 Maria J. Marques1,2*
Maria J. Marques1,2* Bob Woods3†Hannah Jelley3Liselot Kerpershoek4
Bob Woods3†Hannah Jelley3Liselot Kerpershoek4 Louise Hopper5Kate Irving6Anja Bieber7Astrid Stephan7Anders Sköldunger8Britt‐Marie Sjölund8
Louise Hopper5Kate Irving6Anja Bieber7Astrid Stephan7Anders Sköldunger8Britt‐Marie Sjölund8 Geir Selbaek9Janne Røsvik9
Geir Selbaek9Janne Røsvik9 Orazio Zanetti10Daniel M. Portolani10
Orazio Zanetti10Daniel M. Portolani10 João Marôco11Niels Janssen4Eva Y.L. Tan4,12Marjolein de Vugt4
João Marôco11Niels Janssen4Eva Y.L. Tan4,12Marjolein de Vugt4 Frans Verhey4
Frans Verhey4 Manuel Gonçalves-Pereira2,13† on behalf of the Actifcare Consortium
Manuel Gonçalves-Pereira2,13† on behalf of the Actifcare Consortium- 1NOVA National School of Public Health, Public Health Research Centre, NOVA University Lisbon, Lisbon, Portugal
- 2Comprehensive Health Research Centre (CHRC), LA-REAL, NOVA University Lisbon, Lisbon, Portugal
- 3Dementia Services Development Centre (DSDC) Wales, School of Medical and Health Sciences, Bangor University, Bangor, United Kingdom
- 4Department of Psychiatry and Neuropsychology and Alzheimer Centre Limburg, School for Mental Health and Neurosciences, Maastricht University, Maastricht, Netherlands
- 5School of Psychology, Dublin City University, Dublin, Ireland
- 6School of Nursing, Psychotherapy and Community Health, Dublin City University, Dublin, Ireland
- 7Institute for Health and Nursing Science, Martin Luther University Halle-Wittenberg, Halle (Saale), Germany
- 8Division of Neurogeriatrics, Department of Neurobiology, Care Sciences and Society, Karolinska Institutet, Stockholm, Sweden
- 9Norwegian National Centre for Ageing and Health, Vestfold Hospital Trust, Tønsberg, Department of Geriatric Medicine, Oslo University Hospital, Faculty of Medicine, University of Oslo, Oslo, Norway
- 10IRCCS Istituto Centro San Giovanni di Dio Fatebenefratelli, Brescia, Italy
- 11William James Center for Research, Instituto Superior de Psicologia Aplicada – Instituto Universitário (ISPA-IU), Lisboa, Portugal
- 12Institute for Mental Health Care, GGzE, Eindhoven, Netherlands
- 13Faculdade de Ciências Médicas, NOVA Medical School, Universidade NOVA de Lisboa, Lisbon, Portugal
Objective: The quality of the relationship between persons with dementia and family carers influences health and quality-of-life outcomes. Little is known regarding those at higher risk of experiencing a decline in relationship quality, who could potentially benefit the most from interventions. We aimed to identify these risk profiles and explore the underlying factors.
Methods: We applied a latent profile analysis to relationship quality data from a 1-year follow-up of 350 dyads of persons with dementia and their informal carers from the Actifcare cohort in eight European countries. Assessments included sociodemographic, clinical, functional, psychosocial and quality-of-life measures. Relationship quality was assessed with the Positive Affect Index. A discriminant analysis explored factors influencing the risk profiles.
Results: There were two relationship quality profiles among persons with dementia (gradually decreasing, 74.0%; low but improving, 26%) and two among carers (steadily poor, 57.7%; consistently positive, 42.3%). The ‘gradually decreasing’ profile (persons with dementia) was related to their levels of dependence and unmet needs, along with carers’ social distress and negative feelings, lower baseline RQ and sense of coherence. The ‘steadily poor’ profile (carers) was influenced by their social distress and negative feelings, lower sense of coherence and perceived social support. These two predominant profiles showed significant decreases in quality-of-life over one year.
Conclusions: Specific profiles of persons with dementia and their carers are at risk of worse relationship quality trajectories. By considering modifiable related factors (e.g., carers’ stress), our findings can help develop tailored, effective interventions.
Introduction
The presence and nature of close relationships may influence the onset and prognosis of several chronic health conditions, being robust predictors of quality and length of life (1). Among such health conditions, dementia has a heavy ‘burden of disease’ and impact on families and informal carers (2). Worldwide, around 55 million people live with dementia and this number is expected to reach 152.8 million in 2050 (3). Overall, families remain the cornerstone of care for older people, but they need support to persevere in their role as long as possible. It would be helpful if social and health care professionals were able to reliably identify people at risk of poor outcomes based on relationship factors.
In dementia, previous research provided support for the association of the relationship quality between the informal carer (i.e. family, friends) and the person with dementia, and a range of outcomes, including challenging behaviour (e.g., agitation, aggression, apathy), cognitive and functional decline, quality-of-life and institutionalisation (4–7). Carers who report poorer relationship quality are at greater risk of subjective burden and psychological distress, including anxiety and depression (8–10).
Most studies measure relationship quality at a single point, missing temporal changes. The few longitudinal studies of factors associated with poor relationship quality pathways highlighted the role of carers’ stress, depression and anxiety, and neuropsychiatric symptoms and self-reported quality-of-life of persons with dementia (11–13). Overall, these studies relied on relatively small convenience samples (12, 13), excluded the perspectives of persons with dementia (11), focused on young-onset dementia (13), or only examined spousal carers (11, 12). Moreover, they did not analyse profiles at higher risk of poor-quality relationships.
Meanwhile, several reviews called for more robust evidence regarding the role and course of relation quality (14). Particularly, studies on its association with neuropsychiatric symptoms are inconclusive, with findings ranging from no significant association (15) to identifying relationship quality as a target of intervention for less severe neuropsychiatric symptoms (8, 16).
Optimising aspects of the person with dementia-carer relationship could potentially improve outcomes in dementia (17), probably in more effective ways if we could selectively target those persons with dementia and carers at risk of worse relationship quality trajectories over time. To our knowledge, no study has explored the existence of profiles (subpopulations of individuals) differentiated according to this important variable and its influencing factors. To improve our ability to support these families, this evidence gap must be addressed.
In our previous cross-sectional study from a large European cohort (18) carer stress, expressed as anger and frustration, was the only factor associated with both person with dementia and carer perceptions of relationship quality, which frequently diverge. A stronger sense of coherence (SOC) in carers, i.e. a dispositional orientation toward a positive life (19), and being a spouse/partner (versus an adult child carer) were also related to their better perception of the relationship (18). Subsequently, we analysed the same Actifcare cohort regarding the trajectories of relationship quality among persons with dementia and found that their ratings did not decline significantly. In contrast, carer ratings showed a significant decline over time (20). Notably, our longitudinal and comprehensive data would allow us to delve deeper into the existence of relationship quality profiles and examine a broader range of influencing factors than those previously considered; these include demographics and type of relationship but also variables amenable to intervention, such as psychosocial unmet needs, neuropsychiatric symptoms, along with carers’ SOC, stress, depression and anxiety. Additionally, it would be interesting to analyse differences in quality-of-life between these profiles. As relationship quality is a key component of quality-of-life, increasing our understanding of the former, may provide us with a better picture of the many facets of the latter. Altogether, enlarging this evidence-base might shape early interventions targeting relationship quality-based risk profiles.
Therefore, in this paper we aim to: 1) identify distinct profiles based on relationship quality within a large cohort of persons with dementia and their informal carers followed over one year; 2) explore the factors influencing each profile; 3) further characterize the profiles, based on sociodemographic data and quality-of-life measures.
Methods
Participants
The data presented here are drawn from the 1-year prospective cohort Actifcare (ACcess to TImely Formal Care) EU-JPND project, a multimethod study in eight European countries: Germany, Ireland, Italy, Netherlands, Norway, Portugal, Sweden and United Kingdom. Actifcare comprised at least 50 dyads of community-dwellers with mild-to-moderate stages of dementia and their family carers per country, 451 in total.
Participants were recruited from various settings, including general practices, memory clinics and Alzheimer’s Associations. Persons with dementia were diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders (DSM‐IV) criteria, staged mild to moderate using the Clinical Dementia Rating - CDR (21), with Mini Mental State Examination (MMSE) score of 24 or lower (22). Exclusion criteria included alcohol‐related dementia and receiving significant personal care from formal services (e.g., home care, day centres). For each person, their primary informal carer was selected. The full project protocol is detailed elsewhere (23).
Procedures
Participants were assessed on entry (451 dyads), and again at approximately 6 (398 dyads) and 12 months (368 dyads). This paper reports on the 350 dyads that completed all three observations on an index of relationship quality, the Positive Affect Index (PAI) (Online Appendix A).
Participants were seen at home unless they preferred otherwise. Assessments were conducted separately with the person with dementia and their carer but, when necessary, part would take place conjointly (mainly if the person with dementia felt more secure in the presence of their loved one). Typically, each visit lasted up to two hours and was split into two sessions, if needed, to minimise evaluation overload. Trained staff conducted the comprehensive assessments.
Ethical approval was granted in each of the eight countries and all procedures followed the Helsinki Declaration of the World Medical Association. Persons with dementia and their carers provided informed written consent according to national regulations (23).
Measures
Participants completed questionnaires on sociodemographic information (e.g., gender, age, education) and clinical-functional measures (23). Those selected for this study are outlined below.
The PAI (24) assessed current relationship quality, and was rated separately by persons with dementia and carers. Ratings of persons with dementia were used to define their profiles, and carers’ ratings to define their own’s. The PAI comprises five items, closeness, communication, similar views, shared activities, and generally getting along. Responses are rated on a 6-point scale from 1 (not well) to 6 (extremely well), with a total sum score from 5 to 30 (higher scores reflecting better RQ). This scale has been used with persons with dementia (12), showing good internal consistency (Cronbach α = 0.81) and reasonable test-retest reliability (r = .66) (25). In the present study, Cronbach’s αs were 0.82 (people with dementia) and 0.79 (carers).
Measures for persons with dementia included: CDR (21), MMSE (22), Neuropsychiatric Inventory Questionnaire (NPI-Q), with symptom count and separate scores for severity and carer distress (26), Instrumental Activities of Daily Living (IADL) and Physical Self-Maintenance Scale (PSMS) (27). The NPI-Q, IADL and PSMS were completed from carers’ reports. The Quality-of-Life-Alzheimer’s Disease (QOL-AD) (28) and the DEMQOL-U were used as disease-specific quality-of-life scales for use in mild to moderate dementia. Both were interviewer administered and their proxy-report versions were also used (29–31).
Carers’ assessments included the Hospital and Anxiety Depression Scale (HADS) (32) and the Relative Stress Scale (RSS) (33). In addition to RSS total scores, 3 sub-scores were calculated (emotional distress, social distress, negative feelings toward the person with dementia) (34). Carers’ QoL, perceived social network and SOC were measured with the CarerQol (35), the Lubben Social Network Scale (LSNS-6) (36), and the 13-item Orientation to Life Questionnaire, commonly known as the SOC scale (19). The Camberwell Assessment of Need (CANE) assessed 24 areas of need, covering biopsychosocial domains, with two additional items on carers’ own needs: information and psychological distress (37).
Statistical analysis
LPA is a person-centred analytic tool that focuses on similarities and differences among people instead of relations among variables. It assesses whether the probability of belonging to a specific profile can be explained by individual characteristics, such as risk or protective factors (38). LPA utilized the intercept (initial relationship quality level) and slope (change rate) data from both persons with dementia and carers. Demographics and other covariates (e.g., ADL/IADL function, perceived social support) were employed to differentiate the profiles. To identify distinct profiles based on relationship quality, we performed a LPA in the slope and intercept data for both person with dementia and carers samples using the mclust R package (39). Variables with less than 10% missing data were imputed using Full Information Maximum Likelihood (FIML) methods.
Fit was judged from the χ2 goodness of fit statistic, Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC). ‘The smaller the better’ rule was used to choose the best LPA model.
Linear discriminant analysis of profiles obtained for person with dementia and carers was performed with the package MASS (40) for the R Statistical System.
A stepwise forward selection procedure was used to identify the statistically significant predictors of the inclusion of people with dementia and carers into specific profiles for a p-level entry of 0.2 using the package klaR (41) for the R Statistical System.
To examine whether sociodemographic variables and quality-of-life were associated with the profiles we conducted independent‐sample t-tests and repeated measures ANOVA. The significance threshold was set at 0.05.
We used the Statistical Package for the Social Sciences (SPSS) for Windows version 26 and R Statistical System (v. 4.0) (42).
Results
The characteristics of the total Actifcare cohort (451 dyads of persons with dementia and their carers) were previously reported (18, 43).
The demographic and clinical characteristics of participants who completed three PAI assessments (n = 350 dyads) are summarised in Table 1. This sample differed significantly from the remaining Actifcare dyads in persons with dementia’s lower age, dementia severity, level of neuropsychiatric symptoms and dependence, and their carers’ lower level of depressive symptoms and stress (Table 1). Attrition was due to the fact that participants were no longer willing to collaborate, stating exhaustion, health issues, moving abroad, institutionalisation or death (Online Appendix A).
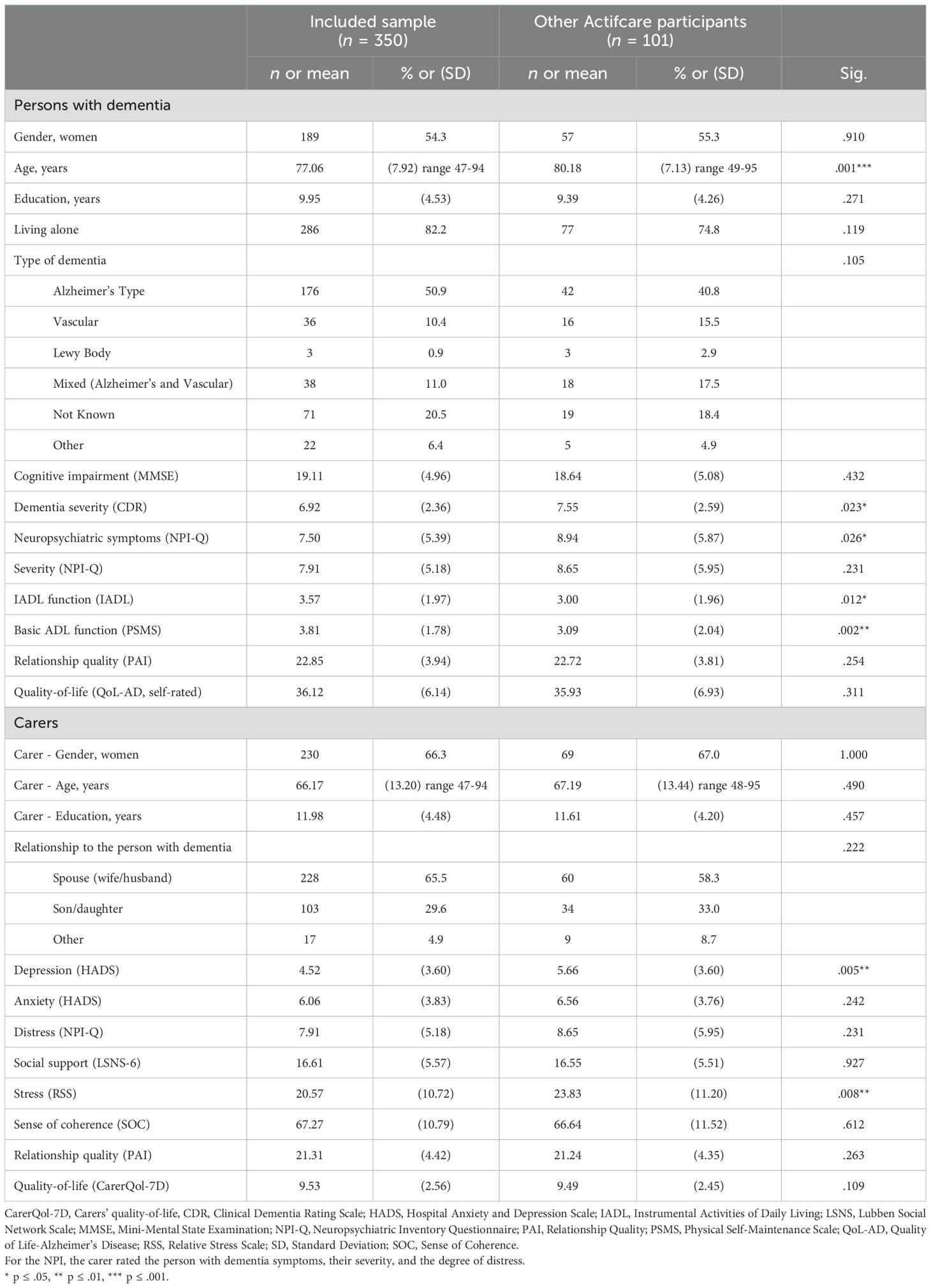
Table 1. Baseline characteristics and summary of measures for those included and excluded from the analyses for both persons with dementia and carers.
Relationship quality profiles among persons with dementia and carers
Mean PAI scores, as rated by people with dementia, did not decline, considering the baseline (T0), 6 months (T1) and 12 months (T2) follow-up assessments (22.91; 22.52; 22.62). However, the differences in PAI assessments by carers across the three time points were are all statistically significant F(2 646) = 36.494, p = .001, with a decline over time (21.32; 20.75; 19.79).
No severe deviations from normality were observed in any PAI score (baseline, 6- and 12-month follow-up) (|Sk|<3 and |ku|<7) and thus Maximum Likelihood methods were appropriate for LPA.
The application of LPA resulted in two distinct profiles of relationship quality among persons with dementia (Online Appendix B). Profile 1 (n = 91, 26%) started with lower PAI and improved (‘low but improving’). The larger profile 2 (n = 259, 74%) started with higher PAI and decreased over time (‘gradually decreasing’) (Online Appendix C). Regarding carers, the best fit in Bayesian Information Criterion (BIC) yielded two profiles with clearly distinguishable relationship quality longitudinal dynamics (Online Appendix D). Profile 1 (‘consistently positive’) represented 42.3% (n = 148) of the carers. Profile 2 (‘steadily poor’) represented 57.7% (n = 202) (Online Appendix E).
Factors influencing profile membership
Mean ratings for potential baseline predictors of persons with dementia and carers’ profile membership, at baseline and one-year follow-up, are displayed in Tables 2, 3.
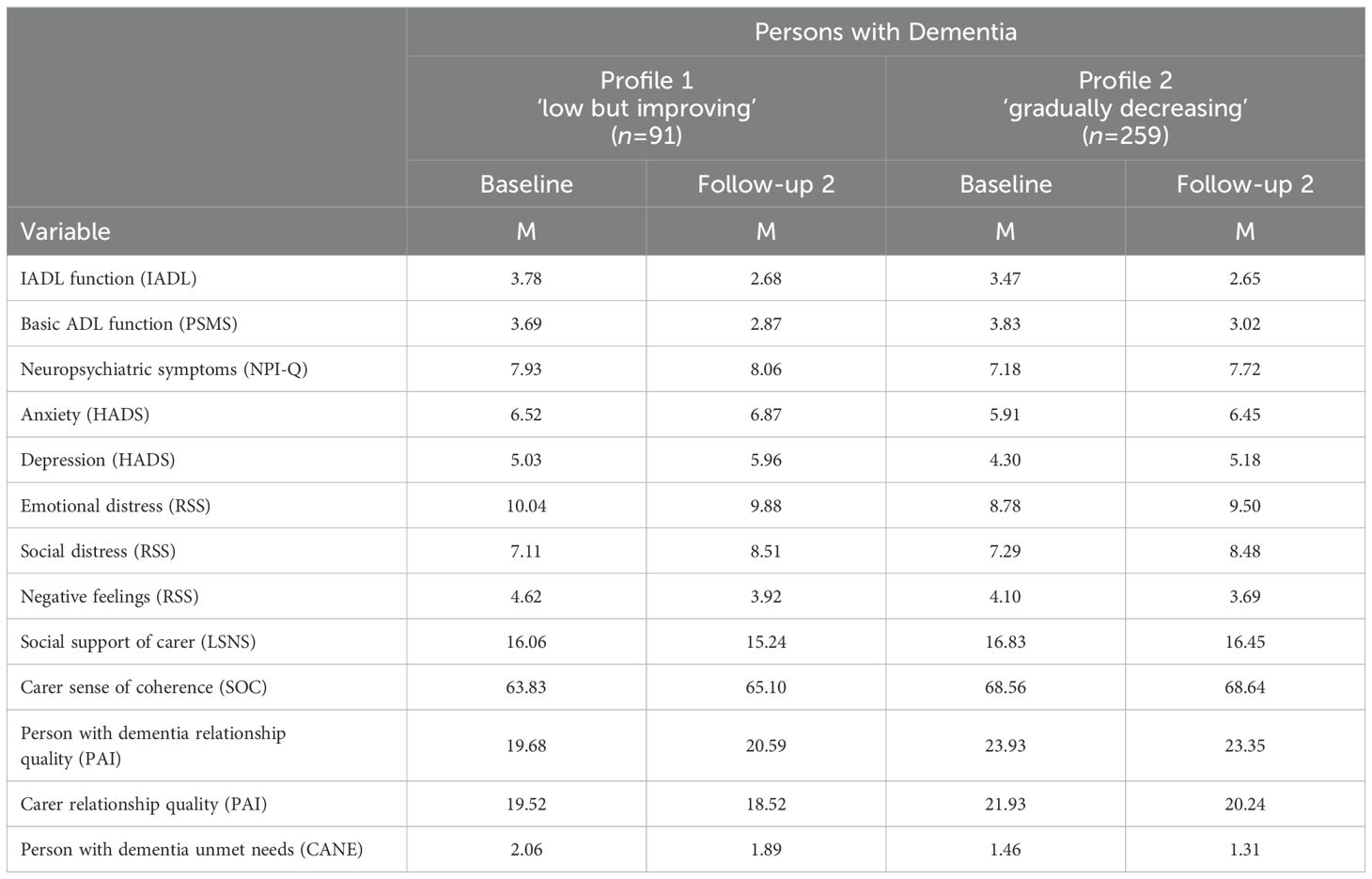
Table 2. Mean ratings for profiles among persons with dementia at baseline and follow-up.
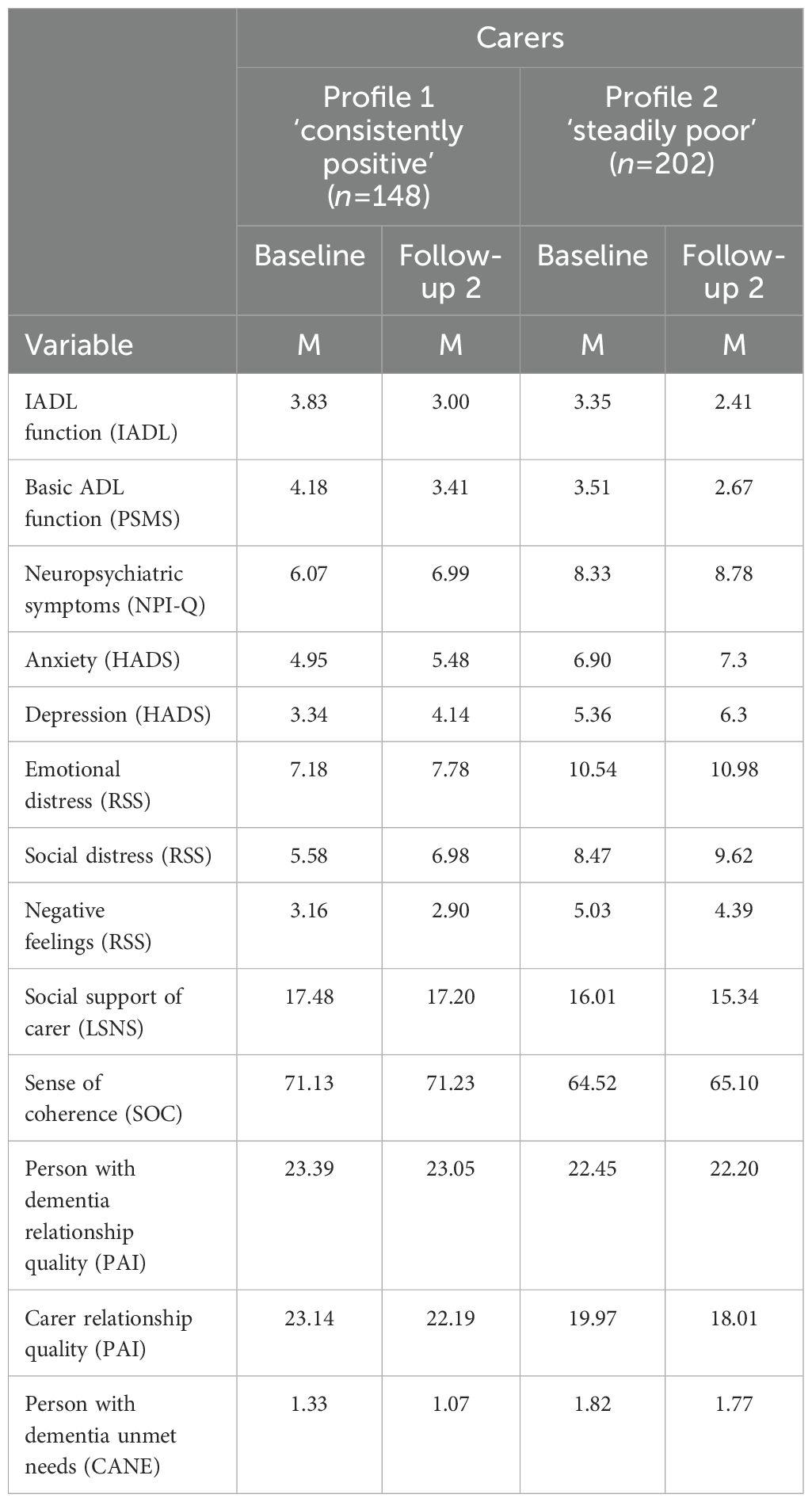
Table 3. Mean ratings for profiles among carers at baseline and follow-up 2.
Persons with dementia’ profiles differed across basic ADL function (PSMS) at baseline, with the largest (standardized) regression coefficient (λ=0.302) followed by IADL function (λ=-0.261) and carers’ psychological distress unmet needs (λ=-0.209), with higher level of ADL function and lower levels of carer distress in profile 1 (‘consistently positive’) (Online Appendix F). Using a stepwise forward selection method, significant predictors of profile membership among persons with dementia, included RQ carer perspective F(1, 342) = 22.799; p<.001, IADL function F(1, 342) = 13.313; p<.001, basic ADL function F(1, 342) = 11.006; p<.001, carers’ SOC F(1, 342) = 8.914; p<.001, social distress F(1, 342) = 7.737; p<.001 and negative feelings F(1, 342) = 22.799; p<.001 and persons with dementia’ unmet needs F(1, 342) = 6.594; p<.001 (Table 4).
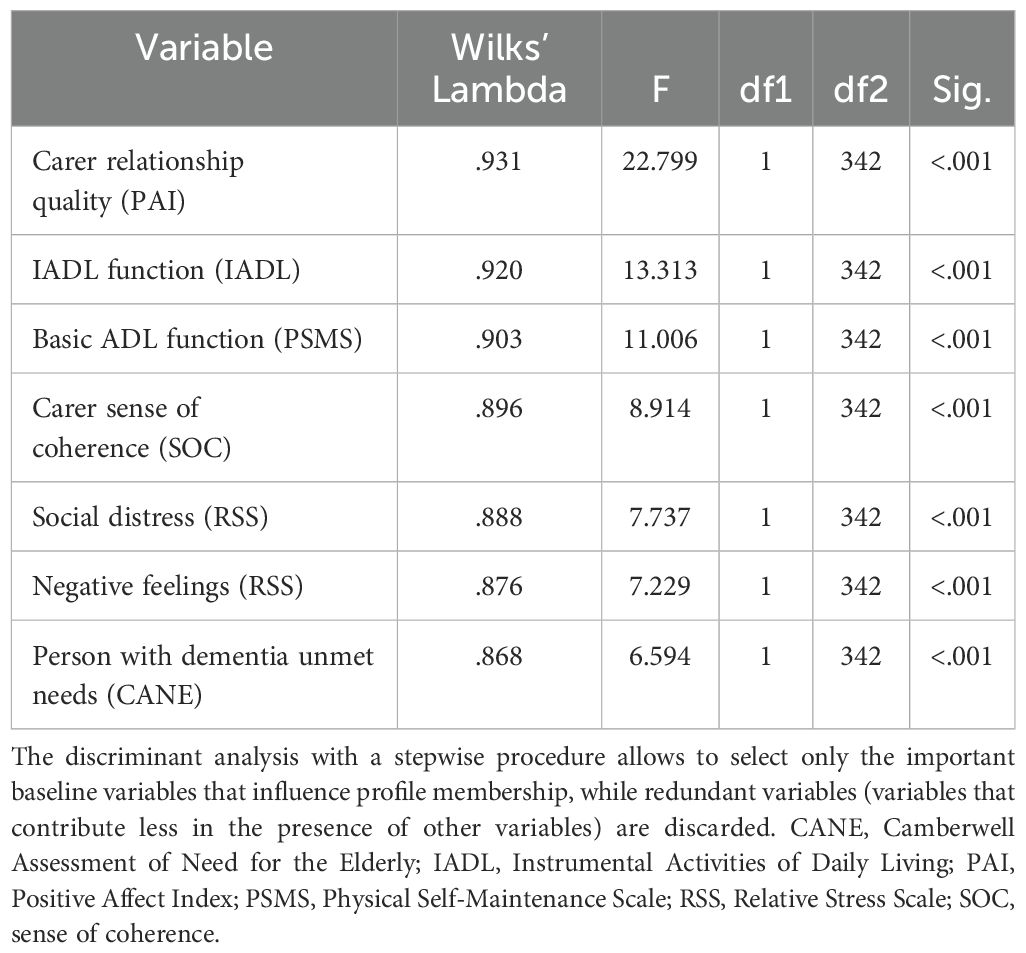
Table 4. Summary of the stepwise regression analysis for the baseline variables influencing profile membership among people with dementia.
Regarding carers, variables contributing the most to discriminate the ‘consistently positive’ and ‘steadily poor’ profiles included carer depression (λ=0.294), type of relationship (e.g., spouse/partner, adult child) (λ=0.291), and RSS ‘negative feelings’(λ=-0.209) (Online Appendix G). Stepwise discriminant analysis identified the most important baseline predictors of carers’ profiles, including RSS ‘negative feelings’ F(1, 345) = 36.899; p<.001, ‘social distress’ F(1, 345) = 6.594; p<.001, SOC F(1, 345) = 24.986; p<.001, and perceived social support F(1, 345) = 18.147; p<.001 (Table 5).
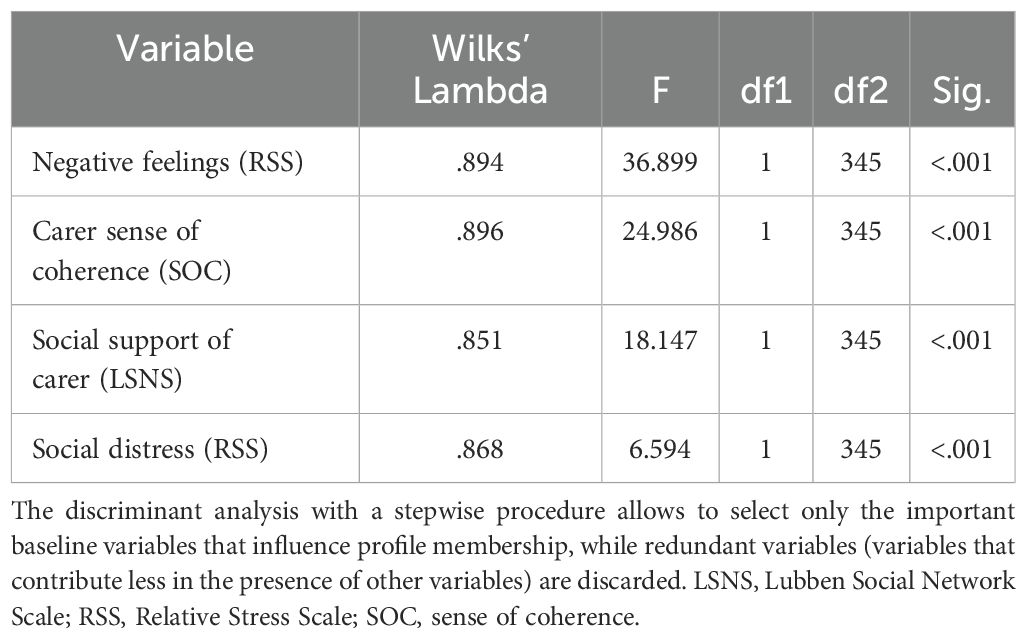
Table 5. Summary of the stepwise regression analysis for the baseline variables influencing profile membership among carers.
Differences between profiles on sociodemographic and quality-of-life variables
Finally, we further characterised the profiles based on baseline sociodemographic characteristics (age, gender, and education) and QoL measures (QoL-AD, DEMQoL-U and CarerQol) across T0, T1 and T2.
No significant differences were found for age, gender, or education within any profile.
When analysing each ‘persons with dementia’ profile for quality-of-life measures, we found significant differences on QoL-AD (self-rated) scores in the largest profile (74%) ‘Relationship quality gradually decreasing’ F(2, 170) = 5.771, p = .004, between T0 and T2 (p = .003), with a higher mean at T0 (36.72 vs 35.62). In the same profile, there were differences regarding QoL-AD (carer’s proxy ratings) scores F(2, 188) = 6.473, p = .002, between T0 and T2 (p = .002) and T1 and T2 (p = .025).
Analysing the other ‘persons with dementia’ profile (‘low but improving’) there were significant differences on DEMQoL-U (proxy) F(2, 51) = 3.975, p = .025, between T0 and T2 (p = .019), with a higher mean at T2. The two profiles differed on the DEMQoL-U proxy (p = .001) and CarerQoL (p = .003) baseline scores.
When analysing each ‘carer’ profile, we found significant differences on QoL-AD (carer’s proxy ratings) scores in the profile ‘steadily poor’ F(2, 164) = 6.121, p = .003. From T0 to T2 (p = .003), the average score decreased (36.17 vs 34.91). The same applied to QoL-AD (self-rated) scores F(2, 185) = 4.261, p = .016, with a lower mean at T2 (30.71 vs 29.58).
The two ‘carer’ profiles (‘steadily poor’, ‘low but improving’) differed on baseline QoL-AD (self-rated) (p = .001), DEMQoL proxy (p = .012) and CarerQoL (p = .012) scores.
Discussion
We identified distinct profiles based on relationship quality, in a large cohort of European community-dwellers with dementia and their family carers, followed over one year. Using a novel statistical approach, our analyses focused on identifying subgroups at risk of poor related outcomes. There were two main profiles, both characterized by relationship quality decline over time: the ‘gradually decreasing’ profile (representing 74% of persons with dementia) and the ‘steadily poor’ profile (corresponding to 58% of their carers). Carer’s stress and SOC emerged as common factors explaining profiles of both persons with dementia and carers at higher risk of decline. We also documented expectable links between carer relationship quality and quality-of-life in dementia. Overall, our objectives were met: first, to identify distinct profiles based on relationship quality; second, to explore the factors influencing each profile; and third, to further characterise the profiles using demographic data and quality-of-life measures.
Profiles of persons with dementia
Using LPA proved useful to identify specific profiles that showed distinct PAI changes over time (‘gradually decreasing’; ‘slow but improving’). The larger profile of persons with dementia (74%), whose relationship quality declined over time (‘gradually decreasing’), was determined by a mix of carer and person with dementia characteristics. These included, from the carer’s perspective, lower PAI, lower SOC, and higher stress, together with reduced function and more unmet needs of the person with dementia.
Regarding the influencing factors, relationship quality (as rated by the carer) added to the prediction of persons with dementia profiles. Since relationships are based on reciprocity, it is reasonable to assume that the person with dementia’s perspective is influenced by the carer’s attitudes (‘partner effect’) (44). This finding supports the value of considering both perspectives within the dyad.
Present findings extend the evidence by supporting lower carer’s SOC as an indicator to help identifying subgroups of persons with dementia at risk. Previously, we had shown how carer’s SOC may protect relationships (18).
In line with previous research, carers’ distress emerged as one of the strongest predictors of relationship quality profiles in persons with dementia. The at-risk profile seemed especially related to carer’s social distress (i.e. feelings of being limited in terms of social life) and negative feelings towards the care-receiver (e.g., anger, frustration), suggesting responsiveness from the person with dementia to the family’s emotional climate (7).
Reduced functional abilities of the person with dementia also influenced inclusion in the vulnerable profile. Perhaps less functional abilities make them more prone to assess relationships negatively, creating imbalances through increased dependence of carers. Alternatively, feeling overwhelmed contributed to carers’ negative appraisals of persons with dementia’ function, as IADL and PSMS are assessed by them.
To our best knowledge, this is the first study to underline links between unmet needs and lower relationship quality in dementia, which was not surprising. Indeed, the most reported unmet need in the Actifcare cohort was ‘company’ (43), a salient unmet need in community-dwellers with dementia (45).
Finally, we characterised the profiles using demographics and quality-of-life measures. Demographics were not associated with any probability of belonging to a specific profile. The profile with a decrease of PAI (‘gradually decreasing’) was also marked by a decline in quality-of-life during the follow-up (QoL-AD and DEMQoL-U scores). Our characterisation of the two profiles of persons with dementia, based on self-report, disease-specific quality-of-life measures (QoL-AD and DEMQoL), enabled us to hear the care-receiver’s perspective first-hand and highlighted the value of focusing on relationship factors to better understand quality-of-life in dementia. Preserving relationship quality proved to be an important key aspect of quality-of-life. As reported for the QoL-AD, persons with mild-to-moderate dementia can reliably appraise their relationships, and their perspective on this specific topic contributes to their self-reported quality-of-life overall (46, 47). This finding contributes to filling gaps in knowledge on how relationship factors impact on persons with dementia quality-of-life, as requested by a recent review (14).
Profiles of carers
The two carer profiles were ‘steadily poor’ and ‘consistently positive’ relationship quality. The larger profile (‘steadily poor’) was determined by carer characteristics only (RSS ‘negative feelings’ and ‘social distress’, SOC and perceived social support). Using LPA enabled us to identify another profile of carers that maintained positive PAI scores (‘consistently positive’) despite adversity and facilitated our exploration of factors contributing to more positive experiences.
Regarding the factors influencing the profiles, and in line with our previous results (18), carers’ negative feelings (e.g., anger, frustration) were significantly associated with lower PAI. Regarding ‘social distress’, one possible interpretation is that, as dementia progresses, the person with dementia becomes more dependent on their carer; with time, this often leads to restrictions on the carer’s social life, increasing feelings of isolation and loss of control.
As expected, their SOC was among the determinants of carers’ relationship quality profiles. A higher SOC predisposes carers to positively reframe or compensate for negative life events, potentially impacting on how relationships are appraised. We also cannot exclude a bidirectional interaction between SOC and relationship quality: poor quality could arguably contribute to lower SOC self-appraisals at a given point.
Also as expected, lower levels of perceived support were associated with more negative relationship quality assessments over time.
The more in-depth comparison of carers’ profiles based on demographics and quality-of-life measures helped us to complete the circle. There were no significant differences found among carer profiles for age, gender and education. Finally, just as relationship quality has a major influence on the quality-of-life of the person with dementia, it is also crucial to the carer’s (48), providing insight on the role of relationships as a component of quality-of-life in dementia. When analysing the ‘steadily poor’ carer’s profile, we found a deterioration of QoL-AD (both on carer’s ratings and care-receiver’s self-reports) over one year. This interestingly underlines that person with dementia quality-of-life self-reports also impact on carer’s relationship quality perspective. Moreover, there were differences between the two carer profiles regarding DEMQoL and CarerQol, as between the two profiles of persons with dementia. In the case of carer profiles, there were also differences on the QoL-AD (person with dementia self-rated). Consistent with reports that higher quality-of-life of the person with dementia was associated with higher relationship quality (both following carers’ perspectives) (13), our study further unveils some links between self-reported quality-of-life of the person with dementia and the carer’s relationship perspective.
Strengths and limitations
The strength of the study lies in the fact that it is one of the very first to use a longitudinal design with repeated assessments to analyse relationship quality, rather than aiming only at a snapshot as in most previous cross-sectional studies. Our work goes beyond the previous literature by considering both persons with dementia and their family carers’ perspectives in a large cohort from different countries in Europe. Moreover, we used a novel statistical approach (LPA), appropriate to identify the profiles.
There are also limitations to acknowledge. First, the sample may not be representative, limiting generalizability. Attrition inevitably led to some degree of selection bias, with those lost to follow-up likely to be older and more severely impaired, and their carers reporting higher levels of depression symptoms and stress. Second, a longer follow-up than our 12 month-period could have resulted in different profiles and identified influencing factors. Finally, we did not consider the influence of a variety of potentially important factors, including the subtype of dementia (although we did consider neuropsychiatric symptoms), the receipt of formal care (in fact, an exclusion criterion at baseline), or time assisting with activities of daily living (analysed in our baseline study of relationship quality (18), but excluded here to achieve a model that strikes a balance between fit and complexity. Relationship quality prior to the onset of dementia obviously influences current relationship appraisals but its retrospective assessment would be heavily prone to bias in this research context.
Conclusions
There is no one-size-fits-all solution to predict how relationship quality will change over time. However, specific factors like carers’ stress and social support are amenable to intervention and may help to identify profiles of persons with dementia or their family carers at risk of worse trajectories. These are the individuals that could benefit the most from timely psychosocial interventions which, by considering relationship quality, turn out to be intrinsically systemic. Our findings show that addressing aspects of the relationship quality may potentially improve health and quality-of-life outcomes in dementia.
Data availability statement
The datasets presented in this article are not readily available due to privacy restrictions on personal data. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
Ethical approval was granted in each of the eight countries: Medische-ethische toetsingscommissie (NL), Wales Research Ethics Committee, Bangor (UK), Ethics committee of the Medical Faculty, Martin Luther University Halle-Wittenberg (DE), Regional committee for medical and health research ethics, South-East B (NO), the Regional Ethics Review Board (SW), Dublin City University Research Ethics Committee (IE), Ethics Committee of the Nova Medical School, Ethics Committee of Centro Hospitalar de Lisboa Ocidental, Ethics Committee of ARSLVT, Ethics Committee of ARS Alentejo, Comissão Nacional de Protecção de Dados (PT), Comitato Etico, IRCCS San Giovanni di Dio-Fatebenefratelli (IT). All participating NHS sites in the UK received permission to perform the study. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MM: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. BW: Methodology, Writing – original draft, Writing – review & editing. HJ: Writing – original draft, Writing – review & editing. LK: Writing – original draft, Writing – review & editing. LH: Writing – original draft, Writing – review & editing. KI: Writing – original draft, Writing – review & editing. AB: Writing – original draft, Writing – review & editing. AsS: Writing – original draft, Writing – review & editing. AnS: Writing – original draft, Writing – review & editing. B-MS: Writing – original draft, Writing – review & editing. GS: Writing – original draft, Writing – review & editing. JR: Writing – original draft, Writing – review & editing. OZ: Writing – original draft, Writing – review & editing. DP: Writing – original draft, Writing – review & editing. JM: Writing – original draft, Writing – review & editing. NJ: Writing – original draft, Writing – review & editing. ET: Writing – original draft, Writing – review & editing. MV: Writing – original draft, Writing – review & editing. FV: Writing – original draft, Writing – review & editing. MG-P: Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The Actifcare project in Portugal had support from Fundação para a Ciência e a Tecnologia (FCT-JPND-HC-0001/2012), under the JPND initiative (JPND/2013/2). MM was supported by POPH/ESF funding (FCT-PD/BD/128011/2016). The present publication was funded by Fundação Ciência e Tecnologia, IP national support through CHRC (UIDP/04923/2020).
Acknowledgments
This is an EU Joint Programme - Neurodegenerative Disease Research (JPND) initiative (http://www.jpnd.eu). The Actifcare Consortium partners are Maastricht University (NL), Martin-Luther University Halle-Wittenberg (DE), Bangor University (UK), Nottingham University (UK), Karolinska Institutet (SE), Oslo University Hospital (NO), Dublin City University (IE), IRCCS Istituto Centro San Giovanni di Dio Fatebenefratelli, Brescia (IT), Nova Medical School/Faculdade de Ciências Médicas, Universidade Nova de Lisboa (PT) (FCT - JPND-HC/0001/2012).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2024.1394665/full#supplementary-material
References
1. Holt-Lunstad J, Robles TF, Sbarra DA. Advancing social connection as a public health priority in the United States. Am Psychol. (2017) 72:517–30. doi: 10.1037/amp0000103
2. Prince M, Wimo A, Maëlenn G, Ali G-C, Wu Y-T, Matthew P. World Alzheimer report 2015: the global impact of dementia - an analysis of prevalence, incidence, cost and trends. London: Alzheimer’s Disease International (2015). doi: 10.1111/j.0963-7214.2004.00293.x.
3. Nichols E, Steinmetz JD, Vollset SE, Fukutaki K, Chalek J, Abd-Allah F, et al. Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: an analysis for the Global Burden of Disease Study 2019. Lancet Public Health. (2022) 7:e105–25. doi: 10.1016/S2468-2667(21)00249-8/ATTACHMENT/60E03FD1-38B2-4B40-A91D-9AFDDA22B45E/MMC1.PDF
4. Fauth E, Hess K, Piercy K, Norton M, Corcoran C, Rabins P, et al. Caregivers’ relationship closeness with the person with dementia predicts both positive and negative outcomes for carers’ physical health and psychological well-being. Aging Ment Health. (2012) 16:699–711. doi: 10.1080/13607863.2012.678482
5. Norton MC, Piercy KW, Rabins PV, Green RC, Breitner JCS, Ostbye T, et al. Caregiver-recipient closeness and symptom progression in alzheimer disease. The cache county dementia progression study. Journals Gerontology Ser B: psychol Sci Soc Sci. (2009) 64B:560–8. doi: 10.1093/geronb/gbp052
6. Spitznagel MB, Tremont G, Davis JD, Foster SM. Psychosocial predictors of dementia carer desire to institutionalize: carer, care recipient, and family relationship factors. J Geriatric Psychiatry Neurol. (2006) 19:16–20. doi: 10.1177/0891988705284713
7. Woods R, Nelis S, Martyr A, Roberts J, Whitaker C, Markova I, et al. What contributes to a good quality-of-life in early dementia? Awareness and the QoL-AD: a cross-sectional study. Health Qual Life Outcomes. (2014) 12. doi: 10.1186/1477-7525-12-94
8. Mahoney R, Regan C, Katona C, Livingston G. Anxiety and depression in family caregivers of people with alzheimer disease: the LASER-AD study. Am J Geriatric Psychiatry. (2005) 13:795–801. doi: 10.1176/appi.ajgp.13.9.795
9. Springate BA, Tremont G. Dimensions of caregiver burden in dementia: impact of demographic, mood, and care recipient variables. Am J Geriatric Psychiatry. (2014) 22:294–300. doi: 10.1016/j.jagp.2012.09.006
10. Steadman PL, Tremont G, Davis JD. Premorbid relationship satisfaction and carer burden in dementia carers. J Geriatric Psychiatry Neurol. (2007) 20:115–9. doi: 10.1177/0891988706298624
11. Bruinsma J, Peetoom K, Millenaar J, Köhler S, Bakker C, Koopmans R, et al. The quality of the relationship perceived by spouses of people with young-onset dementia. Int Psychogeriatrics. (2020), 1–10. doi: 10.1017/S1041610220000332
12. Clare L, Nelis SM, Whitaker CJ, Martyr A, Markova IS, Roth I, et al. Marital relationship quality in early-stage dementia: perspectives from people with dementia and their spouses. Alzheimer Dis Associated Disord. (2012) 26:148–58. doi: 10.1097/WAD.0B013E318221BA23
13. Spector A, Orrell M, Charlesworth G, Marston L. Factors influencing the person-carer relationship in people with anxiety and dementia. Aging Ment Health. (2016) 20:1055–62. doi: 10.1080/13607863.2015.1063104
14. Edwards HB, Ijaz S, Whiting PF, Leach V, Richards A, Cullum SJ, et al. Quality-of-family relationships and outcomes of dementia: a systematic review. BMJ Open. (2018) 8:e015538. doi: 10.1136/bmjopen-2016-015538
15. Feast A, Orrell M, Russell I, Charlesworth G, Moniz-Cook E. The contribution of carer psychosocial factors to distress associated with behavioural and psychological symptoms in dementia. Int J Geriatric Psychiatry. (2017) 32:76–85. doi: 10.1002/gps.4447
16. Vernon E, Cooley B, Rozum W, Rattinger G, Behrens S, Matyi J, et al. Caregiver-care recipient relationship closeness is associated with neuropsychiatric symptoms in dementia. Am J Geriatric Psychiatry. (2019) 27:349–59. doi: 10.1016/J.JAGP.2018.11.010
17. Cheng S, Au A, Losada A, Thompson L, Gallagher-Thompson D. Psychological interventions for dementia caregivers: what we have achieved, what we have learned. Curr Psychiatry Rep. (2019) 21. doi: 10.1007/S11920-019-1045-9
18. Marques MJ, Woods B, Hopper L, Jelley H, Irving K, Kerpershoek L, et al. Relationship quality and sense of coherence in dementia: Results of a European cohort study. Int J Geriatric Psychiatry. (2019) 34:745–55. doi: 10.1002/gps.5082
19. Antonovsky A. The structure and properties of the sense of coherence scale. Soc Sci Med (1982). (1993) 36:725–33. doi: 10.1016/0277-9536(93)90033-Z
20. Marques MJ, Tan EYL, Woods B, Jelley H, Kerpershoek L, Hopper L, et al. Trajectories of relationship quality in dementia: a longitudinal study in eight European countries. Aging Ment Health. (2022) 26:2307–15. doi: 10.1080/13607863.2021.1969641
21. Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology. (1993) 43:2412–4. doi: 10.1212/WNL.43.11.2412-a
22. Folstein MF, Folstein SE, McHugh PR. Mini-mental state: A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
23. Kerpershoek L, de Vugt M, Wolfs C, Jelley H, Orrel M, Woods B, et al. Access to timely formal dementia care in Europe: protocol of the Actifcare (ACcess to Timely Formal Care) study. BMC Health Serv Res. (2016) 16:423. doi: 10.1186/s12913-016-1672-3
24. Bengston V, Schrader S. Parent child relationship. In: Mangen D, Peterson W, editors. Social Roles and Social Participation: Research Instruments in Social Gerontology, vol. 2. Minneapolis: University of Minnesota Press (1982). p. 115–85.
25. Woods B. Relationship quality and quality-of-life in dementia. In: 19th International Congress of Gerontology (2009). 19th International Congress of Gerontology.
26. Kaufer DI, Cummings JL, Ketchel P, Smith V, MacMillan A, Shelley T, et al. Validation of the NPI-Q, a brief clinical form of the Neuropsychiatric Inventory. J Neuropsychiatry Clin Neurosci. (2000) 12:233–9. doi: 10.1176/jnp.12.2.233
27. Lawton MP, Brody EM. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist. (1969) 9:179–86. doi: 10.1093/geront/9.3_Part_1.179
28. Logsdon RG, Gibbons LE, McCurry SM, Teri L. Quality-of-life in Alzheimer’s disease: Patient and carer reports. J Ment Health Aging. (1999) 5:21–32.
29. Handels RLH, Sköldunger A, Bieber A, Edwards RT, Gonçalves-Pereira M, Hopper L, et al. Quality-of-life, care resource use, and costs of dementia in 8 European countries in a cross-Sectional cohort of the actifcare study. J Alzheimer’s Dis. (2018) 66:1027–40. doi: 10.3233/JAD-180275
30. Mulhern B, Rowen D, Brazier J, Smith S, Romeo R, Tait R, et al. Development of DEMQOL-U and DEMQOL-PROXY-U: Generation of preference-based indices from DEMQOL and DEMQOL-PROXY for use in economic evaluation. Health Technol Assess. (2013) 17:1–160. doi: 10.3310/hta17050
31. Rowen D, Mulhern B, Banerjee S, Van Hout B, Young TA, Knapp M, et al. Estimating preference-based single index measures for dementia using DEMQOL and DEMQOL-proxy. Value Health. (2012) 15:346–56. doi: 10.1016/j.jval.2011.10.016
32. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatrica Scandinavica. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
33. Greene JG, Smith R, Gardiner M, Timbury GC. Measuring behavioural disturbance of elderly demented patients in the community and its effects on relatives: a factor analytic study. Age Ageing. (1982) 11:121–6. doi: 10.1093/ageing/11.2.121
34. Ulstein I, Bruun Wyller T, Engedal K. The relative stress scale, a useful instrument to identify various aspects of carer burden in dementia? Int J Geriatric Psychiatry. (2007) 22:61–7. doi: 10.1002/gps.1654
35. Brouwer WBF, van Exel NJA, van Gorp B, Redekop WK. The CarerQol instrument: a new instrument to measure care-related quality-of-life of informal carers for use in economic evaluations. Qual Life Research : Int J Qual Life Aspects Treatment Care Rehabil. (2006) 15:1005–21. doi: 10.1007/s11136-005-5994-6
36. Lubben J, Gironda M. Social support networks. In: Comprehensive Geriatric Assessment. New York: McGraw-Hill (2000). p. 121–37.
37. Reynolds T, Thornicroft G, Abas M, Woods B, Hoe J, Leese M, et al. Camberwell assessment of need for the elderly (CANE). Br J Psychiatry. (2000) 176:444–52. doi: 10.1192/bjp.176.5.444
38. Muthén B, Muthén LK. Integrating person-centered and variable-centered analyses: growth mixture modeling with latent trajectory classes. Alcoholism Clin Exp Res. (2000) 24:882–91. http://www.ncbi.nlm.nih.gov/pubmed/10888079.
39. Scrucca L, Fop M, Murphy TB, Raftery AE. mclust 5: clustering, classification and density estimation using gaussian finite mixture models. R J. (2016) 8:289–317. doi: 10.32614/RJ-2016-021
40. Venables WN, Ripley BD. Modern Applied Statistics with S. New York: Springer (2002). doi: 10.1007/978-0-387-21706-2
41. Weihs C, Ligges U, Luebke K, Raabe N. klaR analyzing german business cycles. In: Data Analysis and Decision Support. Berlin: Springer-Verlag (2005). p. 335–43. doi: 10.1007/3-540-28397-8_36
42. R Core Team. R: A language and environment for statistical computing. Vienna: R Foundation for Statistical Computing (2019). Available at: https://www.r-project.org/.
43. Kerpershoek L, de Vugt M, Wolfs C, Woods B, Jelley H, Orrell M, et al. Needs and quality-of-life of people with middle-stage dementia and their family carers from the European Actifcare study. When informal care alone may not suffice. Aging Ment Health. (2017) 22:1–6. doi: 10.1080/13607863.2017.1390732
45. Miranda-Castillo C, Woods B, Galboda K, Oomman S, Olojugba C, Orrell M. Unmet needs, quality-of-life and support networks of people with dementia living at home. Health Qual Life Outcomes. (2010) 8:132. doi: 10.1186/1477-7525-8-132
46. Clare L, Woods RT, Nelis SM, Martyr A, Marková IS, Roth I, et al. Trajectories of quality-of-life in early-stage dementia: individual variations and predictors of change. Int J Geriatric Psychiatry. (2014) 29:616–23. doi: 10.1002/gps.4044
47. Mortazavizadeh Z, Maercker A, Roth T, Savaskan E, Forstmeier S. Quality of the caregiving relationship and quality-of-life in mild Alzheimer’s dementia. Psychogeriatrics. (2020) 20:568–77. doi: 10.1111/psyg.12546
Keywords: Alzheimer’s disease, close relationships, family care, informal care, latent profile analysis, longitudinal study, social support, quality-of-life
Citation: Marques MJ, Woods B, Jelley H, Kerpershoek L, Hopper L, Irving K, Bieber A, Stephan A, Sköldunger A, Sjölund B, Selbaek G, Røsvik J, Zanetti O, Portolani DM, Marôco J, Janssen N, Tan EYL, de Vugt M, Verhey F and Gonçalves-Pereira M (2024) Addressing relationship quality of people with dementia and their family carers: which profiles require most support? Front. Psychiatry 15:1394665. doi: 10.3389/fpsyt.2024.1394665
Received: 01 March 2024; Accepted: 08 August 2024;
Published: 11 September 2024.
Edited by:
Gaelle Eve Doucet, Boys Town National Research Hospital, United StatesReviewed by:
Jacqueline Claus, Erasmus Medical Center, NetherlandsIsabelle Van Der Velpen, National Institute of Mental Health (NIH), United States
Copyright © 2024 Marques, Woods, Jelley, Kerpershoek, Hopper, Irving, Bieber, Stephan, Sköldunger, Sjölund, Selbaek, Røsvik, Zanetti, Portolani, Marôco, Janssen, Tan, de Vugt, Verhey and Gonçalves-Pereira. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria J. Marques, bWoubWFycXVlc0BlbnNwLnVubC5wdA==
†These authors have contributed equally to this work