 Wei Zhu1
Wei Zhu1 Ying Zhang
Ying Zhang Yanzhi Lan
Yanzhi Lan Xinqiang Song
Xinqiang Song- 1School of Medicine, Xinyang Normal University, Xinyang, China
- 2Xinyang Central Hospital, Xinyang, China
Smartphones have become an integral part of life for an increasing number of people around the world, especially as the range and speed of smartphone functions has expanded. However, excessive use of smartphones can cause not only physical discomfort but also feelings of loneliness, anxiety, and depression. The present review explores the negative effects of excessive smartphone use on physical and mental health. It also surveys measures that can counteract these effects, which include controlling smartphone use, strengthening self-control, and engaging in physical exercise.
Highlights
● Smartphones have become an integral part of modern life.
● Excessive use of smartphones can cause unhealthy physically and mentally.
● Feeling of discomfort include physical discomfort and feelings of loneliness, anxiety, and depression.
● Measures include controlling smartphone use, strengthening self-control, and engaging in physical exercise.
1 Introduction
Smartphones have become an integral part of modern life (1, 2), offering much richer possibilities for communication than the voice calling offered by earlier generations of telephones or mobile phones. Smartphones enable video calls and Internet access for listening to music, watching videos, shopping and accessing information—all in a format more portable and flexible than a desktop computer or even laptop (3–7). In China alone, the number of mobile Internet users was estimated at just over 1 billion in December 2022, which was 36 million more than in December of the previous year, and more than 99% of people in China report accessing the Internet via smartphone (8, 9). The range and portability of Internet services offered by smartphones have made them essential for people who wish to keep pace with the rapid developments of human society and the Internet. Updates and upgrades to smartphones have become a way to express one’s individuality and style.
Precisely because of their multifunctionality, smartphones have created a new form of dependence: whether waiting for a bus or subway, eating a meal, watching TV or preparing for bed, an increasing number of people rely on their smartphones to help them pass the time (10, 11). The growing dependence on smartphones has led to the so-called “heads-down” generation, whose physical and mental well-being may be harmed in several ways (12, 13). Excessive smartphone use, also referred to as “mobile phone dependency”, “mobile phone addiction”, or “problematic mobile phone use” can lead to various psychological, physiological, and social impairments (14–17) (Figure 1).
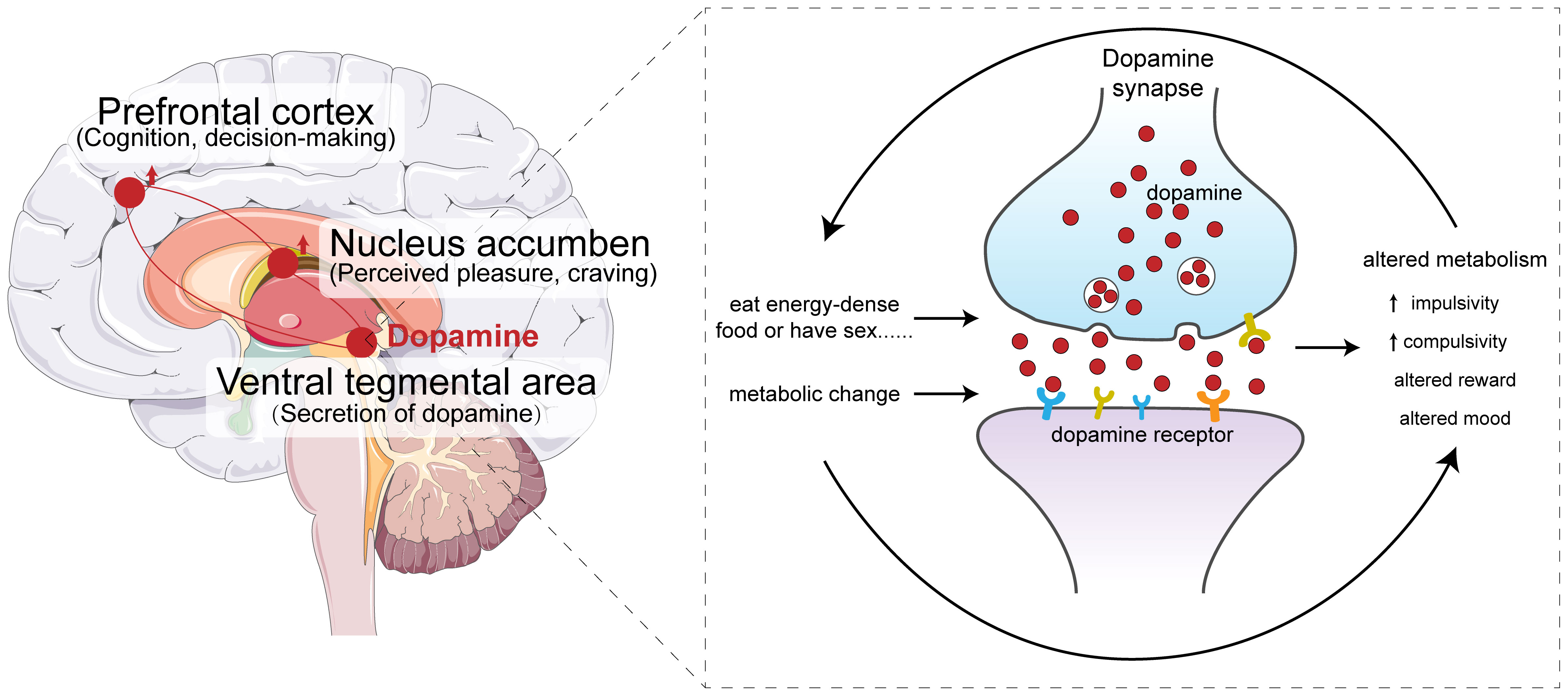
Figure 1. The hypothesis of smartphone addiction.
It is important to note that addiction, including smartphone addiction, is a result of the interaction between genetics and environment. Even if genetic factors increase susceptibility (e.g., making some people more sensitive to the reward of smartphone use or less able to control impulses), environmental factors (e.g., family upbringing, social context, and daily usage habits) play a more direct role in triggering and maintaining the behavior. At present, there is no sufficient evidence to confirm that a single or specific set of genes determines the risk of smartphone addiction.
From a theoretical perspective, smartphone addiction, as a type of non-substance addiction, shares similarities with substance addiction in terms of behavioral characteristics (e.g., compulsive use, reward-seeking) and potential neurobiological mechanisms (e.g., involvement of the brain’s reward circuit and monoamine neurotransmitter systems). Since substance addiction is known to have a genetic component (e.g., genes related to dopamine receptors like DRD4, DRD2, or serotonin transporters like 5-HTTLPR (5-hydroxytryptamine transporter linked polymorphic region, 5-HTTLPR) have been linked to addiction susceptibility) (18–20), researchers speculate that similar genetic factors may also influence the risk of smartphone addiction.This review discusses the various negative impacts on well-being that have been reported for excessive smartphone use, and it explores interventions and measures to mitigate or prevent those impacts.
2 Methods
We carried out a literature search in Pubmed/MEDLINE, Web of Sciences, Scielo and LILACS search using the following MeSH entry terms: “smartphone”, “mobile phone”, “cell phone”, “physical health”, “mental health”, “depression”, “sleep”,”loneliness”, “anxiety” and “dopamine signaling”, “musculoskeletal”, “low vision”, “ophthalmological”and we generated this search strategy for Pubmed: ((“smartphone t”[MeSH Terms]) OR (“mobile phone “[MeSH Terms]) OR (“cell phone” [MeSH Terms])AND (“depression” [MeSH Terms]) OR(”sleep “[MeSH Terms]) OR (”loneliness “[MeSH Terms])OR(”anxiety “[MeSH Terms])OR(”dopamine signaling “[MeSH Terms]) OR (”anxiety “[MeSH Terms])OR(”musculoskeletal “[MeSH Terms])OR (”low vision “[MeSH Terms])OR(”ophthalmological “[MeSH Terms]) OR(”mental health “[MeSH Terms])OR(”physical health “[MeSH Terms])).
We used equivalent strategies in the other databases. We reviewed the articles published between 2002 and August 2023, and no limitation for any language was used. The reference lists of the selected articles were also evaluated to identify other publications. The present study followed the PRISMA guidelines (19). As this study was not quantitative or epidemiological but a descriptive study, we did not assess the selected studies’ quality and did not perform a meta-analysis. An ethical analysis was not needed since it was a literature searching-based study.
3 Problems associated with excessive smartphone use
3.1 Addiction to dopamine signaling
Dopamine plays a crucial role in the brain’s reward system, which drives us to take actions to ensure our survival and pass on our genes to future generations. When we eat or have sex, the brain rewards us with a pleasant release of dopamine, so we strive to repeat those activities in the future in order to experience the same dopamine “rush”. We also experience this rush when we explore unfamiliar places, make new friends, or try things we have never done before, which may have evolved to drive us to explore in order to secure food and safety (21, 22) (Figure 2). We experience this rush when we learn something new, probably reflecting the evolutionary truth that the more we know about the world, the greater our chances of survival. For example, knowing how weather affects lion movements or when gazelles let down their guard can improve our hunting success (23). When confronted with something new, the brain releases dopamine to enhance focus and learning. There are numerous dopamine-producing cells in the brain that respond to novel stimuli but remain quiet in the face of familiar things (24, 25).
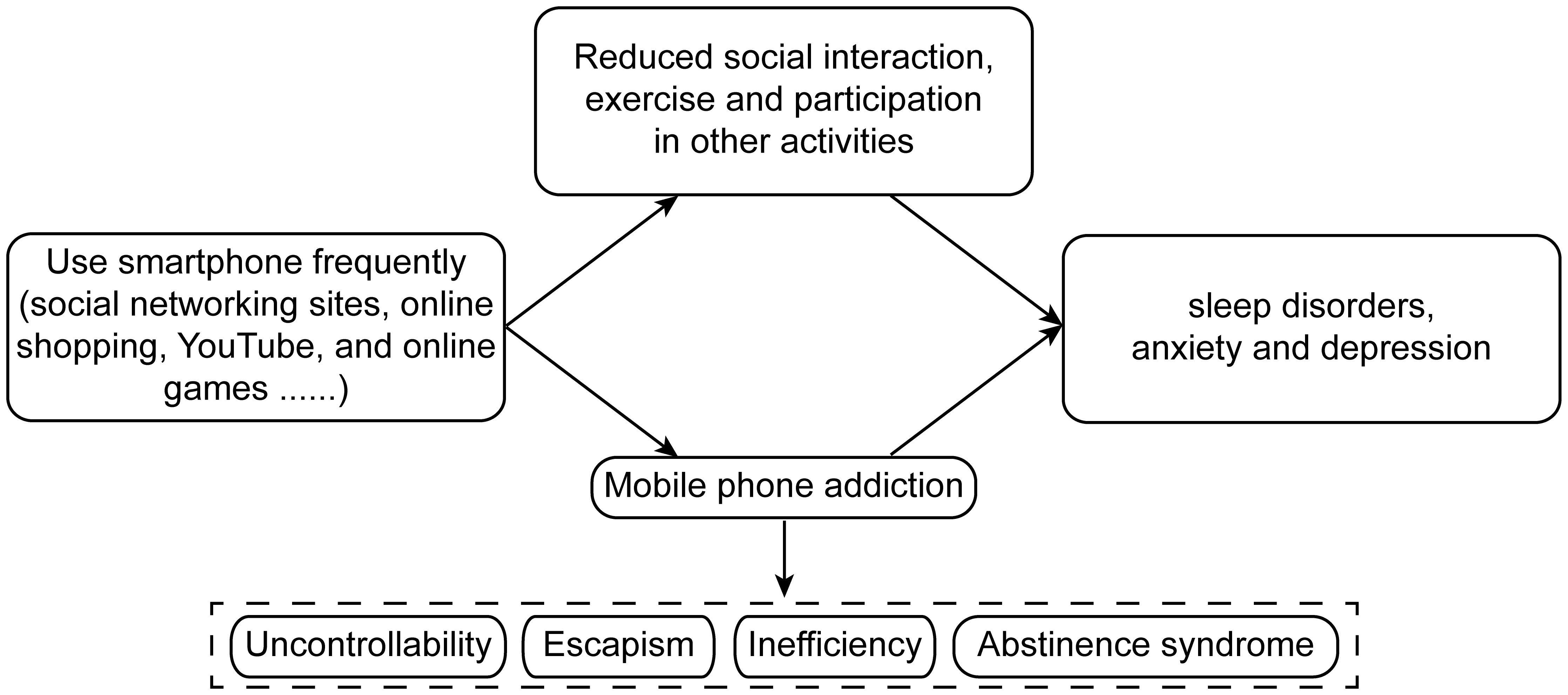
Figure 2. Possible pathways of addiction to dopamine signaling.
Today most of us no longer need to migrate in search of food, so the smartphone offers us an alternative route to the dopamine rush by providing us with a constant, easily accessible source of information (26) (27). Whenever our smartphone notifies us of a new message or development in the Internet, we cannot resist the urge to check it immediately. The reward circuit with the nucleus accumbens as the core plays a crucial role in smartphone addiction. When people obtain positive experiences from smartphones, the reward circuit is activated, and dopaminergic neurons in the nucleus accumbens release dopamine, interacting simultaneously with brain regions such as the prefrontal cortex and the amygdala. The prefrontal cortex is responsible for high-level cognitive functions such as decision-making and impulse control, while the amygdala is involved in emotional processing. In the case of smartphone addiction, the excessive activation of the reward circuit leads to a decrease in the prefrontal cortex’s ability to control impulses. At the same time, the activity of the amygdala increases, making individuals more prone to strong emotional responses and cravings for smartphone-related stimuli, and it becomes difficult for them to suppress the urge to use smartphones. Every time we open a new webpage, the brain releases dopamine, driving us to constantly open new pages without stopping; the “next page” always seems better than the one we just saw. We spend fewer than 4 seconds on each webpage, and only 4% of webpages hold our attention longer than 10 minutes (28).
Smartphone addiction and drug addiction have similar manifestations: both involve a strong craving for the target object (drugs/smartphones), leading to uncontrollable and repeated use, and both are related to the activation of the brain’s reward circuit (such as the dopamine system). However, they also have differences. Drug addiction is driven by chemical substances, with strong physical dependence—long-term use leads to obvious physical withdrawal symptoms (such as vomiting, tremors) after cessation, directly causing organic damage, requiring medical intervention for withdrawal. In contrast, smartphone dependence is driven by digital stimuli and psychological-behavioral mechanisms, with almost no physical dependence; withdrawal mainly causes psychological discomfort (such as restlessness) without severe physical reactions. Its health risks are mostly indirect (like vision loss, sleep disorders), and withdrawal can generally be improved through behavioral adjustments (29–31).
3.2 Poor sleep quality
While the precise function of sleep remains poorly understood, it clearly is important because otherwise it would have been far too dangerous for early humans to spend nearly one-third of the day in an unconscious state, when they were more susceptible to predators and could not search for food, reproduce or otherwise work toward survival. Sleep is not important for helping us save energy: the brain (32) consumes a similar amount of energy during sleep as during wakefulness. Instead, one key function of sleep appears to be allowing the brain to clear protein waste that has accumulated during the day. In fact, the weight of metabolic waste cleared by the brain in a year may be equivalent to one’s body weight (33). Such lack of cleaning may help explain why chronic sleep deprivation can increase the risk of stroke and dementia (34). Another key function of sleep appears to be the “consolidation” of short-term memories into long-term memory (35): during sleep, the brain selects certain events of the day to store as long-term memories, while it also retrieves lost memories.
In China, one of every two people sleeps fewer than the recommended 7–9 hours per night, and the situation appears to be similarly bad in other countries (36). Lack of sleep affects our performance: sleeping fewer than 6 hours on 10 consecutive days decreases our attention to a similar extent as not sleeping for 24 hours (37). Sleep deprivation also intensifies and destabilizes our emotional responses in the amygdala, which drives our responses to stress (38).
By stimulating us even into late hours of the night, smartphones can rob us of the sleep that we need. The brain remains awake under constant stimulation by apps, social media, and other sources of information that trigger dopamine secretion (39). A study of more than 600 adults linked more time on electronic devices such as smartphones to worse sleep quality (40). Participants who reported staying up late to use their smartphones reported difficulties falling asleep and continuously declining sleep quality, leading to fatigue the next day.
The light of the smartphone screen can trick our body into thinking that it is daytime, inhibiting production of the melatonin that tells our body to sleep (41) (42). In fact, the blue light from smartphone screens inhibits melatonin production much more than the white light from ambient lighting (43, 44). As a result, the use of smartphones just before bed delays one’s falling asleep by 2–3 hours, shifting one’s entire circadian rhythm accordingly.
However, smartphones can compromise our sleep even when we are not watching the screen. In a survey of thousands of middle school students, those who reported sleeping next to their smartphones slept an average of 21 minutes less per night than those who did not (45). Based on that study, a smartphone in the same room disturbs sleep more than a television in the same room.
In addition, excessive use of mobile phones can cause stress and anxiety, which in turn reduce the duration and quality of our sleep (46).
Therefore, we should learn to suppress our craving to use smartphones, particularly in the evening before going to bed.
3.3 Depression
Large studies of adolescents in the US over the last decade have consistently linked greater use of digital products such as smartphones to greater risk of depressive emotions (47, 48). For example, adolescents who spend 6–9 hours per week with such products are significantly more likely to feel unhappy than those who spend 4–5 hours per week. The risk and severity of low mood increase with time spent on social networking sites, online shopping, YouTube, and computer games. Conversely, social interaction, exercise, playing musical instruments, and engaging in other activities have been linked to better mood (49, 50). That excessive smartphone use can cause sleep disturbances and depression was confirmed in a longitudinal study of 4,000 adolescents in US, which found that more frequent smartphone use led to higher levels of stress and rates of sleep disorders and depression (51, 52).
An analysis of over 125,000 children and adolescents in US showed that spending more than 2 hours a day on screens increases the risk of depression, and the risk increases with the duration of exposure (53, 54). Similar results were observed in a survey of 130,000 children and adolescents in China (55). A study of 40,000 children and adolescents in Europe found that those who used digital products longer than 7 hours a day were twice as likely to suffer depression or anxiety than those who spent less time in front of screens (56). The threshold of 7 hours per day is impressive because most adolescents have only 8–9 hours of leisure per day when they are not sleeping, studying or eating. It seems that nearly one of five adolescents spends nearly all their waking hours on digital devices (57). While reducing screen time can improve mood, it may be unrealistic to expect adolescents to limit themselves to the recommended one hour per day (58, 59).
It is perhaps no coincidence that adolescents in the US have been reporting progressively stronger feelings of loneliness, worse sleep quality, and less socializing since 2011, when the Apple iPhone dominated the smartphone market with sales of 120 million units, which exceeded the sales for the preceding four years combined (60). At the same time, the documented increases in stress, depression and anxiety among adolescents in various countries should not be attributed entirely to smartphone use (Figure 3). Other factors, for example, likely include increased competitiveness to enter the job market and lower perceived job security (61).
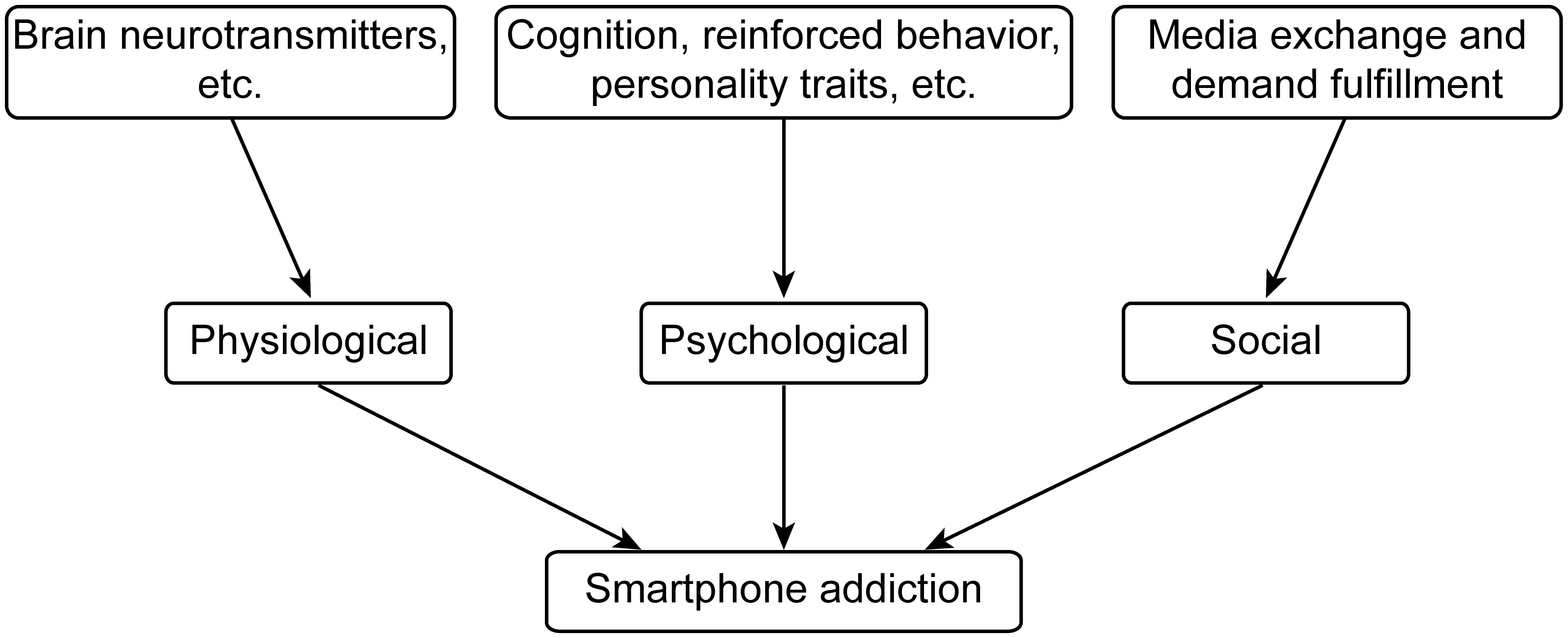
Figure 3. The association between mobile phone addiction and depression.
Smartphone dependence and depression often show a bidirectional relationship rather than a one-way cause-effect link, though both directions of influence are supported by research (62–65).On one hand, smartphone dependence may contribute to depression. Excessive smartphone use can reduce in-person social interactions, leading to feelings of isolation; constant exposure to curated “perfect lives” online may trigger negative self-comparisons; disrupted sleep (due to late-night phone use) can also exacerbate emotional instability—all of which may increase the risk of depression. On the other hand, depression may also lead to smartphone dependence. People with depression may turn to smartphones as an escape: using social media, games, or videos to distract themselves from low mood, loneliness, or negative thoughts. Over time, this can develop into a reliance on phones as a coping mechanism. In short, they often reinforce each other: dependence may worsen depressive symptoms, and depression may deepen dependence (66).
3.4 Physical problems
Extended smartphone use has been shown to adversely affect musculoskeletal health, particularly in the neck and upper extremities (67). Young et al. (68) identified that device characteristics such as larger screen sizes and non-ergonomic grip configurations correlate with increased neck flexion angles and sustained wrist extension. Given the variations in device dimensions, weight distribution, and interaction patterns across different smartphones, these factors may lead to distinct symptom profiles among users. Empirical evidence further indicates that musculoskeletal discomfort most commonly manifests within the first 15–30 minutes of continuous smartphone use. Strategic behavioral modifications, such as adhering to 15-minute usage intervals followed by postural resets, could potentially prevent symptom onset in over 70% of habitual users. A study conducted in Zhuhai City, China, explored the relationship between smartphone usage behavior and low vision. Four primary schools were randomly chosen from four different districts of Zhuhai. A total of 462 fifth - grade students were recruited as survey participants. Employing a retrospective cohort study design, the research combined questionnaire surveys with physical examinations to investigate the associated factors of low vision among pupils. Logistic regression analysis was then used to identify the influencing factors of low vision. The findings showed that the detection rate of low vision among these primary school students was 56.71%. The study also revealed a significant correlation between pupils’ smartphone usage and the incidence of low vision. Low vision was influenced by multiple factors, including heredity, gender, the age at which students started using smartphones, and the daily duration of smartphone use (69).
4 Measures and interventions to counteract the health effects of excessive smartphone use
4.1 Medical methods to address smartphone addiction
Some medications can help regulate neurotransmitters in the brain to reduce the craving and dependence on smartphones. For example, drugs that act on the dopamine system, such as bupropion, may be used to adjust the brain’s reward mechanism and relieve the symptoms of addiction (70, 71). However, the use of drugs needs to be strictly under the guidance of a doctor, as different people may have different reactions and side effects. Cognitive - behavioral therapy (CBT) is a commonly used method (72, 73). It helps patients recognize and change their negative thinking patterns and behaviors related to smartphone use, set goals to limit smartphone use, and learn to cope with stress and emotions in other ways. Motivational interviewing is also an effective approach, which stimulates the patient’s internal motivation to change and enhances their confidence and determination to overcome addiction. Some neurological techniques, such as transcranial magnetic stimulation (TMS) (74, 75), can be used to modulate the activity of specific brain regions related to addiction. By applying magnetic fields to the prefrontal cortex and other areas, it is possible to improve the brain’s executive function and impulse control ability, thereby helping to reduce smartphone addiction. However, this method requires professional medical equipment and trained medical staff to operate.
4.2 Controlling smartphone use
One approach to helping young people reduce smartphone use is to encourage them to have a clear goal in mind when using it: the person should pick up the phone knowing what task he or she wants to accomplish, complete the task, then put the phone aside. This attitude may help the individual control the time and frequency of smartphone use. Another approach is to view one’s smartphone dependence as a normal feeling. This can reduce feelings of self-blame and encourage the individual to engage in mindfulness or meditation to enhance their ability to control their attention (76).
Since excessive smartphone use often goes hand-in-hand with impulsivity or anxiety, parents should be careful to notice when their children may be exhibiting either condition, in which case they should supervise and, if necessary, limit the children’s use of smartphones. Parents should not simply regard all use of smartphones as detrimental to their children, but should investigate the reasons why they wish to use the devices and help them engage with the devices constructively (47).
Educational institutions must struggle with how to keep the classroom sufficiently interesting so that students are not lured to their smartphones. This may be particularly difficult when students are in primary or secondary school, or when courses are quite specialized or theory-laden as at university. In these instances, formal regulations may be needed that regulate smartphone use in the classroom. It may be helpful to separate students physically from their smartphones, such as by asking them to deposit them inside “phone pouches” in every classroom, because the phones themselves trigger craving to check for new information or messages. Outside the university classroom, student counselors, as the school administrators closest to students, can strongly influence students’ awareness of smartphone addiction and their willingness and effectiveness in managing it (23, 77, 78).
4.3 Enhancing self-control
Improving one’s self-control can be quite effective for reducing impulsive behavior such as excessive smartphone use (79). Smartphone addicts must first become aware of their impulsive behavior and recognize it quickly when it occurs, so that they can activate their self-control systems to regulate it. Self-control can be regarded as a finite resource that can be increased through meditation, slow breathing, adequate sleep, and regular exercise (80–88). Developing good habits or automated behaviors can reduce the strain on finite self-control resources, reducing the risk of impulsive behavior (89).
Enhancing the self-control of university students can bring benefits that extend beyond smartphone use, improving their self-management ability in various domains of university life, when they no longer receive constant management from school officials or family members. Even so, parents should continue to support their children in enhancing self-control at university, such as by helping them to identify their shortcomings and to correct impulsive or unproductive behaviors (90, 91).
The efforts of parents should be complemented by those of psychological health centers at universities (45), which can provide education aimed at increasing self-control and inhibiting impulsivity, routine screening for smartphone addiction, and monitoring of students based on their level of dependency with the help of a continuously updated database (92). Health centers should promote awareness of self-control and the need to enhance it through activities off-line and on-line via official social media accounts (Figure 4).
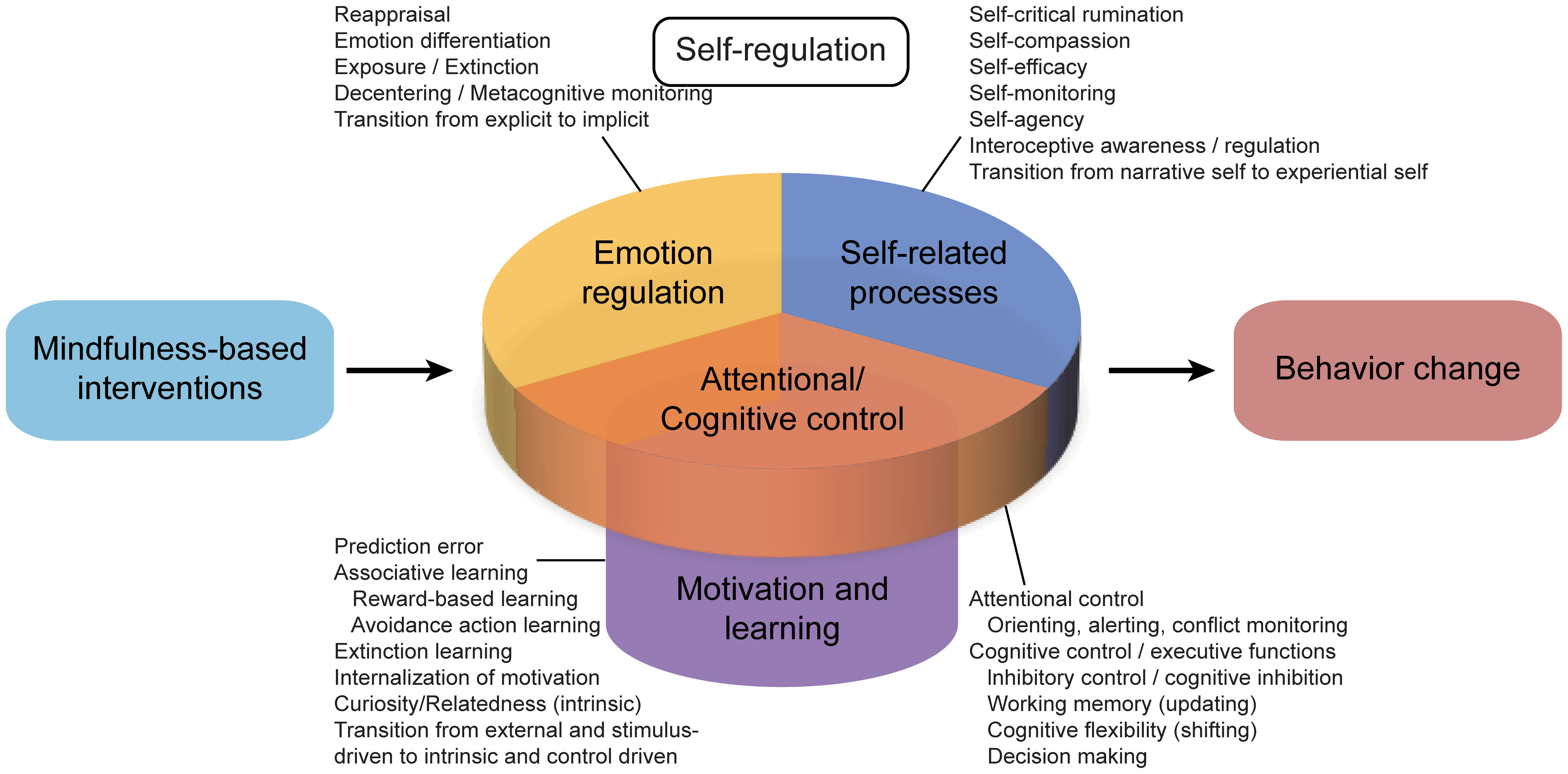
Figure 4. Mindfulness influences on self-regulation and behavior change.
4.4 Engaging in exercise
A longitudinal study of 100 students 18–25 years old in Europe showed that after engaging in physical exercise for four weeks, most showed higher concentration, less lazy attitudes, and faster brain processing (93). A study of 3,000 adolescents in US showed that those who walked more during one week showed better attention. While these benefits of exercise can be detected even after occasional walks or jogging, consistent exercise for several weeks or months is necessary in order to effectively improve executive function (94, 95). One study found that university students in US could reduce their anxiety by walking 20 min per day, three times a week during two weeks, and the reduction persisted for up to one week after students stopped exercising (96). In that study, even stronger and equally persistent reduction was observed in a group of students who ran at high intensity for 20 min rather than walked during the two weeks. A review of nearly 100 studies judged to be rigorous concluded that walking, yoga, running, and muscle exercises can enhance cognition in adults xxx, particularly when the exercise is consistent (97). One study suggests that optimal effects can be achieved by engaging in at least 52 hours of exercise within six months, which breaks down to three 45-minute sessions per week. While low-intensity exercise such as leisure walking already brings benefits, exercise may be more effective when it increases heart rate (98).
Why does exercise enhance focus? It may be because our ancestors needed to concentrate intensely during hunting or when avoiding predators, and these activities may easily occupied them for 2–3 hours per day (99). Since most of us do not require such sustained, intensive concentration for survival, we need to use exercise and physical activity to stimulate the brain’s ancient mechanism of concentration (Figures 5, 6).
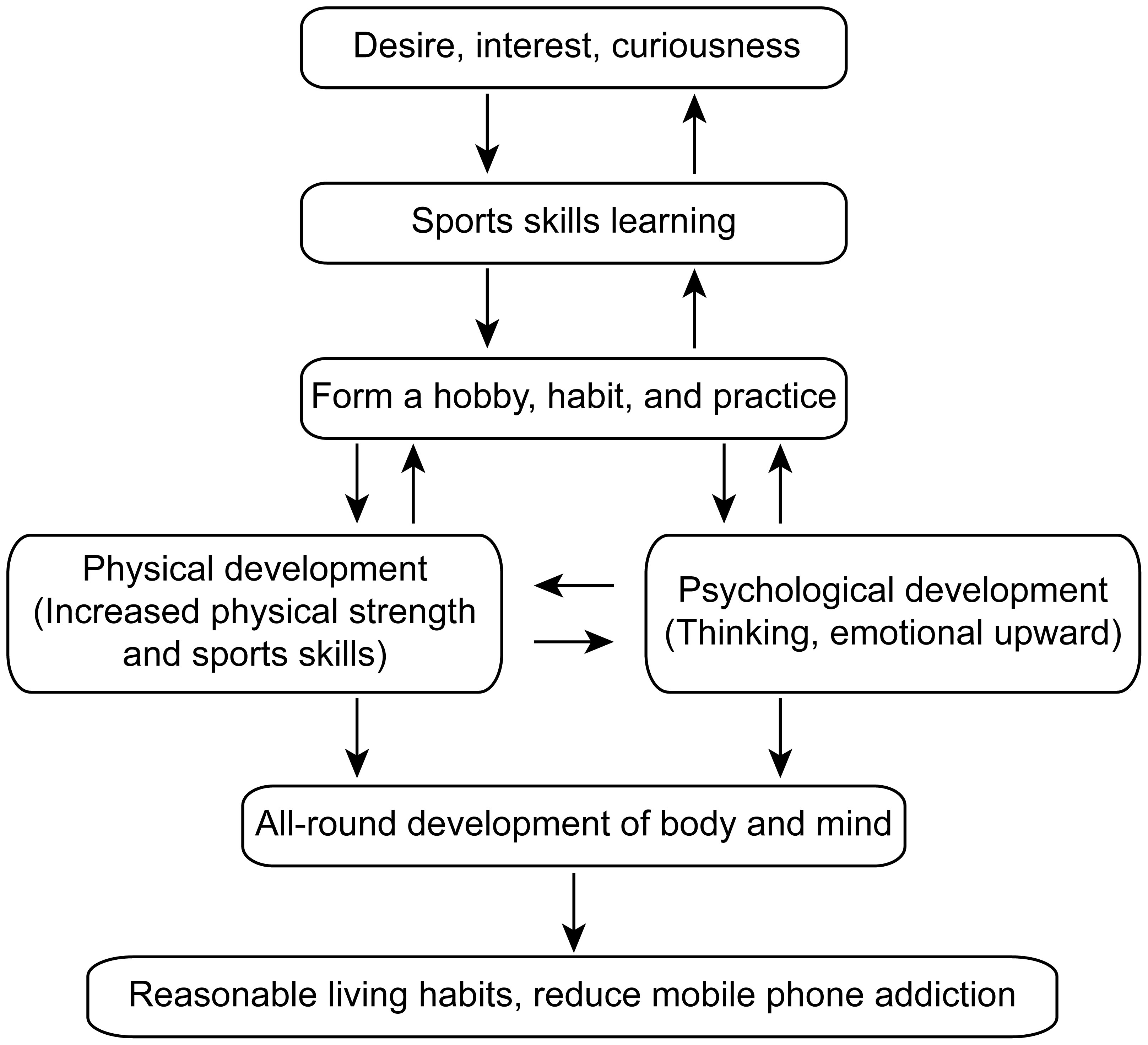
Figure 5. The relationship between sports skills and reducing mobile phone addiction.
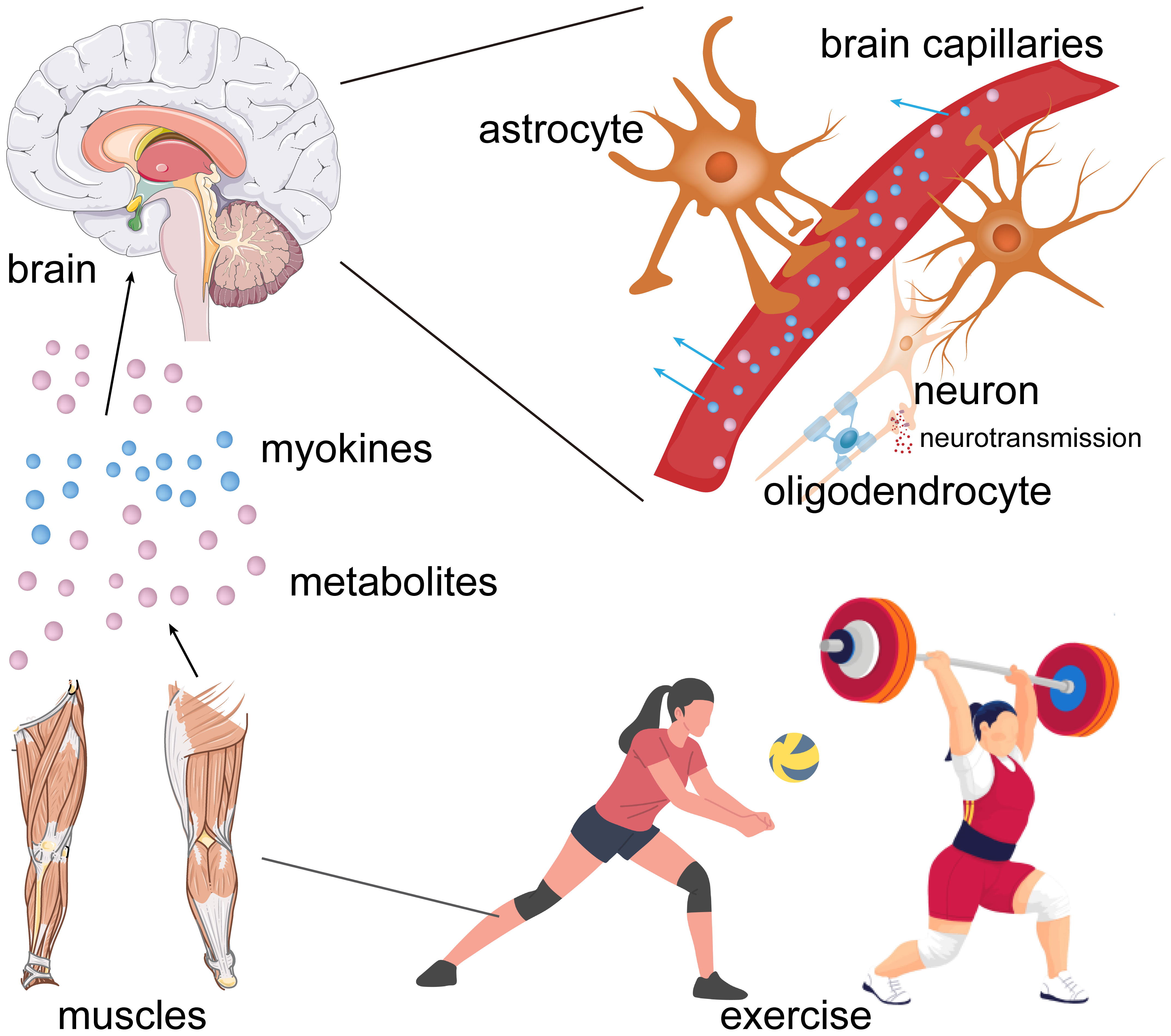
Figure 6. Possible pathway for the exercise-mediated effects on brain functions.
Despite the obvious benefits of exercise, our modern lifestyle has led adults and young people alike to reduce their physical activity, and a major culprit is digital devices such as smartphones (100). While several strategies have emerged to mitigate or even prevent smartphone addiction, such as controlling smartphone use, enhancing self-control and exercising, future research should continue to explore risk factors for smartphone addiction as well as effective prevention measures and treatments. Of course, when controlling smartphone use, smartphone addicts may experience some physical and psychological discomforts. Smartphone addicts who suddenly reduce their phone use may experience withdrawal - like symptoms, including restlessness, anxiety, and a sense of being at a loss. This is because the brain has become accustomed to the stimulation and rewards from smartphone use, and the sudden change disrupts the neural pathways and chemical balances related to addiction (76).
Author contributions
XS: Writing – original draft. WZ: Writing – original draft, Writing – review & editing, Data curation, Methodology, Supervision, Conceptualization, Formal analysis, Project administration, Validation, Investigation. YZ: Data curation, Writing – review & editing. YL: Writing – original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by the National Natural Science Foundation of China (U1804179).
Acknowledgments
We greatly appreciate the time of Yang Xinglong for critical reading of our manuscript and for his contributions and suggestions. We thank Zhang Yu for her illustration contributions to this work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sahu M, Gandhi S, and Sharma MK. Mobile phone addiction among children and adolescents: A systematic review. J Addict Nurs. (2019) 30:261–8. doi: 10.1097/JAN.0000000000000309
2. Hong W, Liu RD, Ding Y, Sheng X, and Zhen R. Mobile phone addiction and cognitive failures in daily life: The mediating roles of sleep duration and quality and the moderating role of trait self-regulation. Addict Behav. (2020) 107:106383. doi: 10.1016/j.addbeh.2020.106383
3. De-Sola Gutierrez J, Rodriguez de Fonseca F, and Rubio G. Cell-phone addiction: A review. Front Psychiatry. (2016) 7:175. doi: 10.3389/fpsyt.2016.00175
4. Lu L, Xu DD, Liu HZ, Zhang L, Ng CH, Ungvari GS, et al. Mobile phone addiction in Tibetan and Han Chinese adolescents. Perspect Psychiatr Care. (2019) 55:438–44. doi: 10.1111/ppc.12336
5. Thapa K, Lama S, Pokharel R, Sigdel R, and Rimal SP. Mobile phone dependence among undergraduate students of a medical college of eastern Nepal: A descriptive cross-sectional study. JNMA J Nepal Med Assoc. (2020) 58:234–9. doi: 10.31729/jnma.4787
6. Bertocchi FM, De Oliveira AC, Lucchetti G, and Lucchetti ALG. Smartphone use, digital addiction and physical and mental health in community-dwelling older adults: a population-based survey. J Med Syst. (2022) 46:53. doi: 10.1007/s10916-022-01839-7
7. Nakshine VS, Thute P, Khatib MN, and Sarkar B. Increased screen time as a cause of declining physical, psychological health, and sleep patterns: A literary review. Cureus. (2022) 14:e30051. doi: 10.7759/cureus.30051
8. Li G, Xie J, An L, Hou G, Jian H, and Wang W. A generalizability analysis of the mobile phone addiction tendency scale for chinese college students. Front Psychiatry. (2019) 10:241. doi: 10.3389/fpsyt.2019.00241
9. Saha I, Som TK, Choudhury S, Ghose G, and Patra M. Mobile phone involvement and dependence among college students. J Assoc Phys India. (2018) 66:104.
10. Kaya F, Bostanci Dastan N, and Durar E. Smart phone usage, sleep quality and depression in university students. Int J Soc Psychiatry. (2021) 67:407–14. doi: 10.1177/0020764020960207
11. Chen PS, Li J, and Kim SY. Structural relationship among mobile phone dependence, self-efficacy, time management disposition, and academic procrastination in college students. Iran J Public Health. (2021) 50(11):2263–73. doi: 10.18502/ijph.v50i11.7582
12. Ochoa-Brezmes J, Ruiz-Hernandez A, Blanco-Ocampo D, Garcia-Lara GM, and Garach-Gomez A. Mobile phone use, sleep disorders and obesity in a social exclusion zone. Pediatr (Engl Ed). (2023) 98:344–52. doi: 10.1016/j.anpede.2022.12.004
13. Laurence PG, Busin Y, da Cunha Lima HS, and Macedo EC. Predictors of problematic smartphone use among university students. Psicol Reflex Crit. (2020) 33:8. doi: 10.1186/s41155-020-00147-8
14. Fransson A, Choliz M, and Hakansson A. Addiction-like mobile phone behavior - validation and association with problem gambling. Front Psychol. (2018) 9:655. doi: 10.3389/fpsyg.2018.00655
15. Jeon M, Lee MS, Yoon JY, and Bhang SY. Mental health literacy of Internet gaming disorder and problematic smartphone use among Korean teenagers. PloS One. (2022) 17:e0270988. doi: 10.1371/journal.pone.0270988
16. Seo BK, Hwang Y, and Cho H. Mental health and personality characteristics of university students at risk of smartphone overdependence. Int J Environ Res Public Health. (2023) 20(3):2331. doi: 10.3390/ijerph20032331
17. Woo KS, Bong SH, Choi TY, and Kim JW. Mental health, smartphone use type, and screen time among adolescents in South Korea. Psychol Res Behav Manag. (2021) 14:1419–28. doi: 10.2147/PRBM.S324235
18. Lai JH, Zhu YS, Huo ZH, Sun RF, Yu B, Wang YP, et al. Association study of polymorphisms in the promoter region of DRD4 with schizophrenia, depression, and heroin addiction. Brain Res. (2010) 1359:227–32. doi: 10.1016/j.brainres.2010.08.064
19. Masiak J, Chmielowiec J, Chmielowiec K, and Grzywacz A. DRD4, DRD2, DAT1, and ANKK1 genes polymorphisms in patients with dual diagnosis of polysubstance addictions. J Clin Med. (2020) 9(11):3593. doi: 10.3390/jcm9113593
20. Choi HD and Shin WG. Meta-analysis of the association between a serotonin transporter 5-HTTLPR polymorphism and smoking cessation. Psychiatr Genet. (2016) 26:87–91. doi: 10.1097/YPG.0000000000000116
21. Ng KC, Wu LH, Lam HY, Lam LK, Nip PY, Ng CM, et al. The relationships between mobile phone use and depressive symptoms, bodily pain, and daytime sleepiness in Hong Kong secondary school students. Addict Behav. (2020) 101:105975. doi: 10.1016/j.addbeh.2019.04.033
22. Jiang Z and Zhao X. Self-control and problematic mobile phone use in Chinese college students: the mediating role of mobile phone use patterns. BMC Psychiatry. (2016) 16:416. doi: 10.1186/s12888-016-1131-z
23. Li L, Lok GKI, Mei SL, Cui XL, Li L, Ng CH, et al. The severity of mobile phone addiction and its relationship with quality of life in Chinese university students. PeerJ. (2020) 8:e8859. doi: 10.7717/peerj.8859
24. Snyder SH. What dopamine does in the brain. Proc Natl Acad Sci U.S.A. (2011) 108:18869–71. doi: 10.1073/pnas.1114346108
25. Barker RA. consortium T: Designing stem-cell-based dopamine cell replacement trials for Parkinson’s disease. Nat Med. (2019) 25:1045–53. doi: 10.1038/s41591-019-0507-2
26. Tong WX, Li B, Han SS, Han YH, Meng SQ, Guo Q, et al. Current status and correlation of physical activity and tendency to problematic mobile phone use in college students. Int J Environ Res Public Health. (2022) 19(23):15849. doi: 10.3390/ijerph192315849
27. Chen C, Shen Y, Lv S, Wang B, and Zhu Y. The relationship between self-esteem and mobile phone addiction among college students: The chain mediating effects of social avoidance and peer relationships. Front Psychol. (2023) 14:1137220. doi: 10.3389/fpsyg.2023.1137220
28. Badgaiyan RD. Imaging dopamine neurotransmission in live human brain. Prog Brain Res. (2014) 211:165–82. doi: 10.1016/B978-0-444-63425-2.00007-6
29. Ayres TC and Taylor S. Drug addiction: failure, feast and phoenix. Int J Environ Res Public Health. (2025) 22(3):370. doi: 10.3390/ijerph22030370
30. Mehr SR, Nakhaei B, Soleimani H, Madadlou SK, Abbasi Maleky A, and Abbasi-Maleki S. Addiction and stress: Exploring the reward pathways in brain affected by different drugs. Prog Brain Res. (2025) 291:381–404. doi: 10.1016/bs.pbr.2025.01.012
31. Lin CY, Ratan ZA, and Pakpour AH. Collection of smartphone and internet addiction. BMC Psychiatry. (2023) 23:427. doi: 10.1186/s12888-023-04915-5
32. Wu MN, Ho K, Crocker A, Yue Z, Koh K, and Sehgal A. The effects of caffeine on sleep in Drosophila require PKA activity, but not the adenosine receptor. J Neurosci. (2009) 29:11029–37. doi: 10.1523/JNEUROSCI.1653-09.2009
33. Nedergaard M and Goldman SA. Glymphatic failure as a final common pathway to dementia. Science. (2020) 370:50–6. doi: 10.1126/science.abb8739
34. Li L, Wang L, and Wang X. Effect of smartphone use before bedtime on smartphone addiction behaviors among Chinese college students. Front Psychol. (2022) 13:1023245. doi: 10.3389/fpsyg.2022.1023245
35. Ibrahim NK, Baharoon BS, Banjar WF, Jar AA, Ashor RM, Aman AA, et al. Mobile phone addiction and its relationship to sleep quality and academic achievement of medical students at king abdulaziz university, jeddah, Saudi Arabia. J Res Health Sci. (2018) 18:e00420.
36. Li Y, Li G, Liu L, and Wu H. Correlations between mobile phone addiction and anxiety, depression, impulsivity, and poor sleep quality among college students: A systematic review and meta-analysis. J Behav Addict. (2020) 9:551–71. doi: 10.1556/2006.2020.00057
37. Khan MA and Al-Jahdali H. The consequences of sleep deprivation on cognitive performance. Neurosci (Riyadh). (2023) 28:91–9. doi: 10.17712/nsj.2023.2.20220108
38. Smith HAB, Besunder JB, Betters KA, Johnson PN, Srinivasan V, Stormorken A, et al. 2022 society of critical care medicine clinical practice guidelines on prevention and management of pain, agitation, neuromuscular blockade, and delirium in critically ill pediatric patients with consideration of the ICU environment and early mobility. Pediatr Crit Care Med. (2022) 23:e74–e110. doi: 10.1097/PCC.0000000000002873
39. Gao X, Li C, Han B, Xu P, and Qu C. The relationship between health belief and sleep quality of Chinese college students: The mediating role of physical activity and moderating effect of mobile phone addiction. Front Public Health. (2023) 11:1108911. doi: 10.3389/fpubh.2023.1108911
40. Xie G, Wu Q, Guo X, Zhang J, and Yin D. Psychological resilience buffers the association between cell phone addiction and sleep quality among college students in Jiangsu Province, China. Front Psychiatry. (2023) 14:1105840. doi: 10.3389/fpsyt.2023.1105840
41. Satyanarayanan SK, Su H, Lin YW, and Su KP. Circadian rhythm and melatonin in the treatment of depression. Curr Pharm Des. (2018) 24:2549–55. doi: 10.2174/1381612824666180803112304
42. Choi Y, Nakamura Y, Akazawa N, Park I, Kwak HB, Tokuyama K, et al. Effects of nocturnal light exposure on circadian rhythm and energy metabolism in healthy adults: A randomized crossover trial. Chronobiol Int. (2022) 39:602–12. doi: 10.1080/07420528.2021.2014517
43. Bonmati-Carrion MA, Arguelles-Prieto R, Martinez-Madrid MJ, Reiter R, Hardeland R, Rol MA, et al. Protecting the melatonin rhythm through circadian healthy light exposure. Int J Mol Sci. (2014) 15:23448–500. doi: 10.3390/ijms151223448
44. Bi J. The relationship between mobile phone anxiety and sleep quality occupational therapy in adolescents and its internal mechanism. Occup Ther Int. (2022) 2022:8489077. doi: 10.1155/2022/8489077
45. Zhang X, Gao F, Kang Z, Zhou H, Zhang J, Li J, et al. Perceived academic stress and depression: the mediation role of mobile phone addiction and sleep quality. Front Public Health. (2022) 10:760387. doi: 10.3389/fpubh.2022.760387
46. Emodi-Perlman A, Hochhauser T, Winocur P, Friedman-Rubin P, and Eli I. The effect of smartphones on daytime sleepiness, temporomandibular disorders, and bruxism among young adults. Quintessence Int. (2021) 52:548–59. doi: 10.3290/j.qi.b1244431
47. Ratan ZA, Parrish AM, Zaman SB, Alotaibi MS, and Hosseinzadeh H. Smartphone addiction and associated health outcomes in adult populations: A systematic review. Int J Environ Res Public Health. (2021) 18(22):12257. doi: 10.3390/ijerph182212257
48. Meng SQ, Cheng JL, Li YY, Yang XQ, Zheng JW, Chang XW, et al. Global prevalence of digital addiction in general population: A systematic review and meta-analysis. Clin Psychol Rev. (2022) 92:102128. doi: 10.1016/j.cpr.2022.102128
49. Ding Y, Wan X, Lu G, Huang H, Liang Y, Yu J, et al. The associations between smartphone addiction and self-esteem, self-control, and social support among Chinese adolescents: A meta-analysis. Front Psychol. (2022) 13:1029323. doi: 10.3389/fpsyg.2022.1029323
50. Matar Boumosleh J and Jaalouk D. Depression, anxiety, and smartphone addiction in university students- A cross sectional study. PloS One. (2017) 12:e0182239. doi: 10.1371/journal.pone.0182239
51. Gligor S and Mozos I. Indicators of smartphone addiction and stress score in university students. Wien Klin Wochenschr. (2019) 131:120–5. doi: 10.1007/s00508-018-1373-5
52. Zou L, Wu X, Tao S, Yang Y, Zhang Q, Hong X, et al. Neural correlates of physical activity moderate the association between problematic mobile phone use and psychological symptoms. Front Behav Neurosci. (2021) 15:749194. doi: 10.3389/fnbeh.2021.749194
53. Zhao C, He J, Du M, Xu H, Lai X, Yu G, et al. A cross-lagged study of the associations among problematic smartphone use, depressive symptoms, and suicidal ideation in chinese university students. Curr Psychol. 2023:1–12. doi: 10.1007/s12144-023-04560-x
54. Wang R, Yang R, Ran H, Xu X, Yang G, Wang T, et al. Mobile phone addiction and non-suicidal self-injury among adolescents in China. PeerJ. (2022) 10:e14057. doi: 10.7717/peerj.14057
55. Pearce M, Garcia L, Abbas A, Strain T, Schuch FB, Golubic R, et al. Association between physical activity and risk of depression: A systematic review and meta-analysis. JAMA Psychiatry. (2022) 79:550–9. doi: 10.1001/jamapsychiatry.2022.0609
56. Twenge JM and Campbell WK. Associations between screen time and lower psychological well-being among children and adolescents: Evidence from a population-based study. Prev Med Rep. (2018) 12:271–83. doi: 10.1016/j.pmedr.2018.10.003
57. Lian SL, Sun XJ, Niu GF, Yang XJ, Zhou ZK, and Yang C. Mobile phone addiction and psychological distress among Chinese adolescents: The mediating role of rumination and moderating role of the capacity to be alone. J Affect Disord. (2021) 279:701–10. doi: 10.1016/j.jad.2020.10.005
58. Tian H and Wang Y. Mobile phone addiction and sleep quality among older people: the mediating roles of depression and loneliness. Behav Sci (Basel). (2023) 13(2):153. doi: 10.3390/bs13020153
59. Gong L and Liu Q. Mobile phone addiction and sleep quality: the mediating role of anxiety and the moderating role of emotion regulation. Behav Sci (Basel). (2023) 13(3):250. doi: 10.3390/bs13030250
60. Zhang Y, Li Y, Xia M, Han M, Yan L, and Lian S. The relationship between loneliness and mobile phone addiction among Chinese college students: The mediating role of anthropomorphism and moderating role of family support. PloS One. (2023) 18:e0285189. doi: 10.1371/journal.pone.0285189
61. Feng Z, Diao Y, Ma H, Liu M, Long M, Zhao S, et al. Mobile phone addiction and depression among Chinese medical students: the mediating role of sleep quality and the moderating role of peer relationships. BMC Psychiatry. (2022) 22:567. doi: 10.1186/s12888-022-04183-9
62. Park S and Yoo JY. A study on smartphone dependence and depression in Korean high school students. Med (Baltimore). (2023) 102:e33354. doi: 10.1097/MD.0000000000033354
63. Li X, Zhang W, Li W, Wang S, and Pan D. Impact of smartphone dependence on depression in Chinese adolescents with a moderated mediation model. Sci Rep. (2025) 15:15589. doi: 10.1038/s41598-025-00276-z
64. Jo S, Baek IC, Fava M, Mischoulon D, Hong JP, Kim H, et al. Association of smartphone overuse with depression, anxiety, and other addictive behaviors: A nationwide community sample of Korean adults. Psychiatry Res. (2021) 304:114133. doi: 10.1016/j.psychres.2021.114133
65. Khan A, McLeod G, Hidajat T, and Edwards EJ. Excessive smartphone use is associated with depression, anxiety, stress, and sleep quality of Australian adults. J Med Syst. (2023) 47:109. doi: 10.1007/s10916-023-02005-3
66. Yang J, Fu X, Liao X, and Li Y. Association of problematic smartphone use with poor sleep quality, depression, and anxiety: A systematic review and meta-analysis. Psychiatry Res. (2020) 284:112686. doi: 10.1016/j.psychres.2019.112686
67. Thorburn E, Pope R, and Wang S. Musculoskeletal symptoms among adult smartphone and tablet device users: a retrospective study. Arch Physiother. (2021) 11:1. doi: 10.1186/s40945-020-00096-6
68. Young JG, Trudeau M, Odell D, Marinelli K, and Dennerlein JT. Touch-screen tablet user configurations and case-supported tilt affect head and neck flexion angles. Work. (2012) 41:81–91. doi: 10.3233/WOR-2012-1337
69. Xu HWB and Wu Z. Pupils in Zhuhai city are using smart phone behavior and low vision analysis. Henan J Prev Med. (2020) 30:5.
70. Huang XQ, Li MC, and Tao R. Treatment of internet addiction. Curr Psychiatry Rep. (2010) 12:462–70. doi: 10.1007/s11920-010-0147-1
71. Santos VA, Freire R, Zugliani M, Cirillo P, Santos HH, Nardi AE, et al. Treatment of internet addiction with anxiety disorders: treatment protocol and preliminary before-after results involving pharmacotherapy and modified cognitive behavioral therapy. JMIR Res Protoc. (2016) 5:e46. doi: 10.2196/resprot.5278
72. Ritvo P, Knyahnytska Y, Pirbaglou M, Wang W, Tomlinson G, Zhao H, et al. Katz J et al: Online Mindfulness-Based Cognitive Behavioral Therapy Intervention for Youth With Major Depressive Disorders: Randomized Controlled Trial. J Med Internet Res. (2021) 23:e24380. doi: 10.2196/24380
73. Bong SH, Won GH, and Choi TY. Effects of cognitive-behavioral therapy based music therapy in korean adolescents with smartphone and internet addiction. Psychiatry Investig. (2021) 18:110–7. doi: 10.30773/pi.2020.0155
74. Cuppone D, Gomez Perez LJ, Cardullo S, Cellini N, Sarlo M, Soldatesca S, et al. The role of repetitive transcranial magnetic stimulation (rTMS) in the treatment of behavioral addictions: Two case reports and review of the literature. J Behav Addict. (2021) 10:361–70. doi: 10.1556/2006.2021.00032
75. Abou El-Magd RM, Obuobi-Donkor G, Adu MK, Lachowski C, Duddumpudi S, Lawal MA, et al. Repetitive transcranial magnetic stimulation with and without internet-delivered cognitive-behavioral therapy for the treatment of resistant depression: protocol for patient-centered randomized controlled pilot trial. JMIR Res Protoc. (2020) 9:e18843. doi: 10.2196/18843
76. He JW, Tu ZH, Xiao L, Su T, and Tang YX. Effect of restricting bedtime mobile phone use on sleep, arousal, mood, and working memory: A randomized pilot trial. PloS One. (2020) 15:e0228756. doi: 10.1371/journal.pone.0228756
77. Han Y, Qin G, Han S, Ke Y, Meng S, Tong W, et al. Effect of mobile phone addiction on physical exercise in university students: moderating effect of peer relationships. Int J Environ Res Public Health. (2023) 20(3):2685. doi: 10.3390/ijerph20032685
78. Shi M, Zhai X, Li S, Shi Y, and Fan X. The relationship between physical activity, mobile phone addiction, and irrational procrastination in chinese college students. Int J Environ Res Public Health. (2021) 18(10):5325. doi: 10.3390/ijerph18105325
79. Li GR, Sun J, Ye JN, Hou XH, and Xiang MQ. Family functioning and mobile phone addiction in university students: Mediating effect of loneliness and moderating effect of capacity to be alone. Front Psychol. (2023) 14:1076852. doi: 10.3389/fpsyg.2023.1076852
80. Lian SL, Cao XX, Xiao QL, Zhu XW, Yang C, and Liu QQ. Family cohesion and adaptability reduces mobile phone addiction: the mediating and moderating roles of automatic thoughts and peer attachment. Front Psychol. (2023) 14:1122943. doi: 10.3389/fpsyg.2023.1122943
81. Geng Y, Gu J, Wang J, and Zhang R. Smartphone addiction and depression, anxiety: The role of bedtime procrastination and self-control. J Affect Disord. (2021) 293:415–21. doi: 10.1016/j.jad.2021.06.062
82. Di Liegro CM, Schiera G, Proia P, and Di Liegro I. Physical activity and brain health. Genes (Basel). (2019) 10(9):720. doi: 10.3390/genes10090720
83. Kandola A, Ashdown-Franks G, Hendrikse J, Sabiston CM, and Stubbs B. Physical activity and depression: Towards understanding the antidepressant mechanisms of physical activity. Neurosci Biobehav Rev. (2019) 107:525–39. doi: 10.1016/j.neubiorev.2019.09.040
84. Wielgosz J, Goldberg SB, Kral TRA, Dunne JD, and Davidson RJ. Mindfulness meditation and psychopathology. Annu Rev Clin Psychol. (2019) 15:285–316. doi: 10.1146/annurev-clinpsy-021815-093423
85. Hofmann SG and Gomez AF. Mindfulness-based interventions for anxiety and depression. Psychiatr Clin North Am. (2017) 40:739–49. doi: 10.1016/j.psc.2017.08.008
86. Creswell JD. Mindfulness interventions. Annu Rev Psychol. (2017) 68:491–516. doi: 10.1146/annurev-psych-042716-051139
87. Schmidt S. Mindfulness and healing intention: concepts, practice, and research evaluation. J Altern Complement Med. (2004) 10 Suppl 1:S7–14. doi: 10.1089/1075553042245917
88. Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen Hosp Psychiatry. (1982) 4:33–47. doi: 10.1016/0163-8343(82)90026-3
89. Singh G, Manjunatha N, Rao S, Shashidhara HN, Moirangthem S, Madegowda RK, et al. Use of Mobile Phone Technology to Improve follow-up at a Community Mental Health Clinic: A Randomized Control Trial. Indian J Psychol Med. (2017) 39:276–80. doi: 10.4103/0253-7176.207325
90. Huang Q, Lin S, Li Y, Huang S, Liao Z, Chen X, et al. Suicidal ideation is associated with excessive smartphone use among chinese college students. Front Public Health. (2021) 9:809463. doi: 10.3389/fpubh.2021.809463
91. Jalali N, Sahu KS, Oetomo A, and Morita PP. Usability of smart home thermostat to evaluate the impact of weekdays and seasons on sleep patterns and indoor stay: observational study. JMIR Mhealth Uhealth. (2022) 10:e28811. doi: 10.2196/28811
92. Zhang A, Xiong S, Peng Y, Zeng Y, Zeng C, Yang Y, et al. Perceived stress and mobile phone addiction among college students: The roles of self-control and security. Front Psychiatry. (2022) 13:1005062. doi: 10.3389/fpsyt.2022.1005062
93. Lu T, Wang C, Chen H, Tao B, Jiang Y, Sui H, et al. Relationship between university students’ physical activity and mobile phone dependence: Mediating effect of subjective well-being and moderating effect of psychological capital. Front Psychol. (2022) 13:983487. doi: 10.3389/fpsyg.2022.983487
94. Buke M, Egesoy H, and Unver F. The effect of smartphone addiction on physical activity level in sports science undergraduates. J Bodyw Mov Ther. (2021) 28:530–4. doi: 10.1016/j.jbmt.2021.09.003
95. Liu H, Soh KG, Samsudin S, Rattanakoses W, and Qi F. Effects of exercise and psychological interventions on smartphone addiction among university students: A systematic review. Front Psychol. (2022) 13:1021285. doi: 10.3389/fpsyg.2022.1021285
96. Chen H, Zhang G, Wang Z, Feng S, and Li H. The associations between daytime physical activity, while-in-bed smartphone use, sleep delay, and sleep quality: A 24-h investigation among chinese college students. Int J Environ Res Public Health. (2022) 19(15):9693. doi: 10.3390/ijerph19159693
97. Liu S, Xiao T, Yang L, and Loprinzi PD. Exercise as an alternative approach for treating smartphone addiction: A systematic review and meta-analysis of random controlled trials. Int J Environ Res Public Health. (2019) 16(20):3912. doi: 10.3390/ijerph16203912
98. Saffari M, Chen JS, Wu HC, Fung XCC, Chang CC, Chang YL, et al. Effects of weight-related self-stigma and smartphone addiction on female university students’ Physical activity levels. Int J Environ Res Public Health. (2022) 19(5):2631. doi: 10.3390/ijerph19052631
99. Kim J and Lee K. The association between physical activity and smartphone addiction in korean adolescents: the 16th korea youth risk behavior web-based survey, 2020. Healthcare (Basel). (2022) 10(4):702. doi: 10.3390/healthcare10040702
Keywords: smartphone dependence, dopamine signaling, sleep, depression, self-control, exercise, mobile phone, cell phone
Citation: Zhu W, Zhang Y, Lan Y and Song X (2025) Smartphone dependence and its influence on physical and mental health. Front. Psychiatry 16:1281841. doi: 10.3389/fpsyt.2025.1281841
Received: 23 August 2023; Accepted: 21 July 2025;
Published: 19 August 2025.
Edited by:
Naohiro Okada, The University of Tokyo Hospital, JapanReviewed by:
Sang-Kyu Lee, Hallym University Medical Center, Republic of KoreaHuiyong Zhang, Henan Agricultural University, China
Copyright © 2025 Zhu, Zhang, Lan and Song. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xinqiang Song, eHFzb25nMjAxMkAxMjYuY29t