 Maciej Żerdziński1,2*
Maciej Żerdziński1,2* Marcin Burdzik1,3*
Marcin Burdzik1,3* Paweł Dębski4,5
Paweł Dębski4,5 Roksana Żmuda1
Roksana Żmuda1 Magdalena Piegza5
Magdalena Piegza5 Piotr Gorczyca5
Piotr Gorczyca5- 1Psychiatric Department No 2, Dr. Krzysztof Czuma’s Psychiatric Center, Katowice, Poland
- 2Department of Psychiatry and Sexology, Faculty of Medicine, Academy of Silesia, Katowice, Poland
- 3Institute of Law at Faculty of Law and Administration, University of Silesia in Katowice, Katowice, Poland
- 4Institute of Psychology, Humanitas University in Sosnowiec, Sosnowiec, Poland
- 5Department of Psychiatry, Faculty of Medical Sciences in Zabrze, Medical University of Silesia in Katowice, Tarnowskie Gory, Poland
Obsessive-compulsive disorder (OCD) is characterized by obsessions and compulsions that significantly impair functioning. Obsessive-compulsive personality disorder (OCPD) co-occurs in 17-45% of OCD patients, worsening outcomes across multiple domains. Therefore, we aimed to study the impact of OCPD in more detail by analyzing selected comorbidities, emotional aspects, and sociodemographic data. This study assessed 78 OCD patients (average age 44.9 years, 34.61% OCPD), using Y-BOCS, BABS, BPAQ, BIS-11, YMRS, HDRS-17, and ASEX. Patients with comorbid OCPD had significantly worse outcomes in symptom severity (Y-BOCS = 0.0006), treatment duration (p = 0.0127), insight (BABS, p = 0.0185), aggression (p = 0.0266), impulsivity (p = 0.0469), depression (HDRS, p = 0.0178), mania (YMRS, p = 0.0003), and sexual dysfunction (ASEX, p = 0.008). OCPD was more prevalent in unemployed individuals (p = 0.046) and older patients (p = 0.009). No significant differences were found regarding gender, education, or relationship status. Obsessions and compulsions, such as contamination (p = 0.025), somatic (p = 0.018), ruminations (p = 0.003), and obsessional slowness (p = 0.007), were more common in the OCPD group. In the group with OCPD, aggression and OCD severity were correlated with increased levels of depression, which can be considered potential correlates of bipolarity in the relationship between OCD and OCPD. In conclusion, OCPD significantly worsens clinical outcomes in OCD across emotional, behavioral, and functional dimensions.
1 Introduction
1.1 OCD
Obsessive-compulsive disorder (OCD) is characterized by the presence of both obsessions and compulsions (OC). Obsessions are defined as recurrent, unwanted thoughts, impulses, or imaginings, most often perceived as intrusive, while compulsions refer to pathological motor activities or mental acts (1–7). Many researchers suggest that the emotional system is also connected to the phenomenology of OCD, especially in relation to anxiety and anger (8–11). Epidemiological studies estimate the prevalence of OCD to be between 2-3, 5% (12, 13). The initiation of therapy for OCD is often delayed and remains unsatisfactory in terms of efficacy (14, 15). Longitudinal studies report varying remission rates, ranging from 12% to 86% (16–18). The literature indicates that even after satisfactory treatment, 40-60% of OCD patients continue to experience disabling residual symptoms (19–21). In severe and chronic cases, even after significant improvement in OC, patients may continue to struggle with adjusting to normal life, a phenomenon referred to as the ‘burden of normality’ (22). This difficulty can be partly attributed to increased aggression and impulsivity, as well as frequent comorbidities, including depression (MD), bipolar disorder (BD), and obsessive-compulsive personality disorder (OCDP) (23–28).
1.2 Obsessive-compulsive personality disorder
OCPD (anankastic personality) is a distinct clinical phenomenon within the obsessive-compulsive spectrum (29, 30). The term ‘anankastic personality’ is rooted in Greek mythology, where Ananke, the goddess of necessity, symbolized inevitability, compulsion, and submission to fate. This term aptly conveys the relentless need for control and the strength of character associated with the concept (31–33). Psychoanalysts concur that the need for control in individuals with OCPD functions as a defense mechanism, concealing deeper desires for dependence rooted in childhood. The anxiety resulting from a perceived loss of control creates a barrier to emotional intimacy (34). This rigidity leads to resistance to new experiences and is reflected in traits such as low agreeableness, overzealousness, and heightened sensitivity to criticism (35–37). As a result, these individuals often exhibit antagonistic behaviors, show increased aggression and impulsivity, struggle with trust, and have difficulty maintaining interpersonal harmony, which may foster tendencies toward dominance or even tyranny (31, 33, 35, 38–43).
In both ICD-10 (F60.5) and DSM-5 (301.4), OCPD is characterized by a pervasive preoccupation with order, rules, and details, often leading to inefficiency in daily life. This rigid focus on perfectionism and control causes individuals to adhere strictly to procedures and routines, limiting their ability to adapt and hindering productivity. Several key traits in OCPD contribute to interpersonal conflicts. First, individuals with OCPD tend to be excessively conscientious and morally scrupulous, frequently imposing their rigid standards on others. This inflexibility leads to tension, particularly in professional and personal environments. Moreover, their extreme reluctance to delegate tasks unless others follow their exact methods is perceived as controlling, exacerbating relational strain. As these individuals push their standards onto others, they often fail to recognize the negative impact on their relationships, leading to a pattern of isolation and increasing emotional distress. This ongoing tension reinforces their need for control, perpetuating a cycle of conflict and emotional dissatisfaction that ultimately worsens their mental health (2, 31, 33, 40, 41, 44).
In ICD-11, the concept of anankastia (6D11.4) represents a shift towards a dimensional approach to diagnosing personality disorders, focusing on traits like perfectionism, control, and inflexibility. This model assesses the severity of these traits within specific domains of personality dysfunction. The characteristics of anankastia are largely consistent with descriptions found in ICD-10 and DSM-5, which emphasize similar patterns of rigidity, emotional constraint, and overemphasis on order and rules (44–46). Some researchers have considered including OCPD in the category of Obsessive-Compulsive and Related Disorders (OCRD) due to shared traits such as rigidity, perfectionism, and excessive control and orderliness. Although the etiological factors for these disorders may differ, the shared comorbidities in OCPD strengthen the proposal for this reclassification (29, 47–49).
The prevalence of OCPD in the general population ranges from 3-8%, with a global estimate of 6.5% based on a meta-analysis conducted by Clemento et al. (50).
OCPD is more common in older, less educated individuals, and in clinical populations, the prevalence varies, ranging from 8.7% to 26% among outpatients, and reaching 23.3% in psychiatric inpatient settings (33, 41, 50–52).
1.3 OCD and OCPD comorbidity
OCPD is thought to occur in 15-36% of individuals with OCD and is generally associated with a worse course and less favorable prognosis (29, 30, 42, 53–56). This correlation indicates an earlier age of OCD onset, stronger OC severity, poorer insight, higher comorbidity with depression and anxiety, and greater impairment in functioning (57). Patients with both OCD and OCPD are more likely to exhibit symptoms related to hoarding, symmetry, ordering, doubting, checking, counting, and arranging (55, 58). Unlike the ego-dystonic obsessions found in OCD, the obsessions in OCPD (if present) are ego-syntonic and align with the patient’s beliefs, meaning they are not necessarily perceived as unhealthy, although they can cause significant distress to others (59, 60). While there are similarities between OCPD and OCD, the later development of obsessive-compulsive symptoms should not be viewed as a direct extension of anankastic character traits (29, 48, 49).
1.4 OCD, OCPD, and affective disorders: understanding the links
The relationships between OCD and MDD, as well as BD, are well-researched. However, the link between OCPD and these conditions - particularly BD - remains less thoroughly explored.
1.4.1 OCD and MDD
OCD and MDD frequently co-occur, with 20-50% of individuals diagnosed with OCD and 20-30% of those with MDD experiencing both disorders (26, 61–63). Epidemiological studies report that the lifetime prevalence of MDD in OCD patients ranges from 40% to 67%, with OCD often preceding depressive symptoms, particularly in early-onset cases (26, 27, 64–67). Additionally, the presence of depression significantly reduces the quality of life in patients with OCD (68). MDD can also delay and complicate the treatment of OCD, with a dual diagnosis being associated with an elevated risk of suicide attempts in 6% to 52% of affected patients (17, 21, 69, 70). Chaudhary et al. (71) studied patients with both depression and OCD, demonstrating that suicidal ideation was present in 52% of the sample, with 16% having a history of suicide attempts. It was also shown that the severity of suicidal ideation correlated with the intensity of depressive symptoms, with suicidal ideation occurring in all cases of severe and very severe depression co-occurring with OCD, compared to 35% in mild and 87.5% in moderate depression. Suicidal thoughts were most commonly associated with cleanliness/contamination and religious obsessions (71). Following the recent study by Hellberg et al. (72), the presence of MDD in OCD predicts poorer treatment outcomes, with severe depression most strongly associated with repugnant or taboo obsessions. Weaker or absent correlations are observed between depression and other OCD dimensions, such as contamination-related obsessions (72).
1.4.2 OCD and BD
The links between OCD and BD have solid historical grounding. In 1921, Emil Kraepelin described cases of ‘anxious mania’ and ‘agitated depression’, highlighting anxiety as a key feature of BD. Around the same period, Abraham and Gero (1921, 1936) identified that individuals in manic episodes often engage in obsessive thinking, especially in relational contexts, where their obsession tends to focus on the object of desire (73, 74). Subsequent studies have confirmed the observation that OC frequently emerge during mixed episodes in BD, often linked with more frequent depressive recurrences (73, 75, 76). Hantouche et al. (77) identified a specific diagnostic subcategory within the group of patients suffering from OCD: ‘Cyclothymic-OCD’. In this subgroup, mood decompensation - both depressive and hypomanic - was particularly common, with OC being more episodic (77). Research indicates that the prevalence of OCD in BD patients ranges from 11% to 35.2%, while lifetime comorbidity rates of BD among OCD patients range from 11.1% to 21%. Additionally, OCD is more commonly observed in children and adolescents with BD compared to adults, and is more frequently reported in population-based studies than in hospital-based ones (7, 28, 73, 78).
The meta-analysis by Amerio et al. (79) reinforces the relationship between OCD and BD, showing that the pooled prevalence of OCD in BD patients is 17%, which is comparable to the prevalence of BD in OCD patients (18.35%). The study also highlights that OCD is more prevalent in BD-I patients (24.6%) compared to mixed BD patients (13.6%), indicating a stronger comorbidity with the more severe form of bipolar disorder (79). Notably, it has been demonstrated that 35% of BD patients in remission exhibit OCD symptoms, suggesting a higher prevalence in this group compared to those with active symptoms (80). It was also observed that among OCD patients, 53.9% were diagnosed with a dominant cyclothymic affective temperament, which was the most represented in the sample (19.2%) (81). OCD-BD was characterized by a more chronic course, higher dysfunction, suicide and hostility. In turn, OC aggressive symptoms, having first-degree relatives with OCD and comorbidity of any anxiety disorders were associated with a reduction in odds of belonging to the OCD-BD group (82). Individuals with bipolar OCD exhibit higher rates of sexual and religious obsessions and lower rates of checking rituals compared to those with non-bipolar OCD. Studies have also shown an association between symmetry obsessions, repetition, and ordering compulsions (83). Sharma and Reddy (73), in their review of the literature on the comorbidity of OCD and BD, highlighted the inconsistency of findings regarding OCS in this patient group. BD combined with OCD was associated with more frequent sexual, religious, aggressive, symmetry, and hoarding obsessions, as well as ordering and hoarding compulsions. However, other studies reported that contamination obsessions and washing compulsions were less common. There was no evidence of more severe OCS in this group, but BD-OCD patients exhibited poorer insight into OCD and experienced more frequent depressive episodes and suicidal thoughts. Additionally, studies showed higher rates of substance abuse and comorbid anxiety disorders, ADHD, and personality disorders in BD-OCD patients (73).
1.4.3 OCPD and MDD
The relationship between OCPD and MDD has been studied more frequently then BD with several findings suggesting that the presence of OCPD traits, particularly perfectionism and high moral standards, significantly increases the recurrence of depressive episodes and the risk of suicide (32, 84, 85). It has also been demonstrated that the presence of OCPD associated with MDD may increase the risk of misdiagnosis, make certain life events more stressful than usual for patients, and, once again, result in an elevated risk of suicide (86). Van Broekhoven et al. (87) highlighted the greater susceptibility of women with OCPD to postpartum depression, emphasizing the need for careful assessment of anankastic personality traits in pregnant women to better monitor and mitigate the risks of depression and suicide (87).
1.4.4 OCPD and BD
The relationship between OCPD and BD has remained significantly understudied. Rossi et al. (87) found that anankastic personality traits were the most frequently co-diagnosed in patients with BD, with a prevalence of 32.4%, compared to 31.6% for dependent personality traits in patients with recurrent depressive disorders (88). Similarly, Altindag (88) reported that OCPD was the most common personality disorder (21%) among patients with BD type I (89). It has also been described that when OCPD co-occurs with OCD, mood instability may exacerbate the presence of OCPD traits. These findings suggest a potentially significant yet underrecognized role of OCPD in influencing the course of OCD in the context of BD, underscoring the need for further research into this complex clinical relationship (90).
When considering the relationships between OCD, OCPD, and BD independently, it is important to note a significant lack of research addressing the impact of OCPD on OCD in the context of its comorbidity with BD.
2 Objectives
● Assess the prevalence of OCPD in individuals with OCD.
● Investigate the associations between OCPD and selected sociodemographic variables, particularly age, as well as factors such as employment status, the ability to maintain close relationships, and sexual functioning.
● Evaluate the impact of OCPD on the clinical course of OCD by examining selected psychopathological factors associated with worse prognosis, including OCD severity, reduced insight, aggression, impulsivity, and the occurrence of depression and mania.
● Identify the most prevalent OC symptoms in patients with coexisting OCPD.
● Analyze statistically significant findings in the OCD with OCPD group to explore their associations with levels of depression and mania, focusing on the role of bipolarity within the context of OCPD’s influence on OCD.
3 Materials and methods
This study involved seventy-eight patients with a confirmed primary diagnosis of obsessive-compulsive disorder (OCD). Participants were selected from the hospital outpatient clinic based on their diagnosis, with no additional selection criteria applied. Although the researchers were affiliated with various academic and hospital institutions, the study was conducted exclusively at a single center, the Dr. Krzysztof Czuma Psychiatric Center in Katowice, Poland. Informed consent was obtained from each participant prior to examination and inclusion in the study. All investigators had extensive experience in managing OCD patients. The study procedures were approved by the local bioethics committee (approval number BNW/NWN/0052/KB/172/23).
The current mental state of all subjects was evaluated using the following validated diagnostic questionnaires:
● OCD assessment (presence and severity): Yale-Brown Obsessive-Compulsive Scale (Y-BOCS) (91),
● Assessment of OCD level of insight: Brown Assessment of Beliefs Scale (BABS) (92),
● Assessment of aggression level: Buss-Perry Aggression Questionnaire (BPAQ) (93),
● Assessment of impulsivity level: Barratt Impulsivity Scale (BIS-11) (94),
● Assessment of the presence of affective symptoms: Young Mania Rating Scale (YMRS) (95) and Hamilton Depression Rating Scale (HDRS-17) (96),
● Sexual functioning evaluation: Arizona Sexual Experiences Scale (ASEX) (97),
● The duration of OCD treatment was assessed based on medical records and medical history collected from the subjects,
● Identification of OCPD traits was conducted according to the DSM-5 criteria (2). These traits had to be chronic, begin in early adulthood, and persist regardless of circumstances.
Based on the obtained results, the total study group was divided into two subgroups: patients with OCD without OCPD and patients with both OCD and OCPD. These subgroups were compared across the following variables:
● age, gender, education, employment status, ability to maintain close relationships, and sexual functioning
● OCD severity, levels of insight, characteristics of obsessive-compulsive symptoms, and duration of treatment
● levels of aggression, impulsivity, depression, and mania
Additionally, an analysis was conducted to determine which of the statistically significant findings correlated with levels of depression and mania.
Data processing was conducted using Excel 2016 and Statistica version 13.3. The normality of the distribution of variables was verified with the Shapiro-Wilk test. Skewness and kurtosis tests were used to assess the data distribution for asymmetry and kurtosis relative to a normal distribution. The Mann-Whitney U test was used to assess the significance of differences in continuous variables between patients with OCD and patients with both OCD and OCPD. The association between the co-occurrence of OCD and OCPD with individual obsessions and compulsions was assessed using the chi-square test. The level of statistical significance was set at α ≤ 0.05.
4 Results
Among the study participants, 36 (46.15%) were men and 42 (53.84%) were women. The average age of the respondents was 44.9 years. Regarding education, 57.69% (n = 45) of respondents had a university degree, while 42.31% (n = 33) had lower levels of education (secondary, vocational, primary). A total of 65.38% (n = 51) of individuals were in a close relationship, while 34.62% (n = 27) were single. Additionally, 61.54% of subjects (n = 48) were employed, and 38.46% (n = 30) were unemployed.
It was found that in the entire study group (n = 78), 34.61% of participants (n = 27) met the criteria for OCPD, while 65.38% (n = 51) did not. According to the chi-square test results, there were no significant differences in the prevalence of OCPD among OCD patients when considering gender (chi-square = 0.553; p = 0.457), education level (chi-square = 2.207; p = 0.137), or relationship status (chi-square = 0.037; p = 0.847). However, OCPD was found to be significantly more common among the unemployed (67.74%) compared to the employed (44.90%) (chi-square = 3.986; p = 0.046). It was also observed that participants with both OCD and OCPD were significantly older (median = 48) compared to those with OCD alone (median = 38) (p = 0.009). Descriptive statistics of continuous variables are presented in Table 1 for patients with OCD and those with both OCD and OCPD.
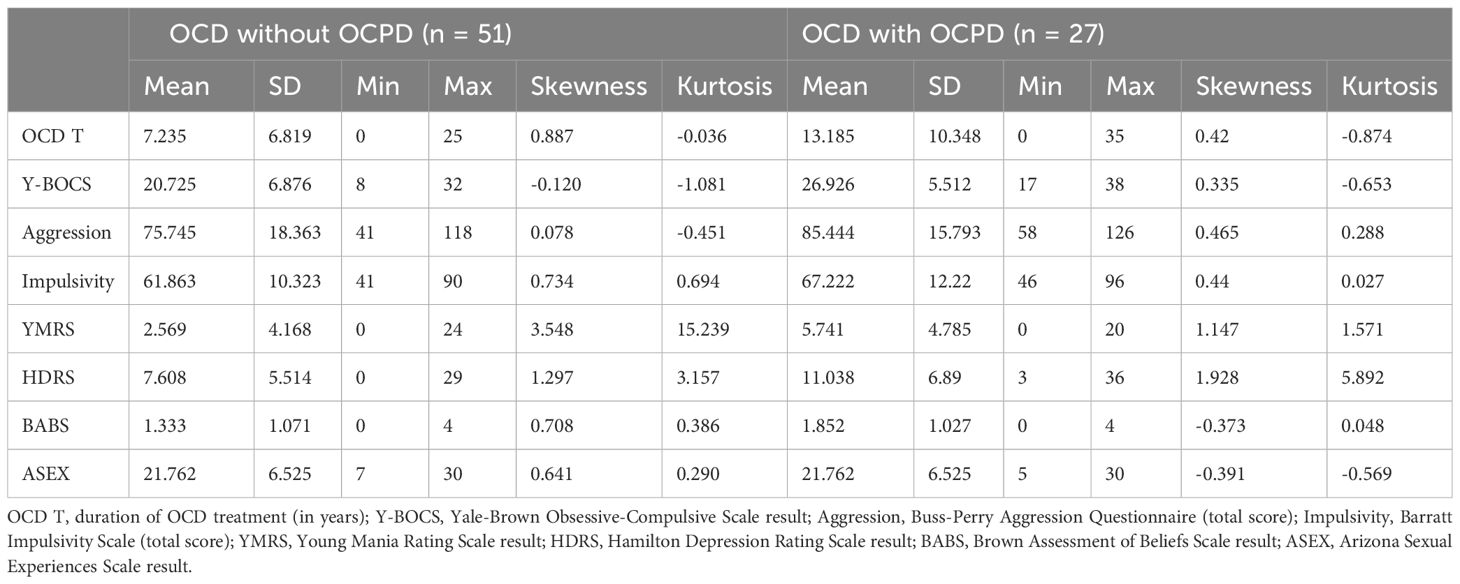
Table 1. Descriptive statistics of variables in the group of patients with OCD without OCPD (n = 51) and with OCD and OCPD (n = 27).
Significance analysis of differences between OCD and OCPD patients using the Mann-Whitney U test showed statistically significant differences between subgroups in Y-BOCS, BPAQ, BIS-11, BABS, YMRS, HDRS, and ASEX scores. In all parameters, significantly higher values were obtained in patients with both OCD and OCPD. This means that those with a dual diagnosis were characterized by higher severity of OCD symptoms, higher levels of aggression and impulsivity, poorer levels of insight, and higher severity of both depression and mania. Patients with OCD and OCPD showed significantly worse sexual functioning as measured by the ASEX scale. This group of patients also had a statistically significant longer duration of treatment than patients with isolated OCD. Differences in the severity of individual variables are shown in Table 2 and Figure 1.
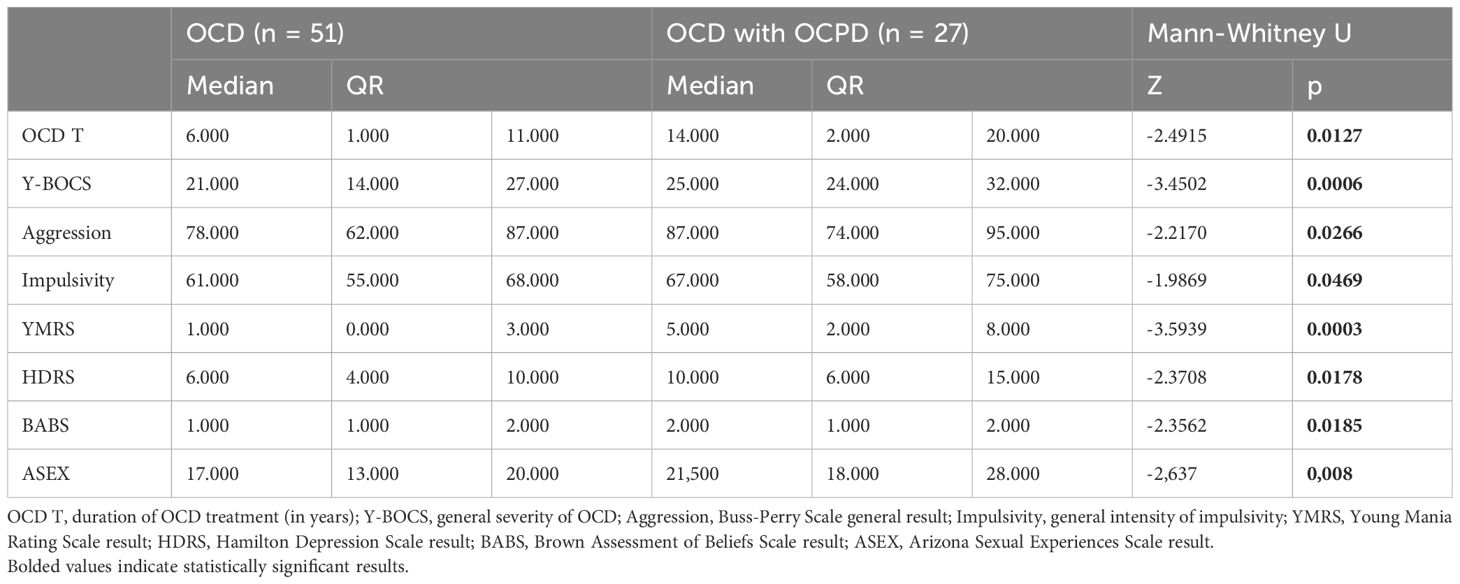
Table 2. Differences in severity of continuous variables between patients with OCD without OCPD and patients with OCD and OCPD.
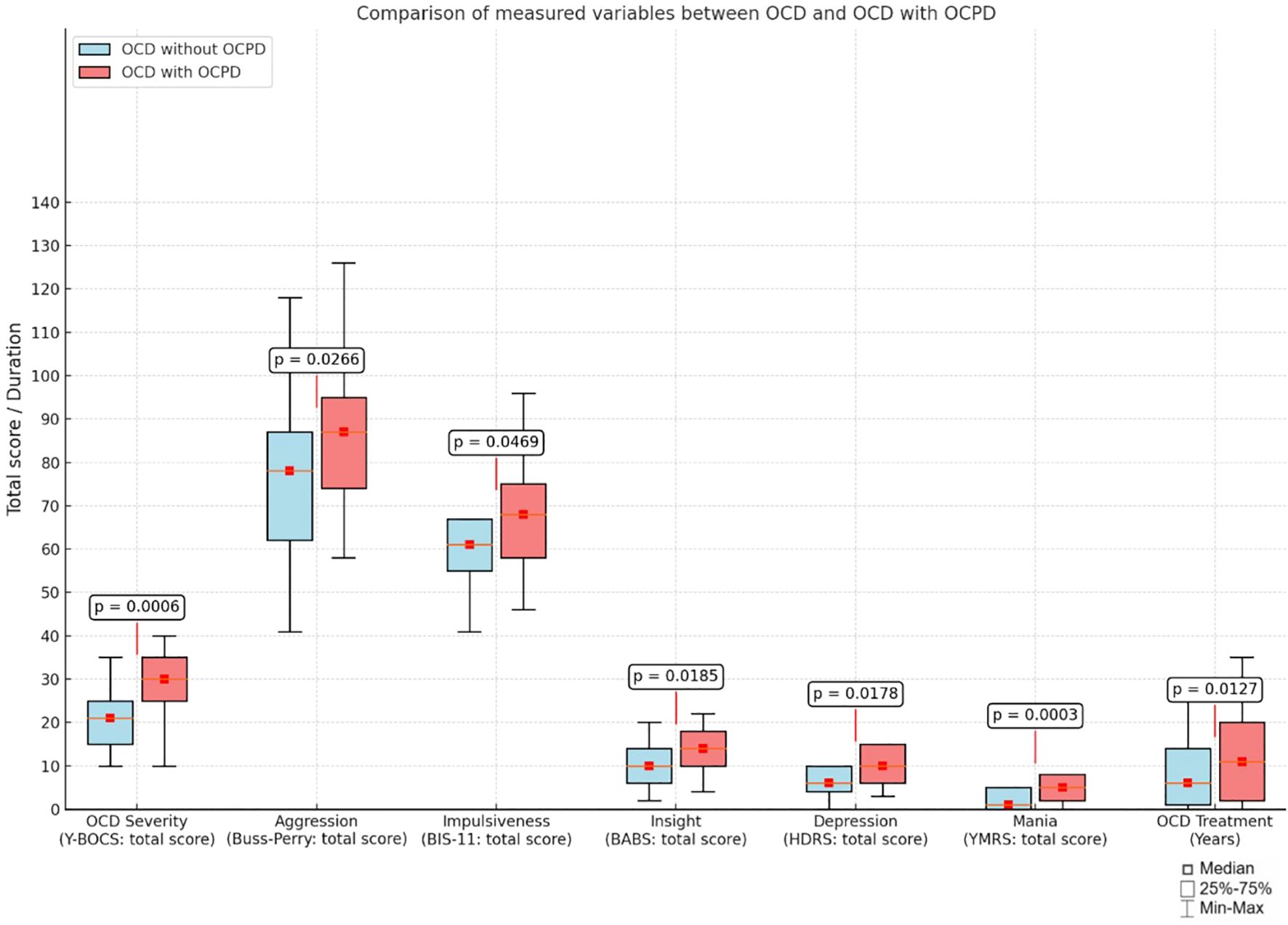
Figure 1. Comparison of continuous variables between patients with OCD without OCPD and patients with both OCD and OCPD.
In assessing the strength of the relationships between variables that were found to be statistically significant for the OCD with OCPD group and levels of mania and depression, statistically significant and positive correlations were found between HDRS and BP-total (p = 0.353), BP-A (p = 0.400), and BP-H (p = 0.322). Additionally, positive correlations were observed between Y-BOCS total (p = 0.421), Y-BOCS obsessions (p = 0.378), and Y-BOCS compulsions (p = 0.423) with HDRS. The following variables did not show statistically significant correlations with either YMRS or HDRS: age (p = 0.035 for YMRS, p = 0.083 for HDRS), BP-PA (p = 0.160 for YMRS, p = 0.088 for HDRS), BP-VA (p = 0.035 for YMRS, p = 0.262 for HDRS), impulsiveness (p = 0.044 for YMRS, p = 0.082 for HDRS), cognitive impulsivity (p = 0.022 for YMRS, p = 0.238 for HDRS), motor impulsivity (p = 0.177 for YMRS, p = -0.011 for HDRS), planning impulsivity (p = -0.044 for YMRS, p = 0.073 for HDRS), BABS (p = 0.081 for YMRS, p = -0.073 for HDRS), and treatment length (p = -0.087 for YMRS, p = 0.064 for HDRS). Table 3 presents Spearman correlation coefficients between selected clinical variables and the YMRS and HDRS in the group of patients with OCD and OCPD.

Table 3. Spearman correlation coefficients for the group of individuals with OCD and OCPD (n = 27).
The chi-square test evaluating the association between distinct obsessive-compulsive symptom dimensions and the presence of OCPD revealed significant differences between patients with OCD alone and those with both OCD and OCPD. In the OCD with OCPD group, significant differences were observed for the following symptoms: contamination obsessions (92.59% vs. 70.59%, chi-square = 5.015, p = 0.025), somatic obsessions (85.19% vs. 58.82%, chi-square = 5.633, p = 0.018), ruminations (96.30% vs. 66.67%, chi-square = 8.731, p = 0.003), obsessive doubts (100% vs. 86.27%, chi-square = 4.071, p = 0.044), avoidance compulsions (77.78% vs. 49.02%, chi-square = 6.035, p = 0.014), prevention compulsions (92.59% vs. 68.63%, chi-square = 5.712, p = 0.017), self-aggressive compulsions (37.04% vs. 15.69%, chi-square = 4.534, p = 0.033), and obsessional slowness (40.74% vs. 13.73%, chi-square = 7.258, p = 0.007). Furthermore, one obsession subtype, specifically sexual obsessions, was observed more frequently in the OCD with OCPD group compared to those with OCD alone, though this difference did not reach statistical significance (50.98% vs. 44.44%, chi-square = 0.302, p = 0.583). In the OCD alone group, while no statistically significant differences were found, several obsession and compulsion subtypes were more frequently observed compared to the group with both OCD and OCPD: hoarding obsessions (68.63% vs. 18.52%, chi-square = 19.194, p < 0.001), hoarding compulsions (68.63% vs. 29.63%, chi-square = 11.051, p = 0.001), control obsessions (100% vs. 88.24%, chi-square = 3.441, p = 0.064), religious obsessions (55.56% vs. 47.06%, chi-square = 0.510, p = 0.475), control compulsions (96.30% vs. 86.27%, chi-square = 1.926, p = 0.165), repetition compulsions (74.07% vs. 66.67%, chi-square = 0.455, p = 0.500), counting compulsions (29.63% vs. 25.49%, chi-square = 0.154, p = 0.695), and order compulsions (81.48% vs. 68.63%, chi-square = 1.483, p = 0.223). Key differences are shown in Figure 2.
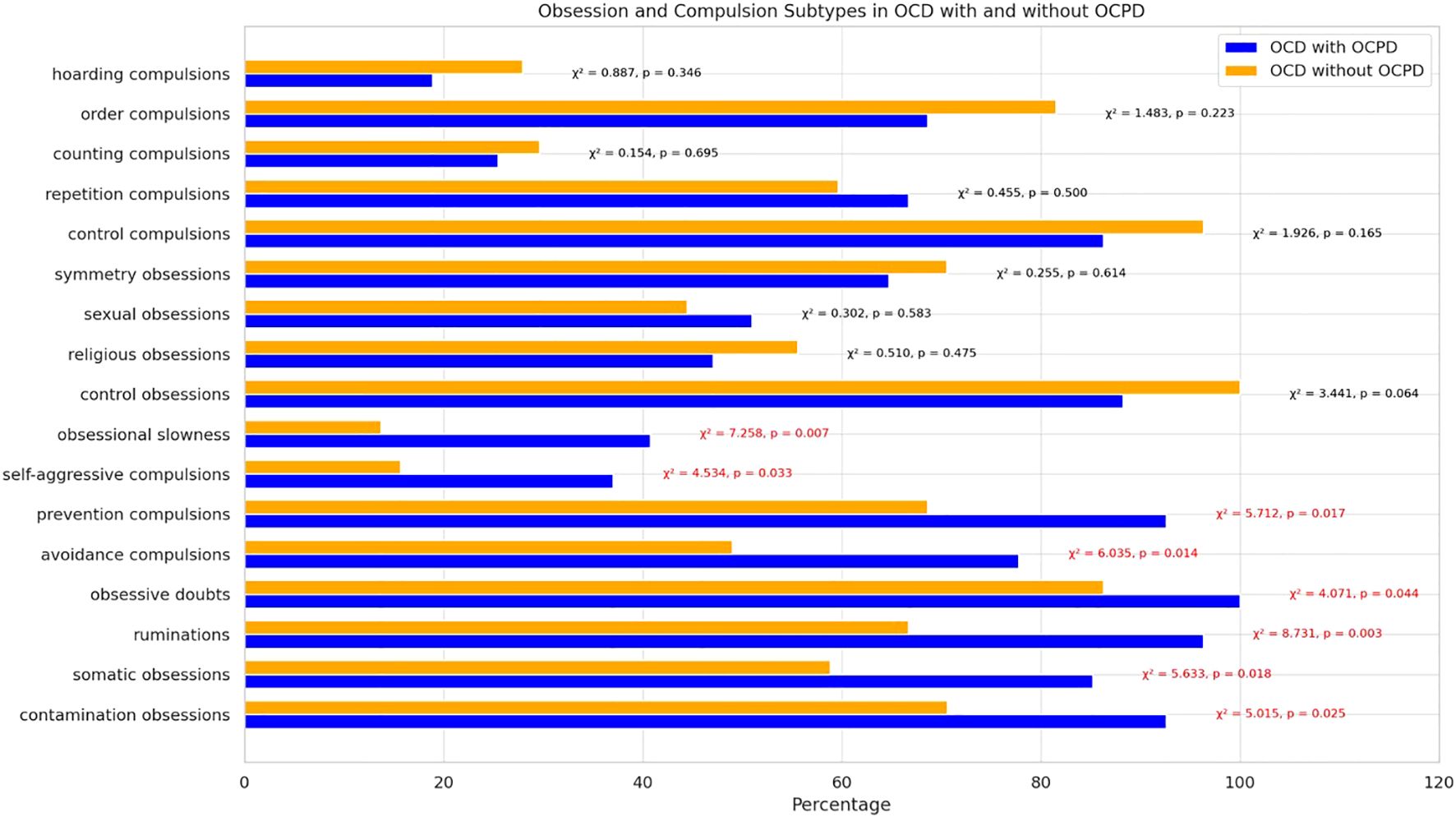
Figure 2. Distribution and comparison of the most common obsessions and compulsions in OCD and OCD with OCPD subgroups based on Y-BOCS results.
5 Discussion
The phenomenon of anankastic personality is still a poorly understood and underestimated problem (40–42, 45, 98). However, the results of our study showed that the co-occurrence of OCD with OCPD is relatively common, which was found in 34.61% of patients in the entire study group. This result confirms the findings obtained by other researchers (42, 53, 54, 98). Furthermore, our study demonstrated that the presence of OCPD significantly affects several critical aspects of OCD. In particular, it exacerbates the severity of OC symptoms and worsens insight into obsessive-compulsive behavior. These findings are also consistent with those reported by other researchers (42, 53, 54, 57). Greater severity of OCD symptoms, accompanied by significantly poorer insight and resulting in ego-syntonic obsessions, has been shown to negatively impact the course of treatment (24, 99, 100). This highlights that ego-syntonicity is associated with reduced motivation and poor treatment adherence (101, 102). Consequently, it is not surprising that the group with both OCD and OCPD had a significantly longer treatment duration (13.185 years) compared to those without OCPD (7.235 years). Our findings indirectly correlate with a longitudinal study by Eisen et al. (102), which found that OCPD comorbidity was associated with more than twice the risk of OCD recurrence after remission over a five-year follow-up period (103).
Comparing the two study subgroups, no significant differences were observed in terms of age, education, and the ability to maintain close relationships. However, among patients with both OCD and OCPD, 67.74% were unemployed compared to 44.90% without OCPD, and they were significantly older than respondents with OCD alone (47.767 and 40.730 years old, respectively). These results, supported by Diedrich and Voderholzer (41), confirm that the presence of OCPD negatively impacts the course of OCD and reduces life satisfaction due to significantly lower sexual functionality (41). These findings are also confirmed by a study in which poorer quality of life and the presence of depression were considered predictors of OCD course severity (99). Thus, as described by Jaisoorya and Janardhan (21), the problem with functional recovery of OCD patients can be explained by the frequent co-occurrence of OCPD (21). Furthermore, the significantly reduced sexual functionality observed in patients with a dual diagnosis may correspond with other findings from our research, such as the increased levels of aggression and impulsivity, which were also found to be significantly higher in subjects with both OCD and OCPD. These results may relate to findings from a study on the severity of impulsivity and aggression among psychiatric patients, where 24-52% of the 118 subjects exhibited features of OCPD (40). In individuals with OCD, elevated anger and impulsivity have been noted to worsen OC symptoms, contributing to increased depression, reduced insight, and the development of dysfunctional beliefs and maladaptive emotion regulation strategies (104–107). These observations suggest that the presence of OCPD, with heightened aggressive impulsivity, may complicate the therapeutic process and consequently prolong treatment duration, as demonstrated in our study, potentially serving as a predictor of poorer outcomes in OCD.
Equally interesting was the demonstration that OCPD contributes to significantly increased levels of depression and mania. It has been confirmed that affective disorders worsen the course of OCD and negatively affect the patient’s quality of life (18, 26, 99, 108, 109). As described in the introduction, a study by Hantouche et al. (109) suggests a distinct form of OCD, referred to as cyclothymic OCD (110). More specifically, it is characterized by the following features: a higher number of manic/hypomanic episodes and major depressive episodes, a higher frequency of aggressive, impulsive, religious, and sexual obsessions, control compulsions, hoarding, repetition; and finally, an elevated rate of mood changes with aggressive behavior (77). Interestingly, despite these findings, Hantouche et al. did not explore the potential impact of OCPD in their conclusions. However, our patients with OCD and OCPD shared very similar phenomena to those reported above: greater symptom severity, higher levels of mania and depression, and increased levels of impulsivity and aggression. In turn, the demonstrated and elevated frequency of obsessive doubts, avoidance and prevention OC may be related to the need for control and repetition described in the by Hantouche’s study. Therefore, it can be hypothesized that,cyclothymic OCD’ is in fact an obsessive-compulsive disorder with a comorbid anankastic personality. In turn, the previously cited Rossi et al. (87) and Altindag (88) both highlighted the prevalence of OCPD in patients with BD (19 - 32%) (88, 89). As our study demonstrated significantly elevated levels of depression and mania in patients with both OCD and OCPD, this suggests a broader connection between these disorders and bipolarity, potentially explaining the higher prevalence of BD in OCD, estimated at 11% to 35%, which is similar to the comorbidity rates of OCD with OCPD, ranging from 15% to 36% (29, 30, 42, 53–56, 78, 111–113).
In our study, we also aimed to assess the strength of correlations between statistically significant variables showed in the group with OCPD and their potential impact on bipolarity.
Significant positive correlations were observed between depressive symptoms (HDRS) and overall aggression (BP-total, p = 0.353), anger (BP-A, p = 0.400), hostility (BP-H, p = 0.322), as well as OCD severity (Y-BOCS total, p = 0.421; Y-BOCS obsessions, p = 0.378; Y-BOCS compulsions, p = 0.423). These findings indicate that passive forms of aggression and higher OCD severity are closely linked to depression in this group. No significant correlations were found between impulsivity or aggression and mania severity. Based on these results, the predictors of bipolarity in the OCD with OCPD may include heightened depressive symptoms, aggression (particularly anger and hostility), and increased OC severity. This highlights the need for further investigation into the relationship between OCPD and bipolarity in OCD. Notably, in the meta-analysis by Amerio et al. (79), which explored the prevalence and predictors of comorbid BD and OCD, OCPD was not mentioned (79). Similarly, in the more recent meta-analysis by de Filippis et al. (113), which framed OCD as a possible epiphenomenon of comorbid bipolar disorder, OCPD was also not considered (114).
In our study, individuals with both OCD and OCPD exhibited significantly higher rates of contamination, somatization, doubt, and rumination obsessions, alongside avoidance, prevention, and self-aggression compulsions. This may contribute to a more unfavorable course of OCD, particularly by exacerbating obsessional slowness. The group with OCPD showed a significantly stronger association with this phenomenon, rarely described in the medical literature, characterized by extreme helplessness during obsessions and avoidance of activities due to the fear of compulsions lasting many hours or even days (6, 60, 74, 115). In contrast, patients with OCD alone showed higher, though not statistically significant, rates of hoarding, control, religious, and symmetry-related obsessions, as well as repetition, counting, and ordering compulsions. Our study included a relatively small sample size, which may account for some of the variations observed compared to the findings of Gordon et al. (58) and Thamby and Khanna (55), where hoarding, symmetry, and ordering symptoms were more prominent in cases of comorbid OCPD. These discrepancies may also reflect differences in methodology or patient populations (55, 58).
In analyzing the identified OC symptoms, it is worth revisiting the influence of OCPD on bipolarity within OCD. Unlike other studies, De Prisco et al. (115), through a meta-analysis, demonstrated that only two OC symptoms - sexual and contamination obsessions - were significant in OCPD-BD comorbidity (116). In our sample of individuals with both OCD and OCPD, we also observed an increased presence of contamination and somatic obsessions, though only contamination obsessions reached statistical significance. These findings suggest that contamination obsessions may serve as indicators of OCPD’s influence on bipolarity within OCD, highlighting the need for further investigation into this relationship.
Reflecting on all the deficits observed due to the presence of OCPD in the course of OCD, this co-occurrence proves to have a significantly negative impact. OCPD exacerbates OCD symptoms by increasing the severity of OC, contributing to obsessive slowness, and leading to reduced insight. Moreover, patients with coexisting OCPD tend to be older, require longer treatment durations, and exhibit increased levels of impulsivity, further complicating the course of OCD. In addition, our analysis revealed that OCPD significantly impacts levels of both depression and mania, with heightened depressive symptoms correlating with increased aggression (anger and hostility), and more severe OCD symptoms, such as obsessive-compulsive behaviors, serving as potential predictors of bipolarity in this group.
Taken together, our findings point to the potential relevance of comorbid OCPD in shaping the clinical course and symptom profile of OCD. Further research based on larger and more diverse clinical samples is needed to confirm these associations, particularly in relation to bipolar features and treatment responsiveness. These preliminary observations may offer a useful starting point for developing more individualized clinical approaches.
6 Conclusions
1. The presence of OCPD is relatively common in individuals with OCD.
2. OCPD in the context of OCD can be considered a predictor of increased OCD severity and reduced insight, being significantly associated with older age.
3. The comorbidity of OCPD with OCD significantly increases levels of depression and mania in individuals with OCD.
4. The influence of OCPD on OCD results in a significant increase in levels of aggression and impulsivity.
5. The presence of OCPD is associated with higher rates of contamination and somatic obsessions, ruminations, avoidance and prevention compulsions, and obsessional slowness.
6. Predictors of bipolarity in OCD with comorbid OCPD include heightened depressive symptoms, aggressive impulses, and obsessive-compulsive symptoms.
7. The presence of OCPD may be associated with factors such as unemployment and reduced quality of sexual life in individuals with OCD.
8. Diagnosing OCPD should be a routine part of assessing patients with OCD.
9. The interactions between OCPD, OCD, and bipolarity should be explored in future studies.
7 Limitations of the study
● The results for assessing the prevalence of individual obsessions and compulsions in both subgroups were based on small patient groups, which could potentially bias the final assessment and limit the generalizability of the findings.
● Only selected phenomena were included in the comparison of both subgroups, suggesting that other variables not covered in the study might differentiate or further align patients with OCD and OCPD.
● The study did not take into account the diversity of treatment approaches, focusing primarily on a sample in which 93.6% of participants received pharmacological treatment (alone or in combination with psychotherapy). As a result, it was not possible to assess the potential differential effects of treatment modalities on the clinical course of OCD in patients with comorbid OCPD.
● Retrospective data on the age of OCD onset were not collected, which limits the ability to reconstruct the chronological development of symptoms. In the case of OCPD, the gradual and often diffuse nature of personality trait formation makes determining a specific onset point inherently difficult.
● The assessment of OCPD may be influenced by the presence of active OCD symptoms. Although diagnoses were based on clinical judgment and DSM-5 criteria, evaluating OCPD during symptom remission might increase diagnostic accuracy.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Bioethics Committee at the Silesian Medical Chamber. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MŻ: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MB: Conceptualization, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. PD: Conceptualization, Data curation, Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. RŻ: Investigation, Writing – original draft, Writing – review & editing. MP: Funding acquisition, Investigation, Writing – original draft, Writing – review & editing. PG: Supervision, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. The Article Processing Charges (APCs) for this article was covered by the Academy of Silesia in Katowice, Poland and Medical University of Silesia in Katowice, Poland.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Abramowitz JS, Taylor S, McKay D. Obsessive-compulsive disorder. Lancet. (2009) 374:491–9. doi: 10.1016/S0140-6736(09)60240-3
2. American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th. Arlington, VA: American Psychiatric Association (2013). doi: 10.1176/appi.books.9780890425596
3. Catts S, McConaghy N. Ritual prevention in the treatment of obsessive-compulsive neurosis. Aust N Z J Psychiatry. (1975) 9:37–41. doi: 10.3109/00048677509159819
4. Crowe E, Rosário MC, Ferrão YA, Albertella L, Miguel EC, Fontenelle LF. Obsessional slowness in obsessive-compulsive disorder: identifying characteristics and comorbidities in a clinical sample. Int J Psychiatry Clin Pract. (2023) 27:161–70. doi: 10.1080/13651501.2022.2147441
5. Sibrava NJ, Boisseau CL, Mancebo MC, Eisen JL, Rasmussen SA. Prevalence and clinical characteristics of mental rituals in a longitudinal clinical sample of obsessive-compulsive disorder. Depress Anxiety. (2011) 28:892–8. doi: 10.1002/da.20869
6. Veale D. Classification and treatment of obsessional slowness. Br J Psychiatry. (1993) 162:198–203. doi: 10.1192/bjp.162.2.198
7. Żerdziński M. Diagnosis of obsessive-compulsive disorder in the course of bipolar disorder. Psychiatr Psychol Klin. (2016) 16:61–7. doi: 10.15557/PiPK.2016.0009
8. Lopez-Sola C, Fontenelle LF, Bui M, Hopper JL, Pantelis C, Yücel M, et al. Aetiological overlap between obsessive-compulsive related and anxiety disorder symptoms: multivariate twin study. Br J Psychiatry. (2016) 208:26–33. doi: 10.1192/bjp.bp.114.156281
9. McCubbin RA, Sampson MJ. The relationship between obsessive–compulsive symptoms and appraisals of emotional states. J Anxiety Disord. (2006) 20:42–57.
10. Moscovitch DA, McCabe RE, Antony MM, Rocca L, Swinson RP. Anger experience and expression across the anxiety disorders. Depress Anxiety. (2008) 25:107–13. doi: 10.1002/da.20280
11. Whiteside SP, Abramowitz JS. Obsessive-compulsive symptoms and the expression of anger. Cognit Ther Res. (2004) 28:259–68.
12. Zohar AH, Ratefui G, Bauls DL, Artet A, Bleich A, Kron S, et al. An epidemiological study of obsessive-compulsive disorder and related disorders in Israeli adolescents. J Am Acad Child Adolesc Psychiatry. (1992) 31:1057–61. doi: 10.1097/00004583-199211000-00010
13. Ruscio AM, Stein DJ, Chiu WT, Kessler RC. The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Mol Psychiatry. (2010) 15:53–63.
14. Sharma E, Math SB. Course and outcome of obsessive-compulsive disorder. Indian J Psychiatry. (2019) 61:43–50. doi: 10.4103/psychiatry.IndianJPsychiatry_521_18
15. Żerdziński M, Burdzik M, Żmuda R, Witkowska-Berek A, Dębski P, Flajszok-Macierzyńska N, et al. Sense of happiness and other aspects of quality of life in patients with obsessive-compulsive disorder. Front Psychiatry. (2022) 13:1077337. doi: 10.3389/fpsyt.2022.1077337
16. Burchi E, Hollander E, Pallanti S. From treatment response to recovery: a realistic goal in OCD. Int J Neuropsychopharmacol. (2018) 21:1007–13. doi: 10.1093/ijnp/pyy079
17. Jakubovski E, Diniz JB, Valerio C, Fossaluza V, Belotto-Silva C, Gorenstein C, et al. Clinical predictors of long-term outcome in obsessive-compulsive disorder. Depress Anxiety. (2013) 30:763–72. doi: 10.1002/da.22013
18. Marcks BA, Weisberg RB, Dyck I, Keller MB. Longitudinal course of obsessive-compulsive disorder in patients with anxiety disorders: a 15-year prospective follow-up study. Compr Psychiatry. (2011) 52:670–7. doi: 10.1016/j.comppsych.2011.01.001
19. Norberg MM, Calamari JE, Cohen RJ, Riemann BC. Quality of life in obsessive-compulsive disorder: an evaluation of impairment and a preliminary analysis of the ameliorating effects of treatment. Depress Anxiety. (2008) 25:248–59. doi: 10.1002/da.20298
20. Del Casale A, Sorice S, Padovano A, Simmaco M, Ferracuti S, Lamis DA, et al. Psychopharmacological treatment of obsessive-compulsive disorder (OCD). Curr Neuropharmacol. (2019) 17:710–36. doi: 10.2174/1570159X16666180813155017
21. Jaisoorya TS, Janardhan Reddy YC. Functional recovery in obsessive–compulsive disorder. J Psychosoc Rehabil Ment Health. (2023) 10:11–3. doi: 10.1007/s40737-022-00325-0
22. Bosanac P, Hamilton BE, Lucak J, Castle D. Identity challenges and ‘burden of normality’ after DBS for severe OCD: a narrative case study. BMC Psychiatry. (2018) 18:186. doi: 10.1186/s12888-018-1771-2
23. Albert U, Maina G, Bogetto F, Chiarle A, Mataix-Cols D. Clinical predictors of health-related quality of life in obsessive-compulsive disorder. Compr Psychiatry. (2010) 51:193–200. doi: 10.1016/j.comppsych.2009.03.004
24. Gan J, He J, Fu H, Zhu X. Association between obsession, compulsion, depression and insight in obsessive-compulsive disorder: a meta-analysis. Nord J Psychiatry. (2022) 76:489–96. doi: 10.1080/08039488.2021.2013532
25. Hollander E. Managing aggressive behavior in patients with obsessive-compulsive disorder and borderline personality disorder. J Clin Psychiatry. (1999) 60:38–44.
26. Masellis M, Rector NA, Richter MA. Quality of life in OCD: differential impact of obsessions, compulsions, and depression comorbidity. Can J Psychiatry. (2003) 48:72–7. doi: 10.1177/070674370304800202
27. Sharma E, Sharma LP, Balachander S, Lin B, Manohar H, Khanna P, et al. Comorbidities in obsessive-compulsive disorder across the lifespan: a systematic review and meta-analysis. Front Psychiatry. (2021) 12:703701. doi: 10.3389/fpsyt.2021.703701
28. Kachungil F, Mohandas E. Management of obsessive-compulsive disorder comorbid with bipolar disorder. Indian J Psychiatry. (2016) 58:259–69. doi: 10.4103/0019-5545.192001
29. Fineberg NA, Reghunandanan S, Kolli S, Atmaca M. Obsessive-compulsive (anankastic) personality disorder: toward the ICD-11 classification. Braz J Psychiatry. (2014) 36:40–50. doi: 10.1590/1516-4446-2013-1282
30. Fineberg NA, Day GA, de Koenigswarter N, Reghunandanan S, Kolli S, Jefferies-Sewell K, et al. The neuropsychology of obsessive-compulsive personality disorder: a new analysis. CNS Spectr. (2015) 20:490–9. doi: 10.1017/S1092852914000662
32. Pinto A, Teller J, Wheaton MG. Obsessive-Compulsive Personality Disorder: A Review of Symptomatology, Impact on Functioning, and Treatment. Focus (Am Psychiatr Publ). (2022) 20:389–96. doi: 10.1176/appi.focus.20220058
33. Rizvi A, Torrico TJ. Obsessive-Compulsive Personality Disorder, in: StatPearls (2024). Treasure Island (FL: StatPearls Publ. Available online at: https://www.ncbi.nlm.nih.gov/books/NBK597372/ (Accessed September 30, 2024).
34. Gabbard G. Psychodynamic Psychiatry in Clinical Practice: The DSM–IV Edition. Washington, DC: American Psychiatric Press (1994).
35. Hertler SC. Migration Load, Ecological Opportunity, and Obsessive Compulsive Personality Disorder Etiology: Obsessive Character as an Adaptation to Seasonality. Evol Psychol Sci. (2015) 1:52–67. doi: 10.1007/s40806-014-0009-x
36. Warner MB, Morey LC, Finch JF, Gunderson JG, Skodol AE, Sanislow CA, et al. The longitudinal relationship of personality traits and disorders. J Abnorm Psychol. (2004) 113:217–27. doi: 10.1037/0021-843X.113.2.217
38. Grumet GW. Tyranny of the Obsessional Character. Psychol Rep. (1991) 68:71–93. doi: 10.2466/pr0.1991.68.1.71
39. Pinto A, Eisen JL, Mancebo MC, Rasmussen SA. “Obsessive-Compulsive Personality Disorder”. In: Abramowitz JS, McKay D, Taylor S, editors. Obsessive-Compulsive Disorder. Subtypes and Spectrum Conditions. Elsevier Ltd, Amsterdam (2007). p. 246–70.
40. Villemarette-Pittman NR, Stanford MS, Grexe KW, Houston RJ, Mathias CW. Obsessive-compulsive personality disorder and behavioral disinhibition. J Psychol. (2004) 138:5–22. doi: 10.3200/JRI.P.138.1.5-22
41. Diedrich A, Vedethaler U. Obsessive-compulsive personality disorder: a current review. Curr Psychiatry Rep. (2015) 17:2. doi: 10.1007/s11920-014-0547-8
42. Reddy MS, Vijay SM, Reddy S. Obsessive-compulsive (Anankastic) Personality Disorder. A Poorly Researched Landscape with Significant Clinical Relevance. Indian J Psychol Med. (2016) 38:1–5. doi: 10.4103/025
43. Rowland TA, Jainst AK, Panchal R. Living with obsessional personality. BJPsych Bull. (2017) 41:366–7. doi: 10.1192/pb.41.6.366a
44. World Health Organization. International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). World Health Organization, Geneva (2019).
45. Gecaite-Stonciene J, Lochner C, Marincowitz C, Fineberg NA, Stein DJ. Obsessive-Compulsive (Anankastic) Personality Disorder in the ICD-11: A Scoping Review. Front Psychiatry. (2021) 12:646030. doi: 10.3389/fpsyt.2021.646030
46. World Health Organization. International Classification of Diseases, Eleventh Revision (ICD-11) (2019/2021) . Available online at: https://icd.who.int/browse11 (Accessed September 30, 2024).
47. Siever LJ, Davis KL. A psychobiological perspective on the personality disorders. Am J Psychiatry. (1991) 148:1647–58.
48. Coles ME, Pinto A, Mancebo MC, Rasmussen SA, Eisen JL. OCD with comorbid OCPD: a subtype of OCD? J Psychiatr Res. (2008) 42:289–96. doi: 10.1016/j.jpsychires.2006.12.009
49. Fineberg NA, Sharma P, Sivakumaran T, Sahakian B, Chamberlain S. Does Obsessive-Compulsive Personality Disorder Belong Within the Obsessive-Compulsive Spectrum? CNS Spectr. (2007) 12:467–82. doi: 10.1017/S1092852900015340
50. Clemento MJ, Silva ASM, Pedro MOP, Paiva HS, Firico CAM, Tarales J, et al. A meta-analysis and meta-regression analysis of the global prevalence of obsessive-compulsive personality disorder. Heliyon. (2022) 8:e09912. doi: 10.1016/j.heliyon.2022.e09912
51. Zimmerman M, Rothschild L, Chelminski L. The prevalence of DSM-IV personality disorders in psychiatric outpatients. Am J Psychiatry. (2005) 162:1911–8. doi: 10.1176/appi.ajp.162.10.1911
52. Rossi A, Marinangeli MG, But G, Baboolal A, Pettorrizzi C. Pattern of comorbidity among anxious and odd personality disorders: the case of obsessive-compulsive personality disorder. CNS Spectr. (2000) 5:23–6. doi: 10.1017/S1092852900009524
53. Pinto A, Mancebo MC, Eisen JL, Pagano ME, Rasmussen SA. The Brown Longitudinal Obsessive Compulsive Study: clinical features and symptoms of the sample at intake. J Clin Psychiatry. (2006) 67:703–11. doi: 10.4088/jcp.v67n0503
54. Prabhu L, Cherian AV, Viswanath B, Kandavel T, Math SB, Reddy YCJ. Symptom dimensions in OCD and their association with clinical characteristics and comorbid disorders. J Obsessive Compuls Relat Disord. (2013) 2:14–21. doi: 10.1016/j.jocrd.2012.10.002
55. Thamby A, Khanna S. The role of personality disorders in obsessive-compulsive disorder. Indian J Psychiatry. (2019) 61:114–8. doi: 10.4103/psychiatry.IndianJPsychiatry_526_18
56. Pozza A, Starcevic V, Ferretti F, Pedani C, Crispino R, Governi G, et al. Obsessive-compulsive personality disorder co-occurring in individuals with obsessive-compulsive disorder: A systematic review and meta-analysis. Harv Rev Psychiatry. (2021) 29:95–107. doi: 10.1097/HRP.0000000000000287
57. Lochner C, Serebro P, van der Merwe L, Hemmings S, Kinnear C, Seedat S, et al. Comorbid obsessive-compulsive personality disorder in obsessive-compulsive disorder (OCD): a marker of severity. Prog Neuropsychopharmacol Biol Psychiatry. (2011) 35:1087–92. doi: 10.1016/j.pnpbp.2011.03.006
58. Gordon O, Salkovskis P, Bream V. The impact of obsessive-compulsive personality disorder on cognitive behaviour therapy for obsessive-compulsive disorder. Behav Cognit Psychother. (2016) 44:444–59. doi: 10.1017/S1352465815000582
59. Insel TR. Obsessive-Compulsive Disorder. Psychiatr Clin North Am. (1985) 8:105–17. doi: 10.1016/S0193-953X(18)30712-3
60. Tynes LL, White K, Steketee GS. Toward a new nosology of obsessive compulsive disorder. Compr Psychiatry. (1990) 31:465–80. doi: 10.1016/0010-440X(90)90033-O
61. Milanfranchi A, Marazziti D, Pfanner C, Presta S, Lensi P, Ravagli S, et al. Comorbidity in obsessive-compulsive disorder: focus on depression. Eur Psychiatry. (1995) 10:379–82. doi: 10.1016/0924-9338(96)80341-5
62. Fineberg NA, Fourie H, Gale TM, Sivakumaran T. Comorbid depression in obsessive compulsive disorder (OCD): Symptomatic differences to major depressive disorder. J Affect Disord. (2005) 87:327–30. doi: 10.1016/j.jad.2005.04.004
63. Abramowitz JS, Franklin ME, Street GP, Kozak MJ, Foa EB. Effects of comorbid depression on response to treatment for obsessive-compulsive disorder. Behav Ther. (2000) 31:517–28. doi: 10.1016/S0005-7894(00)80028-3
64. Quarantini LC, Torres AR, Sampaio AS, Fossaluza V, Mathis MA, Campagnolo AR, et al. Comorbid major depression in obsessive-compulsive disorder patients. Compr Psychiatry. (2011) 52:386–93. doi: 10.1016/j.comppsych.2010.09.006
65. Yap K, Mogan C, Kyrios M, Brennan J, Monahan K, Yap K. Obsessive-compulsive disorder and comorbid depression: The role of OCD-related and non-specific factors. J Anxiety Disord. (2012) 26:565–73. doi: 10.1016/j.janxdis.2012.03.002
66. Crino RD, Andrews G. Obsessive-compulsive disorder and axis I comorbidity. J Anxiety Disord. (1996) 10:37–46. doi: 10.1016/0887-6185(95)00033-X
67. Fineberg N, Roberts A. Obsessive compulsive disorder: a twenty-first century perspective. In: Fineberg N, Marazziti D, Stein DJ, editors. Obsessive Compulsive Disorder. A Practical Guide. Martin Dunitz, London (2001). p. 1–14.
68. Moritz S, Rufer M, Fricke S, Karow A, Morfeld M, Jelinek L, et al. Quality of life in obsessive-compulsive disorder before and after treatment. Compr Psychiatry. (2005) 46:453–9. doi: 10.1016/j.comppsych.2005.04.002
69. Albert U, De Ronchi D, Maina G, Pompili M. Suicide risk in obsessive-compulsive disorder and exploration of risk factors: a systematic review. Curr Neuropharmacol. (2019) 17:681–96. doi: 10.2174/1570159X16666180620155941
70. Pellegrini L, Maietti E, Rucci P, Casadei G, Maina G, Fineberg NA, et al. Suicide attempts and suicidal ideation in patients with obsessive-compulsive disorder: A systematic review and meta-analysis. J Affect Disord. (2020) 276:1001–21. doi: 10.1016/j.jad.2020.07.070
71. Chaudhary RK, Kumar P, Mishra BP. Depression and risk of suicide in patients with obsessive-compulsive disorder: A hospital-based study. Ind Psychiatry J. (2016) 25:166–70. doi: 10.4103/ipj.ipj_63_16
72. Hellberg SN, Abramowitz JS, Ojalehto HJ, Butcher MW, Buchholz JL, Riemann BC. Co-occurring depression and obsessive-compulsive disorder: A dimensional network approach. J Affect Disord. (2022) 317:417–26. doi: 10.1016/j.jad.2022.09.016
73. Sharma LP, Narayanaswamy JC, Seshadri S, Reddy YCJ. Obsessive-compulsive disorder comorbid with schizophrenia and bipolar disorder. Indian J Psychiatry. (2019) 61:S140–8. doi: 10.4103/psychiatry.IndianJPsychiatry_527_18
74. Żerdziński M. Anancastic power or mediocrity in health: dilemmas of patients with obsessive-compulsive disorders in the process of treatment. Case report. Postępy Psychiatrii i Neurologii. (2002) 11:103–9.
75. Dell’Osso L, Pini S, Tundo A, Sarno N, Musetti L, Cassano GB, et al. Clinical characteristics of mania, mixed mania, and bipolar depression with psychotic features. Compr Psychiatry. (2000) 41:242–7.
76. Issler CK, Monkul ES, Amaral JA, Tamada RS, Shavitt RG, Miguel EC, et al. Bipolar disorder and comorbid obsessive-compulsive disorder is associated with higher rates of anxiety and impulse control disorders. Acta Neuropsychiatr. (2010) 22:81–6.
77. Hantouche EG, Angst J, Demonfaucon C, Perugi G, Lancrenon S, Akiskal HS. Cyclothymic OCD: a distinct form? J Affect Disord. (2003) 75:1–10. doi: 10.1016/s0165-0327(02)00461-5
78. Krüger S, Bräunig P, Cooke RG. Comorbidity of obsessive-compulsive disorder in recovered inpatients with bipolar disorder. BP Disord. (2000) 2:71–4. doi: 10.1034/j.1399-5618.2000.020111.x
79. Amerio A, Stubbs B, Odone A, Tonna M, Marchesi C, Ghaemi SN. The prevalence and predictors of comorbid bipolar disorder and obsessive-compulsive disorder: A systematic review and meta-analysis. J Affect Disord. (2015) 186:99–109. doi: 10.1016/j.jad.2015.06.005
80. Zutshi A, Reddy YC, Thennarasu K, Chandrashekhar CR. Comorbidity of anxiety disorders in patients with remitted bipolar disorder. Eur Arch Psychiatry Clin Neurosci. (2006) 256:428–36.
81. D’Ambrosio V, Albert U, Bogetto F, Maina G. Obsessive-compulsive disorder and cyclothymic temperament: an exploration of clinical features. J Affect Disord. (2010) 127:295–9. doi: 10.1016/j.jad.2010.06.007
82. Khalkhali M, Vaghari S, Zare R, Kafi Masouleh SM. Obsessive Compulsive Disorder and Bipolar Disorder Comorbidity: A Comparative Study. Iran J Psychiatry. (2022) 17:127–35. doi: 10.18502/ijps.v17i2.8902
83. Zutshi A, Kamath P, Reddy YCJ. Bipolar and nonbipolar obsessive-compulsive disorder: a clinical exploration. Compr Psychiatry. (2007) 48:245–51. doi: 10.1016/j.comppsych.2006.12.005
84. Hewitt PL, Flett GL, Ediger E. Perfectionism and depression: longitudinal assessment of a specific vulnerability hypothesis. J Abnorm Psychol. (1996) 105:276–80. doi: 10.1037/0021-843X.105.2.276
85. Hewitt PL, Newton J, Flett GL, Callander L. Perfectionism and suicide ideation in adolescent psychiatric patients. J Abnorm Child Psychol. (1997) 25:95–101. doi: 10.1023/a:1025723327188
86. Raja M, Azzoni A. The impact of obsessive-compulsive personality disorder on the suicidal risk of patients with mood disorders. Psychopathology. (2007) 40:184–90. doi: 10.1159/000100366
87. van Broekhoven K, Karreman A, Hartman E, Lodder P, Endendijk J, Bergink V, et al. Obsessive-compulsive personality disorder symptoms as a risk factor for postpartum depressive symptoms. Arch Wom Ment Health. (2019) 22:475–83.
88. Rossi A, Marinangeli MG, Butti G, Scinto A, Di Cicco L, Kalyvoka A, et al. Personality disorders in bipolar and depressive disorders. J Affect Disord. (2001) 65:3–8. doi: 10.1016/s0165-0327(00)00230-5
89. Altindag A, Yanik M, Nebioglu M. Comorbid personality disorders in subjects with bipolar I disorder. Int J Psychiatry Clin Pract. (2006) 10:33–7. doi: 10.1080/13651500500305481
90. Bowen R, Balbuena L, Baetz M, Marwaha S. Mood instability in people with obsessive-compulsive disorder and obsessive-compulsive personality traits. J Obsessive-Compulsive Relat Disord. (2015) 6:108–13. doi: 10.1016/j.jocrd.2015.07.003
91. Goodman WK, Price LH, Rasmussen SA, Mazure C, Fleischmann RL, Hill CL, et al. The Yale-Brown Obsessive Compulsive Scale. I. Development, use, and reliability. Arch Gen Psychiatry. (1989) 46:1006–11. doi: 10.1001/archpsyc.1989.01810110048007
92. Eisen JL, Phillips KA, Baer L, Beer DA, Atala KD, Rasmussen SA. The Brown Assessment of Beliefs Scale: reliability and validity. Am J Psychiatry. (1998) 155:102–8. doi: 10.1176/ajp.155.1.102
93. Buss AH, Perry M. The aggression questionnaire. J Pers Soc Psychol. (1992) 63:452–9. doi: 10.1037//0022-3514.63.3.452
94. Barratt E. Anxiety and impulsiveness related to psychomotor efficiency. Percept Mot Skills. (1959) 9:191–8. doi: 10.2466/pms.1959.9.3.19
95. Young RC, Biggs JT, Ziegler VE, Meyer DA. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. (1978) 133:429–35. doi: 10.1192/bjp.133.5.429
96. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. (1960) 23:56–62. doi: 10.1136/jnnp.23.1.56
97. Elnazer HY, Baldwin DS. Structured review of the use of the Arizona sexual experiences scale in clinical settings. Hum Psychopharmacol. (2020) 35:e2730. doi: 10.1002/hup.2730
98. Fineberg NA, Kaur S, Kolli S, Mpavaenda D, Reghunandanan S. Obsessive-Compulsive Personality Disorder. In: Phillips KA, Stein DJ, editors. Handbook on Obsessive-Compulsive and Related Disorders. American Psychiatric Publishing, Washington DC - London (2015).
99. du Mortier JAM, Remmerswaal KCP, Batelaan NM, Visser HAD, Twisk JWR, van Oppen P, et al. Predictors of intensive treatment in patients with obsessive-compulsive disorder. Front Psychiatry. (2021) 12:659401. doi: 10.3389/fpsyt.2021.659401
100. Rabe-Jabłońska J. Diagnoza i leczenie zaburzenia obsesyjno-kompulsyjnego. Psychiatria. (2007) 4:160–74.
101. Summerfeldt LJ. Incompleteness, ordering, and arranging. In: Anthony MM, Purdon C, Summerfeldt LJ, editors. Cognitive behavior therapy for OCD: Beyond the basics. American Psychological Association, New York (2006). p. 187–208.
102. Belloch A, Roncero M, Perpiñá C. Ego-syntonicity and ego-dystonicity associated with upsetting intrusive cognitions. J Psychopathol Behav Assess. (2012) 34:94–106. doi: 10.1007/s10862-011-9255-4
103. Eisen JL, Sibrava NJ, Boisseau CL, Mancebo MC, Stout RL, Pinto A, et al. Five-year course of obsessive-compulsive disorder: predictors of remission and relapse. J Clin Psychiatry. (2013) 74:233–9. doi: 10.4088/JCP.12m07657
104. Cherian AV, Narayanaswamy JC, Srinivasaraju R, Viswanath B, Math SB, Kandavel T, et al. Does insight have specific correlation with symptom dimensions in OCD? J Affect Disord. (2012) 138:352–9. doi: 10.1016/j.jad.2012.01.017
105. Cludius B, Mannsfeld AK, Schmidt AF, Jelinek L. Anger and aggressiveness in obsessive-compulsive disorder (OCD) and the mediating role of responsibility, non-acceptance of emotions, and social desirability. Eur Arch Psychiatry Clin Neurosci. (2021) 271:1179–91. doi: 10.1007/s00406-020-01199-8
106. Hollander E, Greenwald S, Neville D, Johnson J, Hornig CD, Weissman MM. Uncomplicated and comorbid obsessive-compulsive disorder in an epidemiologic sample. Depress Anxiety. (1996) 4:111–9. doi: 10.1002/(SICI)1520-6394(1996)4:3<111::AID-DA3>3.0.CO;2-J
107. Painuly NP, Grover S, Mattoo SK, Gupta N. Anger attacks in obsessive compulsive disorder. Ind Psychiatry J. (2011) 20:115–9. doi: 10.4103/0972-6748.102501
108. Abramowitz JS, Storch EA, Keeley M, Cordell E. Obsessive-compulsive disorder with comorbid major depression: what is the role of cognitive factors? Behav Res Ther. (2007) 45:2257–67. doi: 10.1016/j.brat.2007.04.003
109. Jahangard L, Fadaei V, Sajadi A, Haghighi M, Ahmadpanah M, Matinnia N, et al. Patients with OCD report lower quality of life after controlling for expert-rated symptoms of depression and anxiety. Psychiatry Res. (2018) 260:318–23. doi: 10.1016/j.psychres.2017.11.080
110. Hantouche EG, Akiskal HS. Toward a definition of a cyclothymic behavioral endophenotype: Which traits tap the familial diathesis for bipolar II disorder? J Affect Disord. (2006) 96:233–7. doi: 10.1016/j.jad.2004.08.013
111. Chen YW, Dilsaver SC. Comorbidity for obsessive-compulsive disorder in bipolar and unipolar disorders. Psychiatry Res. (1995) 59:57–64.
112. Merikangas KR, Akiskal HS, Angst J, Greenberg PE, Hirschfeld RM, Petukhova M, et al. Lifetime and 12-month prevalence of bipolar spectrum disorder in the National Comorbidity Survey replication. Arch Gen Psychiatry. (2007) 64:543. doi: 10.1001/archpsyc.64.5.543
113. Amerio A, Odone A, Liapis CC, Ghaemi SN. Diagnostic validity of comorbid bipolar disorder and obsessive-compulsive disorder: A systematic review. Acta Psychiatr Scand. (2014) 129:343–58.
114. de Filippis R, Aguglia A, Costanza A, Benatti B, Placenti V, Vai E, et al. Obsessive–compulsive disorder as an epiphenomenon of comorbid bipolar disorder? An updated systematic review. J Clin Med. (2024) 13:1230. Available online at: https://www.mdpi.com/2686268 (Accessed April 10, 2025).
115. Ganos C, Kassavetis P, Cerdan M, Erro R, Balint B, Price G, et al. Revisiting the syndrome of “obsessional slowness. ” Mov Disord Clin Pract. (2015) 2:163–9. doi: 10.1002/mdc3.12140
Keywords: OCD, OCPD, OCD comorbidity, OCPD comorbidity, bipolarity, BD predictors, MDD predictors
Citation: Żerdziński M, Burdzik M, Dębski P, Żmuda R, Piegza M and Gorczyca P (2025) The impact of obsessive-compulsive personality disorder on obsessive-compulsive disorder: clinical outcomes in the context of bipolarity. Front. Psychiatry 16:1532966. doi: 10.3389/fpsyt.2025.1532966
Received: 22 November 2024; Accepted: 01 April 2025;
Published: 24 April 2025.
Edited by:
Renato de Filippis, University Magna Graecia of Catanzaro, ItalyReviewed by:
Brijesh Saran, Santosh Medical College, IndiaPerihan Esra Guvenek Cokol, McLean Hospital, United States
Copyright © 2025 Żerdziński, Burdzik, Dębski, Żmuda, Piegza and Gorczyca. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maciej Żerdziński, YXZhbG9uZUB3cC5wbA==; Marcin Burdzik, bWFyY2luLmJ1cmR6aWtAdXMuZWR1LnBs