Abstract
Background:
Depression carries a high risk of suicide, with many individuals failing to receive treatment due to diagnostic challenges and stigma. Gait is linked to depression, underscoring the importance of gait analysis in the diagnosis and treatment of depression. However, comprehensive and objective evaluations of the current research on gait in depression are lacking. This study aims to use bibliometric analysis and knowledge mapping to clarify research trends and status.
Objective:
This study employs bibliometric analysis to investigate gait in depression, summarizing historical and current trends while predicting future directions. This analysis will aid researchers and policymakers in understanding evolving trends and prioritizing research resources effectively.
Methods:
We conducted a computer-based search of the Web of Science core collection to identify articles and reviews related to depression and gait. Bibliometric analysis, involving the analysis of aspects such as countries or regions, institutions, authors, journals, keywords, and references, was performed using Excel 365, CiteSpace, and VOSViewer.
Results:
The analysis included a total of 848 publications from 2005 to 2024. The results showed a phased increase in publications, peaking in 2020 with 102 publications, followed by a gradual decline. Citations in this field showed a yearly increase, peaking in 2022 with 3920 citations before subsequently declining. The United States was identified as the most productive and influential country in this field, with the highest number of publications and citations. They have the institutions with the highest publications and citations. Leading authors in this field include Verghese Joe, Shimada Hiroyuki; and Rochester Lynn. Key journals include BMC Geriatrics, Journals of Gerontology Series and Medical Sciences, and Journal of the American Geriatrics Society. Frequently mentioned keywords in this field are depression, gait, gait speed, older adults, and dementia. Identification of distinctive gait patterns in depression, gait characteristics in the elderly, association between gait and cognitive decline, and interventions for abnormal gait constitute current research forefronts in this domain.
Conclusions:
This study is the first to utilize bibliometrics to visualize research in the field of gait-related depression. It reveals research trends and frontiers, providing valuable references for scholars seeking important research topics and potential collaborators.
1 Introduction
Depression encompasses enduring feelings of low mood and reduced interest in activities, profoundly interpersonal relationships as well as academic and occupational performance. An estimated 3.8% of the global populace grapples with depression, with this condition affecting 5% of the adult population (comprising 4% of men and 6% of women) (1). Among those aged 60 and above, the prevalence rises to 5.7% (1). Notably, depression occurs approximately 50% more frequently in women compared to men. Globally, over 10% of women experience depression during pregnancy or shortly after giving birth (2).
Depression is associated with decreased life satisfaction, impaired psychosocial functioning, and heightened rates of disability, even leading to suicide. Effective treatments for mental disorders exist; however, more than three-quarters of people in low- and middle-income countries do not receive any form of treatment (3). Furthermore, over half of individuals with depression have not received treatment, often due to challenges in diagnosis (4, 5). Another persistent issue is the use of traditional questionnaire-based approaches for depression, which can increase the risk of misdiagnosis and subsequent inappropriate treatment in primary care settings (6–8). From the patient’s perspective, internalized stigma associated with depression correlates with an intensified emphasis on each identified barrier to treatment, including perceived need, negative treatment expectations, and structural obstacles (9). Furthermore, individuals with depression encounter stigma related to antidepressants, along with significant challenges in accessing antidepressant treatment and in doctor-patient communication (10). Evidence suggests that motor symptoms, including gait abnormalities, are crucial manifestations of depression (11, 12). Specifically, gait and postural control are governed by a complex neural network that is also implicated in the pathophysiology of major depression (13). In their 2012 longitudinal study spanning 16 years among the elderly, Joost B. Sanders and colleagues (14) found that walking speed predicted the onset of depression. Additionally, in subsequent research (15), it has been observed that gait correlates with the severity of depression, achieving an accuracy rate of 84.91% in predicting depression through gait analysis. Recently, Yameng Wang et al. (16) have discovered that individuals suffering from depression demonstrate a distinct gait in contrast to participants in the control group. This is marked by a decelerated walking pace and diminished movements across various parameters, including reduced left-arm swing, right-arm swing, head posture, right stride length, left toe clearance, and right toe clearance.
Bibliometrics is a methodological approach that utilizes qualitative and quantitative methods to analyze, evaluate, and manage literature and information resources (17). It is widely applied across various disciplines (18–20). It integrates techniques from information science, statistics, and computer science, primarily aiming to measure and assess the output, impact, and trends of scientific research (17). Bibliometrics involves analyzing indicators such as citation analysis, author collaboration networks, international collaboration networks, institutional collaboration networks, journal citation analyses, and trends in research topics. It aids researchers and decision-makers in understanding the dynamic changes within academic fields, supporting the formulation of research policies and allocation of resources. Despite the rapid evolution of research into depression-related gait characteristics over the past two decades, there exists a deficiency in contemporary bibliometric analyses. Hence, this study endeavors to undertake a bibliometric analysis of depression-related gait research using VOSviewer and CiteSpace, bibliometric software tools. The objective is to discern trends and cutting-edge focal points over the last twenty years, thereby assisting researchers and policymakers in comprehending the dynamic shifts within the scholarly domain and facilitating informed decisions on research policy and resource allocation.
2 Materials and methods
2.1 Search strategy and data retrieval
The bibliometric analysis in this study is based on data from the Web of Science Core Collection (WOSCC), a widely used academic database (21). Our retrieval methodology employs “TS= (“Depression” OR “Emotional Depression” OR “Depression, Emotional” OR “Depressive Disorder” OR “Depressive Disorders” OR “Disorder, Depressive” OR “Disorders, Depressive” OR “Neurosis, Depressive” OR “Depressive Neuroses” OR “Depressive Neurosis” OR “Neuroses, Depressive” OR “Depression, Endogenous” OR “Depressions, Endogenous” OR “Endogenous Depression” OR “Endogenous Depressions” OR “Melancholia” OR “Melancholias” OR “Unipolar Depression” OR “Depression, Unipolar” OR “Depressions, Unipolar” OR “Unipolar Depressions” OR “Depressive Syndrome” OR “Depressive Syndromes” OR “Syndrome, Depressive” OR “Syndromes, Depressive” OR “Depression, Neurotic” OR “Depressions, Neurotic” OR “Neurotic Depression” OR “Neurotic Depressions”)” AND TS= (“Gait” OR “Gaits”). The most recent search update was performed on June 21, 2024. The analysis encompasses publications spanning from January 1, 2005, to June 21, 2024. Included are 848 documents, restricted to types “article” and “review,” and filtered for English language. These documents were exported in plain text format for further examination.
2.2 Statistical analysis and visualization of data
We employed CiteSpace 6.3.R3 Advanced, developed by Chaomei Chen (22), and VOSviewer, created by Nees Jan van Eck et al. (23), to conduct comprehensive visual analyses. By extracting critical information such as titles, authors, affiliations, countries or regions, publication journals, keywords, and references, we visualized collaborative networks among countries, institutions, and authors, keyword co-occurrence networks, keyword timelines, author and journal co-citation analyses, and reference co-citation analysis. Additionally, Microsoft 365 Excel was utilized for data aggregation, organization, and visualization. As all data utilized in this study were sourced from public databases, ethical review was not required.
3 Results
3.1 Retrieval diagram, annual publications, and citations
We retrieved 965 records from searches spanning 2005 to 2024, with English language and selections limited to articles and reviews. Ultimately, 848 documents were included in the analysis (Figure 1). Figure 2 illustrates the annual publication trends and citation frequencies of gait-related depression articles from 2005 to 2024. The annual publication count demonstrates a fluctuating upward trend, reaching its peak of 102 publications in 2020, followed by a gradual decline. Conversely, the citation frequency of gait-related depression articles shows a steady annual increase, reaching its apex of 3920 citations in 2022 before declining in subsequent years.
Figure 1

Flow diagram.
Figure 2
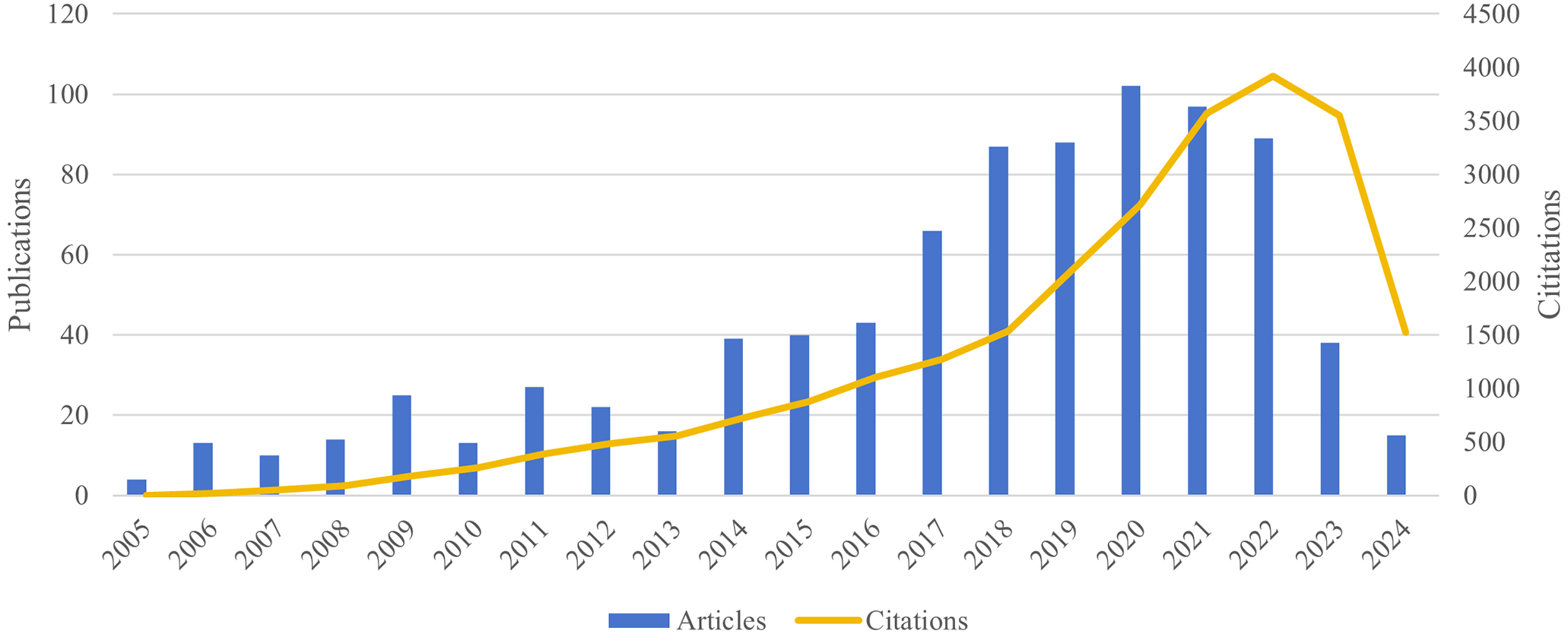
Annual publication output and cumulative citation impact, 2005–2024.
3.2 Distribution of countries or regions
There are a total of 59 countries or regions involved in research on gait-related depression. Table 1 delineates the top 10 countries or regions by publication volume, citation frequency, and the highest average citations per article. The United States (USA) leads in publication volume with 302 articles, while other countries or regions have fewer than 100 publications each. Similarly, the USA tops the citation frequency with 10,683 citations, followed by the United Kingdom with 3,445, Canada with 2,676, and Australia with 2,374 citations; citation frequencies for other countries or regions are below 2,000. Furthermore, Vietnam ranks highest in average citations per article at 76.00, followed closely by Finland at 53.50. All other countries or regions have average citations per article below 50.
Table 1
| Rank | Countries/Regions | Publications | Country/Regions | Citations | Country/Regions | Citations per article |
|---|---|---|---|---|---|---|
| 1 | USA | 302 | USA | 10683 | Vietnam | 76.00 |
| 2 | Canada | 76 | United Kingdom | 3445 | Finland | 53.50 |
| 3 | United Kingdom | 75 | Canada | 2676 | Austria | 49.89 |
| 4 | China | 70 | Australia | 2374 | Israel | 46.53 |
| 5 | Germany | 56 | Germany | 1761 | Argentina | 46.50 |
| 6 | Italy | 56 | Italy | 1617 | Chile | 46.00 |
| 7 | Japan | 56 | Netherlands | 1609 | United Kingdom | 45.93 |
| 8 | Australia | 55 | Japan | 1317 | Netherlands | 43.49 |
| 9 | Brazil | 41 | China | 1274 | Australia | 43.16 |
| 10 | Spain | 38 | Brazil | 1201 | Malaysia | 38.83 |
Top 10 countries or regions by publication count and citation frequency.
Figure 3 depicts the collaboration dynamics among countries and regions engaged in gait-related depression research. Utilizing VOSviewer, these entities are clustered based on the intensity of their collaboration, distinguished by varying colors. The green cluster comprises countries such as USA, China, and Japan; the blue cluster includes Canada, Brazil, and Greece; while the red cluster features the United Kingdom, Italy, and Belgium. Node sizes reflect publication volumes, highlighting larger nodes for countries like USA, United Kingdom, and Canada. The thickness of connecting lines indicates the strength of inter-country collaborations. Results underscore robust ties between the USA and countries such as China, Japan, and Canada, underscoring their pivotal roles in the domain of gait-related depression research.
Figure 3
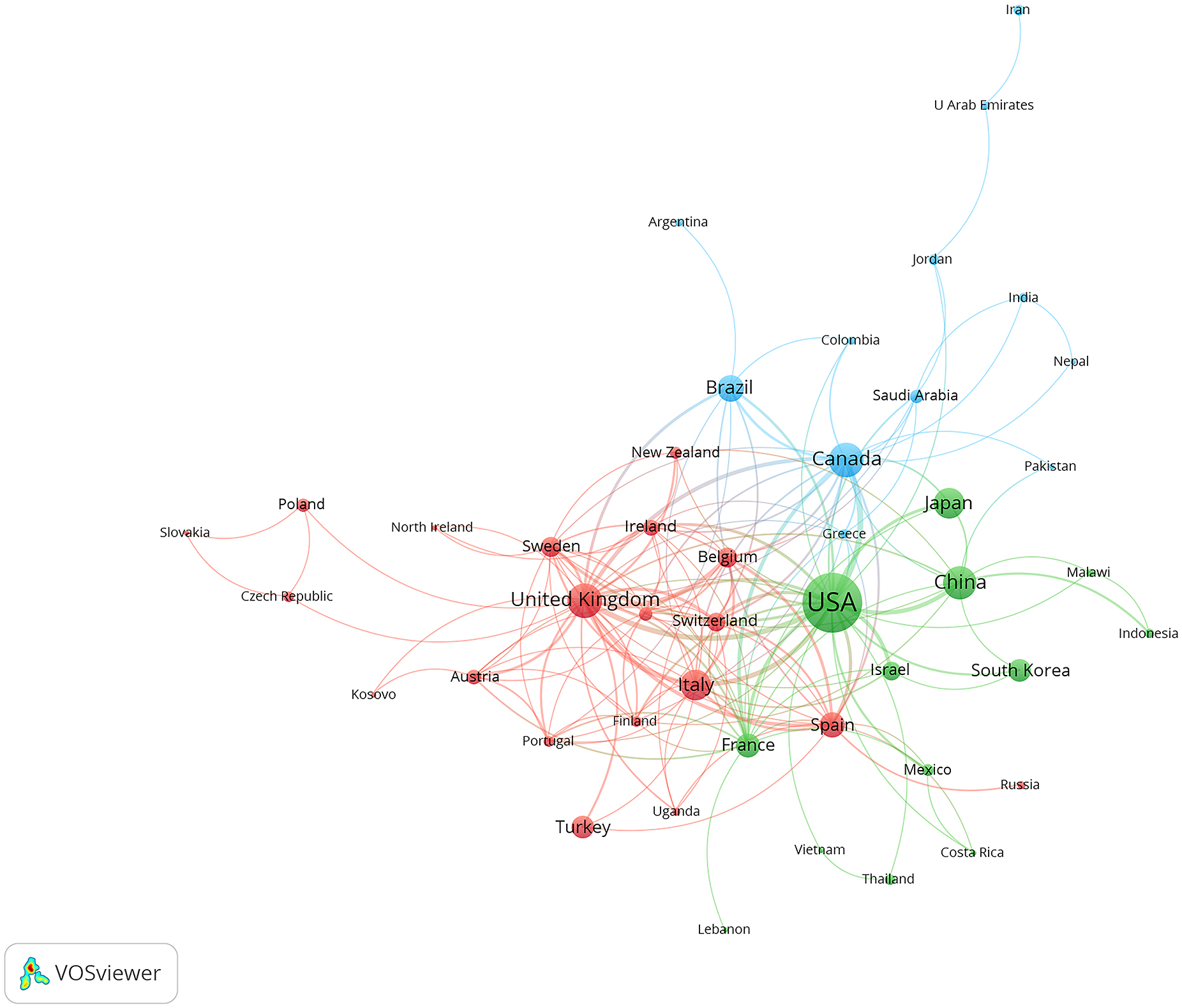
International and regional collaboration network.
3.3 Distribution of institutions
There are 1516 affiliations contributing to research on gait-related depression. Table 2 details the top 10 affiliations by publication count and citation frequency. Leading in publication count is the University of Pittsburgh with 29 articles, followed by the University of California, San Francisco with 21 articles; all other affiliations have fewer than 20 publications. The University of Pittsburgh also tops citation frequency with 1204 citations, while other affiliations have citation frequencies below 1000.
Table 2
| Rank | Institutions | Publications | Institutions | Citations |
|---|---|---|---|---|
| 1 | University of Pittsburgh (USA) | 29 | University of Pittsburgh (USA) | 1204 |
| 2 | University of California, San Francisco (USA) | 21 | University of California, San Francisco (USA) | 902 |
| 3 | Harvard Medical School (USA) | 20 | University of Washington (USA) | 832 |
| 4 | National Center for Geriatrics and Gerontology (Japan) | 20 | Harvard University (USA) | 806 |
| 5 | Columbia University (USA) | 19 | Newcastle University (United Kingdom) | 774 |
| 6 | Albert Einstein College of Medicine (USA) | 18 | National Center for Geriatrics and Gerontology (Japan) | 728 |
| 7 | Duke University (USA) | 17 | Harvard Medical School (USA) | 712 |
| 8 | National Institute on Aging (USA) | 15 | National Institute on Aging (USA) | 709 |
| 9 | University of British Columbia (Canada) | 15 | Tel Aviv University (Israel) | 669 |
| 10 | University of Maryland (USA) | 15 | Queen’s University (Canada) | 578 |
The top 10 institutions by publication volume and citation frequency.
Figure 4 visualizes the collaborative network among institutions engaged in research on gait-related depression. Using VOSviewer, these institutions are categorized into 4 distinct clusters based on the intensity of their collaboration, indicated by different colors. The red cluster includes institutions such as King’s College London, Katholieke Universiteit Leuven, and Newcastle University; the green cluster comprises McGill University, Hebrew SeniorLife, and University of Toronto; the blue cluster features University of Pittsburgh, University of California, San Francisco, and Columbia University; and the yellow cluster includes University of British Columbia, Albert Einstein College of Medicine, and University of Western Ontario. These institutions also represent the nodes with the strongest collaborative ties within their respective clusters. Node sizes reflect the publication volumes, highlighting larger nodes for institutions like University of Pittsburgh, University of California, San Francisco, Harvard Medical School, University of British Columbia, and University of Toronto, which have substantial contributions in this research domain.
Figure 4
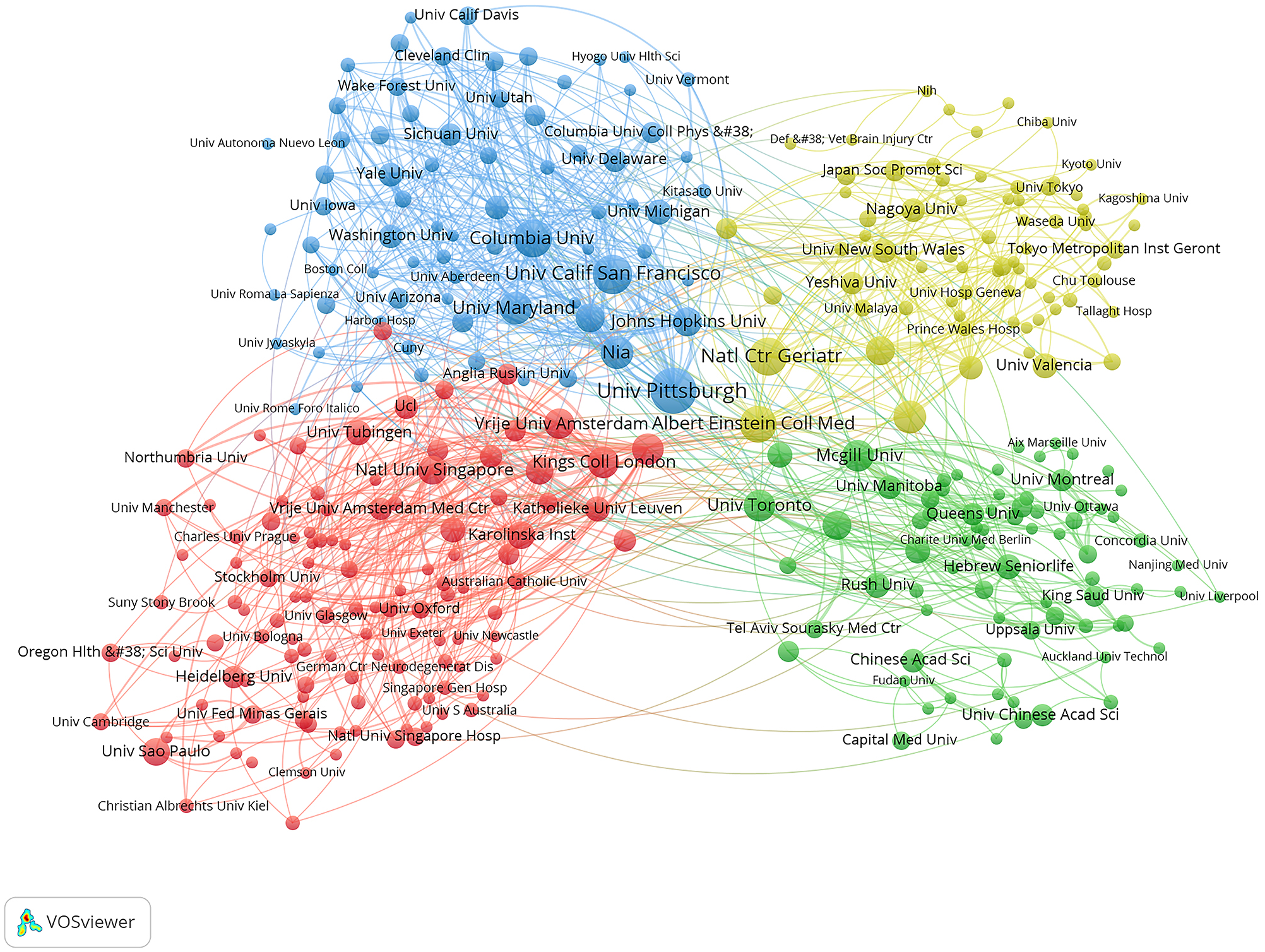
Institutional collaboration network.
3.4 Distribution of authors
By examining the authors with the highest number of publications and co-citation frequencies in gait-related depression research, one can discern the research prowess of these authors as well as the prevailing research trends in this domain. A total of 4,781 authors have engaged in studies on gait-related depression. Table 3 delineates the top 10 authors ranked by publication volume and citation frequency. Verghese, Joe leads with 12 publications, followed by Shimada, Hiroyuki with 11 publications, and Rochester, Lynn with 10 publications, while all other authors have fewer than 10 publications. In terms of citation frequency, Shimada, Hiroyuki ranks highest with 546 citations, followed by Doi, Takehiko with 516 citations, and Tsutsumimoto, Kota with 516 citations; all other authors have fewer than 500 citations.
Table 3
| Rank | Author | Publications | Author | Citations |
|---|---|---|---|---|
| 1 | Verghese, Joe | 12 | Shimada, Hiroyuki | 546 |
| 2 | Shimada, Hiroyuki | 11 | Doi, Takehiko | 516 |
| 3 | Rochester, Lynn | 10 | Tsutsumimoto, Kota | 516 |
| 4 | Brown, Patrick J. | 9 | Makizako, Hyuma | 497 |
| 5 | Lord, Stephen R. | 9 | Michalak, Johannes | 486 |
| 6 | Makizako, Hyuma | 9 | Suzuki, Takao | 480 |
| 7 | Roose, Steven P. | 9 | Herman, Talia | 478 |
| 8 | Rutherford, Bret R. | 9 | Verghese, Joe | 471 |
| 9 | Doi, Takehiko | 8 | Hausdorff, Jeffrey M. | 444 |
| 10 | Tsutsumimoto, Kota | 8 | Rochester, Lynn | 438 |
The top 10 authors by publication volume and citation frequency.
Figure 5a delineates the collaborative network among authors engaged in gait-related depression research. Leveraging VOSviewer, authors are clustered into 10 distinct groups based on the intensity of their collaborations, each represented by a different color. The red cluster encompasses authors such as Hill, Keith D, Brodaty, Henry, and Albert, Steven M; the green cluster includes Doi, Takehiko, Abe, Takafumi, and Akishita, Masahiro; the yellow cluster consists of Abu Alrob, Hajar, Alsaad, Saad M, and Richardson, Julie; the light purple cluster comprises Fanning, Vanessa, Hairi, Farizah, and Mohamad, Zaliton L; the light blue cluster features Brefka, Simone, Casas-Herrero, Alvaro, and Johnson, Mary L; the purple cluster includes Ahmad, Sharifah N, Baldridge, Abigail, and Ayonayon, Hilsa N; the light pink cluster encompasses Houston, Denise K, Jia, Shuli, and Bernhard, Felix P; the blue cluster includes Dean, Catherine M., Dalgas, Ulrik, and Kenneth M; the orange cluster comprises Dong, Birong, Karp, Jordan F., and Elgott, Sara; and the brown cluster includes Neviani, Francesca, Stubbs, Brendon, and Herman, Talia. Node sizes are indicative of the publication volumes of the authors, while the thickness of the connecting lines signifies the strength of the collaborative ties among them. Authors with the highest publication volumes include Verghese, Joe; Shimada, Hiroyuki; and Rochester, Lynn. Overall, the collaborative intensity among authors is relatively modest, with most collaborations occurring within small, closely-knit groups.
Figure 5
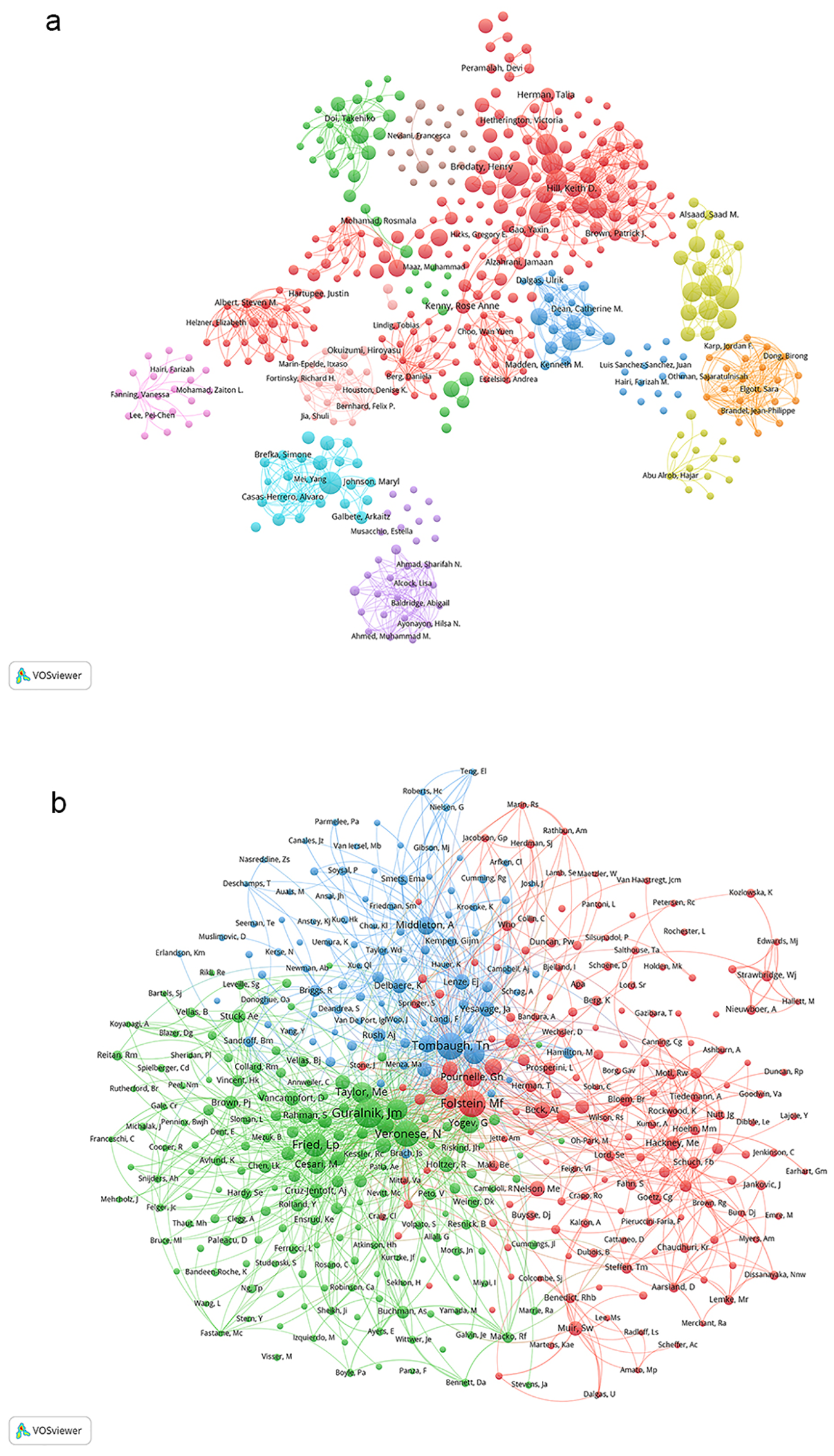
(A) Author collaboration network. (B) Co-citation author network.
Figure 5b illustrates the co-citation network of authors. Leveraging VOSviewer, authors are categorized into three primary clusters based on the intensity of their co-citation relationships, with each cluster denoted by a distinct color. The red cluster encompasses authors such as Folstein, MF; Pournelle, GH; and Bohannon, RW. The green cluster includes authors like Veronese, N; Guralnik, JM; and Fried, LP. The blue cluster features authors such as Tombaugh, TN; Hausdorff, JM; and Louis, ED. The size of the circles in the diagram corresponds to the co-citation frequency of each author, with larger circles indicating higher co-citation weights. The authors are the most highly cited within their respective clusters.
3.5 Distribution of journals
Research on gait-related depression spans across 341 journals. Table 4 presents the top 10 journals ranked by publication volume and citation frequency. BMC Geriatrics leads with 33 publications, followed by Journals of Gerontology Series A-Biological Sciences and Medical with 30 publications; all other journals published fewer than 30 articles. The most cited journals include Journals of Gerontology Series A-Biological Sciences and Medical with 1570 citations, Journal of the American Medical Directors Association with 1125 citations, and Journal of the American Geriatrics Society with 1091 citations; all other journals collectively received fewer than 1000 citations.
Table 4
| Rank | Journals | Publications | Journals | Co-citations |
|---|---|---|---|---|
| 1 | Bmc Geriatrics | 33 | Journals of Gerontology Series A-Biological Sciences and Medical | 1570 |
| 2 | Journals of Gerontology Series A-Biological Sciences and Medical | 30 | Journal of the American Medical Directors Association | 1125 |
| 3 | Journal of the American Geriatrics Society | 29 | Journal of the American Geriatrics Society | 1091 |
| 4 | Plos One | 22 | Movement Disorders | 986 |
| 5 | International Journal of Environmental Research and Public Health | 21 | Archives Of Physical Medicine and Rehabilitation | 729 |
| 6 | American Journal of Geriatric Psychiatry | 20 | Plos One | 672 |
| 7 | Geriatrics & Gerontology International | 20 | American Journal Of Geriatric Psychiatry | 640 |
| 8 | Journal of the American Medical Directors Association | 18 | Nature Reviews Neurology | 566 |
| 9 | Archives of Physical Medicine and Rehabilitation | 17 | Geriatrics & Gerontology International | 389 |
| 10 | Neurorehabilitation | 15 | Bmc Geriatrics | 386 |
The top 10 journals by publication volume and citation frequency.
Figure 6a illustrates the network of journals publishing articles related to gait-related depression research and their interrelationships. Utilizing VOSviewer, these journals are segmented into four distinct color-coded clusters based on their thematic similarities. The red cluster comprises journals such as J Am Geriatr Soc, J Gerontol A-Biol, and Age Ageing. The green cluster includes Movement Disord, Neurology, and J Neurol Neurosurg Psychiatry. The blue cluster encompasses Arch Phys Med Rehab, Gait Posture, and Stroke. Lastly, the yellow cluster features journals like PLOS ONE, Am J Geriatr Psychiat, and J Affect Disorders.
Figure 6
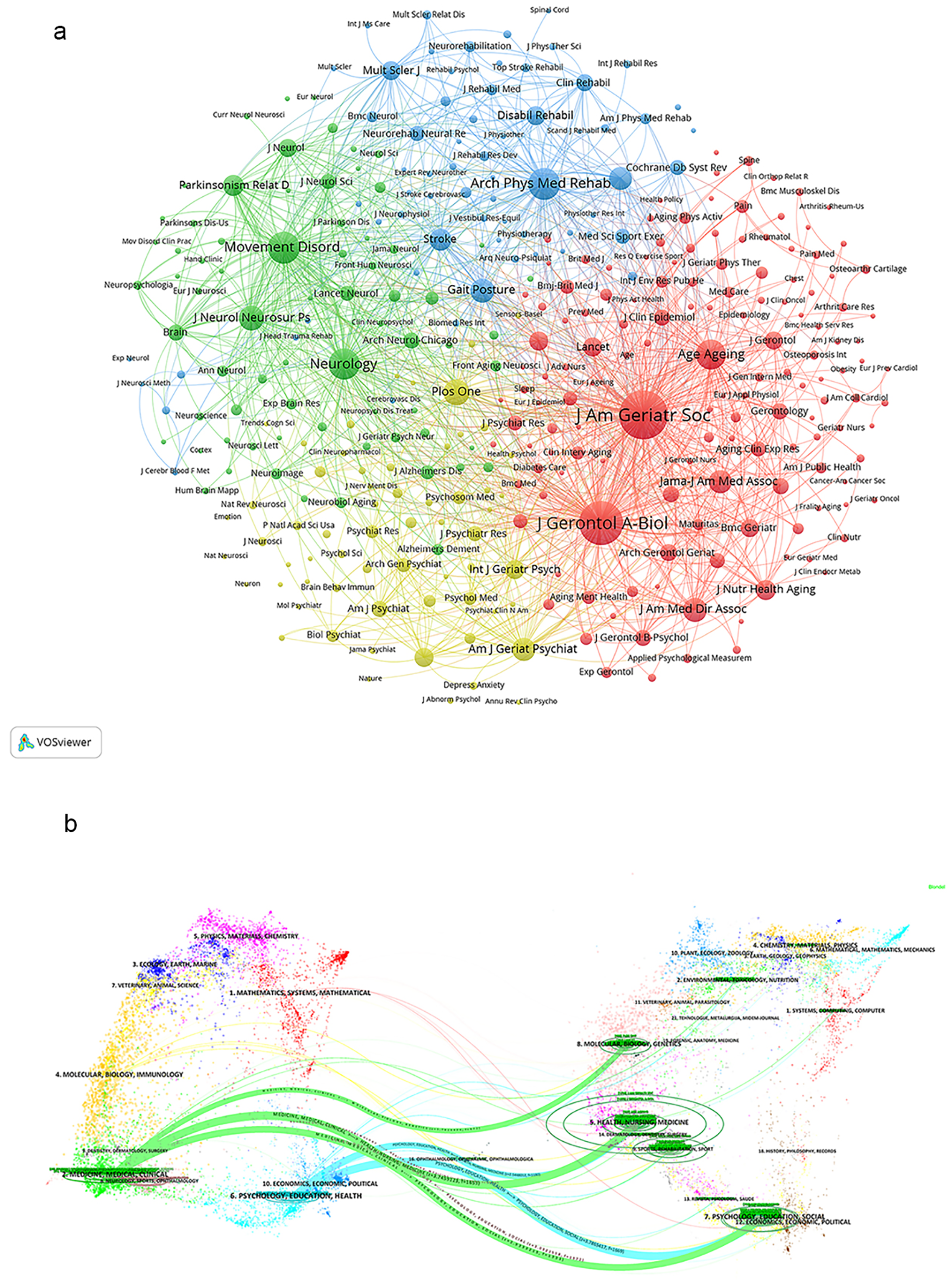
(A) Journal citation network. (B) Dual -map overlay of journals.
We utilized knowledge flow analysis to examine the progression of citation and co-citation patterns between citing journals and cited journals (24). The dual-map overlay of journals illustrates the spread of topics, the paths of citations, and the shifts in research hubs among academic journals (24, 25). On the left side of the Dual-map are labels representing citing journals, while on the right side are labels representing cited journals. The colored curves connecting from the citing map to the cited map depict the comprehensive context of each citation. In the citing map, the vertical axis of the ellipse lengthens with an increase in the number of papers published by a journal, while the horizontal axis lengthens with a larger number of authors. The topics covered by Citing Journals predominantly include fields such as MEDICINE, MEDICAL, CLINICAL, MOLECULAR, BIOLOGY, IMMUNOLOGY, NEUROLOGY, SPORTS, and OPHTHALMOLOGY, representing the forefront of research. The topics addressed by Cited Journals mainly encompass areas like MOLECULAR, BIOLOGY, GENETICS, HEALTH, NURSING, MEDICINE, SPORTS, REHABILITATION, PSYCHOLOGY, EDUCATION, SOCIAL, ECONOMICS, POLITICAL, forming the foundational knowledge base Figure 6b.
3.6 Analysis of keywords
Keywords serve as a fundamental tool to explore the cutting-edge of research on gait-related depression. Figure 7a presents the 20 most frequently occurring keywords. The highest frequency is observed with “depression,” followed by “gait,” “people,” “gait speed,” “older adults,” “quality of life,” “disability,” “health,” “dementia,” “balance,” and “exercise.” All other keywords appear fewer than 100 times. Figure 7b depicts a keyword co-occurrence network where closely associated keywords are grouped into clusters. These clusters are categorized by different colors. The red clusters, encompassing terms like gait speed, older adults, and disability, primarily pertain to elderly populations and their declining physical capabilities. In contrast, the green clusters, featuring terms such as quality of life, balance, and people, are focused on aspects related to balance and overall quality of life. The blue clusters, including keywords like depression, gait, dementia, and cognition, predominantly relate to cognitive functions. Figure 7c illustrates the chronological emergence of these keywords. The size of each square corresponds to the frequency of subsequent occurrences. Keywords listed in the right column represent the thematic clustering observed on the left, predominantly concerning elderly individuals and cognitive decline.
Figure 7
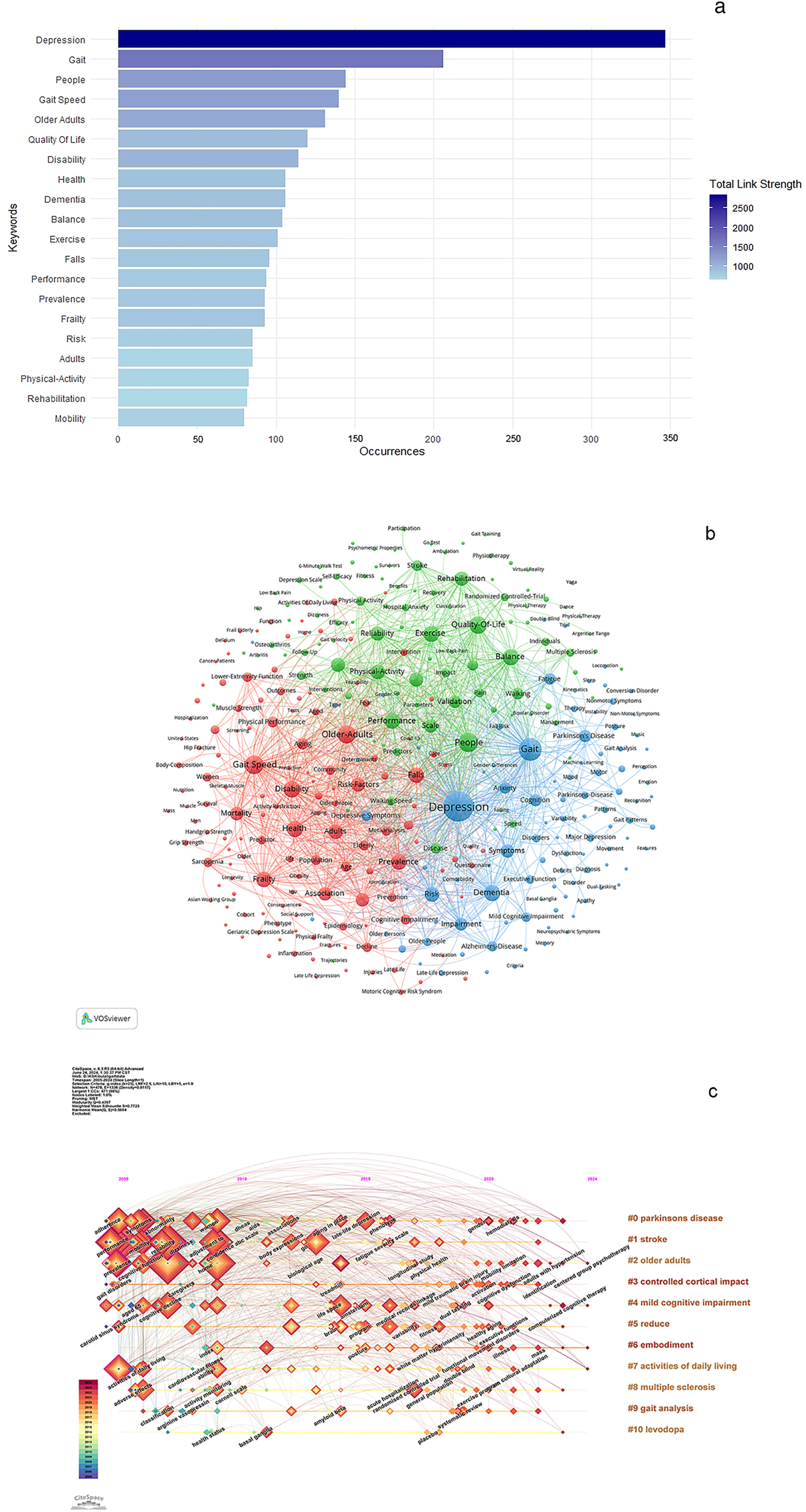
(A) Top 20 Keywords. (B) Keyword co-occurrence network related to gait in depression. (C) Temporal visualization related to gait in depression.
3.7 Analysis of reference
Table 5 presents the top 15 articles ranked by citation frequency, with the most cited being “Executive dysfunction in Parkinson’s disease: A comprehensive review (26),” cited 352 times. This review (26) highlights that executive dysfunction manifests early in Parkinson’s disease (PD), affecting attentional control, planning, and decision-making. Dopaminergic treatment’s impact on executive deficits varies, with implications for motor symptoms like postural instability and gait freezing, alongside psychiatric issues such as depression and apathy, significantly impacting patients’ daily lives. The second most cited article, with 349 citations, is titled “Exercise and Mental Health: Many Reasons to Move (27).” This review (27) scrutinizes the potential of physical exercise as an adjunctive therapy for neuropsychiatric disorders and cognitive decline in aging, emphasizing its capacity to alleviate stress effects and enhance neurotrophic factors, neurotransmitter release, neurogenesis, and cerebral blood flow modulation. Recent studies underscore the substantial influence of exercise on brain health and successful cognitive aging. The article “Cognition, Emotion, and Social Networking in the Community-Dwelling Frail Elderly: A Randomized Clinical Trial” authored by Santabalbina et al. (28), ranks third in citations with 319 mentions. It details a single-blind, interventional, controlled, simple randomized study that examined the impact of a supervised multicomponent exercise program (MEP) on frail older adults. Cognitive assessments, emotional evaluations, and measures of social support demonstrated significant enhancements in the MEP group compared to controls. These results underscore the potential efficacy of structured multicomponent exercise programs in mitigating frailty and improving diverse aspects of health among frail older adults residing in communities. All other articles in the dataset have garnered citations numbering less than 300 each.
Table 5
| Rank | Article title | Authors | Source title | Year | Citations | DOI | Document Type |
|---|---|---|---|---|---|---|---|
| 1 | Executive dysfunction in Parkinson’s disease: A review | Dirnberger, G, et al. (26) | Journal of Neuropsychology | 2013 | 352 | 10.1111/jnp.12028 | Review |
| 2 | Exercise and Mental Health: Many Reasons to Move | Deslandes, A, et al. (27) | Neuropsychobiology | 2009 | 349 | 10.1159/000223730 | Review |
| 3 | A Multicomponent Exercise Intervention that Reverses Frailty and Improves Cognition, Emotion, and Social Networking in the Community-Dwelling Frail Elderly: A Randomized Clinical Trial | Tarazona-Santabalbina, et al. (28) | Journal of the American Medical Directors Association | 2016 | 319 | 10.1016/j.jamda.2016.01.019 | Article |
| 4 | Dual-Task Decrements in Gait: Contributing Factors Among Healthy Older Adults | Hausdorff, JM; Schweiger, A, et al. (29) | Journals of Gerontology Series A-Biological Sciences and Medical Sciences | 2008 | 299 | 10.1093/gerona/63.12.1335 | Article |
| 5 | Cerebral small vessel disease: from a focal to a global perspective | ter Telgte, A, et al. (30) | Nature Reviews Neurology | 2018 | 292 | 10.1038/s41582-018-0014-y | Review |
| 6 | The benefits of exercise training in multiple sclerosis | Motl, RW, et al. (31) | Nature Reviews Neurology | 2012 | 274 | 10.1038/nrneurol.2012.136 | Review |
| 7 | Embodiment of Sadness and Depression-Gait Patterns Associated with Dysphoric Mood | Michalak, J, et al. (32) | Psychosomatic Medicine | 2009 | 272 | 10.1097/PSY.0b013e3181a2515c | Article |
| 8 | Health-related quality of life in early Parkinson’s disease: The impact of nonmotor symptoms | Duncan, GW, et al. (33) | Movement Disorders | 2014 | 254 | 10.1002/mds.25664 | Article |
| 9 | Anxiety Disorders in Parkinson’s Disease: Prevalence and Risk Factors | Dissanayaka, NNW, et al. (34) | Movement Disorders | 2010 | 244 | 10.1002/mds.22833 | Article |
| 10 | Long-term morbidities following self-reported mild traumatic brain injury | Vanderploeg, RD, et al. (35) | Journal of Clinical and Experimental Neuropsychology | 2007 | 238 | 10.1080/13803390600826587 | Article |
| 11 | The relationship between pain, neuropsychological performance, and physical function in community-dwelling older adults with chronic low back pain | Weiner, DK; Rudy, TE, et al. (36) | Pain Medicine | 2006 | 224 | 10.1111/j.1526-4637.2006.00091.x | Article |
| 12 | Performance-based physical function and future dementia in older people | Wang, L; Larson, EB, et al. (37) | Archives of Internal Medicine | 2006 | 220 | 10.1001/archinte.166.10.1115 | Article |
| 13 | Impact of physical frailty on disability in community-dwelling older adults: a prospective cohort study | Makizako, H; Shimada, H, et al. (38) | BMJ Open | 2015 | 184 | 10.1136/bmjopen-2015-008462 | Article |
| 14 | Depression and frailty in later life: a synthetic review | Mezuk, B, et al. (39) | International Journal of Geriatric Psychiatry | 2012 | 183 | 10.1002/gps.2807 | Review |
| 15 | Balance score and a history of falls in hospital predict recurrent falls in the 6 months following stroke rehabilitation | Mackintosh, SF, et al. (40) | Archives of Physical Medicine and Rehabilitation | 2006 | 180 | 10.1016/j.apmr.2006.09.004 | Article |
The top 15 articles by citation frequency.
Reference co-citation analysis, which examines relationships among references based on their shared citation frequency, was employed to analyze reference citation patterns. Figure 8a presents a relational diagram depicting these associations among studies, categorized into five main clusters represented by distinct colors. The red cluster includes seminal references such as Fried LP, 2001 (41); Studenski S, 2011 (42); and Guralnik JM, 1994 (43). The green cluster comprises references such as Folstein MF, 1975 (44); Podsiadlo D, 1991 (45); and Yesavage JA, 1983 (46). References in the blue cluster include Tinetti ME, 1990 (47); and Yardley L, 2005 (48); Scheffer Ac, 2008 (49). The yellow cluster encompasses Lemke MR, 2000 (50); Michalak J, 2009 (32); and Hausdorff JM, 2004 (51). Lastly, the purple cluster includes references such as Yogev-Seligmann G, 2008 (52); Montero-Odasso M, 2012 (53); and Verghese J, 2007 (54). In the figure, the size of each circle correlates with its co-citation weight, indicating the prominence of these references within their respective color-coded clusters.
Figure 8
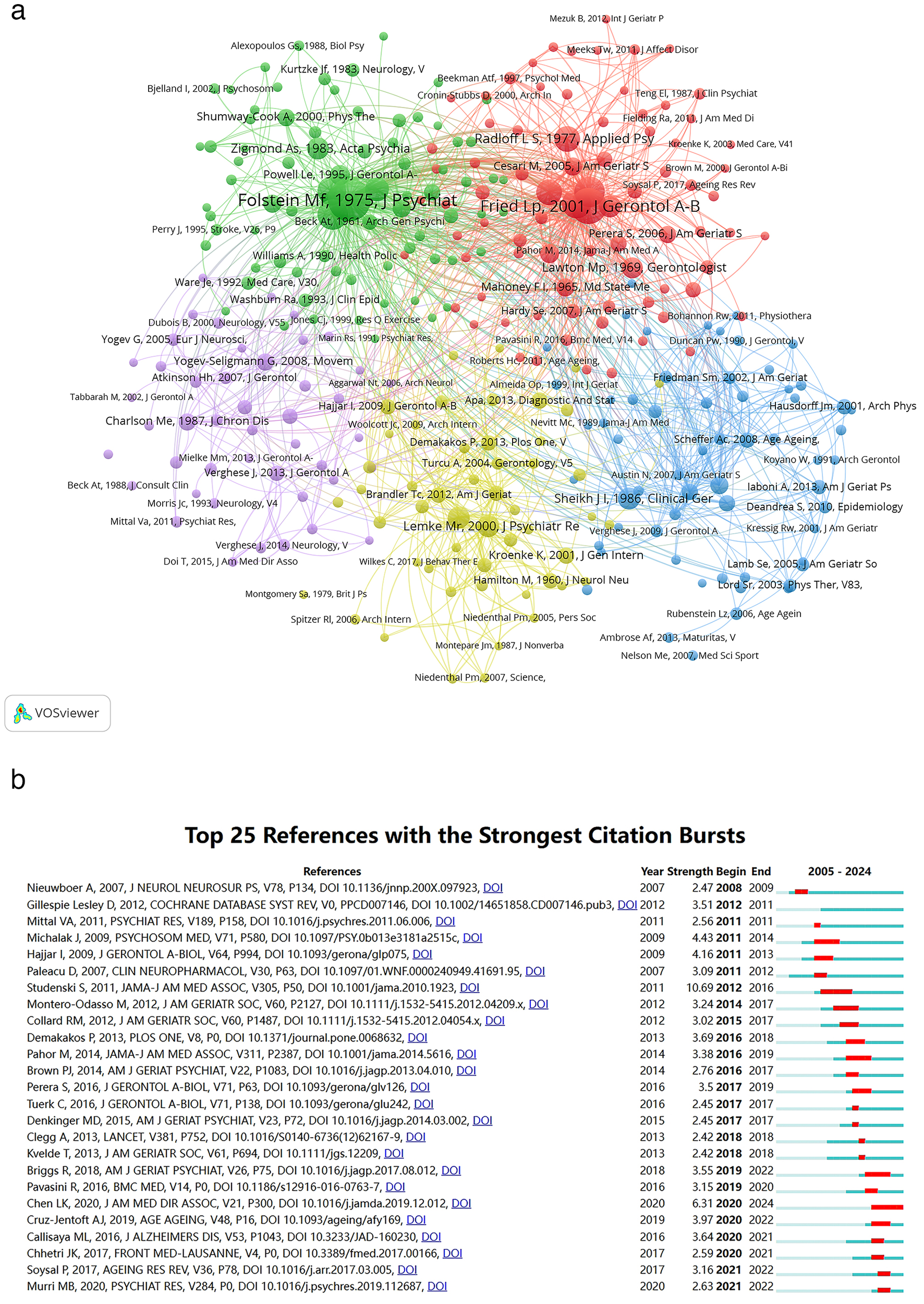
(A) Co-citation networks among references; node area is scaled to the frequency of occurrence. (B) The 25 references with the highest citation burst strengths are presented.
Figure 8b illustrates the top 25 references exhibiting the most pronounced citation bursts. The earliest burst was observed in 2008. Titled “Cueing training in the home improves gait-related mobility in Parkinson’s disease: the RESCUE trial” authored by Nieuwboer A et al. (55), this study was published in 2007 in the J NEUROL NEUROSUR PS journal. Studenski S et al.’s paper (42) “Gait speed and survival in older adults” featured in JAMA in 2011, achieved the highest citation burst intensity of 10.69. Notably, 2011 and 2020 emerged as pivotal years with four citation bursts each.
4 Discussion
Our bibliometric analysis on gait in depression is executed through the utilization of VOSviewer and CiteSpace. This study spans publications from January 1, 2005, to June 21, 2024, encompassing contributions from 59 countries or regions, 1516 institutions, and 4781 authors. Our analysis revealed that the publication output reached its zenith with 102 papers in 2020, while citation frequency attained its pinnacle at 3920 citations in 2022 (Figure 2). In the ensuing years, both publication volume and citation frequency experienced varying degrees of decline.
The analysis of countries or regions reveals that in the field of gait in depression, the USA significantly outpaces other nations in both publication volume and citation frequency, establishing itself as the most influential country in this domain (Table 1). Additionally, among the top 10 institutions by publication volume, eight are based in the USA, and among the top 10 institutions by citation frequency, six are also from the USA (Table 2). The University of Pittsburgh ranks first in both publication volume with 29 papers and citation frequency with 1204 citations, highlighting its predominant impact in the field of gait in depression. In terms of collaboration, the USA occupies a central position with the highest and strongest connections. Furthermore, countries with higher publication volumes such as Canada, the United Kingdom, and China also maintain close exchanges and collaborations with other nations and regions (Figure 3).
Shimada, Hiroyuki holds a prominent position in the field of gait and depression, ranking first in citation frequency and second in publication volume (Table 3). Hausdorff, JM et al. (29) published a study in 2008 titled “Dual-Task Decrements in Gait: Contributing Factors Among Healthy Older Adults,” which ranks fourth in citation frequency. Similarly, Makizako, H et al. (38) conducted a prospective cohort study in 2015 titled “Impact of physical frailty on disability in community-dwelling older adults,” which ranks 13th in citation frequency. Both Hausdorff, JM and Makizako, H is notable for their high citation frequencies. Verghese, Joe and Rochester, Lynn, also influential in this field, rank among the top three authors by publication volume alongside Shimada, Hiroyuki, with their citation frequencies also placing in the top ten. This underscores their significant influence and expertise in the field.
We analyzed journals and found that the following 8 journals are not only ranked in the top ten by publication volume but also in citation frequency (Table 4): Journals of Gerontology Series A-Biological Sciences And Medical, Journal of The American Geriatrics Society, Archives of Physical Medicine And Rehabilitation, American Journal of Geriatric Psychiatry, Geriatrics & Gerontology International, BMC Geriatrics, Journal of The American Medical Directors Association, and PLOS One. The journals largely focus on topics related to elderly individuals, spanning disciplines such as medicine, biological sciences, geriatric health, rehabilitation, mental health, and neuroscience. This thematic focus corresponds with the conclusions drawn from the dual-map analysis depicted in Figure 6b.
Keywords analysis is a critical method in studying depression and gait, offering insights into current research trends and focal points. By examining frequently occurring keywords, researchers can identify core themes and major issues of interest. The keywords in this study—depression, gait, people, gait speed, older adults, quality of life, disability, health, dementia, balance, exercise, falls, performance, prevalence, frailty, risk, adults, physical activity, rehabilitation, mobility—encompass aspects such as depression, aging, cognitive function, and interventions (Figure 7a). These keywords reflect the multidimensional and extensive nature of research on depression and gait.
The frequent occurrence of keywords such as ‘depression,’ ‘gait,’ and ‘gait speed’ reflects growing academic interest in the potential associations and clinical implications of gait-related characteristics in the context of depression. Karl E. Friedl et al. (56) propose that mood states are discernible through specific types of human movement, such as slumped posture and shuffling gait, which serve as indicators of depression. Their study found that individuals with major depression showed decreased gait velocity, reduced arm swing, limited vertical head movements, increased lateral swaying of the upper body, and shorter stride length with decreased double limb support compared to individuals who had never experienced depression. In exploratory experiments, Yameng Wang et al. (16) also noted comparable findings. Moreover, college students experiencing sad or happy moods induced by music displayed similar gait characteristics when in a state of sadness (32). Emma Elkjær et al. recently conducted a meta-analysis (57) revealing that individuals with depression exhibit reduced gait speed, step length, stride length, step width, steps taken to turn, and stepping reaction time, alongside increased overall abnormal movement. Additionally, they demonstrate greater instability and a larger center-of-pressure, as well as increased head flexion and reduced joint range of motion in the knees, hips, wrists, shoulders, and elbows. These findings likely strengthen the argument for a distinct gait pattern associated with depression. However, present findings do not definitively substantiate that gait patterns are exclusive symptoms of depression (56). Current studies typically investigate depression as a homogeneous entity. Patients with depression may manifest either psychomotor retardation or psychomotor agitation, introducing potential inconsistencies in results. Future research should emphasize investigating the temporal and spatial relationships between these unique gait patterns and the disorder, as well as establishing criteria for defining these patterns as distinctly associated with the disorder.
Gait characteristics associated with depression may vary by age, gender, and occupation. Recent studies have indicated that adult patients with depression often exhibit significant impairments in posture, balance, and gait functions, while gait abnormalities in older adults with depression may result from the interplay of physical illness, cognitive impairment, and emotional disturbances (58). Other research has demonstrated that daily gait patterns can provide additional information for predicting the severity of depressive symptoms (59). Age is a key moderator of depression-related gait features. Studies have shown that gait abnormalities are more pronounced in older patients with depression, particularly characterized by slower gait speed and increased gait variability. These changes may be closely related to age-associated neurodegenerative processes and cognitive decline (58). Gender differences also warrant attention. Evidence suggests that in healthy populations, males and females exhibit distinct gait parameters—males generally present with longer stride length and faster gait speed, while females tend to show higher step frequency and different patterns of gait symmetry. However, there is currently a lack of systematic research on gender-related gait differences among patients with depression, highlighting the need for further investigation. Occupational factors may also influence gait performance in individuals with depression through psychosocial stress mechanisms. A systematic review (60) has reported that adverse occupational psychosocial stress is significantly associated with impaired autonomic nervous system function, as indicated by reduced heart rate variability, suggesting that prolonged stress may disrupt parasympathetic activity and autonomic balance. Additionally, another study (61) found that occupational role stress—such as role conflict and ambiguity—elicited stronger acute cortisol responses (p = 0.016), indicating that high-stress work may activate the hypothalamic-pituitary-adrenal (HPA) axis, potentially impairing gait stability and motor control.
Despite the common assumption that motor disturbances are more pronounced in older individuals (62), the moderation analysis indicated no significant moderating effects of age (57). Across various age groups, individuals face challenges such as reduced gait speed, step length, stride length, and step width, as well as increased overall abnormal movement. These issues not only restrict their daily activities but also increase the risks of falls and injuries, impacting their health and quality of life. Such challenges may contribute to conditions of frailty and disability, further limiting their daily activities and social participation.
In depression, concurrent with cognitive decline including reductions in attention and memory is evident. Additionally, depressive symptoms represent a risk factor for mild cognitive impairment in older adults (63). Major depression correlates with increased variability in stride time, stride velocity, and swing time during dual-task activities, indicating compromised executive function and visual memory (64). Depressed elderly patients exhibit slower walking speed, shorter strides, reduced minimum toe clearance, and greater variability in stride length compared to healthy controls (65). Additionally, dual-task conditions exacerbate these impairments, resulting in further reductions in gait speed, stride length, and prolonged swing time relative to single-task conditions (65). In 2021, Mehmet Ilkin Naharci et al. (66) found that slower gait speed is independently associated with depressive symptoms in older adults with mild cognitive impairment. Depression and cognitive impairment may present with distinct gait characteristics, both of which affect stability and balance, thereby increasing the risk of falls. Future research needs to further explore whether depression and cognitive impairment exhibit distinct gait features and elucidate the differences between them.
The high fall rates in depression may be explained by abnormal posture. Gait abnormalities increase the risk of falls, severely affecting patients’ quality of life and mobility. Proactive intervention targeting abnormal gait is crucial for reducing fall risk and enhancing quality of life in individuals with depression. For these patients, altering emotional states through short bodily manipulations has been found to be effective (57), consistent with recent studies in healthy populations (67–69). The major motor system may be a direct target for interventions in depression (57). The number of studies related to physical inactivity has increased significantly (18). Reduced physical activity due to depression can be mitigated through exercise, which is effective in reducing depressive symptoms with just moderate to vigorous physical activity replacing 60 minutes of sedentary time (70–72). Additionally, there is evidence suggesting that (32, 73) certain therapeutic approaches, including mindfulness, can influence the motor system.
With the continuous advancement of technology, artificial intelligence (AI) and wearable devices have gradually become essential tools in gait research related to depression. Bibliometric analysis reveals a sustained growth trend over the past two decades in studies involving wearable health sensors, with an average annual growth rate of approximately 20.7%, providing more ecologically valid and scalable methods for long-term dynamic gait monitoring in depression (74). Additionally, Azliyana Azizan et al. (75) conducted a bibliometric review of sensor-based fall prevention research in the elderly, identifying key research hotspots and future opportunities, which reflects the broad potential of sensor technologies in health monitoring applications.
From the perspective of algorithm development, the introduction of AI models has significantly advanced the intelligence of gait recognition. Nan Zhao et al. (76) utilized Kinect to capture gait images combined with machine learning approaches to accurately predict depression levels, demonstrating the feasibility of integrating visual perception and machine learning. Haifeng Lu et al. (77) proposed an integrated evaluation framework based on multimedia gait data by applying frequency domain analysis of kinetic and potential energy, markedly improving the objectivity and practicality of depression risk detection among graduate students. Tao Wang et al. (78) developed a gait assessment framework that fuses temporal, frequency, and spatial geometric features, achieving efficient, non-contact depression detection with a classification accuracy of 93.75%, indicating strong effectiveness and robustness. Furthermore, Jingjing Yang et al. (79) enhanced depression gait detection models by applying skeletal data augmentation techniques that preserve key skeletal attributes, resulting in accuracy improvements up to 92.15%.
Overall, current bibliometric trends indicate that the integration of AI and wearable technologies is driving depression gait research from simple feature identification toward more precise risk prediction. This evolving direction is expected to facilitate high-throughput, high-accuracy, and highly adaptable clinical applications, representing a major research focus and future trend in the field.
This study has several considerations to note. First, the decline in publications after 2020 may be related to incomplete indexing of recent literature, which could affect the completeness of the dataset. Second, data were obtained solely from the Web of Science Core Collection; incorporating additional databases such as Scopus and PubMed could provide a broader scope of relevant literature and enrich data diversity. Furthermore, bibliometric analysis primarily offers a macroscopic view of research trends and structures and does not directly assess clinical efficacy or causality. Therefore, the findings should be viewed as hypothesis-generating and warrant further validation through clinical studies. Additionally, characteristics inherent to citation practices, variability in keyword definitions, and the absence of individual-level data are factors to consider when interpreting the results.
Future research may benefit from integrating bibliometric methods with qualitative content analysis or systematic clinical reviews to deepen the understanding of gait alterations in depression. The application of machine learning–enhanced text mining, full-text semantic analysis, and multi-database triangulation can further improve the comprehensiveness and granularity of future studies. Natural language processing (NLP) shows promising potential in identifying emerging psychosomatic gait phenotypes across interdisciplinary medical and psychiatric databases. Moreover, fostering interdisciplinary collaboration among psychiatry, biomechanics, computer science, and geriatrics is crucial to translating bibliometric insights into clinical practice, particularly in areas such as digital gait assessment and AI-assisted mental health screening.
5 Conclusions
In our study, we employed bibliometric analysis to examine the research progress and future trends of gait in depression over the past 20 years. The number of publications and citations related to gait in depression has been increasing annually, with a slight decline observed in recent years. The USA holds a central position in this field. The University of Pittsburgh, the University of California, San Francisco, and Harvard Medical School are prominent institutions within this domain. Influential authors include Joe Verghese, Hiroyuki Shimada, and Lynn Rochester. Current research frontiers encompass the identification of distinctive gait patterns in depression, gait characteristics in the elderly, and the association between gait and cognitive decline. Additionally, there are exploratory studies investigating potential interventions for abnormal gait in depressive populations. This bibliometric analysis highlights these research trends and frontiers, providing valuable references for scholars interested in significant topics and potential collaborations. It is important to emphasize that most existing studies are observational and exploratory in nature, lacking systematic clinical validation. Therefore, the findings of this study should be considered hypothesis-generating rather than confirmatory. Future research is needed to further elucidate the mechanisms underlying gait changes in depression and to evaluate the potential clinical utility of related interventions.
Statements
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author contributions
SK: Conceptualization, Data curation, Investigation, Methodology, Software, Validation, Visualization, Writing – original draft. N-NC: Conceptualization, Data curation, Investigation, Methodology, Writing – original draft. BP: Formal Analysis, Funding acquisition, Project administration, Resources, Supervision, Writing – review & editing. YZ: Formal Analysis, Funding acquisition, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. The study was supported by the Fund of the Science and Technology Planning Project of Shenzhen Municipality (20210617155253001) and National Key R&D Program of the Ministry of Science and Technology of the People’s Republic of China (No. 2023YFC3603204).
Acknowledgments
All authors express their profound appreciation to those instrumental in the meticulous curation and analysis of data. Additionally, heartfelt gratitude is extended to the erudite reviewers and esteemed editorial board of frontiers in psychiatry for their discerning insights and invaluable contributions.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1
Global Health Data Exchange (GHDx) . Institute of health metrics and evaluation(2023). Available online at: https://vizhub.healthdata.org/gbd-results/ (Accessed June 10, 2024).
2
Ferrari AJ Woody CA Siskind DJ Whiteford HA Harris MG . A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J Affect Disord. (2017) 219:86–92. doi: 10.1016/j.jad.2017.05.003
3
Evans-Lacko S Aguilar-Gaxiola S Al-Hamzawi A Alonso J Benjet C Bruffaerts R et al . Socio-economic variations in the mental health treatment gap for people with anxiety, mood, and substance use disorders: results from the WHO World Mental Health (WMH) surveys. Psychol Med. (2018) 48:1560–71. doi: 10.1017/S0033291717003336
4
Harman JS Edlund MJ Fortney JC . Disparities in the adequacy of depression treatment in the United States. Psychiatr Serv. (2004) pp:1379–85. doi: 10.1176/appi.ps.55.12.1379
5
Young AS Klap R Sherbourne CD Wells KB . The quality of care for depressive and anxiety disorders in the United States. Arch Gen Psychiatry. (2001) 58(1):55–61. doi: 10.1001/archpsyc.58.1.55
6
Ramin M Mark O . Proportion of antidepressants prescribed without a psychiatric diagnosis is growing. J Health Aff (Millwood). (2011) 30:1434–42. doi: 10.1377/hlthaff.2010.1024
7
Mojtabai R . Clinician-identified depression in community settings: concordance with structured-interview diagnoses. Psychother Psychosom. (2013) 82:161–9. doi: 10.1159/000345968
8
Dowrick C Frances A . Medicalising unhappiness: new classification of depression risks more patients being put on drug treatment from which they will not benefit. BMJ (Clinical Res ed). (2013) 9:f7140. doi: 10.1136/bmj.f7140
9
James MA Anne CK Bryan PM Zhongxue C Andrea KC . The association of depression stigma with barriers to seeking mental health care: a cross-sectional analysis. J Ment Health. (2020) 29:182–90. doi: 10.1080/09638237.2019.1644494
10
Interian A Ang A Gara MA Rodriguez MA Vega WA . The long-term trajectory of depression among Latinos in primary care and its relationship to depression care disparities. Gen Hosp Psychiatry. (2011) 33:94–101. doi: 10.1016/j.genhosppsych.2010.12.001
11
Didier S Wouter H Bernard GCS . Psychomotor symptoms in depression: a diagnostic, pathophysiological and therapeutic tool. J Affect Disord. (2008) 109:1–20. doi: 10.1016/j.jad.2007.10.019
12
Fried EI Nesse RM . The impact of individual depressive symptoms on impairment of psychosocial functioning. PloS One. (2014) 9:e90311. doi: 10.1371/journal.pone.0090311
13
Walther S Bernard JA Mittal VA Shankman SA . The utility of an RDoC motor domain to understand psychomotor symptoms in depression. Psychol Med. (2019) 49:212–6. doi: 10.1017/S0033291718003033
14
Sanders JB Bremmer MA Deeg DJ Beekman AT . Do depressive symptoms and gait speed impairment predict each other’s incidence? A 16-year prospective study in the community. J Am Geriatr Soc. (2012) 60:1673–80. doi: 10.1111/j.1532-5415.2012.04114.x
15
Boolani A Gruber AH Torad AA Stamatis A . Identifying current feelings of mild and moderate to high depression in young, healthy individuals using gait and balance: an exploratory study. Sens (Basel). (2023) 23(14):6624. doi: 10.3390/s23146624
16
Wang Y Wang J Liu X Zhu T . Detecting depression through gait data: examining the contribution of gait features in recognizing depression. Front Psychiatry. (2021) 12:661213. doi: 10.3389/fpsyt.2021.661213
17
Hicks D Wouters P Waltman L de Rijcke S Rafols I . Bibliometrics: The Leiden Manifesto for research metrics. Nature. (2015) 520:429–31. doi: 10.1038/520429a
18
Azizan A Md Fadzil NH . What stops us and what motivates us? A scoping review and bibliometric analysis of barriers and facilitators to physical activity. Ageing Res Rev. (2024) 99:102384. doi: 10.1016/j.arr.2024.102384
19
Azizan A . Mapping the muscle mass: A birds-eye view of sarcopenia research through bibliometric network analysis. Int J Disabil Sports Health Sci. (2023) 134–43. doi: 10.33438/ijdshs.1362539
20
Wan Y Shen J Hong Y Liu J Shi T Cai J . Mapping knowledge landscapes and emerging trends of the biomarkers in melanoma: a bibliometric analysis from 2004 to 2022. Front Oncol. (2023) 13:1181164. doi: 10.3389/fonc.2023.1181164
21
Qiang Z Jin P Josiah P Alexander YL Li Z Yuhua W et al . Worldwide research trends on aristolochic acids (1957-2017): Suggestions for researchers. PloS One. (2019) 14:e0216135. doi: 10.1371/journal.pone.0216135
22
Chen CM . CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol. (2006) 57:359–77. doi: 10.1002/asi.20317
23
van Eck NJ Waltman L . Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. (2010) 84:523–38. doi: 10.1007/s11192-009-0146-3
24
Chen C Leydesdorff L . Patterns of connections and movements in dual-map overlays: a new method of publication portfolio analysis. J Assoc Inf Sci Technol. (2014) 65:334–51. doi: 10.1002/asi.22968
25
Zhang J Song L Xu L Fan Y Wang T Tian W et al . Knowledge domain and emerging trends in ferroptosis research: a bibliometric and knowledge-map analysis. Front Oncol. (2021) 11:686726. doi: 10.3389/fonc.2021.686726
26
Georg D Marjan J . Executive dysfunction in Parkinson’s disease: a review. J Neuropsychol. (2013) 7:193–224. doi: 10.1111/jnp.12028
27
Deslandes A Moraes H Ferreira C Veiga H Silveira H Mouta R et al . Exercise and mental health: many reasons to move. Neuropsychobiology. (2009) 59:191–8. doi: 10.1159/000223730
28
Tarazona-Santabalbina FJ Gomez-Cabrera MC Perez-Ros P Martinez-Arnau FM Cabo H Tsaparas K et al . A multicomponent exercise intervention that reverses frailty and improves cognition, emotion, and social networking in the community-dwelling frail elderly: A randomized clinical trial. J Am Med Dir Assoc. (2016) 17:426–33. doi: 10.1016/j.jamda.2016.01.019
29
Schweiger A Hausdorff JM Herman T Yogev-Seligmann G Giladi N . Dual-task decrements in gait: contributing factors among healthy older adults. J Gerontol A Biol Sci Med Sci. (2008) 63:1335–43. doi: 10.1093/gerona/63.12.1335
30
van Leijsen EMC Ter Telgte A Wiegertjes K Klijn CJM Tuladhar AM de Leeuw FE . Cerebral small vessel disease: from a focal to a global perspective. Nat Rev Neurol. (2018) 14:387–98. doi: 10.1038/s41582-018-0014-y
31
Pilutti LA Motl RW . The benefits of exercise training in multiple sclerosis. Nat Rev Neurol. (2012) 8:487–97. doi: 10.1038/nrneurol.2012.136
32
Troje NF Michalak J Fischer J Vollmar P Heidenreich T Schulte D . Embodiment of sadness and depression–gait patterns associated with dysphoric mood. Psychosom Med. (2009) 71:580–7. doi: 10.1097/PSY.0b013e3181a2515c
33
Khoo TK Duncan GW Yarnall AJ O’Brien JT Coleman SY Brooks DJ et al . Health-related quality of life in early Parkinson’s disease: the impact of nonmotor symptoms. Mov Disord. (2014) 29:195–202. doi: 10.1002/mds.25664
34
Sellbach A Dissanayaka NN Matheson S O’Sullivan JD Silburn PA Byrne GJ et al . Anxiety disorders in Parkinson’s disease: prevalence and risk factors. Mov Disord. (2010) 25:838–45. doi: 10.1002/mds.22833
35
Curtiss G Vanderploeg RD Luis CA Salazar AM . Long-term morbidities following self-reported mild traumatic brain injury. J Clin Exp Neuropsychol. (2007) 29:585–98. doi: 10.1080/13803390600826587
36
Rudy TE Weiner DK Morrow L Slaboda J Lieber S . The relationship between pain, neuropsychological performance, and physical function in community-dwelling older adults with chronic low back pain. Pain Med. (2006) 7:60–70. doi: 10.1111/j.1526-4637.2006.00091.x
37
Larson EB Wang L Bowen JD van Belle G . Performance-based physical function and future dementia in older people. Arch Intern Med. (2006) 166:1115–20. doi: 10.1001/archinte.166.10.1115
38
Makizako H Shimada H Doi T Tsutsumimoto K Suzuki T . Impact of physical frailty on disability in community-dwelling older adults: a prospective cohort study. BMJ Open. (2015) 5:e008462. doi: 10.1136/bmjopen-2015-008462
39
Mezuk B Edwards L Lohman M Choi M Lapane K . Depression and frailty in later life: a synthetic review. Int J Geriatr Psychiatry. (2012) 27:879–92. doi: 10.1002/gps.2807
40
Hill KD Mackintosh SF Dodd KJ Goldie PA Culham EG . Balance score and a history of falls in hospital predict recurrent falls in the 6 months following stroke rehabilitation. Arch Phys Med Rehabil. (2006) 87:1583–9. doi: 10.1016/j.apmr.2006.09.004
41
Linda PF Catherine MT Jeremy W Anne BN Calvin H John G et al . Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. (2001) 56:M146–56. doi: 10.1093/gerona/56.3.m146
42
Studenski S Perera S Patel K Rosano C Faulkner K Inzitari M et al . Gait speed and survival in older adults. JAMA. (2011) 305:50–8. doi: 10.1001/jama.2010.1923
43
Simonsick EM Guralnik JM Ferrucci L Glynn RJ Berkman LF Blazer DG et al . A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. (1994) 49:M85–94. doi: 10.1093/geronj/49.2.m85
44
Folstein SE Folstein MF McHugh PR . Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. (1975) 12:189–98. doi: 10.1016/0022-3956(75)90026-6
45
Richardson S Podsiadlo D . The timed “Up & Go”: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc. (1991) 39:142–8. doi: 10.1111/j.1532-5415.1991.tb01616.x
46
Brink TL Yesavage JA Rose TL Lum O Huang V Adey M et al . Development and validation of a geriatric depression screening scale: a preliminary report. J Psychiatr Res. (1983) 17:37–49. doi: 10.1016/0022-3956(82)90033-4
47
Richman D Tinetti ME Powell L . Falls efficacy as a measure of fear of falling. J Gerontol. (1990) 45:239–43. doi: 10.1093/geronj/45.6.p239
48
Yardley L Beyer N Hauer K Kempen G Piot-Ziegler C Todd C . Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing. (2005) 34:614–9. doi: 10.1093/ageing/afi196
49
Scheffer AC Schuurmans MJ van Dijk N van der Hooft T de Rooij SE . Fear of falling: measurement strategy, prevalence, risk factors and consequences among older persons. Age Ageing. (2008) 37:19–24. doi: 10.1093/ageing/afm169
50
Wendorff T Lemke MR Mieth B Buhl K Linnemann M . Spatiotemporal gait patterns during over ground locomotion in major depression compared with healthy controls. J Psychiatr Res. (2000) 34:277–83. doi: 10.1016/s0022-3956(00)00017-0
51
Hausdorff JM Peng CK Goldberger AL Stoll AL . Gait unsteadiness and fall risk in two affective disorders: a preliminary study. BMC Psychiatry. (2004) 4:39. doi: 10.1186/1471-244X-4-39
52
Yogev-Seligmann G Hausdorff JM Giladi N . The role of executive function and attention in gait. Mov Disord. (2008) 23:329–42; quiz 472. doi: 10.1002/mds.21720
53
Montero-Odasso M Verghese J Beauchet O Hausdorff JM . Gait and cognition: a complementary approach to understanding brain function and the risk of falling. J Am Geriatr Soc. (2012) 60:2127–36. doi: 10.1111/j.1532-5415.2012.04209.x
54
Verghese J Wang C Lipton RB Holtzer R Xue X . Quantitative gait dysfunction and risk of cognitive decline and dementia. J Neurol Neurosurg Psychiatry. (2007) 78:929–35. doi: 10.1136/jnnp.2006.106914
55
Nieuwboer A Kwakkel G Rochester L Jones D van Wegen E Willems AM et al . Cueing training in the home improves gait-related mobility in Parkinson’s disease: the RESCUE trial. J Neurol Neurosurg Psychiatry. (2007) 78:134–40. doi: 10.1136/jnnp.200X.097923
56
Friedl KE Looney DP . With life there is motion. Activity biomarkers signal important health and performance outcomes. J Sci Med Sport. (2023) 26 Suppl 1:S3–8. doi: 10.1016/j.jsams.2023.01.009
57
Elkjaer E Mikkelsen MB Michalak J Mennin DS O’Toole MS . Motor alterations in depression and anxiety disorders: A systematic review and meta-analysis. J Affect Disord. (2022) 317:373–87. doi: 10.1016/j.jad.2022.08.060
58
Murri MB Triolo F Coni A Tacconi C Nerozzi E Escelsior A et al . Instrumental assessment of balance and gait in depression: A systemati c review. Psychiatry Res. (2020) 284:112687. doi: 10.1016/j.psychres.2019.112687
59
Zhang Y Folarin AA Sun S Cummins N Vairavan S Qian L et al . Associations Between Depression Symptom Severity and Daily-Life Gait C haracteristics Derived From Long-Term Acceleration Signals in Real-Wor ld Settings: Retrospective Analysis. JMIR mHealth uHealth. (2022) 10:e40667. doi: 10.2196/40667
60
Jarczok MN Jarczok M Mauss D Koenig J Li J Herr RM et al . Autonomic nervous system activity and workplace stressors–a systemati c review. Neurosci Biobehav Rev. (2013) 37:1810–23. doi: 10.1016/j.neubiorev.2013.07.004
61
Wirtz PH Ehlert U Kottwitz MU La Marca R Semmer NK . Occupational role stress is associated with higher cortisol reactivity to acute stress. J Occup Health Psychol. (2013) 18:121–31. doi: 10.1037/a0031802
62
Jahn K Zwergal A Schniepp R . Gait disturbances in old age: classification, diagnosis, and treatment from a neurological perspective. Dtsch Arztebl Int. (2010) 107:306–15; quiz 316. doi: 10.3238/arztebl.2010.0306
63
Zhou Z He CYY Kan MMP Chan DHY Wong ACT Mok KHY et al . Modifiable risk factors for mild cognitive impairment among cognitively normal community-dwelling older adults: A systematic review and meta-analysis. Ageing Res Rev. (2024) 26:102350. doi: 10.1016/j.arr.2024.102350
64
Gabel NM Crane NA Avery ET Kay RE Laurent A Giordani B et al . Dual-tasking gait variability and cognition in late-life depression. Int J Geriatr Psychiatry. (2015) 30:1120–8. doi: 10.1002/gps.4340
65
Jungen P Batista JP Kirchner M Habel U Bollheimer LC Huppertz C . Variability and symmetry of gait kinematics under dual-task performance of older patients with depression. Aging Clin Exp Res. (2023) 35:283–91. doi: 10.1007/s40520-022-02295-6
66
Naharci MI Katipoglu B Veizi B Tasci I . Gait Speed is independently associated with Depression Symptoms in Mild Cognitive Impairment. Neuropsychol Dev Cognit B Aging Neuropsychol Cognit. (2022) 29:637–50. doi: 10.1080/13825585.2021.1882932
67
Schultz SJ Cuddy AJC Fosse NE . P-curving a more comprehensive body of research on postural feedback reveals clear evidential value for power-posing effects: reply to Simmons and Simonsohn. Psychol Sci. (2017) 29:656–66. doi: 10.1177/0956797617746749
68
Elkjær E Mikkelsen MB Michalak J Mennin DS O’Toole MS . Expansive and contractive postures and movement: A systematic review and meta-analysis of the effect of motor displays on affective and behavioral responses. Perspect psychol Sci. (2020) 17:276–304. doi: 10.1177/1745691620919358
69
Körner R Schütz A . Dominance or prestige: A review of the effects of power poses and other body postures. Soc Pers Psychol Compass. (2020) 14(8):1–19. doi: 10.1111/spc3.12559
70
Alfonso-Rosa RM Del Pozo Cruz B McGregor D Chastin SF Palarea-Albaladejo J Del Pozo Cruz J . Sedentary behaviour is associated with depression symptoms: Compositional data analysis from a representative sample of 3233 US adults and older adults assessed with accelerometers. J Affect Disord. (2020) 15:59–62. doi: 10.1016/j.jad.2020.01.023
71
Kandola AA Del Pozo Cruz B Osborn DPJ Stubbs B Choi KW Hayes JF . Impact of replacing sedentary behaviour with other movement behaviours on depression and anxiety symptoms: a prospective cohort study in the UK Biobank. BMC Med. (2021) 19:133. doi: 10.1186/s12916-021-02007-3
72
Luteberget LS Spencer M Gilgien M . Validity of the catapult ClearSky T6 local positioning system for team sports specific drills, in indoor conditions. Front Physiol. (2018) 9:115. doi: 10.3389/fphys.2018.00115
73
Michalak J Troje NF Heideneich T . The effects of mindfulness-based cognitive therapy on depressive gait patterns. J Cogn Behav Psychotherapies. (2011) 11:13–27. doi: 10.1024/1016-264X/a000029
74
Azizan A Ahmed W Razak AHA . Sensing health: a bibliometric analysis of wearable sensors in healthcare. Health Technol. (2024) 14:15–34. doi: 10.1007/s12553-023-00801-y
75
Azizan A . Challenges and opportunities in sensor-based fall prevention for older adults: a bibliometric review. J Enabling Technol. (2024) 18:306–18. doi: 10.1108/JET-02-2024-0011
76
Zhao N Zhang Z Wang Y Wang J Li B Zhu T et al . See your mental state from your walk: Recognizing anxiety and depressi on through Kinect-recorded gait data. PloS One. (2019) 14:e0216591. doi: 10.1371/journal.pone.0216591
77
Lu H Xu S Hu X Ngai E Guo Y Wang W et al . Postgraduate student depression assessment by multimedia gait analysis. IEEE MultiMedia. (2022) 29:56–65. doi: 10.1109/MMUL.2022.3141118
78
Wang T Li C Wu C Zhao C Sun J Peng H et al . A gait assessment framework for depression detection using kinect sensors. IEEE Sens J. (2021) 21:3260–70. doi: 10.1109/JSEN.2020.3022374
79
Yang J Lu H Li C Hu X Hu B . Data augmentation for depression detection using skeleton-based gait i nformation. Med Biol Eng Comput. (2022) 60:2665–79. doi: 10.1007/s11517-022-02595-z
Summary
Keywords
depression, gait, bibliometric, VOSviewer, CiteSpace, visual analysis
Citation
Kan S-K, Chen N-N, Peng B and Zhang Y-L (2025) Gait in depression: a bibliometric analysis and knowledge mapping of research trends over the past 20 years. Front. Psychiatry 16:1457176. doi: 10.3389/fpsyt.2025.1457176
Received
30 June 2024
Accepted
23 June 2025
Published
20 August 2025
Volume
16 - 2025
Edited by
Shaohua Hu, Zhejiang University, China
Reviewed by
Jung Goo Lee, Inje University Haeundae Paik Hospital, Republic of Korea
Haifeng Lu, Lanzhou University, China
Azliyana Azizan, UiTM, Malaysia
Updates
Copyright
© 2025 Kan, Chen, Peng and Zhang.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ying-Li Zhang, yinglizhang2000@163.com
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.