 Katrin Schroeder
Katrin Schroeder Anja Schätzle1
Anja Schätzle1 Ingo Schäfer
Ingo Schäfer Christian G. Huber
Christian G. Huber- 1Department of Psychiatry and Psychotherapy, University Medical Center Hamburg-Eppendorf, Hamburg, Germany
- 2Universitäre Psychiatrische Kliniken Basel, University of Basel, Basel, Switzerland
Introduction: Auditory verbal hallucinations (AVH), a disturbance of auditory perception, and delusions, a content-related thought disorder, are common in borderline personality disorder (BPD). However, they are not as thoroughly studied and clinically acknowledged as other symptoms. Associations between childhood trauma, dissociative symptoms, and AVH—as well as delusions—have been reported in schizophrenia but remain understudied in BPD.
Methods: We calculated Pearson’s correlations and tested the mediating effects of dissociative symptoms, assessed with the Dissociative Experiences Scale (DES), on the association between childhood trauma, assessed with the Childhood Trauma Questionnaire (CTQ), and both AVH and delusions. A total of 74 BPD patients were examined using the Psychotic Symptoms Rating Scale (PSYRATS) interview. For the mediation analyses, Preacher and Hayes’ SPSS bootstrap macro was used to estimate the significance of the mediator.
Results: AVH were reported by 10 patients (13.5%) and delusional thoughts by eight patients (10.8%). In the mediator analyses, dissociative experiences significantly mediated the association between childhood trauma and auditory verbal hallucinations, with an unstandardized regression coefficient between CTQ-Total and DES-Total of b = 10.0083; p = 0.0008 and between DES-Total and PSYRATS-AVH of b = 0.0102; p = 0.0009. The relationship between CTQ-Total and the PSYRATS-Delusions Scale was not significantly mediated by DES-Total.
Discussion: The results of the mediation analyses are similar to those shown in schizophrenia, suggesting that the examined symptoms in BPD may underlie similar mechanisms. Further research should examine the benefit of the therapeutic approaches for each of the trauma-associated symptom clusters.
Introduction
Auditory verbal hallucinations (AVH) are defined as the perception of spoken words without an external stimulus in a fully conscious state (1). They are a core symptom of schizophrenia but can also occur in various other psychiatric illnesses, e.g., such as bipolar disorder, major depressive disorder, substance use disorders, dissociative disorders, and dementia (2–4). Delusions are a content-related thought disorder where reality testing is impaired. They are defined as having “a false firm conviction […] whose truth is immediately evident to the person and requires no justification […, while the] environment does not share the belief and in the cultural context, the opinion is considered false” (5). Delusions are often considered prototypical psychotic phenomena and can occur in a range of mental illnesses, such as schizophrenia spectrum disorders, affective disorders, substance use disorders, and dementia, but are not typically observed in dissociative disorders (5). Both AVH and delusions are common symptoms in borderline personality disorders (BPD). Approximately 30% of BPD patients experience delusions, and about 50% experience hallucinations (6). However, most studies were conducted in small samples (7) or focused only on AVH (8). AVH in BPD has been found to burden affected patients to a degree comparable to that experienced by patients with schizophrenia (8–10). Additionally, it was found that the phenomenology of the AVH in BPD—e.g., conviction, frequency, or beliefs about the location of the auditory hallucination (8, 9, 11–13), or whether it was a known or unknown person (14)—was comparable to AVH in schizophrenia.
While both the Diagnostic and Statistical Manual of Mental Disorders, Fourth and Fifth Edition (DSM-IV and DSM-5) criteria (15, 16) describe AVH and delusions as transient in BPD, studies exploring the duration of these symptoms show different results (8, 10–13, 17–21). The symptoms examined lasted at least several weeks (18) and up to 18 years (8). Although the burden caused by these symptoms in BPD patients has been examined only with regard to AVH so far, it is clear that these experiences have a significant impact (8, 9, 11, 21, 22). For instance, they have been shown to be associated with suicidal behavior, a key problem in the treatment of borderline patients (10, 23–25).
Another cluster of symptoms commonly found in BPD is dissociative symptoms [e.g., (10, 26–30)]. Associations have been found between these symptoms and childhood sexual abuse (31–33), as well as other forms of childhood maltreatment (30, 34, 35). Dissociation is considered an important element for understanding the relationship between trauma and hallucinations, as well as delusions. However, the relationship between trauma, dissociation, and these symptoms has primarily been studied in schizophrenia: the interrelation of the clinical characteristics, dissociation, and childhood trauma has been the subject of several investigations in schizophrenia [e.g., (24, 36, 37)]. It has been discussed that severe dissociation may produce hallucinations or delusions, or could be a mediating factor in their development [e.g., (38)]. Allen et al. (39) emphasized the special role of dissociative detachment in this context. They suggested that dissociative detachment “undermines the individual’s grounding in the outer world, thereby hampering reality-testing and rendering the individual with posttraumatic symptoms vulnerable to the nightmarish inner world” [(39), p. 332)]. Empirical evidence for the relationship between dissociation and hallucinations/delusions comes, for instance, from a study by Perona-Garcelan and colleagues (40). In a mediation analysis, these authors found that dissociative symptoms were a mediator between childhood trauma and hallucinations, but not between childhood trauma and delusions, in a sample of patients with schizophrenia.
Although AVH, delusions, and dissociative symptoms are also prevalent in BPD, and although the majority of BPD patients have suffered some kind of childhood maltreatment (41–44), no studies exist, to our knowledge, that have examined potential associations between these factors in BPD. The aim of our study, therefore, was to examine whether dissociative symptoms have a mediating effect between childhood maltreatment and the development of AVH and delusions, respectively, in patients with BPD. We hypothesized that, given the similarities between AVH in schizophrenia and BPD, the associations between childhood maltreatment and the occurrence of dissociative and psychotic symptoms would be comparable to those in schizophrenia [e.g., (8, 9, 14)].
Methods
Participants
All participants were inpatients of a specialized ward for personality disorders at the University Medical Center Hamburg-Eppendorf, Germany. Inclusion criteria were a diagnosis of BPD according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) (16), age between 18 and 65 years, and sufficient German language abilities. Exclusion criteria were organic mental disorders, acute intoxication, withdrawal syndrome, dementia, acute suicidality, and schizophrenia spectrum disorders. The final sample consisted of n = 74 patients.
All subjects provided written informed consent. The study was approved by the responsible ethics committee (State Chamber of Physicians, Hamburg, Germany).
Procedures and assessments
The diagnosis of BPD according to the DSM-IV-TR (16) was confirmed using the German version of the Structured Clinical Interview for DSM-IV Axis I Disorders [SCID-l; (45)]. It comprises a screening questionnaire and a structured interview. The criteria are encoded as “1” (not met), “2” (partially met), or “3” (met). To diagnose a personality disorder, a minimum number of criteria must be met.
All patients were screened for comorbid schizophrenia spectrum disorders using the German version of Sections B and C of the SCID-I (45), a structured interview for Axis I disorders. Those who fulfilled the criteria for a schizophrenia spectrum disorder were excluded from the sample.
Psychotic symptoms were assessed using the Psychotic Symptom Rating Scales (PSYRATS). The PSYRATS is a semistructured interview consisting of 17 items, which are assigned to two subscales assessing AVH and delusion. AVH is evaluated with 11 items, and delusional beliefs with six items. Each item is evaluated on a 5-point scale. The PSYRATS has been evaluated as “a reliable and valid assessment tool for delusions and hallucinations” (46).
Dissociative symptoms were measured with the German version of the Dissociative Experiences Scale [DES; (47)]. This reliable and internally consistent self-report questionnaire is the most widely used instrument for dissociative symptoms in clinical samples. It contains items referring to amnesia, depersonalization, derealization, absorption, and identity alteration and comprises three subscales (absorption, depersonalization, and amnesia). The German version of the DES yields good to excellent statistical parameters, similar to the original version (48).
For assessing the type and severity of childhood trauma, the Childhood Trauma Questionnaire [CTQ; (49)] was used. This self-report questionnaire comprised 28 items assessing physical, sexual, and emotional abuse, as well as physical and emotional neglect. The items are rated on a 5-point scale (1 = never true to 5 = very often true). Strong psychometric properties have been demonstrated for the CTQ in both clinical and community samples (50). We categorized the CTQ scores for each subscale as proposed by the authors [“none or low”, “low to moderate”, “moderate to severe”, “severe to extreme”; (49)].
Data analysis
Descriptive statistics are given in total numbers and percentages for nominal scaled variables, and in mean/median and standard deviation (SD) for ordinal and interval-scaled variables. In addition, SEM is reported where relevant.
In a first step, we examined correlations between childhood trauma, dissociation, AVH, and delusions using Pearson’s r. Effect sizes were defined as small (r < 0.3), medium (r = 0.3–0.5), and large (r ≥ 0.5), according to Cohen (51).
To test our main hypotheses, we used a mediation analysis. In the simple mediation model, the total DES score was the mediating variable, and childhood trauma was the independent variable. We used Hayes’s (52) SPSS bootstrap macro to estimate mediator significance with a 95% confidence interval (CI) and 10,000 bootstrap samples. According to the authors, if the 95% CI does not include zero, the effect is significant at p < 0.05. The Sobel test was used to calculate the significance of the indirect effect.
Results
Sample description
The final sample (n = 74) consists of 66 women (89.2%) and eight men (10.8%). The average age of the sample was 27.9 years (range: 18–46 years). The majority of study participants were unmarried (n = 62; 83.8%), and n = 24 (32.4%) were in permanent employment.
Auditory verbal hallucinations and delusions
Delusional thoughts, as assessed by the delusions subscale of the PSYRATS, were reported by eight patients (10.8%), and AVH, as assessed by the AVH subscale of the PSYRATS, by 10 (13.5%). The mean score for the delusions subscale was M = 1.7 (SD = 5.1) in the total sample and M = 15.8 (SD = 4.8) in the affected subgroup. Means for AVH were M = 2.9 (SD = 8.0) in the total sample and M = 21.6 (SD = 8.7) in the affected subgroup.
Childhood trauma
The CTQ showed a mean value of M = 60.4 (SD = 23.5). A total of N = 59 participants completed the CTQ. The frequency of the different forms of childhood abuse is specified in Table 1.
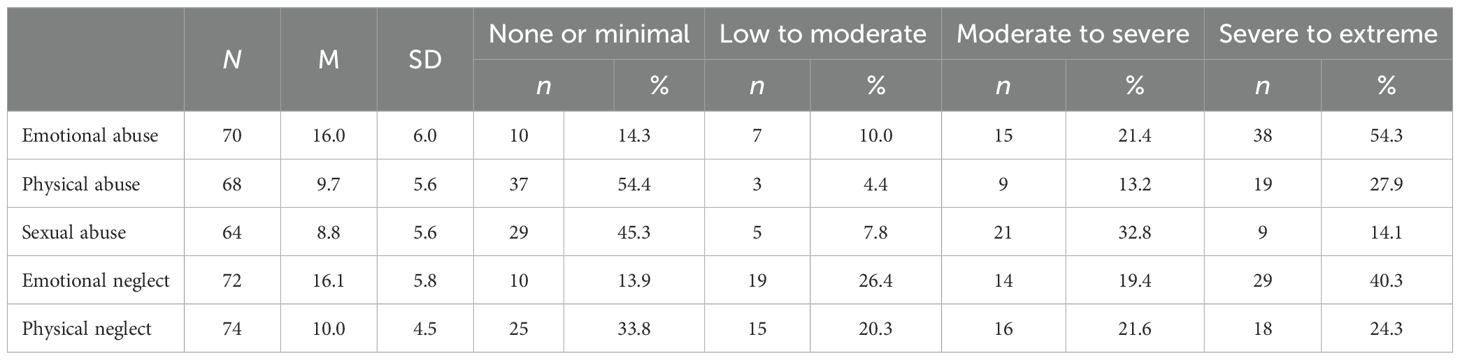
Table 1. Frequency of different forms of childhood abuse assessed with the CTQ.
Dissociative symptoms
The mean score of the DES was M = 23.9 (n = 71). The mean scores of the different subscales of the DES are shown in Table 2.

Table 2. Means of DES.
Associations between childhood trauma, dissociative symptoms, AVH, and delusions
To assess associations between childhood trauma, dissociative symptoms, AVH, and delusions, we calculated Pearson’s correlations between the different types of childhood trauma, the PSYRATS Delusional Thoughts Scale, the PSYRATS-AVH Scale, and the total score of the DES, as well as its subscales (see Table 3).

Table 3. Pearson’s correlations for CTQ-Total and its subscales and PSYRATS-AVH Scale, PSYRATS-Delusions Scale, and DES-Total and its subscales.
Regarding the PSYRATS scales, there was only one significant correlation. PSYRATS-AVH was positively associated with the CTQ scale sexual abuse (r = 0.453; p < 0.001).
Between the DES scores and the CTQ scores, nearly all correlations were significant, with the only exception being the lack of a significant correlation between physical abuse and depersonalization (see Table 3).
For the correlations between the PSYRATS scales and the DES scales, we found significant positive correlations between dissociations and hallucinations, ranging from r = 0.485 and 0.569 (all p < 0.001) for the DES subscales, and r = 0.544 (p < 0.001) for the DES-Total Scale (see also Table 4). The PSYRATS-Delusions Scale, on the other hand, showed weaker and, in some cases, nonsignificant associations with the DES-Total Scale (r = 0.259; p = 0.029) and its subscales (r = 0.218; p = 0.015 to r = 0.286; p = 0.065).
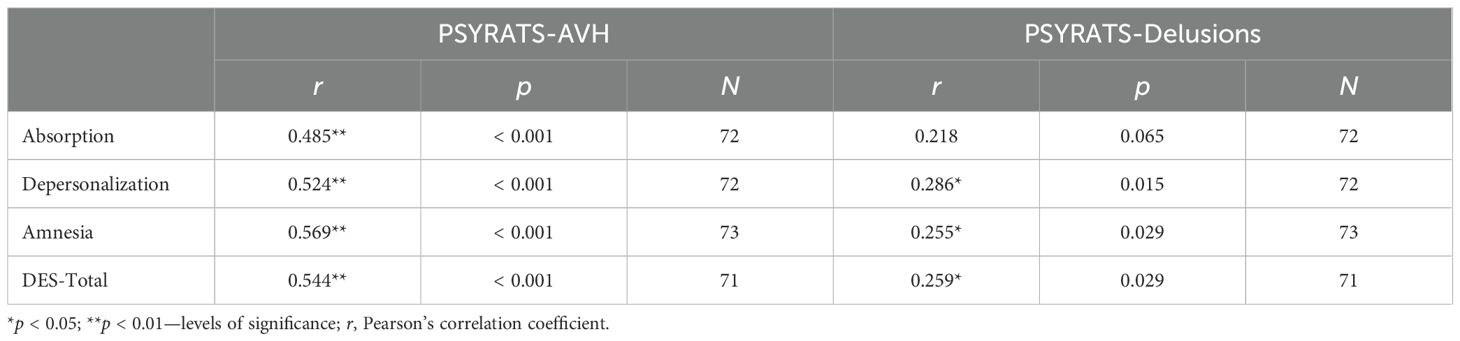
Table 4. Pearson’s correlations for the PSYRATS-AVH Scale, PSYRATS-Delusions Scale, and DES-Total and its subscales.
Mediation analyses
To test whether dissociative symptoms, as measured with the DES, have a mediating effect between childhood maltreatment assessed with the CTQ and AVH or delusional thoughts, we conducted a mediation analysis. Our analysis showed that the DES total score significantly mediated the relationship between the CTQ total score and the PSYRATS-AVH Scale. As Figure 1 illustrates, the unstandardized regression coefficient between the CTQ total score and the DES total score was statistically significant (path a: b = 10.0083; p = 0.0008; 95% CI: 4.3429, 15.6738), as was the unstandardized regression coefficient between the DES total score and the PSYRATS-AVH Scale (path b: b = 0.0102; p = 0.0009; 95% CI: 0.0044, 0.0161); see Figure 1).
![Diagram illustrating a mediation model with three variables: CTQ-total, DES-total, and PSYRATS AVH. Arrows indicate paths: Path a (CTQ-total to DES-total) with b = 10.0083, p = .0008, CI = [4.3429, 15.6738]; Path b (DES-total to PSYRATS AVH) with b = .0102, p = .0009, CI = [.0044, .0161]; Path c (CTQ-total to PSYRATS AVH) indirect effect with b = .1022, p = .0148, CI = [.0308, .2093], and direct effect Path c' with b = -.0155, p = .7606, CI = [-.1168, .0858].](https://www.frontiersin.org/files/Articles/1532234/fpsyt-16-1532234-HTML-r1/image_m/fpsyt-16-1532234-g001.jpg)
Figure 1. Simple mediation model with AVH as the dependent variable. N = 58. DES, Dissociative Experiences Scale; CTQ-Total, Childhood Trauma Questionnaire Total Score; AVH, PSYRATS-AVH Score; CI, confidence interval. The data are specified as nonstandardized B coefficients (b) and are based on 10,000 bootstrapped iterations.
The DES total score did not significantly mediate the relationship between the CTQ total score and the PSYRATS-Delusions Scale. As Figure 2 illustrates, the unstandardized regression coefficient between the CTQ total score and the DES total score was statistically significant (path a: b = 10.0003; p = 0.0008; 95% CI: 4.3429, 15.6738), but the unstandardized regression coefficient between the DES total score and the PSYRATS Delusional Thoughts Scale was not (path b: b = 0.0035; p = 0.1735; 95% CI: −0.0016, 0.0087).
![Diagram illustrating a mediation model with three variables: CTQ-total, DES-total, and PSYRATS delusional thoughts. Path a (CTQ-total to DES total) with b = 10.0083, p = 0.0008, 95% CI = [4.3429, 15.6738]. Path b (DES total to PSYRATS delusional thoughts) with b = 0.0036, p = 0.1735, 95% CI = [-0.0016, 0.0087]. Path c (CTQ-total to PSYRATS delusional thoughts) indirect effect with b = 0.0356, p = 0.2140, 95% CI = [-0.0096, 0.0895], and direct effect Path c' with b = -0.0435, p = 0.1301, 95% CI = [-0.1002, 0.0132].](https://www.frontiersin.org/files/Articles/1532234/fpsyt-16-1532234-HTML-r1/image_m/fpsyt-16-1532234-g002.jpg)
Figure 2. Simple mediation model with delusions as the dependent variable. N = 58. DES-Total, Dissociative Experiences Scale Total Score; CTQ-total, Childhood Trauma Questionnaire Total Score; PSYRATS Delusional Thoughts, PSYRATS Delusional Thoughts Score; CI, confidence interval. The data are specified as nonstandardized B coefficients (b) and are based on 10,000 bootstrapped iterations.
Discussion
The prevalence of delusional thoughts (10.8%) and AVH (13.5%) in our sample was lower than in previous studies of psychotic experiences in patients with BPS. Data on the frequency varied between 20% and 50% in previous studies (6). This could be explained by the recruiting procedures. Patients were recruited from a specialized ward with a standardized therapeutic approach, for which a certain level of global functioning is required. The dissociative symptomatology in our sample was, on average, of moderate severity, which is comparable to other data on the severity of dissociative symptoms in patients with BPD. For example, Zanarini et al. (53) reported that 42.0% of patients with BPD had dissociation levels of moderate severity. A total of 26.2% of patients were affected by severe dissociative symptoms, and 31.7% reported mild dissociative symptoms. The severity of childhood trauma reported by our patients (M = 60.4, SD = 23.5) is comparable to another German study (M = 63.0, SD = 21.0) by Wingenfeld and colleagues (54) and markedly higher than in a representative sample from the German population, where a CTQ total score of 35.97 is computable from the reported data (55). However, higher CTQ scores have also been reported in the literature; e.g., Kratzer et al. (56) found a mean CTQ of 78.8 in their population of BPD patients.
The relationship between childhood maltreatment and AVH, as assessed by the PSYRATS, was significantly mediated by dissociative symptoms, as measured with the DES. Dissociative symptoms, in contrast, did not significantly mediate the relationship between childhood maltreatment or violence and delusions assessed with the PSYRATS. This is in line with findings in schizophrenia, where dissociative symptoms mediated the relationship between childhood trauma and hallucinations or hallucination-proneness (40, 57, 58), but not between childhood trauma and delusions (40). These associations, however, were not replicated in a sample of first-episode psychosis patients. Contrary to previous findings, neither a significant relationship between dissociation and hallucinations nor a mediating effect of dissociation on the association between childhood trauma and hallucinations was found. Instead, in this study, dissociation mediated the relationship between childhood trauma and delusions (59). In healthy individuals, dissociation mediated the relationship between early maltreatment and both hallucination-proneness and delusional ideation (60).
Summing up our results and these studies, this might be another indication that the associations between psychotic symptoms and dissociation are not disorder-specific, but typical for early-traumatized individuals with hallucinations, delusions, and dissociative symptoms. This is another aspect that questions the strict differentiation between AVH and delusions in schizophrenia spectrum disorders on the one hand, and in borderline personality disorder on the other hand.
The current paper is strictly focused on the psychopathological symptom level, i.e., on dissociation, AVH, and delusions. These symptoms are not specific to a diagnosis and can occur in patients with different mental health problems. In particular, they can occur in borderline personality disorder and in patients with schizophrenia spectrum disorders. This is an important point, because at the disorder-specific level, an intensive discussion is still ongoing. For example, there is an ongoing discussion about dissociative symptoms in schizophrenia spectrum disorders (61), raising the question of whether dissociation could also be considered a symptom of comorbid dissociative disorder or borderline personality disorder, rather than an additional symptom in schizophrenia spectrum disorders, increased through adverse childhood events. In addition, there is evidence for a relevant level of comorbid dissociative disorders in patients with BPD (62). This raises the question of whether examining BPD in this population is, in fact, examining comorbidity with dissociative disorders. Furthermore, Sar et al. showed a considerable descriptive overlap between dissociative disorders and BPD (62–66). Following this line of thought, Meares (67) discussed the possibility that BPD itself might be a dissociative disorder. There are efforts to move beyond these discussions by referring to the Research Domain Criteria (RDoC) and the Hierarchical Taxonomy of Psychopathology [HiTOP; (68–70)]. Our work is in line with these concepts and remains at the symptom level. Based on the literature, it is assumed that there may be common pathways (57, 71, 72) leading from predisposing factors (in our case, adverse childhood events) to symptoms such as dissociation, AVH, and delusions. Describing this situation in borderline personality disorder was the objective of the current paper. These pathways could be the same for different diagnosis groups in which the symptoms occur, e.g., borderline personality disorder and schizophrenia spectrum disorders. However, different pathways might be responsible for disturbed perception in AVH and content-related thought disorder with impaired reality testing in delusions, which are, e.g., not typically seen in the context of dissociative disorders. This might explain why there was a significant mediating effect of dissociation on AVH, but not on delusions.
While the strengths of our study include the use of structured interviews for the assessment of hallucinations, delusions, and the verification of BPD, some limitations should be considered. Although only a few exclusion criteria were applied, an important limitation may relate to the representativeness of our sample. As all participants were inpatients on a specialized therapy unit, prevalence rates may not be generalizable to other BPD populations. Moreover, many patients (n = 30, 40.5%) received antipsychotic medication, which may also explain the lower frequency of psychotic symptoms in our sample. Both aspects might limit our conclusions. In addition, the PSYRATS used in the current study have, until now, only been validated for research in schizophrenia spectrum disorders and in affective disorders with delusions (46). However, it has been repeatedly used in studies with other patient populations, particularly borderline personality disorder (25, 73). Moreover, while we established structured diagnostics for BPD and for the absence of schizophrenia spectrum disorders, we did not specifically assess a potential comorbidity with dissociative disorders.
In many aspects, the phenomenology of the AVH in BPD is comparable to AVH in schizophrenia (8, 9, 11–14, 74), and our results add another facet similar to symptoms in schizophrenia. These symptoms should, therefore, receive the same level of attention and should not be trivialized. Trivialization may occur through the use of terms such as pseudo-hallucinations or transient paranoid ideas—terms which should no longer be used (8, 17, 75, 76). Continued use of such terms may also invalidate the patient’s experience of what are often frightening symptoms.
In contrast, hallucinations were associated with childhood trauma through mediation by dissociation and are, therefore, rather a sign of a high burden. This should raise awareness of a positive history of trauma. Treatment of traumatized patients should be trauma-sensitive, which involves siding with patients and taking them and their experiences seriously. The supportive stance should extend to their symptoms as well and should not stop when it comes to acknowledging them. For example, symptoms such as AVH should not be dismissed as pseudo-hallucinations, nor should AVH or delusions be ignored by failing to inquire about them. In schizophrenia-spectrum disorders, trauma-focused psychotherapy has been shown to reduce not only Post-traumatic stress disorder (PTSD) symptoms but also positive symptoms such as hallucinations or delusions (77). Perhaps this also applies to psychotic symptoms in BPD, and therefore innovative therapeutic approaches that are tailored to traumatized BPD patients [e.g., DBT-PTSD; (78)] might represent a promising path. This would align with the theoretical considerations of Morrison et al. (79), who proposed that both posttraumatic stress disorder and psychotic disorders fall within a spectrum of responses to traumatic life events. This spectrum is not always clearly delineated and is characterized by overlapping symptoms (intrusions, flashback experiences, hallucinations, delusions). Further research should address trauma-associated symptoms and evaluate the benefits of therapeutic approaches for each of the symptom clusters.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by State Chamber of Physicians, Hamburg, Germany. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KS: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft. AS: Data curation, Investigation, Project administration, Writing – review & editing. IS: Resources, Supervision, Validation, Writing – review & editing. CH: Conceptualization, Formal analysis, Methodology, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We primarily thank the participating patients for their time and effort. We also thank Oliver Kofler and Janina Billian for their assistance with the literature research and proofreading. Portions of this work were conducted by Pauline Kowohl and Lisa Leske as part of their MD theses.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. De Leede-Smith S and Barkus E. A comprehensive review of auditory verbal hallucinations: lifetime prevalence, correlates and mechanisms in healthy and clinical individuals. Front Hum Neurosci. (2013) 7:367. doi: 10.3389/fnhum.2013.00367
2. Toh WL, Thomas N, and Rossell SL. Auditory verbal hallucinations in bipolar disorder (BD) and major depressive disorder (MDD): a systematic review. J Affect Disord. (2015) 184:18–28. doi: 10.1016/j.jad.2015.05.040
3. Zhuo C, Jiang D, Liu C, Lin X, Li J, Chen G, et al. Understanding auditory verbal hallucinations in healthy individuals and individuals with psychiatric disorders. Psychiatry Res. (2019) 274:213–9. doi: 10.1016/j.psychres.2019.02.040
4. Larøi F, Sommer IE, Blom JD, Fernyhough C, ffytche DH, Hugdahl K, et al. The characteristic features of auditory verbal hallucinations in clinical and nonclinical groups: state-of-the-art overview and future directions. Schizophr Bull. (2012) 38:724–33. doi: 10.1093/schbul/sbs061
5. Reischies FM. Delusion—Content-related thought disorders. In: Reischies FM, editor. Psychopathology: Characteristics of Mental Disorders and Clinical Neuroscience. Springer, Berlin, Heidelberg (2025). p. 335–60.
6. Schroeder K, Fisher HL, and Schäfer I. Psychotic symptoms in patients with borderline personality disorder: prevalence and clinical management. Curr Opin Psychiatry. (2013) 26:113–9. doi: 10.1097/YCO.0b013e32835a2ae7
7. Chopra HD and Beatson JA. Psychotic symptoms in borderline personality disorder. Am J Psychiatry. (1986) 143:1605–7. doi: 10.1176/ajp.143.12.1605
8. Slotema CW, Daalman K, Blom JD, Diederen KM, Hoek HW, and Sommer IEC. Auditory verbal hallucinations in patients with borderline personality disorder are similar to those in schizophrenia. Psychol Med. (2012) 42:1873–8. doi: 10.1017/S0033291712000165
9. Kingdon DG, Ashcroft K, Bhandari B, Gleeson S, Warikoo N, Symons M, et al. Schizophrenia and borderline personality disorder: similarities and differences in the experience of auditory hallucinations, paranoia, and childhood trauma. J Nerv Ment Dis. (2010) 198:399–403. doi: 10.1097/NMD.0b013e3181e08c27
10. Slotema CW, Blom JD, Niemantsverdriet MBA, and Sommer IEC. Auditory verbal hallucinations in borderline personality disorder and the efficacy of antipsychotics: a systematic review. Front Psychiatry. (2018) 9:347. doi: 10.3389/fpsyt.2018.00347
11. Barrera A, Bajorek T, Dekker R, Hothi G, Lewis A, and Pearce S. A phenomenological exploration of the voices reported by borderline personality and schizophrenia patients. Psychopathology. (2021) 54:159–68. doi: 10.1159/000516208
12. Cavelti M, Thompson KN, Hulbert C, Betts J, Jackson H, Francey S, et al. Exploratory comparison of auditory verbal hallucinations and other psychotic symptoms among youth with borderline personality disorder or schizophrenia spectrum disorder. Early Interv Psychiatry. (2019) 13:1252–62. doi: 10.1111/eip.12763
13. Tseng ST and Georgiades A. A phenomenological comparison of auditory hallucinations between borderline personality disorder and schizophrenia: a systematic review. Clin Psychol Psychother. (2024) 31:e2958. doi: 10.1002/cpp.2958
14. Tschöke S, Steinert T, Flammer E, and Uhlmann C. Similarities and differences in borderline personality disorder and schizophrenia with voice hearing. J Nerv Ment Dis. (2014) 202:544–9. doi: 10.1097/NMD.0000000000000159
15. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 5th ed.: DSM-5. Arlington, VA: American Psychiatric Publishing (2013).
16. American Psychiatric Association. Diagnostic and statistical manual of mental disorders, 4th ed., text rev.: DSM-IV-TR. Washington, DC: American Psychiatric Publishing (2000).
17. Adams B and Sanders T. Experiences of psychosis in borderline personality disorder: a qualitative analysis. J Ment Health. (2011) 20:381–91. doi: 10.3109/09638237.2011.577846
18. Miller FT, Abrams T, Dulit R, and Fyer M. Psychotic symptoms in patients with borderline personality disorder and concurrent axis I disorder. Psychiatr Serv. (1993) 44:59–61. doi: 10.1176/ps.44.1.59
19. Pearse LJ, Dibben C, Ziauddeen H, Denman C, and McKenna PJ. A study of psychotic symptoms in borderline personality disorder. J Nerv Ment Dis. (2014) 202:368–71. doi: 10.1097/NMD.0000000000000132
20. Suzuki H, Tsukamoto C, Nakano Y, Aoki S, and Kuroda S. Delusions and hallucinations in patients with borderline personality disorder. Psychiatry Clin Neurosci. (1998) 52:605–10. doi: 10.1046/j.1440-1819.1998.00463.x
21. Yee L, Korner AJ, McSwiggan S, Meares RA, and Stevenson J. Persistent hallucinosis in borderline personality disorder. Compr Psychiatry. (2005) 46:147–54. doi: 10.1016/j.comppsych.2004.07.032
22. Hayward M, Jones AM, Strawson WH, Quadt L, Larsson DEO, Silva M, et al. A cross-sectional study of auditory verbal hallucinations experienced by people with a diagnosis of borderline personality disorder. Clin Psychol Psychother. (2022) 29:631–41. doi: 10.1002/cpp.2655
23. Cavelti M, Thompson K, Chanen AM, and Kaess M. Psychotic symptoms in borderline personality disorder: developmental aspects. Curr Opin Psychol. (2021) 37:26–31. doi: 10.1016/j.copsyc.2020.07.003
24. Schroeder K, Schätzle A, Kowohl P, Leske L, Huber C, and Schäfer I. Prävalenz und Phänomenologie fraglich psychotischer Symptome bei Borderline-Persönlichkeitsstörungen: Assoziationen mit Suizidversuchen und Inanspruchnahme stationär-psychiatrischer Behandlung. Psychother Psychosom Med Psychol. (2018) 68:516–24. doi: 10.1055/s-0043-124473
25. Slotema CW, Niemantsverdriet MBA, Blom JD, van der Gaag M, Hoek HW, and Sommer IEC. Suicidality and hospitalisation in patients with borderline personality disorder who experience auditory verbal hallucinations. Eur Psychiatry. (2017) 41:47–52. doi: 10.1016/j.eurpsy.2016.10.003
26. Al-Shamali HF, Winkler O, Talarico F, Greenshaw AJ, Forner C, Zhang Y, et al. A systematic scoping review of dissociation in borderline personality disorder and implications for research and clinical practice: exploring the fog. Aust N Z J Psychiatry. (2022) 56:1252–64. doi: 10.1177/00048674221077029
27. Carlson EB and Putnam FW. An update on the dissociative experiences scale. Dissociation. (1993) 6:16–27.
28. Lyssenko L, Schmahl C, Bockhacker L, Vonderlin R, Bohus M, and Kleindienst N. Dissociation in psychiatric disorders: a meta-analysis of studies using the Dissociative Experiences Scale. Am J Psychiatry. (2018) 175:37–46. doi: 10.1176/appi.ajp.2017.17010025
29. Ross CA. Borderline personality disorder and dissociation. J Trauma Dissociation. (2007) 8:71–80. doi: 10.1300/J229v08n01_05
30. Zanarini MC, Ruser T, Frankenburg FR, and Hennen J. The dissociative experiences of borderline patients. Compr Psychiatry. (2000) 41:223–7. doi: 10.1016/S0010-440X(00)90051-8
31. Shearer SL. Dissociative phenomena in women with borderline personality disorder. Am J Psychiatry. (1994) 151:1324–8. doi: 10.1176/ajp.151.9.1324
32. Tschöke S, Bichescu-Burian D, Steinert T, and Flammer E. History of childhood trauma and association with borderline and dissociative features. J Nerv Ment Dis. (2021) 209:137–43. doi: 10.1097/NMD.0000000000001270
33. Zweig-Frank H, Paris J, and Guzder J. Dissociation in female patients with borderline and non-borderline personality disorders. J Pers Disord. (1994) 8:203–9. doi: 10.1521/pedi.1994.8.3.203
34. Schulze A, Hughes N, Lis S, and Krause-Utz A. Dissociative experiences, borderline personality disorder features, and childhood trauma: generating hypotheses from data-driven network analysis in an international sample. J Trauma Dissociation. (2024) 25:436–55. doi: 10.1080/15299732.2024.2323974
35. Simeon D, Nelson D, Elias R, Greenberg J, and Hollander E. Relationship of personality to dissociation and childhood trauma in borderline personality disorder. CNS Spectr. (2003) 8:755–62. doi: 10.1017/s109285290001912x
36. Schäfer I, Aderhold V, Freyberger HJ, Spitzer C, and Schroeder K. Dissociative symptoms in schizophrenia spectrum disorders. In: Moskowitz A, Dorahy MJ, and Schäfer I, editors. Psychosis, Trauma and Dissociation: Evolving Perspectives on Severe Psychopathology, 2nd ed, vol. . p . Wiley, Hoboken, NJ (2018). p. 179–94.
37. Scott JG, Ross CA, Dorahy MJ, Read J, and Schäfer I. Childhood trauma in psychotic and dissociative disorders. In: Moskowitz A, Dorahy MJ, and Schäfer I, editors. Psychosis, Trauma and Dissociation: Evolving Perspectives on Severe Psychopathology, 2nd ed. Wiley, Hoboken, NJ (2018). p. 141–57.
38. Steingard S and Frankel FH. Dissociation and psychotic symptoms. Am J Psychiatry. (1985) 142:953–5. doi: 10.1176/ajp.142.8.953
39. Allen JG, Coyne L, and Console DA. Dissociative detachment relates to psychotic symptoms and personality decompensation. Compr Psychiatry. (1997) 38:327–34. doi: 10.1016/S0010-440X(97)90928-7
40. Perona-Garcelan S, Carrascoso-Lopez F, Garcia-Montes J, Ductor-Recuerda MJ, Lopez Jiménez AM, Vallina-Fernandez O, et al. Dissociative experiences as mediators between childhood trauma and auditory hallucinations. J Trauma Stress. (2012) 25:323–9. doi: 10.1002/jts.21693
41. Estric C, Calati R, and Lopez-Castroman J. Adverse childhood experiences and neurocognition in borderline personality disorder: a call-to-action perspective review. Harv Rev Psychiatry. (2022) 30:248–60. doi: 10.1097/HRP.0000000000000344
42. Godbout N, Daspe MÈ, Runtz M, Cyr G, and Briere J. Childhood maltreatment, attachment, and borderline personality–related symptoms: gender-specific structural equation models. Psychol Trauma. (2019) 11:90–8. doi: 10.1037/tra0000403
43. Lewis KL and Grenyer BFS. Borderline personality or complex posttraumatic stress disorder? An update on the controversy. Harv Rev Psychiatry. (2009) 17:322–8. doi: 10.3109/10673220903271848
44. Scalabrini A, Cavicchioli M, Fossati A, and Maffei C. The extent of dissociation in borderline personality disorder: a meta-analytic review. J Trauma Dissociation. (2017) 18:522–43. doi: 10.1080/15299732.2016.1240738
45. Wittchen HU, Zaudig M, and Fydrich T. Strukturiertes klinisches Interview für DSM-IV: Handanweisung. Göttingen (Germany): Hogrefe. (1997).
46. Kronmüller KT, von Bock A, Grupe S, Büche L, Gentner NC, Rückl S, et al. Psychometric evaluation of the psychotic symptom rating scales. Compr Psychiatry. (2010) 52:102–8. doi: 10.1016/j.comppsych.2010.04.014
47. Bernstein EM and Putnam FW. Development, reliability, and validity of a dissociation scale. J Nerv Ment Dis. (1986) 174:727–35. doi: 10.1097/00005053-198612000-00004
48. Spitzer C, Freyberger HJ, Stieglitz R, Carlson EB, Kuhn G, Magdeburg N, et al. Adaptation and psychometric properties of the German version of the Dissociative Experiences Scale. J Trauma Stress. (1998) 11:799–809. doi: 10.1023/A:1024457819547
49. Bernstein DP and Fink L. Childhood Trauma Questionnaire: a retrospective self-report. San Antonio (TX: The Psychological Corporation (1998).
50. Scher CD, Stein MB, Asmundson GJG, McCreary DR, and Forde DR. The Childhood Trauma Questionnaire in a community sample: psychometric properties and normative data. J Trauma Stress. (2001) 14:843–57. doi: 10.1023/A:1013058625719
51. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale (NJ: Lawrence Erlbaum Associates (1988).
52. Hayes AF. Introduction to mediation, moderation, and conditional process analysis: a regression-based approach. New York (NY: Guilford Publications (2017).
53. Zanarini MC, Frankenburg FR, Jager-Hyman S, Reich DB, and Fitzmaurice G. The course of dissociation for patients with borderline personality disorder and axis II comparison subjects: a 10-year follow-up study. Acta Psychiatr Scand. (2008) 118:291–6. doi: 10.1111/j.1600-0447.2008.01247.x
54. Wingenfeld K, Spitzer C, Mensebach C, Grabe H, Hill A, Gast U, et al. Die deutsche Version des Childhood Trauma Questionnaire (CTQ): erste Befunde zu den psychometrischen Kennwerten. Psychother Psychosom Med Psychol. (2010) 60:442–50. doi: 10.1055/s-0030-1247564
55. Klinitzke G, Romppel M, Häuser W, Brähler E, and Glaesmer H. Die deutsche Version des Childhood Trauma Questionnaire (CTQ) – psychometrische Eigenschaften in einer bevölkerungsrepräsentativen Stichprobe. Psychother Psychosom Med Psychol. (2012) 62:47–51. doi: 10.1055/s-0031-1295495
56. Kratzer L, Heinz P, Ehrig C, Schiepek G, and Schennach R. Evidence of a continuum of trait mindfulness deficits in psychiatric disorders. Psychother Psychosom. (2018) 88:43–4. doi: 10.1159/000493365
57. Bloomfield MAP, Chang T, Woodl MJ, Lyons LM, Cheng Z, Bauer-Staeb C, et al. Psychological processes mediating the association between developmental trauma and specific psychotic symptoms in adults: a systematic review and meta-analysis. World Psychiatry. (2021) 20:107–23. doi: 10.1002/wps.20841
58. Varese F, Barkus E, and Bentall RP. Dissociation mediates the relationship between childhood trauma and hallucination-proneness. Psychol Med. (2012) 42:1025–36. doi: 10.1017/S0033291711001826
59. Sun P, Alvarez-Jimenez M, Simpson K, Lawrence K, Peach N, and Bendall S. Does dissociation mediate the relationship between childhood trauma and hallucinations, delusions in first episode psychosis? Compr Psychiatry. (2018) 84:68–74. doi: 10.1016/j.comppsych.2018.04.004
60. Cole CL, Newman-Taylor K, and Kennedy F. Dissociation mediates the relationship between childhood maltreatment and subclinical psychosis. J Trauma Dissociation. (2016) 17:577–92. doi: 10.1080/15299732.2016.1172537
61. Renard SB, Huntjens RJC, Lysaker PH, Moskowitz A, Aleman A, and Pijnenborg GHM. Unique and overlapping symptoms in schizophrenia spectrum and dissociative disorders in relation to models of psychopathology: a systematic review. Schizophr Bull. (2017) 43:108–21. doi: 10.1093/schbul/sbw063
62. Sar V, Akyuz G, Kugu N, Öztürk E, and Ertem-Vehid H. Axis I dissociative disorder comorbidity in borderline personality disorder and reports of childhood trauma. J Clin Psychiatry. (2006) 67:1583–90. doi: 10.4088/jcp.v67n1014
63. Sar V, Alioğlu F, Akyuz G, Tayakısı E, Öğülmüş EF, and Sönmez D. Awareness of identity alteration and diagnostic preference between borderline personality disorder and dissociative disorders. J Trauma Dissociation. (2017) 18:693–709. doi: 10.1080/15299732.2016.1267684
64. Sar V, Alioğlu F, and Akyuz G. Depersonalization and derealization in self-report and clinical interview: the spectrum of borderline personality disorder, dissociative disorders, and healthy controls. J Trauma Dissociation. (2017) 18:490–506. doi: 10.1080/15299732.2016.1240737
65. Sar V, Alioğlu F, Akyuz G, and Karabulut S. Dissociative amnesia in dissociative disorders and borderline personality disorder: self-rating assessment in a college population. J Trauma Dissociation. (2014) 15:477–93. doi: 10.1080/15299732.2014.902415
66. Sar V, Taycan O, Bolat N, Ozmen M, Duran A, Öztürk E, et al. Childhood trauma and dissociation in schizophrenia. Psychopathology. (2010) 43:33–40. doi: 10.1159/000255961
67. Meares R. A dissociation model of borderline personality disorder. New York (NY: W. W. Norton & Company (2012). 396 p.
68. Michelini G, Palumbo IM, DeYoung CG, Latzman RD, and Kotov R. Linking RDoC and HiTOP: a new interface for advancing psychiatric nosology and neuroscience. Clin Psychol Rev. (2021) 86:102025. doi: 10.1016/j.cpr.2021.102025
69. Levin-Aspenson HF and Greene AL. Rethinking trauma-related psychopathology in the Hierarchical Taxonomy of Psychopathology (HiTOP). J Trauma Stress. (2024) 37:361–71. doi: 10.1002/jts.23014
70. Zimmermann J, Wendt LP, Edelhoff H, Wierzba E, Fleck L, Cicero DC, et al. Development and initial evaluation of the German version of the Hierarchical Taxonomy of Psychopathology Self-Report (HiTOP-SR). PsyArXiv (2024). Available online at: https://osf.io/dc8u6.
71. Longden E, Branitsky A, Moskowitz A, Berry K, Bucci S, and Varese F. The relationship between dissociation and symptoms of psychosis: a meta-analysis. Schizophr Bull. (2020) 46:1104–13. doi: 10.1093/schbul/sbaa037
72. Onyeama F, Melegkovits E, Yu N, Parvez A, Rodrigues A, Billings J, et al. A systematic review and meta-analysis of the traumatogenic phenotype hypothesis of psychosis. BJPsych Open. (2024) 10:e146. doi: 10.1192/bjo.2024.52
73. Hernández-Velázquez M, Díaz-Anzaldúa A, Arango I, Rosel-Vales M, and Celada-Borja C. Contrasting characteristics of psychosis in outpatients with borderline personality disorder or schizophrenia at a tertiary care institution. Front Psychiatry. (2024) 15:1485000. doi: 10.3389/fpsyt.2024.1485000
74. Tschöke S, Knauer Y, Flammer E, Usemann P, and Uhlmann C. Psychotic experiences and daily functioning in borderline personality disorder and schizophrenia. J Nerv Ment Dis. (2024) 212:187–9. doi: 10.1097/NMD.0000000000001755
75. Niemantsverdriet MBA, Van Veen RJB, Slotema CW, Franken IHA, Verbraak MJPM, Deen M, et al. Characteristics and stability of hallucinations and delusions in patients with borderline personality disorder. Compr Psychiatry. (2022) 113:152290. doi: 10.1016/j.comppsych.2021.152290
76. Strawson WH, Wang HT, Quadt L, Sherman M, Larsson DEO, Davies G, et al. Voice hearing in borderline personality disorder across perceptual, subjective, and neural dimensions. Int J Neuropsychopharmacol. (2022) 25:375–86. doi: 10.1093/ijnp/pyab093
77. Brand RM, McEnery C, Rossell S, Bendall S, and Thomas N. Do trauma-focused psychological interventions have an effect on psychotic symptoms? A systematic review and meta-analysis. Schizophr Res. (2018) 195:13–22. doi: 10.1016/j.schres.2017.08.037
78. Steil R, Dyer A, Priebe K, Kleindienst N, and Bohus M. Dialectical behavior therapy for posttraumatic stress disorder related to childhood sexual abuse: a pilot study of an intensive residential treatment program. J Trauma Stress. (2011) 24:102–6. doi: 10.1002/jts.20617
Keywords: dissociation, auditory verbal hallucination (AVH), delusions, adverse childhood events, borderline personality disorder
Citation: Schroeder K, Schätzle A, Schäfer I and Huber CG (2025) Dissociative experiences mediate the association between childhood trauma and verbal hallucinations, but not delusional thoughts, in borderline personality disorder. Front. Psychiatry 16:1532234. doi: 10.3389/fpsyt.2025.1532234
Received: 21 November 2024; Accepted: 30 July 2025;
Published: 26 August 2025.
Edited by:
Antoine Bechara, University of Southern California, United StatesCopyright © 2025 Schroeder, Schätzle, Schäfer and Huber. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katrin Schroeder, a2F0cmluLnNjaHJvZWRlckB1a2UuZGU=; Christian G. Huber, Y2hyaXN0aWFuLmh1YmVyQHVuaWJhcy5jaA==