 Zongliang Wen
Zongliang Wen Jintao Xu
Jintao Xu Jinxun Yu
Jinxun Yu Xiaojing Huang
Xiaojing Huang Yuting Ni
Yuting Ni- 1School of Management, Xuzhou Medical University, Xuzhou, China
- 2School of Public Health, Xuzhou Medical University, Xuzhou, China
- 3Affiliated Hospital of Xuzhou Medical University, Xuzhou, China
Background: Countries worldwide face the challenge of how medical personnel manage conflicts between work and family. Especially after the challenge of the COVID-19 epidemic, it is necessary to explore the possible mechanisms of work-family conflict, burnout, and turnover intention among primary medical staff.
Objectives: This study aims to observe the turnover intention of Chinese primary medical staff and explore the relationship between work-family conflict, burnout, and turnover intention.
Methods: A cross-sectional study included a turnover intention questionnaire, the Maslach Burnout Inventory-General Survey (MBI-GS), and the Work-Family Conflict Scale (WFCS) to understand turnover intention, burnout, and work-family conflict among primary medical staff in four cities (Xuzhou, Linyi, Huaibei, and Shangqiu cities) within the Huaihai Economic Zone. Spearman correlation analysis and hierarchical multiple regression analysis were used to examine the related factors of turnover intention. Structural equation modeling (SEM) was used to study the mediating role of burnout between work-family conflict and turnover intention.
Results: In this study, there is a positive correlation between work-family conflict and turnover intention (P < 0.01). Demographic characteristics, work-family conflict, and burnout explained 2.3%, 20.3%, and 8.8% of the incremental variances, respectively. Burnout mediated the association between work-family conflict and turnover intention.
Conclusions: Burnout can be regarded as a mediator between two different variables: work-family conflict and turnover intention. Improving work-family conflict and alleviating burnout may play a key role in reducing the willingness of primary medical staff to resign. Corresponding measures can be taken to balance the conflict between work and family, alleviate burnout, reduce turnover rates, and build a primary medical staff team with higher medical service quality and stability.
1. Introduction
Since the outbreak of COVID-19, China's grassroots medical work has become the top priority nationwide and has attracted much attention because it is the first line of defense on the anti-epidemic front. In the process of combating the epidemic, primary medical staff need to take on responsibilities beyond their original job responsibilities, such as investigating cases, providing psychological and spiritual support to patients, and facing enormous work and life pressures. They make every effort to secure medical supplies, coordinate various resources, and selflessly devote themselves to frontline pandemic prevention efforts (1, 2). After the epidemic was brought under control, China's National Health Commission also introduced a series of measures to support and strengthen primary medical institutions and staff. In addition, with the promotion of China's “Healthy China 2030” policy, primary medical staff need to take on more responsibilities, such as carrying out health education and providing basic medical services and rehabilitation services (3).
Overall, with the outbreak of the epidemic and the implementation of various health policies, primary medical work has received unprecedented attention and deeper reforms, while staff have assumed more responsibilities and obligations. Therefore, the psychological health and team stability of primary medical staff also need to be taken seriously.
Primary medical staff are a key component of the healthcare system, an important human resource of the health system, and the gatekeepers of residents' health. The role of primary medical staff in modern healthcare is becoming increasingly extensive and important (4, 5). However, due to the objective reasons of numerous service objects and high work intensity, stressors such as burnout, high work pressure, long working time, a large workload, low job satisfaction, a lack of incentive mechanisms, and low promotion prospects will adversely affect turnover intention and the stability of primary medical staff (6–9).
The motivation and tendency of in-service personnel to leave their current position is called turnover intention, which is a subjective factor that previously led to turnover behavior (10). Studies have found that turnover intention is associated with professional identity, work environment, burnout, job satisfaction, and stress (11, 12). Scholars in China and abroad have shown through research on the current situation of medical staff that there is a significant positive correlation between burnout and turnover intention, namely, the higher the level of burnout among medical staff, the higher their turnover intention (13–17). In a study involving 2,263 physicians in the United States, only 7% were certain that they would resign within 2 years (18). In Australia's primary health network, 21.3% of general practice nurses plan to leave once it is convenient, and 20.2% of general practice nurses want to leave (19).
Meanwhile, a study in the UK showed that 21.5% of primary healthcare nurses had considered quitting (20). However, the incidence of turnover intention among village doctors in China has reached 44.1%, which is twice or even six times that of primary medical staff in developed countries, seriously damaging the stability of medical staff construction and leading to the decline of medical quality (16). A systematic review and meta-analysis of the turnover intention of Chinese primary medical staff showed that, out of 37,672 primary medical staff, 30.4% are willing to resign (21). Therefore, reducing the primary medical staff's turnover intention is of great significance for stabilizing the primary medical team, heightening primary medical services' level and quality, and safeguarding people's health.
An increasing number of research literature indicates that work-family conflict can influence turnover intention in various ways, including reduction of work stress, improvements in the work environment, enhancement of the psychological contract, and an increase in work satisfaction (22–25). Work-family conflict adversely affects individuals' work and family lives to the extent that it affects overall wellbeing and health and even has dysfunctional and socially expensive effects (26). Previous research has shown that work-family conflict is an important predictive factor of turnover intention (27–29). In addition, work-family conflict could immediately or immediately affect other work-related factors such as presenteeism, anxiety, work engagement, or employee performance through mediation (30–32). In conclusion, reducing primary medical staff's work-family conflict can reduce work stress and turnover intention.
In addition to the aforementioned work-family conflict, burnout has been shown to correlate strongly with turnover intentions (33). Burnout is a long-term response to interpersonal stress and chronic negative emotions at work, defined by three dimensions: cynicism, exhaustion, and ineffectiveness (34). The relationship between turnover intention and factors related to professional identity, emotional labor, and intrinsic motivation could also be moderated by burnout (35–37). Burnout not only affects an individual's quality of life but also has an undeniable effect on organizational performance and costs (38). Burnout can lead to decreased productivity and impaired work quality.
Meanwhile, people suffering from burnout at work can affect the completion of work tasks and transmit this “work state” to colleagues, forming a “contagion” that can be sustained through social interactions at work, thereby affecting the entire work environment (26). Therefore, we hypothesized that burnout might mediate the relationship between turnover intention and other work-related factors, such as work-family conflict. Alleviating burnout among primary medical staff may play an important role in reducing their willingness to resign. Although more and more research focuses on this relationship between work-family conflict and turnover intention among primary medical staff, there is limited research on the mediating role between work-family conflict and turnover intention. Especially in China, there is currently little research on the turnover intention of primary medical staff, and most studies focus solely on the turnover intention of doctors or nurses (12, 16, 17, 22, 23, 35, 37). In rare studies on the turnover intention of primary medical staff, burnout and turnover intention have been involved, but the relationship between work-family conflict and primary medical staff turnover intention has not been explored (7, 9). Therefore, our study focused on primary medical staff in four cities (Xuzhou, Linyi, Huaibei, and Shangqiu) in the Huaihai Economic Zone to measure work-family conflict, turnover intention, and burnout and explore the relationship among them. The following hypotheses guided our analysis:
Hypothesis 1: There is no correlation between work-family conflict and turnover intention.
Hypothesis 2: Burnout has no impact on turnover intention.
Hypothesis 3: Burnout does not play a mediating role between work-family conflict and turnover intention.
2. Materials and methods
2.1. Participants, procedure, and ethics statement
On 15 March 1986, the Huaihai Economic Zone was established, with a total area of 178,000 sq. km. It has 14 prefecture-level cities in Jiangsu, Anhui, Henan, and Shandong provinces and is one of the earliest regional economic cooperation organizations in China. The Huaihai Economic Zone is the intersection of these four provinces. The development speed of cities in this region is relatively slow, with a weak economic foundation and less support from higher-level governments. However, with a large population of 120 million, the task of providing grassroots medical care is significant. Moreover, the cultural and social customs in the region are similar, and the research has promotional significance.
From February 2023 to March 2023, according to the distribution of population and the distribution of primary medical staff, a cross-sectional survey with a simple random sampling design was conducted in Xuzhou, Linyi, Huaibei, and Shangqiu cities of China through multiple communications with the staff of local health commission departments.
The survey was distributed by the administrative personnel of the local Municipal Health Commission to all primary medical institutions within their jurisdiction. Before the survey, all primary medical staff learned about the study through the WeChat working group, knew the purpose, risks, benefits, and process of the study, and ensured the confidentiality of the data. Then, they chose whether to participate in the questionnaire according to their own situation. The questionnaire, developed by Wenjuanxing—a widely used online survey platform in China–was distributed to respondents' mobile phones either as QR codes or links to the questionnaire website. After the respondents submitted their informed consent form, they filled out the corresponding questionnaire on their mobile phones. If there was a pattern of inconsistent answers in the respondents' questionnaire filling (such as selecting the same option for the entire questionnaire) or incomplete filling, the response was considered invalid and was deleted. Respondents had to be at least 20 years old, should have worked for more than 6 months, be limited to doctors, nurses, pharmacists, or administrators, and should voluntarily participate in the survey. The informed consent form included the study's purpose, risks, benefits, and process. In particular, strict protection of their privacy should be ensured in this study.
The questionnaire contained a turnover intention questionnaire, the Maslach Burnout Inventory-General Survey (MBI-GS), the Work-Family Conflict Scale (WFCS), and self-developed questions on demographic characteristics. The validated questionnaire took ~20 min to complete. A total of 2,501 survey questionnaires were received, and 2,259 valid questionnaires were collected, with an effective recovery rate of 90.32%. The study complied with the Declaration of Helsinki as revised in 1989, and the protocol was authorized by the Ethics Committee of Xuzhou Medical University (ID: 225281).
2.2. Baseline characteristics of the primary medical staff
We collected baseline characteristics of primary medical staff, which include age, gender (men and women), monthly income [≤ 3,000 yuan (≤ US $430.9), 3,001–5,000 yuan (US $430.9–$718.2) and >5,000 yuan (>US$718.2)], education (junior college and below, bachelor degree and above), specialty (clinical medicine, medical technology, preventive medicine, nursing, pharmacy or else), technical title (no title, primary title, middle title, vice-senior title, or above), years of work (<2, 3–5, 6–9, or ≥10 years), and weekly hours at work (≤ 40, >40).
2.3. Assessment of turnover intention
We used the Chinese version of the turnover intention questionnaire developed by Cammannet and Mobiley to measure respondents' turnover intention (39). It consists of four items: “Thought of leaving this industry,” “Thought of leaving the organization you serve now,” “Looking for a new job next year,” and “Looking for a new job recently.” The Likert scale uses a 5-point scale, ranging from 1 (very dissatisfied) to 5 (very satisfied), to evaluate all of these items, where higher scores indicate a higher willingness to resign. The Cronbach's alpha coefficient for turnover intention in this study was 0.883.
2.4. Assessment of work-family conflict
The Chinese version of the multidimensional Work-Family Conflict Scale (WFCS) was adopted to evaluate work-family conflict (40). WFC consists of 18 items with two subscales: work-to-family interference (WIF) and family-to-work interference (FIW). WIF refers to the negative impact of work-related requirements and obligations on family life. FIW means that conflicts caused by family obligations can interfere with personal work. Both subscales include conflicts of time, stress, and behavior. Work-family conflict was evaluated using a 5-point Likert scale, ranging from 1 (highly disagree) to 5 (highly agree). The Cronbach's alpha for WFC in this study was 0.940.
2.5. Assessment of burnout
The burnout of primary medical staff was evaluated with the Chinese version of the Maslach Burnout Inventory-General Survey (MBI-GS) (33, 34). The scale includes three subscales: emotional exhaustion, depersonalization, and low personal achievement (reverse score). The response was set to a 7-Likert score, ranging from 0 (never) to 6 (daily). Among them, emotional exhaustion scores >25, depersonalization scores >11, and low personal achievement scores >16 were considered to be high burnout. Burnout can be diagnosed when the score of any dimension of the respondents is greater than the critical value. The Cronbach's alpha coefficient for MBI-GS in this study was 0.793.
2.6. Statistical analyses
Statistical analysis was conducted using SPSS version 23.0 and Amos 26.0 Windows statistical software (IBM Corporation). The Kruskal–Wallis test and one-way analysis of variance (ANOVA) were used to explore the relationship between turnover intention and demographic variables. Pearson correlation analysis was used to examine the correlation between turnover intention, burnout, and work-family conflict.
We used hierarchical multiple regression (HMR) analysis methods to explore the relevant factors affecting turnover intention: Step 1: baseline characteristics of the primary medical staff; Step 2: work-family conflict of the primary medical staff; and Step 3: burnout of the primary medical staff. As a dependent variable, the turnover intention score is continuous in HMR. Using standardized parameter estimation (standardized β) to evaluate the degree of correlation between the dependent and independent variables. We used structural equation modeling (SEM) to explore the mediating role of burnout, with turnover intention as the dependent variable, work-family conflict as the independent variable, and burnout as the mediating variable. A two-tailed P-value of <0.05 was considered statistically significant.
3. Results
3.1. Baseline characteristics of the participants
The baseline characteristics and distribution of turnover intention among primary medical staff are shown in Table 1. A total of 2,259 primary medical staff members participated in the study. Nearly 90% of the participants were over 30 years old (2,022, 89.51%), and more than 60% of the participants were women (1,431, 63.35%). Over three-quarters of the participants had a junior college degree or below (1,709, 75.65%). The number of participants with a primary title is the highest (1,017, 44.98%), and the primary title is the most basic level of technical title. Nearly three-quarters of the participants had worked for over 10 years (1,685, 74.59%). The results of univariate analysis showed that participants over 30 years old had lower turnover intention scores than participants under 30 years old (P = 0.044). Female participants had lower turnover intention (P = 0.005). The higher the monthly income of participants, the lower the turnover intention score (P = 0.019). At the same time, the turnover intention scores were different among participants with different specialties (P < 0.001). Participants with a higher technical title had lower turnover intention (P = 0.018).

Table 1. Baseline characteristics of the distribution of the turnover intention among primary medical staff (N = 2,259).
3.2. Turnover intention of the participants
The average score of the primary medical staff's turnover intention was 7.62 ± 3.66. The total score of turnover intention is less than half of the total score (out of 20), and the level of turnover intention among primary medical staff is relatively low. The item with the highest average score is “Thought of leaving the organization you serve now,” with an average score of 2.20 ± 1.17. The item with the lowest average score is “Looking for a new job next year,” with an average score of 1.62 ± 0.93.
3.3. Work-family conflict among the participants
The average score of the primary medical staff's work-family conflict was 45.68 ± 14.47. The total score of work-family conflict is higher than half of the total score (out of 90), and the level of work-family conflict among primary medical staff is relatively high. The highest average score is the impact of time in WIF, with an average score of 9.52 ± 3.39. The lowest average score is the impact of stress in FIW, with an average score of 5.82 ± 2.81. The average total score of WIF is 8.52 ± 3.34. The average total score of FIW is 6.70 ± 3.03.
3.4. Burnout of the participants
The average score of the primary medical staff's burnout was 36.00 ± 14.32. The total burnout score is less than half of the total score (out of 132), and the level of burnout among primary medical staff is low. The average scores of emotional exhaustion, depersonalization, and low personal achievement were 12.37 ± 7.72, 2.88 ± 3.22, and 20.75 ± 9.18 in this study, respectively.
3.5. Correlations between turnover intention, work-family conflict, and burnout
Table 2 shows that there was a significant correlation between work-family conflict, burnout, and turnover intention (P < 0.01). Work-family conflict had a positive correlation with turnover intention (P < 0.01). At the same time, burnout had a positive correlation with both work-family conflict and turnover intention (P < 0.01).

Table 2. The correlations among turnover intention, work-family conflict, and burnout.
3.6. Factors associated with turnover intention
Table 3 shows the final results of the HMR model for the turnover intention of primary medical staff. The final model explained a total variance of 31.3%. Demographic characteristics, work-family conflict, and burnout demonstrated 2.3%, 20.3%, and 8.8% of the incremental variance, respectively. According to Table 4, age was negatively correlated with turnover intention (P = 0.050). Meanwhile, higher monthly income was negatively correlated with turnover intention (P = 0.005).
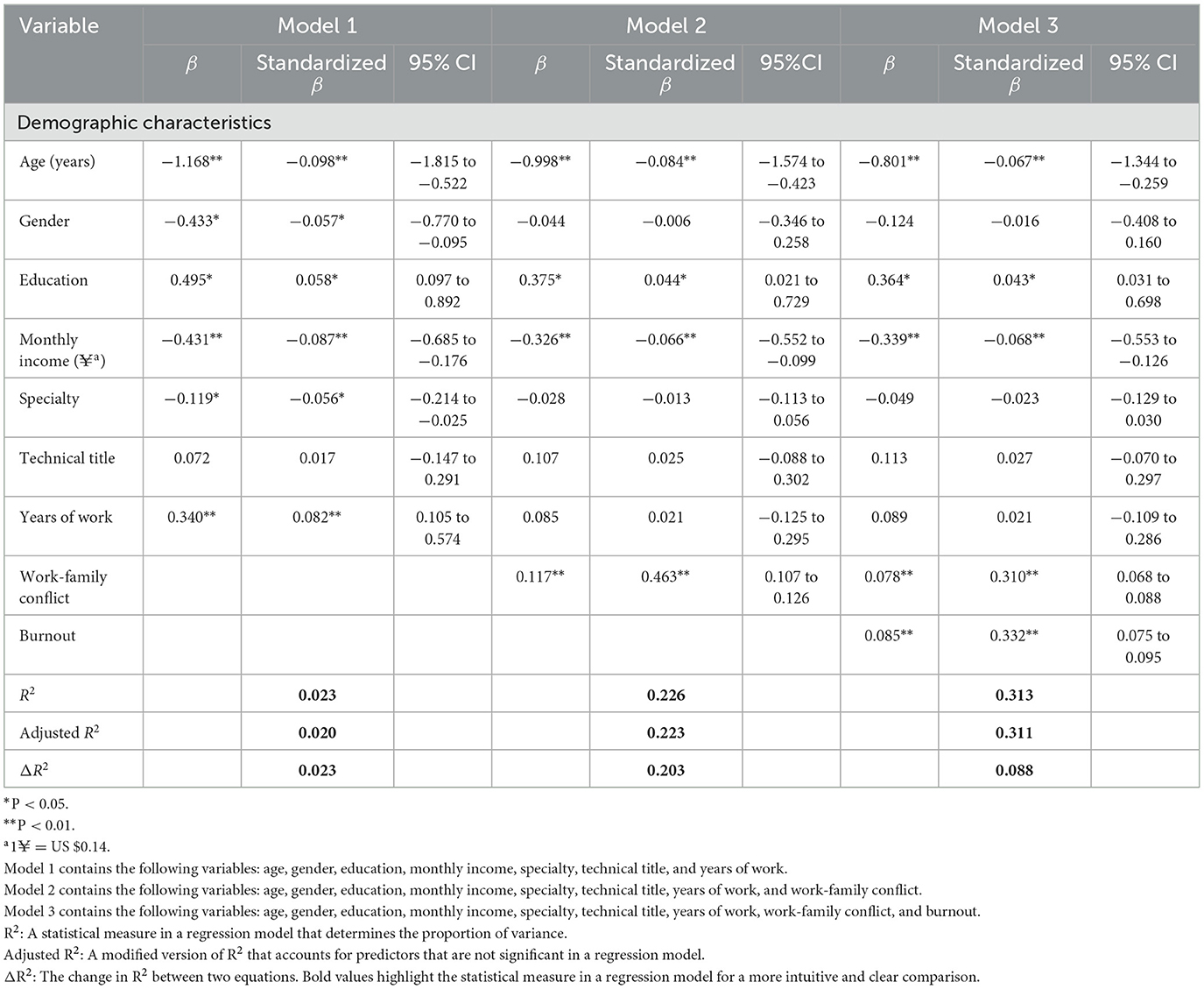
Table 3. The hierarchical multiple regression analysis of turnover intention of the primary medical staff.
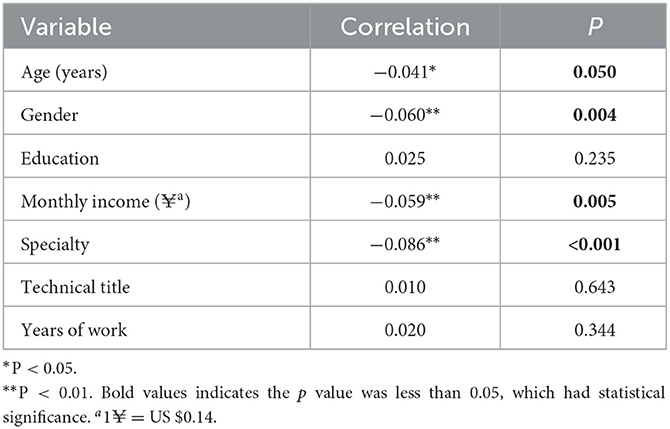
Table 4. The correlations among turnover intention with baseline characteristics.
3.7. Burnout as a mediator between work-family conflict and turnover intention
Table 5 shows the results of the SEM analysis. The path coefficients and standardized solutions of SEM are shown in Figure 1. Work-family conflict influenced turnover intention directly (c = 0.54, P < 0.001). Work-family conflict had a positive correlation with turnover intention (P < 0.001). The model fitting indices meet the requirements (χ2/df = 1.763 <5, GFI = 0.996 > 0.9, AGFI = 0.992 > 0.9, CFI = 0.999 > 0.9, TLI = 0.998 > 0.9, RMSEA = 0.018 <0.05; Figure 1). Burnout was significantly correlated with turnover intention (P < 0.001).

Table 5. The path coefficients of the mediation model.
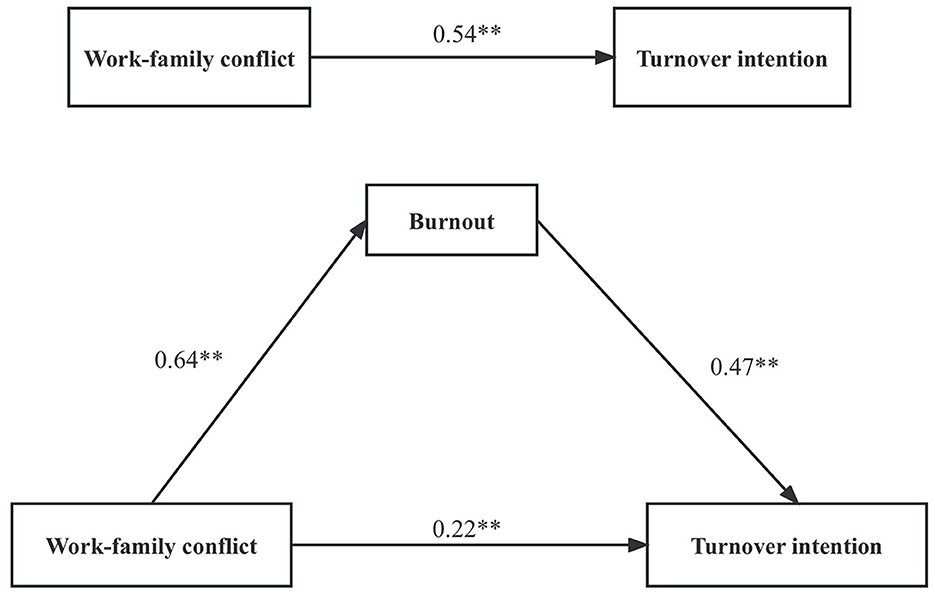
Figure 1. Standardized solution for the structural equation model of work-family conflict and turnover intention. Standardized solution for the structural equation model of burnout, work-family conflict, and turnover intention. **P < 0.01.
When burnout served as a mediator, the path coefficient between work-family conflict and turnover intention significantly decreased (c = 0.22, P < 0.001; Figure 1). After adding burnout mediation, the direct path coefficient of work-family conflict on turnover intention decreased or had no statistical significance, which also indicated the existence of a mediating effect. Burnout mediated the association between work-family conflict and turnover intention (a*b = 0.30, BCa 95% CI: 0.249–0.355, Percentile 95% CI: 0.260–0.360). The model showed a good fit across multiple indices: (χ2/df = 2.922 <5, GFI = 0.991 > 0.9, AGFI = 0.982 > 0.9, CFI = 0.995 > 0.9, TLI = 0.992 > 0.9, and RMSEA = 0.029 <0.05).
4. Discussion
This study aims to examine whether the primary medical staff's turnover intention is related to burnout and work-family conflict and further explore whether burnout plays a mediating role in work-family conflict and turnover intention. The study indicates significant correlations among turnover intention, work-family conflict, and burnout. In addition, this study observed that burnout, to some extent, mediates the relationship between work-family conflict and turnover intention, and the mediating effect is significant. Although there had been studies exploring the relationship between turnover intention, burnout, and work-family conflict, there was limited research literature on the three factors mentioned above among primary medical staff, and there was even more limited research on the role of burnout in the relationship between work-family conflict and turnover intention (41–45). Therefore, attention needs to be paid to work-family conflict, burnout, and turnover intention among primary medical staff (46–48).
This study found that work-family conflict was positively correlated with turnover intention, which is consistent with previous research studies (49, 50). Primary medical staff have a close relationship with the general public and fully understand the local people's family environment, living conditions, and disease history. To provide comprehensive and continuous health services to residents and ensure the health needs of urban and rural residents, they undertook special and complex work tasks, which are not only heavy workloads but also very trivial (51). The huge workload will inevitably lead to the physical and mental exhaustion of primary medical staff, and returning to the family in such a state will inevitably cause issues when handling family affairs. Through HMR analysis, this study found that work-family conflict is a risk factor for turnover intention, indicating that an increase in work-family conflict may lead to higher turnover intention. For married female doctors, factors such as work-family conflict and psychological empowerment were particularly relevant to turnover intention (52). Moreover, when studying the relevant factors of nurses' turnover intention, it was also observed that work-family conflict could predict turnover intention (53). Therefore, attention should be paid to the harm of work to individuals and families and the support of families for work. In addition, the perception of work-family conflict could hinder individuals from entering the field or increase the likelihood of providers leaving the field, exacerbating healthcare shortages (54, 55). Consequently, we should take proactive and effective measures to maintain a balance between work and family, thereby reducing turnover intention among primary medical staff.
Burnout is a long-term response to interpersonal stress and chronic emotions at work (34). When there is a conflict between work and family, and primary medical staff are unable to balance this conflict, it may lead to burnout in this job. Therefore, this study found a positive correlation between work-family conflict and burnout. Previous studies have found that reducing work-family conflict can alleviate the negative consequences of burnout, such as reduced anxiety symptoms, improved professional efficacy and emotional exhaustion, and reduced work pressure (56–58). In practice, reducing the work pressure on primary medical staff can effectively reduce burnout. Studies have found that work pressure affects burnout through work-family conflicts and anxiety symptoms among female nurses (22, 59). The above research indicates that work-family conflict can lead to a decline in an individual's emotional wellbeing, cognitive investment, and overall engagement in the workplace, thereby enhancing the turnover intention. Many scholars have noticed the negative impact of burnout, but few studies have focused on the role of burnout in the relationship between work-family conflict and turnover intention. Therefore, this study provides new inspiration for revealing how work-family conflict affects primary medical staff's careers and turnover intention.
In terms of outcomes, burnout is often associated with various forms of negative reactions and job withdrawal, including absenteeism, low organizational commitment, job dissatisfaction, intention to leave, and turnover (42, 60–63). Consistent with previous studies, this study observed a positive correlation between burnout and turnover intention (60, 61). Burnout often manifests as a negative and negligent approach to work, underestimating one's own work value, and being indifferent to others. Meanwhile, burnout can affect the entire work environment through social interactions at work (34). HMR analysis showed that burnout is a risk factor for high turnover intention. In practice, when there is a high level of work-family conflict, primary medical staff may experience burnout from their work. The work-family conflict itself can lead to a desire to resign, and long-term burnout can exacerbate the desire to resign. Therefore, burnout played a mediating role between work-family conflict and turnover intention. When burnout is considered a mediator, it can buffer the impact of work-family conflicts on turnover intention, indicating that it can effectively control and reduce the conflict between work and family and reduce the willingness to resign. The quality and stability of the staff of primary medical institutions are directly related to the quality and effectiveness of primary medical services and are also closely related to the success or failure of the medical service system reform. Under such high job standards, burnout was a serious factor that affected the work environment and could exacerbate the willingness of primary medical staff to resign (62–64).
Therefore, according to our research results, work-family conflict and burnout are key factors affecting the turnover intention of primary medical staff, and burnout is a mediator between work-family conflict and turnover intention. Thus, we should take effective measures to reduce work-family conflict, burnout, and turnover intention. By creating a positive and harmonious work environment, we can reduce burnout, improve the work satisfaction of primary medical staff, further reduce their willingness to resign, improve the internal stability of the organization, achieve a win-win situation for the organization and primary medical staff, and ultimately improve the quality of medical services.
5. Limitations
Several limitations should be acknowledged in this study. First, since the survey was conducted among primary medical staff in four cities in China–Xuzhou, Linyi, Huaibei, and Shangqiu—the generalizability to other populations is limited. Second, since this study was carried out from February 2023 to March 2023, the outcomes of this study may be limited by the COVID-19 pandemic and other unmeasured confounders. Third, selection bias cannot be ruled out because the survey was conducted online, and the participants were smartphone users only. Finally, this study did not differentiate among service items. Due to a lack of health workforce, respondents generally undertake multiple items. Future research may find differences when investigating this issue within certain primary medical staff profiles.
6. Conclusions
The research results confirm that work-family conflict and burnout have a direct positive impact on turnover intention, and burnout plays a mediating role between work-family conflict and turnover intention. Therefore, the study draws the following conclusion: first, work-family conflict is a risk factor for turnover intention, which can directly lead to turnover intention. Second, burnout is a risk factor for turnover intention and has a positive effect on turnover intention. Finally, work-family conflict, turnover intention, and burnout can form a mediated effect model, and burnout as a mediation variable can increase the impact of work-family conflict on turnover intention. This study has scientific and practical significance for reducing the talent turnover rate in the primary medical system. Primary medical institutions are the foundation of China's health system. Low employee retention rates may lead to a decline in the quality of diagnosis and treatment and the level of medical services, seriously affecting the stability and sustainability of primary healthcare and thus posing a potential threat to public health. In this context, effective psychological intervention measures should be taken to improve the psychological quality and stress resistance of primary medical staff so that they can better adapt to the high intensity and pressure of primary medical work, reduce work-family conflict and burnout, protect the psychological health of primary medical staff, reduce their willingness to resign, and improve medical quality and service level.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Ethics Committee of Xuzhou Medical University. Written informed consent for participation was obtained.
Author contributions
ZW and JX designed the study, conducted the literature review, and wrote the research protocol. JX and JY contributed to the acquisition and interpretation of data and drafted and revised the manuscript. JX, XH, and YN contributed to the revisions in depth for the manuscript. All authors contributed to the article and approved the final manuscript.
Funding
This work was supported by the Ministry of Humanities and Social Science Education Project (No. 19YJC630182), Medical Scientific Research Project of Jiangsu Commission of Health (No. Z2021020), Science and Technology Program Project of Xuzhou (No. KC20200), Scientific Research Foundation for Excellent Talents of Xuzhou Medical University (No. D2019004), and Jiangsu Training Program of Innovation and Entrepreneurship for Undergraduates (No. 202310313018Z).
Acknowledgments
All of the co-authors appreciate the cooperation of the participants and the generous contributions of the research assistants.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2023.1238315/full#supplementary-material
References
1. Li X, Krumholz HM, Yip W, Cheng KK, De Maeseneer J, Meng Q, et al. Quality of primary health care in China: challenges and recommendations. Lancet. (2020) 395:1802–12. doi: 10.1016/S0140-6736(20)30122-7
2. Xu Z, Ye Y, Wang Y, Qian Y, Pan J, Lu Y, et al. Primary care practitioners' barriers to and experience of COVID-19 epidemic control in China: a qualitative study. J Gen Intern Med. (2020) 35:3278–84. doi: 10.1007/s11606-020-06107-3
3. CPC Central Committee, State, Council,. The plan for “Healthy China 2030”. (2016). Available online at: https://www.gov.cn/xinwen/2016-10/25/content_5124174.htm (accessed July 24, 2023; in Chinese).
4. Hongoro C, McPake B. How to bridge the gap in human resources for health. Lancet. (2004) 364:1451–6. doi: 10.1016/S0140-6736(04)17229-2
5. Li X, Lu J, Hu S, Cheng KK, De Maeseneer J, Meng Q, et al. The primary healthcare system in China. Lancet. (2017) 390:2584–94. doi: 10.1016/S0140-6736(17)33109-4
6. Liu JX, Goryakin Y, Maeda A, Bruckner T, Scheffler R. Global health workforce labor market projections for 2030. Hum Resour Health. (2017) 15:11. doi: 10.1186/s12960-017-0187-2
7. Ran L, Chen X, Peng S, Zheng F, Tan X, Duan R. Job burnout and turnover intention among Chinese primary healthcare staff: the mediating effect of satisfaction. BMJ Open. (2020) 10:e036702. doi: 10.1136/bmjopen-2019-036702
8. Sang L, Liu H, Yan H, Rong J, Cheng J, Wang L, et al. Incentive preferences and its related factors among primary medical staff in Anhui Province, China: a cross-sectional study. Front Public Health. (2021) 9:778104. doi: 10.3389/fpubh.2021.778104
9. Chen G, Sang L, Rong J, Yan H, Liu H, Cheng J, et al. Current status and related factors of turnover intention of primary medical staff in Anhui Province, China: a cross-sectional study. Hum Resour Health. (2021) 19:23. doi: 10.1186/s12960-021-00563-6
10. Martin TN Jr. A contextual model of employee turnover intentions. Acad Manage J. (1979) 22:313–24. doi: 10.2307/255592
11. Zhang W, Meng H, Yang S, Liu D. The influence of professional identity, job satisfaction, and work engagement on turnover intention among township health inspectors in China. Int J Environ Res Public Health. (2018) 15:988. doi: 10.3390/ijerph15050988
12. Feng X, Wang Y, Jia P, Wang Y, Guan Z, Meng K. Associations between professional identity and turnover intent in prehospital emergency physicians: the mediating effect of burnout. Front Public Health. (2022) 10:1034925. doi: 10.3389/fpubh.2022.1034925
13. Blanco-Donoso LM, Moreno-Jiménez J, Hernández-Hurtado M, Cifri-Gavela JL, Jacobs S, Garrosa E. Daily work-family conflict and burnout to explain the leaving intentions and vitality levels of healthcare workers: interactive effects using an experience-sampling method. Int J Environ Res Public Health. (2021) 18:1932. doi: 10.3390/ijerph18041932
14. Shen Hsiao ST, Ma SC, Guo SL, Kao CC, Tsai JC, Chung MH, et al. The role of workplace bullying in the relationship between occupational burnout and turnover intentions of clinical nurses. Appl Nurs Res. (2022) 68:151483. doi: 10.1016/j.apnr.2021.151483
15. Mercado M, Wachter K, Schuster RC, Mathis CM, Johnson E, Davis OI, et al. A cross-sectional analysis of factors associated with stress, burnout and turnover intention among healthcare workers during the COVID-19 pandemic in the United States. Health Soc Care Community. (2022) 30:e2690–701. doi: 10.1111/hsc.13712
16. Chen Y, You Y, Shen Y, Du Z, Dai T. Village doctors' dilemma in China: a systematic evaluation of job burnout and turnover intention. Front Public Health. (2022) 10:970780. doi: 10.3389/fpubh.2022.970780
17. Qu G, Feng J, Lei Z, Li X, Sun Y, Ferrier A, et al. Analysis on the relationship between professional identity and turnover intention among general practitioners: the mediating role of job burnout. J Affect Disord. (2023) 339:725–31. doi: 10.1016/j.jad.2023.07.031
18. Kao AC, Jager AJ, Koenig BA, Moller AC, Tutty MA, Williams GC, et al. Physician perception of pay fairness and its association with work satisfaction, intent to leave practice, and personal health. J Gen Intern Med. (2018) 33:812–7. doi: 10.1007/s11606-017-4303-8
19. Halcomb E, Bird S, McInnes S, Ashley C, Huckel K. Exploring job satisfaction and turnover intentions among general practice nurses in an Australian primary health network. J Nurs Manag. (2021) 29:943–52. doi: 10.1111/jonm.13230
20. Stefanovska-Petkovska M, Stefanovska VV, Bojadjieva S, Bojadjiev MI. Psychological distress, burnout, job satisfaction and intention to quit among primary healthcare nurses. Health Serv Manage Res. (2021) 34:92–8. doi: 10.1177/0951484820971444
21. He R, Liu J, Zhang WH, Zhu B, Zhang N, Mao Y. Turnover intention among primary health workers in China: a systematic review and meta-analysis. BMJ Open. (2020) 10:e037117. doi: 10.1136/bmjopen-2020-037117
22. Yuan L, Li Y, Yan H, Xiao C, Liu D, Liu X, et al. Effects of work-family conflict and anxiety in the relationship between work-related stress and job burnout in chinese female nurses: a chained mediation modeling analysis. J Affect Disord. (2023) 324:309–16. doi: 10.1016/j.jad.2022.12.112
23. Lu Y, Hu XM, Huang XL, Zhuang XD, Guo P, Feng LF, et al. The relationship between job satisfaction, work stress, work-family conflict, and turnover intention among physicians in Guangdong, China: a cross-sectional study. BMJ Open. (2017) 7:e014894. doi: 10.1136/bmjopen-2016-014894
24. Li X, Chen X, Gao D. Influence of work-family conflict on turnover intention of primary and secondary school teachers: serial mediating role of psychological contract and job satisfaction. Front Psychiatry. (2022) 13:869344. doi: 10.3389/fpsyt.2022.869344
25. Abdou AH, Khalil AAF, Mahmoud HME, Elsaied MA, Elsaed AA. The impact of hospitality work environment on employees' turnover intentions during COVID-19 pandemic: the mediating role of work-family conflict. Front Psychol. (2022) 13:890418. doi: 10.3389/fpsyg.2022.890418
26. Allen TD, Herst DE, Bruck CS, Sutton M. Consequences associated with work-to-family conflict: a review and agenda for future research. J Occup Health Psychol. (2000) 5:278. doi: 10.1037/1076-8998.5.2.278
27. Belwal S, Belwal R. Work-Family conflict and women's turnover intention: mediating effects of organizational commitment. Appl Res Qual Life. (2023) 1–23. doi: 10.1007/s11482-023-10168-x
28. Gull N, Asghar M, Bashir M, Liu X, Xiong Z. Does a family-supportive supervisor reduce the effect of work-family conflict on emotional exhaustion and turnover intentions? A moderated mediation model. Int J Conf Manag. (2022) 34:253–72. doi: 10.1108/IJCMA-03-2022-0046
29. Ribeiro N, Gomes D, Oliveira AR, Dias Semedo AS. The impact of the work-family conflict on employee engagement, performance, and turnover intention. Int J Organ Anal. (2021) 31:533–49. doi: 10.1108/IJOA-02-2021-2646
30. Ozduran A, Saydam MB, Eluwole KK, Mertens EU. Work-family conflict, subjective wellbeing, burnout, and their effects on presenteeism. Serv Ind J. (2023) 1–27. doi: 10.1080/02642069.2023.2209507
31. Tsai HY. The role of employee assistance programs under COVID-19-induced work-family conflict: effects on service employees' work engagement and burnout. Scand J Psychol. (2023). doi: 10.1111/sjop.12922
32. Zhao L, Wu J, Ye B, Tarimo CS, Li Q, Ma M, et al. Work-family conflict and anxiety among nurses of the maternal and child health institutions: the mediating role of job satisfaction. Front Public Health. (2023) 11:1108384. doi: 10.3389/fpubh.2023.1108384
33. Ozkan AH. The effect of burnout and its dimensions on turnover intention among nurses: a meta-analytic review. J Nurs Manag. (2022) 30:660–9. doi: 10.1111/jonm.13525
34. Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. (2001) 52:397–422. doi: 10.1146/annurev.psych.52.1.397
35. Zhang X, Zhang W, Xue L, Xu Z, Tian Z, Wei C, et al. The influence of professional identity, job satisfaction, burnout on turnover intention among village public health service providers in China in the context of COVID-19: a cross-sectional study. Front Public Health. (2022) 10:925882. doi: 10.3389/fpubh.2022.925882
36. Back CY, Hyun DS, Jeung DY, Chang SJ. Mediating effects of burnout in the association between emotional labor and turnover intention in Korean clinical nurses. Saf Health Work. (2020) 11:88–96. doi: 10.1016/j.shaw.2020.01.002
37. Wang E, Hu H, Mao S, Liu H. Intrinsic motivation and turnover intention among geriatric nurses employed in nursing homes: the roles of job burnout and pay satisfaction. Contemp Nurse. (2019) 55:195–210. doi: 10.1080/10376178.2019.1641120
38. Leitao J, Pereira D, Goncalves A. Quality of work life and contribution to productivity: assessing the moderator effects of burnout syndrome. Int J Environ Res Public Health. (2021) 18:2425. doi: 10.3390/ijerph18052425
39. Mobley WH. Intermediate linkages in the relationship between job satisfaction and employee turnover. J Appl Psychol. (1977) 62:237. doi: 10.1037/0021-9010.62.2.237
40. Carlson DS, Kacmar KM, Williams LJ. Construction and initial validation of a multidimensional measure of work–family conflict. J Vocat Behav. (2000) 56:249–76. doi: 10.1006/jvbe.1999.1713
41. Giao HNK, Vuong BN, Huan DD, Tushar H, Quan TN. The effect of emotional intelligence on turnover intention and the moderating role of perceived organizational support: evidence from the banking industry of Vietnam. Sustainability. (2020) 12:1857. doi: 10.31219/osf.io/chjba
42. Chenevert D, Kilroy S, Johnson K, Fournier PL. The determinants of burnout and professional turnover intentions among Canadian physicians: application of the job demands-resources model. BMC Health Serv Res. (2021) 21:993. doi: 10.1186/s12913-021-06981-5
43. Mehmood S, Aziz A, Husin NS. Does work stress & workplace incivility influence employee turnover intentions? Mediating role of work-family conflict. Int J Soc Sci Econ Rev. (2023) 01–14. doi: 10.36923/ijsser.v5i2.177
44. Wilkinson S, Haar J. Smartdevice use in a COVID-19 world: exploring work–family conflict and turnover intentions. Asia Pac J Hum Resour. (2023). doi: 10.1111/1744-7941.12370
45. Iqbal J, Shagirbasha S, Madhan KP. Service with a sense of belonging: navigating work–family conflict and emotional irritation in the service efforts of health professionals. Int J Confl Manag. (2023) 34:838–61. doi: 10.1108/IJCMA-03-2023-0038
46. Cubitt LJ, Im YR, Scott CJ, Jeynes LC, Molyneux PD. Beyond PPE: a mixed qualitative-quantitative study capturing the wider issues affecting doctors' wellbeing during the COVID-19 pandemic. BMJ Open. (2021) 11:e050223. doi: 10.1136/bmjopen-2021-050223
47. Konlan KD, Asampong E, Dako-Gyeke P, Glozah FN. Burnout syndrome among healthcare workers during COVID-19 pandemic in Accra, Ghana. PLoS ONE. (2022) 17:e0268404. doi: 10.1371/journal.pone.0268404
48. Svantesson M, Durnell L, Hammarstrom E, Jarl G, Sandman L. Moral and exhausting distress working in the frontline of COVID-19: a Swedish survey during the first wave in four healthcare settings. BMJ Open. (2022) 12:e055726. doi: 10.1136/bmjopen-2021-055726
49. Mumu JR, Tahmid T, Azad MAK. Job Satisfaction and intention to quit: a bibliometric review of work-family conflict and research Agenda. Appl Nurs Res. (2021) 59:151334. doi: 10.1016/j.apnr.2020.151334
50. Labrague LJ, Ballad CA, Fronda DC. Predictors and outcomes of work-family conflict among nurses. Int Nurs Rev. (2021) 68:349–57. doi: 10.1111/inr.12642
51. Hamdan M, Hamra AA. Burnout among workers in emergency departments in Palestinian hospitals: prevalence and associated factors. BMC Health Serv Res. (2017) 17:407. doi: 10.1186/s12913-017-2356-3
52. Fahim U, Majeed MA, Asad MS, Tariq I. Work-family conflict, psychological empowerment, and turnover intentions among married female doctors. Bangladesh J Med Sci. (2021) 20:855–63. doi: 10.3329/bjms.v20i4.54145
53. Yildiz B, Yildiz H, Ayaz Arda O. Relationship between work-family conflict and turnover intention in nurses: a meta-analytic review. J Adv Nurs. (2021) 77:3317–30. doi: 10.1111/jan.14846
54. Mahgoub IM, Abdelrahman A, Abdallah TA, Mohamed Ahmed KAH, Omer MEA, Abdelrahman E, et al. Psychological effects of the COVID-19 pandemic: perceived stress, anxiety, work-family imbalance, and coping strategies among healthcare professionals in Khartoum State Hospitals, Sudan, 2021. Brain Behav. (2021) 11:e2318. doi: 10.1002/brb3.2318
55. Weinhold I, Gurtner S. Understanding shortages of sufficient health care in rural areas. Health Policy. (2014) 118:201–14. doi: 10.1016/j.healthpol.2014.07.018
56. Yeh TF, Chang YC, Hsu YH, Huang LL, Yang CC. Causes of nursing staff burnout: exploring the effects of emotional exhaustion, work-family conflict, and supervisor support. Jpn J Nurs Sci. (2021) 18:e12392. doi: 10.1111/jjns.12392
57. Kowalczuk K, Krajewska-Kulak E, Sobolewski M. The effect of subjective perception of work in relation to occupational and demographic factors on the mental health of polish nurses. Front Psychiatry. (2020) 11:591957. doi: 10.3389/fpsyt.2020.591957
58. Mousavi SM, Yazdanirad S, Naeini MJ, Khoshakhlagh A, Haghighat M. Determining the effect of selected mental factors on turnover intention through two modulators - stress and resilience over COVID-19 period. BMC Health Serv Res. (2023) 23:366. doi: 10.1186/s12913-023-09268-z
59. Modaresnezhad M, Andrews MC, Mesmer-Magnus J, Viswesvaran C, Deshpande S. Anxiety, job satisfaction, supervisor support and turnover intentions of mid-career nurses: a structural equation model analysis. J Nurs Manag. (2021) 29:931–42. doi: 10.1111/jonm.13229
60. Jiang S, Jiang C, Cheng Y. Working overtime in social work settings: associations with burnout, person-organization value congruence and turnover intentions among Chinese social workers. Hum Serv Organ Manag Leadersh Gov. (2022) 47:28–41. doi: 10.1080/23303131.2022.2121347
61. Jia CX, Li JC-m. Work-family conflict, burnout, and turnover intention among Chinese social workers: the moderating role of work support. J Soc Serv Res. (2021) 48:12–27. doi: 10.1080/01488376.2021.1942393
62. Jun J, Ojemeni MM, Kalamani R, Tong J, Crecelius ML. Relationship between nurse burnout, patient and organizational outcomes: systematic review. Int J Nurs Stud. (2021) 119:103933. doi: 10.1016/j.ijnurstu.2021.103933
63. Denning M, Goh ET, Tan B, Kanneganti A, Almonte M, Scott A, et al. Determinants of burnout and other aspects of psychological wellbeing in healthcare workers during the COVID-19 pandemic: a multinational cross-sectional study. PLoS ONE. (2021) 16:e0238666. doi: 10.1371/journal.pone.0238666
Keywords: work-family conflict, burnout, turnover intention, Huaihai Economic Zone, primary medical staff
Citation: Wen Z, Xu J, Yu J, Huang X and Ni Y (2023) Effects of work-family conflict on turnover intention among primary medical staff in Huaihai Economic Zone: a mediation model through burnout. Front. Psychiatry 14:1238315. doi: 10.3389/fpsyt.2023.1238315
Received: 11 June 2023; Accepted: 29 August 2023;
Published: 25 September 2023.
Edited by:
Thomas Wenzel, University of Vienna, AustriaReviewed by:
Heinrich Graf von Reventlow, Psychotherapeutische Praxis von Reventlow, GermanyXiaogang Lin, Guangdong University of Technology, China
Bin Cao, Jinan University, China
Copyright © 2023 Wen, Xu, Yu, Huang and Ni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zongliang Wen, d2VuemxAeHpobXUuZWR1LmNu
†These authors have contributed equally to this work and share first authorship