 Alexandre Fraichot
Alexandre Fraichot Sophie Favre
Sophie Favre Hélène Richard-Lepouriel
Hélène Richard-Lepouriel- 1Mood and Anxiety Disorder Unit, Psychiatric Specialties Service, Department of Psychiatry, Geneva University Hospital, Geneva, Switzerland
- 2Department of Psychiatry, University of Geneva, Geneva, Switzerland
Introduction: Intranasal Esketamine is an effective rapid-acting antidepressant currently used to treat treatment-resistant depression. Artificial intelligence is another emerging tool in medicine, but little is known about the effectiveness of combining these innovations in psychiatry.
Methods: This case report presents the outcome of a 37-year-old patient who received intranasal Esketamine treatment (84 mg) and utilized artificial intelligence (ChatGPT-4) to generate images and interpretations of his experiences with dissociation. This process was conducted in the presence of a nurse who assessed and supported the patient. The Montgomery–Åsberg Depression Rating Scale (MADRS) was used to measure the severity of depression at the beginning of each session.
Results: The patient achieved remission from depression, with MADRS scores declining by 50% in the third session, and the scores indicated mild depression or euthymia in the eight subsequent sessions. The patient reported that incorporating artificial intelligence-generated images and interpretations helped him create a timeline of his experiences at the end of each session.
Discussion: This case report highlights the potential effectiveness of combining intranasal Esketamine treatment with generative artificial intelligence images and interpretations as part of an integration process. It also emphasizes the importance of having a nurse present to support the process. Further research is needed to determine which patients may benefit most from this combined treatment approach.
1 Introduction
Intranasal Esketamine has gained attention following its approval by the US Food and Drug Administration (2019) as well as by the European Medicines Agency (2021) to treat treatment-resistant depression, in combination with a selective serotonin reuptake inhibitor or serotonin and norepinephrine reuptake inhibitor. The REAL-ESK study suggests that combining Esketamine with Vortioxetine may benefit patients unresponsive to standard treatments (1). A systematic review of ten studies supports Esketamine’s ability to reduce depressive symptoms (2), with tolerable side effects such as nausea, dizziness, dissociation, and headache, mostly occurring around treatment sessions (3). However, long-term effects after discontinuation remain inconsistent, necessitating more robust randomized controlled trials (4). Some patients show delayed clinical responses at six months, with further symptom improvement even after stopping treatment for clinical reasons (5).
Efficacy tends to increase at doses above 28 mg, with optimal results seen between 56 and 84 mg (6). Continuation beyond the initial 4-week induction phase is recommended to maintain stability and prevent relapse (7). Esketamine, a derivative of ketamine, is a dissociative anesthetic that induces altered states of consciousness by disrupting top-down processing in the brain’s higher association cortex (8). These experiences—altered self-perception, emotional expansion, and increased connectedness—have been described by patients as therapeutically valuable (9). Integration of these experiences is crucial; without proper reflection, such effects may not yield sustained benefits (10).
Esketamine-induced dissociation may be particularly effective in cases of depersonalized depression, helping to restore emotional responsiveness by disrupting rigid patterns of thought and behavior (11). Misconceptions around Esketamine, including its dissociative effects and potential for addiction, persist. However, evidence indicates these effects are transient and generally not central to its antidepressant action (12).
Artificial intelligence (AI) is increasingly integrated into mental health care to enhance diagnostic accuracy, optimize clinical workflows, and facilitate the visualization of complex clinical data (13–17). In psychiatry, AI is applied for screening, symptom monitoring, and the development of personalized treatment plans, including conditions such as depression and treatment-resistant depression. AI-generated imagery has emerged as a novel adjunct in psychiatric care; these tools produce personalized visuals based on user input, enabling patients to explore and process emotions, memories, and fears—thereby supporting therapy through visualization and self-reflection (18).
Beyond its therapeutic uses, AI can analyze clinical data to predict treatment responses, including to interventions like intranasal Esketamine, thus offering opportunities for individualized care (19). Machine-learning models have demonstrated potential in forecasting treatment outcomes, which may support more targeted and efficient use of Esketamine in clinical settings (19, 20).
However, the integration of AI into mental health care presents notable challenges, including algorithmic bias, risks to data privacy, and ethical considerations related to incorporation into medical records (18, 20). For instance, while generative platforms such as ChatGPT-4 can produce emotionally resonant imagery, they may also perpetuate stereotypes, underscoring the necessity for robust ethical oversight (21, 22).
Although AI cannot replace human-led therapy, it can meaningfully enhance therapeutic processes when embedded within professionally guided frameworks. When implemented responsibly, AI—alongside interventions like Esketamine—may represent a promising frontier in the treatment of treatment-resistant depression.
AI-generated imagery is widely accessible and can be integrated into mental health interventions, helping individuals express emotions and engage in self-reflection. Tools like ChatGPT-4 (21) can create personalized visuals based on user input. While GPT-4 improves comprehension and warmth over GPT-3.5, it also shows an increased tendency toward stereotyping, highlighting the need for careful use in therapeutic settings (22).
This case study presents the evolution of a patient over 11 sessions of intranasal Esketamine administration combined with an antidepressant medication and enhanced by AI-generated images and interpretations. The patient contributed to the protocol by introducing ChatGPT-4 to journal his experiences directly after the Esketamine administration. This case report illustrates the emerging use of AI in contemporary clinical practice.
2 Case description
This case report used the CARE Checklist guidelines (23).
Edgar (alias), a 37-year-old man with a history of depression and anxiety, has experienced multiple depressive episodes, with his most severe occurring in 2018 when he was hospitalized, and in 2023. There is a family history of depressive disorders among his maternal relatives. There were no suicide attempts in his family, and he has never attempted suicide himself, although he has experienced suicidal ideation during episodes of depression. He has undergone various treatments, including Trazodone (prolonged formulation, 150 mg) and Bupropion 300 mg; and Pregabalin (25 mg, taken twice daily). He also received treatment with intranasal Esketamine (14 mg) combined with Escitalopram (10 mg) at a university hospital participating in a research program focused on the efficacy of low-dose Esketamine, where he had participated to five sessions and tolerated the low dosage well. However, a potentiation strategy using non-antidepressant medication was lacking to confirm any criteria for drug resistance. To address this, Quetiapine XR (50 mg) was introduced to evaluate whether this potentiation strategy would demonstrate total or partial efficacy. Since this approach did not yield the desired results, treatment with intranasal Esketamine was reconsidered.
2.1 Clinical measures:
Various scales assess depression severity. The Beck Depression Inventory (BDI) is a self-reported scale and may be affected by patients’ inability to assess their symptoms accurately (24). The Hamilton Depression Rating Scale (HDRS) includes non-mood symptoms like anxiety which can persist independently of mood improvement, potentially leading to an overestimation of depression severity after treatment. Additionally, the HDRS may not effectively capture the early response to treatment (25, 26). In Esketamine treatment protocols, the Montgomery–Åsberg Depression Rating Scale (MADRS) (27, 28) is preferred due to its sensitivity to early improvements in depression severity. This clinician-administered scale consists of 10 items rated from 0 to 6, with total scores classifying depression from mild (7–19) to severe (≥35). A two-point improvement is considered clinically relevant (29).
Additionally, blood pressure is monitored, with normal values for males aged 18–39 being 119/70 mm Hg (30).
2.2 Procedure
Esketamine nasal spray, available under a restricted distribution program, is used alongside another antidepressant in two phases: a 4-week induction phase (twice weekly) and a maintenance phase (weekly for responders). Patients are monitored for at least two hours post-administration for side effects, including nausea, dissociation, sedation, and cognitive impairment. Severe risks include abuse or misuse, suicidal thoughts, and elevated blood pressure.
Before treatment, patients undergo a medical check-up, including blood pressure monitoring and an ECG, and are advised against driving until after a whole night’s rest. Esketamine is contraindicated in patients with hypersensitivity to Esketamine/Ketamine, vascular aneurysms, arteriovenous malformations, or intracerebral hemorrhage (31).
In this case study, a senior psychiatrist (HRL) diagnosed the patient with recurrent depression (ICD-11) (32) with comorbid anxiety. The MADRS score was 23/60, indicating moderate depression, with no psychiatric or somatic comorbidities. The psychiatrist carefully monitored side effects after each Esketamine session.
Esketamine was first administered at 28mg and, as it was well tolerated, was then rapidly prescribed at 84 mg and remained with good tolerability and clinical response. The patient was also prescribed Quetiapine XR (50 mg) (Table 1).

Table 1. Scheme of the treatment.
During weekly sessions, the nurse (AF) administered intranasal Esketamine, ensured patient comfort, and monitored effects. He assessed severity of depression using the MADRS, provided feedback, and discussed any lingering feelings or dissociative experiences from previous sessions, and was prepared to manage side effects, particularly anxiety. The patient introduced the use ChatGPT-4 to generate images representing his experiences from the first session on, dictating his visions until the AI-created images aligned with them. He also reflected on these images using ChatGPT’s interpretations after the sessions.
At the time, Edgar was not receiving psychotherapy, and no psychologists were involved in the process.
Ethical review was not required for this single case study, as it did not constitute research involving human subjects under prevailing ethical guidelines. The report described routine clinical care without systematic investigation or experimental intervention, and the case did not involve sensitive information. The patient’s anonymity was preserved, and informed consent was obtained for the publication of both clinical data and the accompanying figure.
2.3 Treatment outcomes
The evolution of the MADRS scores is presented in Table 2.

Table 2. MADRS scores.
During the third Esketamine session, Edgar’s MADRS score dropped by over 50% (from 23 to 9). A reduction of 50% or more in depressive symptoms is typically regarded as a response to antidepressants in clinical trials (33). The severity of depression fluctuated between mild depression and euthymia throughout the treatment. Blood pressure remained stable (mean: 127.2/83.5 mm Hg), and side effects such as mild nausea and transient increases in blood pressure were mild and temporary (grade ≥ 2) (34), typically peaking within 40 minutes post-administration.
Dissociative effects emerged approximately 10 minutes after inhalation and lasted about an hour. Edgar used this time to document his experiences via ChatGPT-4, generating images that reflected his perceptions. He also discussed this with the nurse, integrating the other altered perceptions he had experienced, such as feelings of warmth, tactile sensations, and a sense of detachment.
In session one, he experienced anxiety and disturbing thoughts. In Figure 1, the first image created by ChatGPT-4 during the first session is darker than the following ones. Then, the AI-generated images, which were colorful and dreamlike, depicted themes such as nature, water, space, and abstract shapes. Edgar found most images pleasant, except for the first (darker) and eighth (hospital-like, evoking a sense of dying). The third session was significant, as he envisioned an entity from which he could seek support.
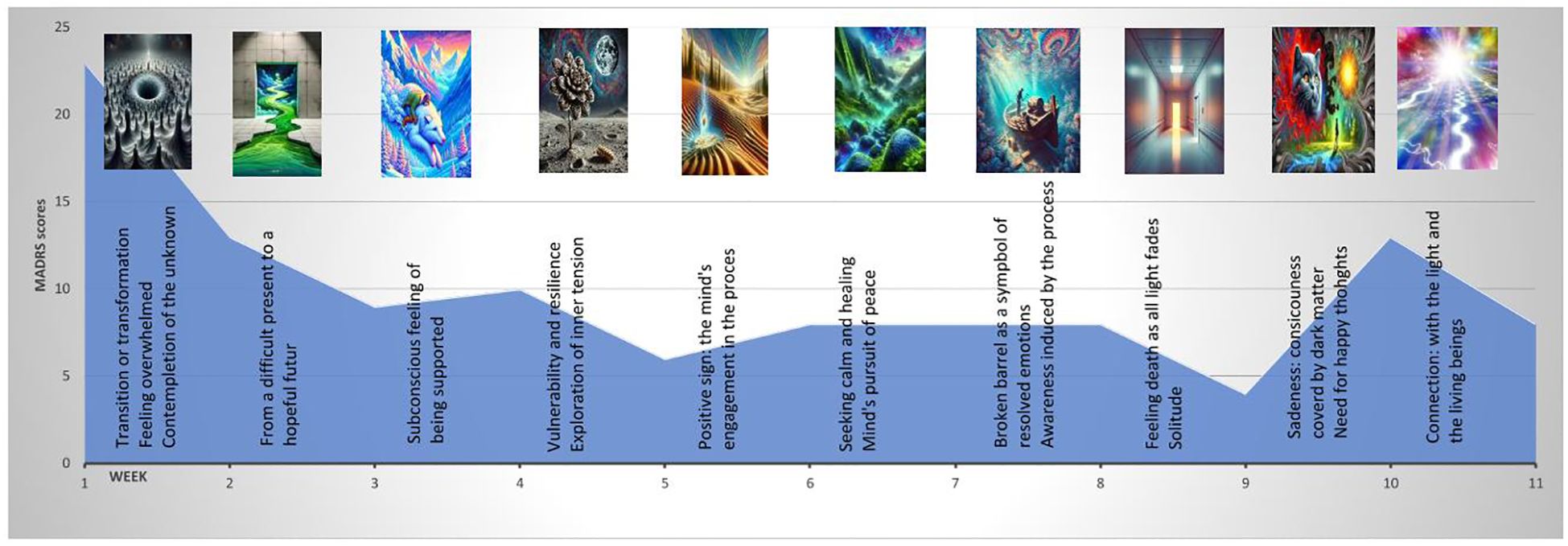
Figure 1. Timeline of the process.
For Figure 1, the patient selected images and interpretations generated with ChatGPT-4. The timeline helped him describe his journey as “a struggle with inner tensions evolving into peace of mind and a feeling of connection.” Figure 1 presents the timeline with the MADRS scores, the images, and the AI-generated interpretation during the first 11 sessions of the treatment.
Edgar valued the AI-generated timeline of his sessions, seeing it as a visual representation of progress that helped him navigate anxiety and depression. He observed that this timeline allowed him to revisit his prior experiences whenever he feels anxious or depressed. He said, “I need to see the progress and representative visual data. I can look back and see where I’m headed and compare my current state with various other moments.
While acknowledging that ChatGPT-4 is algorithm-based, he felt the images reflected truthfully and carefully his unique perspective. That differed from interactions with humans and caregivers, where components that were not his could be added.
3 Patient perspective
The patient expressed that Esketamine allowed him to access a mental space where he could explore important questions about his history and suffering, which had previously been inaccessible to him. Integrating AI into his treatment felt natural, as AI is a regular part of his daily life. Specifically, using ChatGPT-4 helped him create a timeline of his experiences, which he found valuable when managing feelings of anxiety or depression. He noted that this timeline reflected a shift from darker experiences to more colorful ones, representing his assessment of his evolution during treatment. The patient also appreciated the consistency of having the same nurse throughout his treatment, emphasizing how important it was to have someone present during moments of vulnerability.
4 Discussion
In this case report, treatment-resistant depression was treated with intranasal Esketamine, which is considered a “safe, effective, and rapid-acting option” for persons with treatment-resistant depression (33). The MADRS scores indicated a rapid remission that may be associated with factors related to the medication, the patient’s clinical history, and the patient’s age. Research has shown that antidepressant responses tend to be less robust in younger (≥ 21 years old) and older (≤ 35 years old) patients (35), and this patient falls within the age range that generally benefits the most from these treatments. Additionally, in older patients, specific symptoms (such as sadness, appetite changes, and concentration difficulties) can affect residual symptoms in those severely resistant to treatment (36), which was not the case here.
This case report explores the combination of intranasal Esketamine and AI, specifically ChatGPT-4, in the treatment of a patient with treatment-resistant depression. The patient used AI to document and interpret his experiences after inhaling Esketamine, which helped him to express his thoughts and emotions. This form of journaling, supported by the nurse’s empathy, created an integrative therapeutic approach that strengthened the patient-nurse relationship and enhanced the therapeutic process. AI productions also facilitated supportive discussions through storytelling, which, in this case, was broadly an act of sharing experiences and ideas with the nurse, which contributed to helping the patient organize his thoughts and process emotions and personal experiences (37). The patient also shared his AI-generated images with his partner and friends, which may have further enhanced his emotional processing and experiences of belonging.
This patient’s adjunction of ChatGPT’s images and interpretation to monitor his experiences during intranasal Esketamine treatment aligns with current practices that currently investigate real-time monitoring and predictive analytics, precision medicine, and personalized treatment, as well as the role of ChatGPT in telemedicine (38). However, AI is a double-edged sword when growing from personal to medical fields and integrating AI technologies into medical research poses significant ethical challenges. AI systems may compromise patient data privacy and confidentiality, perpetuate biases if trained on non-diverse or nonrepresentative datasets, obscure accountability due to the opacity of AI models, and produce unreliable outputs that could mislead researchers and clinicians (39, 40). ChatGPT-4 is also used as a tool in the medical publication landscape. Experts emphasized human corrections to the analysis produced by this AI tool (41).
This study presents some limitations. In this study, only the primary outcome (depression) was regularly assessed. The lack of measures of anxiety to objectively assess how anxiety evolved during the treatment, as well as the lack of measures of dissociation (42) within sessions that would have informed the severity of dissociation. These data, along with the data on the severity of depression and the measure of long-term follow-up, would have brought a more thorough picture of the process. Finally, one limitation of case report study designs is the impossibility of attributing the treatment’s efficacy to one of the interventions or the combination of both. Symptomatic improvement in depression may result from antidepressants (biological effects), nursing support (emotional stability), or journaling (cognitive processing). However, their effects likely interact. A randomized controlled trial (2x2x2 factorial) is the best procedure to determine whether antidepressant treatment, nursing support, or journaling independently contribute to symptomatic improvement in depression. If similar improvements occur across intervention groups, psychosocial factors or the placebo effect may be more influential than medication. The best outcomes may come from combining biological, psychological, and social interventions rather than relying on a single factor. Moreover, single-case studies have limited generalizability, lack control groups, and may be influenced by bias or individual variability. They make it difficult to establish causation, requiring cautious interpretation and validation through larger studies. Given these limitations, conclusions should be drawn cautiously, avoiding overinterpretation based on limited data. Further research is needed to ascertain the enhanced effectiveness of combining intranasal Esketamine and ChatGPT on the outcome.
This case report indicates that intranasal Esketamine can be combined with AI to document ongoing experiences of dissociation and enhance the therapeutic process. This case report provides insights into the potential effectiveness of merging these two innovative approaches in treating individuals with treatment-resistant depression. Both intranasal Esketamine and AI are readily available resources, and their combination could prove cost-effective in the long run. The presence of a nurse can consist of supporting this journaling process, which might otherwise be limited or misdirected. The individual contributions of each component, as well as their interactions, necessitate further investigation. These multimodal treatments are vital in complex or severe mental health conditions, where tailored and collaborative approaches can improve outcomes. Additional research is needed to establish the broader applicability of the findings from this specific case.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author/s.
Ethics statement
In accordance with national regulations, ethics committee approval is generally not required for case reports in Switzerland, including in the canton of Geneva, as such reports do not fall under the scope of "research involving human subjects" as defined by the Swiss Human Research Act (HRA). The Commission cantonale d’éthique de la recherche (CCER) in Geneva adheres to this legal framework and has clarified that ethics review is not necessary for case reports that describe an individual’s clinical course for educational or illustrative purposes and do not constitute systematic research, as is the case here. Nevertheless, the protection of patient privacy and confidentiality remains paramount. Written informed consent was obtained from the participant for the publication of this case report.
Author contributions
AF: Data curation, Formal Analysis, Investigation, Project administration, Writing – review & editing. SF: Methodology, Writing – original draft. HR-L: Conceptualization, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. Open access funding by University of Geneva.
Conflict of interest
The authors declare that the research was conducted without any commercial or financial relationships that could potentially create a conflict of interest.
Generative AI statement
The author(s) declare that Generative AI was used in the creation of this manuscript. Generative AI was used to create Figure 1.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. d’Andrea G, Miuli A, Pettorruso M, Cavallotto C, Marrangone C, Alessio C, et al. Exploring vortioxetine combination with intranasal esketamine: A feasible alternative to SSRI/SNRI? - Insights from the REAL-ESK study. J Affect Disord. (2024) 367:583–8. doi: 10.1016/j.jad.2024.09.004
2. Sapkota A, Khurshid H, Qureshi IA, Jahan N, Went TR, Sultan W, et al. Efficacy and safety of intranasal esketamine in treatment-resistant depression in adults: A systematic review. Cureus. (2021) 13:e17352. doi: 10.7759/cureus.17352
3. Chiappini S, Guirguis A, Schifano N, Corkery JM, Semeraro F, Mosca A, et al. Comparative safety of prescribed Esketamine and ketamine in relation to renal and urinary disorders: A pharmacovigilance perspective. Prog Neuropsychopharmacol Biol Psychiatry. (2024) 136:111213. doi: 10.1016/j.pnpbp.2024.111213
4. Lima TM, Visacri MB, and Aguiar PM. Use of ketamine and esketamine for depression: an overview of systematic reviews with meta-analyses. Eur J Clin Pharmacol. (2022) 78:311–38. doi: 10.1007/s00228-021-03216-8
5. Rosso G, d’Andrea G, Barlati S, Di Nicola M, Andriola I, Marcatili M, et al. Esketamine treatment trajectory of patients with treatment-resistant depression in the mid and long-term run: data from REAL-ESK study group. Curr Neuropharmacol. (2024) 23(5):612–9. doi: 10.2174/011570159X337670241029062524
6. Seshadri A, Prokop LJ, and Singh B. Efficacy of intravenous ketamine and intranasal esketamine with dose escalation for Major depression: A systematic review and meta-analysis. J Affect Disord. (2024) 356:379–84. doi: 10.1016/j.jad.2024.03.137
7. Capuzzi E, Caldiroli A, Capellazzi M, Tagliabue I, Marcatili M, Colmegna F, et al. Long-term efficacy of intranasal esketamine in treatment-resistant major depression: A systematic review. Int J Mol Sci. (2021) 22:9338. doi: 10.3390/ijms22179338
8. Ballentine G, Friedman SF, and Bzdok D. Trips and neurotransmitters: Discovering principled patterns across 6850 hallucinogenic experiences. Sci Adv. (2022) 8:eabl6989. doi: 10.1126/sciadv.abl6989
9. Breeksema JJ, Niemeijer AR, Krediet E, Vermetten E, and Schoevers RA. Psychedelic treatments for psychiatric disorders: A systematic review and thematic synthesis of patient experiences in qualitative studies. CNS Drugs. (2020) 34:925–46. doi: 10.1007/s40263-020-00748-y
10. Jacobson NC and Nemesure MD. Using artificial intelligence to predict change in depression and anxiety symptoms in a digital intervention: evidence from a transdiagnostic randomized controlled trial. Psychiatry Res. (2021) 295:113618. doi: 10.1016/j.psychres.2020.113618
11. Sarasso P, Billeci M, Ronga I, Raffone F, Martiadis V, and Di Petta G. Disembodiment and affective resonances in esketamine treatment of depersonalized depression subtype: two case studies. Psychopathology. (2024) 57:480–91. doi: 10.1159/000539714
12. Di Vincenzo M, Martiadis V, Della Rocca B, Arsenio E, D’Arpa A, Volpicelli A, et al. Facts and myths about use of esketamine for treatment-resistant depression: a narrative clinical review. Front Psychiatry. (2024) 15:1394787. doi: 10.3389/fpsyt.2024.1394787
13. Chatterjee S, Mishra J, Sundram F, and Roop P. Towards personalised mood prediction and explanation for depression from biophysical data. Sensors (Basel Switzerland). (2023) 24:164. doi: 10.3390/s24010164
14. Abd-Alrazaq A, AlSaad R, Aziz S, Ahmed A, Denecke K, Househ M, et al. Wearable artificial intelligence for anxiety and depression: scoping review. J Med Internet Res. (2023) 25:e42672. doi: 10.2196/42672
15. Park Y, Park S, and Lee M. Effectiveness of artificial intelligence in detecting and managing depressive disorders: Systematic review. J Affect Disord. (2024) 361:445–56. doi: 10.1016/j.jad.2024.06.035
16. Saber AF, Ahmed SK, Hussein S, and Qurbani K. Artificial intelligence-assisted nursing interventions in psychiatry for oral cancer patients: A concise narrative review. Oral Oncol Rep. (2024) 10:100343. doi: 10.1016/j.oor.2024.100343
17. Grosshans M, Paul T, Fischer SKM, Lotzmann N, List H, Haag C, et al. Conversation-based AI for anxiety disorders might lower the threshold for traditional medical assistance: a case report. Front Public Health. (2024) 12:1399702. doi: 10.3389/fpubh.2024.1399702
18. Saeidnia HR. Ethical artificial intelligence (AI): confronting bias and discrimination in the library and information industry. Library Hi Tech News. (2023) 40:1–5. doi: 10.1108/LHTN-10-2023-0182
19. Pettorruso M, Guidotti R, d’Andrea G, De Risio L, D’Andrea A, Chiappini S, et al. Predicting outcome with Intranasal Esketamine treatment: A machine-learning, three-month study in Treatment-Resistant Depression (ESK-LEARNING). Psychiatry Res. (2023) 327:115378. doi: 10.1016/j.psychres.2023.115378
20. Hu C, Lin Z, Zhang N, and Ji LJ. AI-empowered imagery writing: integrating AI-generated imagery into digital mental health service. Front Psychiatry. (2024) 15:1434172. doi: 10.3389/fpsyt.2024.1434172
21. OpenAI. ChatGPT (2023). Available online at: https://chat.openai.com/chat (Accessed March 14, 2023).
22. Fleisig S, Ayyad M, and Al-Sawalmih M. “Linguistic bias in ChatGPT: Language models reinforce dialect discrimination”. In: Proceedings of the 2023 Conference on Empirical Methods in Natural Language Processing (EMNLP). Philadelphia, PA, USA: Association for Computational Linguistics. (2023).
23. Riley DS, Barber MS, Kienle GS, Aronson JK, von Schoen-Angerer T, Tugwell P, et al. CARE guidelines for case reports: Explanation and elaboration document. J Clin Epidemiol. (2017) 89:218–35. doi: 10.1016/j.jclinepi.2017.04.026
24. Rush AJ, Gullion CM, Basco MR, Jarrett RB, and Trivedi MH. The inventory of depressive symptomatology (IDS): psychometric properties. psychol Med. (1996) 26:477–86. doi: 10.1017/S0033291700035558
25. Thase ME and Rush AJ. When at first you don’t succeed: Sequential strategies for antidepressant nonresponders. J Clin Psychiatry. (1997) 58:23–9.
26. Bagby RM, Ryder AG, Schuller DR, and Marshall MB. The Hamilton Depression Rating Scale: Has the gold standard become a lead weight? Am J Psychiatry. (2004) 161:2163–77. doi: 10.1176/appi.ajp.161.12.2163
27. Montgomery SA and Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. (1979) 134:382–9. doi: 10.1192/bjp.134.4.382
28. Bondolfi G, Jermann F, Rouget BW, Gex-Fabry M, McQuillan A, Dupont-Willemin A, et al. Self- and clinician-rated Montgomery-Asberg Depression Rating Scale: evaluation in clinical practice. J Affect Disord. (2010) 121:268–72. doi: 10.1016/j.jad.2009.06.037
29. Canadian Agency for Drugs and Technologies in Health. Aripiprazole (Abilify): depression, major depressive disorder (MDD). In: APPENDIX 5, VALIDITY OF OUTCOME MEASURES. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health (CADTH) (2016). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK409740/.
30. Li W, He Y, Xia L, Yang X, Liu F, Ma J, et al. Association of age-related trends in blood pressure and body composition indices in healthy adults. Front Physiol. (2018) 9:1574. doi: 10.3389/fphys.2018.01574
31. Bahr R, Lopez A, and Rey JA. Intranasal esketamine (Spravato™) for use in treatment-resistant depression in conjunction with an oral antidepressant. P T: peer-reviewed J formulary Manage. (2019) 44:340–75.
32. International Classification of Diseases. Eleventh revision (ICD-11). Geneva, Switzerland: World Health Organization (2018). Available online at: https://icd.who.int/browse11 (Accessed February 18, 2024).
33. Mercado-Rodríguez A, Martín Requena C, Cano Baena A, Zorrilla Martínez I, González-Pinto Arrillaga A, and Mar-Barrutia L. Effectiveness and tolerability of intranasal esketamine in treatment-resistant depression: report of two clinical cases. Eur Psychiatry. (2023) 19:S824. doi: 10.1192/j.eurpsy.2023.1745
34. National Cancer Institute. Common terminology criteria for adverse events (CTCAE) version 5.0. Bethesda, MD, USA: U.S. Department of Health and Human Services, National Institutes of Health (2017). Available online at: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm (Accessed February 18, 2024).
35. Vendrell-Serres J, Soto-Angona Ó, Rodríguez-Urrutia A, Inzoli B, González AL, and Ramos-Quiroga JA. Treating treatment-resistant depression with esketamine nasal spray when all therapeutic options have been exhausted: clinical experience from a spanish cohort of expanded use. Clin Psychopharmacol neuroscience: Off Sci J Korean Coll Neuropsychopharmacol. (2024) 22:159–68. doi: 10.9758/cpn.23.1097
36. Strawn JR, Mills JA, Suresh V, Mayes T, Gentry MT, Trivedi M, et al. The impact of age on antidepressant response: A mega-analysis of individuals with major depressive disorder. J Psychiatr Res. (2023) 159:266–73. doi: 10.1016/j.jpsychires.2023.01.043
37. Kautzky A, Bartova L, Fugger G, Dold M, Souery D, Montgomery S, et al. Age as a moderating factor of treatment resistance in depression. Eur Psychiatry. (2023) 66:e35, 1–9. doi: 10.1192/j.eurpsy.2023.17
38. Van der Kolk B. The body keeps the score: brain, mind, and body in the healing of trauma. New York, NY, USA: Viking Press (2014).
39. Liu J, Wang C, and Liu S. Utility of chatGPT in clinical practice. J Med Internet Res. (2023) 25:e48568. doi: 10.2196/48568
40. Yu S, Lee SS, and Hwang H. The ethics of using artificial intelligence in medical research. Kosin Med J. (2024) 39:229–37. doi: 10.7180/kmj.24.140
41. Gödde D, Nöhl S, Wolf C, Rupert Y, Rimkus L, Ehlers J, et al. A SWOT (Strengths, weaknesses, opportunities, and threats) analysis of chatGPT in the medical literature: concise review. J Med Internet Res. (2023) 25:e49368. doi: 10.2196/4936
Keywords: intranasal esketamine, artificial intelligence, treatment-resistant depression, case report, depression
Citation: Fraichot A, Favre S and Richard-Lepouriel H (2025) Case Report: Intranasal esketamine combined with a form of generative artificial intelligence in the management of treatment-resistant depression. Front. Psychiatry 16:1536232. doi: 10.3389/fpsyt.2025.1536232
Received: 28 November 2024; Accepted: 20 June 2025;
Published: 14 August 2025.
Edited by:
Vassilis Martiadis, Asl Napoli 1 Centro, ItalyReviewed by:
Davide Arillotta, University of Hertfordshire, United KingdomMaria Pepe, Agostino Gemelli University Polyclinic (IRCCS), Italy
Copyright © 2025 Fraichot, Favre and Richard-Lepouriel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandre Fraichot, YWxleGFuZHJlLmZyYWljaG90QGh1Zy5jaA==