 Florence Askenazy1,2
Florence Askenazy1,2 Arnaud Fernandez1,2
Arnaud Fernandez1,2 Levent Altan3
Levent Altan3 Michèle Battista2Michel Dückers4,5,6
Michèle Battista2Michel Dückers4,5,6 Morgane Gindt1,2
Morgane Gindt1,2 Ophélie Nachon1,2Aleksandra Ivankovic3Ingeborg Porcar-Becker7Nathalie Prieto8
Ophélie Nachon1,2Aleksandra Ivankovic3Ingeborg Porcar-Becker7Nathalie Prieto8 Philippe Robert1,9
Philippe Robert1,9 Lise Eilin Stene10
Lise Eilin Stene10 Susanne Thummler1,2
Susanne Thummler1,2 Valeria Manera1,9*
Valeria Manera1,9*- 1Cognition Behaviour Technology (CoBTeK) Lab, Université Côte d’Azur, Nice, France
- 2University Department of Child and Adolescent Psychiatry, Children’s Hospitals of Nice CHU-Lenval, Nice, France
- 3Victim Support Europe, Brussels, Belgium
- 4ARQ Centre of Expertise for the Impact of Disasters and Crises, Diemen, Netherlands
- 5Nivel-Netherlands Institute for Health Services Research, Utrecht, Netherlands
- 6Faculty of Behavioural and Social Sciences, University of Groningen, Groningen, Netherlands
- 7Unit for Trauma, Crisis and Conflicts at the Autonomous University of Barcelona (UAB), Cerdanyola del Vallès, Spain
- 8Cellule d’Urgence Médico-Psychologique, Centre Régional du Psychotraumatisme, Hôpital Edouard Herriot, Lyon, France
- 9Association Innovation Alzheimer, Nice, France
- 10Norwegian Centre for Violence and Traumatic Stress Studies (NKVTS), Oslo, Norway
The acute response after a terror attack may have a crucial impact on the physical and psychological wellbeing of the victims. Preparedness of the professionals involved in the acute response is a key element to ensure effective interventions, and can be improved through trainings. Today in Europe there is a recognized lack of inter-professional and international trainings, which are important, among others, to respond to the needs and the rights of victims affected by a terrorist attack in another country than their home country. In this paper we report the perspectives of an expert panel composed by different categories of professionals on the possible role of interprofessional trainings provided remotely. The experts discussed the pertinence of remote trainings for professionals involved in the acute response of a terror attack, and highlighted their Strengths, Weaknesses, Opportunities and Threats (SWOT analysis). We concluded that, while remote trainings cannot replace in-person trainings, they may be useful to share knowledge about the role and the organization of the different categories of professionals, thus potentially improving response coordination, and to easily share good practices across professionals and countries.
Introduction
The acute response after a terror attack may have a crucial impact on the physical and psychological wellbeing of the direct victims (1–7). The acute phase management plays a key role also on the other impacted persons (family members or friends of the direct victims, members of their community, witnesses, members of the community where the attack took place, as well as a first responder and/or professional involved in the acute phase or in the follow-up (8–11). The acute phase can be defined as the phase during and immediately after the terror attack, and includes the initial steps of the rescue, identification, registration of all impacted persons, reunification, and immediate medical and psychological care (12–15). The duration of this phase depends on several factors (such as the type of event, the number of impacted persons, the rapidity of the response) and may vary from 1 week up to 1 month based on some definitions (16, 17). Several professionals are involved in the acute response phase, including first responders, such as law enforcement officers, paramedics, emergency medical technicians, firefighters, police, no-profit organization volunteers; and different categories of clinicians, such as medical doctors, psychologists, psychotherapists, and nurses (12, 18, 19). All these different professionals need to accomplish their respective tasks under uncertain, often chaotic conditions, and need to coordinate with other professionals, meaning that, at minimum, they should know their respective roles (National Collaborating Centre for Mental Health (11, 19–21)). Furthermore, persons impacted from terror attacks can be foreign tourists or visitors, meaning that they do not necessarily speak the country language and/or have the same social support, health coverage, or juridical and compensation systems. In this context, the European Commission financed the creation of a EU Centre of Expertise for Victims of Terrorism (EUCVT), which aims to bring together different categories of international experts of terrorism and provide European guidelines and trainings to increase knowledge on the victim needs and rights.
Preparedness of the professionals to face mass trauma is a key element, as recognized by professionals themselves (22, 23). Professional training is recognized as the best way to help them to prepare for the emergency response, including the implementation of frequent and realistic planning and training drills (24). Furthermore, several guidelines for psychosocial support stress the importance of training to contribute to preparedness (see (25) for a recent review). However, there is a recognized lack of inter-professional trainings, as well as a lack of international trainings. This is especially important because there is a variability in the level of preparedness in dealing with terrorism across countries (6, 15, 26, 27). Analyses of disaster preparedness definitions typically point at a lack of consensus (28, 29). Definitions depend on the purpose of a study. In our case, we focus specifically on disaster preparedness during the response phase of a threatening situation. We interpret preparedness as a state of professional readiness in the response, reflected in the ability to localize affected people, awareness of their potential and actual immediate support needs and risks, knowledge on how to provide basic support, on the availability of services and how to access them, through traditional and innovative methods, in the context of the support system.
The advances of new Information and Communication Technologies (ICT) allows today to organize trainings remotely, which can be more time and cost effective. Remote professional trainings are more and more widely used also outside universities and classical teaching facilities, especially after the COVID-19 sanitary crisis, and are usually well-accepted (30, 31). They can contribute, among others, to continuing education. Some disadvantages can also be highlighted compared to in-person trainings, including the difficulty to perform role-playing exercises, the reduced interpersonal contact, and lower engagement.
Most of the published evidence collected on training efficacy in the domain of response preparedness focuses on face-to-face trainings (e.g., (32–34)). However, online trainings do also exist, for instance for the continuing education of the law enforcement officers (35, 36). Accelerated by the COVID-19 crisis, online trainings are becoming more common also in the domain of disaster preparedness (e.g., (37)). As online trainings are gaining popularity only recently in this domain, analyses of their advantages and disadvantages are needed. In the present paper, we describe the perspectives discussed by a panel of experts in the context of the EUCVT project concerning the topics that should be taught during inter-professional and international trainings, and the role of remote trainings for the professionals involved in the acute response phase of a terror attack.
Methods
The discussion panel was initiated by the Lenval Foundation and the CoBTeK lab of the Université Cote d’Azur. Based on the collaborative network established in previous projects in the domain of psychotrauma due to terror attacks (such as the EUCVT project), we initially contacted a list of twenty-one internationally recognized experts (hereafter called “core experts”) in the field of psychosocial support in the acute response phase from different countries. These included (more than one response was possible) researchers (N = 14), clinicians (e.g., psychiatrists, psychologists, N = 17) and members of victim support organizations and/or organizations working on psychotrauma/acute response coordination (N = 12). These experts worked in Belgium (N = 2), France (N = 11), Israel (N = 1), Netherlands (N = 2), Norway (N = 1), Spain (N = 1), the United Kingdom (N = 2) and United States (N = 1). They had at least 15 years of professional experience in works related to psychotrauma and traumatic stress (range: 15 years to more than 30 years). All of them had direct experience with the acute response after terrorist attacks.
These core experts helped to define the initial topics and questions, to decide the questions for the web-survey, and/or provided short presentations concerning the organization of the first response protocols in different countries, and/or moderated group sessions during a final plenary meeting. The 11 experts that initiated the expert panel (and were thus more directly involved in the survey creation), were not asked to respond to the questions. To obtain responses from a wider and diverse range of experts at the international level, the core experts shared the survey some professional networks, including the online Hub of Expertise launched by the EU Centre of Expertise for Victims of Terrorism (EUCVT). The extended group of experts (including 10 of the initial core experts that were not directly involved in the survey design, and 26 experts reached through EUCVT hub, for a total of 36 responders) were asked to answer questions via a web-survey (between April and June 2021) using Google Forms. After collecting the results, a facilitator (VM) provided a summary of the experts’ responses, and encouraged the experts to analyze, comment and (eventually) revise their earlier responses considering the commentaries of other members of the panel.
The survey included a section with information on the professional profile and experience of the responders (as detailed in the Participants section), followed by rating questions focused on the design of international and interprofessional trainings (see Table 1). Rating questions employed a 7-point Likert scale (1 = Strongly disagree; 2 = Moderately disagree; 3 = Slightly Disagree; 4 = Neutral; 5 = Slightly agree; 6 = Moderately agree; 7 = Strongly agree). Mean and standard deviation were employed for the data analysis. The listed topics were derived from those described in European disaster mental health guidelines and evaluation studies, including registration of information on affected people, screening/detection of individuals in need for support or at risk, use of basic psychosocial support tools, availability of services, referral to appropriate support providers, how to deal with particular vulnerable or risk groups (e.g., children, people with disabilities), characteristics of the support system for people affected and mental health risks for professionals themselves (11, 12, 21, 38, 39). Topics like these can be considered logical candidates to include in trainings for professionals. Moreover, since new interventions and healthcare technologies are being developed and tested, including ICT, such as online platforms and Virtual Reality, it makes sense to include a rating question on their relevance for an emergency response training for professionals. After each rating question, participants could provide open comments. Finally, the survey included open questions, in which the experts were asked to provide a list of the top 3 advantages and disadvantages of using ICT in the acute response phase and of using ICT for the training of the professionals involved in the acute response phase. These were used to make a SWOT analysis (Strengths, Weaknesses, Opportunities and Threats) of the use remote trainings for professionals involved in the acute response phase of a terror attack, as reported in Table 2. The web-survey results and the open discussion points were revised by the core experts (N = 21) and the extended list of experts (N = 26) during a hybrid plenary meeting held on July 16th, 2021, in Nice (France). 11 out of the 47 experts were physically present in Nice, while the others were connected remotely.
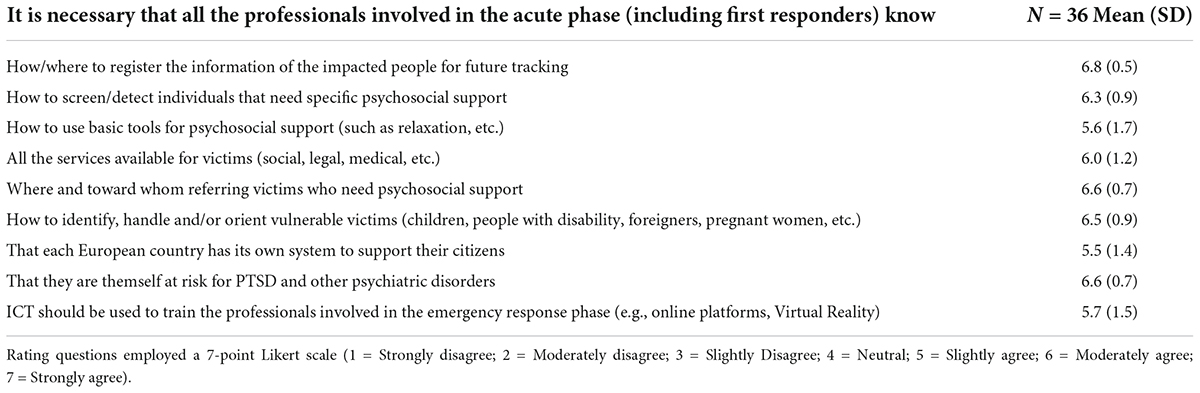
Table 1. Results of the rating questions.
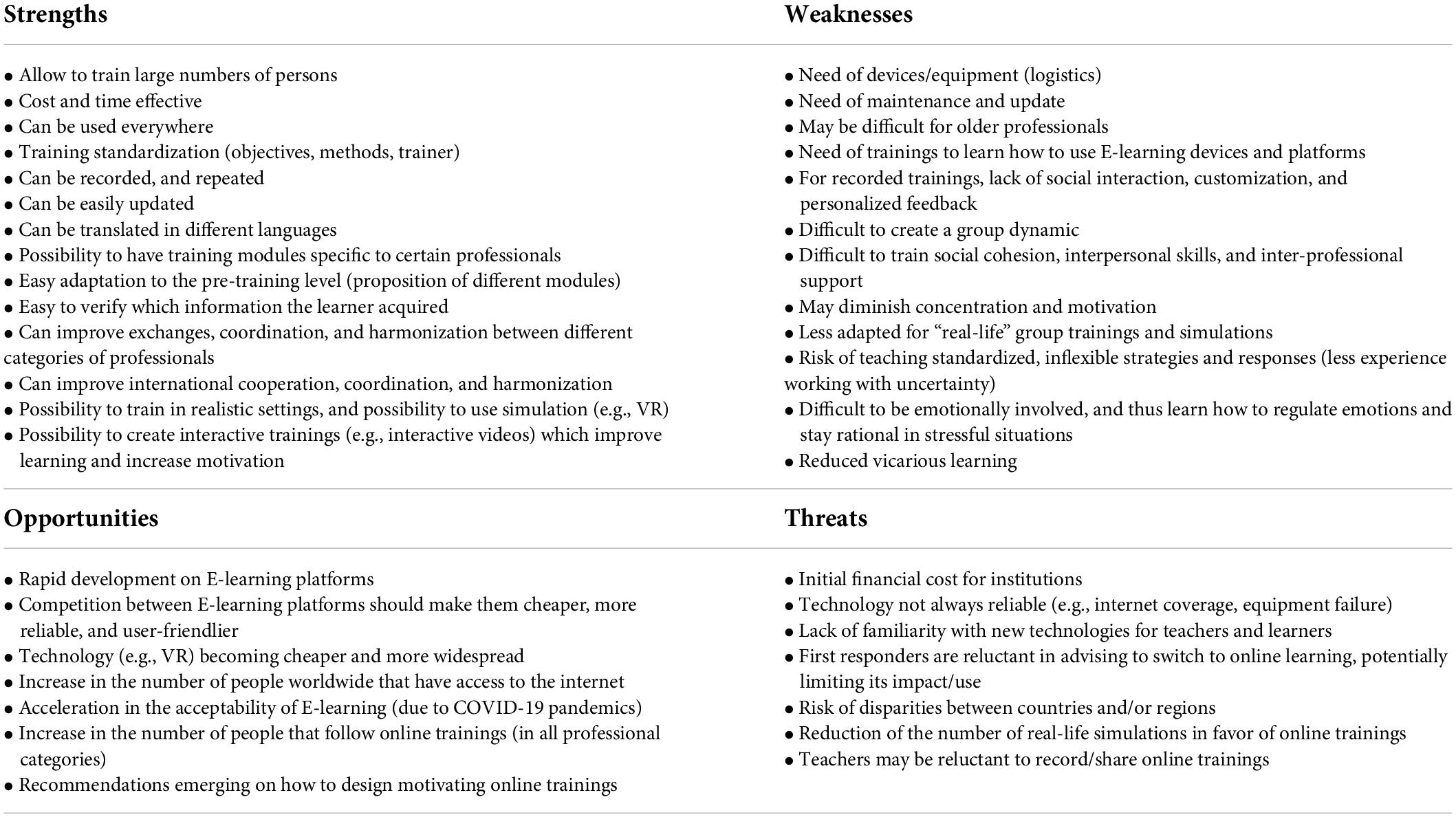
Table 2. Training of professionals in the acute phase: SWOT Analysis of using ICT.
Participants
The survey was completed by 36 international experts working on trauma/traumatic stress. 94% of them (N = 34) reported to have direct experience with the acute response after terrorist attacks in the following countries: Belgium, France, Germany, Finland, Israel, Luxemburg, Norway, Portugal, Spain, United Kingdom. The years of professional experience ranged from 2 to 34 (mean = 16 years, SD = 9 years). The experts included (more than one response was possible): clinicians (89%; N = 32), including psychologists, psychiatrists, and medical doctors; researchers (42%; N = 15) in the domains of psychology, psychiatry, child and adolescent psychiatry, forensic science, public health, sociology/suicidology, or education; first responders (25%; N = 9), including emergency medical technicians, psychologists, psychiatrists, NGO representatives, psychosocial emergency services, policemen and nurses; and people working in victim support organizations (25%; N = 9). In addition to terror attack, the experts worked with the following types of traumas: Single trauma (89%, N = 32), Disaster (89%, N = 32), Death/Bereavement (83%, N = 30), Repeated Trauma (81%, N = 29), Child Abuse/Maltreatment (75%, N = 27), Vicarious Traumatization in Professionals/Helpers (67%, N = 24), Rape/Sexual Assault (64%, N = 23), Refugee/Displacement Experiences (56%, N = 20), Intimate Partner Violence (53%, N = 19), War/Post-Conflict Settings – Civilians (50%, N = 18), Torture (50%, N = 18), Community Violence (47%, N = 17), Medical Trauma (47%, N = 17), Racism/Historical Trauma (25%, N = 9), War – Military/Peacekeepers/Veterans (36%, N = 13). In terms of populations, the experts had professional experience working with adults (89%, N = 32), adolescents (78%, N = 28), children (67%, N = 24), seniors (39%, N = 14), people with special needs (25%, N = 9), and babies/toddlers (22%, N = 8), Overall, 67% of the experts (N = 24) declared to be involved in the organization of specific trainings on acute post-disaster psychosocial care in their country.
Results
The results of the rating questions concerning the topics that are important to include into inter-professional and international trainings are reported in Table 1. As a group, the 36 experts that responded to the survey strongly agreed (mean score greater than 6) that it is necessary that all the professionals involved in the acute phase know how/where to register the information of the impacted people for future tracking, how to screen/detect individuals that need specific psychosocial support, where and towards whom referring victims who need psychosocial support, how to identify, handle and/or orient vulnerable victims (for instance children, people with disability, foreigners, pregnant women), and that they are themself particularly at risk for PTSD and other psychiatric disorders. The experts moderately agreed (scores between 5 and 6) that all the professionals should know how to use basic tools for psychosocial support (such as relaxation), that they should be aware of all the services available for victims (e.g., social, legal, medical), and that each European country has its own system to support their citizens. Furthermore, they moderately agreed on the fact that new ICT, such as online platforms and Virtual Reality, should be used to train the professionals involved in the emergency response phase. In the open comments, the experts stressed that, despite most of these topics are included in existing trainings, it is important that all professionals have common knowledge, to facilitate inter-professional and international exchange. These general trainings are meant to complement – and not to replace - the trainings organized at the national and local level, and those organized for specific categories of professionals, which provide important action plans that are location- and profession- specific.
Concerning the analysis of the positive and negative aspects of organizing remote trainings for professionals involved in the acute response phase of a terror attack, we performed a SWOT analysis based on the open comments provided by the 36 experts that responded to the survey, and by the comments provided during the plenary meeting by all the 47 experts. The results are reported in Table 2.
Strengths
The experts recognized that, as to all professional trainings, remote trainings for professionals involved in the acute response phase can allow to train large numbers of persons everywhere, being thus cost-and time-effective. They suggested that trainings can be recorded, repeated, updated, and translated in different languages (or subtitled), thus allowing training standardization in terms of objectives, methods, and trainers. Similarly, remote trainings offer the possibility to design training modules specific to certain categories of professionals and customized to the pre-training level. In the experts’ opinion, remote trainings can improve exchanges, coordination, and harmonization between different categories of professionals and can improve international cooperation, coordination, and harmonization (or, at minimum, increase the awareness that different countries have in place different regulations and procedures). Furthermore, the experts highlighted that it may be quite easy to verify (e.g., via a multiple-choice questions) which information the learner acquired, at least in terms of explicit knowledge. They advanced that it is possible, even if it requires specific competence, to design trainings in more realistic settings, for instance using Virtual Reality or Augmented Reality applications, and to create interactive trainings (e.g., interactive videos) which may improve learning and increase motivation.
Weaknesses
The experts acknowledged that remote trainings for professionals involved in the acute response phase have the same limitations as those for other professionals in terms of technical requirements, but have also some specificities. As any other remote training, there is a need of devices/equipment (logistics), of maintenance and update, and of learning how to use E-learning devices and platforms. This is especially true for professionals not familiar with new technologies, such as elderly people. The experts suggested that, especially for recorded offline trainings, there is a lack of social interaction, customization, and of personalized feedback, which may diminish concentration and motivation to learn. Vicarious learning may also be also reduced. The experts acknowledged that group dynamics may be more difficult to create. This is particularly important for professionals involved in the acute response phase because they must work on the sense of social cohesion, on interpersonal skills, and inter-professional support. They also highlighted a potential risk of teaching standardized, inflexible strategies and responses, thus reducing the self-awareness of what happens when working under uncertainty and complex, evolving situations. Indeed, in remote trainings it may be harder to become emotionally involved due to the physical distance among participants, and thus participants may have a reduced experience in learning how to regulate emotions and stay rational in stressful situations. In the experts’ opinion, the ability to work in chaotic, stressful settings can be better trained using role-playing and simulation training methods.
Opportunities
The experts acknowledged that, due to the COVID-19 crisis, we are experiencing an acceleration of the development on E-learning platforms from different producers, resulting in cheaper, more reliable, and user-friendlier interfaces. Similarly, the acceptability on online trainings has increased, as both teachers and learners understood the advantages of remote learning (time and cost efficiency, possibility to customize, etc). In parallel, there is an increase worldwide in the number of people that have access to the internet, and technologies are becoming cheaper and more widespread, including VR and other applications to make trainings more immersive and interactive. Importantly, the experts recognized that recommendations are now emerging on how to design motivating online trainings, which are promising for the future of remote teaching (40).
Threats
The experts highlighted that creating high-quality remote trainings may have an initial financial cost for institutions and may be time-consuming, thus limiting the number of trainings that are developed. This may be worsened by the lack of familiarity with new technologies for teachers and learners. In addition, the experts recognized that technologies are not always reliable (e.g., internet coverage, equipment failure), limiting actual use of remote trainings. Based on the expert panel expertise, first responders may be reluctant in advising to switch to online learning, potentially limiting its impact/use. Other listed threats included the risk of disparities between countries and/or regions depending on the internet coverage, and the fact that teachers may be reluctant to record/share online trainings, especially professional teachers that teach as a job. In addition, the reduction of the number of real-life simulations in favor of online trainings may be risky, as role-playing and simulations are considered as essential part of the training for the professionals involved in an emergency response.
Discussion
The expert panel in the context of EUCVT network, including researchers and different categories of professionals working with victims of terror attacks, agreed on the importance of designing international and inter-professional trainings. These training should at least include information on the initial triage, registration, screening, first support, and referral of victims to the right professionals and services, with a special attention to vulnerable victims and victims that were affected by a terrorist attack in another country than their home country. In addition, interprofessional trainings should include modules warning on the increased risk of developing PTSD and other psychiatric disorders for the professionals involved in the acute response phase, and on how to detect potential symptoms and apply selfcare. Despite these topics are included in trainings, the experts acknowledged that it is crucial to get a common ground among professional and countries, with the objective to complement existing national, local and professional-specific trainings, and facilitate the inter-professional exchange. Concerning the use of remote training platforms, converging with previous guidelines (e.g., (41)), the experts highlighted several advantages and opportunities, including the possibility to train more professionals everywhere, possibly sharing the same information across different professionals and countries. This is harder to do with classical training methods, due to logistic complexity. Despite the clear interest, remote trainings have several limitations, and should not replace completely physical trainings. The experts highlighted that real event simulations, role-playing and group exercises are crucial for professionals involved in terror attacks, and should not be replaced, and used in complement with new technologies such as Virtual Reality and Augmented Reality that, when confirmed to be reliable and effective, will be made available to the wide public. Hybrid training formats, combing online trainings for acquiring more theoretical knowledge (know what) and in person trainings to get first-hand experience on emotion regulation, decision making in stressful situation, and interpersonal cooperation (know how) should be favored. While these considerations are valid for all professional trainings, it is important to highlight the strengths and weaknesses of online trainings in the domain of preparedness for the emergency response phase to allow this specific field to grow more rapidly, and design trainings involving different professionals and countries. It would be important to verify if the perspective provided in this paper are shared by larger groups of professionals, as well as to compare the perspectives of different professionals and, even more, to broaden the scope up to victims of other potentially traumatic events and people exposed to disasters. Finally, any form of training can only fulfill its promise of a strengthened service delivery when it is implemented effectively. Among the implementation factors to consider, it is highly likely that the culture and supportive setting within organizations are linked to the motivation, capability, and opportunity of trainees to effectively participate in remote learning and the practical application of the training content.
Data availability statement
The original contributions presented in this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
FA and VM coordinated the expert panel. VM, FA, ON, MG, and ST wrote the first draft of the manuscript. All authors of the manuscript participated to the expert panel organization and discussions, and contributed to the manuscript drafting and revision.
Funding
The expert panel was organized in the context of the “EU Centre of expertise for victims of terrorism” project, financed by the European Commission (2020-2021; service contract: JUST/2018/JPPI/PP/CRIM/0165). LS contribution was funded by the Research Council of Norway (Grant No. 288321).
Acknowledgments
We kindly thank Victim Support Europe team, especially to Annelies Blonde, for the support in the organization of the hybrid plenary meeting, and all the partners of the EUCVT project (VSE -Victims Support Europe, ARQ National Psychotrauma Centre, AFVT -Association française des Victimes du Terrorisme, and the Fondation Lenval). Special thanks to all the experts that participated in the expert panel in addition to the authors, and to the experts that provided talks during the plenary meeting, listed here in alphabetical order: Alicia Alvarez-Garcia, Philippe Auby, Alan Barret, Michel Benoit, Claire Bonafons, Eleonore Brocq, Eric Bui, Terry Conter, Nicholas Desbiendras, Pauline Espi, Olivier Fossard, Matthieu Fraigneau, Iryna Frankova, Eric Gokalsing, Ana Gourves, Talya Greene, Marie Gros, Susheel Gupta, Sigal Haimov, Christophe Laffineur, Tamar Lavi, Patrice Louville, Noortje Jansen, Louis Jehel, Clare Jones, Marie-Line Menard, Idit Michael, Justus Münster, Véronique Nahmias, Ana Oliveira, Julie Safont, Florian Stoeck, Jarno Tuominen, Caroline Turchini, Anne-Julie Vaillant, Guillaume Vaiva, Nils Vandenbroucke, Sébastien Viano, Andrea Walraven-Thissen, Peter Waterstraat, Jelena Watkins, Arthur Welly, and Anna Wergen.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Askenazy F, Gindt M, Chauvelin L, Battista M, Guenolé F, Thümmler S. Early phase psychiatric response for children and adolescents after mass trauma: Lessons learned from the truck-ramming attack in nice on July 14th, 2016. Front Psychiatry. (2019) 10:65. doi: 10.3389/fpsyt.2019.00065
2. Bisson J, Tavakoly B. The TENTS Guidelines for Psychosocial care Following Disasters and Major Incidents. Wales: The European Network for Traumatic Stress (2008).
3. French P, Barrett A, Allsopp K, Williams R, Brewin CR, Hind D, et al. Psychological screening of adults and young people following the Manchester arena incident. BJPsych Open. (2019) 5:e85. doi: 10.1192/bjo.2019.61
4. Karki FU. Norway’s 2011 terror attacks: Alleviating National Trauma with a large-scale proactive intervention model. Psychiatr Serv. (2015) 66(9):910–2. doi: 10.1176/appi.ps.201500050
5. Liu SY, Lim S. Collective trauma and mental health hospitalization rates among children in New York State, 1999–2013: Age. Period, and cohort effects. J Traum Stress. (2020) 33:824–34. doi: 10.1002/jts.22449
6. Mortamet G, Lode N, Roumeliotis N, Baudin F, Javouhey E, Dubos F, et al. Disaster preparedness in French paediatric hospitals 2 years after terrorist attacks of 2015. Arch Dis Child. (2019) 104:322–7. doi: 10.1136/archdischild-2017-314658
7. Prieto N, Cheucle E, Faure P, Digard F, Dalphin C, Pachiaudi V, et al. Defusing of victims of the terrorist attacks in Paris. Elements of assessment one-month post-event. Encephale. (2016) 44:118–21. doi: 10.1016/j.encep.2016.10.002
8. Brewin CR, Scragg P, Robertson M, Thompson M, d’Ardenne P, Ehlers A. Promoting mental health following the London bombings: A screen and treat approach. J Traum Stress. (2008) 21:3–8. doi: 10.1002/jts.20310
9. Haga JM, Thoresen S, Stene LE, Wentzel-Larsen T, Dyb G. Healthcare to parents of young terrorism survivors: A registry-based study in Norway. BMJ Open. (2017) 7:e018358. doi: 10.1136/bmjopen-2017-018358
10. Uchida M, Feng H, Feder A, Mota N, Schechter CB, Woodworth HD, et al. Parental posttraumatic stress and child behavioral problems in world trade center responders. Am J Ind Med. (2018) 61:504–14.
11. Dyregrov A, Djup HW, Barrett A, Watkins J, Kärki FU. Learning from a decade of terror in European cities: Immediate, intermediate, and long-term follow-up. Scand Psychol. (2019) 6. doi: 10.15714/scandpsychol.6.e10
12. Juen B, Warger R, Nindl S, Siller H, Lindenthal MJ, Huttner E, et al. The comprehensive Guideline on Mental Health and Psychosocial Support (MHPSS) in Disaster Settings. Innsbruck: OPSIC (2016).
13. Askenazy F, Chauvelin L, Gindt M, Thümmler S. Emergency child psychiatry response following the 14 July 2016 terrorist attack in Nice, France. Arch Pediatr. (2017) 24:1220–7. doi: 10.1016/j.arcped.2017.09.003
14. Craigie RJ, Farrelly P, Santos R, Smith S, Pollard J, Jones D. Manchester Arena bombing: Lessons learnt from a mass casualty incident. BMJ Mil Health. (2020) 166:72–5.
15. Stene LE, Vuillermoz C, Van Overmeire R, Bilsen J, Dückers M, Govasli Nilsen L, et al. Psychosocial care responses to terrorist attacks: A country case study of Norway, France and Belgium. BMC Health Serv Res. (2022) 22:390. doi: 10.1186/s12913-022-07691-2
16. Jenness JL, Jager-Hyman S, Heleniak C, Beck AT, Sheridan MA, McLaughlin KA. Catastrophizing, rumination, and reappraisal prospectively predict adolescent PTSD symptom onset following a terrorist attack. Depress Anxiety. (2016) 33:1039–47. doi: 10.1002/da.22548
17. Miron LR, Orcutt HK, Kumpula MJ. Differential predictors of transient stress versus posttraumatic stress disorder: Evaluating risk following targeted mass violence. Behav Ther. (2014) 45:791–805. doi: 10.1016/j.beth.2014.07.005
18. Chauvelin L, Gindt M, Olliac B, Robert P, Thümmler S, Askenazy F. Emergency organization of child psychiatric care following the terrorist attack on July 14, 2016, in Nice, France. Disaster Med Public Health Prep. (2019) 13:144–6. doi: 10.1017/dmp.2018.51
19. World Health Organization. Guidelines for the Management of Conditions that are Specifically Related to Stress. Geneva: World Health Organization (2013).
20. National Collaborating Centre for Mental Health. Post-traumatic stress disorder: The management of PTSD in adults and children in primary and secondary care. London: National Collaborating Centre for Mental Health (2005).
21. Jacobs J, Oosterbeek M, Tummers LG, Noordegraaf M, Yzermans CJ, Dückers ML. The organization of post-disaster psychosocial support in the Netherlands: A meta-synthesis. Eur J Psychotraumatol. (2019) 10:1544024. doi: 10.1080/20008198.2018.1544024
22. Magruder KM, Kassam-Adams N, Thoresen S, Olff M. Prevention and public health approaches to trauma and traumatic stress: A rationale and a call to action. Eur J Psychotraumatol. (2016) 7:29715. doi: 10.3402/ejpt.v7.29715
23. Reeping PM, Jacoby S, Rajan S, Branas CC. Rapid response to mass shootings. Criminol Public Policy. (2020) 19:295–315. doi: 10.1111/1745-9133.12479
24. Gowing JR, Walker KN, Elmer SL, Cummings EA. Disaster preparedness among health professionals and support staff: What is effective? An integrative literature review. Prehosp Disaster Med. (2017) 32:321–8. doi: 10.1017/S1049023X1700019X
25. Dückers M, van Hoof W, Willems A, te Brake H. Appraising evidence-based mental health and psychosocial support (MHPSS) guidelines—PART II: A content analysis with implications for disaster risk reduction. Int J Environ Res Public Health. (2022) 19:7798. doi: 10.3390/ijerph19137798
26. Mustafa S, Zhang Y, Zibwowa Z, Seifeldin R, Ako-Egbe L, McDarby G, et al. COVID-19 Preparedness and Response Plans from 106 countries: A review from a health systems resilience perspective. Health Policy Plan. (2022) 37:255–68. doi: 10.1093/heapol/czab089
27. Rerbal D, Prieto N, Vaux J, Gloaguen A, Desclefs JP, Dahan B, et al. Organisation et modalités d’intervention des cellules d’urgence médicopsychologique. Recommandations de la société française de médecine d’urgence (SFMU) en collaboration avec l’association de formation et de recherche des cellules d’urgence médicopsychologique-Société française de psychotraumatologie (AFORCUMP-SFP). Ann Fr Méd Urgence. (2017) 7:410–24.
28. Roudini J, Khankeh HR, Witruk E. Disaster mental health preparedness in the community: A systematic review study. Health Psychol Open. (2017) 4:2055102917711307.
29. Verheul ML, Dückers ML. Defining and operationalizing disaster preparedness in hospitals: A systematic literature review. Prehosp Disaster Med. (2020) 35:61–8. doi: 10.1017/S1049023X19005181
30. Hennus MP, van Dam M. A standard operating procedure for developing and hosting a webinar for healthcare professionals new to online teaching. Postgrad Med J. (2021) 97:683. doi: 10.1136/postgradmedj-2020-138767
31. Hubertus Bessems KMH, Simovska V, Driessen Willems MD, Carlsson M, de Vries NK. Factors influencing sustainability of online platforms for professionals: A mixed-method study in OECD countries. Health Promot Int. (2021) 37:daab063. doi: 10.1093/heapro/daab063
32. Morgan AJ, Ross A, Reavley NJ. Systematic review and meta-analysis of Mental Health First Aid training: Effects on knowledge, stigma, and helping behaviour. PloS one (2018) 13:e0197102. doi: 10.1371/journal.pone.0197102
33. Sijbrandij M, Horn R, Esliker R, O’May F, Reiffers R, Ruttenberg L, et al. The effect of psychological first aid training on knowledge and understanding about psychosocial support principles: A cluster-randomized controlled trial. Int J Environ Res Public Health. (2020) 17:484. doi: 10.3390/ijerph17020484
34. Orui M, Fukasawa M, Horikoshi N, Suzuki Y, Kawakami N. Development and evaluation of a gatekeeper training program regarding anxiety about radiation health effects following a nuclear power plant accident: A single-arm intervention pilot trial. Int J Environ Res Public Health. (2020) 17:4594. doi: 10.3390/ijerph17124594
35. Crisanti AS, Earheart JA, Rosenbaum NA, Tinney M, Duhigg DJ. Beyond crisis intervention team (CIT) classroom training: Videoconference continuing education for law enforcement. Int J Law Psychiatry. (2019) 62:104–10. doi: 10.1016/j.ijlp.2018.12.003
36. Katzman JG, Tomedi LE, Thornton K, Menking P, Stanton M, Sosa N, et al. Innovative COVID-19 programs to rapidly serve New Mexico: Project ECHO. Public Health Rep. (2021) 136:39–46. doi: 10.1177/0033354920969180
37. Evans CM, Adams RM, Peek L. Incorporating mental health research into disaster risk reduction: An online training module for the hazards and disaster workforce. Int J Environ Res Public Health. (2021) 18:1244. doi: 10.3390/ijerph18031244
38. Bisson J I, Tavakoly B, Witteveen AB, Ajdukovic D, Jehel L, Johansen VJ, et al. TENTS guidelines: Development of post-disaster psychosocial care guidelines through a Delphi process. Br J Psychiatry. (2010) 196:69–74. doi: 10.1192/bjp.bp.109.066266
39. Te Brake H, Dückers M. Early psychosocial interventions after disasters, terrorism and other shocking events: Is there a gap between norms and practice in Europe? Eur J Psychotraumatol. (2013) 4:19093. doi: 10.3402/ejpt.v4i0.19093
40. Baldwin-Clark TC. A joke no more: Online education in the face of COVID-19. Local Dev Soc. (2021):1–5. doi: 10.1080/26883597.2021.1935303
Keywords: terror attack, acute response phase, remote training, information and communication technologies, SWOT analysis
Citation: Askenazy F, Fernandez A, Altan L, Battista M, Dückers M, Gindt M, Nachon O, Ivankovic A, Porcar-Becker I, Prieto N, Robert P, Stene LE, Thummler S and Manera V (2022) Remote training as a common tool for the different professionals involved in the acute phase after terror attacks across Europe: Perspectives from an expert panel. Front. Psychiatry 13:915929. doi: 10.3389/fpsyt.2022.915929
Received: 08 April 2022; Accepted: 01 August 2022;
Published: 23 August 2022.
Edited by:
Eva Yin-han Chung, The Education University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Jyoti Belur, University College London, United KingdomCopyright © 2022 Askenazy, Fernandez, Altan, Battista, Dückers, Gindt, Nachon, Ivankovic, Porcar-Becker, Prieto, Robert, Stene, Thummler and Manera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Valeria Manera, dmFsZXJpYS5tYW5lcmFAdW5pdi1jb3RlZGF6dXIuZnI=