 José Wagner Leonel Tavares-Júnior1†
José Wagner Leonel Tavares-Júnior1† Ana Célia Caetano de Souza2,3†
Ana Célia Caetano de Souza2,3† Gilberto Sousa Alves4*Janine de Carvalho Bonfadini1,3José Ibiapina Siqueira-Neto1
Gilberto Sousa Alves4*Janine de Carvalho Bonfadini1,3José Ibiapina Siqueira-Neto1 Pedro Braga-Neto1,2,3
Pedro Braga-Neto1,2,3- 1Department of Clinical Medicine, Division of Neurology, Universidade Federal do Ceará, Fortaleza, Brazil
- 2Center of Health Sciences, Universidade Estadual do Ceará, Fortaleza, Brazil
- 3Neurology Service, Hospital Universitário Walter Cantídio, Universidade Federal do Ceará, Fortaleza, Brazil
- 4Translational Psychiatry Research Group, Universidade Federal do Maranhão, São Luís, Brazil
Introduction: Cognitive assessment of older adults who are either illiterate or with low levels of education is particularly challenging because several battery tasks require a certain educational background. Early detection of mild cognitive impairment (MCI) in the elderly using validated screening tools is of great importance since this population group could benefit from new drugs that are being investigated for the treatment of dementias. Cutoff scores for psychometric properties of cognitive tests are not well established among adults with low levels of education. The present study aimed to critically review the literature on cognitive assessment tools for screening cognitive syndromes including MCI and Alzheimer’s disease (AD) in older adults with low levels of education.
Methods: We conducted a systematic search of MEDLINE, LILACS, Cochrane, and SCOPUS electronic databases of cross-sectional and prospective studies with adults over 55 years of age.
Results: We found a significant number of assessment tools available (n = 44), but only a few of them showed diagnostic accuracy for the diagnosis of MCI and AD in older adults with low levels of education: the Mini-Mental State Exam; the Montreal Cognitive Assessment; the Persian Test of Elderly for Assessment of Cognition and Executive Function; the Six-Item Screener; and the Memory Alteration Test. Few studies evaluated individuals with low levels of education, with a wide range of cutoff scores and cognitive test batteries.
Conclusion: We found that a small number of studies evaluated adults with 4 years of formal education or less. Our findings further support the importance of developing specific tools for the assessment of older adults with low levels of education.
Introduction
Dementia is characterized by cognitive impairment and loss of function (1). The growth of population aging over the past few decades has been associated with an increase in cognitive disorders. Data from Alzheimer’s Disease International (ADI) shows there were 46.8 million people living with dementia worldwide in 2015, and it is estimated this number will be 74.5 million in 2030 and 131.5 million in 2050. Alzheimer’s disease (AD) is the most common form of dementia and accounts for 50–70% of dementia cases. There were an estimated 26 million people living with AD in 2015 and it is believed there will be as many as 41 million by 2030 and 72 million by 2050 (1).
Mild cognitive impairment (MCI) is the intermediate stage between cognitive decline of healthy aging and dementia (2). The prevalence of MCI is 12–18% among adults over 65 years of age and the annual progression rates from MCI to AD are 10–15% (3, 4). Early detection of MCI in the elderly using validated screening tools is of great importance since this population group could benefit from new drugs that are being investigated for the treatment of neurodegenerative diseases including AD. Furthermore, evidence shows that, since MCI is a transitional phase between normal aging and AD, there is less brain involvement and those affected are more likely to benefit from drug therapies (5, 6).
Cognitive assessment tools are commonly used for screening impairment, differential diagnosis, determining disease severity, as well as monitoring disease progression in patients (7). A major challenge for the initial assessment of age-related cognitive changes is to find a screening tool that is both sensitive and specific for differential diagnosis of cognitive impairment. Both ceiling effects and floor effects limit the ability of a test or some of its items to accurately assess cognitive decline (8). These effects have been reported in several studies and they are primarily related to educational background (9). The ceiling effect occurs when score distribution is skewed and a measurement is determined by the proportion of people scoring at the high end, thereby preventing to detect health improvements. The opposite is the floor effect that occurs when a measurement is determined by the proportion of people scoring at the low end, thereby preventing to detect health declines (10).
Another important aspect is to have available free, easy-to-use assessment tools that do not require specialized training and have the ability to accurately discriminate cognitive decline in adults with normal aging, MCI, and dementia (4). Cognitive assessment of older adults who are either illiterate or with low levels of education is particularly challenging because several battery tasks require a certain educational background (11–13). There are an estimated 758 million illiterate adults in the world (11) and 13 million people are estimated to be illiterate in Brazil (11). Prospective cohort studies have shown an association between low education and higher risk of developing AD (14–17). Yet, few studies have examined the performance of cognitive assessment tools in adults with low education.
Cutoff scores for psychometric properties of cognitive tests are not well established among adults with low levels of education. Furthermore, there is a scarcity of studies evaluating assessment tools for screening older adults with low levels of education. A better understanding of the accuracy of different cognitive batteries is crucial for early diagnosis and intervention, and epidemiological studies are needed to further explore how education background affects an individual’s performance on different cognitive dimensions.
The present study aimed to critically review the literature on cognitive assessment tools for screening cognitive syndromes including MCI and AD in older adults with low levels of education.
Methods
An integrative literature review was conducted to gather and summarize the body of evidence available from original articles. This integrative review study included six stages: Step 1—formulation of the central research question (theme identification); Step 2—definition of inclusion and exclusion criteria and literature search; Step 3—categorization of primary studies (definition of data to be extracted from the selected studies); Step 4—assessment of the studies included; Step 5—interpretation of results; Step 6—knowledge synthesis of the results obtained from the studies assessed (18–20).
The central research question was formulated using the PVO method where P is the study population (adults over 55 years of age with low education, i.e., 4 years of formal education or less); V is the variable (cognitive assessment tools); and O is the outcome (MCI and AD).
The guiding question of our review was: “Which assessment tools are used for cognitive screening of MCI or AD in older adults with low levels of education?” The inclusion criteria were English language articles in the electronic databases Medical Literature Analysis and Retrieval System Online (MEDLINE), Latin American and Caribbean Health Sciences Literature (LILACS), Cochrane, and SCOPUS; cross-sectional or prospective design; outpatient or population-based samples of adults over 55 years of age with low education (4 years of education or less); and assessment of the use of cognitive tools for MCI or AD diagnosis. We did not search the following information sources for this review: guidelines; institutional protocols; self-administered or telephone-based cognitive assessment instruments; and studies that used cognitive assessment instruments for diagnosing other psychiatric or neurological conditions. The publications were individually searched and selected by two investigators during June and July 2019.
The Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines (21) were used as a basis for the search and selection of studies (Figure 1). A questionnaire was developed to help data extraction (22). Two matrices were constructed to present the results: the first one included study characteristics and the second one included cognitive tools and main results reported.
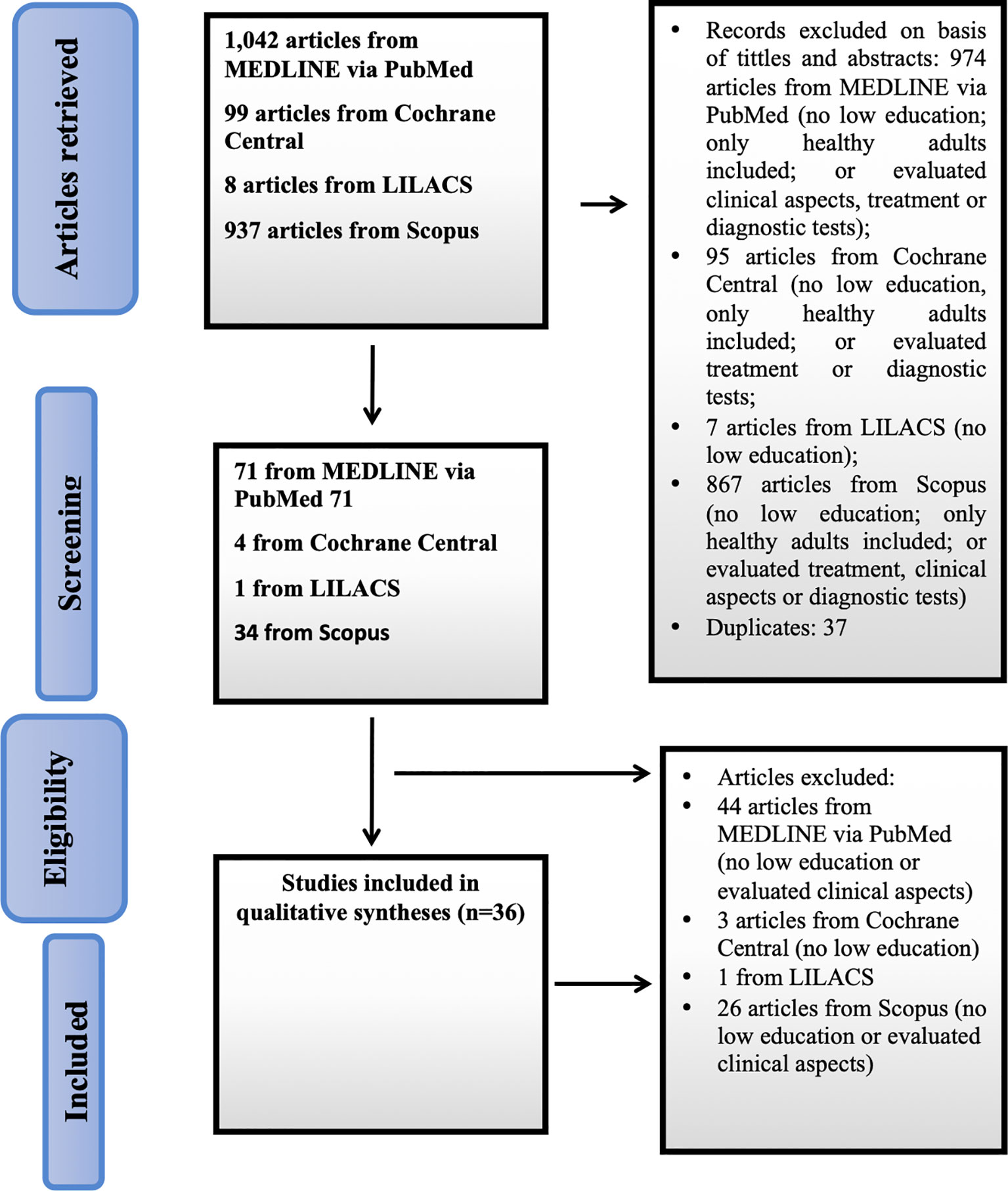
Figure 1 Flowchart of study selection.
A search strategy was created to conduct searches in the following databases: MEDLINE via PubMed from the US National Library of Medicine; LILACS; Cochrane; and SCOPUS via Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) with no time restriction. To expand our search, we chose to use natural controlled language. The following descriptors (bold), synonyms, natural language, and Boolean operators were used to cross-check the databases: MEDLINE (Medical Subject Headings [MeSH]: search strategy—(aged or elderly or old or elder) and (literacy or illiteracy or education or “low education”) and (“mental status and dementia tests” or tool or instrument or status or test) and (“Alzheimer disease” or alzheimer´s) and (“mild cognitive impairment” or “cognitive dysfunction”).
To minimize selection bias (misinterpretation of results and study design), the literature search and data extraction were conducted by two investigators independently and any discrepancies were resolved by consensus.
Results
Figure 1 shows the flowchart of the study selection process according to the PRISMA guidelines. A total of 2,086 articles were retrieved and read. Thirty-six studies were selected for our review.
Table 1 describes the studies assessed. The sample sizes ranged from 50 to 10,432 participants. The studies were conducted in 17 countries, and most of them (13.88%) were from China and Spain.
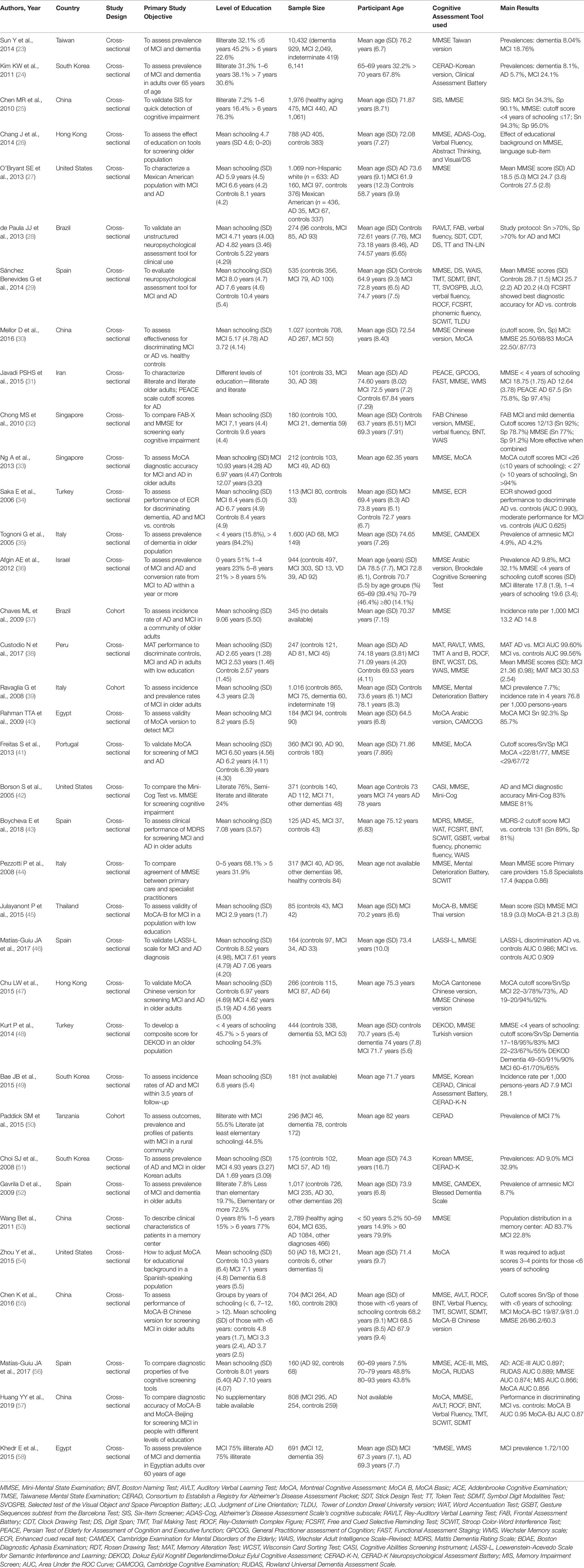
Table 1 Articles included in the integrative literature review.
A wide range of cognitive assessment tools (n = 44) were used for MCI and AD diagnosis (Table 1). Of these, the Mini-Mental State Examination (MMSE) (59) was the most frequently used (86.11%), followed by the Montreal Cognitive Assessment (MoCA) (60) (27.77%).
The studies included in our review evaluated adults with different educational backgrounds. However, detailed information was not available in all studies. Adults with AD had 1.69 (51) to 7.6 years (29) of schooling and those with MCI had 2.53 (38) to 10.93 years (33) of schooling. The proportion of illiterate adults ranged from 1.8% (35) to 32.1% (23).
Most were cross-sectional studies (91.67%), followed by cohort studies (8.33%). Some of the studies (23, 24, 35, 36, 39, 50–52, 58) assessed the prevalence of MCI and AD ranging from 1.72% (58) to 32.9% (52) and 4.2% (35) to 9% (51), respectively. The number of adults with MCI ranged from 12 (58) to 2,049 (30) and the number of adults with AD ranged from 16 (51) to 1,061 (25). Mean age of the study participants ranged from 64.5 (40) to 82 years (50).
The Persian Test of Elderly for Assessment of Cognition and Executive Function (PEACE) was used in one study (28) to establish cutoff scores in individuals with AD. The sample consisted of 38 subjects with AD; some of them were illiterate (proportion not available). A cutoff score of 67.5 was set (sensitivity = 75.8%; specificity = 97.4%). The Six-Item Screener (SIS) was used in another study (25) that evaluated 440 individuals with MCI with a small proportion of individuals (< 25%) with low education (< 6 years of schooling). The SIS showed low sensitivity for screening MCI in this population (sensitivity = 34.3%; specificity = 90.1%). The Memory Alteration Test (MAT) was used in a single study (38) for discriminating MCI and AD from healthy individuals. The AUC of MAT to discriminate between early AD and amnestic mild cognitive impairment (aMCI) was 99.60% (sensitivity = 100.00%; specificity = 97.53%) and to discriminate between aMCI and controls was 99.56% (sensitivity = 99.17%; specificity = 91.11%). The mean score was 17.54 ± 4.67 for individuals with AD, 30.53 ± 2.54 for individuals with MCI and 41.97 ± 2.6 for healthy individuals. AD and MCI individuals and controls had on average 2.65 ± 1.28, 2.53 ± 1.46, and 2.57 ± 1.45 years of education, respectively.
In this review, six studies (Table 2) assessed cutoff scores of the MMSE for adults with 4 years of education or less (25, 36, 38, 40, 45, 48). MCI cutoff scores (SD) ranged from 17.8 (1.9) to 21.36 (0.98), but there was great variation in sensitivity and specificity. The Montreal Cognitive Assessment-Basic (MoCA-B) was evaluated in three studies (45, 55, 57). One of these studies established a cutoff score of 19 for detecting MCI, with 87.9% sensitivity and 81.0% specificity (55). Another one reported a cutoff score (SD) of 21.3 (3.8) for detecting MCI in adults with 4 years of education or less (45). Cutoff scores (SD) for AD ranged from 12.64 (3.78) to 18.32 (2.78) in these same studies. Another cognitive test battery reported was the Addenbrooke’s Cognitive Examination Revised (ACE-R), which was used in only one study but the cutoff score was not adjusted for low educational level. Mean ACE-R scores were 78.12 (12.79) for controls and 53.20 (14.76) for AD. This tool showed good diagnostic accuracy for diagnosing AD (AUC = 0.897) (25).
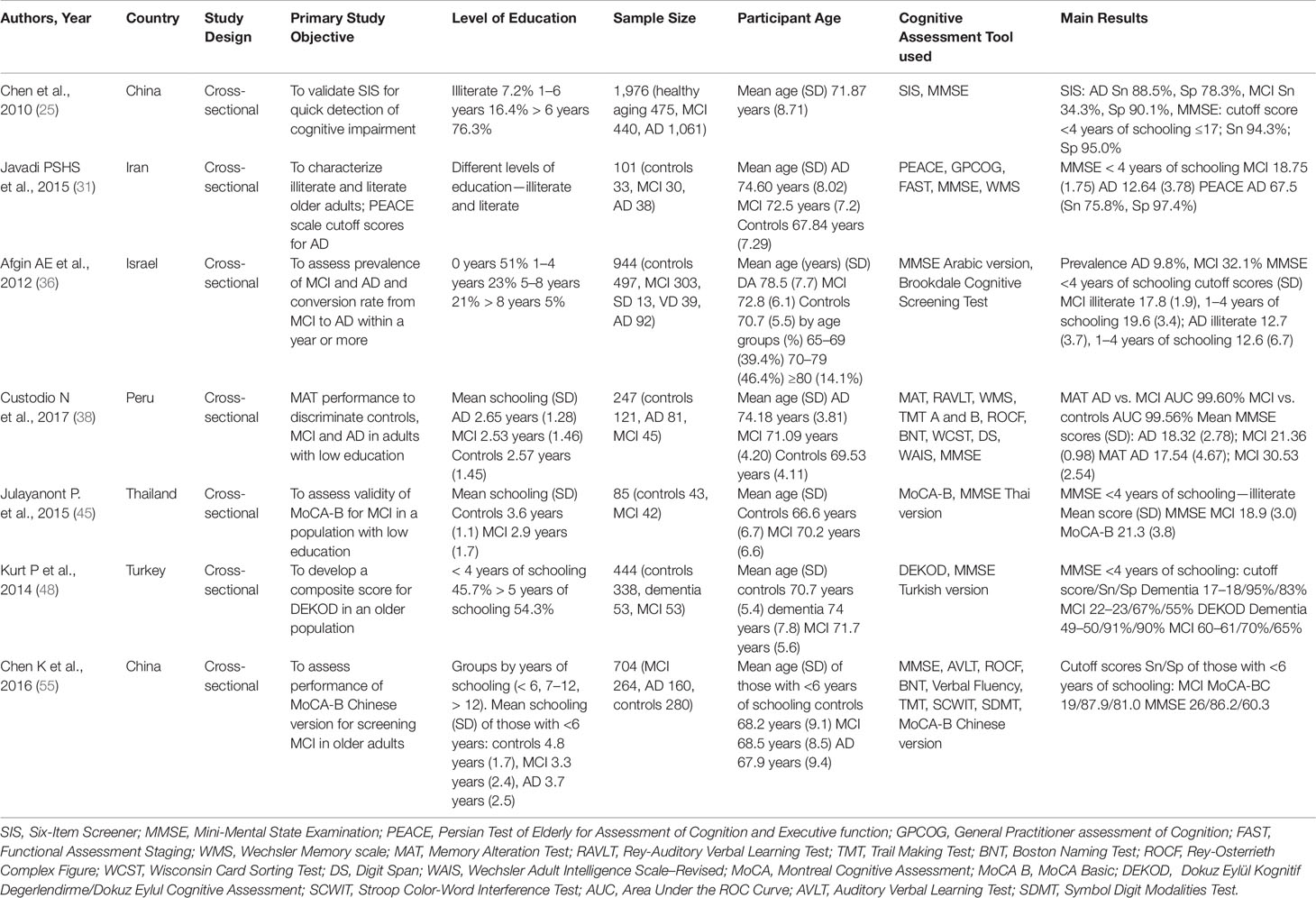
Table 2 Characteristics of studies that established cutoff scores for the MMSE and MoCA in adults with low education.
Discussion
We carried out a critical review of cognitive assessment tools for screening cognitive syndromes in older adults with low levels of education. A significant number of assessment tools (n = 44) were used in the studies reviewed, but only a few of them showed diagnostic accuracy for the diagnosis of MCI and AD in adults with low education including MMSE, MoCA, PEACE, SIS, and MAT. The latter three were each used in one study only.
It is crucial to validate cognitive assessment instruments in populations with low education and to establish cutoff scores for screening these individuals in daily clinical practice. It would enable to monitoring healthy aging in such a quite large population (11) and evaluate older adults with low levels of education who are at risk of developing dementia syndromes (61). Besides, it could offer new insights to better understand the influence of education on cognitive reserve since there is a relationship between literacy and the functional organization of the human brain. Literacy acquisition improves early visual processing and phonological information processing (62). Indeed, functional neuroimaging studies have evidenced that large neural networks in both cerebral hemispheres have less functional connections in less educated individuals (63). Since there has been a move toward the development of disease-modifying drugs for AD, it will be paramount to have validated diagnostic tools for population-based assessments including older adults with low levels of education (64).
In agreement with literature reports, the MMSE was the most frequently used cognitive tool in the studies assessed (65). The MMSE is easy to administer and requires no specialized training and it has been validated in many countries (66). We assessed in our review a study that showed good agreement of the MMSE for cognitive screening (κ = 0.86) between primary care and specialist practitioners (44). However, studies have demonstrated the effect of education on MMSE scores. The MMSE has low sensitivity for MCI, does not perform well in assessing executive functions and has limiting floor and ceiling effects (9, 23, 40). A study conducted in Brazil has established MMSE cutoff scores of 20 for illiterate adults and 25 for those with 4 years of education or less (67).
The second most frequently used cognitive tool was the MoCA. The MoCA is a cognitive battery that includes tests sensitive to executive functions and has higher sensitivity for diagnosing MCI (24, 33, 68). However, MoCA scores are strongly influenced by educational background as MoCA tasks are designed for a certain level of education making it difficult to assess individuals who are either illiterate or with low levels of education (30). Therefore, a MoCA basic version (MoCA-B) was developed to include tasks designed to assess the same cognitive domain regardless of the level of education (45, 60, 68).
A systematic review of cognitive screening tools showed that the ACE-R is an outstanding test battery. It takes approximately 20 minutes to be administered and it includes tasks designed for different levels of schooling (52, 58). In our review, ACE-R cutoff scores for low education were not available.
The studies assessed included recommendations of specific cutoff scores and scales for diagnosis of MCI and AD in adults with low levels of education. One study using the MoCA-B suggested a cutoff score of 19 (55) for MCI diagnosis. For AD, one study showed a cutoff score of 23.5 (30) for the MMSE and another study suggested a cutoff score of 17 (41) for the MoCA.
The scarcity of cognitive assessment tests for evaluating adults with low levels of education is in line with the challenge of assessing cognitive function in individuals with low education (13). Individuals with low levels of education were excluded from many studies because there are no cutoff scores established for several assessment tools. Literacy acquisition increases performance in certain cognitive domains such as executive functions (14), improves visual processing, changes phonological codes, and strengthens the link between phonemic and graphic representation (62) However, to measure literacy through the number of years of formal education is not the most effective approach since there are so many different ways of learning even without attending school (12, 62).
This review study has some limitations that deserve mention. First, no information was available on the diagnostic accuracy of cognitive tools for MCI and AD. Furthermore, little information was available on the diagnostic accuracy of tools for assessing different MCI subtypes and stages of AD. Another caveat is that our search was limited to cognitive assessment tools that require a trained examiner and excluded self-administered and web-based screening tools. Besides, there is no consensus about the definition of low levels of education, which may partly explain heterogeneous results of the cognitive batteries evaluated. Lastly, the studies included this review applied various diagnostic criteria for AD, which prevented comparisons of results across them.
Conclusions
The use of cognitive assessment tools that are easy to administer is still challenging given the high prevalence of low education in the global population. This review provides an overview of the most commonly used instruments for cognitive screening. We found that a small number of studies evaluated adults with 4 years of formal education or less and a wide range of cutoff scores for various cognitive test batteries. Our findings further support the need for the development of specific tools for assessing illiterate adults. Cognitive ability, formal logic, and abstract reasoning should be assessed as they could provide more accurate input for screening and interpretation of cognitive tests in older adults who are either illiterate or with low levels of education. Low-cost test batteries that are easy to administer should be validated because they can make a significant impact on screening of cognitive syndromes and enable early therapeutic interventions aimed at reducing morbidity and mortality of dementia. Further studies of test batteries adjusted to larger groups of adults with low levels of education and specific MCI subtypes and AD stages could help shed light on these points.
Author Contributions
Conception and design of work: JT-J, AS, GA and PB-N. Acquisition, analysis or interpretation of data and work: JT-J, AS, PB-N and GA. Drafting the work: JT-J, AS, GA, JB, JS-N and PB-N. All authors were involved in critical revision of the manuscript for important intellectual content.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the study participants and their families for their collaboration and support.
References
1. Prince M, Wilmo A, Guerchet M, Ali GC, Wu YT, Prina M. World Alzheimer Report 2015: The Global Impact of Dementia an analysis of prevalence, incidence, cost and trends. London: Alzheimer’s Disease International (2015). p. 87. Available from: https://www.alz.co.uk/research/WorldAlzheimerReport2015.pdf (Access in )
2. Petersen RC. Mild cognitive impairment as a diagnostic entity. J Intern Med (2004) 256(3):183–94. doi: 10.1111/j.1365-2796.2004.01388.x
3. Ding D, Zhao Q, Guo Q, Meng H, Wang B, Luo J, et al. Prevalence of mild cognitive impairment in an urban community in china: a cross-sectional analysis of the shanghai aging study. Alzheimers Dement (2015) 11(3):300–9.e2. doi: 10.1016/j.jalz.2013.11.002
4. Petersen RC, Lopez O, Armstrong MJ, Getchius TSD, Ganguli M, Gloss D, et al. Practice guideline update summary: mild cognitive impairment Report of the Guideline Development, Dissemination, and Implementation, Subcommittee of the American Academy of Neurology. Neurol (2018) 90(3):126–35. doi: 10.1212/WNL.0000000000004826
5. Schneider JA, Arvanitakis Z, Leurgans SE, Bennett DA. The Neuropathology of Probable Alzheimer Disease and Mild Cognitive Impairment. Ann Neurol (2009) 66(2):200–8. doi: 10.1002/ana.21706
6. Handels RLH, Vos SJB, Kramberger MG, Jelic V, Blennow K, et al. Predicting progression to dementia in persons with mild cognitive impairment using cerebrospinal fluid markers. Alzheimers Dement (2017) 13(8):903–12. doi: 10.1016/j.jalz.2016.12.015
7. Studart Neto A, Nitrini R. Avaliação cognitiva à beira do leito. In: Frota NAF, Siqueira Neto JI, Balthazar MLF, Nitrini R, editors. Neurologia Cognitiva e do Envelhecimento: do conhecimento básico à abordagem clínica. OmniFarma: São Paulo (2016). p. 433.
8. Orsini A, Pezzuti G, Hulbert S. Beyond the floor effect on the Wechsler Intelligence Scale for Children – 4th Ed.(WISC-IV): calculating IQ and Indexes of subjects presenting a floored pattern of results. J Intellect Disabil Res (2015) 59(5):468–73. doi: 10.1111/jir.12150
9. Dean K, Walker Z, Jenkinson C. Data quality, floor and ceiling effects and test – retest reliability of the Mild Cognitive Impairment Questionnaire. Patient Relat Outcome Meas (2018) 9:43–7. doi: 10.2147/PROM.S145676
10. Everitt BS, Skrondal A. The Cambridge dictionary of statitistics. New York: Cambridge University Press (2010). p. 480.
11. Unesco Institute for Lifelong Learning. 3rd global report on adult learning and education: the impact of adult learning and education on health and well-being, employment and the labour market, and social, civic and community life. Germany: Unesco. (2016), p. 18. Available from: https://unesdoc.unesco.org/ark:/48223/pf0000245917 (Access in September 05, 2019)
12. Tucker-Drob EM, Johnson KE, Jones RN. The cognitive reserve hypothesis: A longitudinal examination of age-associated declines in reasoning and processing speed. Dev Psychol [Internet] (2009) 45(2):431–46. doi: 10.1037/a0014012
13. Mortimer JA, Snowdon DA, Markesbery WR. Head circumference, education and risk of dementia : findings from the nun study. J Clin Exp Neuropsychol (2003) 25(5):671–9. doi: 10.1076/jcen.25.5.671.14584
14. Kosmidis MH, Zafiri M, Politimou N. Literacy versus formal schooling: influence on working memory. Arch Clin Neuropsychol (2011) 26:575–82. doi: 10.1093/arclin/acr063
15. Da Silva CG, Petersson KM, Faísca G, Ingvar H, Reis A. The effects of literacy and education on the quantitative and qualitative aspects of semantic verbal fluency. J Clin Exp Neuropsychol (2004) 26(2):266–77. doi: 10.1076/jcen.26.2.266.28089
16. Wajman JR, Oliveira FF, Schultz RR, Marin SMC, Bertolucci PHF. Educational bias in the assessment of severe dementia: Brazilian cutoffs for severe Mini-Mental State Examination. Arq. Neuro-Psiquiatr (2014) 72(4):273–77. doi: 10.1590/0004-282X20140002
17. Scazufca M, Almeida OP, Vallada HP, Tasse WA, Menezes PR. Limitations of the Mini-Mental State Examination for screening dementia in a community with low socioeconomic status: results from the Sao Paulo Ageing & Health Study. Eur Arch Psychiatry Clin Neurosci (2009) 259(1):8–15. doi: 10.1007/s00406-008-0827-6
18. Whittemore R, Knafl K. The integrative review : updated methodology. J Adv Nurs (2005) 52(5):546–53. doi: 10.1111/j.1365-2648.2005.03621.x
19. Mendes KDS, Silveira RCCP, Galvão CM. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto Contexto – enferm (2008) 17(4):758–64. doi: 10.1590/S0104-07072008000400018
20. Jackson GB. Methods for Integrative Reviews. Rev Educ Res Fall (1980) 50(3):438–60. doi: 10.3102/00346543050003438
21. Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs (2005) 52(5):546–53. doi: 10.1111/j.1365-2648.2005.03621.x
22. Fuchs SC, Paim BS. Revisão Sistemática de Estudos Observacionais com Metanálise. Clinical & Biomedical Research (2010) 30(3). Available at: https://seer.ufrgs.br/hcpa/article/view/16551.
23. Sun Y, Lee HJ, Yang SC, Chen TF, Lin KN, Lin CC, et al. A Nationwide Survey of Mild Cognitive Impairment and Dementia, Including Very Mild Dementia, in Taiwan. PloS One (2014) 9(6):e100303. doi: 10.1371/journal.pone.0100303
24. Kim KW, Park JH, Kim MH, Kim MD, Kim BJ, Kim SK, et al. A nationwide survey on the prevalence of dementia and mild cognitive impairment in South Korea. J Alzheimers Dis (2011) 23(2):281–91. doi: 10.3233/JAD-2010-101221
25. Chen MR, Guo QH, Cao XY, Hong Z, Liu XH. A preliminary study of the Six-Item Screener in detecting cognitive impairment. Neurosci Bull (2010) 26(4):317–21. doi: 10.1007/s12264-010-0106-1
26. Chang J, Tse CS, Leung GT, Fung AW, Hua KT, Chiu HF, et al. Bias in discriminating very mild dementia for older adults with different levels of education in Hong Kong. Int Psychogeriatr (2014) 26(6):995–1010. doi: 10.1017/S1041610214000234
27. O’Bryant SE, Johnson G, Balldin V, Edwards M, Barber R, Williams B, et al. Characterization of Mexican Americans with Mild Cognitive Impairment and Alzheimer’s Disease. J Alzheimers Dis (2013) 33(2):373–9. doi: 10.3233/JAD-2012-121420
28. De Paula JJ, Bertola L, Ávila RT, Moreira L, Coutinho G, de Moraes EN, et al. Clinical Applicability and Cutoff Values for an Unstructured Neuropsychological Assessment Protocol for Older Adults with Low Formal Education. PloS One (2013) 8(9):e73167. doi: 10.1371/journal.pone.0073167
29. Sánchez-Benevides G, Peña-Casanova J, Casals-Coll M, Gramunt N, Molinuevo JL, Gómes-Ansón B, et al. Cognitive and Neuroimaging Profiles in Mild Cognitive Impairment and Alzheimer’s Disease: Data from the Spanish Multicenter Normative Studies (NEURONORMA Project). J Alzheimers Dis (2014) 41(3):887–901. doi: 10.3233/JAD-132186
30. Mellor D, Lewis M, McCabe M, Byrne L, Wang T, Wang J, et al. Determining Appropriate Screening Tools and Cut-Points for Cognitive Impairment in an Elderly Chinese Sample. Psychol Assess (2016) 28(11):1345–53. doi: 10.1037/pas0000271
31. Javadi PSHS, Zendehbad A, Darabi F, Khosravifar S, Noroozian M. Development and implementation of Persian test of Elderly for Assessment of Cognition and Executive function (PEACE). Electron Physician (2015) 7(7):1549–56. doi: 10.19082/1549
32. Chong MS, Lim WS, Chan SP, Feng L, Niti M, Yap P, et al. Diagnostic Performance of the Chinese Frontal Assessment Battery in Early Cognitive Impairment in an Asian Population. Dement Geriatr Cognit Disord (2010) 30(6):525–32. doi: 10.1159/000321665
33. Ng A, Chew I, Narasimhalu K, Kandiah N. Effectiveness of Montreal Cognitive Assessment for the diagnosis of mild cognitive impairment and mild Alzheimer’s disease in Singapore. Singapore Med J (2013) 54(11):616–9. doi: 10.11622/smedj.2013220
34. Saka E, Mihci E, Topcuoglu MA, Balcânica S. Enhanced cued recall has a high utility as a screening test in the diagnosis of Alzheimer’s disease and mild cognitive impairment in Turkish people. Arch Clin Neuropsychol (2006) 21(7):745–51. doi: 10.1016/j.acn.2006.08.007
35. Tognoni G, Ceravolo R, Nucciarone B, Bianchi F, Dell’Agnello G, Ghicopulos I, et al. From mild cognitive impairment to dementia: a prevalence study in a district of Tuscany, Italy. Acta Neurol Scand (2005) 112(2):65–71. doi: 10.1111/j.1600-0404.2005.00444.x
36. Afgin AE, Massarwa H, Schechtman E, Israeli-Korn SD, Strugatsky R, Abuful A, et al. High Prevalence of Mild Cognitive Impairment and Alzheimer’s Disease in Arabic Villages in Northern Israel: Impact of Gender and Education. J Alzheimers Dis (2012) 29(2):431–9. doi: 10.3233/JAD-2011-111667
37. Chaves ML, Camozzato AL, Godinho C, Piazenski I, Kaye J. Incidence of Mild Cognitive Impairment and Alzheimer Disease in Southern Brazil. J Geriatr Psychiatry Neurol (2009) 22(3):181–7. doi: 10.1177/0891988709332942
38. Custódio N, Lira D, Herrera-Perez E, Montesinos R, Castro-Suarez S, Cuenca-Alfaro J, et al. Memory Alteration Test to Detect Amnestic Mild Cognitive Impairment and Early Alzheimer’s Dementia in Population with Low Educational Level. Front Aging Neurosci (2017) 9:278. doi: 10.3389/fnagi.2017.00278
39. Ravaglia G, Forti P, Montesi F, Lucicesare A, Pisacane N, Rietti E, et al. Mild Cognitive Impairment: Epidemiology and Dementia Risk in an Elderly Italian Population. J Am Geriatr Soc (2008) 56(1):51–8. doi: 10.1111/j.1532-5415.2007.01503.x
40. Rahman TTA, Gaafary MME. Montreal Cognitive Assessment Arabic version: Reliability and validity prevalence of mild cognitive impairment among elderly attending geriatric clubs in Cairo. Geriatr Gerontol Int (2009) 9(1):54–61. doi: 10.1111/j.1447-0594.2008.00509.x
41. Freitas S, Simões MR, Alves G, Santana I. Montreal Cognitive Assessment Validation Study for Mild Cognitive Impairment and Alzheimer Disease. Alzheimer Dis Assoc Disord (2013) 27(1):37–43. doi: 10.1097/WAD.0b013e3182420bfe
42. Borson S, Scanlan JM, Watanabe J, Tu SP, Lessig M. Simplifying Detection of Cognitive Impairment: Comparison of the Mini-Cog and Mini-Mental State Examination in a Multiethnic Sample. J Am Geriatr Soc (2005) 53(5):871–4. doi: 10.1111/j.1532-5415.2005.53269.x
43. Boycheva E, Contador I, Fernández-Calvo B, Ramos-Campos F, Puertas-Martín V, Villarejo-Galende A, et al. Spanish version of the Mattis Dementia Rating Scale-2 for early detection of Alzheimer’s disease and mild cognitive impairment. Int J Geriatr Psychiatry (2018) 33(6):832–40. doi: 10.1002/gps.4707
44. Pezzotti P, Scalmana S, Mastromattei A, Di Lallo D. for the “Progetto Alzheimer” Working Group. The accuracy of the MMSE in detecting cognitive impairment when administered by general practitioners: A prospective observational study. BMC Fam Pract (2008) 9:29. doi: 10.1186/1471-2296-9-29
45. Julayanont P, Tangwongchai S, Hemrungrojn S, Tunvirachaisakul C, Phanthumchinda K, Hongsawat J, et al. The Montreal Cognitive Assessment—Basic: A Screening Tool for Mild Cognitive Impairment in Illiterate and Low-Educated Elderly Adults. J Am Geriatr Soc (2015) 63(12):2550–54. doi: 10.1111/jgs.13820
46. Matías-Guiu JA, Curiel RE, Rognoni T, Valles-Salgado M, Fernández-Matarrubia M, Hariramani R, et al. Validation of the Spanish Version of the LASSI-L for Diagnosing Mild Cognitive Impairment and Alzheimer’s Disease. J Alzheimers Dis (2017) 56(2):733–42. doi: 10.3233/JAD-160866
47. Chu LW, Ng KHY, Law ACK, Lee AM, Kwan F. Validity of the Cantonese Chinese Montreal Cognitive Assessment in Southern Chinese. Geriatr Gerontol Int (2015) 15(1):96–103. doi: 10.1111/ggi.12237
48. Kurt P, Keskinoglu P, Yaka E, Uçku R, Yener G. A composite score for Dokuz Eylul Cognitive state neurocognitivetest battery: a door-to-door survey study with illiterate, low and high educated elderly in Turkey. Turk J Geriatr (2013) 17(2):143–51. Available at: https://www.researchgate.net/publication/288575275.
49. Bae JB, Kim YJ, Han JW, Kim TH, Park JH, Lee SB. Incidence of and Risk Factors for Alzheimer’s Disease and Mild Cognitive Impairment in Korean Elderly. Dement Geriatr Cognit Disord (2015) 39(1–2):105–15. doi: 10.1159/000366555
50. Paddick SM, Kisoli A, Samuel M, Higginson J, Gray WK, Dotchin CL, et al. Mild Cognitive Impairment in Rural Tanzania: Prevalence, Profile, and Outcomes at 4-Year Follow-up. Am J Geriatr Psychiatry (2015) 23(9):950–9. doi: 10.1016/j.jagp.2014.12.005
51. Choi SJ, Jung SS, You Y, Shin BS, Kim JE, Yoom SW, et al. Prevalence of Alzheimer’s Dementia and its risk factors in community dwelling elderly Koreans. Psychiatry Invest (2008) 5(2):78–85. doi: 10.4306/pi.2008.5.2.78
52. Gavrila D, Antúnez C, Tormo MJ, Carles R, García Santos JM, Parrilla G, et al. Prevalence of dementia and cognitive impairment in Southeastern Spain: the Ariadna study. Acta Neurol Scand (2009) 120(5):300–7. doi: 10.1111/j.1600-0404.2009.01283.x
53. Wang B, Guo QH, Chen J, Zhao QH, Zhou Y, Hong Z. The clinical characteristics of 2,789 consecutive patients in a memory clinic in China. J Clin Neurosci (2011) 18(11):1473–7. doi: 10.1016/j.jocn.2011.05.003
54. Zhou Y, Ortiz F, Nuñez C, Elashoff D, Woo E, Apostolova LG, et al. Use of the MoCA in Detecting Early Alzheimer’s Disease in a Spanish-Speaking Population with Varied Levels of Education. Dement Geriatr Cognit Disord (2015) 5:85–95. doi: 10.1159/000365506
55. Chen KL, Xu Y, Chu AQ, Ding D, Liang XN, Nasreddine ZS, et al. Validation of the Chinese Version of Montreal Cognitive Assessment Basic for Screening Mild Cognitive Impairment. J Am Geriatr Soc (2016) 64(12):e285–90. doi: 10.1111/jgs.14530
56. Matias-Guiu JA, Valles-Salgado H, Rognoni T, Hamre-Gil F, Moreno-Ramos T, Matias-Guiu J. Comparative Diagnostic Accuracy of the ACE-III, MIS, MMSE, MoCA, and RUDAS for Screening of Alzheimer Disease. Dement Geriatr Cognit Disord (2017) 43(5–6):237–46. doi: 10.1159/000469658
57. Huang YY, Qian SX, Guan QB, Chen KL, Zhao QH, Lu JH, et al. Comparative study of two Chinese versions of Montreal Cognitive Assessment for Screening of Mild Cognitive Impairment. Appl Neuropsychol Adult (2019), 1–6. doi: 10.1080/23279095.2019.1602530
58. Khedr EMH, Fawi G, Abbas MAA, Mohammed TAA, El-Fetoh NA, Attar GSA, et al. Prevalence of Mild Cognitive Impairmentand Dementia among the Elderly Population of Qena Governorate, Upper Egypt: A Community-Based Study. J Alzheimers Dis (2015) 45(1):117–26. doi: 10.3233/jad-142655
59. Folstein MF, Folstein SE, McHugh PR. Mini-mental state: a practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res (1975) 12(3):189–98. doi: 10.1016/0022-3956(75)90026-6
60. Nasreddine ZS, Phillips NA, Bédirian V, Charbonneau S, Whitehead V, Collin I, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for Mild Cognitive Impairment. J Am Geriatr Soc (2005) 53(4):695–9. doi: 10.1111/j.1532-5415.2005.53221.x
61. Roe CM, Xiong C, Miller JP, Morris JC. Education and Alzheimer disease without dementia: support for the cognitive reserve hypothesis. Neurol (2007) 68(3):223–8. doi: 10.1212/01.wnl.0000251303.50459.8a
62. Dehaene S, Cohen L, Morais J, Kolinsky R. Illiterate to literate: behavioural and cerebral changes induced by reading acquisition. Nat Rev Neurosci (2015) 16(4):234–44. doi: 10.1038/nrn3924
63. Marques P, Soares JM, Magalhães R, Santos NC, Sousa N. The bounds of education in the human brain connectome. Sci Rep (2015) 5:12812. doi: 10.1038/srep12812
64. De Roeck EE, Engelborghs S, Dierckx E. Next generation brain health depends on early Alzheimer disease diagnosis: from a timely diagnosis to future population screening. J Am Med Dir Assoc (2016) 17:452–3. doi: 10.1016/j.jamda.2016.02.015
65. De Roeck EE, De Deyn PP, Dierckx E, Engelborghs S. Brief cognitive screening instruments for early detection of Alzheimer’s disease: a systematic review. Alzheimers Res Ther (2019) 11(1):21. doi: 10.1186/s13195-019-0474-3
66. Mitchell AJ. A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. J Psychiatr Res (2009) 43(4):411–31. doi: 10.1016/j.jpsychires.2008.04.014
67. Brucki SMD, Nitrini R, Caramelli P, Bertolucci PHF, Okamoto IH. Sugestões para o uso do mini-exame do estado mental no Brasil. Arq Neuro-psiquiatr (2003) 61(3B):777–81. doi: 10.1590/S0004-282X2003000500014
68. Julayanont P, Phillips N, Chertkow H, Nasreddine ZS. Montreal Cognitive Assessment (MoCA): Concept and clinical review. In: Larner AJCognitive Screening Instruments: A Practical Approach. London: Springer (2013) p. 111–51. Available from: https://www.concordia.ca/content/dam/artsci/research/caplab/docs/Julayanontetal2013MoCAreview.pdf (Access in September)
Keywords: mental status tests, dementia tests, literacy, educational status, mild cognitive impairment
Citation: Tavares-Júnior JWL, de Souza ACC, Alves GS, Bonfadini JdC, Siqueira-Neto JI and Braga-Neto P (2019) Cognitive Assessment Tools for Screening Older Adults With Low Levels of Education: A Critical Review. Front. Psychiatry 10:878. doi: 10.3389/fpsyt.2019.00878
Received: 16 September 2019; Accepted: 07 November 2019;
Published: 13 December 2019.
Edited by:
Fabrizio Piras, Santa Lucia Foundation (IRCCS), ItalyReviewed by:
Sara L. Weisenbach, Stony Brook Medicine, United StatesDeana Davalos, Colorado State University, United States
Copyright © 2019 Tavares-Júnior, de Souza, Alves, Bonfadini, Siqueira-Neto and Braga-Neto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gilberto Sousa Alves, Z3NhbHZlczEyM0Bob3RtYWlsLmNvbQ==
†These authors have contributed equally to this work