 Alicia Norma Alayón1
Alicia Norma Alayón1 Nohora Ochoa Arizal2
Nohora Ochoa Arizal2 Manuel Noreña Correa2*
Manuel Noreña Correa2* Jose López Toro2
Jose López Toro2 Francisco Hernández Rojas3
Francisco Hernández Rojas3- 1Biomedical Research Group, Faculty of Health Sciences, Bacteriology Program, Universidad de San Buenaventura, Seccional Cartagena, Cartagena, Colombia
- 2Psychology Research Group, Faculty of Human and Social Sciences, Psychology Program, Universidad de San Buenaventura, Seccional Cartagena, Cartagena, Colombia
- 3Planning Department, Universidad de San Buenaventura, Seccional Cartagena, Cartagena, Colombia
Background: Considering the general trend toward an increased occurrence of cardiovascular and mental health diseases, we studied the relationship between the presence of trait and state anxiety and the alteration of serum cortisol, lipid, and glycemia levels.
Material and methods: The study assessed 90 full-time workers waist circumferences, as well as their cortisol levels at 8 AM and 4 PM, and their fasting serum glucose and lipid profiles. The construct of trait and state anxiety was assessed by means of the Inventory of Trait-State Anxiety (IDARE Spanish version).
Results: The state anxiety scale showed high reliability (ω = 0.94, α = 0.939). Moderate to high state anxiety was observed in 61.1% of participants, while 71.1% had moderate to high trait anxiety. Most participants (94.4%) had AM and PM cortisol levels within normal ranges. PM cortisol levels were lower than AM cortisol levels in 95.6% of participants (86/90). Dyslipidemia was present in 60.4% of participants. No significant sex differences were found in AM and PM cortisol or anxiety levels, except for triglycerides, which were higher in men (p = 0.013). State anxiety was positively correlated with PM cortisol levels (r = 0.232, p = 0.028), no significant associations were found with AM cortisol or age. A significant association was observed between waist circumference and fasting glycemia, with 68.9% of participants exceeding the recommended waist circumference threshold. Obesity was significantly associated with hyperglycemia (p = 0.010). An ANOVA revealed a significant effect of state anxiety on evening cortisol levels (F(2, 87) = 7.336, p = 0.001), with the high state anxiety group exhibiting the highest PM cortisol levels. Additionally, a t-test found a significant difference in triglyceride levels between the presence and absence of state anxiety t (87.999) = -2.244, p = 0.027.
Conclusions: The presence of state anxiety proved to be the type of anxiety most associated with increased evening cortisol levels and triglyceride levels. Understanding the relationships between mental states and biochemical physical conditions will be essential in the future for maximizing the benefits of technological developments applied to the diagnosis, prognosis, and monitoring of patients’ overall health.
1 Introduction
Mental health is a significant component of the well-being of human beings. The World Health Organization describes it as a state of well-being in which individuals exercise their abilities, cope with the stresses of life, work productively and fruitfully, and give something to their community (1). Mental disorders cause alterations in individuals’ thoughts, emotions, and behaviors, which interfere with their quality of life and functionality (2). Additionally, mental disorders are associated with different medical conditions. They may affect their etiology or be correlated or coexist with physical diseases, for example, cardiovascular conditions, diabetes, infectious diseases, cancer (3), and chronic pain (4).
Anxiety disorders are the most prevalent mental disorders in the world; in 2019, they affected 301 million people (5). In Colombia, the 2015 National Survey of Mental Health conducted in adults reported a prevalence of 1.6% for major depression, 0.3% for generalized anxiety, and 2.1% for any anxiety disorder (6). It can be seen that anxiety, in particular, is one of the most frequent health concerns in the world and Colombia, so actions for its prevention and effective treatment are needed.
Clark and Beck (7) define anxiety as “a behavioral, physiological, affective, and cognitive response to events that are perceived as threats to vital interests and as uncontrollable or unpredictable.” These authors differentiate anxiety from fear by considering the latter as a primitive automatic neurophysiological response to perceived imminent dangers to physical or psychological safety.
Some common physical symptoms of anxiety are tremors in the body or hands, hot flashes, chills, palpitations, dry mouth, sweating, shortness of breath, chest pain or pressure, and muscle tension (8). Moreover, the neuroendocrine or metabolic basis of anxiety initially has an adaptive purpose, as it physically prepares the organism to face a possible threat. This is evident in some hyperactivation signs triggered by anxiety, such as peripheral blood vessel constriction, increased skeletal muscle strength, increased heart rate and lung contraction and expansion capacity to promote oxygenation, dilation of the pupils to improve vision, reduced digestive activity, increased basal metabolism, and increased epinephrine and norepinephrine release from the adrenal medulla (7).
Faculty members are not exempt from anxiety-related phenomena and, in fact, may be exposed to particularly anxiety-inducing situations. Research has shown that academic environments present unique stressors that contribute to faculty distress, including workload, performance pressures, and student interactions. A study conducted at West Visayas State University identified paperwork and administrative responsibilities as primary sources of stress among faculty, with high blood pressure and anxiety reported as common physiological and emotional consequences (9). Similarly, Filaire et al. (10) found that lecturing to a large audience led to significant increases in salivary cortisol and alpha-amylase, indicating heightened activation of the hypothalamic–pituitary–adrenal (HPA) axis and sympathetic-adrenal-medullary (SAM) system. These physiological changes were accompanied by elevations in pro-inflammatory cytokines, suggesting an immune response to acute psychological stress. Additionally, Sabagh et al. (11) highlighted that faculty burnout is strongly associated with excessive job demands, value conflict, and lack of institutional support, leading to adverse psychological and physical health effects, such as depression and reduced job performance. These findings collectively underscore the impact of chronic and acute stress in academia, reinforcing the need for institutional strategies to mitigate anxiety and cortisol dysregulation among faculty members.
More generally, given that anxiety is the most prevalent mental disorder, it correlates with a wide range of physical diseases; for example, anxiety correlates with endocrine disorders, including diabetes mellitus, thyroid disease, and catecholamine-producing neuroendocrine tumors like pheochromocytomas (12). It is also associated with gastrointestinal disorders such as peptic ulcers, celiac disease, and irritable bowel syndrome. In addition, it is associated with musculoskeletal disorders such as fibromyalgia/chronic fatigue syndrome and arthritis, as well as neurological disorders such as migraines, epilepsy, and neurodegenerative diseases. Cardiorespiratory diseases such as asthma, angina pectoris, chronic obstructive pulmonary disease, mitral valve prolapse, cystic fibrosis, and obesity also show a relationship with anxiety. Furthermore, chronic pain, including burns and cancer, as well as infectious diseases such as human immunodeficiency virus and tuberculosis, may be exacerbated by anxiety (3). The relationship between mood and metabolic dysfunctions may perpetuate the cycle (13).
In this study, we use the concepts of trait anxiety and state anxiety put forward by Spielberger et al. (14). On the one hand, “trait anxiety” refers to constant anxiety experienced by individuals and is identified as a personality trait, so it is more stable and permanent over time. On the other hand, “state anxiety” is considered a transitory emotional state occurring in response to a particular stressful situation. These concepts are crucial to understanding how external and internal (e.g., cognitive) factors can trigger anxiety (8).
One of the metabolic responses related to coping with a stressful situation is the secretion of cortisol, a cholesterol-derived hormone and the main glucocorticoid produced in the cortex of the adrenal glands, located in the upper part of both kidneys. Its main functions include lipid reorganization and metabolism, as well as insulin secretion, blood pressure increase, and suppression of the immune system as an anti-inflammatory mechanism (15).
When released, it can inhibit the hypothalamic release of corticotropin-releasing hormone and pituitary release of adrenocorticotropic hormone, known as negative feedback. Under persistent stress conditions, this negative feedback loses effectiveness, and high cortisol levels may remain for a long time, so it can still exercise its supportive functions to face situations that may be perceived as threats (16, 17).
Similarly, it has been evidenced that glucocorticoids and insulin enhance the consumption of fatty foods, which allows us to suppose that the combination of high insulin and cortisol levels can be a powerful inducer of obesity and insulin resistance (18, 19). Currently, it is estimated that there are more than 300 million individuals with obesity, and this figure is expected to increase considerably in the coming years (20). In addition, cardiovascular risk is still one of the leading causes of death in the world.
A meta-analysis encompassing data from 33 studies and over 43,000 participants concluded that elevated stress hormone levels are associated with a higher risk of cardiovascular disease (risk ratio [RR], 1.63; 95% confidence intervals [CIs]: 1.36, 1.97) (21). Discrepancies observed when comparing results from various studies on the relationship between cardiovascular risk and hormones related to anxiety and stress highlight the complexity of this association (22). Part of this complexity lies in the fact that this relationship is influenced by other risk behaviors such as unhealthy diets, physical inactivity, or tobacco use, among others (23). Nevertheless, it is known that hormones associated with states of anxiety, worry, or stress, such as cortisol, can activate pathways leading to increased inflammation and heart rate, as well as platelet alterations, increased sympathetic activity, and reduced parasympathetic activity (24). Therefore, as suggested by Merswolken et al. (25), the evidence linking cortisol level alterations with hypertension, obesity, insulin resistance, hyperlipidemia, and prothrombotic activity suggests that adrenal axis dysfunction may be responsible for the metabolic disturbances that promote cardiovascular disease.
In Colombia, data collected by the Instituto Colombiano de Bienestar Familiar (Colombian Institute of Family Welfare) in the 2015 Colombian Nutrition Survey evidenced that 37.8% of adults between 18 and 64 years of age were overweight and 18.7% were obese (26). Overweight and obesity were more frequent in women than in men (33% vs. 31.1%) (27). There is scientific evidence that describes weight gain, insulin resistance, and hypercortisolism as biochemical factors that could be activated by different life situations, including anxiety and stress (28).
Considering the mental health statistics of the Colombian population and the consistent trend in morbidity and mortality statistics for cardiovascular diseases, the purpose of this study was to evaluate the possible association between trait and state anxiety and altered serum levels of cortisol, lipids, and glycemia, as well as central obesity. These are known factors for cardiovascular risk, which has been scarcely studied in Cartagena and Colombia.
2 Methods
2.1 Participants
We included 90 participants of both sexes (47 female, 43 male), ranging in age from 25 to 69 years (X̅ = 44.1, SD = 10.9), who met the inclusion criteria. They were selected from a list of 148 faculty members employed full-time. The study sample was drawn from faculty members of a private higher education institution, which comprises five faculties: Education, Social Sciences, Health Sciences, Administrative and Accounting Sciences, Political Sciences, and Engineering, with a student population of approximately 3,300.
As inclusion criteria, we selected faculty members with full-time contracts and more than two years of experience at the university. As exclusion criteria, those receiving medication or dietary regimens that could alter glucose or cortisol levels, diabetes mellitus diagnosis, or adrenal axis dysfunction were not accepted as they could interfere with the results. Each participant provided their written informed consent, and the study was granted ethical approval from the University’s Research Ethics Committee (project code: CIB-CS-2023-01; date of approval: April 18, 2023; Ethics Approval Code Record No. 02/2023). This study followed the guidelines set by the Declaration of Helsinki, and all participants provided written informed consent.
2.2 Procedures
2.2.1 Biochemical and anthropometric variables
This quantitative study was conducted with an analytical cross-sectional design, with fasting blood sampling to determine participants’ glycemia and lipid profile levels through spectrophotometric techniques. Participants were instructed to refrain from engaging in physical exercise on the day of sample collection and to abstain from consuming alcoholic beverages for three days prior to venipuncture. Additionally, they were asked to arrive 15 minutes in advance. Dyslipidemia was considered when two or more lipid profile values were altered. Cortisol was measured at 8 AM and 4 PM using a commercial kit based on an electrochemiluminescent immunoassay (Elecsys cortisol II®). In all cases, quality controls were used to ensure the validity of the results.
Serum cortisol measurement was preferred in both samples, despite being more invasive than its salivary equivalent, because available evidence has shown that it provides more reliable results and greater discriminatory power (29, 30). Saliva samples, on the other hand, require more stringent collection protocols and exhibit greater variability due to factors such as body weight, caffeine and alcohol intake, antibiotic use, or recent infections (31).
The morning (AM) samples were collected between 8:00 and 9:00 AM, while the evening (PM) samples were taken between 4:00 and 4:30 PM, following the established biosafety protocols for this type of sample. The samples were collected at the clinical laboratory facilities of the university. Serum was immediately separated by centrifugation and stored at 4°C until processing.
Participants’ waist circumference was measured at the midpoint between the last rib and the iliac crest in expiration, using a non-stretch tape measure. To this end, the International Diabetes Federation recommendations for Central and South America were used as cut-off point (>90 cm in men and 80 cm in women) (32).
2.2.2 Psychological variables
To assess trait and state anxiety, we used the Inventory of Trait-State Anxiety (IDARE Spanish version) by Spielberger, C. D., Gorsuch, R. L., Lushene, R., Vagg, P. R., and Jacobs, G. A., which consists of two separate self-assessment scales, each with 20 statements (1983).
This test has several adaptations that ratify its reliability. In the Peruvian adaptation carried out with patients attending weight control, it was found that the Inventory had consistent, objective, and significant psychometric features regarding content, construct, concurrent, and clinical validity. It also has reliability in terms of internal consistency and stability (33). Another study conducted during the COVID-19 pandemic in Peru confirms its psychometric reliability, concluding that it has an adequate factorial structure, measures correctly, and maintains its qualities as an instrument for the evaluation of anxiety (34).
3 Data analysis
All data were initially organized using Microsoft Excel and then analyzed using JASP. Descriptive statistics were computed first to summarize the dataset. To examine sex differences, independent samples Student’s t-tests were conducted for morning cortisol (AM), evening cortisol (PM), state anxiety, trait anxiety, and triglycerides. Pearson’s correlation analyses were performed to assess the relationships between morning cortisol, evening cortisol, state anxiety, trait anxiety, and age. Additional Pearson’s correlations were conducted to examine associations between waist circumference and glucose levels.
A Chi-square test was performed to examine the association between abdominal obesity and hyperglycemia, as well as other variables from the lipid profile. Next, a one-way ANOVA was conducted to compare evening cortisol (PM) levels across low, medium, and high state anxiety groups. Finally, a Welch’s t-test was performed to compare triglyceride levels between the presence and absence of state anxiety, as the Brown-Forsythe test indicated a violation of homogeneity of variances.
4 Results
The group consisted of 90 participants, with an average age of 44.1 years (SD = 10.9; range = 25–69) and a slight female predominance (47/90; 52.2%).
The internal consistency of the state anxiety items was assessed using McDonald’s Omega (ω) and Cronbach’s Alpha (α). The results indicated high reliability, with ω = 0.94, 95% CI [0.922, 0.958] and α = 0.939, 95% CI [0.918, 0.959].
61.1% (55/90) of participants had medium and high levels of state anxiety, and 71.1% (64/90) had medium and high levels of trait anxiety. Women more frequently exhibited high state anxiety and moderate trait anxiety, whereas men more commonly reported moderate trait anxiety (Figure 1).
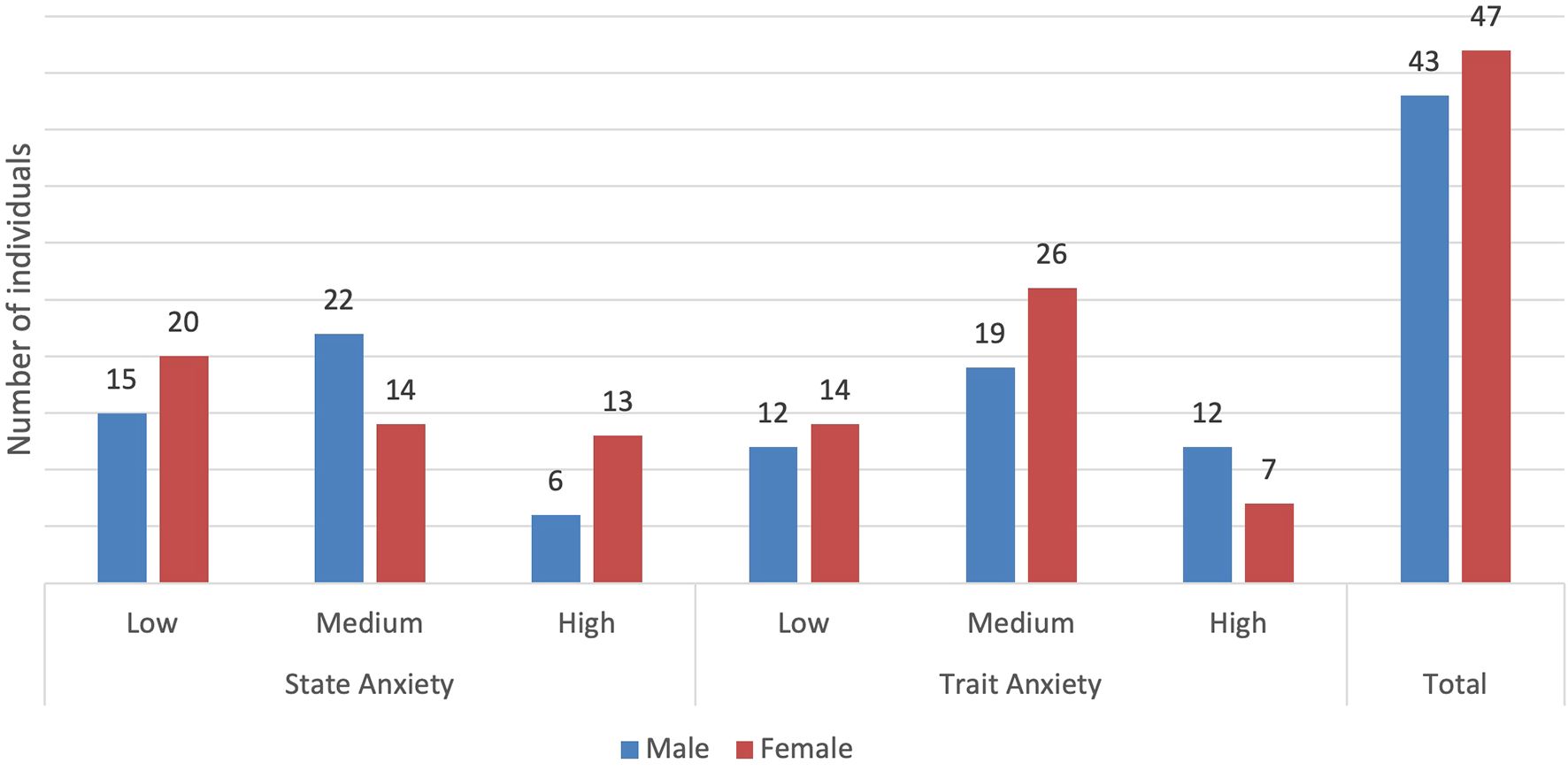
Figure 1. Presence of state and trait anxiety by levels and sex (frequency).
Most participants (94.4%) had AM and PM cortisol levels within normal ranges. The mean AM cortisol was 9.83 µg/dL (SD = 3.63, 95% CI = 9.07–10.59), while the mean PM cortisol was 5.96 µg/dL (SD = 2.74, 95% CI = 5.38–6.53). Cortisol levels were lower in the evening than in the morning for 95.6% of participants (86/90), with AM cortisol ranging from 0.22 to 23.11 µg/dL and PM cortisol from 0.34 to 19.29 µg/dL (Table 1). Below-normal levels were observed in 3.3% of participants, and 2.2% had above-normal levels in both measurements. The reference limits were those established by Maji Llinin and Durán Pincay (35).
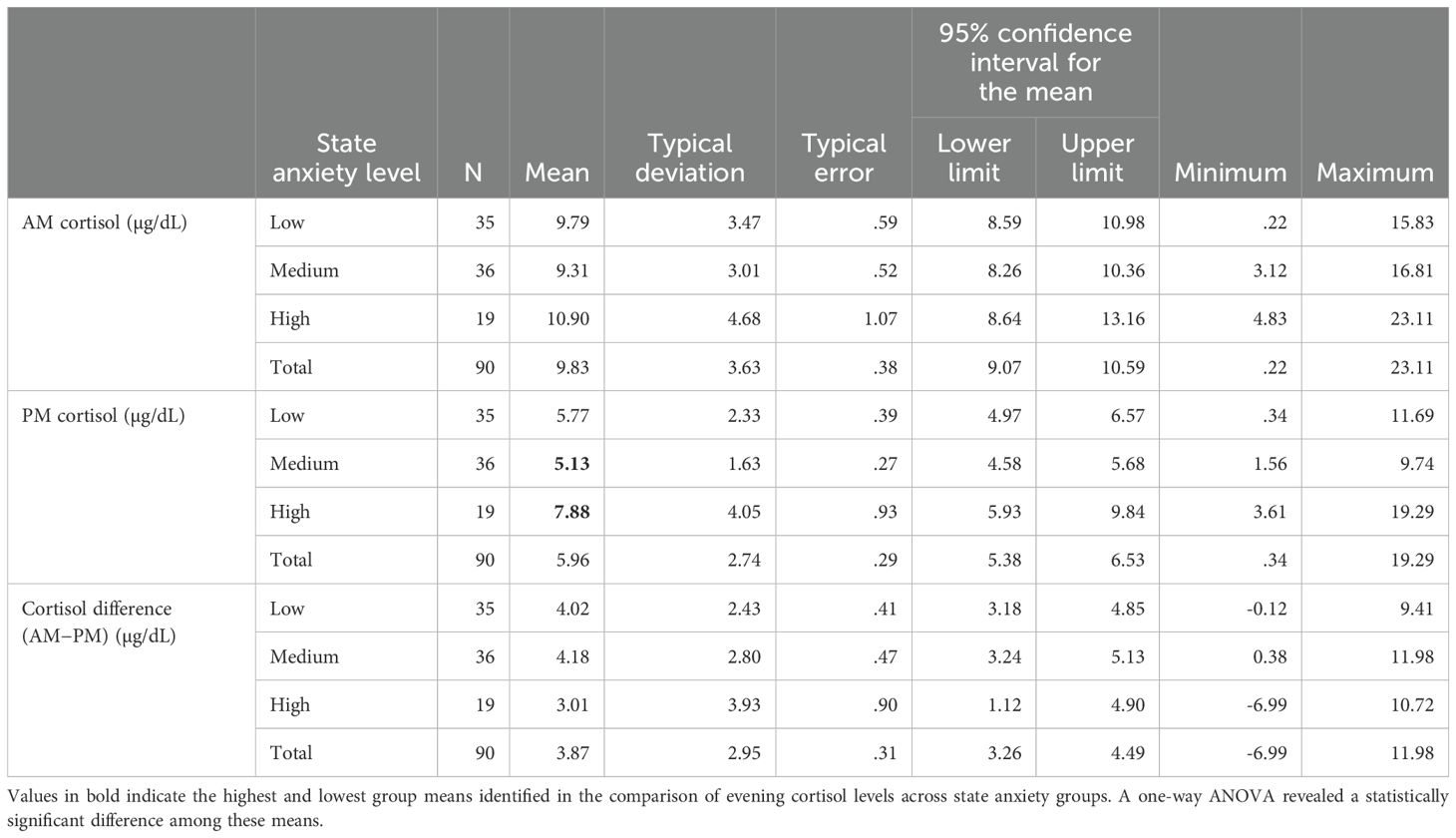
Table 1. AM and PM cortisol levels; total values and values discriminated by state anxiety levels.
The presence of dyslipidemia, defined as the simultaneous alteration of two or more lipid parameters (total cholesterol, triglycerides, and HDL and LDL cholesterol fractions), was observed in 60.4% of the sample (54/90) (Figure 2).
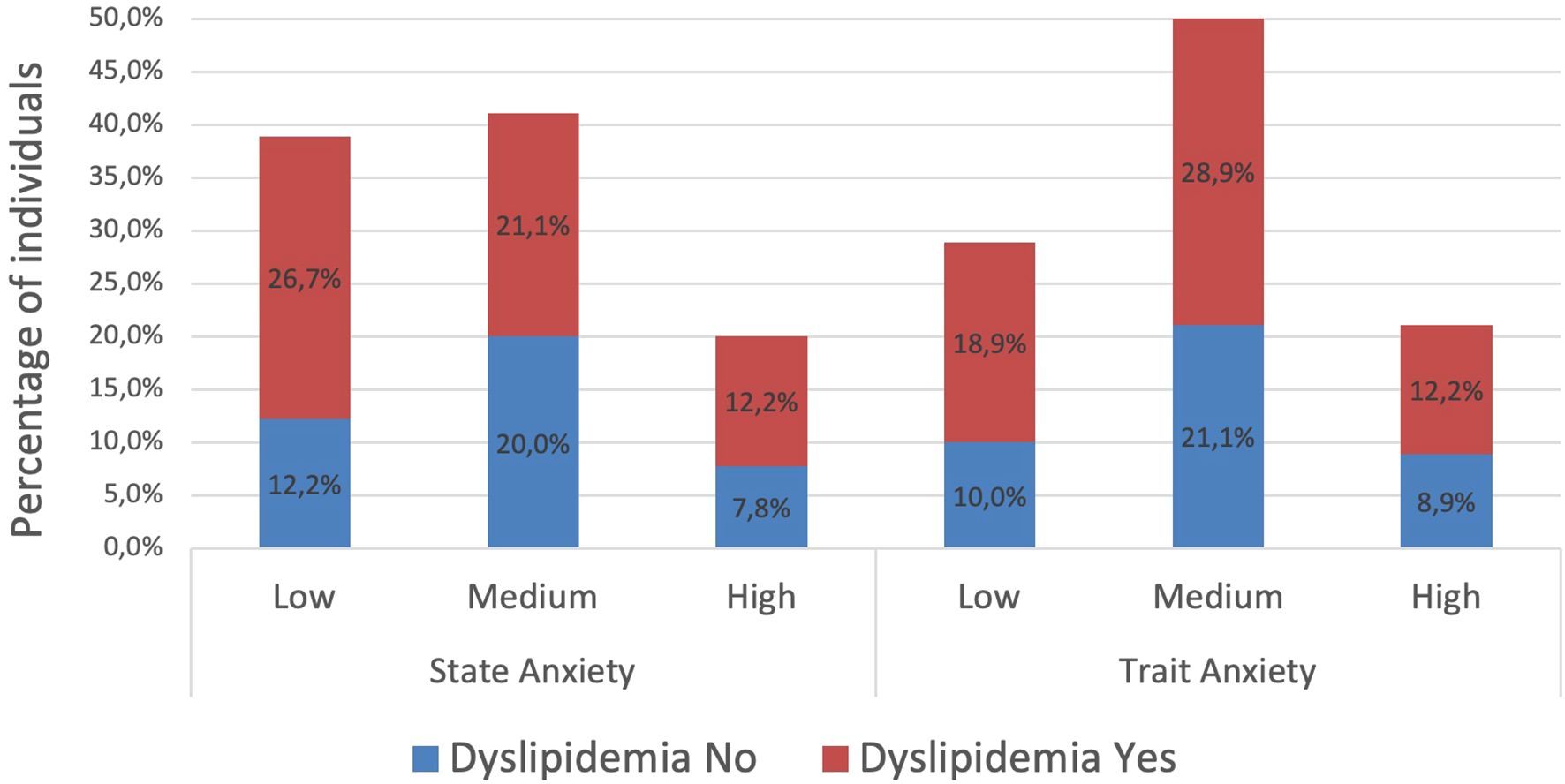
Figure 2. Dyslipidemia (two or more altered parameters) observed in participants divided by level of state or trait anxiety.
Independent t-tests were conducted to compare differences by sex in morning and evening cortisol levels, as well as in state and trait anxiety scores. No significant differences were found between male and female participants in any of these variables, except for triglycerides (t = -2.535, df 89, p= 0.013) (Table 2).
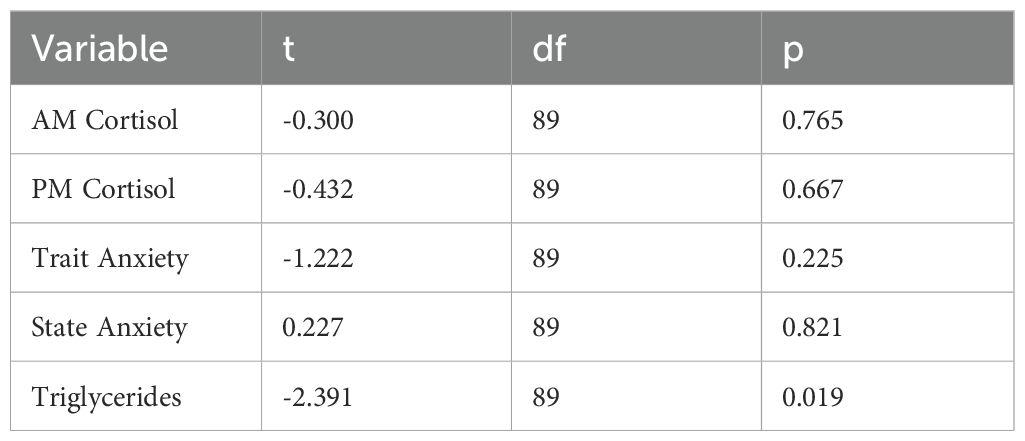
Table 2. Independent samples t-test.
Pearson’s correlation analysis showed a significant positive association between state anxiety and PM cortisol levels (r = 0.232, p = 0.028), while no significant relationship was found with AM cortisol concentrations. Additionally, neither cortisol patterns nor anxiety measures (state or trait) were significantly associated with age (Table 3).
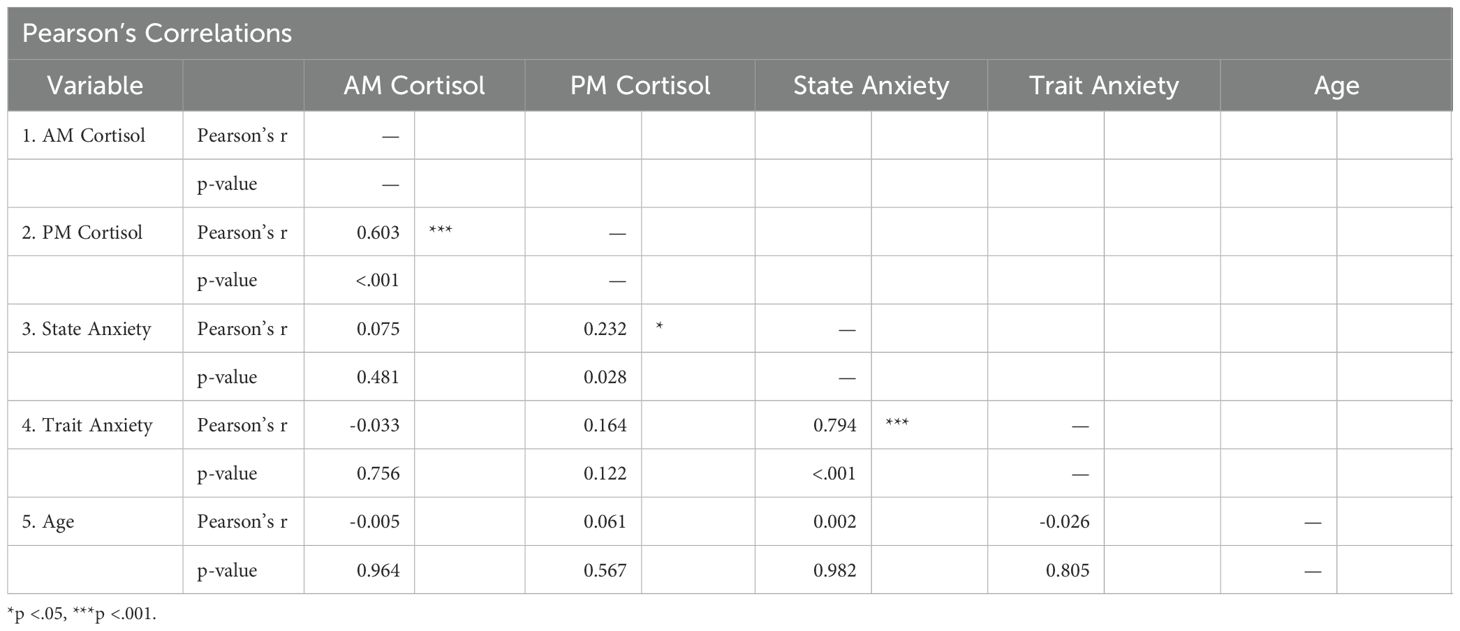
Table 3. Pearson’s correlations between cortisol levels, anxiety scores, and age.
Of all participants, 68.9% (62/90) had a waist circumference greater than 80 cm in women and 90 cm in men. Pearson’s correlation analysis showed a significant association between waist circumference and fasting glycemia (Table 4). Additionally, fasting glycemia was elevated in 11 participants (12.2%).
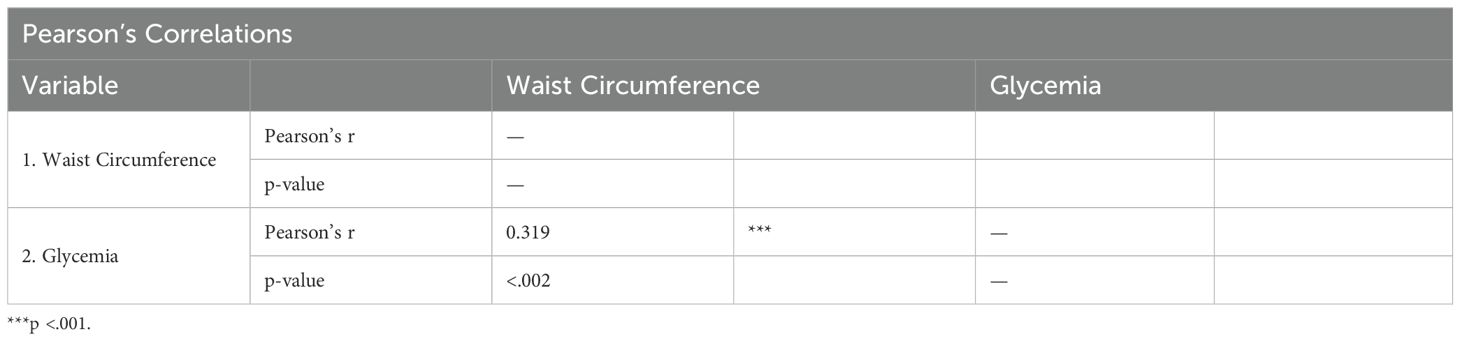
Table 4. Pearson’s correlation between waist circumference and glycemia.
Using a Chi-square test, the presence of abdominal obesity showed a significant association with hyperglycemia (p = 0.010, df = 2), but not with the other variables from the lipid profile.
A one-way ANOVA was conducted to examine differences in evening cortisol levels across state anxiety levels (low, medium, and high). The results indicated a significant effect of state anxiety on evening cortisol levels, F(2, 87) = 7.336, p = 0.001. Mean comparisons showed that individuals in the high state anxiety group had the highest evening cortisol levels (X̅ = 7.88, SD = 4.05), followed by those in the low state anxiety group (X̅ = 5.77, SD = 2.37), while the moderate state anxiety group had the lowest levels (X̅ = 5.13, SD = 1.63).
Similarly, the one-way ANOVA revealed a statistically significant difference in mean PM cortisol levels among state anxiety groups (F(2, 87) = 7.336, p = 0.001). The high state anxiety group had the highest mean cortisol levels (X̅ = 7.88 µg/dL), followed by the low state anxiety group (X̅ = 5.77 µg/dL) and the moderate state anxiety group, which had the lowest mean levels (X̅ = 5.13 µg/dL).
An independent samples Welch’s t-test was conducted to compare the concentrations of each evaluated lipid fraction based on the absence (low levels) and presence (medium and high levels) of state anxiety. Welch’s t-test was preferred since the Brown-Forsythe test indicated a violation of homogeneity of variances when using Student’s t-test in multiple comparisons. A significant difference was found only for triglyceride levels between the absence and presence groups. The Welch’s t-test indicated a statistically significant difference, t(87.999) = -2.244, p = 0.027. The presence group had a higher mean triglyceride level (X̅ = 129.58, SD = 62.32) compared to the absence group (X̅ = 105.53, SD = 39.32).
5 Discussion
No significant differences were observed between sexes for any type of anxiety, although higher levels may be expected in women, as it has been evidenced in several epidemiological studies in which anxiety has a marked influence on females (8). This effect, however, could be more pronounced with larger samples.
It was found that substantial cortisol alterations in the afternoon were associated with state anxiety, which highlights the importance of studying the presence of other medical and mental health conditions due to the high correlation among anxiety, other mental health conditions, and physical diseases (3). Our findings also support the role that mental diseases, and particularly anxiety, may play in the onset or prevalence of medical conditions via cortisol alterations (36). In the following paragraphs, our study results are contrasted with those of previous studies that support the conclusions mentioned above.
Anxiety as an assessment measure for psychological dysfunction is particularly relevant, not only because it is the most prevalent mental disorder, but also because it has regularly been found as a comorbidity of other mental health conditions. For example, Mielimąka et al. (37) found that 69% of patients with personality disorders had state anxiety and 64.7% had trait anxiety. For this reason, personality disorders are a primary condition to take into account in the mental health assessment and intervention of anxious patients.
The results of studies with different designs focused on social anxiety are consistent with our findings and conclusions about the relevance of anxiety as a risk factor, especially in stressful situations. Mirete et al. (38) studied the increase in salivary cortisol levels in individuals with high and low levels of social anxiety in the face of stressful situations and found that in both groups, cortisol levels varied under stress conditions, although the response was significantly higher in individuals with high anxiety levels.
Our findings showed a significant relationship between the presence of state anxiety and the increase in evening cortisol concentrations. In addition, there is a tendency toward an inverse relationship with a reduced difference between AM and PM cortisol levels in the groups with higher levels of trait anxiety. This is consistent with the evidence showing a relationship between circadian rhythm maintenance and health and points to the importance of assessing cortisol levels at these two times to conduct a comprehensive monitoring of the psychological and biological state of individuals (39).
The relationship between PM cortisol levels and state anxiety has also important implications for the development of anxiety management strategies. In particular, the possible dysregulation of the HPA axis in response to stress, along with the association between elevated PM cortisol levels, greater emotional reactivity, and a lower capacity for stress recovery (40, 41), suggests the need to explore interventions focused on stress regulation, lifestyle, and sleep. These strategies may contribute to better physiological and emotional adaptation to stress, as well as a reduction in state anxiety.
In this regard, Cognitive Behavioral Therapy (CBT) has shown promising effects in regulating cortisol levels and sleep patterns across various populations. In older adults with generalized anxiety disorder, combining CBT with SSRI treatment significantly reduced peak cortisol levels compared to SSRI use alone (42). Similarly, pregnant women receiving CBT for stress management experienced reductions in both hair cortisol levels and psychological stress (43). In heart failure patients, although CBT for insomnia did not directly affect cortisol levels, improvements in sleep-related symptoms were associated with an increased day-to-night cortisol ratio (44).
Mindfulness-based interventions have also demonstrated positive effects on stress regulation and cortisol levels. Long-term meditators exhibit reduced morning cortisol levels, while novices who completed an eight-week Mindfulness-Based Stress Reduction (MBSR) program showed lower cortisol levels and improved sleep quality (45). In cancer patients, MBSR helped normalize cortisol levels by increasing low baseline levels and reducing elevated ones (46). Even short programs, such as a four-day mindfulness meditation training for medical students, have been shown to significantly reduce serum cortisol levels (47).
Additionally, physical activity plays a key role in stress regulation and cortisol levels. Regular aerobic exercise has been associated with more adaptive cortisol secretion patterns and lower stress reactivity (48). Moreover, sleep hygiene interventions, such as Cognitive Behavioral Therapy for Insomnia (CBT-I), have shown positive effects in normalizing circadian cortisol rhythms and reducing state anxiety (49). Since both sleep and physical activity directly influence HPA axis function, integrating these strategies into stress management programs could enhance the effects of other psychological interventions and improve long-term emotional regulation.
Given the significant association between cortisol and anxiety in educators, implementing evidence-based stress reduction programs specifically tailored to this population could be instrumental in promoting faculty well-being and preventing burnout. Wagner and Pearcey (50) found that different stress reduction activities had varying effects on salivary cortisol levels in educators. Specifically, meditation and yoga significantly reduced cortisol levels 30 minutes post-activity, while aerobic exercise paradoxically increased cortisol levels, suggesting that certain interventions may be more effective in mitigating physiological stress responses. Similarly, von der Embse et al. (51) conducted a systematic review of teacher stress interventions, concluding that mindfulness-based, behavioral, and cognitive-behavioral approaches were the most effective at reducing educator stress and improving occupational outcomes. These findings align with our results, emphasizing the need for targeted interventions that address both the psychological and physiological aspects of anxiety among faculty members.
Although the cross-sectional design of this study does not allow for the establishment of cause-and-effect relationships, it is important to consider that the relationship between cortisol levels and mental states could be bidirectional, as stated by Qin et al. (52). This situation once again highlights the complexity that must be acknowledged when studying human beings, given that the presence of anxiety triggers cortisol release and alters cardiovascular health, including body weight and fat distribution, which in turn also influences anxiety levels. Longitudinal studies under more controlled conditions could be useful in clarifying the predominant directionality.
The evidence obtained in a group of patients with depression showed that alterations in the circadian rhythm of cortisol were more frequent in the group that also had anxiety, which suggests that these values should be used as one of the markers of depression and anxiety (53) and should be taken into account when assessing cardiovascular risk related to excess cortisol and rhythm alterations (54).
Other studies have shown that cortisol levels are positively associated with negative thoughts, and the intensity of the latter affects the onset of anxiety and depression. This justifies the need to include these values in screening this type of disorder (55).
An experimental study with young individuals with high and low social anxiety evidenced a positive correlation for cortisol increase as a consequence of a greater stress factor in the group with high social anxiety, which implies a greater reactivity of the adrenocortical axis under these conditions (38). In fact, these alterations could be associated with chronic diseases, such as cancer, and it has been suggested that glucocorticoid levels may favor tumor growth and be related to psychological states (56).
In 2009, Veen et al. published the results of a study of 72 adults with depression or anxiety, in which they concluded that high baseline cortisol concentrations and decreased circadian variability of cortisol were associated with less favorable lipid profiles, in particular due to decreased high-density lipoprotein–cholesterol. This supported the hypothesis of a verifiable relationship between affective disorders and cardiovascular disease mediated by the adrenal axis (57).
More recently, Anni et al. (58) found that stressful life events were significantly associated with altered lipid patterns and elevated serum triglyceride levels in middle-aged Korean men, highlighting the potential metabolic impact of psychological stress. Other authors, on the contrary, have reported an increase in cholesterol and no association with triglycerides (59). These discrepancies may be attributed to the approach used to define the presence of anxiety, an aspect that should be standardized and validated through its application in population studies, given that different stressors could trigger various forms of adrenal axis activation and, consequently, different impacts on serum biochemical levels.
Studies exploring suicidal ideation, acute coronary syndrome, and cortisol levels have shown that the prediction of suicide could be improved by assessing serum cortisol in its acute phase, which could also impact morbidity and mortality in patients with heart conditions, which is especially relevant in cardiovascular clinics (60). Among young people, depression was associated with increased cortisol in saliva and serum triglycerides, which may also increase their cardiovascular risk (61).
Regarding the presence of state and trait anxiety in our study group, we found medium and high levels of 61.5% and 71.4% for state and trait anxiety, respectively, with no difference between the sexes. Previous studies in healthcare workers had shown moderate or severe anxiety levels in 26.1% of participants; these values, which are very low when compared with our findings, reported an association with dyslipidemia (PR = 2.07; 95% CI = 1.74–2.45). This differs from our results, although there is a similarity regarding the high frequency of dyslipidemia (54.8%) (62).
In addition, it is known that anxiety-related disorders have been linked to alterations in lipid metabolism due to chronic deregulation of the adrenal axis and the action of the hormones related to this state, such as catecholamines and gamma-aminobutyric acid. Cholesterol, the main source of steroid hormones, plays a very important role in this axis, including circadian rhythm, stress, and neuropsychiatric disorders (63).
Based on the results obtained, it is possible to suggest that state anxiety may be associated with the sustained elevation of cortisol levels. No studies were found that specifically examined the impact of each type of anxiety on the expected decline in serum cortisol concentrations in the afternoon. However, our findings align with the evidence reported by Mohd Azmi et al. (54), which indicates that cortisol regulates the circadian rhythm and is linked to cardiovascular disease.
In cases of sleep disorders, jet lag, or mental conditions such as stress or anxiety, circadian dysfunction can be explained by the loss of negative feedback on the adrenal axis, which could account for the sustained increase in cortisol levels in the afternoon among individuals with higher anxiety levels. Additionally, the greater incidence of circadian cortisol alterations observed in patients with depression accompanied by anxiety (53) further supports this association.
In contrast to our findings, a study conducted in 2013 with a sample of 142 individuals showed that total cholesterol and high-density lipoprotein levels were higher in the group with higher levels of anxiety, but no differences were found for triglyceride, high-density lipoprotein, and platelets (59).
In addition to the above, a study conducted in patients with personality disorders also showed a positive relationship between cortisol and testosterone levels, which seems to suggest that sex could be related to alterations in the adrenal axis (64). Previous studies have shown that gender perception was related to different biological responses to an intervention aimed at improving regulation, suggesting that gender roles may influence the hypothalamic–pituitary–adrenal axis function during episodes of acute stress (65).
Multiple studies agree on the effect of negative experiences in childhood on alterations of the adrenal axis (66, 67), and show varying degrees of association with the onset of depression and anxiety, establishing a link between these experiences and adult mental health (68). In contrast to these findings, our results showed no differences between sexes, suggesting that it may be necessary to study this aspect in depth and include other variables, improving the approach to gender perceptions and childhood experiences that could affect adulthood.
Currently, hybrid models have been proposed to promptly identify heart diseases (69), accurately and reliably classify lung cancer types (70), and, by leveraging the strengths of combined models, integrate complex aspects such as space-time relationships, as proposed by Ali et al. (71). These models would be particularly useful for establishing more precise relationships between variables that follow a circadian rhythm, such as cortisol.
One limitation of our study is that it did not address aspects related to participants’ previous experiences, including their childhood and adolescence, which could have provided robust follow-up of these disorders. In addition, lifestyle assessments that could positively or negatively affect the associations observed were not included. However, it is worth mentioning that participants who followed special diets or used medications that could affect the results were excluded.
6 Conclusion
The presence of abdominal obesity and lipid profile alterations were frequent, regardless of age or sex, as well as medium and high levels of trait and state anxiety.
Our study results showed cortisol levels within the reference values in most of the participants, although alterations in the afternoon were also observed. These were associated with state anxiety, which highlights the importance of studying the presence of other medical and mental conditions due to the high correlation between anxiety, other mental conditions, and physical diseases. Our findings also support the role that mental diseases, particularly anxiety, may play in the onset of medical conditions via cortisol alterations.
Furthermore, this study confirms the association between lipids, cortisol and anxiety, which has been reported by a growing number of studies, which highlights the potential value of measuring this hormone during medical examinations, preventive medicine, and mental health interventions, either through psychopharmacological and/or psychotherapeutic treatments.
Our findings, together with those of similar studies following the same lines, support the statement that mental health interventions, such as psychoeducation, training in stress management, problem-solving skills, social skills, and emotional regulation, among others, are important for preventing diseases. In the case of anxiety, interventions aimed at its mitigation or prevention may also help prevent cardiovascular diseases (and others) resulting from the sum of lipid and glycemia alterations and consistently high cortisol levels. The presence of state anxiety was found to be the type of anxiety most associated with increased evening cortisol levels and triglyceride levels.
It is relevant to continue exploring the relationships between psychological and biochemical variables, as they could serve as important inputs for developing AI-supported programs that enhance the diagnosis, monitoring, and outcomes of physical and mental health treatments.
The differences observed in other studies regarding the association found between the levels of anxiety, cortisol, and lipids could be due, in part, to the high frequency of alterations in the biochemical variables in most of the study population. This reflects the importance of approaching health from a global perspective that integrates biological and psychological factors to contribute to the present and future well-being of the population.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by University’s Research Ethics Committee (project code: CIB-CS-2023-01; date of approval: April 18, 2023; Ethics Approval Code Record No. 02/2023). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AA: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. NO: Investigation, Writing – review & editing. MN: Data curation, Writing – review & editing. JL: Investigation, Writing – review & editing. FH: Funding acquisition, Project administration, Resources, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by the Universidad de San Buenaventura, Cartagena, Colombia (grant number: CIB-CS-2023-01).
Acknowledgments
The authors would like to thank the study participants and Universidad de San Buenaventura, Cartagena, for making this research possible. The authors thank Crimson Interactive Pvt. Ltd. (Enago) – https://www.enago.com/es/ for their assistance in manuscript translation and editing. Generative AI (ChatGPT, OpenAI) was used to assist in refining specific elements of the manuscript’s wording. All content was reviewed and approved by the authors.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Pan American Health Organization. Plan de acción sobre Salud mental 2015-2020, in: 2015-2020 mental health action plan (2014). Available online at: https://www.paho.org/hq/dmdocuments/2015/plan-de-accion-SM-2014.pdf (Accessed 3.24.24). WWW Document.
2. Pan American Health Organization. La OMS y la OIT piden nuevas medidas para abordar los problemas de salud mental en el trabajo, in: WHO and ILO call for new measures to address mental health problems at work (2022). Pan American Health Organization. Available online at: https://www.paho.org/es/noticias/28-9-2022-oms-oit-piden-nuevas-medidas-para-abordar-problemas-salud-mental-trabajo (Accessed March 27, 2024).
3. Sartorius N, Holt RIG, Maj M. Comorbidity of mental and physical disorders. Basel, Switzerland:Karger (2015).
4. Scott KM, Hwang I, Chiu WT, Kessler RC, Sampson NA, Angermeyer M, et al. Chronic physical conditions and their association with first onset of suicidal behavior in the world mental health surveys. Psychosom Med. (2010) 72:712–9. doi: 10.1097/PSY.0b013e3181e3333d
5. World Health Organization. Trastornos de ansiedad, in: Anxiety disorders (2023). Available online at: https://www.who.int/es/news-room/fact-sheets/detail/anxiety-disorders (Accessed 4.28.24).
6. Ministerio de Salud y Protección Social de Colombia [Colombian Ministry of Health and Social Protection]. Minsalud, comprometido con la salud mental de los Colombianos, in: Ministry of Health: committed to Colombians’ mental health (2021). Available online at: https://www.minsalud.gov.co/Paginas/Minsalud-comprometido-con-la-salud-mental-de-los-Colombianos.aspx (Accessed 5.2.24). WWW Document.
7. Clark DA, Beck AT. Terapia cognitiva para trastornos de ansiedad [Cognitive therapy for anxiety disorders. Desclée Brouwer. (2012).
8. Barlow DH, Allen LB, Choate ML. Anxiety and its disorders, The nature and treatment of anxiety and panic. New York, NY, United States: Guildford Press (2002).
9. Colacion-Quiros H, Gemora RB. Causes and effects of stress among faculty members in a state university. Asia Pacific J Multidiscip Res. (2016) 4:18–27.
10. Filaire E, Larue J, Portier H, Abed A, Pavon-Djavid G, Teixeira A, et al. Lecturing to 200 students and its effects on cytokine concentration and salivary markers of adrenal activation. Stress Health. (2011) 27(2):e25–35. doi: 10.1002/smi.1332
11. Sabagh Z, Hall NC, Saroyan A. Antecedents, correlates and consequences of faculty burnout. Educ Res. (2018) 60(2):131–56. doi: 10.1080/00131881.2018.1461573
12. Jia S, Li C, Lei Z, Xia Q, Jiang Y. Determinants of anxiety and depression among pheochromocytoma patients: A case–control study. Medicine. (2021) 100:e24335. doi: 10.1097/MD.0000000000024335
13. Fulton S, Décarie-Spain L, Fioramonti X, Guiard B, Nakajima S. The menace of obesity to depression and anxiety prevalence. Trends Endocrinol Metab. (2022) 33:18–35. doi: 10.1016/j.tem.2021.10.005
14. Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, Jacobs GA. Manual for the state-trait anxiety inventory (Form Y). Palo Alto, CA: Consulting Psychologists Press (1983).
15. Katsu Y, Baker ME. Cortisol, in: handbook of hormones. Elsevier. (2021) pp:947–9. doi: 10.1016/B978-0-12-820649-2.00261-8
16. Calle Vera VD, Rodríguez Guaraca GP. Determinación de los niveles de cortisol durante y posterior al período de evaluación académica en los alumnos de la escuela de Bioquímica y Farmacia de la Universidad de Cuenca. In: Determination of cortisol levels during and after the academic evaluation period in students of the School of Biochemistry and Pharmacy of Universidad de Cuenca. Cuenca, Ecuador: Universidad de Cuenca (2015).
17. Incollingo Rodriguez AC, Epel ES, White ML, Standen EC, Seckl JR, Tomiyama AJ. Hypothalamic-pituitary-adrenal axis dysregulation and cortisol activity in obesity: a systematic review. Psychoneuroendocrinology. (2015) 62:301–18. doi: 10.1016/j.psyneuen.2015.08.014
18. Cortés Romero CE, Escobar Noriega A, Cebada Ruiz J, Soto Rodríguez G, Bilbao Reboredo T, Vélez Pliego M. Estrés y cortisol: implicaciones en la ingesta de alimento [Stress and cortisol: implications for food intake. Rev Cubana Investigaciones Biomédicas. (2018) 37:1–15.
19. Wondmkun YT. Obesity, insulin resistance, and type 2 diabetes: associations and therapeutic implications. Diabetes Metab Syndr Obes Volume. (2020) 13:3611–6. doi: 10.2147/DMSO.S275898
20. Álvarez-Castro P, Sangiao-Alvarellos S, Brandón-Sandá I, Cordido F. Función endocrina en la obesidad [Endocrine function in obesity. Endocrinología y Nutrición. (2011) 58:422–32. doi: 10.1016/j.endonu.2011.05.015
21. Tsai S-Y, Hsu J-Y, Lin C-H, Kuo Y-C, Chen C-H, Chen H-Y, et al. Association of stress hormones and the risk of cardiovascular diseases: systematic review and meta-analysis. Int J Cardiol Cardiovasc Risk Prev. (2024) 23:200305. doi: 10.1016/j.ijcard.2024.200305
22. Weber C, Fangauf SV, Michal M, Ronel J, Herrmann-Lingen C, Ladwig K-H, et al. Cortisol awakening reaction and anxiety in depressed coronary artery disease patients. J Clin Med. (2022) 11:374. doi: 10.3390/jcm11020374
23. Celano CM, Daunis DJ, Lokko HN, Campbell KA, Huffman JC. Anxiety disorders and cardiovascular disease. Curr Psychiatry Rep. (2016) 18:101. doi: 10.1007/s11920-016-0739-5
24. Reiner IC, Tibubos AN, Werner AM, Jurinovic V, Fischer JE, Beutel ME. The association of chronic anxiousness with cardiovascular disease and mortality in the community: results from the Gutenberg Health Study. Sci Rep. (2020) 10:12436. doi: 10.1038/s41598-020-69427-8
25. Merswolken M, Deter HC, Siebenhuener S, Orth-Gomér K, Weber CS. Anxiety as predictor of the cortisol awakening response in patients with coronary heart disease. Int J Behav Med. (2013) 20:461–7. doi: 10.1007/s12529-012-9233-6
26. Instituto Colombiano de Bienestar Familiar. Encuesta nacional de la situación nutricional indicadores priorizados [National survey on nutritional situation - prioritized indicators], in: ENSIN 2015 (2015). Available online at: https://www.icbf.gov.co/sites/default/files/tabla_de_indicadores_23012019_0.pdf (Accessed 5.2.24). WWW Document.
27. Fundación Colombiana de Obesidad [Colombian Obesity Foundation]. Guías Colombianas para el Manejo Científico de la Obesidad y Sobrepeso, in: Colombian guidelines for the scientific management of obesity and overweight (2019). Available online at: https://www.med-informatica.net/TERAPEUTICA-STAR/Obesidad_GuiasColombianasParaManejoCientificoObesidad_FUNCOBES.pdf (Accessed 5.2.24). WWW Document.
28. Gianotti L, Belcastro S, D’Agnano S, Tassone F. the stress axis in obesity and diabetes mellitus: an update. Endocrines. (2021) 2:334–47. doi: 10.3390/endocrines2030031
29. Ciancia S, van den Berg SAA, van den Akker ELT. The reliability of salivary cortisol compared to serum cortisol for diagnosing adrenal insufficiency with the gold standard ACTH stimulation test in children. Children. (2023) 10:1569. doi: 10.3390/children10091569
30. Kosak M, Hana V, Hill M, Simunkova K, Lacinova Z, Krsek M, et al. Reliability of serum versus salivary cortisol in ACTH test. Endocrine Abstracts. (2013) 32:P31. doi: 10.1530/endoabs.32.P31
31. James KA, Stromin JI, Steenkamp N, Combrinck MI. Understanding the relationships between physiological and psychosocial stress, cortisol, and cognition. Front Endocrinol. (2023) 14:1085950. doi: 10.3389/fendo.2023.1085950
32. Alberti KGMM, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome. Circulation. (2009) 120:1640–5. doi: 10.1161/CIRCULATIONAHA.109.192644
33. Castro IM. Propiedades psicométricas del Inventario de Ansiedad: Rasgo – Estado (IDARE) en pacientes que asisten a la clínica de control de peso Isell figura Vital de Trujillo 2015. Trujillo, Peru: Universidad César Vallejo (2016).
34. Anicama Gómez J, Pizarro Arteaga RD, Pineda López CE, Vallenas Pedemonte FA, Aguirre Morales MT, Villanueva Blas LF. Evidencias psicométricas del inventario ansiedad estado-rasgo: IDARE en universitarios de Lima en tiempos de COVID-19. Psychologia. (2021) 15:49–62. doi: 10.21500/19002386.5911
35. Maji Llinin CV, Durán Pincay YE. Determinación del cortisol y su relación con el síndrome de burnout en pacientes de 20 a 40 años de la ciudad de Ambato. Ciencia Latina Rev Científica Multidisciplinar. (2022) 6:816–33. doi: 10.37811/cl_rcm.v6i2.1925
36. O’Donovan A, Hughes BM, Slavich GM, Lynch L, Cronin MT, O’Farrelly C, et al. Clinical anxiety, cortisol and interleukin-6: Evidence for specificity in emotion–biology relationships. Brain Behav Immun. (2010) 24:1074–7. doi: 10.1016/J.BBI.2010.03.003
37. Mielimąka M, Rutkowski K, Cyranka K, Sobański J, Dembińska E, Müldner-Nieckowski Ł. Trait and state anxiety in patients treated with intensive short-term group psychotherapy for neurotic and personality disorders. Psychiatr Pol. (2017) 51:1165–79. doi: 10.12740/PP/OnlineFirst/60537
38. Mirete M, Molina S, Villada C, Hidalgo V, Salvador A. Subclinical social anxiety in healthy young adults: Cortisol and subjective anxiety in response to acute stress. Anales Psicologia. (2021) 37:432–9. doi: 10.6018/analesps.483411
39. Zheng X, Zhang K, Zhao Y, Fent K. Environmental chemicals affect circadian rhythms: an underexplored effect influencing health and fitness in animals and humans. Environ Int. (2021) 149:106159. doi: 10.1016/j.envint.2020.106159
40. Adam EK, Quinn ME, Tavernier R, McQuillan MT, Dahlke KA, Gilbert KE. Diurnal cortisol slopes and mental and physical health outcomes: A systematic review and meta-analysis. Psychoneuroendocrinology. (2017) 83:25–41. doi: 10.1016/j.psyneuen.2017.05.018
41. van Eck M, Berkhof H, Nicolson N, Sulon J. The effects of perceived stress, traits, mood states, and stressful daily events on salivary cortisol. Psychosomatic Med. (2020) 58:447–58. doi: 10.1097/00006842-199609000-00007
42. Rosnick CB, Wetherell JL, White KS, Andreescu C, Dixon D, Lenze EJ. Cognitive-behavioral therapy augmentation of SSRI reduces cortisol levels in older adults with generalized anxiety disorder: A randomized clinical trial. J Consulting Clin Psychol. (2016) 84:345–52. doi: 10.1037/a0040113
43. Romero-González B, Puertas-González JA, Strivens-Vílchez H, González-Pérez R, Peralta-Ramírez MI. Effects of cognitive-behavioural therapy for stress management on stress and hair cortisol levels in pregnant women: A randomised controlled trial. J Psychosomatic Res. (2020) 135:110162. doi: 10.1016/j.jpsychores.2020.110162
44. Redeker NS, Jeon S, Andrews L, Cline J, Mohsenin V, Jacoby D. Effects of cognitive behavioral therapy for insomnia on sleep, symptoms, stress, and autonomic function among patients with heart failure. Behav Sleep Med. (2019) 17:342–54. doi: 10.1080/15402002.2018.1546709
45. Brand S, Holsboer-Trachsler E, Naranjo JR, Schmidt S. Influence of mindfulness practice on cortisol and sleep in long-term and short-term meditators. Neuropsychobiology. (2012) 65:109–18. doi: 10.1159/000330362
46. Bränström R, Kvillemo P, Åkerstedt T. Effects of mindfulness training on levels of cortisol in cancer patients. Psychosomatics. (2013) 54:158–64. doi: 10.1016/j.psym.2012.04.007
47. Turakitwanakan W, Mekseepralard C, Busarakumtragul P. Effects of mindfulness meditation on serum cortisol of medical students. J Med Assoc Thailand. (2013) 96:S90–5.
48. Zschucke E, Renneberg B, Dimeo F, Wüstenberg T, Ströhle A. The stress-buffering effect of acute exercise: Evidence for HPA axis negative feedback. Psychoneuroendocrinology. (2015) 51:414–25. doi: 10.1016/j.psyneuen.2014.10.019
49. Hiller RM, Lovato N, Gradisar M, Oliver M, Slater A. Trying to fall asleep while catastrophizing: What sleep is like for anxious children. J Anxiety Disord. (2017) 48:51–9. doi: 10.1016/j.janxdis.2016.09.016
50. Wagner D, Pearcey SM. Perceived stress and salivary biomarkers in educators: Comparison among three stress reduction activities. Health Psychol Behav Med. (2022) 10:617–31. doi: 10.1080/21642850.2022.2102016
51. von der Embse N, Ryan SV, Gibbs T, Mankin A. Teacher stress interventions: A systematic review. Psychol Schools. (2019) 56:1328–43. doi: 10.1002/pits.22279
52. Qin DD, Rizak J, Feng XL, Yang SC, Lü LB, Pan L, et al. Prolonged secretion of cortisol as a possible mechanism underlying stress and depressive behaviour. Sci Rep. (2016) 6:30187. doi: 10.1038/srep30187
53. Xie Z, Deng Y, Xie C, Yao Y. Changes of adrenocorticotropic hormone rhythm and cortisol circadian rhythm in patients with depression complicated with anxiety and their effects on the psychological state of patients. Front Psychiatry. (2023) 13:1030811. doi: 10.3389/fpsyt.2022.1030811
54. Mohd Azmi NAS, Juliana N, Azmani S, Mohd Effendy N, Abu IF, Mohd Fahmi Teng NI, et al. Cortisol on circadian rhythm and its effect on cardiovascular system. Int J Environ Res Public Health. (2021) 18:676. doi: 10.3390/ijerph18020676
55. Thomas SJ, Larkin T. Cognitive Distortions in Relation to Plasma Cortisol and Oxytocin Levels in Major Depressive Disorder. Front Psychiatry. (2020) 10:971. doi.org/doi: 10.3389/fpsyt.2019.00971
56. Su K, Din ZU, Cui B, Peng F, Zhou Y, Wang C, et al. A broken circadian clock: the emerging neuro-immune link connecting depression to cancer. Brain Behav Immun Health. (2022) 26:100533. doi: 10.1016/j.bbih.2022.100533
57. Veen G, Giltay EJ, DeRijk RH, van Vliet IM, van Pelt J, Zitman FG. Salivary cortisol, serum lipids, and adiposity in patients with depressive and anxiety disorders. Metabolism. (2009) 58:821–7. doi: 10.1016/j.metabol.2009.02.009
58. Anni NS, Jung SJ, Shim JS, Jeon YW, Lee GB, Kim HC. Stressful life events and serum triglyceride levels: The Cardiovascular and Metabolic Diseases Etiology Research Center cohort in Korea. Epidemiol Health. (2021) 43:e2021042. doi: 10.4178/epih.e2021042
59. Pooradl M, Alipour A, Aliakbari Dehkordi M, Farrokhi M. Associations between self-reported anxiety and serum lipid, lipoprotein concentrations and platelets in healthy men. Neurol Asia. (2013) 18:87–93.
60. Park J-Y, Kim J-W, Kang H-J, Choi W, Lee J-Y, Kim S-W, et al. Effect modification of cortisol on the associations between obsessive-compulsive symptoms on suicidality in patients with acute coronary syndrome. Psychiatry Investig. (2023) 20:707–13. doi: 10.30773/pi.2023.0085
61. Syros I, Pervanidou P, liapi C, Apostolakou F, Chrousos GP, Kolaitis G. Increased diurnal salivary cortisol and morning serum triglycerides and decreased apo A1 concentrations in children and adolescents with clinical depression. OBM Neurobiol. (2020) 4:1–24. doi: 10.21926/obm.neurobiol.2002060
62. Barbosa C, da S, das Merces MC, Costa Santana AI, de Souza e Silva D, Pimentel RFW, et al. Anxiety and dyslipidemia among primary health care professionals: A Cross-sectional study. Work. (2022) 71:739–48. doi: 10.3233/WOR-205095
63. Cheon SY. Impaired cholesterol metabolism, neurons, and neuropsychiatric disorders. Exp Neurobiol. (2023) 32:57–67. doi: 10.5607/en23010
64. Dyson T, Thomas SJ, Townsend ML, Finch A, South A, Barkus E, et al. Salivary testosterone and cortisol levels in borderline personality disorder before and after a 12-week group dialectical behavior therapy intervention. Front Psychol. (2023) 14:1195187. doi: 10.3389/fpsyg.2023.1195187
65. Manigault AW, Shorey RC, Appelmann H, Hamilton KR, Scanlin MC, Juster R-P, et al. Gender roles are related to cortisol habituation to repeated social evaluative stressors in adults: secondary analyses from a randomized controlled trial. Stress. (2021) 24:723–33. doi: 10.1080/10253890.2021.1892069
66. Ju Y, Wang M, Lu X, Sun J, Dong Q, Zhang L, et al. The effects of childhood trauma on the onset, severity and improvement of depression: The role of dysfunctional attitudes and cortisol levels. J Affect Disord. (2020) 276:402–10. doi: 10.1016/j.jad.2020.07.023
67. Sun J, Jiang Y, Zilioli S, Xie M, Chen L, Lin D. Psychological and physical abuse and cortisol response to stress: the moderating role of psychosocial resources. J Youth Adolesc. (2023) 52:91–104. doi: 10.1007/s10964-022-01699-x
68. Panagou C, MacBeth A. Deconstructing pathways to resilience: a systematic review of associations between psychosocial mechanisms and transdiagnostic adult mental health outcomes in the context of adverse childhood experiences. Clin Psychol Psychother. (2022) 29:1626–54. doi: 10.1002/cpp.2732
69. Bilal H, Tian Y, Ali A, Muhammad Y, Yahya A, Izneid BA, et al. An intelligent approach for early and accurate prediction of cardiac disease using hybrid artificial intelligence techniques. Bioengineering. (2024) 11:1290. doi: 10.3390/bioengineering11121290
70. Ansari MM, Kumar S, Bin Heyat MB, Ullah H, Bin Hayat MA, Parveen S, et al. SVMVGGNet-16: A novel machine and deep learning-based approach for lung cancer detection using combined SVM and VGGNet-16. Curr Med Imaging. (2025) 21:e15734056348824. doi: 10.2174/0115734056348824241224100809
Keywords: anxiety state, anxiety trait, cardiovascular risk, cortisol, circadian rhythm
Citation: Alayón AN, Ochoa Arizal N, Noreña Correa M, López Toro J and Hernández Rojas F (2025) Cortisol, cardiovascular risk, and anxiety in full-time workers in Cartagena, Colombia, 2023. Front. Psychiatry 16:1491987. doi: 10.3389/fpsyt.2025.1491987
Received: 11 September 2024; Accepted: 19 March 2025;
Published: 10 April 2025.
Edited by:
Julia M. Stephen, Mind Research Network (MRN), United StatesReviewed by:
Francesco Perrotta, Magna Græcia University, ItalyAhmad Ali, Shanghai Jiao Tong University, China
Copyright © 2025 Alayón, Ochoa Arizal, Noreña Correa, López Toro and Hernández Rojas. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manuel Noreña Correa, bWFudWVsLm5vcmVuYUB1c2JjdGcuZWR1LmNv