 Romain Icick1,2,3*
Romain Icick1,2,3* Ingrid Melle1,4
Ingrid Melle1,4 Bruno Etain2,3,5,6
Bruno Etain2,3,5,6 Margrethe Collier Høegh1
Margrethe Collier Høegh1 Sébastien Gard3,7
Sébastien Gard3,7 Sofie R. Aminoff4,8
Sofie R. Aminoff4,8 Marion Leboyer2,9,10
Marion Leboyer2,9,10 Ole A. Andreassen1,4Raoul Belzeaux11Chantal Henry5,12
Ole A. Andreassen1,4Raoul Belzeaux11Chantal Henry5,12 Thomas D. Bjella1Jean-Pierre Kahn13
Thomas D. Bjella1Jean-Pierre Kahn13 Nils Eiel Steen1,4
Nils Eiel Steen1,4 Frank Bellivier2,3,5,6Trine Vik Lagerberg1,4
Frank Bellivier2,3,5,6Trine Vik Lagerberg1,4- 1Norwegian Centre for Mental Disorders Research (NORMENT), Division of Mental Health and Addiction, Oslo University Hospital, Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 2FondaMental Foundation, Créteil, France
- 3INSERM U1144, Université Paris Cité, Paris, France
- 4Institute of Clinical Medicine, University of Oslo, Oslo, Norway
- 5Université Paris Cité, Paris, France
- 6Assistance Publique – Hôpitaux de Paris, GH Saint-Louis – Lariboisière – F. Widal, Département de Psychiatrie, Paris, France
- 7Hôpital Charles Perrens, Centre Expert Trouble Bipolaire, Pôle de Psychiatrie Générale et Universitaire (3/4/7), Bordeaux, France
- 8Early Intervention in Psychosis Advisory Unit for South East Norway, Division of Mental Health and Addiction, Oslo University Hospital, Oslo, Norway
- 9Paris Est Créteil, INSERM U955, IMRB, Laboratoire Neuro-Psychiatrie Translationnelle, Créteil, France
- 10Assistance Publique – Hôpitaux de Paris (AP-HP), HU Henri Mondor, Département Medico-Universitaire de Psychiatrie et d’Addictologie (DMU ADAPT), Fédération Hospitalo-Universitaire de Médecine de Precision (FHU IMPACT), Créteil, France
- 11Assistance Publique – Hôpitaux de Marseille (AP-HM), Hôpital Sainte-Marguerite, Pôle de Psychiatrie, INT-UMR 7289, CNRS, Aix-Marseille University, Marseille, France
- 12Department of Psychiatry, Service Hospitalo-Universitaire, GHU Paris Psychiatrie & Neurosciences, Paris, France
- 13Université de Lorraine, CHRU de Nancy et Pôle de Psychiatrie et Psychologie Clinique, Centre Psychothérapique de Nancy, Laxou, France
Objective: The potential role of sub-optimal pharmacological treatment in the poorer outcomes observed in bipolar disorder (BD) with vs. without comorbid substance use disorders (SUDs) is not known. Thus, we investigated whether patients with BD and comorbid SUD had different medication regimens than those with BD alone, in samples from France and Norway, focusing on compliance to international guidelines.
Methods: Seven hundred and seventy patients from France and Norway with reliably ascertained BD I or II (68% BD-I) were included. Medication information was obtained from patients and hospital records, and preventive treatment was categorized according to compliance to guidelines. We used Bayesian and regression analyses to investigate associations between SUD comorbidity and medication. In the Norwegian subsample, we also investigated association with lack of medication.
Results: Comorbid SUDs were as follows: current tobacco smoking, 26%, alcohol use disorder (AUD), 16%; cannabis use disorder (CUD), 10%; other SUDs, 5%. Compliance to guidelines for preventive medication was lacking in 8%, partial in 44%, and complete in 48% of the sample. Compliance to guidelines was not different in BD with and without SUD comorbidity, as was supported by Bayesian analyses (highest Bayes Factor = 0.16). Cross national differences in treatment regimens led us to conduct country-specific adjusted regression analyses, showing that (1) CUD was associated with increased antipsychotics use in France (OR = 2.4, 95% CI = 1.4–3.9, p = 0.001), (2) current tobacco smoking was associated with increased anti-epileptics use in Norway (OR = 4.4, 95% CI = 1.9–11, p < 0.001), and (3) AUD was associated with decreased likelihood of being medicated in Norway (OR = 1.2, 95% CI = 1.04–1.3, p = 0.038).
Conclusion: SUD comorbidity in BD was overall not associated with different pharmacological treatment in our sample, and not related to the level of compliance to guidelines. We found country-specific associations between comorbid SUDs and specific medications that warrant further studies.
Introduction
Bipolar disorder (BD) is a chronic and relapsing condition associated with a high burden for individuals, caregivers, and societies (1). This burden is strongly associated with the high level of comorbidity in BD (2, 3). Comorbid substance use disorders (SUDs, including nicotine dependence/tobacco smoking) are found in up to 50–60% individuals with BD (4–6). Compared to BD alone, the presence of comorbid SUD (BD + SUD) has been associated with poorer outcomes, including premature mortality (7), higher rates of suicide attempts (8), and suicide mortality (9), as well as delayed remission from acute mood episodes (10). The presence of comorbid SUDs may complicate the pharmaceutical management of BD (11); e.g., tobacco use disorders have been associated both with a more severe psychopathology, as shown by our group (8) and others (12), and complicated pharmaceutical management (13). Beyond age and gender, additional dimensions related to abnormal self-awareness might contribute to increased SUD risk in BD, namely sensation seeking (14) and anxiety (15). These may co-exist in individuals with particularly complex BD course in case of, e.g., comorbid borderline personality disorders (16), further increasing the likelihood of complicated pharmaceutical management.
To date, there is no specific guideline for the pharmaceutical treatment of BD + SUD (17). Indeed, guidelines are often limited by the fact that they are typically based on the results of randomized controlled double-blind trials, which include selected BD patients. Consequently, patients with psychiatric comorbidities such as SUDs are often excluded. Moreover, a substantial proportion of BD patients show inadequate response to medication (18). Medication patterns in community BD samples and naturalistic settings often diverge from guidelines, increasing the risk of poor clinical outcome (19). This includes scarce lithium use (20), polypharmacy (21), frequent antidepressant (22), and benzodiazepine use (23) despite lack of evidence for their efficacy in BD and additional risk of addiction for the latter (24).
Comorbid SUDs are may play a role in both the lack of treatment response and the use of non-recommended medication regimens in BD for several reasons. Firstly, psychoactive substances can elicit a wide range of BD symptoms [e.g., psychotic and manic symptoms with cannabis (25)], which may increase the need for symptomatic treatment. Secondly, substance use also alters the pharmacodynamics [e.g., amphetamines (26)] and the pharmacokinetics [e.g., tobacco and P450 enzymes (13)] of medications for BD. Thirdly, BD + SUD has been associated with reduced treatment adherence compared to BD alone (27) – although this may be accounted for by impulsiveness (28). Fourthly, both clinicians’ and patients’ perceptions might influence prescription attitudes and modify the pharmaceutical treatment of BD in case of comorbid SUD. This might be due to lower psychoeducation level, increased stigma, or lack of confidence in treatment efficacy (29, 30). With that regards, one study reported no difference of medication profiles in BD + SUD vs. BD inpatients at discharge (31). Two other studies, although not specifically aimed at comparing BD with vs. without SUDs, reported discrepant results. One study conducted among homeless persons with BD showed that comorbid SUDs were significantly associated with inappropriate prescription regimens (32), while a nationwide French cohort study (independent from the sample analyzed in the current study) did not observe any difference in preventive BD medication in outpatients with vs. without SUDs (33). Given the paucity of available literature, knowledge about the sources of variability (34) and non-compliance to guidelines of pharmacological treatment in BD + SUD remains limited. Furthermore, the clinical management of BD patients can be affected by local customs, expert opinions, and differences in treatment availability. Likewise, the epidemiology of SUD also shows major cross-national differences. This warrants cross-national comparisons to disentangle the effects of SUDs from national trends in SUD and medication usage.
To investigate this issue, we used data from a large, well-characterized sample of patients with BD from France and Norway. Our objective was to investigate whether the presence of SUDs would be associated with different preventive medication regimens, including more frequent deviations from European guidelines, differences in the use of individual medication classes, and different likelihood of receiving current preventive medication. We further aimed to clarify whether putative relationships between medication regimens and SUDs are independent from clinical and demographic variables, especially country of inclusion.
Materials and Methods
This was a post hoc study of a sample of patients with ascertained BD recruited in France (2000–2012) and Norway (2003–2020). Both original studies aimed to extensively characterize BD in order to inform future prevention and treatment strategies, using similar assessment protocols.
Participants
Inclusion criteria for France were: (1) age ≥18 years; (2) meeting criteria for a diagnosis of BD-I or BD-II disorder according to the Diagnostic and Statistical Manual for Mental Disorders, 4th edition, text revised (DSM-IV-TR) (35); and (3) willingness and ability to provide written informed consent. In France, participants also had to (1) be under preventive medication and be euthymic at inclusion, as defined by a Montgomery-Asberg Depression Rating Scale (MADRS) score ≤8 (36) and a Young Mania Rating Scale (YMRS) score of ≤5 (37); (2) master the French language. Moreover, in France, ability to provide written informed consent also required the absence of clinically significant cognitive impairment, which was assessed using clinical judgment. In Norway, although euthymia was not a formal inclusion criterion, participants had to be clinically stable and to master a Scandinavian language. Also, specific effort was made to include cases early in their first treatment for BD. Additional exclusion criteria in Norway were: (1) history of severe head trauma and (2) intellectual disability. For Norwegian cases, who participated in a neurocognitive assessment we used an estimated IQ based on two subtests of the WAIS with a good concordance with total IQ. For a small subset of participants who did not attend the neurocognitive assessment, we undertook a comprehensive review of educational attainment, school grades, and general interview performance to rule out the presence of intellectual disability (which is defined as an IQ < 70).
Written informed consent was obtained from all participating patients in both countries. In France, The Research Ethics Board of Pitié-Salpêtrière Hospital reviewed and approved this study. In Norway, the project was approved by the Regional Committee for Medical Research Ethics and the Norwegian Data Inspectorate. This involved being registered in the database and having one’s data analyzed for research purposes.
Study Sample
A total of 770 patients with BD-I (n = 526) or BD-II (n = 244) and reliable medication status were included. Recruitment was consecutive in both countries. Patients who sought treatment for BD in psychiatric units were evaluated for eligibility for study participation by their treating clinician. We do not know how many who refused to participate, but of those referred, the refusal rate was <5%. Due to ethical regulation, data about patients, who refused to enter the study could not be analyzed. The study of treatment compliance to guidelines and individual medication classes was performed in 670 medicated cases from France and Norway. All French cases received some medication at the time of inclusion in line with inclusion criteria. They were therefore excluded from the medicated vs. unmedicated analysis. Thus, the comparison of medicated vs. unmedicated status was performed in 525 cases from Norway only (Figure 1).
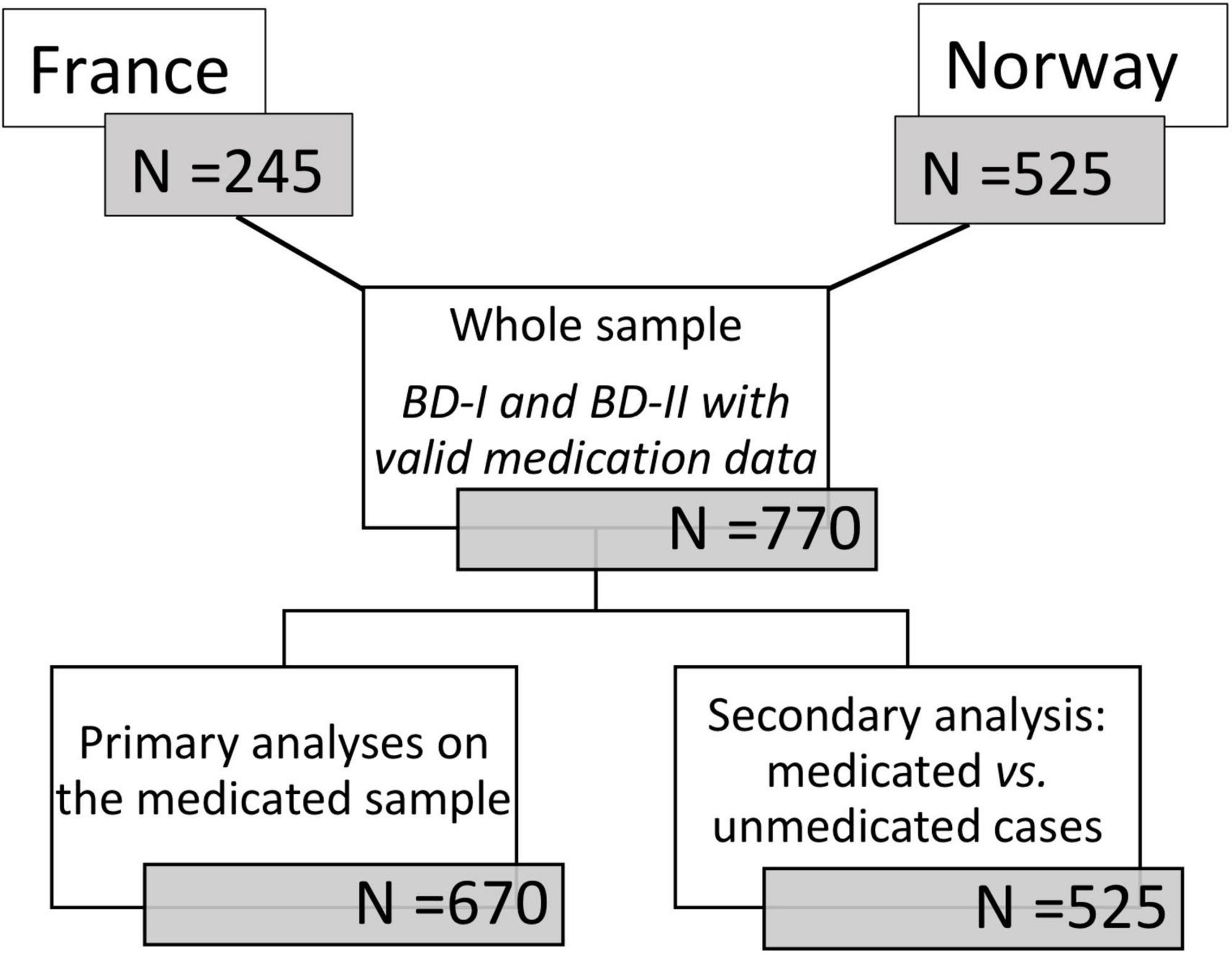
Figure 1. Flowchart for sample selection.
Clinical Assessment
Trained psychiatrists, medical doctors, and clinical psychologists carried out clinical assessments aimed at providing reliable lifetime DSM-IV BD and SUD diagnoses in both samples. Investigators used the Diagnostic Interview for Genetic Studies [DIGS (38)] in France and the Structured Clinical Interview for DSM-IV axis-I disorders [SCID-I (39)] in Norway. The course of BD was also extensively characterized.
Substance Use Assessments
Tobacco smoking was defined as smoking on a daily basis – a reliable proxy of DSM-IV nicotine dependence (40). In the French subsample, lifetime tobacco smoking (former + current) was assessed, while in the Norwegian subsample, only current tobacco smoking was considered. As such, tobacco smokers in the French subsample (N = 160) were both current (N = 99) and former smokers (N = 61), whereas those from the Norwegian subsample were current smokers only (N = 261). Diagnoses of abuse or dependence to other substances were combined to obtain single binary variables of “use disorder” for alcohol and cannabis use disorders (hereafter termed AUD and CUD, respectively), yielding the following categories: current tobacco smoking, lifetime AUD, lifetime CUD, and lifetime SUDs not related to tobacco nor alcohol nor cannabis, hereafter termed “other SUDs.” Additionally, we kept the possibility of analyzing all SUDs that were not AUD, i.e., CUD + “other SUDs,” in case the subgroups would be deemed too small and/or yielded borderline associations.
Medication Regimens
In both countries, current medications were recorded and categorized by the investigator into: lithium, anti-epileptics (valproate derivatives including valpromide, carbamazepine, lamotrigine), antipsychotics, antidepressants, and benzodiazepines. The sample can be considered as naturalistic with regards to medications since participants were recruited with their treatment as prescribed by the clinician in charge, which was thus unrelated to the current study (although being medicated was an inclusion criterion in the French sample).
Treatment Compliance to Guidelines
Firstly, we categorized the sample in relation to level of compliance to recommendations for preventive treatment of international guidelines [e.g., NICE (41), CANMAT/ISBD (42)], where lithium, several antiepileptics (valproate/valpromide/carbamazepine/lamotrigine) and antipsychotics are considered first-line mood-stabilizers. Antiepileptics and antipsychotics with primary indication in BD were identified from the Norwegian and French national recommendations. Compliance to those guidelines was deemed absent when the participant was using antidepressant or benzodiazepine without mood-stabilizer, partial if any antidepressant or benzodiazepine was used together with mood-stabilizer and complete when no antidepressant or benzodiazepines and any mood-stabilizer was used. Importantly, we focused on preventive treatment, since the samples are euthymic or next-to-euthymic and the range of episode-specific treatments was deemed too large. Regardless of underlying mood-stabilizing treatment, we considered that antidepressants and benzodiazepines remained not fully compliant in the maintenance phase of BD. Such medications are often used at some point in the course of BD, whether during the initial – often undiagnosed – phase where unspecific depressive and anxiety can prevail (43), to alleviate symptoms of comorbid anxiety disorders (3), or for the acute treatment of depressive episodes. Benzodiazepines and/or antidepressants are not easily discontinued. This may be due to prevasive residual symptoms (44) and/or clinicians’ beliefs and patients’ anticipatory anxiety regarding medication cessation (28). However, they have been associated with a wide range of adverse features in BD, including manic symptoms and rapid cycling for antidepressants (45) and cognitive impairment and addictive disorders for benzodiazepines (23). Additionally, both the possible causes and consequences of prescribing antidepressants and/or benzodiazepines in BD have been associated with SUD comorbidity in BD (46, 47), further warranting the focus on these medication classes as proposed in the current study.
Individual Medical Classes
Secondly, we analyzed each individual medication class and their relationship to SUD and key sociodemographic and clinical variables, by country.
Medicated vs. Unmedicated
Thirdly, in the Norwegian subsample we were also able to compare SUD rates in those not using any psychotropic treatment (“unmedicated”) vs. those receiving psychotropic medication (“medicated”). Here, we excluded cases in their first treatment episode for (hypo)mania (n = 195), as preventive treatment may not yet have been initiated in these cases. We analyzed the “medicated” status separately because we anticipated that this would be associated with different patient histories and clinical correlates as compared to guidelines compliance and medication regimens. In order to explore these results further, we also present data from a subsample of 161 cases, who filled in both the Medication Adherence Rating Scale (MARS) (48) to measure adherence, and the Beliefs about Medicines Questionnaire (BMQ) (49) to measure the general attitude toward medicine and medication and to estimate how much the patients’ concerns overcome his/her perceived needs for medication, using the general and the specific subscales. Of note, these secondary analyses are provided for discussion purposes only.
Statistics
Data are described as means (standard deviation, SD), medians (interquartile range, IQR) or counts (frequency). Bivariate tests were performed for SUDs only and medication-related variables, namely: in the sample as a whole and – if any of these variables exhibited cross-national differences – in each country, separately for compliance to guidelines and individual medication classes (lithium, anti-epileptics, antipsychotics, antidepressants, and benzodiazepines) and in the Norwegian subsample for the status “being medicated.” We used trend tests for variables with >2 groups and Chi-squared or Fisher’s exact tests for the others, based on a threshold for statistical significance at p < 0.05 (two-tailed tests). In order to verify the null hypothesis when a lack of difference in the medication pattern according to the SUD status will be observed, we computed Bayes factors (BF) with the R package BayesFactor. A BF can take any decimal value above zero. A value of 1 indicates equal evidence for both the H1 and H0 hypotheses. The more the value closes to zero, the stronger evidence for an absence of difference. To interpret BFs, we used the recommended thresholds (50) (Supplementary Table 1).
Each medication pattern variable (compliance to guidelines, specific medication classes and being medicated vs. unmedicated) significantly associated with one of the SUD variables was used as the dependent variable into regression models to ascertain the independence of associations from potential confounders. These confounders were chosen when they were associated with a given medication variable, at p < 0.05, two-tailed bivariate tests. In the case of a lack of association between and SUDs and our main medication-related variables – namely: compliance to guidelines and the status of “being medicated,” an exploratory regression model was still performed in order to fully test our main hypotheses. All analyses were conducted with R version 4.0.2 (51) through R studio version 1.3.1093 for Mac OS® X.14.6. A summary of the packages that were used is available as a Supplementary Methods.
Results
Description of Medication and Substance Use Disorder in the Whole Sample (n = 670)
Compliance with international guidelines was distributed as follows: absent in 53 (8%) cases, partial in 296 (44%) cases, and complete in the remaining 321 (48%) cases. A majority of patients (55%) reported polypharmacy. Current smoking was reported by 174 participants (26%). AUD was diagnosed in 104 (16%), CUD in 66 (10%), and other SUDs in 28 (5%) patients (Table 1).
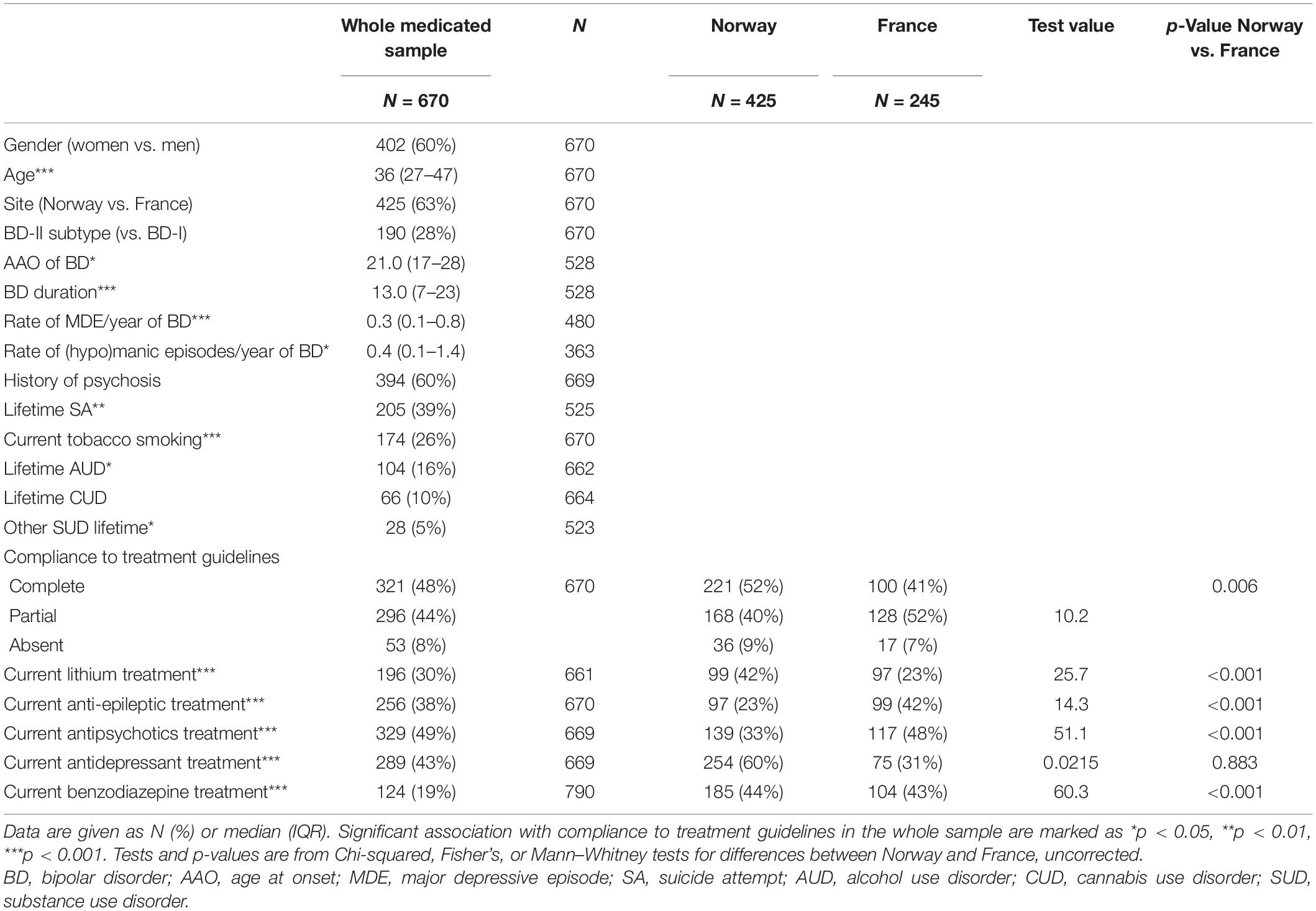
Table 1. Description of the medicated sample, as a whole, and by country.
Compliance to Guidelines Across Substance Use Disorders
We found no difference in terms of compliance to guidelines regarding comorbid SUDs (Table 2); fully consistent with Bayes Factors (Supplementary Figure 1), which indicated strong evidence for a lack of difference. In ordinal logistic regression, neither current smoking, AUD or CUD were associated with non-guideline compliant treatment (lowest p-value = 0.21 for CUD). However, in this model, female gender (OR = 1.6, p = 0.014) and BD-II subtype (OR = 2.6, p < 0.001) remained independently associated with lower compliance to guidelines (data not shown).
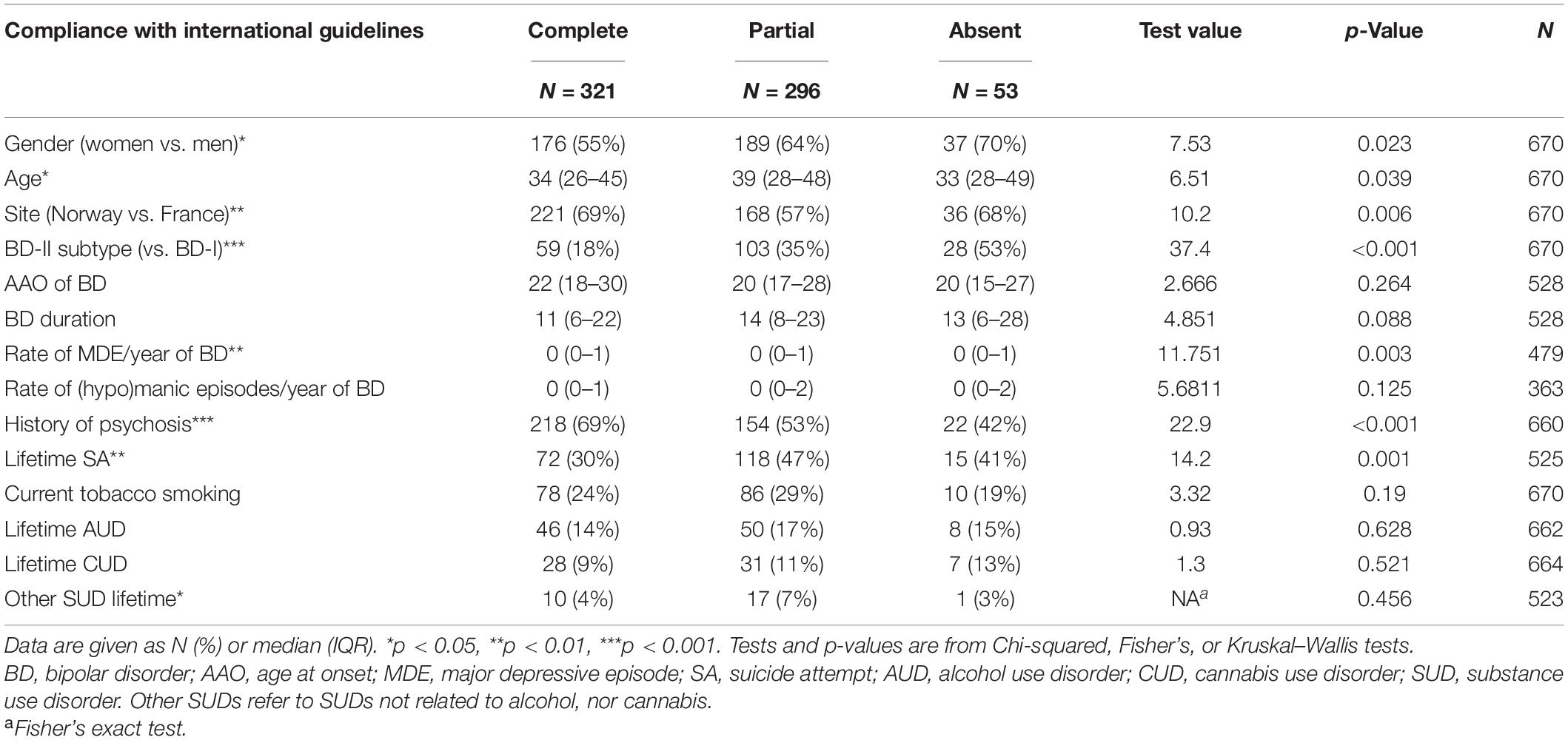
Table 2. Variables associated with compliance to treatment guidelines in the whole medicated sample (N = 670).
Individual Medication Classes Across Substance Use Disorders
There was no significant difference in individual medication classes as a function of SUDs (Supplementary Table 2), which was supported by Bayes Factors as well (Supplementary Figure 1). The complete medication patterns as a function of SUD comorbidity is shown in Supplementary Figure 2. Since there were significant differences in the proportion of French vs. Norwegian cases regarding compliance to guidelines (Table 1) and every individual medication classes but antidepressants (highest p = 0.006), we further characterized country effects and country-specific medication regimens.
Norwegian cases were more likely than the French to receive compliant treatment (52 vs. 41%, overall p = 0.006), probably due to the higher proportion of French cases receiving treatment with partial compliance to guidelines (40 vs. 52%). This was likely driven by large differences in benzodiazepine use (10 vs. 34%). Additionally, the absence of compliance to guidelines seemed more frequent in Norway compared to France (9 vs. 7%), which further legitimated country-specific follow-up analyses of the relationship between (1) SUDs and compliance to guidelines and (2) SUDs and individual medication classes, as shown below.
Country-Specific Associations Between Substance Use Disorders and Compliance to Guidelines
Both BFs (Supplementary Figure 2) and exploratory ordinal regressions (data not shown) supported an absence of country effect in the compliance to guidelines (lowest p-values = 0.21 for AUD in France and 0.45 for CUD in Norway, respectively).
Country-Specific Associations Between Substance Use Disorders and Individual Medication Classes
In Norway (Supplementary Table 3), antiepileptics use was more frequent in current compared to former + never smokers (p = 0.001). Follow-up binary regressions showed that tobacco smoking remained significantly associated with increased antiepileptics use (OR = 2.4, 95% CI = 1.4–3.9, p = 0.001) after controlling for the effects of BD subtype (BD-II vs. BD-I, OR = 1.7, 95% CI = 1.1–2.6, p = 0.019) (Figure 2A). The AUC of the model was 0.68, based on 239 cases. There was no other association between individual SUD and individual medication classes in the Norwegian subsample.
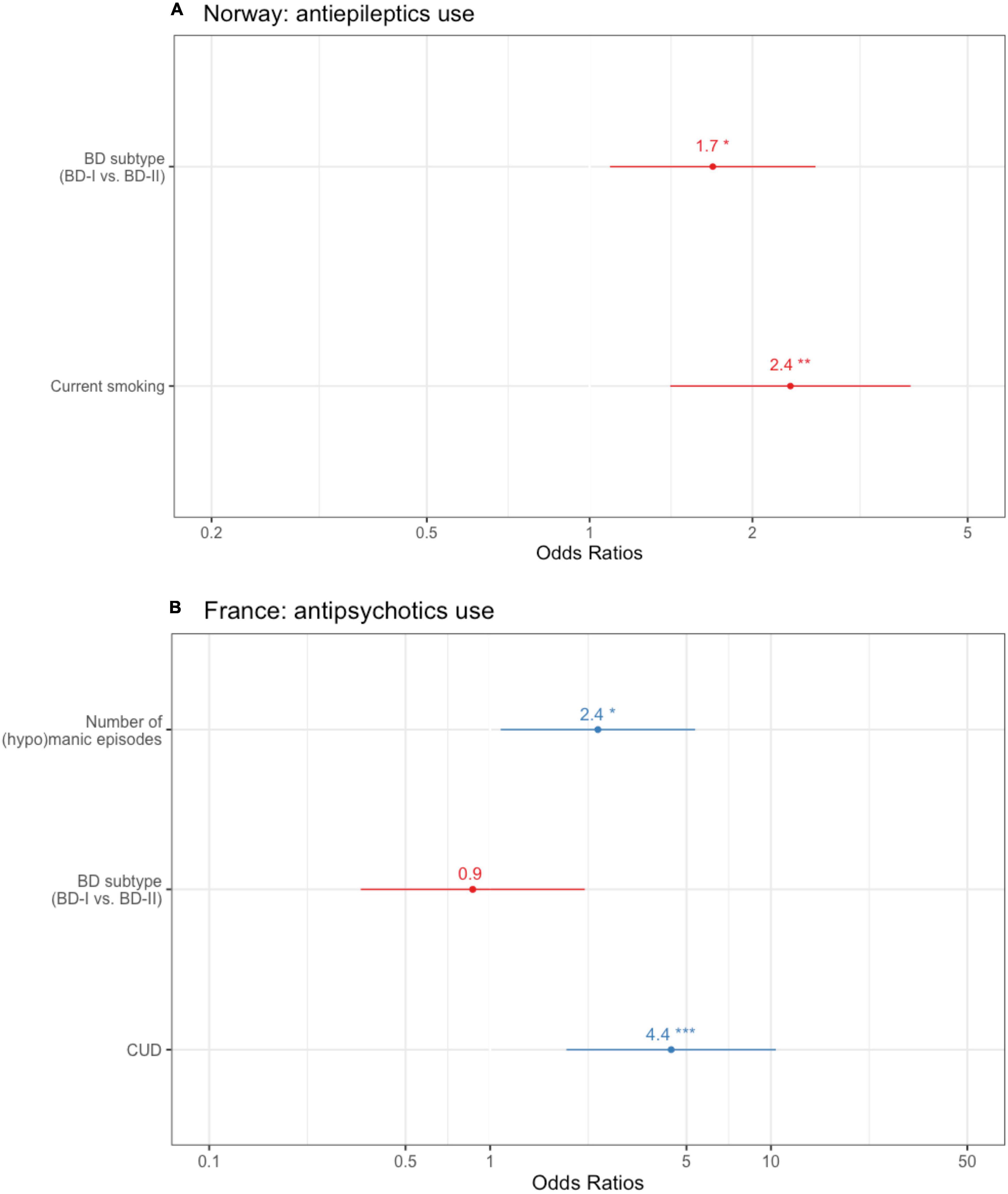
Figure 2. Country-specific binary logistic regressions with (A) anti-epileptics use in the Norwegian subsample (N = 425) and (B) antipsychotics use as the dependent variable in the French subsample (N = 243; the SUD predictor of interest is CUD). Bar length indicates 95% confidence interval. AAO, age at onset; BD, bipolar disorder; CUD, cannabis use disorder. Other SUD refers to SUDs not related to alcohol, nor cannabis. *p < 0.05, **p < 0.01, ***p < 0.001.
In France (Supplementary Table 4), antipsychotics use was more frequent in case of lifetime CUD (p < 0.001). This was confirmed by binary regression, where CUD remained significantly associated with antipsychotics use (OR = 4.4, 95% CI = 1.9–11, p < 0.001) after controlling for the effect of BD subtype (p = 0.8), and history of psychosis (OR = 2.2, 95% CI = 1.1–5.6, p = 0.03) (Figure 2B). The AUC of the model was 0.77 based on 191 cases. There was no other association between individual SUDs and individual medication classes in the French subsample.
Substance Use Disorder and Medicated vs. Unmedicated Cases
The Norwegian subsample comprised 274 (83%) medicated and 56 (17%) unmedicated cases after exclusion of first-treatment cases (n = 195). Being medicated vs. unmedicated had no significant association with any SUD (Table 3).
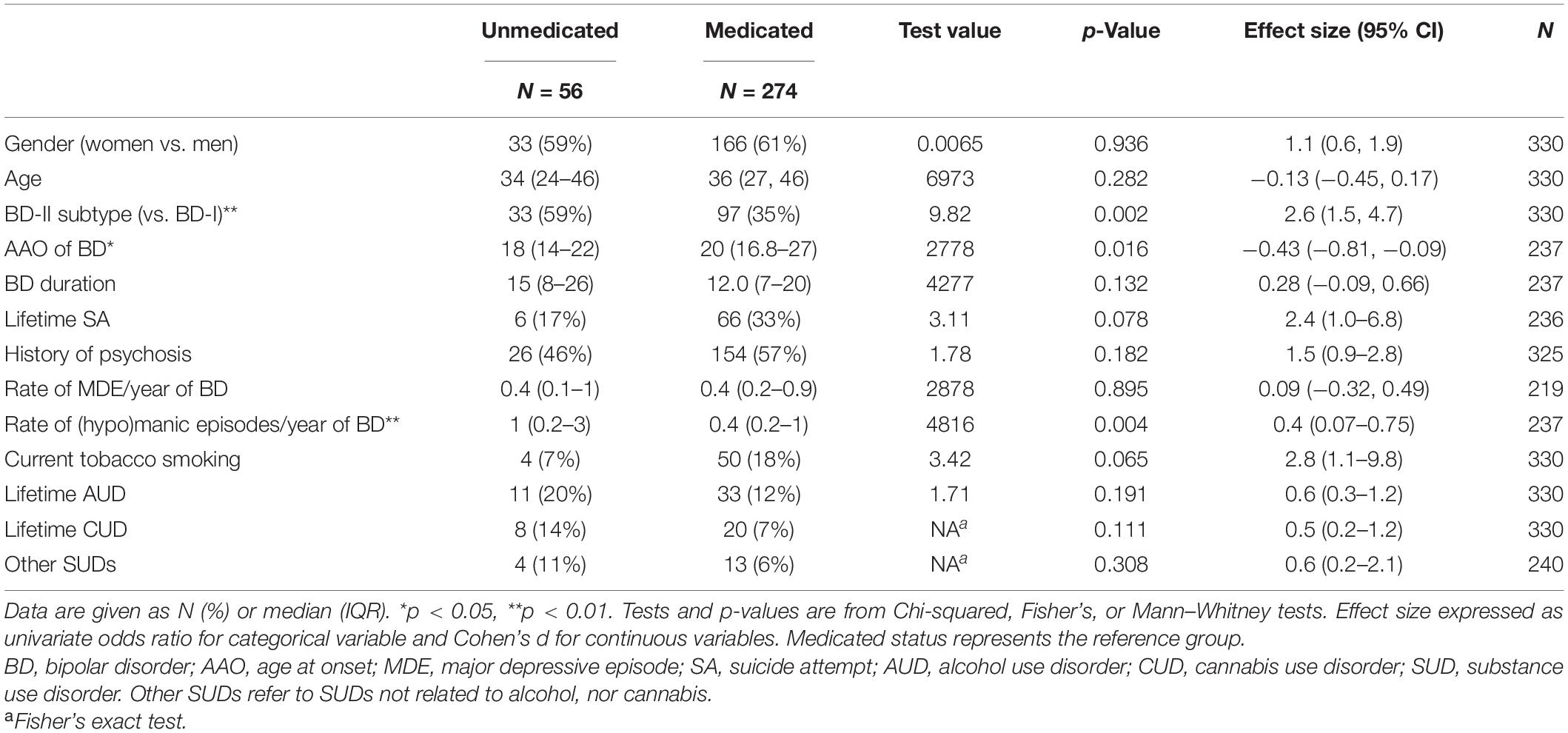
Table 3. Variables associated with the current medicated status in the Norwegian subsample, who was not in their first mood episode.
When including current smoking and both lifetime AUD and CUD in a binary regression analysis (Figure 3), we uncovered an independent association between being unmedicated and AUD (OR = 1.2, 95% CI = 1.04–1.3, p = 0.038). Being currently unmedicated was also independently associated with a higher number of (hypo)manic episodes (OR = 1, 95% CI = 1.02–1.07, p < 0.001) and a lower probability of lifetime suicide attempt (OR = 0.88, 95% CI = 0.79–0.97, p = 0.014). AUC of this model was 0.78, based on 195 cases. Of note, we entered AAO of BD and the absolute number of (hypo)manic episodes together instead of the rate of (hypo)manic episodes in order to avoid multicollinearity and to be able to dissect the effects from both AAO and the number of episodes.
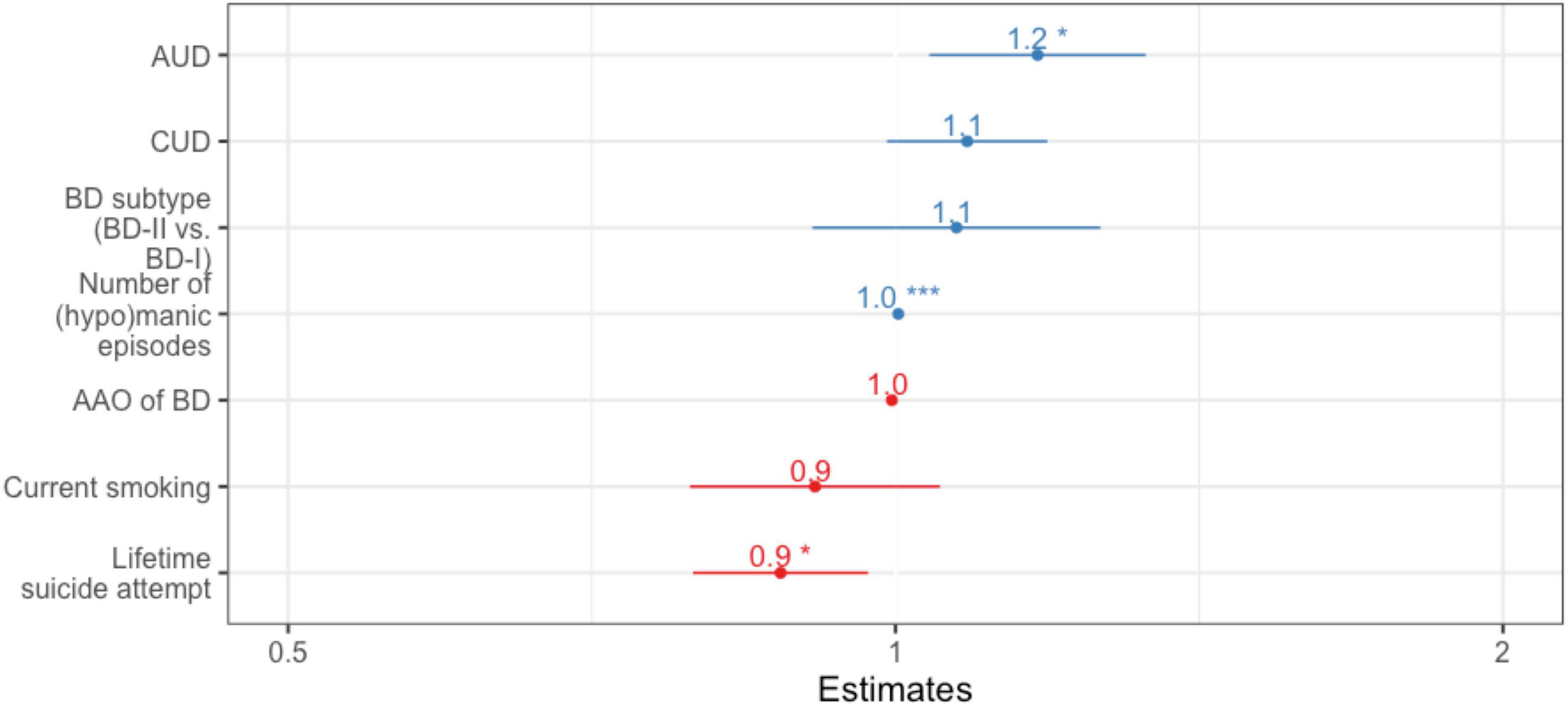
Figure 3. Forest plot for binary logistic regression in Norway, with “being unmedicated vs. medicated” as the dependent variable. N = 195 after exclusion of first-episode cases. Bar length indicates 95% confidence interval. AAO, age at onset; BD, bipolar disorder; AUD, alcohol use disorder; CUD, cannabis use disorder. *p < 0.05, **p < 0.01, ***p < 0.001.
Finally, there was no indication that BD cases with comorbid SUD had higher resistance (lowest p-values = 0.499 for the BMQ-general and 0.374 for the BMQ-specific) or lower adherence (p-value = 0.39 for MARS) regarding their medication, as compared to BD cases without any SUD. Interestingly though, the BMQ necessity subscore was higher in the BD+AUD than in the BD alone group, p = 0.037.
Discussion
In this study of a large sample of patients from France and Norway, who were extensively characterized for both BD and SUD history, we found no significant association between the compliance to pharmacological treatment guidelines and comorbid SUDs. Thus, our results suggest that it is feasible to follow existing guidelines to treat BD, also for patients with comorbid SUD. In line with this, no SUD was associated with individual medication classes in the sample as a whole. However, country-specific analyses identified independent associations between current tobacco smoking and anti-epileptics use and between AUD and being unmedicated in the Norwegian subsample; as well as between CUD and antipsychotics use in France. To the best of our knowledge, this study reports among the most detailed characterization of the links between comorbid SUD and preventive medication in BD, with a focus on both medication patterns and level of medication compliance to guidelines. Our main finding, which is negative, was ascertained with the computation of Bayes factors, meaning that we had adequate statistical power and that this finding can be considered as reliable. Importantly as regards generalizability, the medication regimens of our samples were similar to previous studies. For instance, in 7,406 individuals with BD-I, II and NOS diagnoses from the United States community (52), 18% would have been categorized as having non-compliant preventive treatment, 51% received polypharmacy, 24% benzodiazepines, and 71% antidepressants (the only category that seemed to differ from our sample). As for the prevalence of SUD, our sample remains within the range of tertiary care samples for BD (53, 54), which often show relatively low rates of SUDs compared to other clinical samples (5).
Available literature examining the possibility that comorbid SUD would be associated with non-evidence based treatment in BD reported either less specific or borderline findings, as compared to ours. One study found that BD-SUD inpatients showed less use of mood-stabilizers at discharge, as compared to BD only patients (31). The second study reported the absence of association between SUD and a reduced adherence to BD medication guidelines, but with p = 0.06 (55). This may be due to the smaller size of these samples. In a larger registry study (52), BD subjects with AUD or other SUDs showed a decrease in mood-stabilizers use during follow-up, as measured by medication possession ratio. Although this was primarily interpreted as lower adherence to treatment, the authors acknowledged that their measurement captured all kinds of treatment interruption. Thus, this finding was in line with that of Norwegian cases having less likelihood of proper preventive treatment for BD in case of comorbid AUD. Interesting as well in this study was that bipolar illness complexity was also associated with reduced mood-stabilizer use. More precisely, we replicated an association between reduced compliance to guidelines and BD-II vs. BD-I subtype (55), and evidenced an independent association between female gender and lack of compliance to guidelines, which had not been specifically reported previously (55). This finding was not due to common characteristics of BD associated with female gender (56, 57), most of which were controlled for in our study. However, this could have been due to other factors associated with antidepressant prescription, which was significantly higher in women vs. men (Supplementary Table 2) and likely drove the association between gender and compliance to guidelines in our study. This includes anxiety/anxiety disorders (58) and fear of weight gain (59). We suggest that the fear of weight gain could be much higher for mood-stabilizers and antipyschotics than for antidepressants, thereby increasing the likelihood for prescribing antidepressants as opposed to mood-stabilizers in women. In line with this, we found previous associations between female gender and complex polypharmacy in BD (60). Overall, these data highlight the need for further research regarding gender issues in patients’ and prescribers’ adherence to guidelines.
We investigated the correlates of being unmedicated in the Norwegian subsample. The regression analysis showed that comorbid AUD was associated with current lack of pharmacological treatment. AUD may increase the likelihood of delayed diagnosis/underdiagnosis of BD in these patients, especially if AUD preceded BD (61). Conversely, cocaine use disorders have been associated with a risk of overdiagnosing and/or precipitating BD (62, 63). Compared to BD without AUD, comorbid AUD in BD is rather associated with depressive symptoms in BD, including a positive correlation between depressive symptoms and alcohol craving (64), and – possibly – a more frequent depressive predominant polarity (65, 66). This may hamper identification of the BD and thus delay treatment. However, studies reporting associations between AUD and bipolar depression have often yielded discrepant results (67, 68), noting that merely all SUDs may predict longer time to recovery from bipolar depression (10, 67). In line with underdiagnosis, our results also raise the possibility that clinicians are less inclined to initiate mood-stabilizers in cases with continuous alcohol use, even in the presence of mood episodes. Thus, until the years 2010s, it was usually recommended to start such treatment after alcohol detoxification or – at least – after a large reduction in alcohol use (61). In line with this general hypothesis of difficult diagnosis/treatment choice in BD with vs. without AUD, we found no evidence of decreased adherence or increased concern/necessity ratio across AUD groups. This suggests that non-prescription may have prevailed over non-adherence regarding the unmedicated status associated with AUD in our sample. One of the key issues might be the consideration of current vs. past AUD (10) and of moderate vs. heavy alcohol drinking (69), the latter being more strongly associated with incident bipolar depression than the former (70).
In the Norwegian subsample, we also found an independent association between current smoking vs. past- and never-smoking and increased anti-epileptics use. We can hardly think of the rationale for this association. Anti-epileptics were also more commonly prescribed to BD-II cases, but this did not alter the association with current tobacco smoking. Other possible reasons due to gender differences (valproate being avoided in women of childbearing age) or to the clinical expression of BD were ruled out, yet, there may be some bias due to the fact that “non-current smokers” were a mixed group of never + former smokers. We did not retrieve previous evidence of such association in the literature, so that a pilot, prospective study on this specific issue with detailed data regarding the reasons for prescribing/choosing to take anti-epileptics seems warranted.
Cannabis use disorder has overall been associated with a heavy burden in BD (71, 72). In the French subsample, it was associated with increased use of antipsychotics, suggesting that clinicians may have needed to maintain these medications to manage persistent mood instability and/or psychotic symptoms.
Limitations
The study was cross-sectional and medication data were collected by self-report, thus sensitive to recall bias and making us less able to disentangle non-prescription from patients’ non-adherence. We did not collect individual treatment names or dosages to assess fine-grained compliance to guidelines and polypharmacy. No correction was applied for multiple testing, however, we believe that using Bayes and regression analyses reduced the risk of both false positives and false negatives. We did not assess further comorbidity such as anxiety, personality and attention deficit/hyperactivity (ADHD) disorders, which have been associated with BD+SUD comorbidity (3) and could lead to altered medication regimens. We relied on lifetime SUD diagnoses, although the amount and recency of exposure to addictive substances may have played an additional role in prescription patterns, especially by encouraging clinicians to wait for abstinence before prescribing proper BD medication. Importantly, the associations evidenced here are likely bi-directional, without any possible conclusion about causal inference.
Conclusion
Overall, SUDs were not associated with lack of compliance toward guidelines for preventive BD treatment in a large, cross-national sample. However, individuals with comorbid AUD were significantly less likely to be medicated in the Norwegian sample. Specific guidelines are lacking for the subgroup of BD+SUD cases, and treating clinicians in our study seem to have remained compliant to general guidelines for BD despite the presence of comorbid SUD. In the absence of specific treatment, available evidence thus suggests that intensive and early mood-stabilizing therapy can be used for BD+SUD. With that regards, more specific psychosocial treatments showed promise for BD+SUD cases (73, 74). We believe our study also highlights the fact that, in general, it is necessary to examine SUD comorbidity by individualizing tobacco, alcohol, cannabis, and other substances of abuse given that each of these categories showed relevant associations that would not have been uncovered if we had regrouped them. Moreover, our findings contribute to a better knowledge for both patients and clinicians. In dually diagnosed BD patients, integrated care and improved diagnostic and therapeutic strategies are urgently required. Some of these strategies have already shown promising results (46, 73, 75–77) and should be implemented in both psychiatric and addiction care settings.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by the Comité de Protection des Personnes, Hôpital Pitié-Salpêtrière, and Regional Committee for Medical Research Ethics and Norwegian Data Inspectorate. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
RI, TL, and IM wrote the first draft of the manuscript. BE, MH, SG, SA, ML, OA, RB, CH, TB, J-PK, NS, and FB designed the initial study and recruited the sample. All authors have contributed to and critically reviewed the manuscript.
Funding
Supported by grants from KG Jebsen Stifelsen (Grant No. SKGJ−MED−008), Research Council of Norway (Grant No. 223273), and South-East Health Authority (Grant No. 2012-132). This work was supported by INSERM (Research Protocol C0829), Assistance Publique des Hôpitaux de Paris (Research Protocol GAN12), and by the Investissements d’Avenir program managed by the ANR under reference ANR-11-IDEX-0004 and Fondation FondaMental (RTRS Santeì Mentale). This work was performed with further support by the Research Council of Norway through an “INTPART” grant. These organizations had no role in the design of the study, the collection, analysis and interpretation of data, the writing of the report, and in the decision to submit the manuscript for publication.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank all the support personnel at NORMENT.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2022.813256/full#supplementary-material
References
1. Charlson FJ, Baxter AJ, Dua T, Degenhardt L, Whiteford HA, Vos T. Excess mortality from mental, neurological, and substance use disorders in the global burden of disease study 2010. 3rd ed. In: Patel V, Chisholm D, Dua T, Laxminarayan R, Medina-Mora ME editors, Mental, Neurological, and Substance Use Disorders: Disease Control Priorities. (Vol. 4), Washington, DC: The International Bank for Reconstruction and Development (2016).
2. Crump C, Sundquist K, Winkleby MA, Sundquist J. Comorbidities and mortality in bipolar disorder: a Swedish national cohort study. JAMA Psychiatry. (2013) 70:931–9. doi: 10.1001/jamapsychiatry.2013.1394
3. Spoorthy MS, Chakrabarti S, Grover S. Comorbidity of bipolar and anxiety disorders: an overview of trends in research. World J Psychiatry. (2019) 9:7–29. doi: 10.5498/wjp.v9.i1.7
4. Thomson D, Berk M, Dodd S, Rapado-Castro M, Quirk SE, Ellegaard PK, et al. Tobacco use in bipolar disorder. Clin Psychopharmacol Neurosci. (2015) 13:1–11.
5. Hunt GE, Malhi GS, Cleary M, Lai HMX, Sitharthan T. Prevalence of comorbid bipolar and substance use disorders in clinical settings, 1990-2015: systematic review and meta-analysis. J Affect Disord. (2016) 206:331–49. doi: 10.1016/j.jad.2016.07.011
6. Hunt GE, Malhi GS, Cleary M, Lai HMX, Sitharthan T. Comorbidity of bipolar and substance use disorders in national surveys of general populations, 1990-2015: systematic review and meta-analysis. J Affect Disord. (2016) 206:321–30. doi: 10.1016/j.jad.2016.06.051
7. Hjorthøj C, Østergaard MLD, Benros ME, Toftdahl NG, Erlangsen A, Andersen JT, et al. Association between alcohol and substance use disorders and all-cause and cause-specific mortality in schizophrenia, bipolar disorder, and unipolar depression: a nationwide, prospective, register-based study. Lancet Psychiatry. (2015) 2:801–8. doi: 10.1016/S2215-0366(15)00207-2
8. Icick R, Melle I, Etain B, Ringen PA, Aminoff SR, Leboyer M, et al. Tobacco smoking and other substance use disorders associated with recurrent suicide attempts in bipolar disorder. J Affect Disord. (2019) 256:348–57. doi: 10.1016/j.jad.2019.05.075
9. Østergaard MLD, Nordentoft M, Hjorthøj C. Associations between substance use disorders and suicide or suicide attempts in people with mental illness: a Danish nation-wide, prospective, register-based study of patients diagnosed with schizophrenia, bipolar disorder, unipolar depression or personality disorder. Addiction. (2017) 112:1250–9. doi: 10.1111/add.13788
10. Gold AK, Peters AT, Otto MW, Sylvia LG, Magalhaes PV, Berk M, et al. The impact of substance use disorders on recovery from bipolar depression: results from the systematic treatment enhancement program for bipolar disorder psychosocial treatment trial. Aust N Z J Psychiatry. (2018) 52:847–55. doi: 10.1177/0004867418788172
11. Clerici M, de Bartolomeis A, De Filippis S, Ducci G, Maremmani I, Martinotti G, et al. Patterns of management of patients with dual disorder (psychosis) in Italy: a survey of psychiatrists and other physicians focusing on clinical practice. Front Psychiatry. (2018) 9:575.
12. Ducasse D, Jaussent I, Guillaume S, Azorin JM, Bellivier F, Belzeaux R, et al. Increased risk of suicide attempt in bipolar patients with severe tobacco dependence. J Affect Disord. (2015) 183:113–8. doi: 10.3389/fpsyt.2018.00575
13. Berk M, Ng F, Wang WV, Tohen M, Lubman DI, Vieta E, et al. Going up in smoke: tobacco smoking is associated with worse treatment outcomes in mania. J Affect Disord. (2008) 110:126–34. doi: 10.1016/j.jad.2008.01.018
14. Fornaro M, Ventriglio A, De Pasquale C, Pistorio ML, De Berardis D, Cattaneo CI, et al. Sensation seeking in major depressive patients: relationship to sub-threshold bipolarity and cyclothymic temperament. J Affect Disord. (2013) 148:375–83. doi: 10.1016/j.jad.2013.01.002
15. Vellante F, Ferri F, Baroni G, Croce P, Migliorati D, Pettoruso M, et al. Euthymic bipolar disorder patients and EEG microstates: a neural signature of their abnormal self experience? J Affect Disord. (2020) 272:326–34. doi: 10.1016/j.jad.2020.03.175
16. Fornaro M, Orsolini L, Marini S, De Berardis D, Perna G, Valchera A, et al. The prevalence and predictors of bipolar and borderline personality disorders comorbidity: systematic review and meta-analysis. J Affect Disord. (2016) 195:105–18. doi: 10.1016/j.jad.2016.01.040
17. Coles AS, Sasiadek J, George TP. Pharmacotherapies for co-occurring substance use and bipolar disorders: a systematic review. Bipolar Disord. (2019) 21:595–610. doi: 10.1111/bdi.12794
18. Tundo A, De Crescenzo F, Gori D, Cavalieri P. Long-term treatment response to continuous cycling course in bipolar disorders: a meta-analysis. J Affect Disord. (2018) 241:367–70. doi: 10.1016/j.jad.2018.08.067
19. García S, Martínez-Cengotitabengoa M, López-Zurbano S, Zorrilla I, López P, Vieta E, et al. Adherence to antipsychotic medication in bipolar disorder and schizophrenic patients: a systematic review. J Clin Psychopharmacol. (2016) 36:355–71. doi: 10.1097/JCP.0000000000000523
20. Karanti A, Kardell M, Lundberg U, Landén M. Changes in mood stabilizer prescription patterns in bipolar disorder. J Affect Disord. (2016) 195:50–6. doi: 10.1016/j.jad.2016.01.043
21. Puspitasari IM, Sinuraya RK, Rahayu C, Witriani W, Zannah U, Hafifah A, et al. Medication profile and treatment cost estimation among outpatients with schizophrenia, bipolar disorder, depression, and anxiety disorders in Indonesia. Neuropsychiatr Dis Treat. (2020) 16:815–28. doi: 10.2147/NDT.S240058
22. Köhler-Forsberg O, Sylvia LG, Fung V, Overhage L, Thase M, Calabrese JR, et al. Adjunctive antidepressant treatment among 763 outpatients with bipolar disorder: findings from the Bipolar CHOICE and LiTMUS trials. Depress Anxiety. (2020). Available online at: http://onlinelibrary.wiley.com/doi/abs/10.1002/da.23069 (accessed August 20, 2020). doi: 10.1002/da.23069
23. Bobo WV, Reilly-Harrington NA, Ketter TA, Brody BD, Kinrys G, Kemp DE, et al. Complexity of illness and adjunctive benzodiazepine use in outpatients with bipolar I or II disorder: results from the bipolar CHOICE study. J Clin Psychopharmacol. (2015) 35:68–74. doi: 10.1097/JCP.0000000000000257
24. Guina J, Merrill B. Benzodiazepines I: upping the care on downers: the evidence of risks, benefits and alternatives. J Clin Med. (2018) 7:17. doi: 10.3390/jcm7020017
25. Gibbs M, Winsper C, Marwaha S, Gilbert E, Broome M, Singh SP. Cannabis use and mania symptoms: a systematic review and meta-analysis. J Affect Disord. (2015) 171:39–47. doi: 10.1016/j.jad.2014.09.016
26. Simmler LD, Liechti ME. Pharmacology of MDMA- and amphetamine-like new psychoactive substances. Handb Exp Pharmacol. (2018) 252:143–64. doi: 10.1007/164_2018_113
27. Gaudiano BA, Weinstock LM, Miller IW. Improving treatment adherence in patients with bipolar disorder and substance abuse: rationale and initial development of a novel psychosocial approach. J Psychiatr Pract. (2011) 17:5–20. doi: 10.1097/01.pra.0000393840.18099.d6
28. Belzeaux R, Correard N, Boyer L, Etain B, Loftus J, Bellivier F, et al. Depressive residual symptoms are associated with lower adherence to medication in bipolar patients without substance use disorder: results from the FACE-BD cohort. J Affect Disord. (2013) 151:1009–15. doi: 10.1016/j.jad.2013.08.028
29. Chakrabarti S. Treatment attitudes and adherence among patients with bipolar disorder: a systematic review of quantitative and qualitative studies. Harv Rev Psychiatry. (2019) 27:290–302. doi: 10.1097/HRP.0000000000000228
30. Samalin L, Guillaume S, Auclair C, Llorca P-M. Adherence to guidelines by French psychiatrists in their real world of clinical practice. J Nerv Ment Dis. (2011) 199:239–43. doi: 10.1097/NMD.0b013e3182125d4c
31. Barral D, Barral F, Cruz N, Molina JD, Sánchez V, Rosique T. Comparison of psychodrug prescription patterns in patients diagnosed with bipolar disorder and addiction. Actas Esp Psiquiatr. (2016) 44:222–30.
32. Fond G, Tinland A, Boucekine M, Girard V, Loubière S, Auquier P, et al. Prescription of potentially inappropriate psychotropic drugs in homeless people with schizophrenia and bipolar disorders. Results from the French housing first (FHF) program. Prog Neuropsychopharmacol Biol Psychiatry. (2019) 89:84–9. doi: 10.1016/j.pnpbp.2018.08.024
33. Brodeur S, Terrisse H, Pouchon A, Godin O, Aouizerate B, Aubin V, et al. Pharmacological treatment profiles in the FACE-BD cohort: an unsupervised machine learning study, applied to a nationwide bipolar cohort✰. J Affect Disord. (2021) 286:309–19. doi: 10.1016/j.jad.2021.02.036
34. Bauer M, Glenn T, Alda M, Sagduyu K, Marsh W, Grof P, et al. Drug treatment patterns in bipolar disorder: analysis of long-term self-reported data. Int J Bipolar Disord. (2013) 1:5. doi: 10.1186/2194-7511-1-5
35. American Psychiatric Association.The Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition-Text Revised (DSM IV-TR). Washington, DC: American Psychiatric Association (2000).
36. Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. (1979) 134:382–9. doi: 10.1192/bjp.134.4.382
37. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
38. Preisig M, Fenton BT, Matthey ML, Berney A, Ferrero F. Diagnostic interview for genetic studies (DIGS): inter-rater and test-retest reliability of the French version. Eur Arch Psychiatry Clin Neurosci. (1999) 249:174–9. doi: 10.1007/s004060050084
39. First MB, Spitzer MR. SCID – Structured Clinical Interview for DSM-IV Axis I Disorders, Patient Edition (SCID-P), version 2 [Internet]. New York, NY: New York State Psychiatric Institute (1995).
40. Hughes JR, Shiffman S, Naud S, Peters EN. Day to day variability in self-reported cigarettes per day. Nicotine Tob Res. (2017) 19:1107–11. doi: 10.1093/ntr/ntx057
41. National Institute for Clinical Excellence.Overview | Bipolar Disorder: Assessment and Management | Guidance | NICE [Internet]. (2020). Available online at: https://www.nice.org.uk/guidance/cg185 (accessed August 20, 2020).
42. Yatham LN, Kennedy SH, Parikh SV, Schaffer A, Bond DJ, Frey BN, et al. Canadian network for mood and anxiety treatments (CANMAT) and international society for bipolar disorders (ISBD) 2018 guidelines for the management of patients with bipolar disorder. Bipolar Disord. (2018) 20:97–170. doi: 10.1111/bdi.12609
43. Loftus J, Scott J, Vorspan F, Icick R, Henry C, Gard S, et al. Psychiatric comorbidities in bipolar disorders: an examination of the prevalence and chronology of onset according to sex and bipolar subtype. J Affect Disord. (2020) 267:258–63. doi: 10.1016/j.jad.2020.02.035
44. Dell’Osso B, Arici C, Cafaro R, Vismara M, Cremaschi L, Benatti B, et al. Antidepressants in bipolar disorder: analysis of correlates overall, and in BD-I and BD-II subsamples. J Affect Disord. (2021) 292:352–8. doi: 10.1016/j.jad.2021.05.043
45. Cheniaux E, Nardi AE. Evaluating the efficacy and safety of antidepressants in patients with bipolar disorder. Expert Opin Drug Saf. (2019) 18:893–913. doi: 10.1080/14740338.2019.1651291
46. Salloum IM, Brown ES. Management of comorbid bipolar disorder and substance use disorders. Am J Drug Alcohol Abuse. (2017) 43:366–76. doi: 10.1080/00952990.2017.1292279
47. Vorspan F, Mehtelli W, Dupuy G, Bloch V, Lépine J-P. Anxiety and substance use disorders: co-occurrence and clinical issues. Curr Psychiatry Rep. (2015) 17:4. doi: 10.1007/s11920-014-0544-y
48. Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new medication adherence rating scale (MARS) for the psychoses. Schizophr Res. (2000) 42:241–7. doi: 10.1016/s0920-9964(99)00130-9
49. Thorneloe RJ, Griffiths CEM, Ashcroft DM, Cordingley L. The challenges of assessing patients’ medication beliefs: a qualitative study. BMC Health Servic Res. (2017) 17:119. doi: 10.1186/s12913-017-2020-y
50. Schönbrodt FD, Wagenmakers E-J. Bayes factor design analysis: planning for compelling evidence. Psychon Bull Rev. (2018) 25:128–42. doi: 10.3758/s13423-017-1230-y
51. R Core Team.R: A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing (2020).
52. Baldessarini RJ, Leahy L, Arcona S, Gause D, Zhang W, Hennen J. Patterns of psychotropic drug prescription for U.S. patients with diagnoses of bipolar disorders. Psychiatr Serv. (2007) 58:85–91. doi: 10.1176/ps.2007.58.1.85
53. Henry C, Etain B, Godin O, Dargel AA, Azorin J-M, Gard S, et al. Bipolar patients referred to specialized services of care: not resistant but impaired by sub-syndromal symptoms. Results from the FACE-BD cohort. Aust N Z J Psychiatry. (2015) 49:898–905. doi: 10.1177/0004867415585582
54. Kim S-W, Dodd S, Berk L, Kulkarni J, de Castella A, Fitzgerald PB, et al. Impact of cannabis use on long-term remission in bipolar I and schizoaffective disorder. Psychiatry Investig. (2015) 12:349–55. doi: 10.4306/pi.2015.12.3.349
55. Paterniti S, Bisserbe J-C. Pharmacotherapy for bipolar disorder and concordance with treatment guidelines: survey of a general population sample referred to a tertiary care service. BMC Psychiatry. (2013) 13:211. doi: 10.1186/1471-244X-13-211
56. Levine J, Chengappa KR, Brar JS, Gershon S, Yablonsky E, Stapf D, et al. Psychotropic drug prescription patterns among patients with bipolar I disorder. Bipolar Disord. (2000) 2:120–30. doi: 10.1034/j.1399-5618.2000.020205.x
57. Buoli M, Cesana BM, Dell’Osso B, Fagiolini A, de Bartolomeis A, Bondi E, et al. Gender-related differences in patients with bipolar disorder: a nationwide study. CNS Spectr. (2019) 24:589–96. doi: 10.1017/S1092852918001529
58. Cunningham R, Crowe M, Stanley J, Haitana T, Pitama S, Porter R, et al. Gender and mental health service use in bipolar disorder: national cohort study. BJPsych Open. (2020) 6:e138. doi: 10.1192/bjo.2020.117
59. Kriegshauser K, Sajatovic M, Jenkins JH, Cassidy KA, Muzina D, Fattal O, et al. Gender differences in subjective experience and treatment of bipolar disorder. J Nerv Ment Dis. (2010) 198:370–2. doi: 10.1097/NMD.0b013e3181da8ef7
60. Kim AM, Salstein L, Goldberg JF. A systematic review of complex polypharmacy in bipolar disorder: prevalence, clinical features, adherence, and preliminary recommendations for practitioners. J Clin Psychiatry. (2021) 82:20r13263. doi: 10.4088/JCP.20r13263
61. Grunze H, Schaefer M, Scherk H, Born C, Preuss UW. Comorbid bipolar and alcohol use disorder—a therapeutic challenge. Front Psychiatry. (2021) 12:660432. doi: 10.3389/fpsyt.2021.660432
62. de Azevedo Cardoso T, Jansen K, Mondin TC, Pedrotti Moreira F, de Lima Bach S, da Silva RA, et al. Lifetime cocaine use is a potential predictor for conversion from major depressive disorder to bipolar disorder: a prospective study. Psychiatry Clin Neurosci. (2020) 74:418–23. doi: 10.1111/pcn.13012
63. Goldberg JF, Garno JL, Callahan AM, Kearns DL, Kerner B, Ackerman SH. Overdiagnosis of bipolar disorder among substance use disorder inpatients with mood instability. J Clin Psychiatry. (2008) 69:1751–7. doi: 10.4088/jcp.v69n1110
64. Prisciandaro JJ, DeSantis SM, Chiuzan C, Brown DG, Brady KT, Tolliver BK. Impact of depressive symptoms on future alcohol use in patients with co-occurring bipolar disorder and alcohol dependence: a prospective analysis in an 8-week randomized controlled trial of acamprosate. Alcohol Clin Exp Res. (2012) 36:490–6. doi: 10.1111/j.1530-0277.2011.01645.x
65. Janiri D, Di Nicola M, Martinotti G, Janiri L. Who’s the leader, mania or depression? Predominant polarity and alcohol/polysubstance use in bipolar disorders. Curr Neuropharmacol. (2017) 15:409–16. doi: 10.2174/1570159X14666160607101400
66. Popovic D, Torrent C, Goikolea JM, Cruz N, Sánchez-Moreno J, González-Pinto A, et al. Clinical implications of predominant polarity and the polarity index in bipolar disorder: a naturalistic study. Acta Psychiatr Scand. (2014) 129:366–74. doi: 10.1111/acps.12179
67. Ostacher MJ, Perlis RH, Nierenberg AA, Calabrese J, Stange JP, Salloum I, et al. Impact of substance use disorders on recovery from episodes of depression in bipolar disorder patients: prospective data from the systematic treatment enhancement program for bipolar disorder (STEP-BD). Am J Psychiatry. (2010) 167:289–97. doi: 10.1176/appi.ajp.2009.09020299
68. González-Pinto A, Alberich S, Barbeito S, Alonso M, Vieta E, Martínez-Arán A, et al. Different profile of substance abuse in relation to predominant polarity in bipolar disorder: the Vitoria long-term follow-up study. J Affect Disord. (2010) 124:250–5. doi: 10.1016/j.jad.2009.11.005
69. Pary R, Patel M, Lippmann S. Depression and bipolar disorders in patients with alcohol use disorders. Fed Pract. (2017) 34(Suppl. 2):37S–41S.
70. Jaffee WB, Griffin ML, Gallop R, Meade CS, Graff F, Bender RE, et al. Depression precipitated by alcohol use in patients with co-occurring bipolar and substance use disorders. J Clin Psychiatry. (2009) 70:171–6. doi: 10.4088/jcp.08m04011
71. Lagerberg TV, Icick R, Andreassen OA, Ringen PA, Etain B, Aas M, et al. Cannabis use disorder is associated with greater illness severity in tobacco smoking patients with bipolar disorder. J Affect Disord. (2016) 190:286–93. doi: 10.1016/j.jad.2015.10.023
72. Lev-Ran S, Le Foll B, McKenzie K, George TP, Rehm J. Bipolar disorder and co-occurring cannabis use disorders: characteristics, co-morbidities and clinical correlates. Psychiatry Res. (2013) 209:459–65. doi: 10.1016/j.psychres.2012.12.014
73. Biseul I, Icick R, Seguin P, Bellivier F, Scott J. Feasibility and acceptability of the “HABIT” group programme for comorbid bipolar and alcohol and substance use disorders. Clin Psychol Psychother. (2017) 24:887–98. doi: 10.1002/cpp.2053
74. Gold AK, Otto MW, Deckersbach T, Sylvia LG, Nierenberg AA, Kinrys G. Substance use comorbidity in bipolar disorder: a qualitative review of treatment strategies and outcomes. Am J Addict. (2018) 27:188–201. doi: 10.1111/ajad.12713
75. Jones SH, Riste L, Robinson H, Holland F, Peters S, Hartwell R, et al. Feasibility and acceptability of integrated psychological therapy versus treatment as usual for people with bipolar disorder and co-morbid alcohol use: a single blind randomised controlled trial. J Affect Disord. (2019) 256:86–95. doi: 10.1016/j.jad.2019.05.038
76. Mestre-Pintó JI, Domingo-Salvany A, Martín-Santos R, Torrens M, PsyCoBarcelona Group. Dual diagnosis screening interview to identify psychiatric comorbidity in substance users: development and validation of a brief instrument. Eur Addict Res. (2014) 20:41–8. doi: 10.1159/000351519
Keywords: bipolar disorder, substance use disorder, treatment guidelines, tobacco smoking, comorbidity
Citation: Icick R, Melle I, Etain B, Høegh MC, Gard S, Aminoff SR, Leboyer M, Andreassen OA, Belzeaux R, Henry C, Bjella TD, Kahn J-P, Steen NE, Bellivier F and Lagerberg TV (2022) Preventive Medication Patterns in Bipolar Disorder and Their Relationship With Comorbid Substance Use Disorders in a Cross-National Observational Study. Front. Psychiatry 13:813256. doi: 10.3389/fpsyt.2022.813256
Received: 11 November 2021; Accepted: 11 April 2022;
Published: 03 May 2022.
Edited by:
Heinz Grunze, Paracelsus Medical Private University, Nuremberg, GermanyReviewed by:
Claudia Pisanu, University of Cagliari, ItalyDomenico De Berardis, Mental Health Center (CSM) and Psychiatric Service of Diagnosis and Treatment (SPDC), Italy
Copyright © 2022 Icick, Melle, Etain, Høegh, Gard, Aminoff, Leboyer, Andreassen, Belzeaux, Henry, Bjella, Kahn, Steen, Bellivier and Lagerberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Romain Icick, cm9tYWluLmljaWNrQGFwaHAuZnI=