 Diana Roeg1,2*
Diana Roeg1,2* Lars de Winter3
Lars de Winter3 Cris Bergmans3Chrisje Couwenbergh3Peter McPherson4
Cris Bergmans3Chrisje Couwenbergh3Peter McPherson4 Helen Killaspy4
Helen Killaspy4 Jaap van Weeghel2,3
Jaap van Weeghel2,3- 1Research Department, Kwintes Supported Housing, Zeist, Netherlands
- 2Academic Center Mental Health, Tranzo, Tilburg University, Tilburg, Netherlands
- 3Phrenos Center of Expertise for Severe Mental Illness, Utrecht, Netherlands
- 4Division of Psychiatry, University College London, London, United Kingdom
Background: People with severe mental illness have difficulties finding and maintaining competitive employment. This is particularly so for those living in supported housing who, by definition, have significant day-to-day support needs: in the Netherlands only 3 to 5% of people with serious mental health problems who live in supported housing are competitively employed. To support these people in finding and maintaining competitive employment, Individual Placement, and Support (IPS) was introduced within supported housing services in the Netherlands in 2015. As this is the first country that broadly implemented IPS in supported housing settings, this paper will focus on the first results regarding feasibility and effects on employment in clients of IPS in this sector.
Methods: We investigated the feasibility and employment outcomes of delivering IPS in supported housing services using fidelity assessments and quarterly employment outcomes on IPS program level within eight supported housing organizations, and compared these with 21 mental health treatment organizations in the Netherlands over a 4 year period. We investigated possible reasons for our findings and their implications through qualitative evaluations of the IPS fidelity assessors' notes and additional focus groups with IPS specialists and coordinators from supported housing services and fidelity assessors.
Results: The overall fidelity scores indicated reasonable implementation of the IPS model within both supported housing services and mental health services. However, there were differences between services with regard to specific fidelity items; mental health treatment organizations scored higher for team integration, whereas supported housing services scored higher for rapid job search and caseload size, diversity of jobs, and employers. Our qualitative data suggested that the difference in team integration between the two sectors was due to differences in their organizational and financial structures, as well as in the specific needs of their clients. Conversely, supported housing services had better connections with employers which facilitated more rapid job searching and greater diversity in employment opportunities. The average total client employment rate did not significantly differ; and was 25.8% per quarter in supported housing services and 29.6% in mental health treatment services.
Conclusion: Implementing IPS in supported housing settings is both feasible and effective.
Introduction
People with severe mental illness face particular difficulties with meaningful social participation; research suggests that factors such as hospitalization, time spent in therapy, stigma and a lack of relevant skills, experiences, and educational opportunities, may limit the capacity and opportunity of individuals with severe mental illness to participate in valued social activities (1–3). This situation is worse for people with serious mental health problems living in supported housing services, who, by definition, have higher support needs with regard to activities of daily living and interpersonal skills and are at greater risk of social exclusion (1, 4–7). Employment is a key factor in the social recovery of persons with mental health problems; being in competitive employment can have numerous advantages for clients, beyond financial independence, such as improved mental health, self-esteem, personal recovery, and quality of life (8, 9). However, employment rates are lower amongst persons with severe mental illness compared to the general population. National surveys in the Netherlands have found that only 10–17% of clients with severe mental illness under the care of mental health services were competitively employed, with no indication that this situation is improving over time (10–12). For clients living in supported housing, the employment rate is even lower; despite there being no differences with clients from mental health treatment services in financial disincentives for working in terms of any impact on the individual's welfare benefits, only 3–5% of this group are reported to be competitively employed (5). These data highlight the need for broader implementation of vocational rehabilitation and supported employment services within the Netherlands, specifically targeting people with severe mental illness living in supported housing settings.
Individual Placement and Support (IPS) is a specific model of supported employment, developed to assist people with mental health problems find and maintain competitive employment (13). The model involves embedding a specific employment specialist within a community mental health team, and follows eight basic principles: the goal of competitive employment for clients; zero exclusion, and eligibility based on client choice; attention to client preferences; rapid job search; integration of employment services and mental health treatment; personalized welfare benefits counseling; targeted job development; and individualized, long-term support. IPS has been implemented in many parts of the world, across North America, Europe, Asia, and Australia, and its effectiveness has been extensively investigated (14). Numerous systematic reviews and meta-analyses have demonstrated the superiority of IPS over traditional vocational services, across multiple employment outcomes [see (15–19)]. In the Netherlands, a 30-month randomized controlled trial demonstrated the positive effects of IPS, with the intervention leading to greater improvements in employment outcomes for people with severe mental illness, when compared to other vocational services (9). Until recently, IPS had primarily been implemented within mental health treatment settings in the Netherlands; since 2015, however, it has also been implemented in supported housing services. Offering IPS in this setting extends the accessibility of evidence based vocational services, and complements existing vocational services already provided by supported housing staff.
In the current study, we examined IPS model fidelity and employment outcomes in supported housing services and mental health treatment services. Additional qualitative investigations were conducted to assist interpretation of the findings. The main research questions were: 1. How is IPS implemented in supported housing services, compared to mental health treatment services? 2. How are differences in the implementation of IPS between supported housing and mental health treatment services explained? 3. What are the employment outcomes in supported housing services?
Methods
Context
In the Netherlands, most clients (72.5%) of supported housing services receive floating outreach (ambulatory support), where support is provided in the service users own home (5). The remaining services offer accommodation-based support, typically organized as grouped apartments, with or without a shared living room and kitchen, and staff support available up to 24 h a day on-site (20, 21). In terms of the Simple Taxonomy for Supported Accommodation, these reflect Type 4 (individual accommodation, low/moderate support and no staff on-site), Type 2 and Type 3 services (congregate setting, high to moderate support, strong emphasis on move-on) (7). All service types have a strong emphasis on recovery and rehabilitation. Supported housing services provide support of varying intensity, addressing a range of service user needs including practical assistance with medication management, personal care, cooking, cleaning, and financial administration, and rehabilitative support to gain the skills and confidence to manage these tasks and to achieve personal goals in social and vocational domains (22, 23). Supported housing service users in the Netherlands are predominately male (65%), with a mean age between 44 and 50 years; approximately half have a primary diagnosis of a psychotic disorder (5, 22). Most supported housing clients (81%) receive additional treatment from mental health treatment services and, before moving to supported housing, most had either been hospitalized (36%) or living independently (43%) (22, 24). Any client with severe mental illness living in supported housing or receiving care from a mental health treatment organization who wishes to seek competitive work, is eligible for IPS.
Sample
In the Netherlands, IPS outcome data and fidelity assessments have been collected nationally since 2016. IPS fidelity assessments are conducted by nine trained fidelity assessors, unaffiliated with the assessed IPS program, or organization. Program fidelity is assessed every 2 years and employment outcome data are collected every 3 months by the local IPS coordinator. The data are sent to the data coordinator of Phrenos Center of Expertise (LdW), who completes a quality check of accuracy, and consistency with the outcome reporting manual, before processing the data. For the current study, we analyzed data collected up to the end of 2019, including outcome and fidelity data from eight IPS programs within supported housing services, and 21 IPS programs within mental health treatment organizations.
Measurements and Data Collection
Fidelity
During a full-day visit at the IPS program, two fidelity assessors conduct fidelity assessments according to the procedure described by Becker et al. (25). Data are collected from five different sources: interviews with IPS specialists, staff members, clients, family members and directors, observations of team meetings and vocational unit meetings, and review of program documents and client records. After the completion of the visit, assessors independently complete a 25-item fidelity rating scale (see below). Any rating discrepancies are discussed to achieve consensus ratings. Qualitative remarks are added for each item, when relevant, and programs receive a report with recommendations to help them improve quality.
IPS fidelity is assessed using the 25-item IPS fidelity scale (25). Each item is rated on a 5-point scale, ranging from 1 (no implementation) to 5 (full implementation), with intermediate numbers representing progressively greater degrees of implementation (25). The total score of the IPS fidelity scale is generated by summing all item scores, producing a total score ranging from 25 to 125 points. The scale developers defined benchmarks to assess descriptive labels regarding IPS fidelity (26). IPS programs scoring between 74 and 99 are considered to have ‘fair’ fidelity, programs scoring between 100 and 114 have “good” fidelity and programs scoring between 115 and 125 have “exemplary” fidelity. IPS programs scoring below 74 are considered to provide “no IPS,” indicating that IPS was not implemented in accordance with the model (25). The IPS-25 scale has good internal consistency (α = 0.88) and moderate predictive validity (r = 0.34) (26). Previous reports indicate that fidelity scores are positively associated with employment outcomes, and that improvement in fidelity scores predict improvement of program-level employment outcomes over time (26, 27). Therefore, fidelity assessment is a crucial element for quality improvement of IPS services.
Program Characteristics and Employment Outcomes
Data relating to program characteristics and employment outcomes are collected using a Dutch translation of the IPS Quarterly Employment Reporting Form (28). The form is administered quarterly and allows for the collection of the following data: the number of clients that received IPS, the number of clients that were competitively employed; the number of clients that left IPS services, and; the number and full-time equivalent of all employment specialists working in the IPS program. Employment rates are considered to be the main program outcomes, and are calculated by dividing the total number of clients competitively employed during the quarter by the total number of clients on the IPS workers' caseload over the same time frame. The total caseload is a dynamic cohort with clients leaving and joining the program at variable times. In order to achieve consistency in the reporting and interpretation of each variable on the Employment Reporting Form, definitions are provided in a manual for use by all IPS programs.
Data Management
Each IPS program initiated IPS fidelity reviews, and submitted outcome data, at different time points between 2016 and 2019; programs were also at varying stages of implementation. Therefore, we used the first outcome report and fidelity assessment of each IPS program as the baseline measurement for our longitudinal analysis of each outcome. As each IPS program commenced at a different date, the time span of the data available per program differed; very few programs were in operation for the entire 4 year period. As such, we were only able to collate an overview of program characteristics and employment outcomes over the first 3 years from the start of implementation of IPS.
Focus Groups
As described above, fidelity assessors are able to provide comments on each item of the IPS fidelity scale. We used thematic analysis to analyze these comments, with the intention of providing a more complete understanding of the context and reasoning that led to the fidelity scores. We also organized a focus group with IPS assessor trainers and employment specialists involved in IPS coordination within the eight supported housing services. In this focus group, we discussed the validity of our findings from the thematic analysis, and explored participants' experiences and challenges with IPS implementation in supported housing services, with particular emphasis on fidelity items that differed between the sectors. The focus group was co-facilitated by DR and LW, with one co-facilitator taking notes. The focus group was audio recorded.
Ethical Approval
As per national legislation and standards, including the Medical Research Involving Human Subjects Act, and the Netherlands Code of Conduct for Research Integrity, ethical approval was not required for this study. The research relied on secondary analyses of national available data; focus group participants provided informed consent to participate.
Data-Analysis
Quantitative Data Analysis
Program Characteristics and Employment Outcomes
We performed descriptive analyses of program characteristics (i.e., the number of clients receiving IPS, the number of clients newly enrolled in IPS, the number of clients that ended IPS services and the number and full-time equivalent of all employment specialists in the IPS programs), and employment outcomes in the first 3 years after the start of implementation of IPS, for supported housing and mental health services separately. Differences between supported housing and mental health services for each year were analyzed using a one-way analysis of variance (ANOVA). We controlled for the assumptions of homoscedasticity and normality of residuals.
Fidelity
We also conducted descriptive analyses on all individual fidelity item scores and the total score for supported housing and mental health services separately. As explained above, we used the first fidelity assessment for all IPS programs, for reasons of comparability. We analyzed differences between supported housing and mental health services using a one-way analysis of variance (ANOVA); the alpha level was set at 0.10 due to the small number of supported housing services (8) vs. mental health services (21). Stevens (29) suggests that when small group sizes are involved it is necessary to adjust the alpha level to compensate and set a cut-off of 0.10 or 0.15 rather than the traditional 0.05.
Qualitative Data-Analysis
Fidelity Assessors' Notes
To understand more about the implementation of IPS in supported housing settings, and why aspects of the IPS approach may have differed from its implementation in mental health treatment organizations, we used thematic analysis (30) to analyze the remarks fidelity assessors made to substantiate their scores. Two researchers (LG, DR, & LW) independently read all assessor comments from the fidelity score forms, with a focus on items where fidelity scores differed between the two sectors. They labeled all factors explaining the fidelity scores as either a facilitator or barrier, according to the content of the assessors' notes. They also compared the assessor notes for each IPS service with the official fidelity criteria. The inter-rater reliability (κ) of the results was calculated and discrepancies were discussed to achieve consensus.
Focus Group
Two trained IPS fidelity assessors, and seven employment specialists involved in IPS coordination in six supported housing organizations, participated in the focus groups. Focus group data were analyzed by reviewing the notes relating to each fidelity item, and by listening and re-listening to the focus group recording to ensure the participant comments were written down and interpreted correctly. Thematic analysis was used to analyze the data (30). The co-facilitator (LW) performed an interrater check. Any identified discrepancies were discussed and double checked using the audio recording, until consensus was reached.
Results
Quantitative Data-Analysis
Program Characteristics
IPS programs provided by supported housing services employed fewer IPS specialists, had fewer new enrollments and smaller caseloads, compared with mental health services (Table 1). For example, by the third year of the programs, IPS programs in mental health treatment organizations employed 10 IPS specialists (on average), who worked with an average 156 clients; in comparison, IPS programs in supported housing services employed 5.5 IPS specialists (on average), who worked with an average of 43 clients. This equates to an average caseload 15.6 vs. 7.8 per IPS specialist respectively.
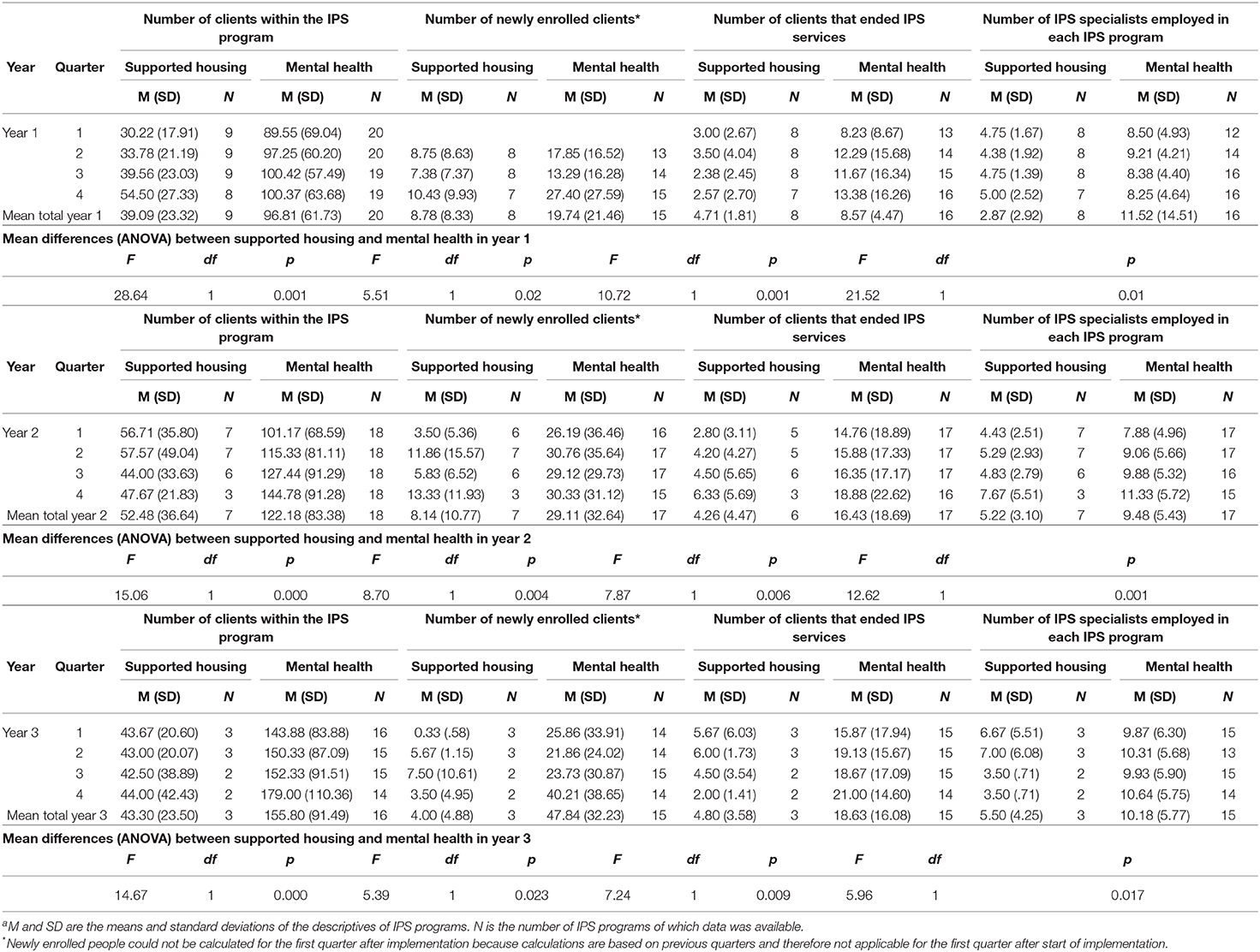
Table 1. Program characteristics over timea.
Employment Outcomes
The quarterly employment rate for IPS programs in supported housing services was, on average, 25.8% of the total caseload and in the mental health treatment organizations this was 29.6%. There were no significant differences in employment rates between supported housing and mental health services in the first (F = 3.41; df = 1; p = 0.07), second (F = 0.63; df = 1; p = 0.43), and third year (F = 1.20; df = 1; p = 0.28) after the start of IPS (Figure 1).
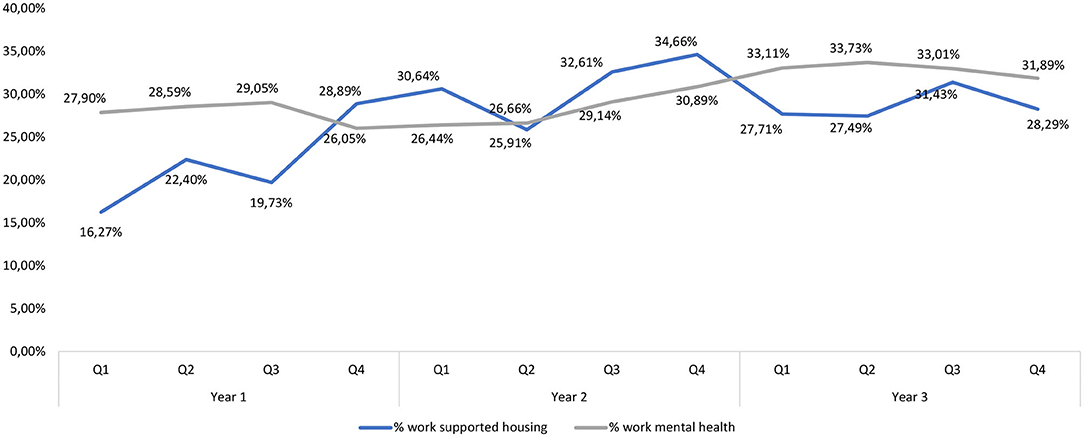
Figure 1. Employment rate as percentage of the total caseload of IPS programs in mental health and supported housing.
Fidelity Assessment
The average IPS fidelity score in supported housing was 94.63, indicating “fair” implementation; this was not significantly different from the average score of mental health service provided IPS programs (M = 94.63; SD = 9.36 vs. M = 90.43; SD = 11.25; F = 1.23; p = 0.28; Table 2).
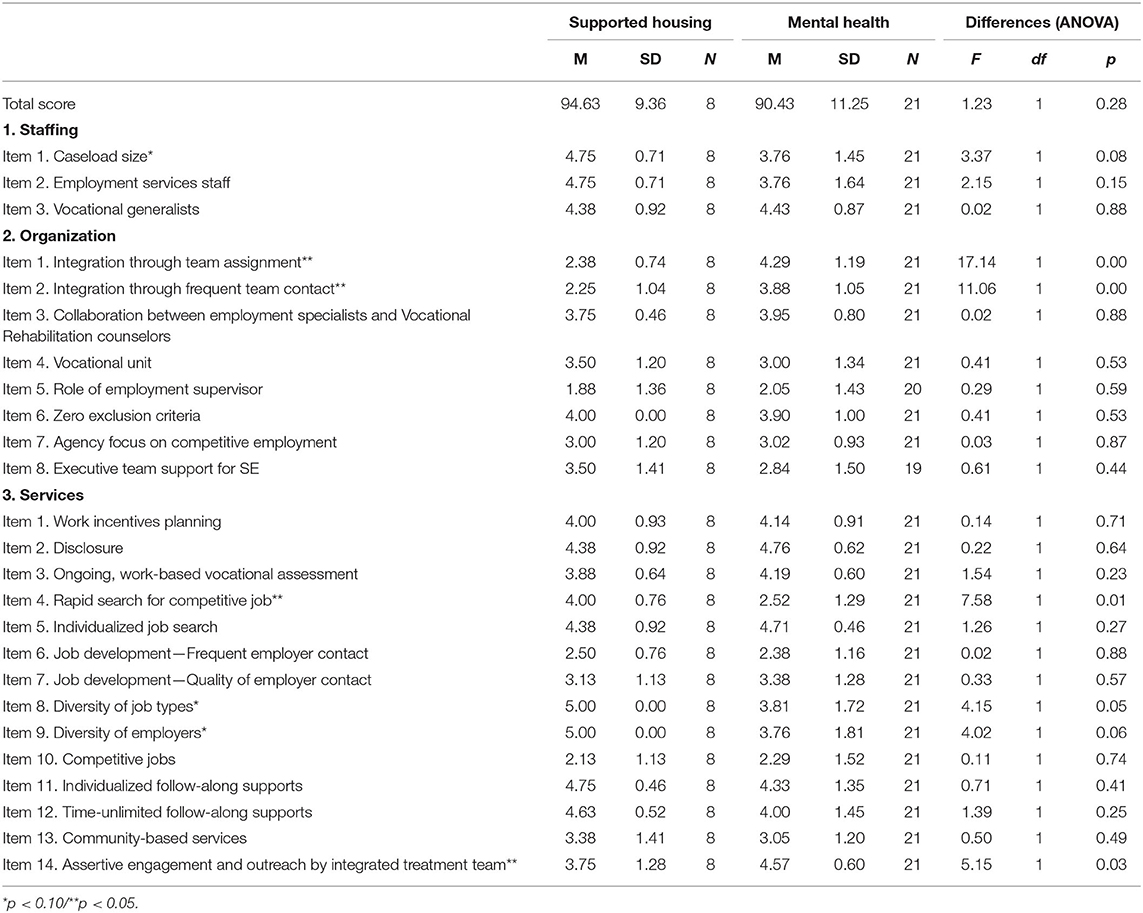
Table 2. Fidelity assessments mental health vs. supported housing organizations.
However, there were differences in some individual fidelity item scores. Mental health treatment organizations scored significantly higher on Items 1 and 2 of the organization section: “Integration through team assignment” and “Integration through frequent team contact,” and Item 14 of the services section: “Assertive engagement and outreach by integrated treatment team.” On the other hand, IPS fidelity was higher in supported housing services for Item 1 of the staffing section: “Caseload,” and items 4, 8, and 9 of the services section: “Rapid search for competitive job,” “Diversity of job types,” and “Diversity of employers.” See attachment for the total IPS-25 scale, including explanation for each item.
Qualitative Data-Analysis
Below, we present possible explanations for the differences in individual fidelity score item, derived from thematic analyses of the IPS fidelity assessors' notes (see Table 3) and focus group data. In addition, results from the focus groups are presented here to explain, expand upon, and/or give context to the audit data. We calculated inter-rater reliability by coding the themes that were rated equally by both assessors with “1” and themes that needed consensus with “0”; this coding system allowed us to calculate inter-rater reliability. The inter-rater reliability of the analysis of the assessors notes between the assessors was moderate (κ = 0.56).
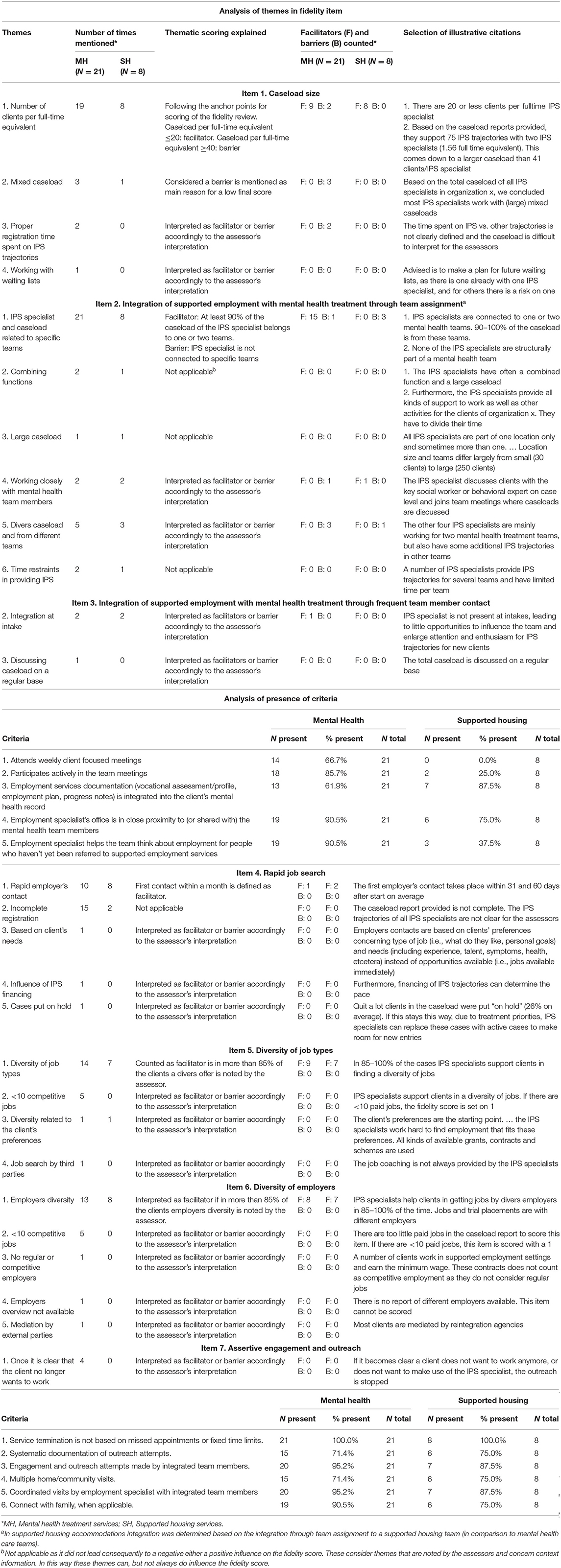
Table 3. Thematic analysis of the seven fidelity items on which supported housing accommodations and mental health treatment institutes differed.
Higher Fidelity IPS Items in Mental Health Services
Integration Through Team Assignment
We compared the average score and assessors' notes for the item “Integration through team assignment” for the IPS programs in mental health and the IPS programs in supported housing. The score on this item is based on the number of teams that one IPS specialist is assigned to (on average) and the percentage of clients in the caseload that come from these assigned teams (i.e., not from multiple other referrals). The rationale is that with a low number of assigned teams, and by receiving most referrals via these teams, the integration of IPS services and treatment is higher. The thematic analysis showed that IPS specialists in mental health treatment more often serve one or two mental health treatment teams; conversely, IPS specialists in supported housing services were less integrated, often serving more than two teams. In the majority of the IPS programs within mental health treatment organizations, at least 90% of the caseload of individual IPS specialists was from one or two mental health treatment teams, compared with a minority of the IPS specialists working with supported housing services. In the focus group, IPS coordinators in supported housing services explained this finding as being due to the fact that clients living in supported housing tended to have more intensive support needs, and supported housing teams also tended to be smaller, with fewer clients per team than mental health treatment teams; as such, IPS specialists in these settings had to work across a number of locations or teams in order to achieve a full caseload (maximum of 20 clients).
An IPS specialist explained this as follows: “That has also to do with the geographical spread and the number of clients. We are organized by self-organization and work in small teams of 8 to 12 team members. In our branch, [as an IPS specialist] you need at least five teams for your caseload.”
Integration Through Frequent Team Contact
The thematic analysis of the IPS fidelity assessors' notes showed that IPS specialists were only able to fully integrate within team meetings in a relatively small number of supported housing services, whereas those working in mental health treatment organizations tended to attend the weekly mental health treatment team meetings more often, and actively participate in treatment team meetings more frequently. They also helped the team think about employment for people who hadn't yet been referred to supported employment services more often than IPS specialists working with supported housing services. In the focus groups, IPS specialists explained that due to the practical barriers for team assignment mentioned above, the contact intensity between IPS specialists with teams and their members, as well as active participation in meetings was lower in supported housing services. Most IPS specialists described this as a structural factor that was characteristic of the sector and could not be solved. Despite this, the IPS assessor acknowledged that in some supported housing organizations quite good integration was achieved. Difficulties with team integration exist for IPS specialists in supported housing services, when teams are small and located in rural areas so IPS specialists cannot fill their caseload by integrating with a maximum of two teams. Furthermore, participating in the regular team meetings was more difficult in some services than others. For instance, some supported housing services did not have a formal, regular team meeting. Some IPS specialists solved this by building on their personal contact with team members, and “being available” for the team when they had employment or education related queries about their clients; these steps served to increase their integration within the service.
The IPS fidelity assessor explained how this was addressed when measuring fidelity on integration, next to joining and integrating in team meetings and being located close by team locations: “What is relevant is whether paid work is mentioned as a goal in the guidance plan. We ask about joining team meetings and how integration is sought in other ways with their colleagues involved by the client. … In that context, the contact with a person's main social worker is highly relevant, as this is the person that integrates the IPS goals in the broader guidance plan.”
Assertive Engagement and Outreach by Integrated Treatment Team
The thematic analysis of the assessor notes did not identify any clear evidence to explain these findings. In the focus group, participants did not recognize the somewhat lower score in supported housing services, which would reflect fewer outreach attempts and more missed appointments, resulting in higher rates of discharge from IPS. They stated they would have expected supported housing services to score higher on this item than IPS specialists working in mental health services, as the first is primarily concerned with community living, rehabilitation and practical housing support. One participant suggested that the weekly mental health treatment team meetings might add to the early detection of employment needs in mental health treatment services, though the other participants did not agree.
Higher Fidelity IPS Items in Supported Housing Services
Caseload Size
Analysis showed that all IPS programs in supported housing services supported 20 or fewer clients per IPS specialist, which is the standard in for the IPS model. In contrast, less than half of mental health treatment organizations supported 20 or fewer clients per IPS specialist, with some IPS programs supporting more than 40 clients. In addition, IPS specialists within mental health treatment organizations more frequently worked with a “mixed caseload,” supporting clients in both IPS and other forms of (vocational) rehabilitation. In the focus group, these findings were explained: participants suggested that that, due to the different support needs of clients living in supported housing, IPS specialists required more time to work with each client, compared to IPS specialists working with clients in mental health services. Furthermore, participants indicated that supported housing services had more problems arranging funding for clients to access IPS, leading to reduced accessibility for supported housing clients. As a consequence, clients for which IPS funding was available were sometimes spread over a large geographical area, with IPS specialists requiring more traveling time.
An IPS coordinator mentioned: “At our organization, we invested strongly in IPS. We wanted to be able to provide IPS to all clients that were interested. … However, we experienced on the way that not all IPS hours can easily be financed in our sector.”
The IPS assessor explained that the most important funding scheme for both sectors includes the subsidy scheme from the Employee Insurance Agency commissioned by the Ministry of Social Affairs and Employment, and for persons receiving welfare payments, municipalities are financially responsible for vocational trajectories. Funding for the treatment and housing services is different: health insurers pay for treatment, while municipalities pay for supported housing services. As a consequence, in mental health treatment organizations, the first eight IPS contacts are often paid by insurers.
Rapid Search for Competitive Job
The thematic analysis of the fidelity assessors' notes showed that, compared with mental health treatment organizations, a higher percentage of IPS programs in supported housing services were able to arrange the initial face-to-face contact between client and employer within 1 month of program entry (4.8 vs. 25%, respectively). However, this finding may have been influenced by the fact that the assessors were less likely to be able to identify the time between first employer contact and program entry due to incomplete registrations in IPS services in mental health services than those delivered in supported housing services. In the focus groups, participants suggested that IPS specialists in supported housing services were able to invest more time into job searches due to lower caseloads, and often had contact with clients prior to starting with IPS and so knew at an early stage what kind of work clients were interested in.
An IPS specialist explained this further: “In team x, I know all the clients, even though I do not coach them in their job search. As soon as they formulate a wish for work, and I am consulted, then I already know a little what his/her preferences are. I think this is helpful.”
Diversity of Job Types and Diversity of Employers
The thematic analysis of the fidelity assessors' notes showed that the lower fidelity on these two items was due to IPS specialists in supported housing services being more able to support their clients into different types of jobs, as well as in different types of employers/companies. In all supported housing services, IPS specialists assisted clients in obtaining different types of jobs, while this was the case in only half of the mental health treatment organizations. Additionally, most of the supported housing services (85%) also worked together with several companies. Five IPS programs within mental health treatment services supported <10 clients into competitive employment, which automatically led to a score of one; this was not the case in any IPS programs in supported housing during the first fidelity assessment. Focus group participants suggested that supported housing services are, from origin, needs based and may have developed particular strengths in creatively searching for services and facilities that fit clients' needs. They indicated that this should also be the case in mental health treatment organizations.
An IPS coordinator simply stated: “that is what you need to do in IPS.”
Discussion
Summary of the Findings
In the current study, we analyzed fidelity scores of IPS programs in supported housing services in The Netherlands and compared them with fidelity scores of IPS programs in mental health treatment organizations. The purpose was to understand feasibility of IPS implementation in supported housing services, in order to increase the accessibility of evidence based vocational services for persons with severe mental illness. Employment rates were examined to understand the relative impact of the IPS programs. Results showed that overall IPS fidelity in supported housing services was “fair,” with services scoring, on average, 94.63; no significant difference was found in overall fidelity scores between supported housing, and mental health treatment organization, based IPS programs suggesting that IPS is feasible in both sectors. Item-level analyses of the IPS fidelity scale indicated that mental health treatment organizations demonstrated better integration of the IPS programs, and higher scores on engagement and outreach; conversely, IPS programs in supported housing services provided more rapid job search processes and more diverse selection of competitive work types and employers. IPS programs in supported housing services were also found to have smaller caseloads per IPS specialist than those provided in mental health treatment services. The quarterly employment rate for IPS programs in supported housing services was 25.8% on average, similar to the rate in mental health treatment organizations, suggesting that these are relatively successful programs; recent research suggests employment levels amongst supported housing clients in The Netherlands is typically 3–5% (5). The fidelity scores and employment rates reported in the current study are similar to longstanding averages reported for Dutch IPS practice (31). Although, we need to be careful in our conclusions based on these statistics, in which details on population characteristics including diagnosis, age and health care needs are missing, our findings are encouraging, particularly considering the higher needs of those living in supported housing (1, 4–7, 10–12).
Interpretation of the Results
Our results suggest that IPS, an evidence-based vocational intervention (15, 17–19), is as feasible and as effective when implemented within in supported accommodation services and mental health treatment organizations in The Netherlands. This is an important finding, considering that so few clients of supported housing have competitive employment (5). Data from the current study indicates that IPS provided in supported housing can support a substantial number of clients, willing to participate in an IPS program, to find a competitive job or education.
Although IPS was originally developed for mental health treatment services (25), by analyzing the IPS fidelity assessors' reports and through staff focus groups, we were able to further understand the facilitators and barriers in implementing IPS in supported housing settings. It should be noted when considering the differences between mental health care and supported housing services on the fidelity items that the baseline fidelity measures we compared were conducted at different time over a 4 year period (from 2015 to 2019) and over this timeframe both IPS and the services within which it was implemented have developed in terms of organizational structures, quality of IPS training and quality of fidelity assessments and this may have influenced our findings. Participants of the focus group reported that the smaller IPS caseload size in supported hosing services was an important facilitator of successful job searching as their clients needed more intensive support with this.
An important difference between the sectors was the integration of the IPS workers within the service, which was lower in supported housing services. This was due to the fact that these workers were often working across multiple supported hosing sites whereas IPS workers in mental health treatment organizations were usually embedded within a single team. However, the overall fidelity rating and employment outcomes were similar for both sectors suggesting that it can be successfully implemented despite differences in specific aspects of fidelity.
Despite the positive results, the data suggest that both mental health treatment and supported housing services score, on average, “fair” on the IPS fidelity scale in their first audit. This leaves room for improvement in both sectors which could lead to greater success in employment outcomes (27). It is known from the national data set that fidelity increases in time and currently fidelity scores in both sectors are above 100, indicating good implementation. Our results also give indications as to how further improvements could be made and suggest that exchange of experiences and expertise between supported housing and mental health treatment organizations on working with IPS is potentially helpful. The main advantage of providing IPS in both sectors is the expansion of the model to a greater number of people with severe mental illness with the associated benefits of facilitating people's access to competitive employment which in turn, improves societal integration and many aspects of well-being (8, 9).
Further research is needed to understand how best to integrate IPS workers in non-clinical settings and how to ensure good liaison between sectors. This is relevant to ensure that if the IPS model expands to other sectors, the critical features are preserved and assessed. There is also more to learn from supported housing services about how they succeed in rapid job searching and engaging a diverse range of employers in the program.
Finally, the results of the focus group indicate that ongoing funding for IPS is needed. Although, in the Netherlands, currently a subsidy scheme is available for IPS, some IPS coordinators participating in the focus group experienced difficulties in accessing funding for all supported housing clients who wished to engage with IPS.
Limitations and Strengths
In interpreting the results, it must kept in mind that the analyses were performed on a small number of IPS programs. IPS in supported housing services is a new development and the results may therefore not be generalizable. Another important limitation is the fact that we were not able to distinguish differences in features of the sample of clients that received IPS between both sectors; as our data were collated at the program level, individual client characteristics were not available. Differences in features of the sample might have been an additional indicator in the description of differences between mental health and supported housing, although in both sectors the population concerns persons with serious mental health problems and research indicates a large overlap as 80% of the supported housing clients receive mental health treatment. The main difference is that supported housing clients have higher care needs on housing and daily living, and a smaller proportion has paid work (22), which suggests that realizing paid employment might even be more difficult in this group In that light, our findings are more positive than would have been expected. An obvious strength is that this is internationally the first study providing indications on the feasibility, experiences, and effects of IPS provided in supported housing services.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
DR wrote the manuscript, performed the focus group, the qualitative analysis, and co authored the quantitative analyses. LW, CB, CC, PM, HK, and JW were involved in the outline and reasoning of the manuscript and critically reviewed the manuscript. JW is also the director of Phrenos, coordinating the IPS audits, and quantitative data collection. LW performed the quantitative analyses and the qualitative analyses. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
Leonie van Grootel helped with the scoring during the thematic analysis. We want to thank her for her time and effort.
References
1. Albers WMM, Roeg DPK, Nijssen Y, van Weeghel J, Bongers IMB. Profiling of victimization, perpetration, and participation: a latent class analysis among people with severe mental illness. PLoS ONE. (2018) 13:e0208457. doi: 10.1371/journal.pone.0208457
2. Richter D, Hoffmann H. Social exclusion of people with severe mental illness in Switzerland: Results from the Swiss health survey. Epidemiol Psychiatr Sci. (2019) 28:427–35. doi: 10.1017/S2045796017000786
3. Sanches SA, Swildens WE, van Busschbach JT, van Weeghel J. Identifying social participation subgroups of individuals with severe mental illnesses: a latent class analysis. Soc Psychiatry Psychiatr Epidemiol. (2019) 54:1067–77. doi: 10.1007/s00127-019-01704-y
4. Bitter N, Roeg D, van Nieuwenhuizen C, van Weeghel J. Recovery in supported accommodations: a scoping review and synthesis of interventions for people with severe mental illness. Community Mental Health J. (2020) 56:1053–76. doi: 10.1007/s10597-020-00561-3
5. Bitter N, Roeg DPK, van Nieuwenhuizen C, van Weeghel J. Identifying profiles of service users in housing services and exploring their quality of life and care needs. BMC Psychiatry. (2016) 16:419. doi: 10.1186/s12888-016-1122-0
6. Killaspy H, Priebe S, Bremner S, McCrone P, Dowling S, Harrison I, et al. Quality of life, autonomy, satisfaction, and costs associated with mental health supported accommodation services in England: a national survey. Lancet Psychiatry. (2016) 3:1129–37. doi: 10.1016/S2215-0366(16)30327-3
7. McPherson P, Krotofil J, Killaspy H. What works? Toward a new classification system for mental health supported accomodation services: the simple taxonomy for supported accomodation (STAX-SA). Int J Environ Res Public Health. (2018) 15:190. doi: 10.3390/ijerph15020190
8. Dunn EC, Wewiorski NJ, Rogers ES. The meaning and importance of employment to people in recovery from serious mental illness: results of a qualitative study. Psychiatr Rehabil J. (2008) 32:59–62. doi: 10.2975/32.1.2008.59.62
9. Michon H, van Busschbach JT, Stant AD, van Vugt MD, van Weeghel J, Kroon H. Effectiveness of individual placement and support for people with severe mental illness in the Netherlands: A 30-month randomized controlled trial. Psychiatr Rehabil J. (2014) 37:129–36. doi: 10.1037/prj0000061
10. Kortrijk HE, Mulder NL, Kamperman AM, van Weeghel J. Employment rates in flexible assertive community treatment teams in the Netherlands: an observational study. Community Ment Health J. (2018) 55:350–9. doi: 10.1007/s10597-018-0233-0
11. Nugter MA, Engelsbel F, Bähler M, Keet R, van Veldhuizen R. Outcomes of FLEXIBLE assertive community treatment (FACT) implementation: a prospective real life study. Community Ment Health J. (2016) 52:898–907. doi: 10.1007/s10597-015-9831-2
12. Van Hoof F, Knispel A, Hulsbosch L, de Lange A, Michon H, Kroon H. Landelijke Monitor Ambulantisering en Hervorming Langdurige GGZ 2017 (National monitor Deinstitutionalization and reform of long term mental health care 2017). Utrecht: Trimbos-instituut (2017).
13. Becker DR, Drake RE. A Working Life for People With Severe Mental Illness. New York, NY: Oxford University Press (2003).
14. Drake RE. (2020). Introduction to the special issue on individual placement and support (IPS) international. Psychiatr Rehabil J. 43:1. doi: 10.1037/prj0000401
15. Brinchmann B, Widding-Havneraas T, Modini M, Rinaldi M, Moe CF, McDaid D, et al. A meta-regression of the impact of policy on the efficacy of individual placement and support. Acta Psychiatr Scand. (2019) 141:206–20. doi: 10.1111/acps.13129
16. Killackey E, Allott K, Woodhead G, Connor S, Dragon S, Ring J. Individual placement and support, supported education in young people with mental illness: an exploratory feasibility study. Early Interv Psychiatry. (2017) 11:526–31. doi: 10.1111/eip.12344
17. Metcalfe JD, Drake RE, Bond GR. Economic, labor, and regulatory moderators of the effect of individual placement and support among people with severe mental illness: a systematic review and meta-analysis. Schizophr Bull. (2017) 44:22–31. doi: 10.1093/schbul/sbx132
18. Modini M, Tan L, Brinchmann B, Wang MJ, Killackey E, Glozier N, et al. Supported employment for people with severe mental illness: systematic review and meta-analysis of the international evidence. Br J Psychiatry. (2016) 209:14–22. doi: 10.1192/bjp.bp.115.165092
19. Suijkerbuijk YB, Schaafsma FG, van Mechelen JC, Ojajärvi A, Corbière M, Anema JR. Interventions for obtaining and maintaining employment in adults with severe mental illness, a network meta-analysis. Cochrane Database Systemat Rev. (2017) 9:CD011867. doi: 10.1002/14651858.CD011867.pub2
20. Bitter N, Roeg D, van Assen M, van Nieuwenhuizen C, van Weeghel J. How effective is the comprehensive approach to rehabilitation (CARe) methodology? A cluster randomized controlled trial. BMC Psychiatry. (2017) 17:396. doi: 10.1186/s12888-017-1565-y
22. De Heer-Wunderink C, Visser E, Sytema S, Wiersma D. Social inclusion of people with severe mental illness living in community housing programs. Psychiatr Serv. (2012) 63:1102–7. doi: 10.1176/appi.ps.201100538
23. Killaspy H. Supported accommodation for people with mental health problems. World Psychiatry. (2016) 15:74–5. doi: 10.1002/wps.20278
24. de Heer-Wunderink C, Visser E, Caro-Nienhuis A, Sytema S, Wiersma D. Supported housing and supported independent living in the netherlands, with a comparison with England. Community Ment Health J. (2012) 48:321–7. doi: 10.1007/s10597-011-9381-1
25. Becker DR, Swanson SJ, Reese SL, Bond GR, McLeman BM. Supported Employment Fidelity Review Manual. A Companion Guide to the Evidence-Based IPS Supported Employment Fidelity Scale. Third Edition. Darthmouth IPS Employment Center (2015).
26. Bond GR, Peterson AE, Becker DR, Drake RE. Validation of the revised individual placement and support fidelity scale (IPS-25). Psychiatr Serv. (2012) 63:758–63. doi: 10.1176/appi.ps.201100476
27. de Winter L, Couwenbergh C, van Weeghel J, Bergmans C, Bond GR. Fidelity and IPS: does quality of implementation predict vocational outcomes over time for organizations treating persons with severe mental illness in the Netherlands? Soc Psychiatry Psychiatr Epidemiol. (2020) 55:1607–17. doi: 10.1007/s00127-020-01890-0
28. IPS Employment Center. IPS Quarterly Employment Reporting Form. (2019). Retrieved from https://ipsworks.org/wp-content/uploads/2018/01/IPS-Learning-Community-Outcomes2018.pdf
29. Stevens J. Applied Multivariate Statistics for the Social Sciences. Mahwah, NJ: Lawrence Erlbaum (1996).
30. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. (2006) 3:77–101. doi: 10.1191/1478088706qp063oa
Keywords: employment, IPS, supported housing, severe mental illness, fidelity
Citation: Roeg D, de Winter L, Bergmans C, Couwenbergh C, McPherson P, Killaspy H and van Weeghel J (2021) IPS in Supported Housing: Fidelity and Employment Outcomes Over a 4 Year Period. Front. Psychiatry 11:622061. doi: 10.3389/fpsyt.2020.622061
Received: 27 October 2020; Accepted: 15 December 2020;
Published: 14 January 2021.
Edited by:
Hector Wing Hong Tsang, Hong Kong Polytechnic University, Hong KongCopyright © 2021 Roeg, de Winter, Bergmans, Couwenbergh, McPherson, Killaspy and van Weeghel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diana Roeg, ZGlhbmEucm9lZ0Brd2ludGVzLm5s