 Benjamin Calvet1,2,3*†
Benjamin Calvet1,2,3*† Jean-Luc Vallejo4Yves Plu5Isabelle Soulat4Alexandra Foucher3
Jean-Luc Vallejo4Yves Plu5Isabelle Soulat4Alexandra Foucher3 Jean-Pierre Clément1,2,3†
Jean-Pierre Clément1,2,3†- 1Institut National de la Santé Et de la Recherche Médicale (INSERM) U1094, Institut de Recherche pour le Développement (IRD) UMR270, Univ. Limoges, CHU Limoges, EpiMaCT - Epidemiology of chronic diseases in tropical zone, Institute of Epidemiology and Tropical Neurology, OmegaHealth, Limoges, France
- 2Pôle Universitaire de Psychiatrie de l’Adulte, de la Personne âgée et d’Addictologie, centre hospitalier Esquirol, Limoges, France
- 3Centre mémoire de ressources et de recherche du Limousin, centre hospitalier Esquirol, Limoges, France
- 4Institut Limousin de Formation et de Gestalt-Thérapie, Limoges, France
- 5Institut Gestalt+, Rennes, France
Background: Gestalt therapy (GT) is a dynamic, integrative, embodied approach that addresses human existence as a fundamentally relational modality, in which the experience of the self is situated in a dynamic organism–environment field. Assessments of GT are scarce, often avoided, and generally qualitative. The Therapy Gestalt TCI (THEGETCI) study aimed to show that the modifiable character dimensions of the 125-item Temperament and Character Inventory (TCI-125), as well as other personality temperament dimensions and emotional measures, change after a GT program.
Methods: A psychotherapeutic program consisting of 33 one-hour sessions (minimum of 12 sessions), spaced over several months, was offered to 319 subjects with mood and/or anxiety disorders. The TCI-125, Hospital Anxiety and Depression Scale, and visual analog scale (VAS) were used to assess subjective psychological states before and after the program. All TCI-125 scores were adjusted for potential confounding factors.
Results: Statistically significant differences between the initial and final mean scores were observed for anxiety (t = 16.46; p < 0.0001), depression (t = 11.24; p < 0.0001), and harm avoidance (t = 8.82; p < 0.0001), and global psychological distress assessed by VAS (t = 18.7; p < 0.0001) (all showing decreased scores). Significant increases were observed for the three maturity dimensions: Self-Directedness (t = −11.49; p < 0.0001), Cooperativeness (t = −2.77; p < 0.006), and Self-Transcendence (t = −4.52; p < 0.0001).
Conclusion: The THEGETCI study is one of the first to demonstrate the effectiveness of specific, current GT strategies on personality dimensions using rigorous evaluation methods. Further research is needed to confirm these results and to better identify both the expected benefits for practitioners and the problem profiles most likely to benefit from GT.
1 Introduction
Gestalt therapy (GT) is a humanistic, experiential, integrative, and embodied approach that considers contact with one’s environment as the “simplest primary reality” for any living organism’s survival and growth (1). GT approaches human existence from a fundamentally relational modality, in which the experience of the self is situated in a dynamic organism–environment field that encompasses both the individual and their environment (1–6). The experience of contact (7) occurs in a space–time referred to as the contact boundary, where the relationship between the individual and their world takes shape (Gestalt) moment by moment. It is in this space–time, at the limit between the two—”here and now”—that the way a person functions, their self, can be observed, and psychological events unfold: “Our thoughts, our actions, our behaviors, our emotions, are different ways of experiencing the encounter with these border events (8)”. The self is defined as “the system of contacts, which always integrates perceptual and proprioceptive functions, motor and muscular functions, and organic needs”. It is the agent that responds to variations in dominant organic needs and the pressure of stimuli from the environment (1). The self is our specific way of being in the world at each moment and the agent of contact with the environment, which allows creative adjustment (9). GT focuses on the forms and disturbances, as well as inhibitions and interruptions, of the contact process that occurs during the session. GT is a relational therapy oriented toward processes (10). Gestalt therapists, through their attitude of presence, awareness, and responsibility, invite the patients to focus on the present—their thoughts, emotions, and movements—”here and now”. They help patients become aware of what is emerging in their current experience, rather than turning to specific, painful experiences from the past that have not been assimilated or anticipating a threatening or hostile future. Finally, they invite the clients to clarify their needs, goals, and values and to express them through role-playing or creative exercises (11). Presence, awareness, and responsibility are key characteristics of GT, which aims to restore the patients’ capacity for creative adjustment in their current environment and awaken new possibilities for growth and understanding (12). GT focuses on self-awareness, acceptance, personal responsibility, authenticity, and personal growth (13). Wholeness is a cornerstone of GT, which considers the field or context in which the client lives (14). Patients change only when they fully accept themselves and become who they are at present (15).
Studies on GT usually prefer narrative inquiries with data analysis involving the reduction, synthesis, and reconfiguration of clients’ stories (16). In their research, Kelly and Howie identified several emerging themes located in a temporal framework of experiences evolving through stages and as a circle (17). Cycles of experiences are micro- and macroscopic, and small and large, such as stories within stories (18). According to Clarkson (13), themes in the Gestalt experience cycle include fertile voids, sensation, awareness mobilization, action, contact, satisfaction, and withdrawal. A hallmark of GT is awareness of feelings, thoughts, actions, perceptions, and beliefs; awakening one’s awareness is its main purpose (19). Clients block or cloud their awareness through defects in projection, retroflection, confluence, and introjection. For therapists, the most important healing presence they can provide is caring, support, empathy, non-judgment, careful listening, seeing and hearing, a selective sense of humor, attention to meaning, and a lack of expectations about outcomes (20).
All exist in a unitary function, which is the total organism–environment process. Paying attention to any one of these components is appropriate for promoting personality integration (1). Even if GT presents the self as a function of three structures—namely, the id, ego, and personality (21)—which are the major stages of creative adjustment (7), assessing personality, particularly personality changes, is a way to consider progress in the psychotherapy process in outpatients with no major psychopathologies.
Assessments of GT are scarce, largely qualitative (22, 23), and often concerned with fidelity, adherence to therapists (24, 25), and aesthetic sensibility (2, 26–28). Only the Clinical Outcomes in Routine Evaluation–Outcome Measure (CORE-OM) has been used to measure clients’ levels of distress on a session-by-session basis, but it is more oriented toward comparing the effectiveness of counselors (29, 30).
Any psychotherapeutic process should be able to mobilize emotions, affect, and character; the Gestalt approach focuses on these objectives (31). This study aimed to assess the efficacy of GT and the usefulness of Cloninger’s Temperament and Character Inventory (TCI) as a robust tool for doing so. For Perls and Goodman, personality is a kind of “verbal copy of the self”: “[ … ] it is the hypothesis of what one is and which serves as a basis from which one would explain one’s own behavior if asked” (1). To adhere to this definition, we opted for a dimensional and lexical assessment method of personality and its evolution: the Cloninger’s TCI.
In 1987, Cloninger (32) postulated a unified biopsychosocial theory of personality that included four predominantly genetically determined temperamental dimensions and three predominantly developmentally determined character dimensions. Temperament dimensions are related to the immediate response of humans to basic environmental stimuli (danger, punishment, novelty, and reward). Character, by contrast, is described as a response to different aspects of one’s own identity or self-experience (individual differences in goal values and self-consciousness, and ego-syntonic emotions such as shame, guilt, and empathy). The aspects of the self correspond to how the self is identified as an autonomous individual, an integral part of society, and an integral part of all things (the universe). The three character dimensions are considered to be influenced by learning processes throughout the lifespan, including psychotherapeutic processes.
Within temperament, Novelty Seeking (NS) is thought to be related to the behavioral activation system (in response to novelty and signals of reward or relief from punishment). NS reflects the tendency to seek strong new sensations from unknown stimuli and reward signals. Harm Avoidance (HA) is related to the behavioral inhibition system (in response to punishment or non-reward signals) and corresponds to the tendency to respond to aversive stimuli with inhibition to avoid suffering, punishment, and frustration. Reward Dependence (RD) is related to the behavioral maintenance system (behaviors maintained without reinforcement) and is associated with being sentimental, warm, dedicated, and attached—versus withdrawn and cold. RD reflects the tendency to respond consistently to reward signals and to avoid punishment. The Persistence (P) dimension is related to perseverance—the ability to continue a behavior without considering its consequences in the absence of immediate reinforcement, despite fatigue and frustration.
Self-Directedness (SD) refers to individuals’ ability to control, regulate, and adapt their behavior in accordance with chosen goals and values. SD corresponds to individual maturity—the ability to adapt behavior based on values and personal orientations—which encompasses will to succeed, personal effectiveness, and self-esteem. Cooperativeness (C) relates to the tendency toward social tolerance, empathy, compassion, and helpfulness. C reflects social maturity, characterized by interpersonal relationships and social consciousness, as well as the acceptance of others. Self-Transcendence (ST) reflects spiritual maturity, designating spiritual realization and the ability for meditation and non-materialist thinking that allows the individual to represent the universe (33).
Cloninger et al. proposed several versions of the TCI (34). The version used in this study was a short form consisting of 125 self-reported true/false (yes/no) items (TCI-125). As in the original inventory, the TCI-125 temperament section includes 20 items for NS, 20 for HA, 15 for RD, and 5 for P; the character section includes 25 items for SD, 25 for C, and 15 for ST. Each dimension has one to five facets (see Table 1); thus, 25 facets were also measured as subscales of the seven main TCI scores.
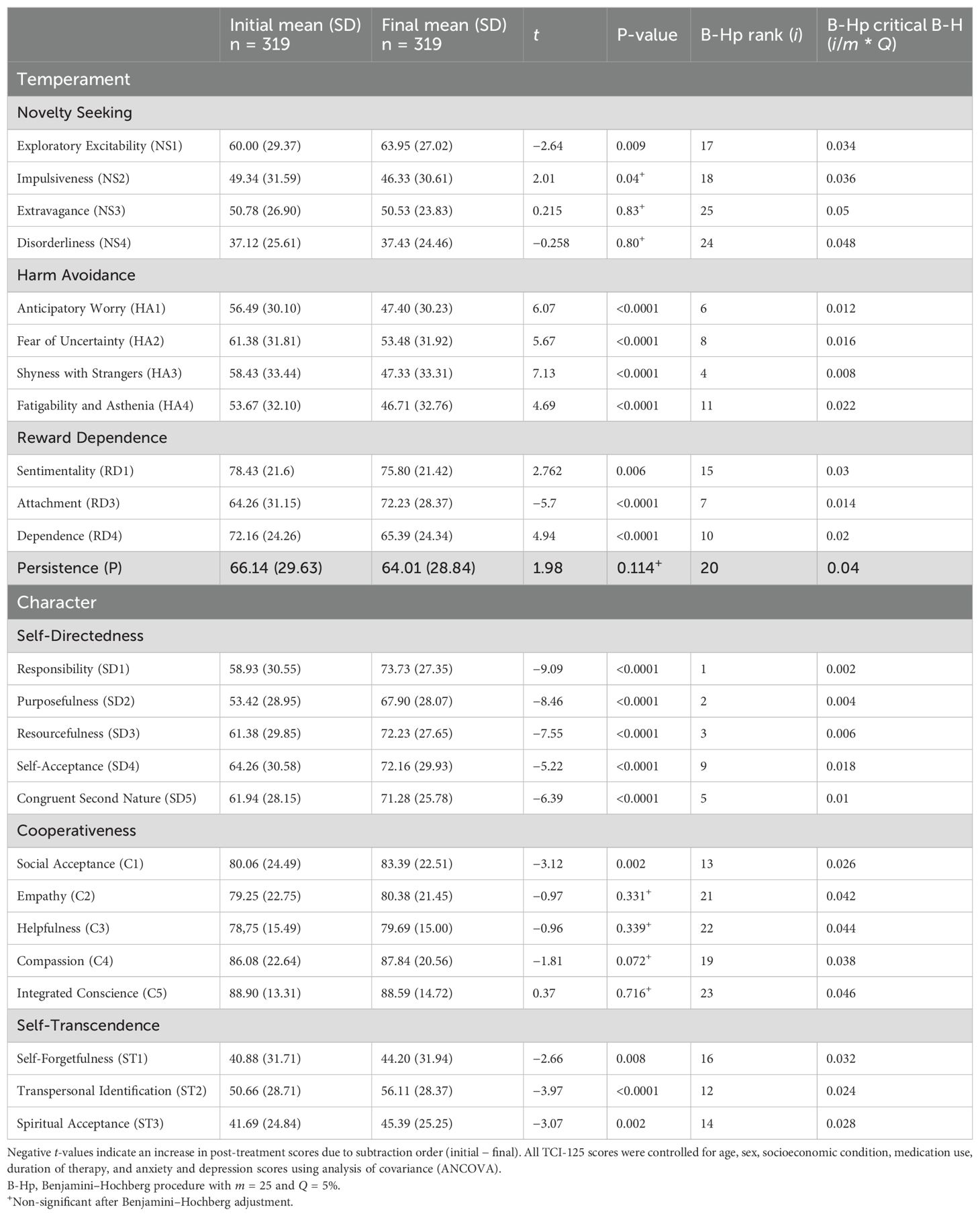
Table 1. Mean comparisons (paired t-test) between initial and final TCI-125 facet scores with post-hoc Benjamini–Hochberg procedure to control false discovery rates.
Each facet corresponds to two opposing poles within its respective dimension, enabling the assessment of higher or lower dimensional levels depending on proximity to either pole. For NS, high Exploratory Excitability (NS1) indicates enjoyment of unfamiliar situations and a tendency to seek novelty, thrills, and adventure. High Impulsiveness (NS2) suggests poor impulse control and hasty decision-making. High Extravagance (NS3) is linked to excessive spending of money, energy, or emotions. High Disorderliness (NS4) is associated with irritability and disorganization. In HA, high Anticipatory Worry (HA1) indicates anxiety or pessimism, often expecting danger or failure in relatively safe situations. High Fear of Uncertainty (HA2) reflects discomfort with ambiguity and unfamiliar circumstances perceived as threatening. High Shyness with Strangers (HA3) indicates low self-confidence in social settings, whereas high Fatigability and Asthenia (HA4) is linked to low energy and susceptibility to exhaustion. In RD, high Sentimentality (RD1) indicates emotional sensitivity and compassion. High Attachment (RD3) reflects a preference for sharing experiences and forming warm, lasting bonds. High Dependence (RD4) indicates reliance on others for emotional support and approval. The P dimension has no subfacets; high scores indicate perseverance, resourcefulness, and resilience despite frustration and fatigue. In SD, high Responsibility (SD1) reflects autonomy and accountability; high Purposefulness (SD2) indicates goal orientation and determination; high Resourcefulness (SD3) reflects competence and problem-solving ability; high Self-Acceptance (SD4) indicates confidence and acceptance of strengths and limitations; and high Congruent Second Nature (SD5) reflects habitual alignment of actions with values and long-term goals. In C, high Social Acceptance (C1) reflects tolerance and friendliness; high Empathy (C2) reflects perspective-taking; high Helpfulness (C3) is associated with supportive, encouraging, or reassuring behaviors; high Compassion (C4) reflects kindness, forgiveness, and generosity; and high Integrated Conscience (C5) reflects fairness, sincerity, and principled behavior. In ST, high Creative Self-Forgetfulness (ST1) reflects the ability to transcend personal boundaries during deep engagement; high Transpersonal Identification (ST2) reflects a profound connection with nature and the universe; and high Spiritual Acceptance (ST3) indicates belief in miracles or supernatural experiences, sometimes involving magical thinking. The main objective of this study was to show that modifiable character dimensions, other personality traits (temperament), and emotional measures change as a result of GT. The secondary objective was to demonstrate that these changes are specifically related to motives for seeking psychotherapeutic help and to the specific psychotherapeutic alternatives that GT can offer for different types of suffering or disorders (see Table 2) that generate these motives. Therefore, the results for each type are discussed separately.
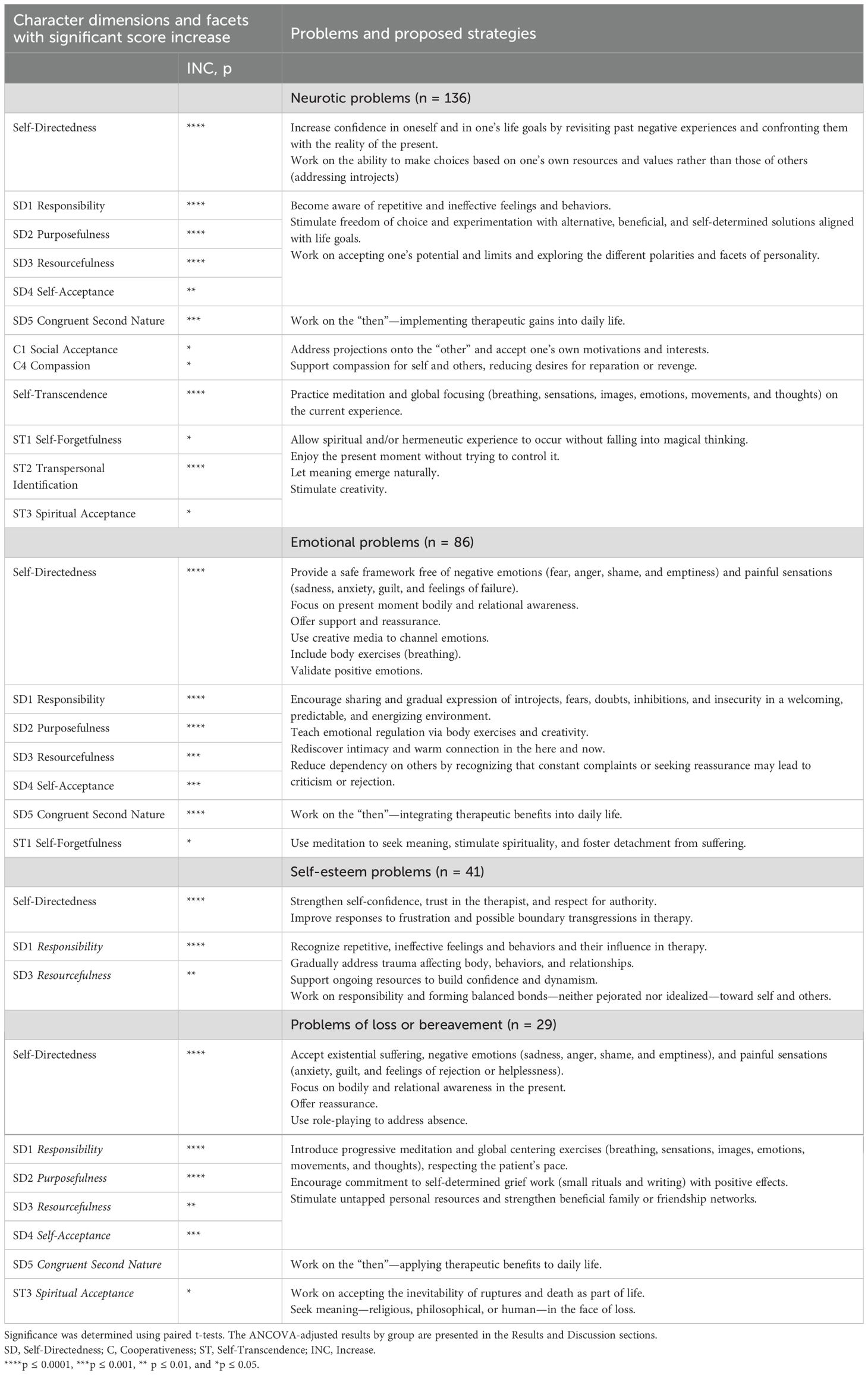
Table 2. Therapeutic strategies currently proposed in Gestalt therapy.
2 Materials and methods
2.1 Study design and participants
Therapy Gestalt TCI (THEGETCI) is an observational, longitudinal, prospective study. The investigators were Gestalt therapists informed of the goals (to promote the therapy), objectives (to show its efficacy), and methods. They were recruited through a network of students from the Limoges Institute of Formation in Gestalt Therapy and the Rennes Gestalt-plus Formation Center. All were graduates of accredited Gestalt institutes and certified by French and/or European professional bodies (FF2P, Fédération Française de Psychothérapie et de Psychanalyse; EAGT, European Association for Gestalt Therapy; and EAP, European Association for Psychotherapy). This study was approved by the local institutional review board (Ethics Committee of Limoges University Hospital, reference: CPP16-009/2015-A01208-41).
Although the therapists received payment from their clients, their participation in the study was voluntary and unrewarded. They were required to collect information about patients (age, sex, educational attainment, and usual medications) and briefly describe the reasons for clients’ requests for psychotherapy and its usefulness. The active client list of Gestalt psychotherapists is primarily composed of individuals with mild-to-moderate anxiety and depressive disorders (35, 36), often associated with neurotic, self-esteem, loss, grief, and separation issues. The authors examined the problems mentioned by patients, as well as the symptoms and behaviors identified by the psychotherapist, and classified them according to International Statistical Classification of Diseases and Related Health Problems 10th Revision into six categories: neurotic problems (F43.0 and F43.1), emotional problems (F32.0, F32.1, F41.0, F41.1, and F41.2), self-esteem problems (F60.30, F60.31, and F60.8), psychosomatic problems (F45.0 and F45.1), grief- and loss-related distress (F43.2), and other problems. These issues were examined separately to guide therapeutic strategies.
All therapists were trained by a group of experts in GT, and the content of care was formalized. All had been trained in GT institutes accredited by the European Association for GT and the European Association for Psychotherapy and were required to hold a European Certificate of Psychotherapy.
Following a semi-structured interview, therapists included clients meeting the inclusion and exclusion criteria and proposed a psychotherapeutic program consisting of 33 one-hour sessions (minimum of 12), spaced over several months, with a maximum duration of 2 years.
During the initial session, clinicians completed an observation note and asked patients to answer items related to personality, anxiety, and depression. Both therapist and patient independently assessed psychological distress using a 10-point visual analog scale.
The inclusion criteria were as follows: male or female patients aged 18 years or older, affiliated with health insurance, diagnosed with mood disorders (F32–F39, excluding bipolar affective disorders and manic episodes), possibly associated with an anxiety disorder (F41.0, F41.1, and F41.2) according to ICD-10 criteria, and with mild-to-moderate severity and no suicidal intent. All patients received oral and written explanations of the study’s purpose, research instruments, privacy protections, and their right to withdraw at any time. They provided written informed consent. The exclusion criteria were as follows: psychotic disorders, addictive behavior to one or more substances, cognitive deficits suggesting neurocognitive disorders, and legal protection status (guardianship).
There was no limit on the number of clients included during the 1-year recruitment period.
Of 59 Gestalt therapists (432 clients), 53 finalized 319 cases (77%). The main reasons for non-completion were abandonment (patient left before 12 sessions for personal, family, or work-related reasons) and loss to follow-up (patient left without explanation and was no longer in contact).
2.2 Measurement instruments and procedure
Individual development through psychotherapy was assessed using various tools. The primary instrument was the 125-item TCI, translated and validated in French (37, 38). Analyses were based on total scores for each dimension and facet (subdimension). All raw scores were weighted (out of 100) for readability.
Anxiety and depression were assessed using the validated French version of the Hospital Anxiety and Depression Scale (39, 40), a self-report questionnaire consisting of 14 four-point items: seven for anxiety and seven for depression, with each subscale scored from 0 to 21.
The visual analog scale (VAS) was used to assess subjective psychological states such as distress, anxiety, and moral pain. It is a simple, rapid, single-item measure in which the patients marked their perceived state on a visual line, and the therapists recorded their clinical global impression (41). The VAS is also suitable for assessing state changes. The scale consists of a line anchored by two extremes: “no distress” on the far left and “extreme distress” on the far right (42). Both patient and therapist marked the point corresponding to perceived intensity. Scores were calculated by measuring the distance in millimeters from the “no distress” anchor to the mark. VAS assessments were performed independently.
All measures were completed at the initial and final visits.
2.3 Statistical methods
Quantitative variables were described as means and standard deviations; qualitative variables were described as numbers and percentages. The Kolmogorov–Smirnov and Shapiro–Wilk tests were used to assess the normal distribution of quantitative variables. Paired t-tests were used to compare initial and final scores, given the one-to-one correspondence between samples (43), despite some deviations from normality, due to the test’s robustness with large samples (n > 30), as in this study (n = 319). All TCI scores were adjusted for potential confounders (age, sex, socioeconomic status, psychotropic medication use, duration of therapy, anxiety, and depression) using analysis of covariance (ANCOVA). All tests were two-sided, with the significance level set at α = 0.05 (p ≤ 0.05). To account for multiple comparisons, the Benjamini–Hochberg procedure was applied to control the false discovery rate, maintaining statistical power while limiting false positives (44). This procedure involves ranking p-values from multiple tests in ascending order and comparing each to a critical threshold calculated as (i/m) × α, where i is the rank, m is the total number of tests, and α is the predetermined false discovery rate (typically 0.05). A p-value is significant if ≤ (i/m) × α.
All analyses were performed using XLSTAT 2021.2.1 (45). and SPSS 29.0.2.0.
3 Results
The 319 subjects [78 men and 241 women; mean age = 41.01 ± 11.05 (range, 19–76)] had an average of approximately 31 ± 6 sessions (range, 12–53). The 53 therapists had an average of approximately six finalized cases each (range, 1–36). The mean duration between the initial and final sessions was 393 ± 150 days (range, 70–1155). Duration and number of sessions were statistically correlated (ρ = 0.36, p < 0.001). The evolution of different measures of mental state between the first and last sessions is presented in Table 3 for the Hospital Anxiety and Depression Scale (HADS), TCI, and VAS assessment scales and in Table 1 for the facets of the TCI. Post-treatment changes in the TCI dimensions remained significant in paired comparisons (Table 3) and were not explained by covariates such as age, sex, education level, psychotropic medication use, therapy duration, or baseline anxiety and depression scores. ANCOVA confirmed the independence of these changes from potential confounding variables, and these findings remained significant after applying the Benjamini–Hochberg procedure to control the false discovery rate.
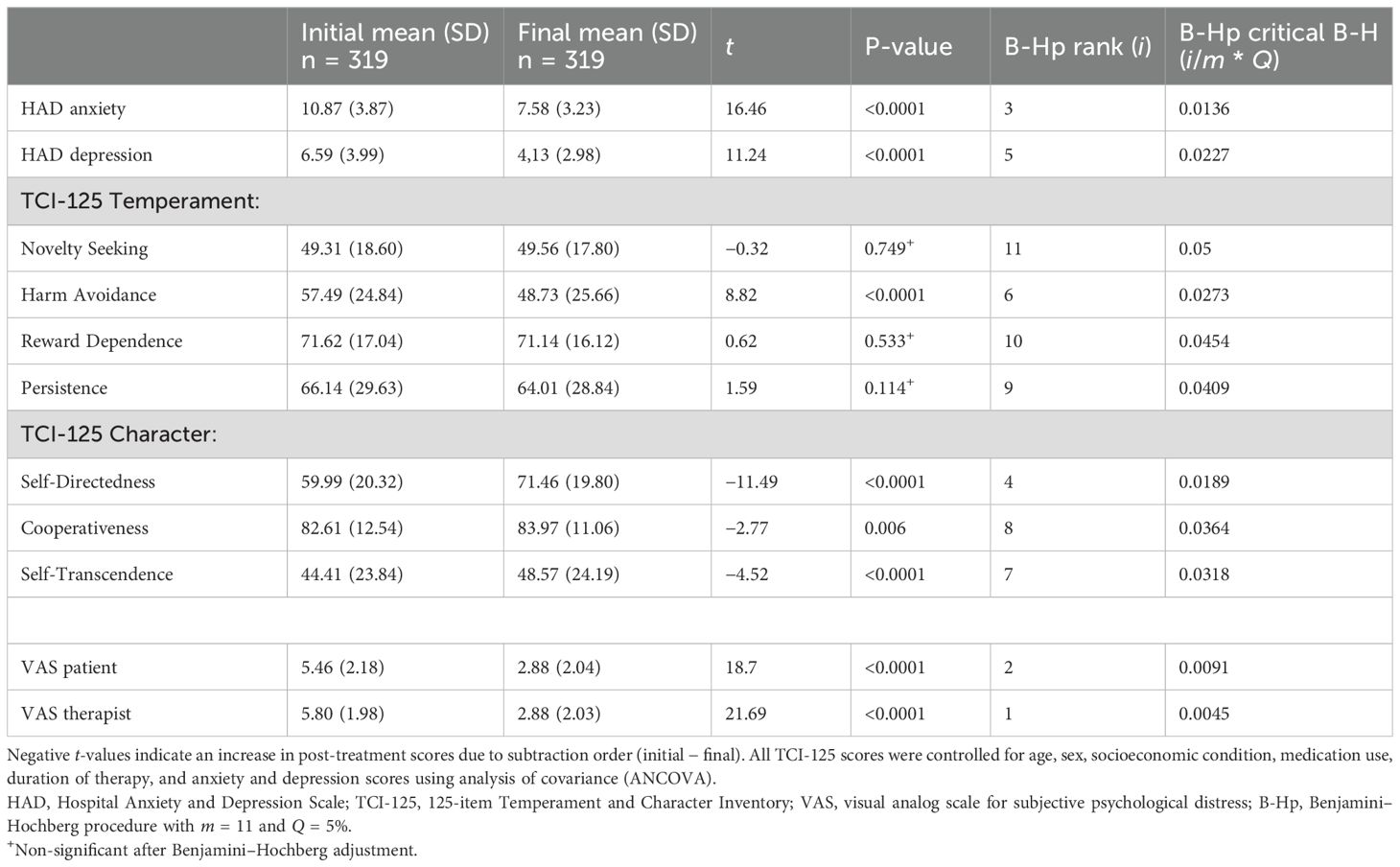
Table 3. Mean comparisons (paired t-test) between initial and final scores with post-hoc Benjamini–Hochberg procedure to control false discovery rates.
Statistically significant differences between the initial and final mean scores were observed for anxiety, depression, harm avoidance, and global psychological distress assessed using the VAS (all decreasing) and for the three maturity dimensions (all increasing) (Table 3). When considering the 25 facets, statistically significant differences between the initial and final mean scores were observed for Exploratory Excitability (NS1), Impulsiveness (NS2) (non-significant after the Benjamini–Hochberg procedure), Social Acceptance (C1), and all HA, RD, SD, and ST facets (Table 1).
Table 4 shows statistically significant differences between the initial and final anxiety scores for all clinical motives underlying the request for psychotherapy. Group classification was based on patients’ presenting complaints rather than formal psychiatric diagnoses as defined by the ICD-10. Across the various groups, an overall increase was observed in SD scores—especially in the SD3 facet (Resourcefulness)—and a general decrease in HA, particularly in the HA2 facet (Fear of Uncertainty). In the grief/loss distress group and emotional disorder group, these changes were significant in paired t-tests but were not confirmed in ANCOVA models adjusted for age, sex, and baseline anxiety.
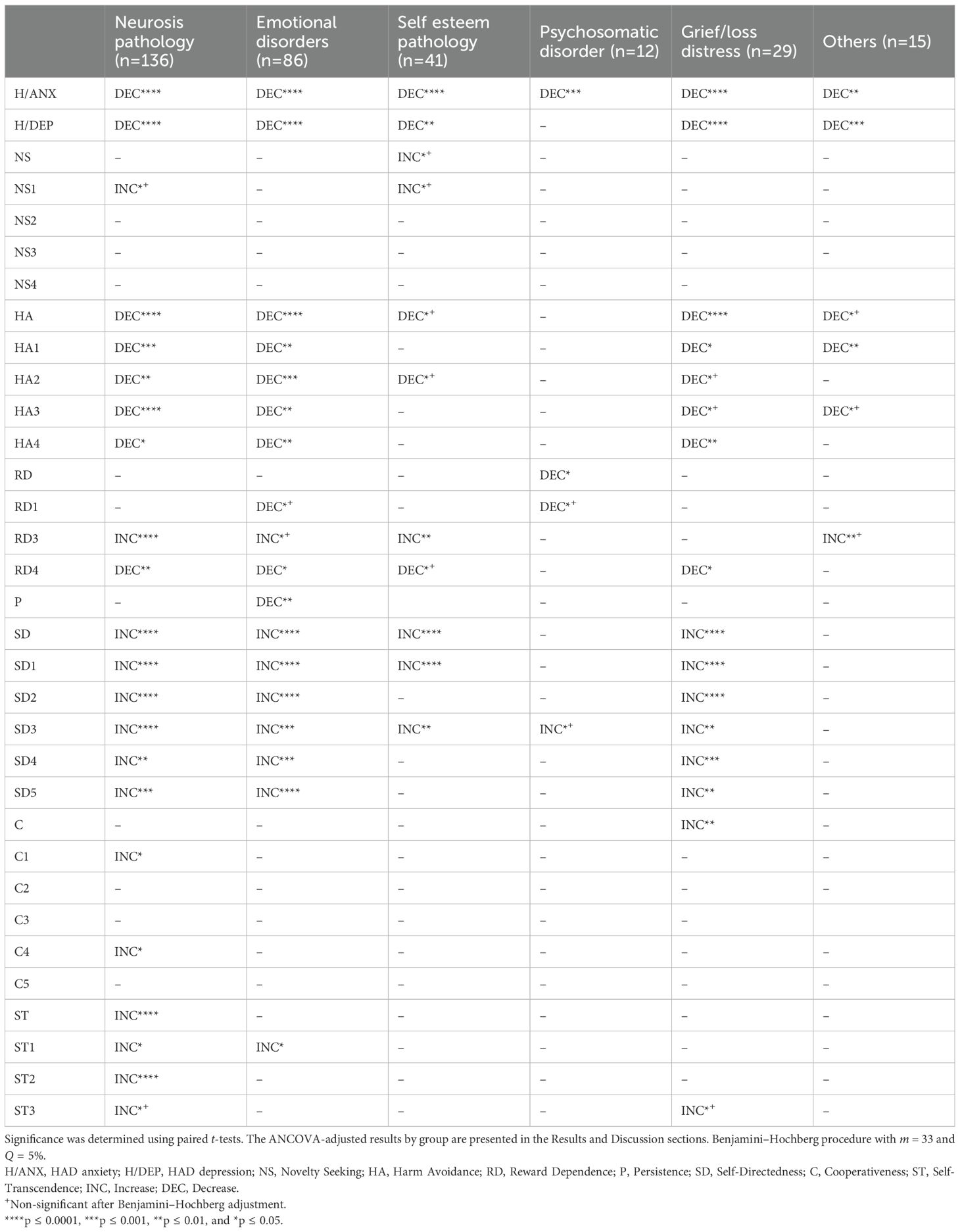
Table 4. Mean comparisons between initial and final TCI-125 dimension and facet scores according to the six different motives for requesting GT.
With the VAS, statistically significant decreases in the measurements of distress were observed in both patients and therapists, with correlated scores at the initial and final sessions (r = 0.62, p < 0.001, and r = 0.73, p < 0.001, respectively).
4 Discussion
As assumed, the results of THEGETCI showed a significant increase in the three dimensions of character. As outlined in other studies, SD shows the greatest increase (46–48). Character is based on a continuous maturation process, and Self-Directedness increases throughout life (33, 49–51), confirming the hypothesis that maturity, an epigenetic factor, increases with experience. Each session, through the proposed techniques, is an experience that tends to develop the different facets of SD by reducing the patient’s repetitive behaviors, fostering awareness of “conservative adjustments”, and inviting the patient to adjust in new and creative ways to the therapeutic situation. This regularly renewed experience aims to develop maturity, autonomy, reliability, responsibility, awareness, and self-esteem. However, the evolution varied according to the identified problems. Interestingly, Cooperativeness increased less strongly, indicating a positive evolution in the ability to create constructive social relationships, particularly among those with better social acceptance. Overall, C remained broadly stable, except in the neurotic group, where social tolerance (Social Acceptance C1) and indulgence (Compassion C4) significantly increased. For this group, the data may indicate an improved capacity to build constructive relationships. The significant increase in Self-Transcendence (for its three facets—Self-Forgetfulness, Transpersonal Identification, and Spiritual Acceptance) is a corollary of the increase in maturity. During Gestalt therapy sessions, ST is stimulated by the quest for meaning in sensations, emotions, postures, and thoughts that emerge in the present situation. This results in a co-construction between patient and therapist that promotes detachment from oneself and recognition of shared human experience. A significant increase was observed for the Transpersonal Identification (ST2) facet. Meditative exercises can positively influence this aspect through the dual movement of relaxation and concentration they demand, promoting not only detachment from self and suffering but also focused attention on ongoing psychocorporeal manifestations. Spiritual Acceptance (ST3) can also be sharpened through the shared quest and co-construction of meaning, which can evolve into a possible spiritual and/or hermeneutic experience without falling into magical thinking or superstition.
The results also showed changes in temperament dimension scores, although to a lesser extent. HA was the only dimension that decreased significantly, as observed in other treatments [46–48]. This indicates that therapeutic work promotes increased energy, courage, and optimism in patients with depression or anxiety. This dimension aligns with the goals of accountability and patient empowerment in GT. All four facets—Anticipatory Worry (HA1), Fear of Uncertainty (HA2), Shyness with Strangers (HA3), and Fatigability and Asthenia (HA4)—decreased significantly, especially among patients with emotional, neurotic, and grief/loss problems.
The focus on the present—through meditation, breathing exercises, body relaxation, updating internalized parental or educational injunctions (introjects), and examining their effects on the therapeutic situation—can be assumed to influence the decrease in Anticipatory Worry (HA1) and Shyness with Strangers (HA3), particularly in emotional or neurotic problems (see Table 2 for current strategies used in GT). Regarding loss and grief issues, dialogue, empathic listening to existential distress, feelings of abandonment or rejection, and developing past or anticipated relationships in role-playing tended to help patients recognize their own resources and reduce asthenia.
The reduction in HA was more discreet for self-esteem and psychosomatic problems, where doubt toward others and attachment to symptoms require more detailed psychotherapeutic work over a longer period due to alexithymia (52). In the emotional disorder and grief/loss groups, changes in SD and HA that were significant in paired t-tests did not remain significant after ANCOVA adjustment for age, sex, and baseline anxiety, suggesting that these effects may be explained by these covariates rather than by the treatment itself. It is also important to note that ANCOVA could not be applied in groups with small sample sizes (e.g., psychosomatic disorders and other problem groups), and due to limited statistical power in subgroup analyses, not all relevant covariates (e.g., education level, medication use, therapy duration, and depression) could be included in the adjusted models for every group. Notably, when baseline anxiety was excluded from the model in the emotional disorder group, the improvement in SD was significant again, suggesting that anxiety levels may mediate or obscure the treatment effect on this dimension in patients with emotional disorders.
While NS did not increase significantly overall, the NS1 facet (Exploratory Excitability) increased significantly in the neurotic and self-esteem groups (p < 0.05). This increase can be explained by accountability work in therapy, aimed at refocusing the patients’ demand for change toward themselves and their representations, rather than toward others or the therapist, in the form of victimization, claims, or grandiosity—common in self-esteem problems (53, 54). The stability of the other facets may indicate that impulsiveness, extravagance, and disorderliness (NS2, NS3, and NS4) are controlled in GT by a clear therapeutic framework, awareness of transference phenomena in the patient–therapist relationship, and exploration of their traumatic or phantasmatic origins.
The stability of RD may indicate the integrity and healthy narcissistic balance of Gestalt therapists, who aim primarily for patient autonomy while avoiding overly strong suggestions or manipulations. Nevertheless, there were differences between the facets of this dimension after treatment. The invitation to become aware of and share emotions can influence the Attachment (RD3) facet, which showed a significant increase in emotional, neurotic, and self-esteem pathologies. This seems to be a good indicator of the quality of the client–therapist bond, which was built and strengthened during sessions, but without fostering dependency (Dependence RD4), a facet that significantly decreased. Persistence remained stable because it is not a primary objective of GT, at least in its compulsive dimension. For all patients, the average HADS score at the beginning of treatment was approximately 17, corresponding to “severe anxiety or depression”, and decreased to approximately 12 post-treatment, corresponding to a “mild anxious or depressive state” (39). The decrease in anxiety was significant (p < 0.0001) for neurotic, emotional, grief/loss, and self-esteem problems, representing more than 90% of the patients (Table 4). This decrease remained significant, although more moderate, for psychosomatic problems (p = 0.003) and for other patients (p = 0.002). The reduction in depressive symptoms was also significant (p < 0.0001) for neurotic, emotional, and grief/loss problems and was more moderate for self-esteem issues (p < 0.003), while remaining stable for psychosomatic problems. In both cases, this represents a fundamental issue (55, 56) that may only evolve over a longer period through the exploration of trauma and its effects on the therapeutic relationship. Finally, the small patient sample for psychosomatic problems limits interpretation.
The VAS results, with blind assessments by both patients and practitioners, tended to show consistency in their perceptions of the positive evolution of the therapeutic process.
4.1 Limitations
This was a 1-year longitudinal study. However, it is not known whether this effect persists long after treatment. It would be interesting to investigate the long-term effects of GT and compare them with data from other established psychotherapies. Furthermore, we are not certain that patients who refused to participate in the study were actually identical to those included, nor whether they would have had a higher rate of failure than the study sample. We did not include a control group, which limited the scope of our study. However, we adjusted our results for many confounding factors such as age, sex, socioeconomic status, medication use, duration of therapy, and anxiety and depression scores. The therapist effect is indeed an important factor in any relational psychotherapy where the therapist is simultaneously one of the protagonists in the therapeutic relationship (57). In this study, all therapists had the same training, used the same method, and had at least 8 years of experience, which may have reduced differences between therapists’ results. However, future research should further explore the statistical and methodological considerations relevant to the therapist effect (58). Moreover, although there was a blind procedure for assessing effectiveness between the therapist and the patient and for recording initial assessments, self-assessment of effectiveness inevitably carries a bias of social desirability.
5 Conclusions
This study is one of the first to show the effectiveness of GT on personality dimensions through classical care. The rigorous evaluations presented herein demonstrate the importance of this technique. The specific contribution of GT lies in the therapist’s transmission of a particular attitude, consisting of a focus on the present, awareness, and responsibility: “These three elements (evaluation of current events, state of consciousness and responsibility) are the aspects of the same way of being in the world. Being responsible (able to respond) involves being present, being there. And being truly present is being conscious. And finally, being aware is presence (reality), a condition incompatible with the illusion of irresponsibility by which we avoid living our lives, rather than living them without caring what we think” (59).
Cloninger’s TCI-125 has shown its usefulness in assessing the effectiveness of GT. The results principally show that an increase in SD and a decrease in HA can serve as benchmarks for individual management. These significant personality changes can be considered indicators of progress in the psychotherapy process and, consequently, of the effectiveness of GT. Moreover, GT appears to improve state variables such as depression and anxiety, as well as subjective psychological distress. Recently, we developed a new version based on Cloninger’s biopsychosocial model, which integrates an eighth dimension for assessing alexithymia to better understand the evolution of patients with somatic disorders. This TCAI-150-LR (Temperament, Character, and Alexithymia Inventory with 150 items in a Lexical Revision) is currently under validation.
Further studies in other cohorts are needed to confirm the results presented here and to better determine the expected benefits for practitioners, as well as the patient profiles most likely to benefit from GT.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://doi.org/10.6084/m9.figshare.19345487.
Ethics statement
The THEGETCI study was submitted to an ethics committee. This study was approved by the local institutional review board (Ethical Committee of the Limoges University Hospital, Reference: CPP16-009/2015-A01208-41). All methods were carried out in accordance with relevant guidelines and regulations. We ensured that data collection complied with French general data protection regulations (RGPD) and that respondent privacy was guaranteed. The participants provided their written informed consent to participate in this study.
Author contributions
BC: Conceptualization, Formal analysis, Methodology, Validation, Supervision, Writing – original draft, Writing – review & editing. J-LV: Conceptualization, Investigation, Methodology, Validation, Writing – original draft, Writing – review & editing. YP: Investigation, Writing – original draft. IS: Investigation, Writing – original draft. AF: Data curation, Resources, Writing – review & editing. J-PC: Conceptualization, Formal analysis, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, and/or publication of this article.
Acknowledgments
We gratefully thank all participating Gestalt therapists (THEGETCI group/see Supplementary Information File) and the investigation carried out by the THEGETCI group and patients for their response and their help. We are grateful for the data curation carried out by the Centre mémoire de ressources et de recherche du Limousin at CH Esquirol. We would like to thank Mrs. Pamela Sharman and Editage (www.editage.com) for the English-language editing.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1280954/full#supplementary-material
Abbreviations
C, Cooperativeness; GT, Gestalt therapy; HA, Harm Avoidance; HADS, Hospital Anxiety and Depression Scale; NS, Novelty Seeking; P, Persistence; RD, Reward Dependence; SD, Self-Directedness; ST, Self-Transcendence; TCI, Temperament and Character Inventory; TCI-125, 125-item Temperament and Character Inventory; VAS, visual analog scale.
References
1. Perls FS, Hefferline RF, and Goodman P. Gestalt therapy: excitement and growth in the human personality. US: Julian Press (1951).
2. Francesetti G. From individual symptoms to psychopathological fields. Towards a field perspective on clinical human suffering. Br Gestalt J. (2015) 24:5–19. doi: 10.53667/QQWT3472
3. Wheeler G and Axelsson L. Gestalt Therapy. Washington DC: American Psychological Association (2015).
4. Bloom D. The relation function of self: Self function on the most human Plane. Self-A Polyphony of Contemporary Gestalt Therapists In: Robine JM, editor. St. Romaine-la-Virvée: L’Exprimerie (2016). p. 665–84.
5. Francesetti G and Roubal J. Field theory in contemporary gestalt therapy, part 1: modulating the therapist’s presence in clinical practice. Gestalt Rev. (2020) 24:113–36. doi: 10.5325/gestaltreview.24.2.0113
6. Sarasso P, Tschacher W, Schoeller F, Francesetti G, Roubal J, Gecele M, et al. Nature heals: An informational entropy account of self-organization and change in field psychotherapy. Phys Life Rev. (2024) 51:64–84. doi: 10.1016/j.plrev.2024.09.005
7. Robine JM. Le contact, expérience première. In: Robine JM, editor. Gestalt-thérapie, la construction du soi. l’Harmattan, Paris (1998). p. 61–79.
8. Perls F. The Gestalt approach and Eye witness to therapy. Palo Alto: Sci Behav Books;. (1973), 16–7.
10. Francesetti G and Gecele M. A Gestalt therapy perspective on psychopathology and diagnosis. Br Gestalt J. (2009) 18:5–20. doi: 10.53667/QHOT7139
11. Yontef GM and Jacobs L. Gestalt therapy. In: Corsini RJ and Wedding D, editors. Current Psychotherapies, 8th, ed. Thompson Brooks/Cole, Belmont, CA (2007). p. 328–67.
12. Hurley J, Barrett P, and Reet P. ‘Let a hundred flowers blossom, let a hundred schools of thought contend’: A case for therapeutic pluralism in mental health nursing. J Psychiatr Ment Health Nurs. (2006) 13:173–9. doi: 10.1111/j.1365-2850.2006.00938.x
14. Melnick J. Welcome to the gestalt review. editorial Gestalt Review. (1997) 1:1–8. doi: 10.2307/44394007
15. Joyce P and Sills C. Skills in Gestalt Counselling and Psychotherapy. 2nd, ed. London: Sage Publications (2010).
16. Polkinghorne DE. Narrative configuration in qualitative analysis. In: Hatch JA and Wisniewski R, editors. Life History and Narrative. The Falmer Press, London (1995). p. 5–23.
17. Kelly T and Howie L. Exploring the influence of gestalt therapy training on psychiatric nursing practice: Stories from the field. Int J Ment Health Nurs. (2011) 20:296–304. doi: 10.1111/j.1447-0349.2010.00729.x
19. Aiaach Dominitz V. Gestalt Therapy Applied: a case study with an inpatient diagnosed with substance use and bipolar disorders. Clin Psychol Psychother. (2017) 24:36–47. doi: 10.1002/cpp.2016
20. Imes SA, Clance PR, Gailis AT, and Atkeson E. Mind’s response to the body’s betrayal: gestalt/existential therapy for clients with chronic of life-threatening illnesses. J Clin Psychol. (2002) 58:1361–73. doi: 10.1002/jclp.10084
22. Brownell P. Assessment in Gestalt therapy. In: Gestalt therapy. A guide to contemporary practice. Springer, New York (2010). p. 189–212.
23. Roubal J, Francesetti G, Brownell P, Melnick J, and Zeleskov-Djoric J. Bridging practice and research in gestalt therapy. In: Roubal J, Francesetti G, Melnick J, Zeleskov-Djoric J, and Bownell P, editors. Towards a Research Tradition in Gestalt Therapy, 1st ed, vol. p . Cambridge Scholars Publishing, UK (2016). p. 1–17.
24. Stevens C, Stringfellow J, Wakelin K, and Waring J. The UK Gestalt psychotherapy CORE research project: The findings. Br Gestalt J. (2011) 20:22–7. doi: 10.53667/HFQY7525
25. Fogarty M, Bhar S, and Theiler S. Development and validation of the gestalt therapy fidelity scale. Psychother Res. (2019) 30:495–509. doi: 10.1080/10503307.2019.1571688
26. Francesetti G. Pain and beauty: from the psychopathology to the aesthetics of contact. Br Gestalt J. (2012) 21:4–18. doi: 10.53667/BZZH5404
27. Sarasso P, Francesetti G, Roubal J, Gecele M, Ronga I, Neppi-Modona M, et al. Beauty and uncertainty as transformative factors: A free energy principle account of aesthetic diagnosis and intervention in gestalt psychotherapy. Front Hum Neurosci. (2022) 16:906188. doi: 10.3389/fnhum.2022.906188
28. Spagnuolo Lobb M, Sciacca F, Iacono Isidoro S, and Di Nuovo S. The therapist's intuition and responsiveness: what makes the difference between expert and in training gestalt psychotherapists. Eur J Investig Health Psychol Educ. (2022) 12:1842–51. doi: 10.3390/ejihpe12120129
29. Evans C, Connell J, Barkham M, Margison F, McGrath G, Mellor-Clark J, et al. Towards a standardized brief outcome measure: psychometric properties and utility of the CORE-OM. Br J Psychiatry. (2002) 180:51–60. doi: 10.1192/bjp.180.1.51
30. Armstrong J. How effective are minimally trained/experienced volunteer mental health counsellors? Evaluation of CORE outcome data. Counsel Psychother Res. (2010) 10:22–31. doi: 10.1080/14733140903163284
31. Lambie JA. The demanding world of emotion: A Gestalt approach to emotion experience. News Ideas Psychol. (2020) 56:100751. doi: 10.1016/j.newideapsych.2019.100751
32. Cloninger CR. A systematic method for clinical description and classification of personality variants. A proposal Arch Gen Psychiatry. (1987) 44:573–88. doi: 10.1001/archpsyc.1987.01800180093014
33. Cloninger CR, Svrakic DM, and Przybeck TR. A psychobiological model of temperament and character. Arch Gen Psychiatry. (1993) 50:975–90. doi: 10.1001/archpsyc.1993.01820240059008
34. Cloninger CR, Przybeck TR, Svrakic DM, and Wetzel RD. The Temperament and Character Inventory (TCI): a guide to its development and use. 1st edition. Saint-Louis, Mo: Washington University (1994).
35. Herrera P, Mstibovskyi I, Roubal J, and Brownell P. Researching gestalt therapy for anxiety in practice-based settings. A Single-Case Exp Design Psychotherapie-Wissenschaft. (2019) 9:53b–68b. doi: 10.30820/1664-9583-2019-2-53b
36. Francesetti G and Roubal J. Gestalt Therapy approach to depressive Experiences. Psychotherapie-Wissenschaft. (2020) 10:39–45. doi: 10.30820/1664-9583-2020-2-39
37. Pélissolo A and Lépine JP. Traduction française et premières études de validation du questionnaire de personnalité TCI. Ann Méd Psychol. (1997) 155:497–508.
38. Chakroun-Vinciguerra N, Faytout M, Pélissolo A, and Swendsen J. Validation française de la version courte de l’inventaire du tempérament et du caractère (TCI-125). J Thérapie Comportementale Cognitive. (2005) 15:27–33. doi: 10.1016/S1155-1704(05)81209-1
39. Zigmond AS and Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 286:171–3. doi: 10.1111/j.1600-0447.1983.tb09716.x
40. Lépine JP, Godchau M, Brun P, and Lempérière T. Evaluation de l’anxiété et de la dépression chez des patients hospitalisés dans un service de médecine interne. Ann Med Psychol. (1985) 2:175–85.
41. Rossi V and Pourtois G. Transient state-dependent fluctuations in anxiety measured using STAI, POMS, PANAS or VAS: a comparative review. Anxiety Stress Coping. (2012) 25:603–45. doi: 10.1080/10615806.2011.582948
42. Gift AG. Visual Analogue Scales: Measurement of subjective phenomena. Nurs Res. (1989) 38:286–8. doi: 10.1097/00006199-198909000-00006
43. McCrum-Gardner E. Which is the correct statistical test to use? Br J Oral Maxillofac Surg. (2008) 46:38–41. doi: 10.1016/j.bjoms.2007.09.002
44. Benjamini Y and Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc Ser B Stat Methodol. (1995) 57:289–300. doi: 10.1111/j.2517-6161.1995.tb02031.x
45. Addinsoft. XLSTAT statistical and data analysis solution. Paris: France: Levimero (2021). Available online at: https://www.xlstat.com.
46. Hofmann SG and Loh R. The Tridimensional Personality Questionnaire: changes during psychological treatment of social phobia. J Psychiatr Res. (2006) 40:214–20. doi: 10.1016/j.jpsychires.2005.03.010
47. Mörtberg E, Bejerot S, and Aberg Wistedt A. Temperament and character dimensions in patients with social phobia: Patterns of change following treatments? Psychiatr Res. (2007) 152:81–90. doi: 10.1016/j.psychres.2006.10.003
48. Mazza M, Mazza O, Pomponi M, Di Nicola M, Padua L, Vicini M, et al. What is the effect of selective serotonin reuptake inhibitors on temperament and character in patients with fibromylgia? Comp Psychiatr. (2009) 50:240–4. doi: 10.1016/j.comppsych.2008.08.004
49. Rigozzi C and Rossier J. Validation d’une version abrégée du TCI (TCI-56) sur un échantillon de jeunes fumeurs et non-fumeurs. Ann Méd Psychol. (2004) 162:541–8. doi: 10.1016/j.amp.2003.09.013
50. Fresán A, Robles-García R, López-Avila A, and Cloninger CR. Personality differences according to age and sex in a Mexican sample using the Temperament and Character Inventory-Revised. Comp Psychiatr. (2011) 52:774–9. doi: 10.1016/j.comppsych.2010.11.003
51. Calvet B, Péricaud M, Parneix M, Jouette A, Bricaud M, and Clément JP. Age and sex differences in temperament and character dimensions in a french nonclinical population. J Individ Differ. (2016) 37:168−80. doi: 10.1027/1614-0001/a000203
52. Terock J, Janowotz D, Spitzer C, Miertsch M, Freyberger HJ, and Grabe HJ. Alexithymia and self-directedness as predictors of psychopathology and psychotherapeutic treatment outcome. Comp Psychiatr. (2015) 62:34–41. doi: 10.1016/j.comppsych.2015.06.007
53. Kohut H. Le processus thérapeutique dans les tranferts en miroirs. In: Kohut H, editor. Le soi. PUF, Paris (1974). p. 152–209.
54. Kernberg O. Principes généraux du traitement. In: Kernberg O, editor. Les troubles limites de la personnalité. Dunod, Paris (1997). p. 99–145.
55. Bergeret J. Théorie de la dépression-limite. In: Bergeret J, editor. La dépression et les états limites: points de vue théorique, clinique et thérapeutique. Payot, Paris (1992). p. 137–51.
56. Smadja C. La dépression inachevée. Rev Fr Psychanal. (2004) 68:1239–52. doi: 10.3917/rfp.684.1239
57. Crits-Christoph P, Baranackie K, Kurcias J, Beck A, Carroll K, Perry K, et al. Meta-analysis of therapist effects in psychotherapy outcome studies. Psychother Res. (1991) 1:81–91. doi: 10.1080/10503309112331331335511
58. Constantino MJ, Boswell JF, Coyne AE, Kraus DR, and Castonguay LG. Who works for whom and why? Integrating therapist effects analysis into psychotherapy outcome and process research. In: Castonguay LG and Hill CE, editors. How and why are some therapists better than others?: Understanding therapist effects. American Psychological Association, New York (2017). p. 55–68.
Keywords: Gestalt therapy, Temperament and Character Inventory, personality, effectiveness, temperament, character, anxiety, depression
Citation: Calvet B, Vallejo J-L, Plu Y, Soulat I, Foucher A and Clément J-P (2025) Use of the Temperament and Character Inventory to describe the effectiveness of Gestalt therapy. Front. Psychiatry 16:1280954. doi: 10.3389/fpsyt.2025.1280954
Received: 21 August 2023; Accepted: 04 September 2025;
Published: 26 September 2025.
Edited by:
Paula Yanes-Lukin, New York State Psychiatric Institute (NYSPI), United StatesReviewed by:
Pietro Sarasso, University of Turin, ItalyMargherita Spagnuolo Lobb, Istituto di Gestalt HCC Italy, Italy
Copyright © 2025 Calvet, Vallejo, Plu, Soulat, Foucher and Clément. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Benjamin Calvet, YmVuamFtaW4uY2FsdmV0QGNoLWVzcXVpcm9sLWxpbW9nZXMuZnI=
†ORCID: Benjamin Calvet, orcid.org/0000-0001-7628-0430
Jean-Pierre Clément, orcid.org/0000-0001-8690-1050