 Laura Carballeira Carrera1,2*
Laura Carballeira Carrera1,2* Sarah Lévesque-Daniel2,3
Sarah Lévesque-Daniel2,3 Rahmeth Radjack2,4
Rahmeth Radjack2,4 Marie Rose Moro2,4,5
Marie Rose Moro2,4,5 Jonathan Lachal2,4,5
Jonathan Lachal2,4,5- 1Alicia Koplowitz Short-Term Fellowship, Madrid, Spain
- 2APHP, Hôpital Cochin, Maison de Solenn, Paris, France
- 3Centre integré universitaire de santé et de services sociaux de l'Est-de-l'île-de-Montréal (CIUSSS) du Nord-de-l'Île-de-Montréal, Université de Montréal, Montréal, QC, Canada
- 4Université Paris-Saclay, UVSQ, Inserm, CESP, Team DevPsy, Villejuif, France
- 5Université de Paris, PCPP, Boulogne-Billancourt, France
Background: Cultural context substantially affects the experience and clinical expression of psychiatric diseases, while cultural factors limit both access to and effectiveness of care, especially for migrant families requiring specific types of services. We conducted a scoping review on psychiatric services adapted to cultural diversity, to compare these models of care to the French Transcultural Psychotherapy model.
Methods: Systematic electronic search of databases (PubMed and PsycINFO), manual search of archives of journals dealing with transcultural psychiatry, and consultations with international experts, to identify all papers describing clinical models devoted to psychiatric care for migrants, published between January 1990 and October 2018. Narrative synthesis of the included articles.
Results: The study included 29 papers. The specificities of psychiatric services for migrant families are linked to the host country's migration patterns and citizenship model. In English-speaking countries, specialized services for ethnic minorities offer ethnic matching of the therapist and patient. In Canada, indirect transcultural consultation services have existed since the late 1990s. Australia emphasizes the networking of consultation services and professional training in cultural competence, while the Nordic countries (Sweden, Finland, Norway, and Denmark) focus management on trauma. In France, psychotherapy services, with flexible numbers of therapists involved according to the situation, have existed since 1990.
Discussion: Most initiatives place emphasis on training and supervision, in an indirect approach not specifically focused on the patient, or offer cultural matching of patient and therapist. The French transcultural approach, on the contrary, makes the family's culture and its cultural diversity an integral part of the therapy process.
Background
Julian Tudor Hart set forth his famous Inverse Care Law in the Lancet (1971) (1): “The availability of good medical care tends to vary inversely with the need for it in the population served.” That is, the people who need medical care most receive the least, while its availability is concentrated in the population groups that need it least. Migrants and ethnic minorities are the casualties of this systemic inequality in access to the healthcare system, especially to psychiatric facilities. Reports from the World Health Organization (2) and humanitarian groups such as Doctors of the World (3) reveal that the resources dedicated to psychiatry remain inadequate, are distributed unequally, and used inefficiently. These organizations therefore seek to promote the development of public policies to reverse this situation—indisputably needed in this ever more globalized world, where migrants currently account for hundreds of millions of the world's population (4).
At the macro level, this population faces problems including a lack of health insurance coverage, lack of knowledge of the healthcare system, and linguistic barriers. At a micro level, its members run up against the lack of understanding, prejudices, and negative attitudes of many professionals (5). A therapist, for example, may be less interested in and devote less effort to an intervention with a patient perceived as not cooperating or as having a different system of values and with whom the therapist finds it harder to identify culturally. This affects the quality of the intervention, reproducing the Inverse Care Law (6).
This inequality in access to care has consequences at several levels. On the one hand, migrant families and ethnic minorities underutilize the primary healthcare system, at the same time as they overuse emergency departments. On the other hand, these issues can impede the professionals' understanding of the particular psychopathology and can lead to differences in the prescription of drugs, decisions about hospitalization, availability of psychotherapy, and course under treatment (7, 8).
Added to that are pre- and post-migration factors that act as social determinants of mental health: exposure to violence and traumatic migration experiences, the process of acculturation, situations of loss and mourning, adverse socioeconomic conditions, conflicts due to cultural differences, discrimination, and social isolation (3, 8–10).
Finally, it is appropriate to note the major influence of cultural factors on the ways that diseases and their treatments are conceptualized. In every culture, the manner in which symptoms are experienced and interpreted is part of its systems of meaning, and these meanings will model the ways people in those cultures become sick, or cope with feelings of unease, or seek help (11).
There are two positions about how to work with the cultural diversity of families in the organization of health care. The first expects migrant patients to adapt to conventional care, by normalizing or ignoring the differences. The second position recognizes and seeks to remedy these differences by the development of culturally sensitive approaches and clinical practices. Unfortunately, culture is often mentioned only when there are misunderstandings or at least difficulties in mutual comprehension between the professional and the patient or lack of adherence to treatment. Culture then designates a thing that belongs only to the patient and that represents an obstacle to communication and cooperation (8).
Healthcare systems can adapt in several ways (Table 1): using interpreters and cultural mediators, training professionals in cultural competence and supervision, making innovations in the therapeutic framework of general psychiatric services, and developing specialized clinics for ethnic minorities (8, 10, 12–19). In France, a complete psychotherapeutic method was conceived in the 1980s by T. Nathan and then expanded by MR Moro (one of the authors) for the management of migrant families facing issues that cannot be solved in standard psychotherapy: Transcultural Psychotherapy (TPT). As therapists applying this method, we have reflected at length on the French model, its specificities, and its construction inside the French sociocultural context.
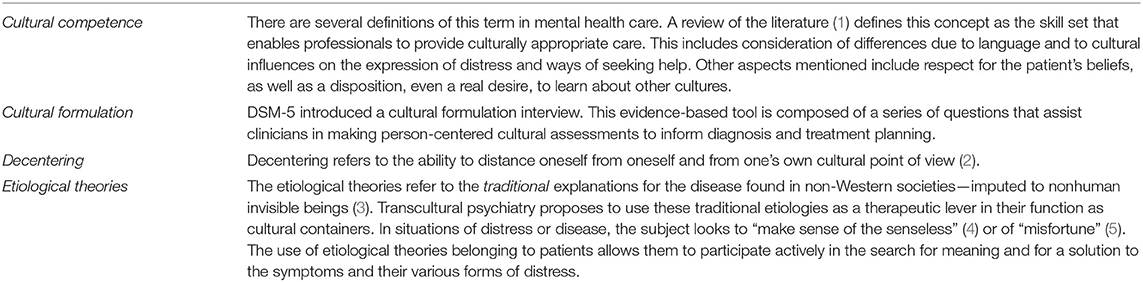
Table 1. Definitions.
We propose to conduct a scoping review to list and describe the multiple ways of providing psychiatric healthcare adapted to cultural diversity and compare these models to the French Transcultural Psychotherapy model, which is the only to propose a complete psychotherapeutic method.
Methods
This is a scoping review of the international literature on clinical approaches to cultural diversity in psychiatric care.
Search (Figure 1)
We used three different strategies for the literature search.
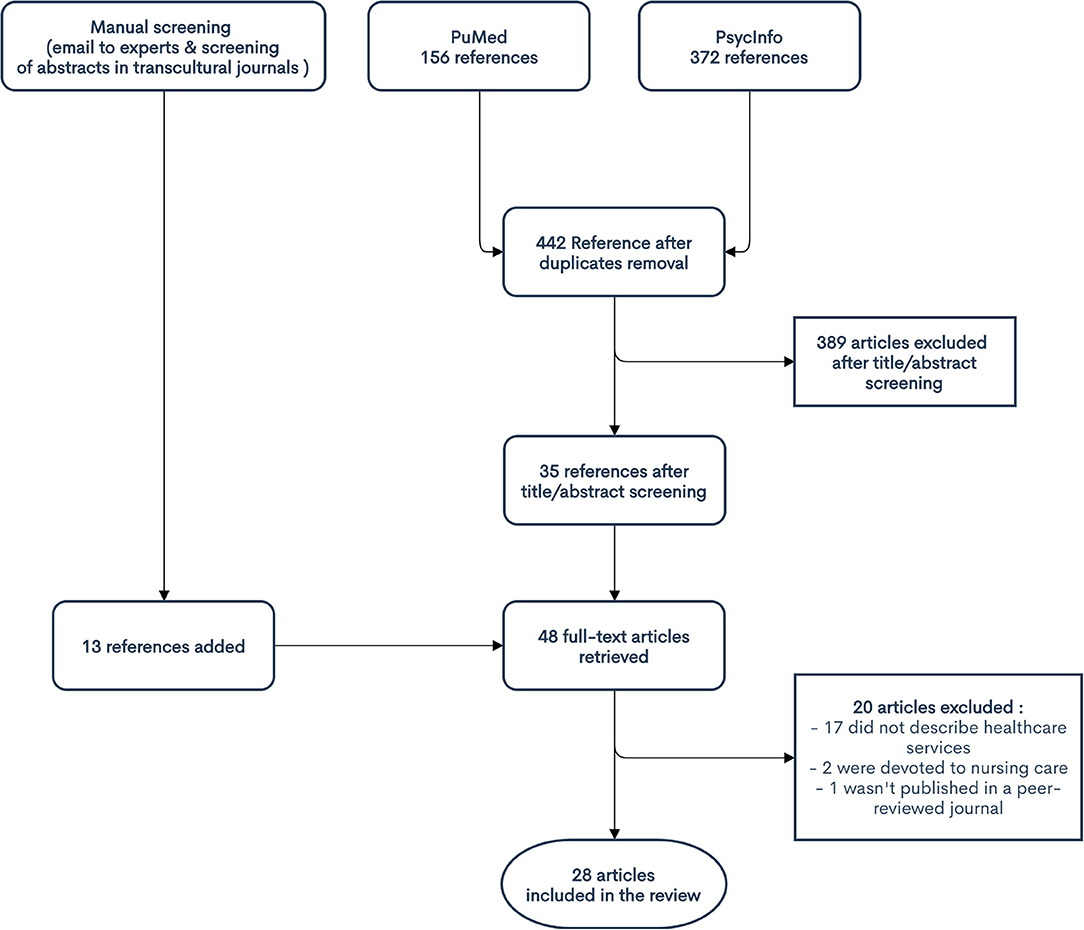
Figure 1. Flowchart of the studies included.
First, on October 1, 2018, we conducted a systematic search for articles identified in the PubMed and PsycINFO databases in response to the Boolean queries in Table 2.
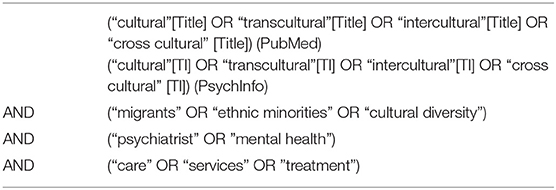
Table 2. Boolean queries for database searches.
After duplicates were removed, 592 titles and abstracts were screened by two researchers (LCC & JL). The inclusion/non-inclusion criteria were the following:
Peer reviewed journal articles (to ensure enough quality on the selected papers
Dealing specifically with clinical models for handling cultural diversity in psychiatric treatment (articles which only referred to transcultural psychiatry at a theoretical level were discarded)
Referring to psychiatric healthcare services that provide care adapted to cultural diversity
Describing the modalities of care
Published between January 1, 1990, and October 1, 2018
In English, French, or Spanish.
Thirty-five full texts were retrieved.
Second, we asked within our international network of transcultural therapists (and researchers) for references to provide any journal article that met these inclusion criteria.
Finally, the research was completed by an analysis of the abstracts of the two principal journals in the national and international transcultural field: L'autre (French) and Transcultural Psychiatry (English).
These methods identified an additional 13 full-text papers.
After full-text screening, 29 papers were finally included in the review.
Quality Appraisal
All the papers included were conceptual articles, and we found no existing checklists by which we could systematically assess their quality. To improve the rigor of our review, we created a simple tool to assess the quality of each paper, shown in Table 3. After the research group constructed the appraisal tool, two researchers (LCC and JL) independently evaluated each paper and the working group reached a consensus about it. Fleiss Kappa was used to measure inter-rater agreement using R software 4.0.2.
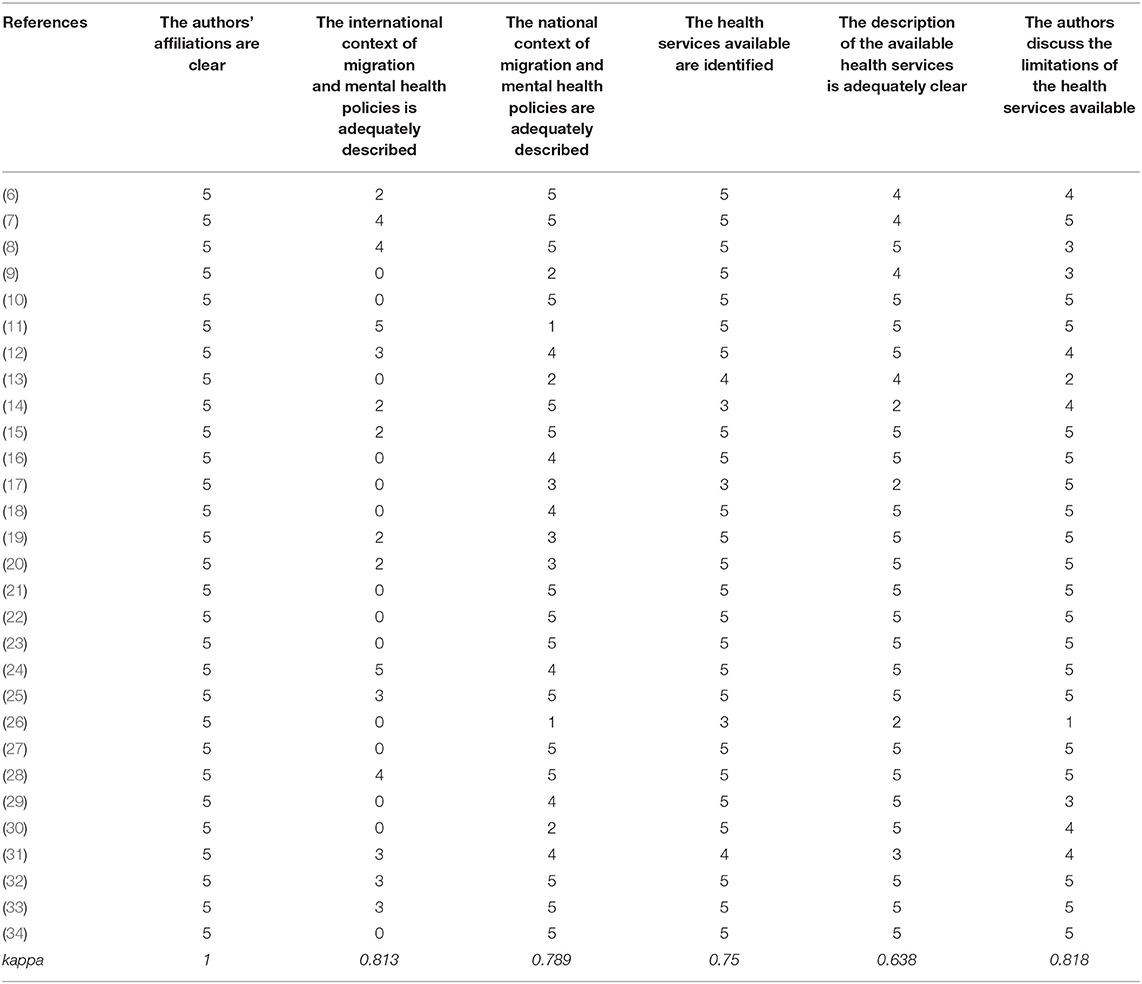
Table 3. Evaluation of the quality of the studies—graded from 0 (absent) to 5 (clear).
Analysis
The articles were read by three authors (LCC, JL, and MRM), and summarized by the first author. The results and their presentation were then discussed during research group meetings. To synthesize them, we looked for similarities between the care models described in the different papers and organized the results inductively. They nonetheless reflect, as previously described in the literature (20), the association of countries' histories, patterns of migration, citizenship models, and particularities in the development of psychiatric services for immigrant populations. The French model is presented in a second part of the results and is then discussed in relation to the different models in the discussion.
Results
This review includes 29 articles. Table 4 presents the principal characteristics of the articles, and Table 5 the principal characteristics of the services and care that the articles describe. Table 6 details the categories of “adaptations of the healthcare system” used by the authors, according to their similarities.
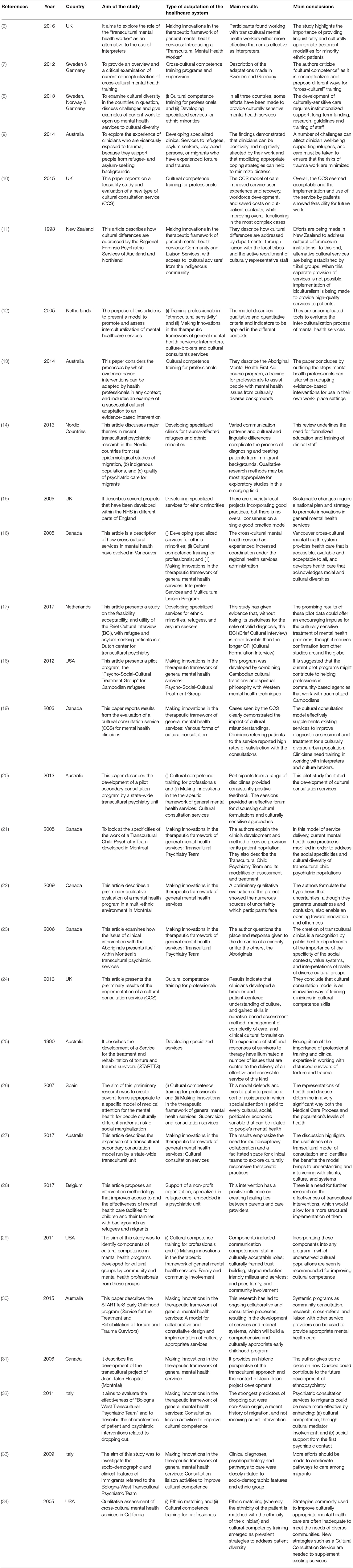
Table 4. Characteristics of the studied included.
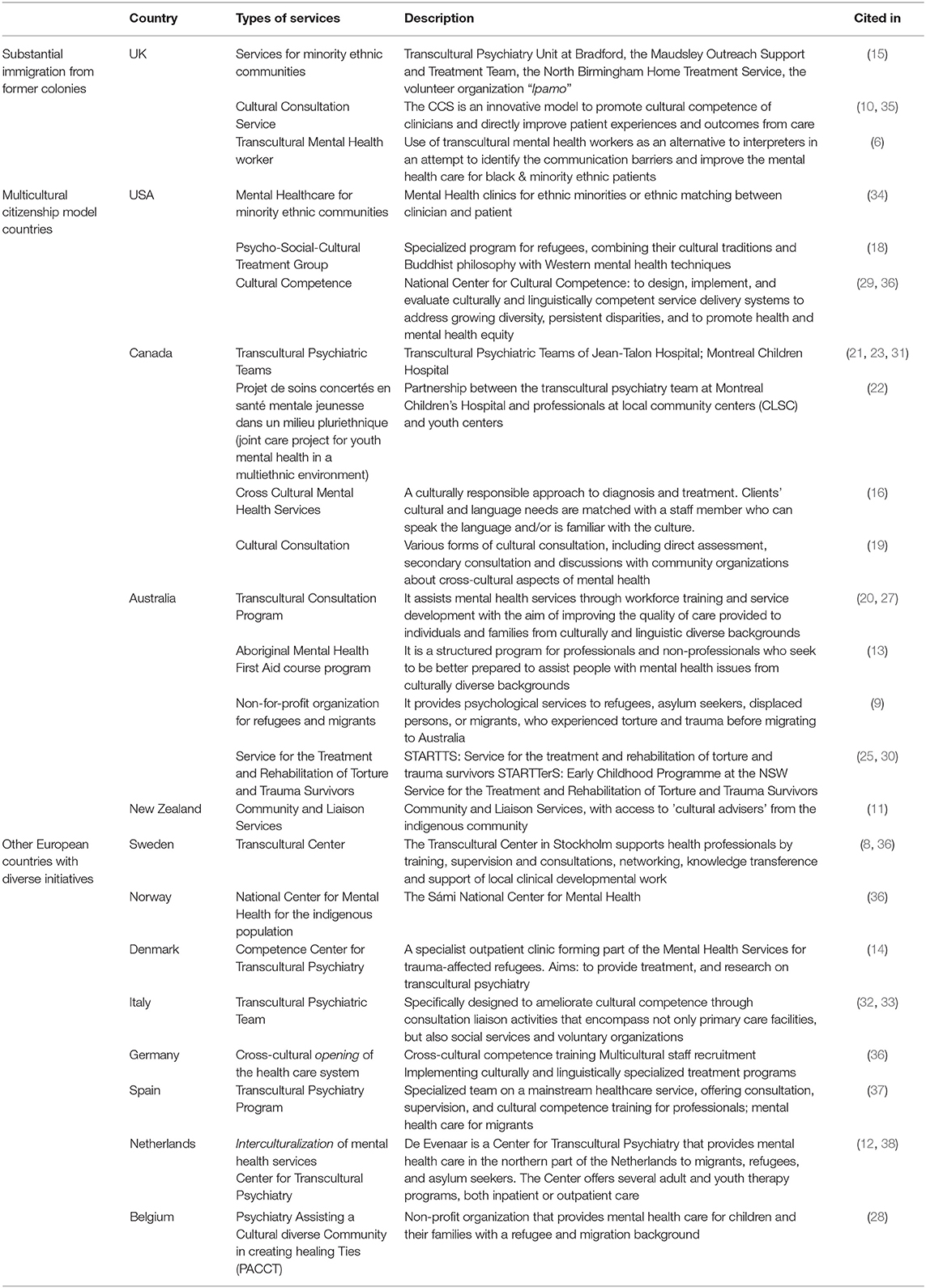
Table 5. Description of the international transcultural services.
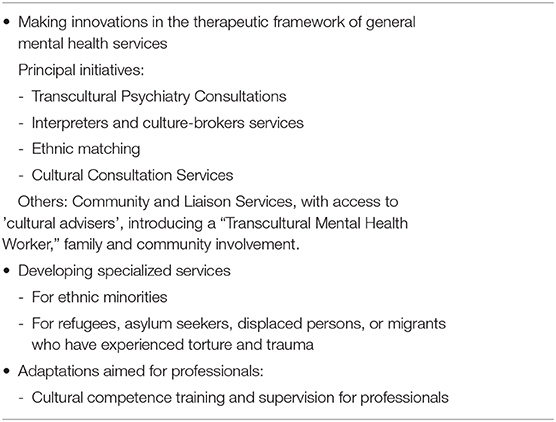
Table 6. Type of adaptation of the healthcare system.
The results of the critical appraisal are reported in Table 3. The quality of the articles was globally good, except for the criterion concerning the description of the international context of immigration policies. No article was excluded solely on the basis of inadequate quality.
The adaptation of psychiatric care to a context of cultural diversity began in English-speaking countries in the 1970s and in France in the 1980s (12, 14).
Different Types of Services Developed Across the World
In this first part, we sketch the different international models described in the literature. As stated above, these models have been regrouped according to their similarities and they reflect the countries' histories, patterns of migration, and citizenship models (20).
First, we find countries such as the United Kingdom and France, which have had substantial immigration from their former colonies. These migrant populations very often faced racism and discrimination on their arrival.
In England, transcultural psychiatry began to develop at the end of the 1970s, with the creation of specialized services for ethnic minorities. Later, professionals were introduced to concepts such as cultural sensitivity, antiracist practices, and misdiagnosis (diagnostic errors due to the failure to take cultural factors into account). Multicultural and multidisciplinary advisory teams appeared, and professionals of varied cultural origins were recruited (12). More recently, the United Kingdom has developed an innovative model: the Cultural Consultation Service (CCS). This is an adaptation of the model developed at McGill University in Canada (and described more fully below), which uses an ethnographic methodology and is based on medical-anthropological knowledge. These departments aim to improve the evaluation, treatment, and outcome of immigrant families. They also seek to act on the structural determinants of inequality in access to psychiatric care and increase the cultural competence of professionals (17, 18). Various practices are therefore recommended without any general consensus around a single model (12).
Some countries, such as the United States, Canada, and Australia, whose populations were shaped by successive waves of migrants, have a multicultural citizenship model. This model promotes the existence of multiple cultural communities within the society. These countries thus tend to recognize cultural diversity and its stakes for health in general. There are also ethnospecific clinics (20).
The United States is a country that was built largely through immigration, but has also been deeply marked by its history of slavery and racism. Despite the existence of policies promoting assimilation, migration flows have led to the preservation of different cultural communities. The development of ethnospecific clinics is a response to this diversity. In these clinics, the professionals know the language and the culture of the community they serve (20, 21). Ethnic matching of therapists and patients is also facilitated in general medical care (8, 22). Moreover, it is recommended that components of cultural competence be incorporated into any psychiatric program covering cultural minorities (22, 23).
The United States is also where ethnopsychiatry and ethnopsychoanalysis were born, after World War II, at the Menninger Clinic (in Kansas until 2002, when it moved to Texas), which used anthropology and clinical practice complementarily and strongly influenced the principal French model (24).
In Canada, cultural identity is considered fairly positively, and the concept of “reasonable accommodation” is relatively widespread. The law encourages pluralism and diversity to preserve the language and culture of ethnic minority groups and to combat racism (20). Cultural psychiatry has attempted to meet the challenges presented by the diversity of the population in general healthcare facilities, beyond the development of ethnospecific services in some cities. At the beginning of the 1990s, combining the Canadian concepts of “multiculturalisme de convivence” (multiculturalism of living together, as opposed to that of dominance) with French ethnopsychoanalytic traditions, several plans for transcultural teams took form in the Montréal region (8, 25, 26). Clinical interventions with multi-ethnic populations and the indigenous are included, as well as a specific Transcultural Child Psychiatry Team (27–29), In 1999, to cope with the limitations of this system, the Cultural Consultation Service (CCS) of McGill University was created. It used a consultation-liaison model, which integrates the medical-anthropological approach and Western psychiatric care. Families are referred by a professional who considers that cultural factors are compromising the evaluation, treatment, or therapeutic relationship. The CCS, with the aid of interpreters and cultural mediators, assembles the information necessary to understand the patients' narratives. The team then researches and drafts a cultural formulation (Table 1), which is submitted to the referring professional, accompanied by treatment guidelines and possible management strategies (8, 30).
In Australia, various services have been developed to meet the needs of ethnic minorities and Indigenous communities. The choice for the Indigenous communities was to give them the control in the development and management of care services. Efforts for migrant families have primarily concentrated on language barriers and cultural competence training for professionals (20, 31). Accordingly, all states and territories in Australia have transcultural mental health resources, funded by the public healthcare system. They make up the Australian Transcultural Mental Health Network, whose function is to support mental health care nationwide, through research, professional training, and innovation in services. Its objective is to improve the accessibility, quality, and cultural appropriateness of mental health care for migrants. Specific innovations include the creation of jobs such as consultant in ethnic mental health and the recruitment of bilingual staff (16, 19, 32). Moreover, specialized services have been developed for the treatment of victims of torture and trauma to help refugees (33, 34).
In New Zealand, cultural differences are addressed through Community and Liaison Services, with access to 'cultural advisers' from the indigenous community (35).
Countries that have not traditionally received large populations of migrants are also now attempting to respond to cultural diversity to provide greater social justice and appropriate care for all patients. In particular, the Nordic countries, which have been culturally homogeneous until recently (except for several indigenous minorities) have experienced an increase in the diversity of their populations. In Sweden, Finland, Norway, and Denmark, special focus has been placed on developing services to treat the sequelae of violence and trauma as well as on training in cultural competence in general healthcare facilities. Psychiatric services specific for indigenous populations have also been set up (5, 36–38).
In other European countries, isolated initiatives have been launched to respond to the increase in cultural diversity. Nonetheless, no government policies have sought to improve the access of migrant families to psychiatric care. Italy, Germany, and Spain have set up teams aimed at providing transcultural training for psychiatric professionals (7, 15, 39, 40). Italy has several transcultural care teams in departments of psychiatry and child psychiatry; not only do they offer consultation-liaison services, but they can conduct psychosocial and psychotherapeutic interventions in the most complex cases (7, 15). In particular, Italy has developed cultural mediators, as in Milan (Crinali) (41). Germany and the Netherlands are trying to guarantee greater cultural openness in public psychiatric facilities (5, 42), while in Belgium this initiative depends more on non-profit organizations (9).
The French Model: Trans cultural Psychotherapy Services, With Flexible Numbers of Therapists Involved According to the Situation
The French citizenship model tends to minimize the importance of cultural differences in individuals in favor of adherence to the shared values of the Republic. Traditionally, the multiculturalism established in France is one that might be called a multiculturalism “of dominance,” in which cultural identity can be expressed in the private sphere but is not recognized or valued in the public sphere. There is a widely shared fear of migrant communities. For the sake of integration, homogenization of these differences is expected in the public space (25, 26). Therefore, health care in France is traditionally considered to be addressed to everyone, with no specificity linked to their cultural origins and without any recognition of the obstacles that might prevent patients from access to these services, which are theoretically available to all.
Nonetheless, French psychiatrists and psychologists who see migrant patients must deal with the limitations of this concept of care. In the 1980s, the first foundations of transcultural psychiatry were laid in France, based on the ethnopsychoanalytic theories developed by Devereux (43). According to Devereux, the basic mechanisms of mental functioning are universal, but the processes of an individual's socialization in their culture of origin must be understood to be able to access this universal dimension, since these cultural processes generate diverse and varied clinical events (10, 14). From this paradigm, Tobie Nathan at the Avicenne Public Hospital created an innovative psychotherapeutic framework intended for migrant families: the ethnopsychiatry group. Marie Rose Moro, who became director of the program in 1989, modified some elements to adapt it to the children of migrants (the second generation). She insists on the importance of the process of cultural métissage (hybridization) and of decentering (Table 1) (14). A group of transcultural therapists is a central element of this flexible service offered to families, and its most original aspect. We will therefore analyze it now, noting that it does not summarize the model, which can also work in small groups or on an individual basis (with or without an interpreter).
This group-based model of transcultural service shares the factors common to all psychotherapy, such as the construction of a narrative, the establishment of a therapeutic relationship, and a variety of specific theoretical and methodological factors (44).
Organization of Transcultural Therapy
Transcultural psychotherapy applies a therapy technique based on two complementary interpretations of symptoms rather than a simultaneous reading. Accordingly, anthropological and clinical psychoanalytic approaches are used. The clinical approaches rest on elements from psychoanalytic parent-children therapy, narrative therapy, and systemic and psychoanalytic family therapy, combined with techniques of cultural mediation (14).
Most often, referrals for transcultural management arise during the treatment of children, when medical, social, educational, or other institutions consider that second-line treatment is needed after the failure of standard management. The indication is stated in terms of the complexity of the situation and of the clinical problem, when the team referring the patient considers a cultural clinical approach necessary. In some cases, these referring teams can be seen in an indirect consultation, that is, without the family, to analyze the interventions and help adapt the care strategies (10, 44).
The first consultations are intended to construct the alliance and the treatment plan with the family. Once the plan is constructed, the usual follow-up is then organized in sufficiently long sessions (around 90 min), scheduled every 6–8 weeks.
Patients are invited to bring their families to these consultations. They are received by a group composed of several therapists of diverse cultural origins and an interpreter-cultural mediator of the same culture as the family, who can interpret successively in both directions (patient-therapist or therapist-patient). At least one professional from the referring team, who is managing and knows the patient, is also invited.
The group is multicultural and multilingual. It is directed by a principal therapist and relies on the trained co-therapists. For the management of children, one of the co-therapists becomes the auxiliary co-therapist for the child, by sitting down to play with him or her, in an area set up for this in the center of the group, with a table, crayons, and games to play. The group represents and embodies otherness and makes it possible to transform this otherness into a therapeutic lever. It thus serves as a support for psychological construction (45). The framework of the group functions as a transitional space in the sense used by Winnicott: a space for listening and receiving, enabling patients to talk about their cultural representations, protected from criticism and lack of understanding. The group holds the family and the child—in Winnicott's sense of “holding” (46). It becomes a transitional space: in the face of the cleavage of migration, the group is a mediator that makes it possible to integrate the culture of origin and that of the host country (14). Finally, management by a group is congruent with the collective approach to care found in traditional societies (8, 14, 45, 47).
The transcultural consultation is a flexible system, and the size of the group can be adapted to the situation. The classic large group includes around 10 co-therapists, as well as trainees. Over the years, the transcultural framework has progressively dealt with new domains, including questions of intergenerational transmission, family dynamics, and child development in the context of migration and even adoption (14, 48). The referrals of unaccompanied minors or patients needing specific work around psychological trauma have required some modifications in the size of the group or the function of the co-therapists (10). Experiments with smaller groups have also been proposed according to the family's cultural origin, when large groups have no particular anthropological interest (in families from Southeast Asia, for example), contrary to the families from North Africa and West Africa, who accounted for most families at the time the group system was created and for whom the group has a protective valence that facilitates expression.
The presence of the interpreter is a key parameter in transcultural work, both at the linguistic level (understanding one another) and the symbolic level (recognizing the identity and singularity of the other). The interpreter enables each family member to speak their own native tongue and to recognize its value to themselves and their children, an element that facilitates the construction of their identity (44, 49). It has been shown that this interpreter has a function as much for second-generation children, speaking French, as for the first generation (49).
Therapeutic Processes
The objective of transcultural therapy is to promote a creative dialogue and a co-construction of personal and family narratives that lean on the representations and experiences of the patients, whether they are individuals, families, or collective groups. The principal therapist gives the floor to participants and is always the person addressed. This mode of communication, which anthropologists call indirect, enables great emotional containment. During the sessions, the co-therapists speak at the principal therapist's request to propose their hypotheses, representations, or images, relying on their own attachments, history, and culture. They may evoke myths, history, traditions, etc. These references to personal experience open the door to a dialogue about cultural complexity and the different readings possible in situations of cultural métissage (hybridization) (10, 14, 44).
On this basis, the group enables the formulation of different conceptions of reality and of what the patient and the family are experiencing. It makes it possible to open the discussion to various—and sometimes divergent—daily realities. This self-disclosure by the group authorizes and supports the family members' self-narrativity. The group accompanies them in a reflexive process in which they can question themselves and transform their subjective representations. Each can thus attain a more flexible and complex self-identification and use all of their skills to find new ways of resolving their conflicts (10, 14, 44, 48).
Finally, the framework enables the emergence of narratives that are difficult to share in the framework of individual therapy. These narratives deal, for example, with migration experiences, questions about cultural métissage, and transmission, but also etiological theories about the origin of both the disease and the distress (10) (Table 1). The etiological theories can thus serve as cultural containers that make it possible to ascribe a meaning to the symptoms and to the psychological distress.
The transcultural group opposes an ethnocentric perspective and promotes transcultural encounters. The viewpoint proposed is that of the wealth and multiplicity that results from situations of métissage. It thus becomes a space where the dominant cultural discourse can be questioned, with the suspension of the psychiatric diagnosis performed from western classifications (14, 48).
The process of decentering is essential to allow this encounter. One of its techniques involves the analysis of cultural countertransference, defined as therapists' explicit and implicit emotional reactions to the otherness of a patient who belongs to a different culture. Therapists try to be aware of these reactions, most often during work with the group, both before and after the consultation (10, 14, 45, 48). This can also take place later, as part of group seminars where they try to describe and then analyze this cultural countertransference.
Discussion
Varied models lead to different methods of taking cultural diversity into account in psychiatric treatment. Nonetheless, most of these initiatives have stressed training and supervision—the approach to care is thus indirect and does not take the patient as its object—or the cultural matching of patient and therapist. The aim of these methods is to modify the framework of care, that is, the services provided, to search for a compromise between the patient and the therapist, etc. The French transcultural pychotherapy approach, on the contrary, is a complete psychotherapeutic method aimed at patients rather than at the framework of care.
The models that offer matching between the therapist and patient by language or ethnicity or both present the problem that in fact language, ethnicity, and culture are not equivalent concepts. Even more, the patients have all taken part in an acculturation process that requires the métissage (mixing or blending) of ways to think about distress. In the French transcultural pychotherapy approach, the therapists of the group are not experts in the patient's culture, but rather in the very concept of culture and cultural attachments. The therapeutic work, which involves understanding and reflecting about the notions of cultural diversity, authorizes the family, with the group's help, to co-construct ways to think about the distress and the disease and to resolve the conflicts. These ways of thinking will in fact be métissées or hybridized, since migrant subjects, whether born abroad or of parents born abroad, are necessarily a hybridization of two cultures, that of their origins and that of their host country (50). The “understanding of cultural diversity” tends to predominate over “cultural competence” today (36).
The co-construction of meaning is a primary objective of the French transcultural pychotherapy approach. The cultural elements of the patients' attachments are not considered to be obstacles, but rather “active catalysts of the care relationship” (10). The patient's culture and various attachments are thus an integral part of the process of therapy. In this sense, the French transcultural approach is radically different from the models proposing to adapt the standard framework of care by training professionals in cultural competence (5, 13, 16, 17, 19, 22, 23, 31, 40, 51) or via integration through using interpreters or cultural mediators (35, 38, 52).
The objective is not to adapt the framework of care to the patients' particularities, but rather to change the paradigm of care. The treatment setting is organized to enable the emergence of cultural theories that explain the symptoms, and the recourse to traditional care by the patient and family, which will be the materials to work on in therapy. The introduction of cultural rationales into therapy and the acceptance and attribution of value to non-Western representations of distress and disease become important symbolic acts, because they belong to the families and to their history, and they can appropriate them or not, according to their desire and their pathway. The therapeutic relationship is thus rebalanced, more symmetric, because the family members put into this therapeutic relationship that which they consider important and which gives meaning to what is happening to them. It is no longer the therapist alone who decides what makes sense. The patient and family members have an active position in this therapy. The group of therapists and the family co-construct the meaning. Accordingly, real therapeutic work can occur; in a situation where it was previously impossible because of the asymmetry inherent in receiving a patient of a minority culture in a facility that symbolizes the majority culture of the host country.
Along the same lines, the models of training and liaison consulting (7, 8, 15–17, 19, 51), all involving advice to first-line therapists by transcultural experts, are limited by the adaptability of standard treatments. To the potential rigidity of the patient's psychological functioning is added the potential rigidity imposed by the type of supervision the patient's therapist receives. Transcultural psychotherapy, on the other hand, is addressed to the patient. Although the presence of the first-line therapist is encouraged to promote the patient's global therapeutic alliance, it is never compulsory, and the impossibility of working with the first-line team is never a per se limitation to the therapeutic work.
Finally, transcultural services are directed to all types of transcultural situations, unlike those aimed at specific symptoms, such as trauma (33, 34, 53) or at a specific type of population or ethnic group (27, 31, 35). The early data of a retrospective study underway show the clinical and cultural wealth of situations encountered (54).
Strengths and Limitations
The scoping review approach presents some limitations. Nevertheless, the reason to choose this type of review was to permit the inclusion of a wide range of sources in order to present a broad overview of the available literature.
As a scoping review, information from a wide range of study designs and methods was gathered. The heterogeneity of the articles made it difficult to use an existing checklist to asses their quality, thus we ourselves created a simple tool to this end.
A broad search was necessary to collect all available information. To overcome this limitation, we used three different strategies for the literature search (systematic search for articles identified in scientific databases, direct questioning of our international network of transcultural therapists, and analysis of the abstracts of the principal journals in the field).
The final outcome of the review was not therefore an answer to a specific question, but rather a synthesized overview of the available literature.
Data Availability Statement
The original contributions generated for this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
All authors participated in every step of the conception of this paper, its writing, and its final approval.
Funding
LC received a grant from the Alicia Koplowitz Foundation (Spain) for a research stay in Maison de Solenn (AP-HP, Cochin Hospital Paris, France), which allowed her to conduct this study.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
With thanks to Jo Ann Cahn for the translation. This manuscript has been released as a pre-print at: https://www.researchsquare.com/article/rs-3501/v2 (55).
References
1. Tudor Hart J. The inverse care law. Lancet. (1971) 297:405–12. doi: 10.1016/S0140-6736(71)92410-X
2. WHO. mhGAP Mental Health Gap Action Programme. Scaling up Care for Mental, Neurological, and Substance use Disorders. Geneva: World Health Organization (2008).
3. Centre Primo Levi Médecins du Monde. La souffrance psychique des exilés: Une urgence de santé publique. Paris: Centre Primo Levi/Médecins du Monde (2018).
4. IOM IO for M. World Migration Report 2018. Geneva: International Organization for Migration (2018).
5. Bäärnhielm S, Jávo C, Mäsko MO. Opening up mental health service delivery to cultural diversity: current situation, development and examples from three northern European countries. Cult Psychiatry. (2013) 33:40–55. doi: 10.1159/000348730
6. Carmona M. Perspectivas en cuidados en salud mental. XI congreso de la AMSM [Video file] [Internet]. (2018) Available online at: https://www.youtube.com/watch?v=RSesión_-5sw6Ik8 https://www.youtube.com/watch?v=RSesión_-5sw6Ik8
7. Tarricone I, Braca M, Atti AR, Pedrini E, Morri M, Poggi F, et al. Clinical features and pathway to care of migrants referring to the Bologna Transcultural Psychiatric Team. Int J Cult Ment Health. (2009) 2:1–15. doi: 10.1080/17542860802560314
8. Kirmayer LJ. Cultural consultation. In: Kirmayer LJ, Guzder J, Rousseau C, editors. Cultural Consultation. Encountering the Other in Mental Health Care. New York, NY: Springer (2014). p. 2–4. doi: 10.1007/978-1-4614-7615-3
9. Serneels G, Villanueva O'Driscoll J, Imeraj L, Vanfraussen K, Lampo A. An intervention supporting the mental health of children with a refugee background. Issues Ment Health Nurs. (2017) 38:327–36. doi: 10.1080/01612840.2017.1285969
10. Radjack R, Rizzi AT, Harf A, Moro MR. Actualités en psychiatrie transculturelle en France. Ann Med Psychol (Paris). (2017) 175:561–6. doi: 10.1016/j.amp.2017.05.004
11. Groleau D, Young A, Kirmayer LJ. The McGill Illness Narrative Interview (MINI): an interview schedule to elicit meanings and modes of reasoning related to illness experience. Transcult Psychiatry. (2006) 43:671–91. doi: 10.1177/1363461506070796
12. Fernando S. Multicultural mental health services: projects for minority ethnic communities in England. Transcult Psychiatry. (2005) 42:420–36. doi: 10.1177/1363461505055624
13. Ganesan S, Janzé T. Overview of culturally-based mental health care in Vancouver. Transcult Psychiatry. (2005) 42:478–90. doi: 10.1177/1363461505055628
14. Sturm G, Heidenreich F, Moro M. Transcultural Clinical work with immigrants, asylum seekers and refugees at Avicenne Hospital, France. Int J Migr Heal Soc Care. (2009) 4:33–40. doi: 10.1108/17479894200800022
15. Tarricone I, Atti AR, Braca M, Pompei G, Morri M, Poggi F, et al. Migrants referring to the Bologna Transcultural Psychiatric Team: reasons for drop-out. Int J Soc Psychiatry. (2011) 57:627–30. doi: 10.1177/0020764010382368
16. McDonough S, Chopra P, Tuncer C, Schumacher B, Bhat R. Enhancing cultural responsiveness: the development of a pilot transcultural secondary consultation program. Australas Psychiatry. (2013) 21:494–8. doi: 10.1177/1039856213501562
17. Owiti JA, Ajaz A, Ascoli M, de Jongh B, Palinski A, Bhui KS. Cultural consultation as a model for training multidisciplinary mental healthcare professionals in cultural competence skills: preliminary results. J Psychiatr Ment Health Nurs. (2014) 21:814–26. doi: 10.1111/jpm.12124
18. Bhui K, Warfa N, Edonya P, McKenzie K, Bhugra D. Cultural competence in mental health care: a review of model evaluations. BMC Health Serv Res. (2007) 7:15. doi: 10.1186/1472-6963-7-15
19. Santhanam-Martin R, Fraser N, Jenkins A, Tuncer C. Evaluation of cultural responsiveness using a transcultural secondary consultation model. Transcult Psychiatry. (2017) 54:488–501. doi: 10.1177/1363461517724984
20. Kirmayer LJ, Minas H. The future of cultural psychiatry: an international perspective. Can J Psychiatry. (2000) 45:438–46. doi: 10.1177/070674370004500503
21. Montijo JA, Juan S, Rico P. Therapeutic relationships with the poor: a Puerto Rican perspective. Psychotherapy. (1985) 22:436–40. doi: 10.1037/h0085525
22. Ton H, Koike A, Hales RE, Johnson Jo A, Hilty DM. A qualitative needs assessment for development of a cultural consultation service. Transcult Psychiatry. (2005) 42:491–504. doi: 10.1177/1363461505055629
23. Siegel C, Haughland G, Reid-Rose L, Hopper K. Components of cultural competence in three mental health programs. Psychiatr Serv. (2011) 62:626–31. doi: 10.1176/ps.62.6.pss6206_0626
25. Sironi F, de La Noë Q, Cao Huu Hai E, Fermi P, Mestre C, Abdessalem Y, et al. Quelques lieux de consultation d'ethnopsychiatrie. Carnet Psy. (1998) 33:19–27.
26. Sterlin C. L'ethnopsychiatrie au Québec : bilan et perspectives d'un témoin acteur clé. Sante Ment Que. (2006) 31:179. doi: 10.7202/014811ar
27. Noël D. Mental health for the Aboriginals: a transcultural response. Ethnopsychiatrie. (2006) 31:153–64. doi: 10.7202/014809ar
28. Measham T, Rousseau C, Nadeau L. The development and therapeutic modalities of a transcultural child psychiatry service. Can Child Adolesc Psychiatr Rev. (2005) 14:68–72.
29. Nadeau L, Rousseau C, Séguin Y. Preliminary qualitative evaluation of a shared-care mental health programme with youths in Montréal: facing institutional and cultural uncertainty. Santé Ment en première ligne. (2009) 43.
30. Kirmayer LJ, Groleau D, Guzder J, Blake C, Jarvis E. Cultural consultation: a model of mental health service for multicultural societies. Can J Psychiatry-Revue Can Psychiatr. (2003) 48:145–53. doi: 10.1177/070674370304800302
31. Doyle K, Hungerford C. Adapting evidence-based interventions to accommodate cultural differences: where does this leave effectiveness? Issues Ment Health Nurs. (2014) 35:739–44. doi: 10.3109/01612840.2014.901452
32. Barrington AJ, Shakespeare-Finch J. Giving voice to service providers who work with survivors of torture and trauma. Qual Health Res. (2014) 24:1686–99. doi: 10.1177/1049732314549023
33. Reid J, Silove D, Tarn R. The Development of the New South Wales Service for the Treatment and Rehabilitation of Torture and Trauma Survivors (STARTTS): the first year. Aust New Zeal J Psychiatry. (1990) 24:486–95. doi: 10.3109/00048679009062904
34. Signorelli RG, Coello M, Momartin S. Change and recovery: culturally appropriate early childhood programmes with refugee families and communities. Child Aust. (2015) 40:195–204. doi: 10.1017/cha.2015.29
35. Chaplow D, Chaplow R, Winston T. Addressing cultural differences in institutions: changing health practices in New Zealand. Crim Behav Ment Heal. (1993) 3:307–21. doi: 10.1002/cbm.1993.3.4.307
36. Shahnavaz S, Ekblad S. Understanding the culturally diverse in psychiatry rather than being culturally competent–a preliminary report of Swedish Psychiatric Teams' views on transcultural competence. Int J Migr Heal Soc Care. (2007) 3:14–30. doi: 10.1108/17479894200700024
37. Ekblad S, Kastrup MC. Current research in transcultural psychiatry in the Nordic countries. Transcult Psychiatry. (2013) 50:841–57. doi: 10.1177/1363461513511181
38. Groen SPN, Richters A, Laban CJ, Devillé WLJM. Implementation of the Cultural Formulation through a newly developed Brief Cultural Interview: pilot data from the Netherlands. Transcult Psychiatry. (2017) 54:3–22. doi: 10.1177/1363461516678342
39. Sanjuan L. Propuesta de materiales para atención en salud mental en un contexto intercultural. Rev Recer i Form en Antropol. (2007) 6:1–32. doi: 10.5565/rev/periferia.169
40. Bäärnhielm S, Mösko M. Cross-cultural training in mental health care–challenges and experiences from Sweden and Germany. Eur Psychiatry. (2012) 27:70–5. doi: 10.1016/S0924-9338(12)75711-5
42. de Jong JTVM, Van Ommeren M. Mental health services in a multicultural society: interculturalization and its quality surveillance. Transcult Psychiatry. (2005) 42:437–56. doi: 10.1177/1363461505055625
43. Devereux G. De l'angoisse à la méthode dans les sciences du comportement. Paris: Flammarion (1967). p. 474.
44. Moro MR, De La Noë Q, Mouchenik Y. Manuel de psychiatrie transculturelle. Grenoble, France: La pensée (2006).
45. Moro MR. Comprendre et soigner. La consultation d'Avicenne: un dispositif métissé et cosmopolite. Bobigny: Association Internationale d'EthnoPsychanalyse (2016).
47. Sturm G, Guerraoui Z, Bonnet S, Gouzvinski F, Raynaud JP. Adapting services to the needs of children and families with complex migration experiences: the Toulouse University Hospital's intercultural consultation. Transcult Psychiatry. (2017) 54:445–65. doi: 10.1177/1363461517724277
48. Sturm G, Nadig M, Moro MR. Current developments in French ethnopsychoanalysis. Transcult Psychiatry. (2011) 48:205–27. doi: 10.1177/1363461511402868
49. Rousseau C, Measham T, Moro MR. Working with interpreters in child mental health. Child Adolesc Ment Health. (2011) 16:55–9. doi: 10.1111/j.1475-3588.2010.00589.x
50. Moro MR. Parents-enfants en situation migratoire: une nouvelle clinique des métissages. In: Baubet T and Moro MR, editors. Psychopathologie transculturelle. Paris: Elsevier Masson (2009). doi: 10.1016/B978-2-294-70434-5.00010-1
51. Bhui KS, Owiti JA, Palinski A, Ascoli M, De Jongh B, Archer J, et al. A cultural consultation service in East London: experiences and outcomes from implementation of an innovative service. Int Rev Psychiatry. (2015) 27:11–22. doi: 10.3109/09540261.2014.992303
52. Arafat NM. Language, culture and mental health: a study exploring the role of the transcultural mental health worker in Sheffield, UK. Int J Cult Ment Health. (2016) 9:71–95. doi: 10.1080/17542863.2015.1112419
53. Han M, Valencia M, Lee YSOO, Leon JDE. Development and implementation of the culturally competent program with cambodians: the pilot psycho-social-cultural treatment. J Ethn Cult Divers Soc Work. (2012) 21:212–30. doi: 10.1080/15313204.2012.700494
54. Lachal J, Simon A, Hassler C, Barry C, Camara H, Massar IN, et al. An epidemiological description of 529 families treated by the French method of Transcultural Psychotherapy: a decade of experience. PLoS ONE. (2020) 15: e0236990. doi: 10.1371/journal.pone.0236990
55. Carballeira Carrera L, Lévesque-Daniel S, Radjack R, Moro MR, Lachal J. Clinical approaches to cultural diversity in mental health care and specificities of French transcultural consultations: a narrative review Available online at https://www.researchsquare.com/article/rs-3501/v2
Keywords: transcultural psychiatry, migrant families, mental healthcare, psychiatric care, cultural diversity
Citation: Carballeira Carrera L, Lévesque-Daniel S, Radjack R, Moro MR and Lachal J (2020) Clinical Approaches to Cultural Diversity in Mental Health Care and Specificities of French Transcultural Consultations: A Scoping Review. Front. Psychiatry 11:579147. doi: 10.3389/fpsyt.2020.579147
Received: 31 July 2020; Accepted: 02 October 2020;
Published: 27 October 2020.
Edited by:
Ashwani Kumar Mishra, All India Institute of Medical Sciences, IndiaReviewed by:
Mona Pathak, Kalinga Institute of Medical Sciences (KIMS), IndiaSiddharth Sarkar, All India Institute of Medical Sciences, India
Copyright © 2020 Carballeira Carrera, Lévesque-Daniel, Radjack, Moro and Lachal. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laura Carballeira Carrera, bGF1cmEuY2FyYmFsbGVpcmFAc2FsdWQubWFkcmlkLm9yZw==