 Carlos Cordero-García1*
Carlos Cordero-García1* Judith Sánchez-Raya2Tamara L. Rodríguez-Araya3María Dolores López-Alarcón4Eva Trillo-Calvo5
Judith Sánchez-Raya2Tamara L. Rodríguez-Araya3María Dolores López-Alarcón4Eva Trillo-Calvo5 Jerónimo Balsalobre-Aznar6
Jerónimo Balsalobre-Aznar6 Maria Pérez-Páramo7
Maria Pérez-Páramo7- 1Department of Physical Medicine and Rehabilitation, Hospital Universitario Juan Ramón Jiménez, Huelva, Spain
- 2Physical Medicine and Rehabilitation Department, Hospital Universitari Vall d'Hebron, Barcelona, Spain
- 3Rheumatology Service, Hospital Clinic, Barcelona, Spain
- 4Pain Unit, General University Hospital of Valencia, Valencia, Spain
- 5Primary Care, Aragon Institute for Health Research (IIS Aragón), Primary Care Center Campo de Belchite, Zaragoza, Spain
- 6Rheumatology Service, Hospiten, Santa Cruz de Tenerife, Spain
- 7Medical Department, Viatris, Madrid, Spain
Introduction: Low back pain (LBP) is one of the most prevalent chronic pain conditions that affects nearly 50% of the population. Its complex pathophysiology may involve both nociceptive and neuropathic mechanisms and is often resistant to standard treatment. Pregabalin has emerged as a potential alternative owing to its mechanism of action, the inhibition of excitatory neurotransmitter release. This meta-analysis aimed to evaluate the efficacy and safety of pregabalin in managing LBP.
Methods: A systematic review of three major databases was conducted following the PRISMA guidelines. Studies were included if they were comparative studies of pregabalin with placebo or other pain medications, focusing on adult patients with LBP. Data were extracted on efficacy outcomes including pain reduction, anxiety, depression, quality of life, quality of sleep, disability, and adverse events. Statistical analysis was performed using Review Manager 5.4.1.
Results: A total of 18 studies (n = 5,000) were included. Pregabalin demonstrated significant pain reduction at 4 weeks (Standardized Mean Difference (SMD) = −0.64, 95% Confidence Interval (CI) = −1.09 to −0.20), 6 weeks (SMD = −0.72, 95% CI = −1.15 to −0.29), and 8 weeks (SMD = −0.50, 95% CI = −0.71 to −0.29) compared to control group. Pregabalin also showed a significant greater improvement in anxiety (Mean Difference (MD) = −1.38, 95% CI = −1.74 to −1.02, p < 0.00001), depression (MD = −1.40, 95% CI = −1.71 to −1.08, p < 0.00001), quality of life (SMD = 0.22, 95% CI = 0.07 to 0.37, p = 0.003) and sleep quality (SMD = −0.61, 95% CI = −0.87 to −0.36, p < 0.00001). There were no significant differences regarding disability and adverse events.
Conclusion: Pregabalin in the treatment of neuropathic LBP demonstrated significant improvements in pain relief, associated symptoms of anxiety and depression, and enhancements in quality of life and sleep quality. In addition, it exhibits a favorable safety profile. Nevertheless, these findings should be interpreted with caution due to the limited quality of the evidence and the inadequate reporting of pain etiology in several included studies.
1 Introduction
Low back pain (LBP) is one of the most prevalent pain conditions and a leading cause of disability worldwide. Its complex pathophysiology may involve both nociceptive and neuropathic mechanisms, contributing to the heterogeneous nature of the condition. In 2020, LBP affected 619 million (95% uncertainty interval 554–694) people globally (GBD, 2021 Low Back Pain Collaborators, 2023).
In LBP, nociceptive pain results from activation of nociceptors that innervate ligaments, joints, muscles, fascia and tendons as a response to tissue injury or inflammation and biomechanical stress. Neuropathic back pain describes pain arising from injury or disease directly affecting the nerve roots that innervate the spine and lower limbs, and pathological invasive innervation of the damaged lumbar discs. Chronic LBP is increasingly considered to be a mixed pain syndrome consisting of both nociceptive and neuropathic components, and it has been suggested that neuropathic components in chronic LBP may be under-recognized and therefore undertreated (Baron et al., 2016).
This mixed pain condition is notoriously difficult to manage and resistant to treatments (Ghazisaeidi et al., 2023; Sharma and McAuley, 2022; Mák et al., 2021). Pain is also associated with a significant decline in quality of life and leads to both direct and indirect costs (Ghazisaeidi et al., 2023; Sharma and McAuley, 2022; Mák et al., 2021; Shetty et al., 2022). Studies suggest that nearly a quarter of individuals with LBP suffer from psychiatric comorbidities, such as depression and anxiety, which has led to advocate for psychiatric screenings in these patients (Dickson et al., 2023; Hu et al., 2022). Furthermore, the indirect costs of managing lumbar pain can reach up to 68% of total costs (Morera-Domínguez et al., 2010). Pharmacy costs alone may account for as much as 13% of the total expenses related to this condition while the cost of physical therapy account for up to 17% (Dagenais et al., 2008). Additionally, all the costs incurred, such as those resulting from reduced productivity at work, are significant, because LBP is the leading cause of disability in the United States and the main reason for absenteeism (Areias et al., 2023).
Current treatments for lower back pain, such as NSAIDs and opioids, often have significant drawbacks. NSAIDs, for instance, are associated with considerable health risks, including gastrointestinal toxicity, which can impose a substantial economic burden (Kikuchi et al., 2021). The majority of guidelines for the treatment of low back pain recommend paracetamol as the first-line option, with NSAIDs (that are readily accessible in various types and brands, both over-the-counter and by prescription) as a subsequent choice if paracetamol proves inadequate. While most NSAIDs are taken in oral preparations, topical formulations are also available to avoid systemic side effects, particularly in patients with allergies to specific medications, gastroesophageal reflux disease, and cardiac disease (Enthoven et al., 2016; Wang and Doan, 2024).
In addition, a Cochrane review noted by Cashin et al. (2023) found that opioids can lead to adverse events like nausea, headaches, constipation, and dizziness, which can severely affect a patient’s quality of life. The rapid escalation of the opioid epidemic reveals critical issues like addiction and dependency, complicating long-term treatment and management. This situation underscores the urgent need for alternative strategies to address these challenges effectively (Damiescu et al., 2021).
Although recent national guidelines have offered conflicting recommendations on the role of opioids in treating chronic LBP, opioids remain widely used in both Europe and North America. The prolonged use of opioids for chronic non-cancer pain has played a significant part in the opioid crisis in North America, contributing to a rise in opioid prescriptions, non-medical use, and the associated increase in mortality rates (Petzke et al., 2020). The guidelines from the European Medicines Agency and the American CDC highlight the need to assess physical dependence, abuse, and addiction in opioid trials, but these outcomes were not analyzed in the most systematic reviews for chronic LBP (Petzke et al., 2020).
For all these reasons, the need arose to seek more treatments that could be incorporated into clinical guidelines. Pregabalin emerges as treatment for neuropathic lumbar pain due to its ability to selectively bind to the α2-δ subunit of voltage-dependent calcium channels, inhibiting calcium influx, reducing excitatory neurotransmitter release and, as a consequence, reducing nerve impulse and pain sense (Taylor et al., 2007). This molecular action decreases pain signal transmission, alleviates symptoms, and enhances functionality, thus highlighting its potential in the management of LBP (Taylor et al., 2007).
Original studies on the pharmacological management of low back pain revealed mixed effectiveness across treatments. Robertson et al. (2019) favour gabapentin (GBP) for its minimal adverse effects and significant pain relief, whereas Sakai et al. (2015) and Mathieson et al. (2017) found no substantial benefits of pregabalin over opioids or placebo, respectively. Park et al. (2024) suggest that the choice between pregabalin and limaprost should be tailored to the individual, while Kalita et al. (2014) highlights amitriptyline’s superior functionality improvement.
Contrarily, Gammoh et al. (2021) report pregabalin as more effective than GBP, Romanò et al. (2009) see added benefits with pregabalin combined with celecoxib but only in cases where both nociceptive and neuropathic elements were present, and Saldaña et al. (2010a) note its cost-effectiveness in clinical practice.
Some previous meta-analyses, as noted by Wewege et al. (2023), did not specifically focus on pregabalin but considered a wider array of medications, complicating the isolation of variables that could influence outcomes. Another meta-analysis by Giménez-Campos et al. (2022) included only three randomised controlled trials (RCTs) for pregabalin, and they did not account for dosage, controls, and other confounding variables. Baron et al. (2010) concluded that “further work” was required to understand the potential of pregabalin in treating LBP. These insights underscore the necessity for a new meta-analysis aimed at objectively assessing the therapeutic value of pregabalin, addressing the gaps identified in earlier studies.
This meta-analysis addresses gaps by providing an up-to-date, focused synthesis of studies that evaluate both the efficacy and safety of pregabalin specifically in non-surgical LBP. Through rigorous inclusion criteria and the integration of recent data, this work aims to comprehensively assess the efficacy and safety of pregabalin in the management of LBP, addressing gaps in current research and providing clear, evidence-based insights to guide clinical practice.
2 Materials and methods
2.1 Eligibility criteria
The study protocol has been registered with PROSPERO (CRD42025642429) and follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Page et al., 2021). PICOS strategy was used as follows: Patients (P): adult patients diagnosed with low back pain, radiculopathy, or spinal stenosis, the Intervention (I) under scrutiny was the administration of pregabalin, which was Compared (C) against placebos or alternative pain medications; the primary Outcomes (O) assessed were the efficacy and safety of the treatments and the analysis was strictly confined to data extracted from Studies (S) that were comparative studies.
The exclusion criteria were rigorously applied as follows: duplicates were excluded to prevent data redundancy and potential analytical bias. The focus on adult populations led to the exclusion of non-adult studies, ensuring consistency in pharmacological responses and treatment effects. Studies involving patients who received surgery were also excluded. Additionally, studies with incomplete or missing data, or those that failed to report on all relevant variables, were excluded to enhance the robustness and accuracy of the statistical analysis.
2.2 Information sources and search methods for identification of studies
The literature search was conducted on December 2024 across PubMed, Scopus, and the Cochrane Library without restrictions on publication date or language. The search strategy employed keywords such as “Pregabalin,” “Lyrica,” “low backache,” “radiculopathy,” “spinal stenosis,” “neurogenic claudication,” “sciatica,” “low back pain,” “lumbalgia,” “lumbar,” and “spine,” detailed further in Supplementary File S1. Additionally, a manual search of references was performed to ensure comprehensive coverage. Two reviewers independently screened the studies, and any discrepancies or disagreements were resolved by involving a third reviewer.
2.3 Data extraction and data items
Data extraction was carried out by two reviewers, with any disagreements resolved by a third reviewer. They meticulously gathered baseline characteristics, including study details, region, period, type of study, follow-up duration, patient count, age, number of females, patient demographics, and detailed intervention information. Treatment regimens and dosages were also extensively documented. The primary outcomes measured included pain, assessed using the Visual Analogue Scale (VAS) for back and leg pain, Brief Pain Inventory and Pain Rating Index; anxiety and depression, evaluated with the Hospital Anxiety and Depression Scale (HADS); disability, assessed by the Oswestry Disability Index (ODI), Roland-Morris Disability Questionnaire, and Sheehan Disability Inventory; sleep disturbances, measured using the Daily Sleep Interference Scale, Insomnia Severity Index (ISI), Medical Outcomes Study Sleep Scale (MOS), and Pain-Related Sleep Interference Scale (PRSIS); and quality of life, evaluated using the EuroQol-5 Dimension (EQ-5D) health status index and the Short Form-12 (SF-12). Adverse events and costs were also systematically recorded.
2.4 Assessment of risk of bias in included studies
The assessment of the risk of bias was conducted using the Cochrane Collaboration’s tool (RoB 2) and implemented through Review Manager software (RevMan, version 5.4.1, The Cochrane Collaboration, London, United Kingdom) for studies that were RCTs. This analysis encompassed six domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting. Each study was evaluated for these criteria and categorized as having a low, high, or unclear risk of bias based on how well they addressed these key aspects of trial integrity.
The methodological quality of the comparative studies that were non-RCTs were independently evaluated by two reviewers using the Methodological Index for Non-Randomized Studies (MINORS) criteria (Slim et al., 2003). This instrument contains items to evaluate key methodological aspects such as study design, patient selection, outcome measures, and follow-up. Scoring ranges from 0 to 24 for comparative designs. Comparative studies scoring 0–6 will be deemed very low-quality, 7–10 as low quality, 11–15 as fair quality, and 16–24 as high quality. Any discrepancies in the quality assessment scoring between the two reviewers were discussed to reach a consensus.
2.5 Assessment of results
The statistical analyzes were conducted using RevMan version 5.4.1 Dichotomous variables were analyzed using odds ratios (ORs) with 95% confidence intervals (CIs), while continuous variables were assessed through mean differences (MDs) and 95% CIs. For continuous variables with non-compatible units or scales, standardized mean differences (SMDs) and 95% CIs were calculated. In this meta-analysis, positive or negative values of MD and SMD were used to indicate the direction of effect, depending on whether the outcome favored the intervention (pregabalin) or the control. A negative value indicates an effect in favor of pregabalin when lower scores are associated with better outcomes, while positive values reflect outcomes favoring the control or indicating increased values in the pregabalin group. Heterogeneity among study results was evaluated using the chi-square statistic and the I2 test, with I2 values ranging from 0% to 100% indicating low, moderate, and high heterogeneity at values of 25%, 50%, and 75%, respectively (Lorente et al., 2024). A fixed-effects model was applied in cases of no significant heterogeneity, and a random-effects model was used when heterogeneity was substantial (I2 ≥ 50%). For extracting data from figures, WebPlotDigitizer version 4.5 (Automeris, Pacifica, California, United States) was employed. Any missing data were addressed following guidelines from the Cochrane Handbook, ensuring a rigorous and methodical approach to data synthesis and interpretation (Higgins et al., 2019).
2.6 Publication bias
The assessment of publication bias in the analysis was conducted using Review Manager version 5.4.1 software. To detect any asymmetry indicative of bias, funnel plots were generated and subjected to careful visual inspection. This method involves plotting the treatment effects from individual studies against a measure of study size or precision, allowing for the identification of any systematic deviations from the expected distribution.
2.7 Additional analyses
Subgroup analyzes were conducted when the dataset included a sufficient and statistically robust number of studies, ensuring the reliability of the findings. These analyzes included assessments based on different follow-up periods: 2, 4, 6, 8, and more than 8 weeks. Additionally, a subgroup of patients treated with pregabalin plus another intervention was examined to assess the combined effect of pregabalin separately.
Sensitivity analyzes were conducted by excluding the study with the greatest weight to test the robustness of the results.
The certainty of the results was evaluated using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework in GRADEpro, which considers study design, risk of bias, inconsistency, indirectness, imprecision, and publication bias (Guyatt et al., 2013).
3 Results
3.1 Study selection
The initial search in the databases yielded 959 studies. After adjusting for duplicates and clinical trials, 870 studies were excluded, leaving 89 studies. Upon reviewing the titles and abstracts, 60 studies were excluded for the following reasons: they did not include pregabalin, they involved pregabalin in both groups without a distinct control group, they were not studies on humans, they did not focus on low back pain, they included surgical patients, or they lacked efficacy and/or safety data. After a full-text review of the remaining studies, 11 were further excluded due to missing data, non-comparable data, or inconsistent variables, resulting in a total of 18 studies eligible for inclusion. A manual review of the references from these studies did not yield any additional studies to include. Ultimately, 18 studies were included in the meta-analysis (Figure 1; Table 1) (Morera-Domínguez et al., 2010; Robertson et al., 2019; Sakai et al., 2015; Mathieson et al., 2017; Park et al., 2024; Kalita et al., 2014; Gammoh et al., 2021; Romanò et al., 2009; Saldaña et al., 2010a; Baron et al., 2010; Baron et al., 2014; Chye et al., 2021; Kim et al., 2016; Markman et al., 2015; Pota et al., 2012; Saldaña et al., 2010b; Sicras-Mainar et al., 2013; Taguchi et al., 2015; Yeole et al., 2022).
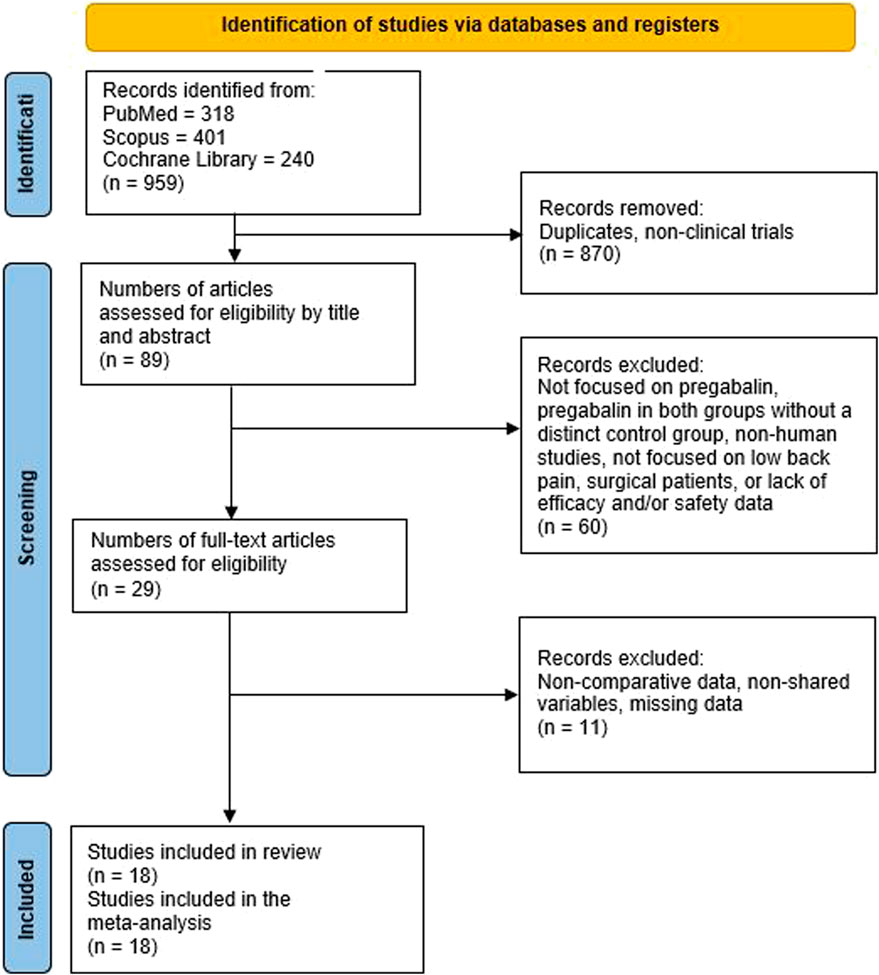
Figure 1. PRISMA flowchart illustrating the study selection process for the systematic review and meta-analysis.
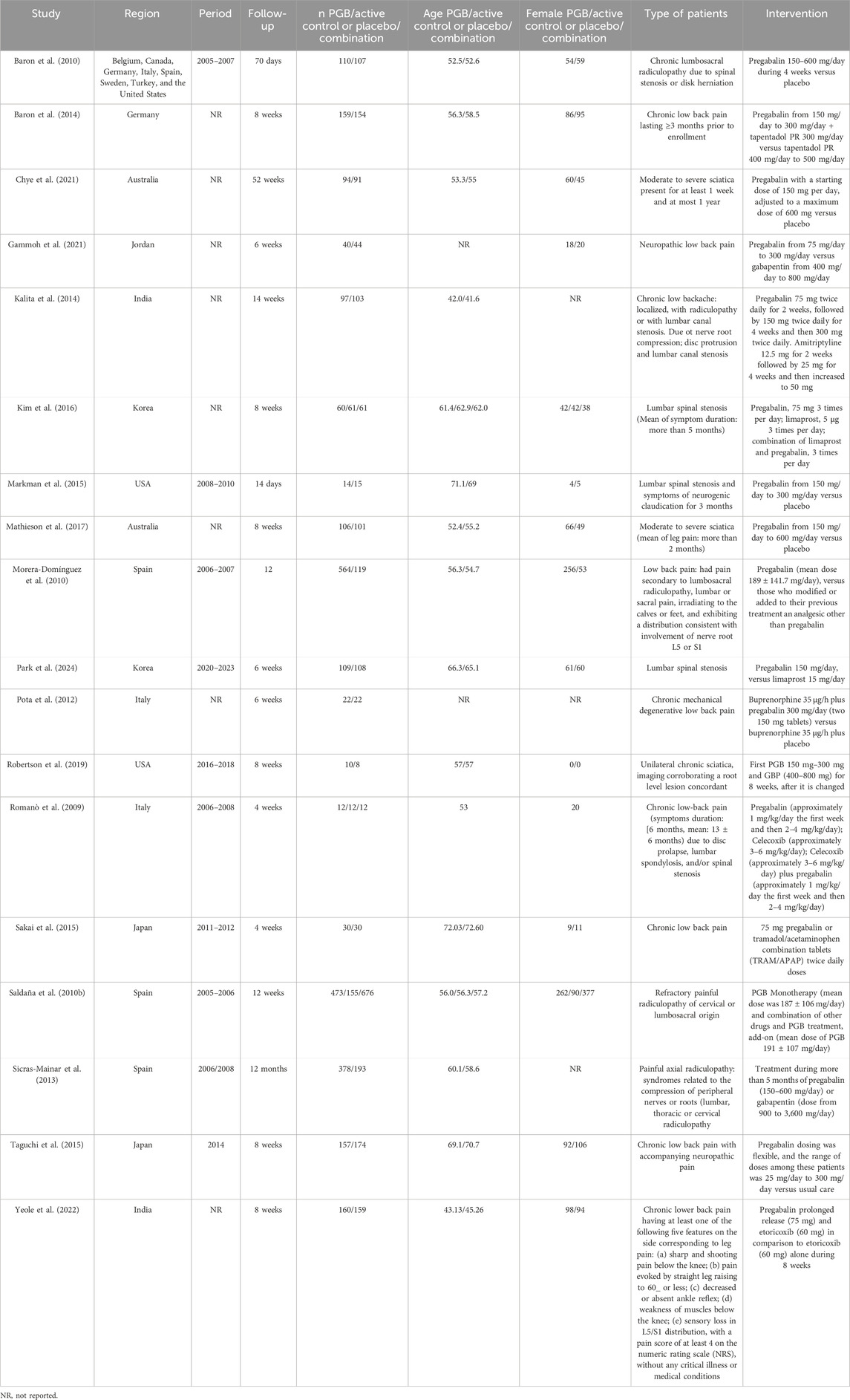
Table 1. Baseline characteristics of the included studies.
3.2 Risk of bias
The overall and individualized risks of bias for the included RCTs studies are shown in Figure 2. These studies demonstrated a low risk of bias regarding reporting bias and random sequence generation. There was a moderate risk of bias for incomplete outcome data, allocation concealment and patient and personnel blinding and high risk of bias of blinding of outcome assessment.
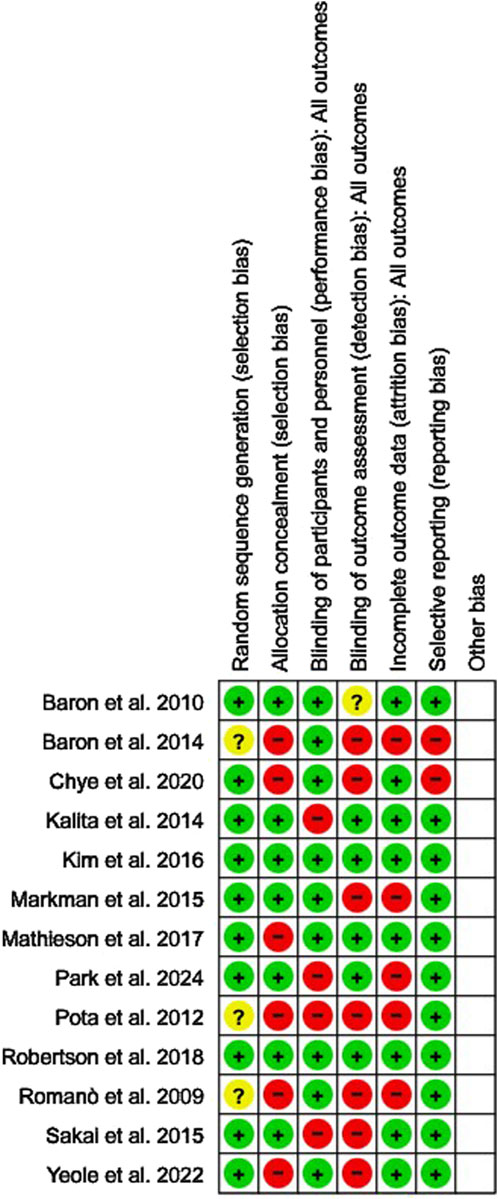
Figure 2. Risk of bias assessment of randomized controlled trials (RCTs) included in the meta-analysis, conducted using the Cochrane Collaboration’s RoB 2 tool.
The quality of the included non-RCT studies, as assessed by the MINORS tool and deemed to have high quality, is shown in Supplementary Table S1.
3.3 Study characteristics
Table 1 presents the basic characteristics of the studies included. Eighteen studies and 5,000 patients were included. Most of the studies were from Europe and Asia (seven studies each). The mean age ranged from 42.0 to 72.6 years in the pregabalin group. The number of female participants, the type of patients and interventions are presented in Table 1. The therapeutic regimens are shown in Supplementary Table S2.
3.4 Outcomes
3.4.1 Pain assessment
LBP assessed and VAS scale was studied according to different follow-up times (Figure 3). Attending the shortest follow-up time, at 2 weeks, pregabalin or combination with pregabalin (tapentadol or other combination) did not show better results in reducing pain intensity when it is compared to active control group (diphenhydramine, tapentadol, tramadol/acetaminophen or other drug combination) (SMD = −0.03, 95% CI = −0.34 to 0.28, participants = 1,842, studies = 4, I2 = 80%; p = 0.85). However, pregabalin or combination with pregabalin (combination with tapentadol or buprenorphine, etoricoxib, celecoxib, among others) significantly improved pain level at 4 weeks of follow-up when it is compared to active controls (tapentadol, tramadol/acetaminophen, buprenorphine, etoricoxib, celecoxib, other drug combination or usual care treatment) (SMD = −0.64, 95% CI = −1.09 to −0.20, participants = 2,619, studies = 7, I2 = 95%, p = 0.005). Similar results were obtained when pregabalin or combination with pregabalin (combination with tapentadol or buprenorphine, mainly) were analyzed versus other interventions at 6 weeks (SMD = −0.72, 95% CI = −1.15 to −0.29, participants = 2,284, studies = 6, I2 = 94%, p = 0.001) and 8 weeks (SMD = −0.50, 95% CI = −0.71 to −0.29, participants = 2,284, studies = 6, I2 = 80%, p = 0.0005) Three studies analyzed pain level at follow-up times of more than 8 weeks. Morera-Domínguez et al. (2010) and Saldaña et al. (2010b) performed the analysis at 12 weeks of follow-up and Kalita et al. (2014) at 14 weeks from the start of intervention. In this case, there were no significant differences from active controls (SMD = −0.25, 95% CI = −0.66 to 0.16, participants = 2,289, studies = 3, I2 = 93%, p = 0.23).
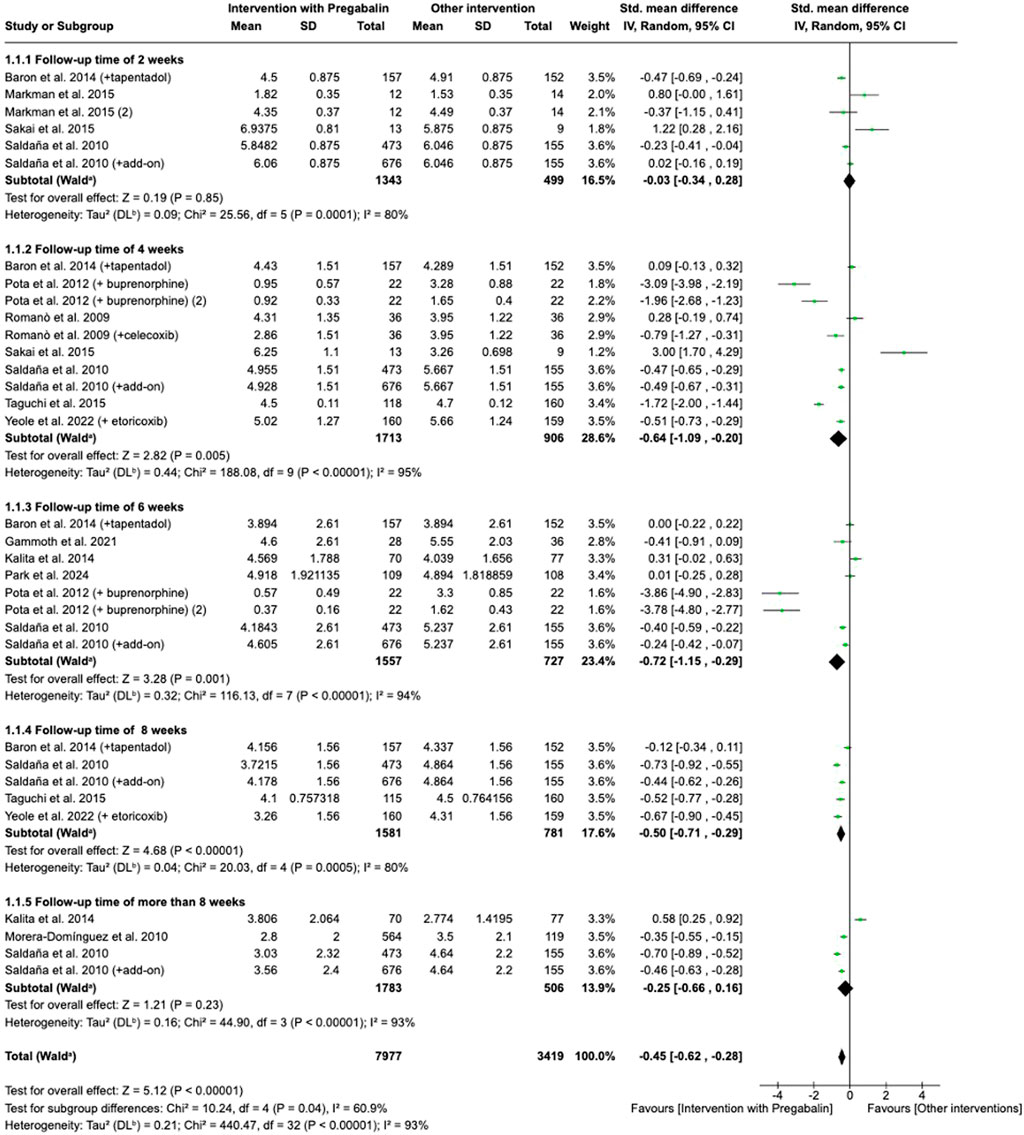
Figure 3. Forest plot of standardized mean differences (SMDs) for back pain intensity (Visual Analogue Scale) comparing pregabalin versus control interventions across follow-up periods: 2 weeks; 4 weeks; 6 weeks; 8 weeks; and >8 weeks. Squares represent study-specific effect sizes (SMD), with horizontal lines indicating 95% confidence intervals. Study of Saldaña et al. (2010a) refers to Saldaña et al. (2010b).
Four studies analyzed effects of pregabalin on leg pain through VAS scale (Robertson et al., 2019; Mathieson et al., 2017; Park et al., 2024; Chye et al., 2021). When effect of pregabalin or combination with pregabalin was compared to alternative on leg pain, there were no significant differences (MD = 0.08, 95% CI = −0.17 to 0.33, participants = 624, studies = 4, I2 = 53%, p = 0.54).
3.4.2 Anxiety and depression
Hospital Anxiety and Depression Scale (HADS) were used to analyze anxiety and depression by the authors. An intervention with pregabalin showed an improvement of anxiety levels at different endpoints of follow-up compared to active control group (placebo, other analgesic than pregabalin, tapentadol) (MD = −1.38, 95% CI = −1.74 to −1.02, participants = 2,650, studies = 3, I2 = 25%, p < 0.00001) (Figure 4A). The same studies analyzed depression levels through HADS test. Pregabalin presented significantly less depressive symptoms (MD = −1.40, 95% CI = −1.71 to −1.08, participants = 2,650, studies = 3, I2 = 0%, p < 0.00001) (Figure 4B).
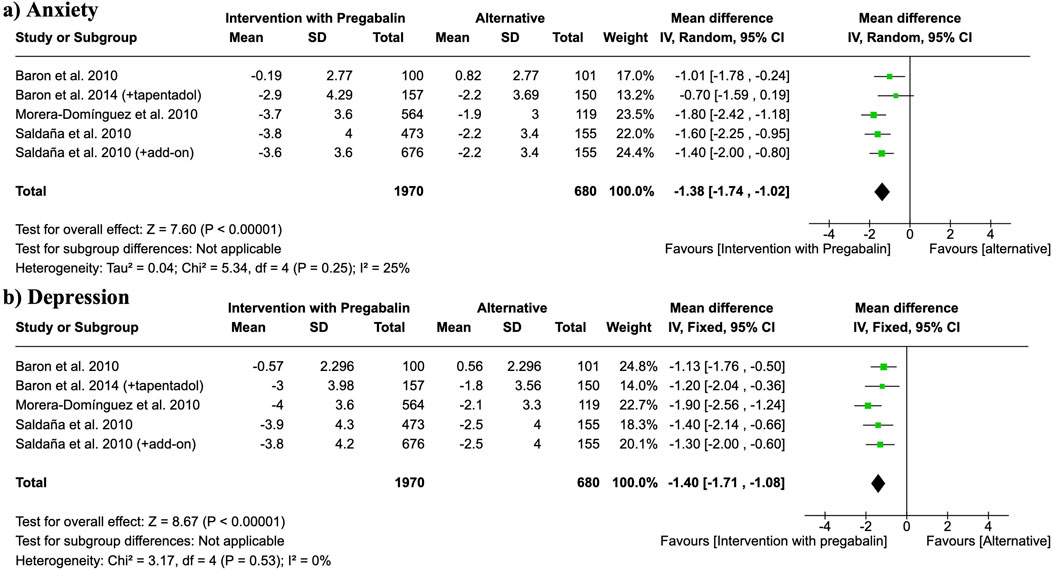
Figure 4. Forest plots of mean differences (MDs) for (a) anxiety and (b) depression scores (measured by Hospital Anxiety and Depression Scale, HADS) comparing pregabalin interventions versus control groups. Study of Saldaña et al. (2010a) refers to Saldaña et al. (2010b).
3.4.3 Quality of life, disability
Quality of life was studied by six studies through EQ-5D and SF-12 tests. Forest plot showed an improvement of quality of life when patients were treated with pregabalin compared to control group (tapentadol, limaprost, other analgesic than pregabalin, tramadol/acetaminophen combination, or placebo) (SMD = 0.22, 95% CI = 0.07 to 0.37, participants = 3,963, studies = 6, I2 = 74%, p = 0.003) (Figure 5).

Figure 5. Forest plot of standardized mean differences (SMDs) for quality of life outcomes (measured by EQ-5D or SF-12) comparing pregabalin interventions versus control groups. Study of Saldaña et al. (2010a) refers to Saldaña et al. (2010b).
The effect of pregabalin on the improvement of disability was studied by eight of the included studies. Authors used different scales like ODI, Roland-Morris Disability Questionnaire or Sheehan Disability Inventory. An intervention with pregabalin did not significantly improve disability levels (SMD = −0.20, 95% CI = −0.40 to 0.00, participants = 2,508, studies = 8, I2 = 76%, p = 0.05) (Figure 6).
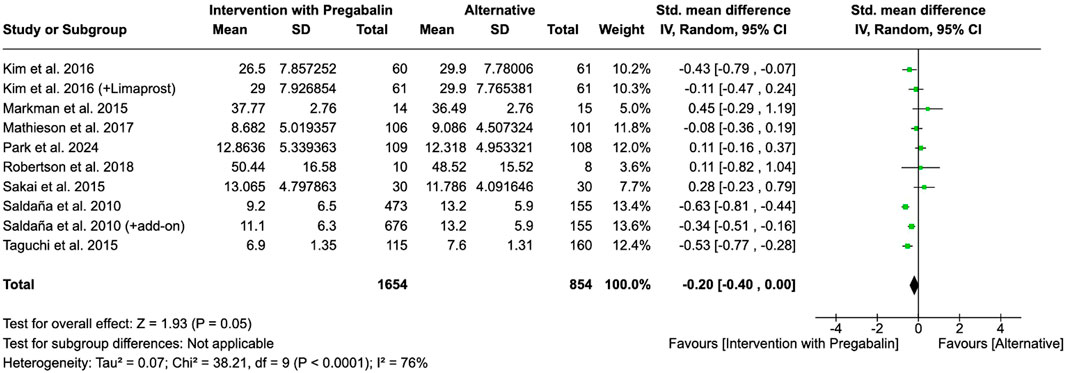
Figure 6. Forest plot of standardized mean differences (SMDs) for disability outcomes comparing pregabalin interventions versus control groups. Study of Saldaña et al. (2010a) refers to Saldaña et al. (2010b).
3.4.4 Sleep disturbance
Four studies analyzed the effect of an intervention with pregabalin versus buprenorphine, other analgesic, or placebo on sleep disturbance. An intervention with ‘pregabalin (buprenorphine and pregabalin, other analgesics and pregabalin, or pregabalin alone) showed a reduction on sleep disturbance when it was compared to alternative treatments or placebo (SMD = −0.61, 95% CI = −0.87 to −0.36, participants = 1,982, studies = 4, I2 = 80%, p < 0.00001) (Figure 7).
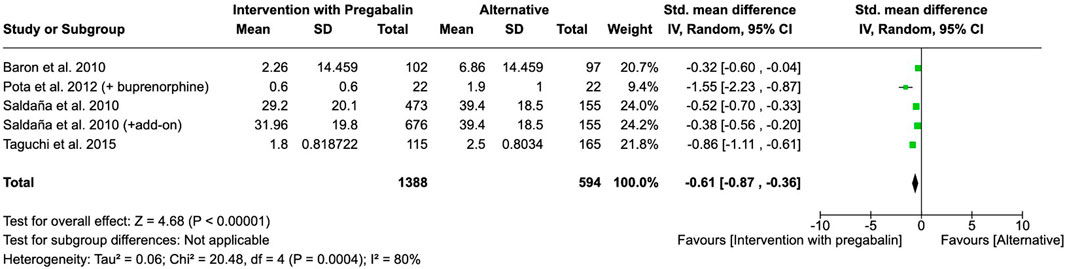
Figure 7. Forest plot of standardized mean differences (SMDs) for sleep disturbance outcomes comparing pregabalin interventions versus control groups. Study of Saldaña et al. (2010a) refers to Saldaña et al. (2010b).
3.4.5 Adverse events
There were no significant differences with respect to the adverse events assessed by five of the included studies: dizziness, nausea, drowsiness, bowel disturbance, and edema (Table 2), in the case where the treatment involved a combination of other medications with pregabalin (buprenorphine, limaprost, or GBP) and whether the intervention was pregabalin alone versus an active control.
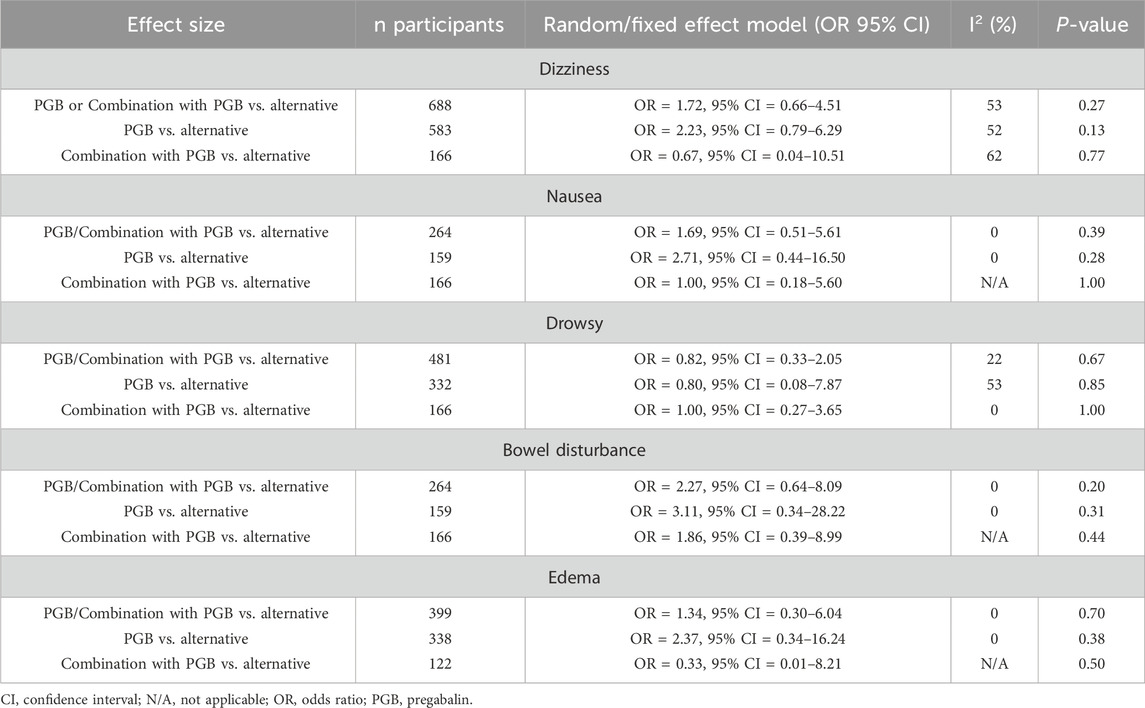
Table 2. Adverse effect assessment.
3.4.6 Total cost
Total cost of a treatment with pregabalin versus placebo or other treatments was analyzed by four studies. This analysis showed that a treatment with pregabalin resulted in lower total costs per patient at the end of the various follow-up periods (from 12 to 52 weeks) of each study (SMD = −0.16, 95% CI = −0.25 to −0.07, participants = 2,898, studies = 4, I2 = 9%, p = 0.0003).
3.4.7 Sensitivity analyses
Sensitivity analyzes were conducted by excluding the study with the greatest weight to test the robustness of the results obtained on pain, anxiety and depression, quality of life, sleep, disability and total cost outcomes. Results did not change significantly, except in the case of follow-up time of 4 weeks when back pain was assessed where, upon removing the study with the greatest weight, the significance was lost and no beneficial effects were observed at this period of treatment with pregabalin versus an active control (SMD = −0.66, 95% CI = −1.36 to 0.04, participants = 1,080, studies = 6, I2 = 96%, p = 0.07).
3.5 Publication bias
Upon visual inspection of the funnel plots, asymmetry was observed indicating publication bias in most of the variables. Symmetry was observed in case of leg pain, depression assessment, total cost, and for some of the adverse events (nausea, drowsiness, bowel disturbance, and edema).
3.6 GRADE
The GRADE assessment of the main outcomes (back pain, anxiety, depression, disability, quality of life and sleep) is presented in Table 3. The certainty of anxiety and the back pain outcomes was low, whereas depression, quality of life, sleep, and disability outcomes were moderate. The studies mainly presented a high risk of publication bias, differences in inclusion criteria and four of the included studies had moderate or high risk of bias.
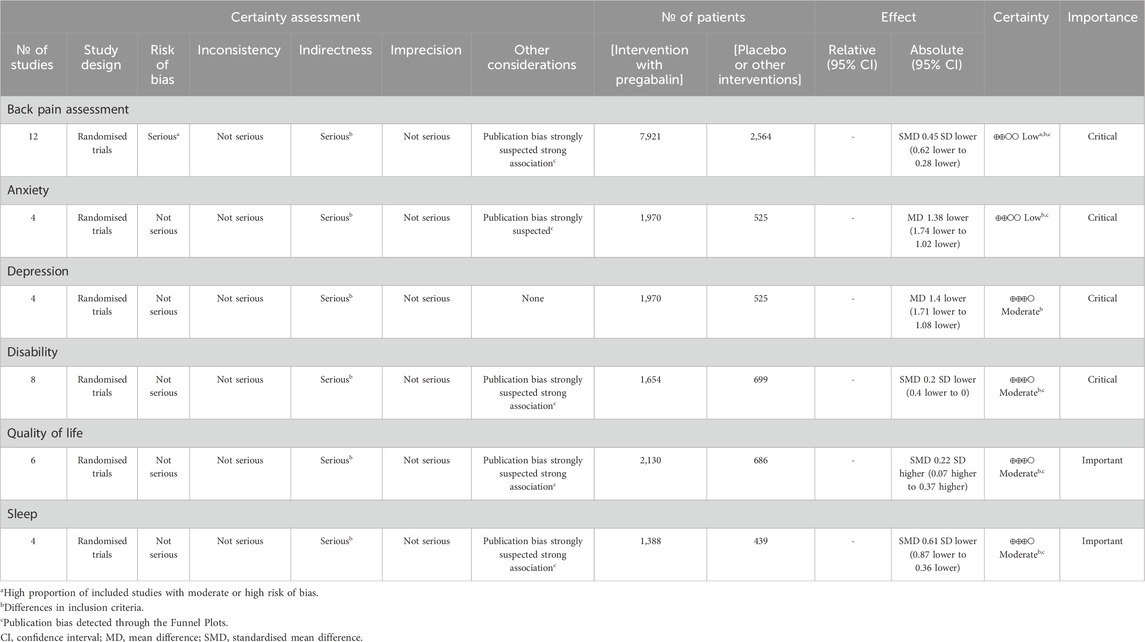
Table 3. GRADE assessment.
4 Discussion
Despite the development of multiple drugs targeting diverse mechanisms of action for predominantly nonspecific axial LBP syndromes, no therapy has been approved for neuropathic LBP conditions such as sciatica (Markman et al., 2018). Pregabalin has shown efficacy in several neuropathic and nociplastic pain conditions, including diabetic peripheral neuropathy (Zhang et al., 2015; Parsons et al., 2018) and fibromyalgia (Zareba, 2008; Migliorini et al., 2022). However, evidence remains inconsistent for other conditions, such as LBP, particularly in neuropathic subtypes like sciatica.
Pregabalin has demonstrated improvements in LBP at 4, 6, and 8 weeks, underscoring the importance of addressing the multidimensional nature of this condition, which can involve both neuropathic and nociceptive pain components. Notably, our meta-analysis indicates that the most pronounced effectiveness of pregabalin emerges from 4 weeks onward, which contrasts with findings for other compounds such as buprenorphine (Pota et al., 2012) or conventional care (Taguchi et al., 2015), where the onset of pain relief may differ. In addition to its analgesic effects, pregabalin has shown efficacy in improving reduction in sleep disturbance and anxiety symptoms, which are frequently associated with chronic LBP (Montaño et al., 2025). This psychiatric benefit may help explain the significant improvements in quality of life observed, even in the absence of marked changes in functional or disability scores. It is important to note that many of the included studies had relatively short follow-up durations (≤12 weeks), which may have limited the detection of changes in disability outcomes. Improvements in sleep quality associated with pregabalin may contribute to overall symptom relief, as a strong relationship between sleep quality and quality of life has been documented (Perotta et al., 2021).
In conditions such as sciatica and radiculopathy, pulsed radiofrequency has demonstrated efficacy in pain relief (Chao et al., 2008) both as a standalone treatment and when combined with steroid injection (Napoli et al., 2023). However, these approaches have not yet been specifically evaluated in combination with pregabalin for these indications. Interestingly, the combination of pregabalin with radiofrequency has been shown to improve sleep quality in patients with herpetic neuralgia, further supporting its beneficial effects on overall patient wellbeing (Chen et al., 2023). These findings suggest that exploring combined treatment approaches could be valuable for enhancing outcomes in patients with neuropathic pain conditions.
The heterogeneity of comparators in existing studies—including gabapentin (GBP), amitriptyline, limaprost, diphenhydramine, NSAIDs, and opioids—has limited the number of trials directly comparing pregabalin to individual agents, constraining robust conclusions. However, the literature indicates that pregabalin showed superiority over gabapentin in cancer-related neuropathic pain (Mishra et al., 2012) and over opioids for lower-limb symptoms in elderly patients with chronic LBP (Sakai et al., 2015).
In this meta-analysis, the combination of pregabalin with other pharmacological agents demonstrated a significant improvement in pain outcomes compared to active control or placebo. These findings suggest that adjunctive pregabalin may represent an optimal strategy for enhancing pain management in patients with lower back pain, particularly when a neuropathic component is present (Romanò et al., 2009). It is important to note that certain combinations, such as pregabalin with opioids, have been associated with increased risks of sedation and falls (Virnes et al., 2022) as well as dizziness, cognitive dysfunction, and respiratory depression (Hahn et al., 2022).
Another important question to address is regarding the comparative effectiveness and safety of higher doses of pregabalin versus alternative regimens. Future research should categorize pregabalin dosing (e.g., ≤150 mg, 150–300 mg, >300 mg) to better elucidate potential dose–response relationships. In our meta-analysis, only three studies explicitly reported mean doses above 300 mg; however, this does not necessarily indicate that all patients received doses exceeding 300 mg, but rather that the average dose within those studies was higher. Similarly, the initial starting dose did not appear to influence outcomes, as studies commencing pregabalin at 75 mg and those starting between 150 and 300 mg achieved comparable results, provided they reached the same final dose. Our analysis also did not demonstrate any clear differences in the incidence of adverse events across dosing regimens. Moreover, future studies should consider stratifying patients using validated tools such as the Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) or the DN4 questionnaire to further clarify pregabalin’s role in individuals with prominent neuropathic features. For example, the study by Romano et al. found that pregabalin was particularly effective in patients with LANSS scores indicative of neuropathic pain, even when nociceptive components were also present (Romanò et al., 2009). The concept that pain with different mechanistic characteristics—nociceptive, neuropathic, or nociplastic—can coexist in the same patient, in any combination, has been further developed by Freynhagen et al. (2019) in their narrative review describing the phenomenon of ‘mixed pain.’ Given pregabalin’s demonstrated efficacy in both neuropathic and nociplastic pain models, it may be particularly well-suited for the management of these complex, overlapping pain phenotypes.
Pregabalin has demonstrated efficacy in spinal conditions beyond those included in the present meta-analysis. Specifically, pregabalin has been shown to be more effective than gabapentin in reducing pain associated with Failed Back Surgery Syndrome (Al-Ameri et al., 2024). Additionally, pregabalin has been associated with reductions in postoperative pain and opioid consumption following spinal fusion, highlighting its potential as an adjunct in postoperative pain management (Fujita et al., 2016). In line with these findings, the present meta-analysis revealed that pregabalin was associated with lower total costs compared to other interventions. This cost-effectiveness is further supported by evidence indicating that pregabalin’s efficacy in managing not only pain but also comorbid symptoms, such as anxiety and depression, contributes to a reduction in indirect costs, including loss of productivity and diminished quality of life, which are significant drivers of the economic burden in neurological disorders (Morera-Domínguez et al., 2010; Dagenais et al., 2008). These indirect costs are recognized as the most substantial component in the overall treatment burden for these conditions (Chodavadia et al., 2023).
Few meta-analyses have specifically examined the isolated effect of pregabalin for low back pain, which limits the ability to consistently analyze heterogeneity focused on pregabalin. For example, Wewege et al. (2023) reported only limited pain improvement with various medications, including pregabalin, and highlighted the low certainty of evidence for any pain reduction achieved with these agents. Similarly, Giménez-Campos et al. included pregabalin alongside gabapentin in their analysis, but only three studies specifically evaluated pregabalin. They found no evidence of efficacy for either drug in sciatica, with no benefit over placebo for pain relief and a worse safety profile, characterized by increased rates of dizziness and nausea/vomiting (Giménez-Campos et al., 2022). Consistent with these findings, Mascarenhas et al. (2023) observed that opioids provided greater pain relief than pregabalin in older adults with chronic nonspecific low back pain. Additionally, Shanthanna et al. (2017) found no benefit of pregabalin, even when used as an adjunct to opioids.
4.1 Limitations
A primary limitation of this meta-analysis is the inadequate reporting of pain etiology and symptom duration across the included studies, factors that are likely to influence pregabalin’s efficacy and contribute to the inconsistent outcomes observed, particularly in chronic cases (Romanò et al., 2009; Pota et al., 2012; Kalita et al., 2014; Park et al., 2024). Specifically, Kalita et al. (2014) included a mixed population of patients with neuropathic and non-neuropathic pain. The same situation was found in the case of Romanò et al. (2009) where the efficacy results of pregabalin were not stratified by neuropathic vs. non-neuropathic, presenting only aggregated results for the entire population. Additionally, Pota et al. (2012) mentioned that approximately 85% of the patients showed signs of a neuropathic pain component, they did not specify the criteria used for this determination or provide details about the specific underlying neuropathic conditions. In this sense, inadequate reporting of pain etiology is a critical limitation (these trials enrolled mixed populations or did not specify pain etiology in sufficient detail, which posed a significant challenge to conduct subgroup analyses stratified by pain type). Therefore it is essential to advocate for future research that more specifically addresses the underlying causes of pain, allowing for more precise analyzes based on etiology. Given this limitation, our findings should be interpreted with caution, especially when considering their applicability to mechanical or non-neuropathic LBP. There was also considerable heterogeneity in the types of pain assessed, with studies variably focusing on acute or chronic pain and on lumbar pain with or without radiculopathy, which complicates direct comparisons and affects generalizability. Another limitation of this review was the deviation from the originally registered PROSPERO protocol, which included EMBASE as a planned data source. Due to procedural adjustments, this search was not conducted during the initial search phase. However, a subsequent post hoc search in EMBASE using our predefined terms did not yield any additional unique articles. Moreover, we performed manual searching (handsearching) of reference lists from relevant studies to further minimize the risk of missing eligible publications, enhancing the thoroughness of our study selection process. A further limitation of this meta-analysis concerns the estimation of standard deviations, which in some cases had to be calculated using the Cochrane Review Manager software due to incomplete data reporting. The representativeness of certain subgroups was limited, as few studies specifically targeted these populations, and the wide variation and length of follow-up periods made it challenging to perform accurate subgroup analyses. Reporting of adverse events was inconsistent, with considerable variability in the timeframes for recording such events across studies, and the limited number of articles addressing each safety variable further compounded this issue. The potential for publication bias also exists and may have influenced the overall results. Also, there was a lack of evaluation of different pregabalin dosages, underscoring the need for future studies to determine the optimal therapeutic dose. Furthermore, significant differences among control groups—especially when pregabalin was compared with interventions other than placebo—and the scarcity of studies with a pregabalin-only control group limit the ability to draw definitive conclusions about its isolated effect. It should also be noted that the potential use of additional conservative treatments, such as electrotherapy, physiotherapy, rehabilitation, or exercise programs, could not be controlled for due to insufficient reporting in the included studies.
5 Conclusion
Pregabalin, whether administered as monotherapy or in combination with other treatments, has demonstrated efficacy in the management of LBP. Notable benefits include significant reductions in pain (observed from weeks four to eight of follow-up) as well as improvements in associated symptoms such as anxiety, depression, sleep disturbances, and overall quality of life. Additionally, pregabalin exhibited a safety profile comparable to that reported in existing literature and similar to other therapeutic alternatives, based on the adverse events analyzed. However, these findings should be interpreted with caution due to the overall limited and heterogeneous quality of the available evidence, particularly the inadequate reporting of pain etiology and symptom duration across studies. Several included trials enrolled mixed populations or did not clearly distinguish between neuropathic and non-neuropathic LBP, which limits the generalizability of the results and precludes robust subgroup analyses. Therefore, further well-designed, standardized studies are warranted to clarify pregabalin’s role across various LBP subtypes and to establish optimal dosing strategies.
Author contributions
CC-G: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. JS-R: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. TR-A: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. ML-A: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. ET-C: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. JB-A: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. MP-P: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was financially supported by Viatris, which funded the statistical analysis and the medical writing services.
Conflict of interest
MP-P was employed by Viatris Spain.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that this study received funding from Viatris. The funder had the following involvement in the study: analysis and the writing of this article.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fphar.2025.1659531/full#supplementary-material
SUPPLEMENTARY FILE S1 | PubMed search strategy.
SUPPLEMENTARY TABLE S1 | Assessment of the quality of studies through Methodological Index for Non-Randomized Studies (MINORS).
SUPPLEMENTARY TABLE S2 | Treatment schemes and free-drug period of the included studies.
References
Al-Ameri, L. T., Al-Saffar, F. A., Al-Badri, S. S., and Al-Rudainy, R. J. (2024). Pregabalin versus gabapentin efficacy in the management of neuropathic pain associated with failed back surgery syndrome. J. Korean Neurosurg. Soc. 67, 202–208. doi:10.3340/jkns.2022.0225
Areias, A. C., Luo, L., Flores, A., Fonseca, F., Simões, S., Teixeira, P., et al. (2023). Impact on productivity impairment of a digital care program for chronic low back pain: a prospective longitudinal cohort study. Musculoskelet. Sci. Pract. 63, 102709. doi:10.1016/j.msksp.2022.102709
Baron, R., Freynhagen, R., Tölle, T. R., Cloutier, C., Leon, T., Murphy, K. T., et al. (2010). The efficacy and safety of pregabalin in the treatment of neuropathic pain associated with chronic lumbosacral radiculopathy. Pain 150, 420–427. doi:10.1016/j.pain.2010.04.013
Baron, R., Jansen, J. P., Binder, A., Pombo-Suarez, M., Kennes, L., Richter, E., et al. (2014). Effectiveness and safety of tapentadol prolonged release (PR) versus a combination of tapentadol PR and pregabalin for the management of severe, chronic low back pain with a neuropathic component: a randomized, double-blind, phase 3b study. Pain Pract. 15, 455–470. doi:10.1111/papr.12200
Baron, R., Binder, A., Attal, N., Casale, R., Dickenson, A. H., Treede, R. D., et al. (2016). Neuropathic low back pain in clinical practice. Eur. J. Pain 20, 861–873. doi:10.1002/ejp.838
Cashin, A. G., Wand, B. M., O'Connell, N. E., Lee, H., Bagg, M. K., O'Hagan, E., et al. (2023). Pharmacological treatments for low back pain in adults: an overview of Cochrane reviews. Cochrane Database Syst. Rev. 4, CD013815. doi:10.1002/14651858.CD013815.pub2
Chao, S. C., Lee, H. T., Kao, T. H., Yang, M. Y., Tsuei, Y. S., Shen, C. C., et al. (2008). Percutaneous pulsed radiofrequency in the treatment of cervical and lumbar radicular pain. Surg. Neurol. 70, 59–65. doi:10.1016/j.surneu.2007.05.046
Chen, J., Li, L., Ge, Q., Yuan, W., Du, F., Shi, X., et al. (2023). Efficacy and safety of pulsed radiofrequency combined with pregabalin for herpetic neuralgia: a systematic review and meta-analysis. Medicine 102, e33932. doi:10.1097/MD.0000000000033932
Chodavadia, P., Teo, I., Tan, G. S., Tan, K. B., Finkelstein, E. A., and Vrijhoef, H. J. M. (2023). Prevalence and economic burden of depression and anxiety symptoms among Singaporean adults: results from a 2022 web panel. BMC Psychiatry 23, 367. doi:10.1186/s12888-023-04581-7
Chye, A., Armour, M., Mofizul Islam, M. M., Sanci, L. A., Makate, M., Maher, C. G., et al. (2021). Healthcare expenditure and its predictors in a cohort of Australians living with sciatica. Eur. Spine J. 30, 878–885. doi:10.1007/s00586-020-06605-2
Dagenais, S., Caro, J., and Haldeman, S. (2008). A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 8, 8–20. doi:10.1016/j.spinee.2007.10.005
Damiescu, R., Heuninck, J., Yousuf, S., Efferth, T., and Dawood, M. (2021). Health(care) in the crisis: reflections in science and society on opioid addiction. Int. J. Environ. Res. Public Health 18, 341. doi:10.3390/ijerph18010341
Dickson, C., Dickson, H., Ploubidis, G. B., Green, J., and Muthuri, S. G. (2023). Do chronic low back pain and chronic widespread pain differ in their association with depression symptoms in the 1958 British birth cohort? Pain Med. 24, 644–651. doi:10.1093/pm/pnac170
Enthoven, W. T. M., Roelofs, P. D. D. M., Deyo, R. A., van Tulder, M. W., and Koes, B. W. (2016). Non-steroidal anti-inflammatory drugs for chronic low back pain. Cochrane Database Syst. Rev. 2, CD012087. doi:10.1002/14651858.CD012087
Freynhagen, R., Parada, H. A., Calderon-Ospina, C. A., Chen, J., Rakhmawati Emril, D., Fernández-Villacorta, F. J., et al. (2019). Current understanding of the mixed pain concept: a brief narrative review. Curr. Med. Res. Opin. 35, 1011–1018. doi:10.1080/03007995.2018.1552042
Fujita, N., Tobe, M., Tsukamoto, N., Saito, S., and Obata, H. (2016). A randomized placebo-controlled study of preoperative pregabalin for postoperative analgesia in patients with spinal surgery. J. Clin. Anesth. 31, 149–153. doi:10.1016/j.jclinane.2016.01.010
Gammoh, O., Mayyas, F., Darwish, E. F., and Al-Smadi, J. (2021). The clinical difference between Gabapentin and pregabalin: data from a pilot comparative trial. Recent Pat. Biotechnol. 16, 279–287. doi:10.2174/1574887116666210201110507
GBD 2021 Low Back Pain Collaborators (2023). Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021. Lancet Rheumatol. 5, e316–e329. doi:10.1016/S2665-9913(23)00098-X
Ghazisaeidi, S., Muley, M. M., and Salter, M. W. (2023). Neuropathic pain: mechanisms, sex differences, and potential therapies for a global problem. Annu. Rev. Pharmacol. Toxicol. 63, 565–583. doi:10.1146/annurev-pharmtox-051421-112259
Giménez-Campos, M. S., Pacheco-da-Costa, S., Martínez-Pozas, O., Sánchez-Romero, E. A., Villafañe, J. H., and Pedersini, P. (2022). A systematic review and meta-analysis of the effectiveness and adverse events of gabapentin and pregabalin for sciatica pain. Aten. Primaria 54, 102144. doi:10.1016/j.aprim.2021.102144
Guyatt, G. H., Oxman, A. D., Santesso, N., Helfand, M., Vist, G., Kunz, R., et al. (2013). Findings tables and evidence profiles—continuous outcomes. J. Clin. Epidemiol. 66, 173–183. doi:10.1016/j.jclinepi.2012.08.001
Hahn, J., Murnion, B., Haber, P. S., Schneider, U., Wodarz, N., Wilhelm, J., et al. (2022). Risk of major adverse events associated with gabapentinoid and opioid combination therapy: a systematic review and meta-analysis. Front. Pharmacol. 13, 1009950. doi:10.3389/fphar.2022.1009950
Higgins, J. P. T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J., et al. (2019). Cochrane handbook for systematic reviews of interventions. 2nd ed. (Wiley).
Hu, Y., Xu, W., Zhang, Z., Wang, J., Li, M., Wu, Y., et al. (2022). Anxiety symptoms and associated factors among chronic low back pain patients in China: a cross-sectional study. Front. Public Health 10, 878865. doi:10.3389/fpubh.2022.878865
Kalita, J., Chandra, S., Misra, U. K., and Bhoi, S. K. (2014). An open labeled randomized controlled trial of pregabalin versus amitriptyline in chronic low backache. J. Neurol. Sci. 342, 127–132. doi:10.1016/j.jns.2014.05.002
Kikuchi, S., Kato, H., Fujii, T., Okubo, T., Ono, R., Abraham, L., et al. (2021). A retrospective database study of gastrointestinal events and medical costs associated with nonsteroidal anti-inflammatory drugs in Japanese patients of working age with osteoarthritis and chronic low back pain. Pain Med. 22, 1029–1038. doi:10.1093/pm/pnaa421
Kim, H. J., Lee, H. M., Kim, H. S., Moon, S. H., Kim, N. H., Park, J. O., et al. (2016). Comparative study of the efficacy of limaprost and pregabalin as single agents and in combination for the treatment of lumbar spinal stenosis: a prospective, double-blind, randomized controlled non-inferiority trial. Spine J. 16, 756–763. doi:10.1016/j.spinee.2016.02.049
Lorente, A., Gómez, J., Gil, V., Jiménez, A., Palop, C., Montaner-Alonso, D., et al. (2024). Predictive factors of functional outcomes and quality of life in patients with ankle fractures: a systematic review. J. Clin. Med. 13, 1188. doi:10.3390/jcm13051188
Mák, K., Maróti, P., Szabó, Á., Kökény, T., Balogh, Z., Molnár, M. J., et al. (2021). Neuropathic low back pain and burnout among Hungarian workers. Int. J. Environ. Res. Public Health 18, 2693. doi:10.3390/ijerph18052693
Markman, J. D., Frazer, M. E., Rast, S. A., McDermott, M. P., Gewandter, J. S., Chowdhry, A. K., et al. (2015). Double-blind, randomized, controlled, crossover trial of pregabalin for neurogenic claudication. Neurology 84, 265–272. doi:10.1212/WNL.0000000000001168
Markman, J. D., Baron, R., and Gewandter, J. S. (2018). Why are there no drugs indicated for sciatica, the most common chronic neuropathic syndrome of all? Drug Discov. Today 23, 1904–1909. doi:10.1016/j.drudis.2018.06.004
Mascarenhas, V. G., de Oliveira, P. V., de Almeida, M. B., Ferreira, P. H., de Oliveira, V. C., Resende, M. A., et al. (2023). Effectiveness of pharmacological and non-pharmacological therapy on pain intensity and disability in older people with chronic nonspecific low back pain: a systematic review with meta-analysis. Eur. Spine J. 32, 3245–3271. doi:10.1007/s00586-023-07857-4
Mathieson, S., Maher, C. G., McLachlan, A. J., Latimer, J., Koes, B. W., Hancock, M. J., et al. (2017). Trial of pregabalin for acute and chronic sciatica. N. Engl. J. Med. 376, 1111–1120. doi:10.1056/NEJMoa1614292
Migliorini, F., Maffulli, N., Eschweiler, J., Knobe, M., Tingart, M., and Baroncini, A. (2022). Pregabalin administration in patients with fibromyalgia: a Bayesian network meta-analysis. Sci. Rep. 12, 12148. doi:10.1038/s41598-022-16146-x
Mishra, S., Bhatnagar, S., Goyal, G. N., Rana, S. P. S., and Upadhya, S. P. (2012). A comparative efficacy of amitriptyline, Gabapentin, and pregabalin in neuropathic cancer pain: a prospective randomized double-blind placebo-controlled study. Am. J. Hosp. Palliat. Care 29, 177–182. doi:10.1177/1049909111412539
Montaño, J. J., Sánchez-Romero, E. A., Villafañe, J. H., Alonso-Pérez, J. L., Martín-Pintado-Zugasti, A., and Pedersini, P. (2025). From acute to chronic low back pain: the role of negative emotions. Psychol. Health Med., 1–14. doi:10.1080/13548506.2025.2478657
Morera-Domínguez, C., Ceberio-Balda, F., Flórez-García, M., García-Pérez, L., Hidalgo-Vega, Á., and Artacho-Perula, E. (2010). A cost-consequence analysis of pregabalin versus usual care in the symptomatic treatment of refractory low back pain: sub-analysis of observational trial data from orthopedic surgery and rehabilitation clinics. Clin. Drug Investig. 30, 517–531. doi:10.2165/11536280-000000000-00000
Napoli, A., Anzidei, M., Ciolina, F., Marotta, E., Cavallo, M. B., Brachetti, G., et al. (2023). CT-guided pulsed radiofrequency combined with steroid injection for sciatica from herniated disk: a randomized trial. Radiology 307, e221478. doi:10.1148/radiol.221478
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 372, n71. doi:10.1136/bmj.n71
Park, J. H., Kim, H. J., Yeom, J. S., Lee, Y. S., Lee, S. U., Lee, D. G., et al. (2024). Comparative study on the efficacy of pregabalin versus limaprost in patients with lumbar spinal stenosis: a prospective, randomized controlled trial. World Neurosurg. 186, e694–e701. doi:10.1016/j.wneu.2024.04.033
Parsons, B., Emir, B., Clair, A., Lockhart, E., Ortiz, M., and Whalen, E. (2018). Comparison of the efficacy and safety of pregabalin for postherpetic neuralgia in Chinese and international patients. J. Pain Res. 11, 1699–1708. doi:10.2147/JPR.S157856
Perotta, B., Arantes-Costa, F. M., Enns, S. C., Figueiro-Filho, E. A., Paro, H. B. M. S., Santos, I. S., et al. (2021). Sleepiness, sleep deprivation, quality of life, mental symptoms and perception of academic environment in medical students. BMC Med. Educ. 21, 111. doi:10.1186/s12909-021-02544-8
Petzke, F., Klose, P., Welsch, P., Sommer, C., Häuser, W., Tolle, T., et al. (2020). Opioids for chronic low back pain: an updated systematic review and meta-analysis of efficacy, tolerability and safety in randomized placebo-controlled studies of at least 4 weeks of double-blind duration. Eur. J. Pain 24, 497–517. doi:10.1002/ejp.1519
Pota, V., Barbarisi, M., Sansone, P., Moraci, M., Barbarisi, A., Pace, M. C., et al. (2012). Combination therapy with transdermal buprenorphine and pregabalin for chronic low back pain. Pain Manag. 2, 23–31. doi:10.2217/pmt.11.71
Robertson, K., Marshman, L., Plummer, D., and Downs, E. (2019). Effect of gabapentin vs pregabalin on pain intensity in adults with chronic sciatica: a randomized clinical trial. JAMA Neurol. 76, 28–34. doi:10.1001/jamaneurol.2018.3077
Romanò, C. L., Romanò, D., Bonora, C., and Mineo, G. (2009). Pregabalin, celecoxib, and their combination for treatment of chronic low-back pain. J. Orthop. Traumatol. 10, 185–191. doi:10.1007/s10195-009-0077-z
Sakai, Y., Ito, K., Hida, T., Ito, S., and Harada, A. (2015). Pharmacological management of chronic low back pain in older patients: a randomized controlled trial of the effect of pregabalin and opioid administration. Eur. Spine J. 24, 1309–1317. doi:10.1007/s00586-015-3812-6
Saldaña, M. T., Navarro, A., Pérez, C., Rejas, J., and Rojas, R. (2010a). Patient-reported-outcomes in subjects with painful lumbar or cervical radiculopathy treated with pregabalin: evidence from medical practice in primary care settings. Rheumatol. Int. 30, 1005–1015. doi:10.1007/s00296-009-1086-1
Saldaña, M. T., Navarro, A., Pérez, C., Masramón, X., and Rejas, J. (2010b). A cost-consequences analysis of the effect of pregabalin in the treatment of painful radiculopathy under medical practice conditions in primary care settings. Pain Pract. 10, 31–41. doi:10.1111/j.1533-2500.2009.00312.x
Shanthanna, H., Gilron, I., Rajarathinam, M., AlAmri, R., Kamath, S., Thabane, L., et al. (2017). Benefits and safety of gabapentinoids in chronic low back pain: a systematic review and meta-analysis of randomized controlled trials. PLoS Med. 14, e1002369. doi:10.1371/journal.pmed.1002369
Sharma, S., and McAuley, J. H. (2022). Low back pain in low- and middle-income countries, part 1: the problem. J. Orthop. Sports Phys. Ther. 52, 233–235. doi:10.2519/jospt.2022.11145
Shetty, G. M., Jain, S., Thakur, H., Khanna, T., Gotecha, S., Patil, A., et al. (2022). Prevalence of low back pain in India: a systematic review and meta-analysis. Work 73, 429–452. doi:10.3233/WOR-205300
Sicras-Mainar, A., Rejas, J., Navarro-Artieda, R., Blanca-Tamayo, M., Pérez-Paramo, M., Villarroya, C., et al. (2013). Cost comparison of adding pregabalin or gabapentin for the first time to the therapy of patients with painful axial radiculopathy treated in Spain. Clin. Exp. Rheumatol. 31, 372–381.
Slim, K., Nini, E., Forestier, D., Kwiatkowski, F., Panis, Y., and Chipponi, J. (2003). Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J. Surg. 73, 712–716. doi:10.1046/j.1445-2197.2003.02748.x
Taguchi, T., Iseki, M., Kido, K., Tanigawa, T., Tonomura, S., Shimoyama, N., et al. (2015). Effectiveness of pregabalin for the treatment of chronic low back pain with accompanying lower limb pain (neuropathic component): a non-interventional study in Japan. J. Pain Res. 8, 487–497. doi:10.2147/JPR.S88642
Taylor, C. P., Angelotti, T., and Fauman, E. (2007). Pharmacology and mechanism of action of pregabalin: the calcium channel alpha2-delta (Alpha2-delta) subunit as a target for antiepileptic drug discovery. Epilepsy Res. 73, 137–150. doi:10.1016/j.eplepsyres.2006.09.008
Virnes, R. E., Tiihonen, M., Karttunen, N., van Poelgeest, E. P., van der Velde, N., and Hartikainen, S. (2022). Opioids and falls risk in older adults: a narrative review. Drugs Aging 39, 199–207. doi:10.1007/s40266-022-00929-y
Wang, J., and Doan, L. V. (2024). Clinical pain management: current practice and recent innovations in research. Cell Rep. Med. 5, 101786. doi:10.1016/j.xcrm.2024.101786
Wewege, M. A., Bagg, M. K., Jones, M. D., McAuley, J. H., Wand, B. M., O'Hagan, E. T., et al. (2023). Comparative effectiveness and safety of analgesic medicines for adults with acute non-specific low back pain: systematic review and network meta-analysis. BMJ 380, e072962. doi:10.1136/bmj-2022-072962
Yeole, A. B., Patil, S. D., Khan, F., Gaikwad, S., Patel, H., Gawde, H., et al. (2022). Efficacy and safety of pregabalin prolonged release-etoricoxib combination compared to etoricoxib for chronic low back pain: phase 3, randomized study. Pain Ther. 11, 1451–1469. doi:10.1007/s40122-022-00437-2
Zareba, G. (2008). New treatment options in the management of fibromyalgia: role of pregabalin. Neuropsychiatr. Dis. Treat. 4, 1193–1201. doi:10.2147/NDT.S3257
Keywords: low back pain, radiculopathy, sciatica, neuropathic pain, meta-analysis
Citation: Cordero-García C, Sánchez-Raya J, Rodríguez-Araya TL, López-Alarcón MD, Trillo-Calvo E, Balsalobre-Aznar J and Pérez-Páramo M (2025) Efficacy and safety of pregabalin in the management of low back pain: a comprehensive meta-analysis. Front. Pharmacol. 16:1659531. doi: 10.3389/fphar.2025.1659531
Received: 04 July 2025; Accepted: 15 August 2025;
Published: 08 September 2025.
Edited by:
Mamdouh M. El-Shishtawy, Mansoura University, EgyptReviewed by:
Jaroslav Pejchal, University of Defence, CzechiaNoha O. Mansour, Mansoura University, Egypt
Copyright © 2025 Cordero-García, Sánchez-Raya, Rodríguez-Araya, López-Alarcón, Trillo-Calvo, Balsalobre-Aznar and Pérez-Páramo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Cordero-García, Y2NvcmRlcm8ucmhiQGdtYWlsLmNvbQ==