al. (2022). Effect of pneumococcal conjugate vaccines and SARS-CoV-2 on antimicrobial resistance and the emergence of Streptococcus pneumoniae serotypes with reduced susceptibility in Spain, 2004-20: a national surveillance study. Lancet Microbe 3, e744–e752. doi:10.1016/s2666-5247(22)00127-6
Sempere, J., Yuste, J., and Domenech, M. (2024). PCV13 vaccine prevents pneumococcal biofilms without affecting Staphylococcus aureus population within the polymicrobial biofilm. Front. Immunol. 15, 1495932. doi:10.3389/fimmu.2024.1495932
Singh, C. K., and Sodhi, K. K. (2023). Antimicrobial resistance in the time of COVID-19. Appl. Microbiol. 3 (4), 1388–1391. doi:10.3390/applmicrobiol3040093
Singh, C. K, and Sodhi, K. K. (2024). Targeting bioinformatics tools to study the dissemination and spread of antibiotic resistant genes in the environment and clinical settings. Crit. Rev. Microbiol. 51, 860–878. doi:10.1080/1040841X.2024.2429603
Song, J. H., Dagan, R., Klugman, K. P., and Fritzell, B. (2012). The relationship between pneumococcal serotypes and antibiotic resistance. Vaccine 30 (17), 2728–2737. doi:10.1016/j.vaccine.2012.01.091
Spagnolo, F., Trujillo, M., and Dennehy, J. J. (2021). Why do antibiotics exist? mBio 12 (6), e0196621. doi:10.1128/mBio.01966-21
Yamada, M., Watanabe, T., Miyara, T., Baba, N., Saito, J., Takeuchi, Y., et al. (2007). Crystal structure of cefditoren complexed with Streptococcus pneumoniae penicillin-binding protein 2X: structural basis for its high antimicrobial activity. Antimicrob. Agents Chemother. 51 (11), 3902–3907. doi:10.1128/aac.00743-07
Yang, Q., Xu, Y., Chen, M., Wang, H., Sun, H., Hu, Y., et al. (2012). In vitro activity of cefditoren and other comparators against Streptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis causing community-acquired respiratory tract infections in China. Diagn Microbiol. Infect. Dis. 73 (2), 187–191. doi:10.1016/j.diagmicrobio.2012.03.005
Yek, C., Mancera, A. G., Diao, G., Walker, M., Neupane, M., Chishti, E. A., et al. (2025). Impact of the COVID-19 pandemic on antibiotic resistant infection burden in U.S. Hospitals: retrospective cohort study of trends and risk factors. Ann. Intern Med. 178 (6), 796–807. doi:10.7326/ANNALS-24-03078
Keywords: AMR, PCV21, PCV20, serotype 11A, serotype 19A, serotype 24F, serotype 14, serotype 9V
Citation: Llamosí M, Pérez-García C, Úbeda A, Vidal-Alcántara EJ, Pareja-Cerbán I, Gómez-Rubio E, Coronel P, Sanz JC, Domenech M, Sempere J and Yuste J (2025) Antimicrobial activity of β-lactam antibiotics against pneumococcal isolates causing pneumococcal disease in adults immediately before and after the COVID-19 pandemic in Spain (2019–2020). Front. Pharmacol. 16:1658431. doi: 10.3389/fphar.2025.1658431
Received: 02 July 2025; Accepted: 15 September 2025;
Published: 30 September 2025.
Edited by:
Chao Huang, Chongqing University, ChinaReviewed by:
Kushneet Kaur Sodhi, University of Delhi, IndiaZiyi Yan, Sichuan University, China
LiangJing Xin, Chongqing Medical University, China
Copyright © 2025 Llamosí, Pérez-García, Úbeda, Vidal-Alcántara, Pareja-Cerbán, Gómez-Rubio, Coronel, Sanz, Domenech, Sempere and Yuste. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julio Sempere, anNlbXBlcmVAaXNjaWlpLmVz; Jose Yuste, anl1c3RlQGlzY2lpaS5lcw==
†These authors have contributed equally to this work