 Hamid Sharif Nia1
Hamid Sharif Nia1 Ozkan Gorgulu2
Ozkan Gorgulu2 Navaz Naghavi3
Navaz Naghavi3 María Auxiliadora Robles-Bello4
María Auxiliadora Robles-Bello4 David Sánchez-Teruel5
David Sánchez-Teruel5 Fatemeh Khoshnavay Fomani6
Fatemeh Khoshnavay Fomani6 Long She7
Long She7 Pardis Rahmatpour8*
Pardis Rahmatpour8* Kelly-Ann Allen9,10
Kelly-Ann Allen9,10 Gokmen Arslan11Saeed Pahlevan Sharif12
Gokmen Arslan11Saeed Pahlevan Sharif12- 1Psychiatry and Behavioral Sciences Research Center, Addiction Institute, Mazandaran University of Medical Sciences, Sari, Iran
- 2Department of Biostatistics and Medical Information, Faculty of Medicine, Kirsehir Ahi Evran University, Kirsehir, Turkey
- 3Taylor's Business School, Taylor's University, Subang Jaya, Malaysia
- 4Area of Developmental and Educational Psychology, Department of Psychology, Faculty of Humanities, University of Jaén, Jaén, Spain
- 5Department of Personality, Evaluation and Psychological Treatment, Faculty of Psychology, University of Granada, Granada, Spain
- 6School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
- 7Faculty of Business and Law, Taylor's University, Subang Jaya, Malaysia
- 8Department of Nursing, School of Nursing, Alborz University of Medical Sciences, Karaj, Iran
- 9School of Educational Psychology and Counselling, Faculty of Education, Monash University, Clayton, VIC, Australia
- 10Centre for Wellbeing Science, The Melbourne Graduate School of Education, The University of Melbourne, Parkville, VIC, Australia
- 11Mehmet Akif Ersoy University, Burdur, Turkey
- 12Faculty of Business and Law, Taylor's University, Subang Jaya, Malaysia
This study investigates the relationship between spiritual well-being, social support, and financial distress with depressive symptoms due to the COVID-19 pandemic. A path analysis was used to analyze data collected from 1,156 Iranian participants via an online survey. The results showed that spiritual well-being and social support were negatively related to depressive symptoms and financial distress. The impact of COVID-19 events showed negative associations with depressive symptoms. In addition, the link between spiritual well-being and financial distress with depressive symptoms was partially mediated by the impact of events.
Introduction
The unprecedented rate of mortality from the coronavirus (COVID-19) pandemic has caused times of distress and uncertainty for people across the globe (1–4). Iran has not been an exception. At the time of writing this paper (16 July 2021), Iran had 3,440,400 confirmed cases and 86,391 virus-related deaths since the beginning of the pandemic (5).
Restrictions to curb the spread of the COVID-19 virus, such as quarantine measures, stay-at-home recommendations, physical distancing orders, as well as the fear of potential exposure to infection and misinformation, have taken a heavy toll on public psychological well-being (6). The effects of the pandemic have disrupted not only peoples' everyday lives but also reduced social connections and a sense of belonging that people would usually experience (7–9). Such outcomes are strongly linked to depression (3, 10–12). In addition, the economic recession due to lockdowns, an increase in unemployment (13), and uncertainty about the affordability of health costs (14) may lead to stressors that trigger depression and other mental disorders (15).
It has been reported that anxiety and depression due to COVID-19 have had a prevalence rate between 16 and 20% across the general population in various countries (16). Specifically, findings from a meta-analysis suggested a significant difference in the general population between global depression rates in 2017 (3.44%) and 2020 (25%) (17).
Literature Review
Many factors have been put forth in the body of literature focusing on the determinants of depression among the public during the pandemic. The first strand of literature sheds light on various types of self-care due to physical and social constraints (18), out of which spirituality has drawn growing attention (18–20). The underpinning theory for this category of literature is the mindful consumption notion proposed by Sheth et al. (21), which discusses the human capability to develop resilient solutions in times of hardship. From this point of view, spirituality is an intrinsic motivation to seek satisfaction and maintain a harmonious relationship with oneself/others in times of stress or crisis (20–23). Studies that have examined spirituality during COVID-19 have found that it can facilitate self-reported self-care, connectedness, and meaning and purpose in life (18, 24, 25).
Given this, spiritual dimensions have been integrated into research on coping, well-being, and mental health promotion across the lifespan, as a way to prevent mental health disorders such as depression (26–29). The impact of COVID-19 on spirituality has been assessed by some literature, which found that a higher perceived COVID-19 risk predicted more significant depressive symptoms (30). In most cases, when people perceive a stressful, aversive, or traumatic event, such as a pandemic they may engage in religious activities or rituals to cope with depressive symptoms (31–33). Although the most literature has found a positive relationship between spirituality and mental health (34), some research has reported a negative or neutral relationship (4, 35).
Another strand of literature highlights the importance of social support as a psychosocial protective factor concerning mental health adversity (36–39). Social support is the subjective evaluation of friends', family members', and significant others' ability to provide support in challenging times (40). The stress-buffering hypothesis (41) posited that interpersonal social support could buffer the negative impact of hardship and enhance an individual's ability to reduces stress, anxiety, and depression (42–44). There is a plethora of research on the negative association between social support and severity of mental health outcomes, such as depression and anxiety (43, 45, 46). The vital role of social support has been highlighted during the pandemic (47–49) with some studies finding the impact of COVID-19 improved individuals' perceived social support (50). Yu et al. (51) found that during the COVID-19 pandemic, participants with the highest amount of psychological distress received the least amount of social support. They also displayed more passive coping styles compared to participants with lower distress. Along these lines, the current study seeks to investigate the relationship between social support and depressive symptoms during the pandemic among the Iranian public.
Apart from introspective (e.g., spiritual well-being) or extroverted (e.g., social support) factors, the financial burden caused by the pandemic is another influential factor related to mental health issues. Economic burden from the pandemic includes both direct costs (e.g., virus-related medical treatment) and indirect costs (e.g., job loss) (52, 53). The enforced lockdowns of many businesses to control the infection rate have caused increased unemployment in many sectors. The high transmission rate of the virus has inflicted medical costs, including those from diagnosis, treatment, and hospitalization (if required) to many infected individuals and families. Such financial pressures may cause stressors that can contribute to depression.
Although the relationship between perceived financial burden and depression in patients with chronic disease has been extensively investigated in the literature (54–57), limited research has investigated this during the COVID-19 pandemic. A few recent studies have affirmed perceived financial burden as an emerging worrying factor for some specific groups of people during the pandemic (58, 59). There is, however, a need for a detailed investigation into this relationship by examining the possible variables that may affect financial burden and depression in different settings.
To ensure the current study captures the impact of the pandemic on individuals' mental health, event-specific distress is taken into consideration. The Impact of Event Scale-Revised used in this study measures stress or distress by evaluating: Intrusions (unwanted thoughts and images related to the event such as nightmares), Avoidance (the effort to avoid thinking about the traumatic or stressful event), and Hyperarousal (anger, irritability, difficulty concentrating) [Hair (60–62)]. This scale has been widely used in literature to measure COVID-19's impact on individuals' stress levels (63–67).
According to a review conducted by Rajkumar (16), only eight publications have explored mental health problems as influenced by the COVID-19 pandemic in the general population. While only a few studies have focused on the prevalence of anxiety and depression among healthcare professionals (68–71) and COVID-19-infected patients (72) since the start of the pandemic. Limited attention has been given to the public. Moreover, to date, factors influencing depression and depressive symptoms among the general population remain largely unknown (38, 73). Therefore, the current study investigates some factors related to depressive symptoms in the general population due to the pandemic. Moreover, this study goes one step further to investigate the mediating role of stress related to the impact of the pandemic (i.e., “impact of the event”) on the relationships between spiritual well-being, financial distress, and social support with depression. In this vein, the current study aims to analyze the direct relationship between spiritual well-being, social support, and financial distress with depressive symptoms and endeavors to explore if there are any indirect relationships among the aforementioned variables with the impact of the event as a mediator.
This study intends to investigate the factors influencing depression due to the COVID-19 pandemic, which will provide policymakers insight into what factors and approaches could be prioritized. The noteworthy contributions of the present study are 2-fold. To the best of the authors' knowledge, it is the first study considering the indirect relationship between spiritual well-being (SWB), social support, and financial distress with depressive symptoms during the pandemic. Secondly, owing to the widespread impact of the pandemic, this study surveys the general population in Iran.
Hypotheses
Seven hypotheses were investigated in the current study:
H1: Social support will have a significant negative correlation with impact of event, and social support will be a significant predictor of impact of event.
H2: Social support will have a significant negative correlation with depression, and social support will be a significant predictor of depression.
H3: Spiritual well-being will have a significant negative correlation with impact of event, and spiritual well-being will be a significant predictor of impact of event.
H4: Spiritual well-being will have a significant negative correlation with impact of event, and spiritual well-being will be a significant predictor of depression.
H5: Financial distress will have a significant positive correlation with impact of event, and financial distress will be a significant predictor of impact of event.
H6: Financial distress will have a significant positive correlation with depression, and financial distress will be a significant predictor of depression.
H7: Impact of event will have a significant positive correlation with depression, and impact of event will be a significant predictor of depression.
Method
A predictive, cross-sectional online questionnaire-based survey was used in this study to investigate the relationships between spiritual well-being, social support, and financial distress with depressive symptoms due to the pandemic and the mediating role of the impact of the COVID-19 event in these relationships.
Participants
The requisite sample size was estimated to be 1,156 with a probability of 0.05, the statistical power of 80%, the anticipated medium effect size of 0.13, and 64 items measuring five constructs. This estimate was calculated a-priori using a sample size calculator for Structural Equation Models (SEM) (74). The minimum statistical power analysis in humanities and social sciences studies should be 80% (75). In total, 1,156 participants in Iran participated between April and July 2020 during the initial stages of the COVID-19 pandemic. The questionnaire was designed with Google Form and was made available to the public through Telegram channels and WhatsApp public groups. The mean age of participants was 32.78 (SD = 7.7) (range 20 to 60) years old, and most were female (83.5%), married (51.3%), and had a bachelor's degree (48.1%). The other socio-demographic information is provided in Table 1.
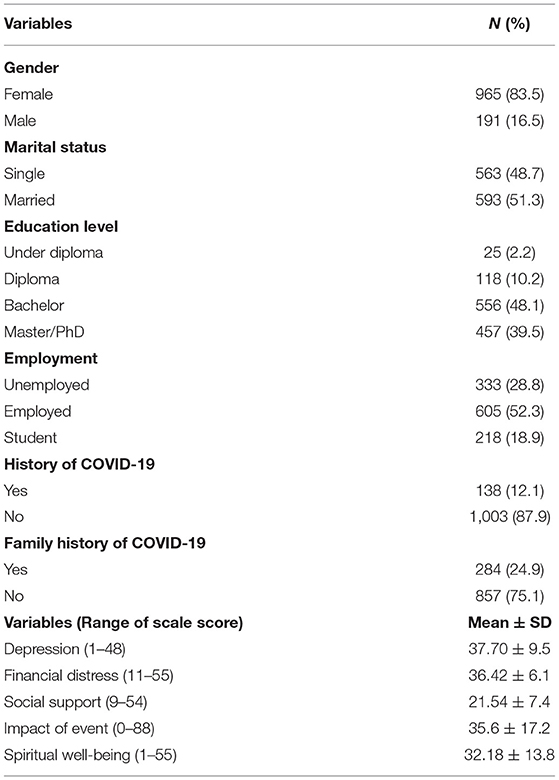
Table 1. Demographic characteristics of participants (n = 1,156).
Instruments
A demographic form and the Persian version of the following scales were used in this study: ENRICHD Social Support Inventory (ESSI), the Spiritual Well-Being (SWB) Scale, the Comprehensive Score for Financial Toxicity (COST), the Center for Epidemiological Studies Depression scale (CES-D), and the Impact of Events Scale-Revised (IES-R).
The Persian version of ENRICHD Social Support Inventory (ESSI) consists of six questions and utilizes a five-point Likert scale, ranging from 1 (none of the time) to 5 (all of the time) (76). Construct validity of the Persian scale was conducted by maximum likelihood exploratory factor analysis. The results extracted one factors accounting for 64.307% of the variance. The reliability of the ESSI was determined by Cronbach's alpha and McDonald's omega, which were found to be 0.91.
The Persian version of the SWB Scale (27) consists of two subscales: connecting with God and meaningless life. Only the subscale “connecting with God” (eight items) was used in the current study. The items were measured using a 6-point Likert-type scale from 1 (completely disagree) to 6 (completely agree). A higher score indicated greater spiritual well-being or greater connection with God in the present study. The reliability of the SWB Scale was determined by Cronbach's alpha and McDonald's omega, which were found to be 0.911 (CI 95%: 0.904 to 0.917) and 0.935 (CI 95%: 0.930 to 0.941), respectively.
The Persian version of the Comprehensive Score for Financial Toxicity (COST) scale (77) contains 11 questions is scored from 1 (strongly disagree) to 5 (strongly agree) (78). The reliability of the COST scale was determined by Cronbach's alpha and McDonald's omega, which were found to be 0.820 (CI 95%: 0.804 to 0.835) and 0.823 (CI 95%: 0.808 to 0.838), respectively.
The Persian version of the center for epidemiological studies depression scale (CES-D) was used to measure symptoms associated with depression. It consists of 16 items with three factors, namely somatic affect (7 items), negative affect (5 items), and positive affect (4 items), with a four-point Likert response (79). The reliability of the CES-D was determined by Cronbach's alpha and McDonald's omega, which were found to be 0.874 (CI 95%: 0.864 to 0.884) and 0.883 (CI 95%: 0.874 to 0.893), respectively.
The Persian version of the Impact of Events Scale-Revised (IES-R) consists of 18 items and three factors that measure different dimensions of stress response, including intrusion (6 items), avoidance (7 items), and hyperarousal (5 items). The IES-R is a short, easily administered scale that can be used with most individuals exposed to any specific traumatic event. The IES-R is scored on a 5-point Likert-type scale from 0 (not at all) to 4 (extremely) (61). The reliability of the IES-R was determined by Cronbach's alpha and McDonald's omega, which were found to be 0.930 (CI 95%: 0.924 to 0.936) and 0.929 (CI 95%: 0.923 to 0.935), respectively.
Data Analysis
A path analysis was used in the present study. It is used to determine how much of the total effects of independent variables on the dependent variables occur directly and indirectly. The method of path analysis was originated and developed by the geneticist Sewall Wright as early as 1918 (80, 81). Path analysis uses multiple regression techniques that allow a second dimension-time sequence to enter the analysis (82). As used in this study, path analysis utilizes a standard multiple regression technique to estimate the path coefficients. The standard regression coefficients from the multiple regressions were the path coefficient (83). In path analysis, four different effects as direct, indirect, U, and S between variables are defined.
Statistical Package for Social Sciences (version 25) for Windows (IBM SPSS Statistics for Windows, Version 21.0; IBM Corp., Armonk, NY) was used for the analyses in the study. JASP 14.0.0 was also used to evaluate McDonald's omega. A probability level of p < 0.05 was used to determine statistical significance.
Ethical Considerations
The study aims, number of items, time to complete the survey, the researcher's affiliation and email for queries, and the ethical code of study were inserted on the first page of the online questionnaire. These items informed participants that their participation was voluntary and that their responses would be published anonymously as group data. The protocol of this study was approved by the Mazandaran University of Medical Sciences Research Ethics Committee (IR.MAZUMS.REC.1399.7461).
Results
According to the path diagram (Figure 1) and the results of the path analysis (Table 3), this study revealed that the total effects of social support on depression (total effect = −0.378**, p < 0.01), and spiritual well-being on depression (total effect = –0.357**, p < 0.01) were negative and significant. In addition, the results indicated that the total effect of financial distress on depression (total effect = 0.473**, p < 0.01), and impact of event on depression were positive and significant (total effect = 0.416**, p < 0.01).
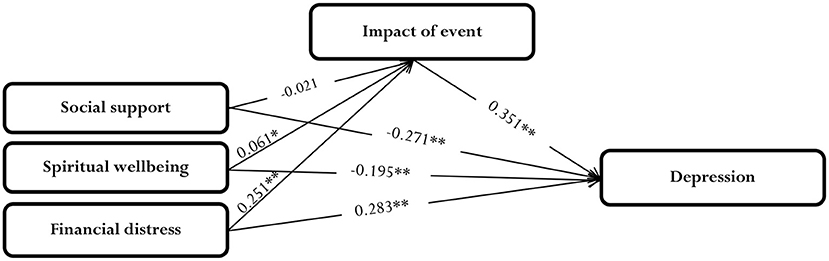
Figure 1. Path diagram. **p < 0.01, *p < 0.05.
The correlation matrix displaying the relationships between depression and other variables is given in Table 2. There was a significant positive relationship between financial distress and impact of event with depression (r = 0.469**, r = 0.430**, p < 0.01). The relationships between social support and spiritual well-being with depression were significant and negative (r = −0.389**, r = −0.344**, p < 0.01). The correlations between social support, spiritual well-being, and financial distress variables were positive and statistically significant (p < 0.01). These correlations created the unanalyzed effect in the model (see Figure 1).

Table 2. Correlations between variables.
The coefficients, which show the direct and indirect effects of the variables on depression, are summarized in Table 3. According to these results, social support had a negative significant direct effect on depression (PYX1 = −0.271**, p < 0.01). Social support indirectly affected depression through spiritual well-being and financial distress. The ratio of the U effects of the social support variable on spiritual well-being and financial distress were 12.08 and 13.62% within the total effect, respectively.
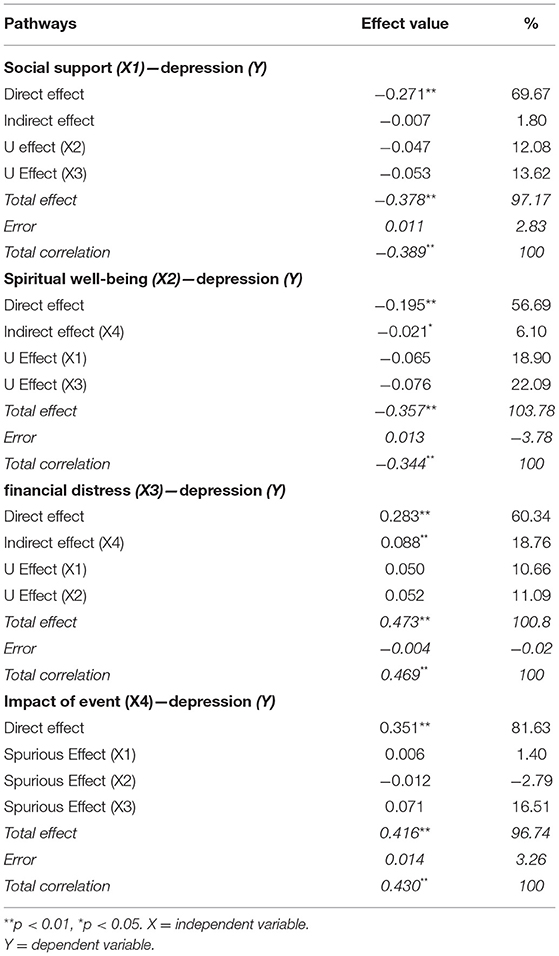
Table 3. Path effects.
The direct effect of the spiritual well-being variable (PYX2 = −0.195**, p < 0.01) on depression constituted 56.69% of the total effect. The U effect of spiritual well-being on financial distress accounted for 22.09% of the total correlation. The direct effect of financial distress on depression was quite high (PYX3 = 0.283**, p < 0.01, 60.34%). The indirect effect on impact of event was the highest (18.76%). When the variables are examined in terms of direct effects, it is seen that the highest effect is calculated in the impact of event variable. Indirect effects can be interpreted using the mediator variable. The mediator variable in this study was impact of event as can be seen in the model and path diagram. The effects of the social support, spiritual well-being, and financial distress variables on depression through impact of event provided the indirect effects in the framework of the model. The results showed that effects of social support (−0.007, p = 0.46), spiritual well-being (−0.021* p < 0.05), and financial distress (0.088**, p < 0.0.01) on depression through impact of event demonstrated that impact of event mediated the relationship between spiritual well-being and depression, and between financial distress and depression, but not the relationship between social support and depression. Moreover, the significant direct effects of spiritual well-being (PYX2 = −0.195**, p < 0.01) and financial distress (PYX3 = 0.283**, p < 0.01) on depression in the mediation model indicated both mediation effects were partial. Lastly, impact of event had a strong and positive direct effect on depression (Pyx4 = 0.351**, p < 0.01, 81.63%). In addition to the direct effect of the impact of event variable, it also significantly (16.51%) spurious effect on depression of financial distress variable.
Discussion
The current study investigated certain factors that associated with depressive symptoms as reported by Iranians during the COVID-19 pandemic. More specifically, this study examined how social support, spiritual well-being, and financial distress predicted depression among the general population in Iran during the COVID-19 pandemic.
The findings revealed that there was a significant positive correlation between financial distress and the impact of events (e.g., quarantine during COVID-19) with depressive symptoms. Global economic instability, changes in employment, and fear of future financial outcomes due to the COVID-19 pandemic are some possible causes of financial distress among individuals (84). Many businesses were forced to shut down, and some small businesses closed permanently. While overcoming economic upheaval is helped markedly by an individuals' financial standing (85), COVID-19 affected such a large number of people with varying financial needs and capacities that financial distress for many was unavoidable. The positive correlation between financial distress and depressive symptoms has been identified in several studies [see (86–88)]. There is also evidence of increased suicide rates (89), aggression, and litigation (90) during previous quarantine periods. Furthermore, gender differences have been found in terms of mental health consequences during the COVID-19 outbreak. Females may experience more severe stress, depression, and anxiety symptoms during the COVID-19 (91–93). As most of the participants (83.5%) in the present study were female, the relationship between the impact of event (e.g., quarantine) and depressive symptoms may be overemphasized.
Quarantine is an unpleasant experience for many, in part due to a loss of freedom, uncertainty over the virus, and separation from close social contacts (94). In the COVID-19 pandemic, restrictions due to lockdown measures, a reduction of social connections, and greater perceived uncertainty have been identified as variables associated with greater mental health problems and depressive symptoms (8). Consistent with past studies (38, 43), the current study findings revealed a negative relationship between social support and depressive symptoms. However, the exact relationship between depression and social support has varied in the literature. While some study findings have found a negative relationship between these variables (95), others have found differences between the support offered by family, neighbors, or friends with social support from the family having a more substantial effect on mental health (96). Social support has been found to buffer the effect of stress on depression (97) through increasing self-disclosure and creating feelings of safety (98). Torkian et al. (99) reported that a moderate to high number of Iranians received social support during the COVID-19 outbreak, which improved their social adjustment. One explanation for the current findings could be that social support facilitates social adjustment to change and uncertainty, which mitigates the risk of depression.
Congruent with past studies (100–102), the results indicated that there is a negative relationship between spiritual well-being and depressive symptoms, which has been supported by past research (100, 101, 103). Few studies have focused on the relationship between religion and depression in the Iranian population. The existing literature indicates there is a negative association between religiosity and depression among medical students (104), Iranian patients with spinal cord injury (105), and infertile women (106). A qualitative systematic review of 4,944 papers provided evidence of the significant role of spirituality in improving mental health, namely that spirituality gives meaning to life. It improves coping skills that may help mitigate depressive symptoms (34). Furthermore, a study with a sample of Palestinian adults during the spread of COVID-19 found a negative correlation between positive religious coping and depressive symptoms (35). Similarly, the findings of a study with an Arab population showed negative religious coping was associated with depression (4). However, a reverse relationship between spirituality and depression has been demonstrated by several other study findings (107). While religious beliefs and practices may help people to cope better with life adversities via giving their life meaning and hope, in some cases, religious beliefs may also increase feelings of guilt and failure (108).
One important consideration when interpreting the relationship between religion and mental health is the context. One study compared 268 regions within 28 European countries and found that individuals from a religious minority reported more depressive symptoms than individuals from non-minorities, except in regions where there is a majority of Muslims (109). Another study showed that the mental health of Iranian people is driven by extrinsic religious motivation more than people living in Western countries (110). Therefore, when Iranian people cannot attend religious places and perform group ceremonies or rituals due to quarantine, their mental health may be more affected (110). It is worth mentioning that women tend to participate more frequently than men in religious practices, which may have influenced the present study's findings (111, 112). The development of online spiritual health programs for the Iranian population during times of lockdown may have merit in the future.
The current study revealed that spiritual well-being and financial distress had significant indirect relationships with depressive symptoms through the different dimensions of stress response caused by the impact of event (e.g., COVID-19). Among these variables, financial distress and the impact of event had the highest direct and indirect effect with depressive symptoms, respectively. The virus outbreak and the quarantine that followed may have led to widespread stress, especially stigmatization and social exclusion, which may escalate into other negative psychological reactions, including adjustment disorder and depression (113). During the COVID-19 pandemic, many people went through financial hardship due to the increasing cost of healthcare expenditures (114). Furthermore, the COVID-19 pandemic resulted in an unprecedented decline in economic activity with employment and a decline in income (100). Despite the government's protective measures to reduce peoples' anxiety about the virus, the fear of economic loss has increased mental health problems among Iranian people. While the government launched social support programs and psychological services for patients, it remained incapable of offering economic stimulus packages (115) or proactive and preventative approaches for the general population.
The findings of a large national study in Iran found a high level of stress among the general Iranian population during the COVID-19 outbreak in which those in middle age groups and low to moderate socioeconomic status experienced the highest stress due to worry about losing their jobs or income (116). In particular, middle-income earners (e.g., laborers) experienced stress from their inability to physically attend work. While low-income earners, who attended work, would do so on crowded buses, subways, or other vehicles and experienced stress from the fear of infection or dismissal for non-attendance (117). From these findings, it appears that the COVID-19 pandemic has most negatively affected the socially vulnerable Iranian population. Public policies to protect these groups are essential to minimize the spread of COVID-19 in the country and prevent the development of clinical disorders such as depression.
The impact of the COVID-19 events significantly mediated the relationship between spiritual well-being and depression. Although spiritual well-being has been identified as a protective factor for depression during the COVID-19 outbreak (118), the impact of religion on better mental health outcomes is dependent on the number of religious activities engaged in, physical religious attendance, and increased spiritual growth (33, 119). Since quarantine began in Iran, many public spiritual or religious activities were ceased due to mosques and religious places closing. Given that the majority of Iranians are Muslim, public spiritual activities such as congregational prayer have long been an important practice for them. Accordingly, it is plausible that Iranians barred from attending public religious practice may feel psychological distress. In this regard, the findings of a meta-analysis study that investigated the spirituality of religious effects on mental health revealed that among different religious or spiritual factors, only participation in public religious activities and the importance of religion were significantly related to mental health (120).
In general, although the correlations between the current study variables have been addressed by previous studies, the present study revealed the significant positive mediating role of the COVID-19 pandemic on the relationship between spiritual well-being and financial distress with depression. What sets this study apart from previous studies is that it identifies how the effects of the COVID-19 pandemic can affect the relationship between spirituality, financial distress, social support, and the development of depressive symptoms. While many studies suggest that promoting spirituality in times of crisis and epidemics can ensure mental health (33, 121), the present study showed that this is not possible without considering the impact of the event.
Study Limitation
While the study provides new information relative to the mediating role of the impact of event on the relationship between financial distress and spiritual well-being with depression, it is not without its limitations. The cross-sectional design of this study does not allow for firm causal conclusions. Conducting longitudinal studies by collecting data at different points in time as well as experimental studies are recommended for future research since there are numerous complex and dynamic processes by which spirituality relates to mental health outcomes. In terms of mediation studies, the most salient mediating processes seem to involve religiosity/spirituality dimensions, values/attitudes, and social control/norms, which need to be investigated in further studies. Furthermore, the data were gathered via online data collection. Despite its advantages (e.g., affordability and accessibility), online surveys have been criticized for selection bias and difficulty reaching certain types of participants (122, 123). Finally, the questionnaire length (64 items) and the order of instruments may have affected careless responding (124) or reduced response rate due to response burden (125).
Conclusion
The current study revealed that during the COVID-19 pandemic, financial distress may have influenced depressive symptoms, however this can be explained through impact of event. In addition, spiritual well-being may not always serve a protective role in terms of the impact of stress on depression. Consequently, when pandemic-related protective measures are rolled out (e.g., quarantine), the positive relationship between spiritual well-being and depression appears. The visibility of protective factors in addition to risk factors can offer a broader view on measures to deal with depression in the general population resulting from global adverse situations such as the ongoing COVID-19 pandemic. The current study findings are applicable for health policy-makers to help them for developing health promotion programs and fostering resilience among the general population. It will also be the responsibility of governments to help improve public health through economic protection policies in the event of epidemics.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
The studies involving human participants were reviewed and approved by Mazandaran University of Medical Sciences Research Ethics Committee (IR.MAZUMS.REC.1399.7461). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
PR, HS, and GA contributed to the study conception and design. Material preparation and data collection was performed by FK and PR. OG, HS, and SP performed data analysis. The first draft of the manuscript was written by NN, PR, LS, FK, DS-T, K-AA, and MR-B. All authors commented on previous versions of the manuscript and read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank all of our participants in this study.
References
1. Ammar A, Trabelsi K, Brach M, Chtourou H, Boukhris O, Masmoudi L, et al. Effects of home confinement on mental health and lifestyle behaviours during the COVID-19 outbreak: insights from the ECLB-COVID19 multicentre study. Biol Sport. (2021) 38:9–21. doi: 10.5114/biolsport.2020.96857
2. Arslan G, Allen KA. Exploring the association between coronavirus stress, meaning in life, psychological flexibility, subjective well-being. Psychol Health Med. (2021) 1–12. doi: 10.1080/13548506.2021.1876892
3. Mencacci C, Salvi V. Expected effects of COVID-19 outbreak on depression incidence in Italy. J Affect Disord. (2020) 278:66–7. doi: 10.1016/j.jad.2020.09.043
4. Yildirim M, Güler A. Positivity explains how COVID-19 perceived risk increases death distress and reduces happiness. Pers Individ Dif. (2021) 168:110347. doi: 10.1016/j.paid.2020.110347
5. Statista. Number of Coronavirus (COVID-19) Cases Worldwide as of October 1, 2021, by Country. (2020). Available online at: https://www.statista.com/statistics/1043366/novel-coronavirus-2019ncov-cases-worldwide-by-country/ (access November 23, 2020).
6. Serrano-Ripoll MJ, Meneses-Echavez JF, Ricci-Cabello I, Fraile-Navarro D, Fiol-deRoque MA, Pastor-Moreno G, et al. Impact of viral epidemic outbreaks on mental health of healthcare workers: a rapid systematic review and meta-analysis. J Affect Disord. (2020) 277:347–57. doi: 10.1016/j.jad.2020.08.034
7. Allen K-A, Furlong M. Leveraging belonging in response to global loneliness. Aust J Psychol. (2021) 73:1–3. doi: 10.1080/00049530.2021.1875532
8. Benke C, Autenrieth LK, Asselmann E, Pané-Farré CA. Lockdown, quarantine measures, and social distancing: associations with depression, anxiety and distress at the beginning of the COVID-19 pandemic among adults from Germany. Psychiatry Res. (2020) 293:113462. doi: 10.1016/j.psychres.2020.113462
9. Lim MH, Allen K-A, Furlong MJ, Craig H, Smith DC. Introducing a dual continuum model of belonging and loneliness. Aust J Psychol. (2021) 73:81–6. doi: 10.1080/00049530.2021.1883411
10. Allen KA, Kern ML, Vella-Brodrick D, Waters L, Hattie J. What schools need to know about belonging: a meta-analysis. Educ Psychol Rev. (2018) 30:1–34. doi: 10.1007/s10648-016-9389-8
11. Allen KA, McKenzie VL. Adolescent mental health in an Australian context and future interventions. Int J Ment Health. (2015) 44:80–93. doi: 10.1080/00207411.2015.1009780
12. Parr EJ, Shochet IM, Cockshaw WD, Kelly RL. General belonging is a key predictor of adolescent depressive symptoms and partially mediates school belonging. School Ment Health. (2020) 12:626–37. doi: 10.1007/s12310-020-09371-0
13. Dawel A., Shou Y., Smithson M., Cherbuin N., Banfield M., Calear A. L., Farrer L. M., Gray D., Gulliver A., Housen T., McCallum S. M., Morse A. R., Murray K., Newman E., Rodney Harris R. M., Batterham P. J. (2020). The Effect of COVID-19 on Mental Health and Wellbeing in a Representative Sample of Australian Adults. Frontiers in Psychiatry, 11, 579985-579985. https://doi.org/10.3389/fpsyt.2020.579985
14. Wapner J. Covid-19: medical expenses leave many Americans deep in debt. BMJ. (2020) 370:m3097. doi: 10.1136/bmj.m3097
15. Alnazly E, Khraisat OM, Al-Bashaireh AM, Bryant CL. Anxiety, depression, stress, fear and social support during COVID-19 pandemic among Jordanian healthcare workers. PLoS ONE. (2021) 16:e0247679. doi: 10.1371/journal.pone.0247679
16. Rajkumar RP. COVID-19 and mental health: a review of the existing literature. Asian J Psychiatr. (2020) 52:102066–102066. doi: 10.1016/j.ajp.2020.102066
17. Bueno-Notivol J, Gracia-García P, Olaya B, Lasheras I, López-Antón R, Santabárbara J. Prevalence of depression during the COVID-19 outbreak: a meta-analysis of community-based studies. Int J Clin Health Psychol. (2020) 21:100196. doi: 10.1016/j.ijchp.2020.07.007
18. Castañeda RFG, Hernández-Cervantes Q. Self-care and spirituality in times of contingency due to COVID-19. Cogitare Enfermagem. (2020) 25:73518. doi: 10.5380/ce.v25i0.73518
19. Boas AV. Spirituality and health in pandemic times: lessons from the ancient wisdom. Religions. (2020) 11:1–19. doi: 10.3390/rel11110583
20. Mehta S, Saxena T, Purohit N. The new consumer behaviour paradigm amid COVID-19: permanent or transient?. J Health Manag. (2020) 22:291–301. doi: 10.1177/0972063420940834
21. Sheth JN, Sethia NK, Srinivas S. Mindful consumption: a customer-centric approach to sustainability. J Acad Mark Sci. (2011) 39:21–39. doi: 10.1007/s11747-010-0216-3
22. Kazemi A, Azimian J, Mafi M, Allen K-A, Motalebi SA. Caregiver burden and coping strategies in caregivers of older patients with stroke. BMC Psychol. (2021) 9:1–9. doi: 10.1186/s40359-021-00556-z
23. Sharif Nia H, Pahlevan Sharif S, Goudarzian AH, Allen KA, Jamali S, Gorji MAH. The relationship between religious coping and self-care behaviors in Iranian medical students. J Relig Health. (2017) 56:2109–17. doi: 10.1007/s10943-017-0376-2
24. Clark M, Emerson A. Spirituality in psychiatric nursing: a concept analysis. J Am Psychiatr Nurses Assoc. (2020) 27:22–32. doi: 10.1177/1078390320902834
25. Weathers E, McCarthy G, Coffey A. Concept analysis of spirituality: an evolutionary approach. Nursing Forum. (2016) 51:79–96. doi: 10.1111/nuf.12128
26. Frydenberg E, Deans J, Allen K-A. Developing Children's Coping in the Early Years: Strategies for Dealing With Stress, Change and Anxiety. (Sydney: Bloomsbury Academic) (2012).
27. Sharif Nia H, Mohammadinezhad M, Allen KA, Boyle C, Sharif SP, Rahmatpour P. Psychometric evaluation of the Persian version of the spiritual well-being scale (SWBS) in Iranian patients with cancer. Palliative Support Care. (2021) 1–9. doi: 10.1017/S1478951521000407
28. Soleimani MA, Pahlevan Sharif S, Allen KA, Yaghoobzadeh A, Sharif Nia H, Gorgulu O. Psychometric properties of the Persian version of spiritual well-being scale in patients with acute myocardial infarction. J Relig Health. (2017) 56:1981–97. doi: 10.1007/s10943-016-0305-9
29. Yaghoobzadeh A, Soleimani MA, Allen KA, Chan YH, Herth KA. Relationship between spiritual well-being and hope in patients with cardiovascular disease. J Relig Health. (2018) 57:938–50. doi: 10.1007/s10943-017-0467-0
30. Kim AW, Nyengerai T, Mendenhall E. Evaluating the mental health impacts of the COVID-19 pandemic: perceived risk of COVID-19 infection and childhood trauma predict adult depressive symptoms in urban South Africa. Psychol Med. (2020) 1–13. doi: 10.1017/S0033291720003414
31. Galea S, Merchant RM, Lurie N. The mental health consequences of COVID-19 and physical distancing: the need for prevention and early intervention. JAMA Intern Med. (2020) 180:817–8. doi: 10.1001/jamainternmed.2020.1562
32. Koenig HG. Maintaining health and well-being by putting faith into action during the COVID-19 pandemic. J Relig Health. (2020) 59:2205–14. doi: 10.1007/s10943-020-01035-2
33. Lucchetti G, Góes LG, Amaral SG, Ganadjian GT, Andrade I, Almeida POA, et al. Spirituality, religiosity and the mental health consequences of social isolation during Covid-19 pandemic. Int J Soc Psychiatry. (2020). p.1-8 doi: 10.1177/0020764020970996
34. Milner K, Crawford P, Edgley A, Hare-Duke L, Slade M. The experiences of spirituality among adults with mental health difficulties: a qualitative systematic review. Epidemiol Psychiatr Sci. (2020) 29:e34. doi: 10.1017/S2045796019000234
35. Mahamid FA, Bdier D. The association between positive religious coping, perceived stress, and depressive symptoms during the spread of coronavirus (COVID-19) among a sample of adults in palestine: across sectional study. J Relig Health. (2021) 60:34–49. doi: 10.1007/s10943-020-01121-5
36. Eagle DE, Hybels CF, Proeschold-Bell RJ. Perceived social support, received social support, and depression among clergy. J Soc Pers Relat. (2018) 36:2055–73. doi: 10.1177/0265407518776134
37. Eslahi Z, Bahrami N, Allen KA, Alimoradi Z. Spouse's social support in the postpartum period, predictors and its relationship with postpartum depression in a sample of Iranian primiparous women. Int J Gynecol Obstetr. (2021) 154:24–30. doi: 10.1002/ijgo.13488
38. Grey I, Arora T, Thomas J, Saneh A, Tohme P, Abi-Habib R. The role of perceived social support on depression and sleep during the COVID-19 pandemic. Psychiatry Res. (2020) 293:113452. doi: 10.1016/j.psychres.2020.113452
39. Nikbakht Nasrabadi A, Pahlevan Sharif S, Allen KA, Naghavi N, Sharif Nia H, Salisu WJ, et al. The role of socioeconomic status in the relationship between social support and burden among cancer caregivers. Eur J Cancer Prev. (2021) doi: 10.1097/CEJ.0000000000000683
40. Kaniasty K, Norris FH. Longitudinal linkages between perceived social support and posttraumatic stress symptoms: sequential roles of social causation and social selection. J Trauma Stress. (2008) 21:274–81. doi: 10.1002/jts.20334
41. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. (1985) 98:310–57. doi: 10.1037/0033-2909.98.2.310
42. John-Henderson NA, Stellar JE, Mendoza-Denton R, Francis DD. Socioeconomic status and social support: social support reduces inflammatory reactivity for individuals whose early-life socioeconomic status was low. Psychol Sci. (2015) 26:1620–9. doi: 10.1177/0956797615595962
43. Qi M, Zhou S-J, Guo Z-C, Zhang L-G, Min H-J, Li X-M, et al. The effect of social support on mental health in Chinese adolescents during the outbreak of COVID-19. J Adolesc Health. (2020) 67:514–8. doi: 10.1016/j.jadohealth.2020.07.001
44. Sperry DM, Widom CS. Child abuse and neglect, social support, and psychopathology in adulthood: a prospective investigation. Child Abuse Negl. (2013) 37:415–25. doi: 10.1016/j.chiabu.2013.02.006
45. Guntzviller LM, Williamson LD, Ratcliff CL. Stress, social support, and mental health among young adult hispanics. Fam Commun Health. (2020) 43:82–91. doi: 10.1097/FCH.0000000000000224
46. Simons HR, Thorpe LE, Jones HE, Lewis JB, Tobin JN, Ickovics JR. Perinatal depressive symptom trajectories among adolescent women in New York City. J Adolesc Health. (2020) 67:84–92. doi: 10.1016/j.jadohealth.2019.12.017
47. Glozah FN. Exploring Ghanaian adolescents' meaning of health and well-being: a psychosocial perspective. Int J Qual Stud Health Well Being. (2015) 10:26370. doi: 10.3402/qhw.v10.26370
48. Liu CH, Zhang E, Wong GTF, Hyun S, Hahm HC. Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for U.S. young adult mental health. Psychiatry Res. (2020) 290:113172. doi: 10.1016/j.psychres.2020.113172
49. Xiao H, Zhang Y, Kong D, Li S, Yang N. The effects of social support on sleep quality of medical staff treating patients with coronavirus disease 2019 (COVID-19) in January and February 2020 in China. Med Sci Monit Int Med J Exp Clin Res. (2020) 26:e923549. doi: 10.12659/MSM.923549
50. El-Zoghby SM, Soltan EM, Salama HM. Impact of the COVID-19 pandemic on mental health and social support among adult Egyptians. J Community Health. (2020) 45:689–95. doi: 10.1007/s10900-020-00853-5
51. Yu H, Li M, Li Z, Xiang W, Yuan Y, Liu Y, et al. Coping style, social support and psychological distress in the general Chinese population in the early stages of the COVID-19 epidemic. BMC Psychiatry. (2020) 20:426. doi: 10.1186/s12888-020-02826-3
52. Pahlevan Sharif S, Naghavi N, Nia HS, Waheed H. Financial literacy and quality of life of consumers faced with cancer: a moderated mediation approach. Int J Bank Mark. (2020) 5:1009–31. doi: 10.1108/IJBM-10-2019-0355
53. Sherman EJ, Pfister DG, Ruchlin HS, Rubin DM, Radzyner MH, Kelleher GH, et al. The Collection of Indirect and Nonmedical Direct Costs (COIN) form: a new tool for collecting the invisible costs of androgen independent prostate carcinoma. Cancer. (2001) 91:841–853. doi: 10.1002/1097-0142(20010215)91:4<841::AID-CNCR1072>3.0.CO;2-B
54. Chongpison Y, Hornbrook MC, Harris RB, Herrinton LJ, Gerald JK, Grant M, et al. Self-reported depression and perceived financial burden among long-term rectal cancer survivors. Psychooncology. (2016) 25:1350–6. doi: 10.1002/pon.3957
55. Hastert TA, Ruterbusch JJ, Nair M, Noor MI, Beebe-Dimmer JL, Schwartz K, et al. Employment outcomes, financial burden, anxiety, and depression among caregivers of African American Cancer survivors. JCO Oncol Pract. (2020) 16:e221–33. doi: 10.1200/JOP.19.00410
56. Jones SM, Henrikson NB, Panattoni L, Syrjala KL, Shankaran V. A theoretical model of financial burden after cancer diagnosis. Fut Oncol. (2020) 16:3095–105. doi: 10.2217/fon-2020-0547
57. Santos S, Crespo C, Canavarro MC, Alderfer MA, Kazak AE. Family rituals, financial burden, and mothers' adjustment in pediatric cancer. J Fam Psychol. (2016) 30:1008. doi: 10.1037/fam0000246
58. Barzilay R, Moore TM, Greenberg DM, DiDomenico GE, Brown LA, White LK, et al. Resilience, COVID-19-related stress, anxiety and depression during the pandemic in a large population enriched for healthcare providers. Transl Psychiatry. (2020) 10:1–8. doi: 10.1038/s41398-020-00982-4
59. Gur RE, White LK, Waller R, Barzilay R, Moore TM, Kornfield S, et al. The disproportionate burden of the COVID-19 pandemic among pregnant black women. Psychiatry Res. (2020) 293:113475. doi: 10.1016/j.psychres.2020.113475
60. Salsman JM, Schalet BD, Andrykowski MA, Cella D. The impact of events scale: a comparison of frequency versus severity approaches to measuring cancer-specific distress. Psychooncology. (2015) 24:1738–45. doi: 10.1002/pon.3784
61. Sharif Nia H, Kaur H, Rahmatpour P, Pahlevansharif S, Venugopal AV, Hosseini L. Psychometric properties of the impact of events scale-revised (IES-R) among general iranian population during the COVID-19 pandemic. Front Psychiatry. (2021) 12:1177. doi: 10.3389/fpsyt.2021.692498
62. Weiss DS. The impact of event scale: revised. In: Cross-Cultural Assessment of Psychological Trauma and PTSD. Springer: Boston, MA (2007). p. 219–38.
63. Paulino M, Dumas-Diniz R, Brissos S, Brites R, Alho L, Simões MR, et al. COVID-19 in Portugal: exploring the immediate psychological impact on the general population. Psychol Health Med. (2020) 26, 44–55. doi: 10.1080/13548506.2020.1808236
64. Rodríguez-Rey R, Garrido-Hernansaiz H, Collado S. Psychological impact and associated factors during the initial stage of the coronavirus (COVID-19) pandemic among the general population in Spain. Front Psychol. (2020) 11:1540. doi: 10.3389/fpsyg.2020.01540
65. Spoorthy MS, Pratapa SK, Mahant S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic–a review. Asian J Psychiatr. (2020) 51:102119. doi: 10.1016/j.ajp.2020.102119
66. Tee ML, Tee CA, Anlacan JP, Aligam KJG, Reyes PWC, Kuruchittham V, et al. Psychological impact of COVID-19 pandemic in the Philippines. J Affect Disord. (2020) 277:379–91. doi: 10.1016/j.jad.2020.08.043
67. Zhang C, Ye M, Fu Y, Yang M, Luo F, Yuan J, et al. The psychological impact of the COVID-19 pandemic on teenagers in China. J Adolesc Health. (2020) 67:747–55. doi: 10.1016/j.jadohealth.2020.08.026
68. Amin F, Sharif S, Saeed R, Durrani N, Jilani D. COVID-19 pandemic- knowledge, perception, anxiety and depression among frontline doctors of Pakistan. BMC Psychiatry. (2020) 20:459. doi: 10.1186/s12888-020-02864-x
69. Muller AE, Hafstad EV, Himmels JPW, Smedslund G, Flottorp S, Stensland SØ, et al. The mental health impact of the covid-19 pandemic on healthcare workers, and interventions to help them: a rapid systematic review. Psychiatry Res. (2020) 293:113441. doi: 10.1016/j.psychres.2020.113441
70. Pappa S, Ntella V, Giannakas T, Giannakoulis VG, Papoutsi E, Katsaounou P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. (2020) 88:901–7. doi: 10.1016/j.bbi.2020.05.026
71. Vindegaard N, Benros ME. COVID-19 pandemic and mental health consequences: systematic review of the current evidence. Brain Behav Immun. (2020) 89:531–42. doi: 10.1016/j.bbi.2020.05.048
72. Cai X, Hu X, Ekumi IO, Wang J, An Y, Li Z, et al. Psychological distress and its correlates among COVID-19 survivors during early convalescence across age groups. Am J Geriatr Psychiatry. (2020) 28:1030–9. doi: 10.1016/j.jagp.2020.07.003
73. Holmes EA, O'Connor RC, Perry VH, Tracey I, Wessely S, Arseneault L, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. (2020) 7:547–60. doi: 10.1016/S2215-0366(20)30168-1
74. Calculator FS. A-Priori Sample Size for Structural Equation Models Calculator. Available online at: https://www.danielsoper.com/statcalc/calculator.aspx?id=89 (accessed September 1, 2021).
76. Mitchell PH, Powell L, Blumenthal J, Norten J, Ironson G, Pitula CR, et al. A short social support measure for patients recovering from myocardial infarction: the ENRICHD Social Support Inventory. J Cardiopulm Rehabil Prev. (2003) 23:398–403. doi: 10.1097/00008483-200311000-00001
77. Pahlevan Sharif S Sim OF Moshtagh M Naghavi N Sharif Nia. H. Psychometric evaluation of the comprehensive score for financial toxicity scale among Iranian cancer patients. (2020). doi: 10.21203/rs.2.22672/v1
78. De Souza JA, Yap BJ, Hlubocky FJ, Wroblewski K, Ratain MJ, Cella D, et al. The development of a financial toxicity patient-reported outcome in cancer: the COST measure. Cancer. (2014) 120:3245–53. doi: 10.1002/cncr.28814
79. Sharif Nia H, Rezapour M, Allen KA, Sharif SP, Jafari A, Torkmandi H, et al. The psychometric properties of the center for epidemiological studies depression scale (CES-D) for Iranian cancer patients. Asian Pacific J Cancer Prev. (2019) 20:2803–9. doi: 10.31557/APJCP.2019.20.9.2803
80. Duncan OD. Path analysis: sociological examples. Am J Sociol. (1966) 72:1–16. doi: 10.1086/224256
81. SahInler S, Görgülü Ö. Path analysis and an application. Ziraat Fakultesi Dergisi, Mustafa Kemal Universitesi. (2000) 5:87–102.
82. Curtis CR, Erb HN, Sniffen CJ, Smith RD, Kronfeld DS. Path analysis of dry period nutrition, postpartum metabolic and reproductive disorders, and mastitis in Holstein cows. J Dairy Sci. (1985) 68:2347–60. doi: 10.3168/jds.S0022-0302(85)81109-7
83. Erb H, Martin S, Ison N, Swaminathan S. Interrelationships between production and reproductive diseases in Holstein cows. Path analysis. J Dairy Sci. (1981) 64:282–9. doi: 10.3168/jds.S0022-0302(81)82565-9
84. Anoushiravani AA, O'Connor CM, DiCaprio MR, Iorio R. Economic Impacts of the COVID-19 crisis: an orthopaedic perspective. J Bone Joint Surg Am. (2020) 102:937–41. doi: 10.2106/JBJS.20.00557
85. Roll S, Despard M. Income loss and financial distress during COVID-19: the protective role of liquid assets. (2020) 3733862. doi: 10.2139/ssrn.3733862
86. Assari S. Race, depression, and financial distress in a nationally representative sample of American adults. Brain Sci. (2019) 9:29. doi: 10.3390/brainsci9020029
87. Mamun MA, Akter S, Hossain I, Faisal MTH, Rahman MA, Arefin A, et al. Financial threat, hardship and distress predict depression, anxiety and stress among the unemployed youths: a Bangladeshi multi-city study. J Affect Disord. (2020) 276:1149–58. doi: 10.1016/j.jad.2020.06.075
88. Rogers ES. Financial distress and smoking-induced deprivation in smokers with depression. Am J Health Behav. (2019) 43:219–27. doi: 10.5993/AJHB.43.1.18
89. Barbisch D, Koenig KL, Shih F-Y. Is there a case for quarantine? Perspectives from SARS to Ebola. Disaster Med Public Health Prepared. (2015) 9:547–53. doi: 10.1017/dmp.2015.38
91. Hou F, Bi F, Jiao R, Luo D, Song K. Gender differences of depression and anxiety among social media users during the COVID-19 outbreak in China:a cross-sectional study. BMC Public Health. (2020) 20:1648. doi: 10.1186/s12889-020-09738-7
92. Özdin S, Bayrak Özdin S. Levels and predictors of anxiety, depression and health anxiety during COVID-19 pandemic in Turkish society: the importance of gender. Int J Soc Psychiatry. (2020) 66:504–11. doi: 10.1177/0020764020927051
93. Sønderskov KM, Dinesen PT, Santini ZI, Østergaard SD. The depressive state of Denmark during the COVID-19 pandemic. Acta Neuropsychiatr. (2020) 32:226–8. doi: 10.1017/neu.2020.15
94. Brooks SK, Webster RK, Smith LE, Woodland L, Wessely S, Greenberg N, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. (2020) 395:912–20. doi: 10.1016/S0140-6736(20)30460-8
95. Alsubaie MM, Stain HJ, Webster LAD, Wadman R. The role of sources of social support on depression and quality of life for university students. Int J Adolesc Youth. (2019) 24:484–96. doi: 10.1080/02673843.2019.1568887
96. Bostean G, Andrade FCD, Viruell-Fuentes EA. Neighborhood stressors and psychological distress among U.S. Latinos: measuring the protective effects of social support from family and friends. Stress Health. (2019) 35:115–26. doi: 10.1002/smi.2843
97. Lee HS, Kim C. Structural equation modeling to assess discrimination, stress, social support, and depression among the elderly women in South Korea. Asian Nurs Res. (2016) 10:182–8. doi: 10.1016/j.anr.2016.06.003
98. Zhen R, Quan L, Zhou X. How does social support relieve depression among flood victims? The contribution of feelings of safety, self-disclosure, and negative cognition. J Affective Disord. (2018) 229:186–92. doi: 10.1016/j.jad.2017.12.087
99. Torkian S, Akhlaghi E, Khosravi V, Etesami R, Ahmadi A, Khanjani N, et al. Social support and adjustment during COVID-19 epidemic: a community-based study in Iran. Iran J Psychiatry Behav Sci. (2020) 14:e108503. doi: 10.5812/ijpbs.108503
100. Aktürk S, Aktürk Ü. Determining the spiritual well-being of patients with spinal cord injury. J Spinal Cord Med. (2020) 43:69–76. doi: 10.1080/10790268.2018.1490875
101. Duran S, Avci D, Esim F. Association between spiritual well-being and resilience among Turkish hemodialysis patients. J Relig Health. (2020) 59:3097–109. doi: 10.1007/s10943-020-01000-z
102. Smith-MacDonald L, Norris JM, Raffin-Bouchal S, Sinclair S. Spirituality and mental well-being in combat veterans: a systematic review. Mil Med. (2017) 182:e1920–40. doi: 10.7205/MILMED-D-17-00099
103. Al-Nasa'h M. A spiritual-based intervention in enhancing factors of well-being among older adults in home-based care. J Relig Spiritual Aging. (2020) 1–22. doi: 10.1080/15528030.2020.1818160
104. Vasegh S, Mohammadi MR. Religiosity, anxiety, and depression among a sample of Iranian medical students. Int J Psychiatry Med. (2007) 37:213–27. doi: 10.2190/J3V5-L316-0U13-7000
105. Rahnama P, Javidan AN, Saberi H, Montazeri A, Tavakkoli S, Pakpour AH, et al. Does religious coping and spirituality have a moderating role on depression and anxiety in patients with spinal cord injury? A study from Iran. Spinal Cord. (2015) 53:870–4. doi: 10.1038/sc.2015.102
106. Honarvar N, Taghavi M. Relation of religious coping and depression levels in infertile women. Iran J Psychiatry. (2020) 15:134–42. doi: 10.18502/ijps.v15i2.2685
107. Sharif Nia H, Pahlevan Sharif S, Esmaeili R, Goudarzian AH, Tahmasbi B, Yaghoobzadeh A, et al. Factors influencing the level of death depression in patients with cancer: a path analysis. J Mazandaran Univ Med Sci. (2017) 26:318–31.
108. Bonelli R, Dew RE, Koenig HG, Rosmarin DH, Vasegh S. Religious and spiritual factors in depression: review and integration of the research. Depress Res Treat. (2012) 2012:962860. doi: 10.1155/2012/962860
109. Van de Velde SM, Buffel V, Van Praag L. Depressive feelings in religious minorities: does the religious context matter? J Relig Health. (2020) 59:2504–30. doi: 10.1007/s10943-020-00999-5
110. Watson PJ, Ghorbani N, Davison HK, Bing MN, Hood RW, Ghramaleki AF. RESEARCH: negatively reinforcing personal extrinsic motivations: religious orientation, inner awareness, and mental health in Iran and the United States. Int J Psychol Relig. (2002) 12:255–76. doi: 10.1207/S15327582IJPR1204_04
111. Robinson OC, Hanson K, Hayward G, Lorimer D. Age and cultural gender equality as moderators of the gender difference in the importance of religion and spirituality: comparing the United Kingdom, France, and Germany. J Sci Study Relig. (2019) 58:301–8. doi: 10.1111/jssr.12567
112. Simpson DB, Cloud DS, Newman JL, Fuqua DR. Sex and gender differences in religiousness and spirituality. J Psychol Theol. (2008) 36:42–52. doi: 10.1177/009164710803600104
113. Zhang J, Wu W, Zhao X, Zhang W. Recommended psychological crisis intervention response to the 2019 novel coronavirus pneumonia outbreak in China: a model of West China Hospital. Precis Clin Med. (2020) 3:3–8. doi: 10.1093/pcmedi/pbaa006
114. Bartsch SM, Ferguson MC, McKinnell JA, O'Shea KJ, Wedlock PT, Siegmund SS, et al. The potential health care costs and resource use associated with COVID-19 in the United States. Health Aff. (2020) 39:927–35. doi: 10.1377/hlthaff.2020.00426
115. Yoosefi Lebni J, Abbas J, Moradi F, Salahshoor MR, Chaboksavar F, Irandoost SF, et al. How the COVID-19 pandemic effected economic, social, political, and cultural factors: a lesson from Iran. Int J Soc Psychiatry. (2021) 67:298–300. doi: 10.1177/0020764020939984
116. Maarefvand M, Hosseinzadeh S, Farmani O, Safarabadi Farahani A, Khubchandani J. Coronavirus outbreak and stress in Iranians. Int J Environ Res Public Health. (2020) 17:4441. doi: 10.3390/ijerph17124441
117. Seddighi H, Dollard MF, Salmani I. Psychosocial safety climate of employees during the COVID-19 pandemic in Iran: a policy analysis. Disaster Med Public Health Prep. (2020) 1–7. doi: 10.1017/dmp.2020.370
118. González-Sanguino C, Ausín B, Castellanos MÁ, Saiz J, López-Gómez A, Ugidos C, et al. Mental health consequences during the initial stage of the 2020 Coronavirus pandemic (COVID-19) in Spain. Brain Behav Immun. (2020) 87:172–6. doi: 10.1016/j.bbi.2020.05.040
119. Roger KS, Hatala A. Religion, spirituality and chronic illness: a scoping review and implications for health care practitioners. J Relig Spiritual Soc Work Soc Thought. (2018) 37:24–44. doi: 10.1080/15426432.2017.1386151
120. Garssen B, Visser A, Pool G. Does spirituality or religion positively affect mental health? Meta-analysis of longitudinal studies. Int J Psychol Relig. (2021) 31:4–20. doi: 10.1080/10508619.2020.1729570
121. del Castillo FA. Health, spirituality and Covid-19: themes and insights. J Public Health. (2020) 43:e254–5. doi: 10.1093/pubmed/fdaa185
122. Vaske JJ. Advantages and disadvantages of internet surveys: introduction to the special issue. Hum Dimens Wildl. (2011) 16:149–53. doi: 10.1080/10871209.2011.572143
123. Wright KB. Researching internet-based populations: advantages and disadvantages of online survey research, online questionnaire authoring software packages, and web survey services. J Comput Mediat Commun. (2017) 10. doi: 10.1111/j.1083-6101.2005.tb00259.x
124. Gibson AM, Bowling NA. (2019) The effects of questionnaire length and behavioral consequences on careless responding. Eur J Psychol Assess. doi: 10.1027/1015-5759/a000526
Keywords: COVID-19, depression, financial distress, Iran, social support, spiritual well-being, stress
Citation: Sharif Nia H, Gorgulu O, Naghavi N, Robles-Bello MA, Sánchez-Teruel D, Khoshnavay Fomani F, She L, Rahmatpour P, Allen K-A, Arslan G and Pahlevan Sharif S (2021) Spiritual Well-Being, Social Support, and Financial Distress in Determining Depression: The Mediating Role of Impact of Event During COVID-19 Pandemic in Iran. Front. Psychiatry 12:754831. doi: 10.3389/fpsyt.2021.754831
Received: 07 August 2021; Accepted: 28 September 2021;
Published: 28 October 2021.
Edited by:
Roberto Nuevo, Rey Juan Carlos University, SpainReviewed by:
Hesham Fathy Gadelrab, Mansoura University, EgyptSi-Tong Chen, Victoria University, Australia
Copyright © 2021 Sharif Nia, Gorgulu, Naghavi, Robles-Bello, Sánchez-Teruel, Khoshnavay Fomani, She, Rahmatpour, Allen, Arslan and Pahlevan Sharif. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pardis Rahmatpour, cGFyLnJhaG1hdHBvdXJAZ21haWwuY29t