 Sima Garmehi1
Sima Garmehi1 Bahareh Hakimi
Bahareh Hakimi Fateme Farhoudi
Fateme Farhoudi- 1Department of Psychiatry, School of Medicine, Imam Reza Hospital, North Khorasan University of Medical Sciences, Bojnourd, North Khorasan, Iran
- 2Psychiatry and Behavioral Sciences Research Center, Mazandaran University of Medical Sciences, Sari, Iran
- 3Psychiatry and Psychology Research Center, Tehran University of Medical Sciences, Tehran, Iran
- 4Research in Health Sciences, Research and Technology Vice-Chancellor, Mazandaran University of Medical Sciences, Sari, Iran
Background: Several instruments have been developed to measure stigma associated with mental disorders. The Reported and Intended Behaviour Scale (RIBS) is one of the validated questionnaires to assess the presence of stigma and discrimination against people with mental illness in the general population. It consists of eight items, divided into two subscales that measure reported and intended stigmatizing behaviours. This study aimed to translate and validate the RIBS in Persian.
Methods: We translated the RIBS questionnaire from English into Persian (RIBS-P) and back-translated it into English. Thereafter, ten psychiatrists evaluated its face validity. Between 2020 and 2021, 384 Persian-speaking adults (aged 18–60) residing in various cities across Iran, with internet access, participated in the study. Exploratory factor analyses were performed to determine the construct validity. The reliability of the questionnaire was assessed using internal consistency (Cronbach’s alpha coefficient) and test-retest methods.
Results: Most of the participants were 28-37 (53.9%), female (64.6%), married (51.6%), unemployed (67.7%) and educated (100%). The total Cronbach’s alpha coefficient for the RIBS-P questionnaire was high (0.732) and The test-retest results showed no significant difference. Factor analysis was used for construct validity and resulted in the extraction of one factor, the mean, standard deviation, and Cronbach’s alpha coefficient for the extracted factor were 3.25, 1.02 and 0.807. The items with the highest correlation with the extracted factor from the exploratory analysis were identified (>0.6). Age (0.00000010701), working status (0.00000010833), and education (0.00000010329) had a significant relationship with stigmatisation behaviour.
Conclusion: The findings indicate that the Persian version of the RIBS is valid and reliable for assessing stigmatizing behaviours among Iranians.
1 Introduction
Mental illness is one of the most common health problems in the world (1, 2). Although there are several treatments for psychiatric disorders, there is still a gap between getting sick and asking for help (3). Stigma seems to be one of the barriers to this gap (4, 5). Stigma was expressed as a universal term that includes ignorance, prejudice and discrimination (6). There are several types of mental health-related stigma, including self-stigma, public stigma, professional stigma and institutional stigma. (7–12). The stigma generally results from irrational generalizations, ignorance and fear of those who are different from others (13–15). Hayward and Bright investigated the root causes of stigma toward patients with mental illness and mentioned four public perceptions: 1) Fear of dangerousness, 2) Poor prognosis of mental illness, 3) Attribution of responsibility, and 4) Disruption of social interaction (16). People avoid psychiatric patients in public because they believe that they are dangerous, rare, untreatable, unpredictable and they are responsible for their condition. (17). These discriminatory behaviours cause a gap between the general public and mentally ill patients and create barriers to social interactions, access to help and overall well-being for these patients. By avoiding discriminatory behaviours, the general public can play an important role in the rehabilitation of patients with mental disorders through positive programs in social media, campaigns, and education. In this regard, international organizations such as the World Health Organization (WHO) and the United Nations (UN) strongly recommend systematic and multifaceted interventions to tackle stigma against people with mental illness (18, 19).
Various instruments have been developed to assess specific components of stigma, including the Discrimination and Stigma Scale (DISC) (20), the Inventory of Subjective Stigma Experiences (ISE) (21), and the Consumer Experiences of Stigma Questionnaire (CESQ) (22). In Iran many stigma-related scales were validated to evaluate the dimensions of stigma: OMSHC questionnaire (23), Social distance items(SDI), Perceived dangerousness of mental patient items(PDMPI) (24), Community attitudes towards the mentally ill (CAMI) (25), Stigma of Suicide Scale (SOSS) (26).
The Reported and Intended Behaviour Scale (RIBS) is a valid questionnaire for analysing the existence of reported and intended stigmatizing behaviours against people with mental illness and this scale measures public stigma towards mentally ill patients. RIBS has been used in several local and national studies on stigma, particularly in the UK (27). Considering that the RIBS is a short and easy scale for assessing public behaviour against mentally ill patients and it can estimate stigmatizing behaviour in future (27) and due to the lack of scales for measuring discriminatory behaviours in present and estimating this behaviour in future in Iran, the main purpose of this study was to develop a Persian version of the RIBS questionnaire and to evaluate its validity and reliability. This study could provide a valid and reliable tool to evaluate the reported and intended stigmatizing behaviour among Persian language societies. Such an evaluation might lead to future programs aimed at reducing the public stigma against patients suffering from mental disorders.
2 Material and methods
2.1 Participants
We developed an online questionnaire and used convenience/accidental sampling to recruit. A total of 384 Persian-speaking adults (aged 18–60 years) residing in various cities across Iran, with internet access, participated in the study between 2020 and 2021. Exclusion criteria included low literacy levels and unwillingness to sign the consent form.
2.2 Ethical considerations
The study was reviewed and approved by the Ethical Committee of Mashhad University of Medical Sciences (Ethical code: IR.MAMS.MEDICAL.REC.1399.570). The participants provided their written informed consent to participate in this study.
2.3 Reported and Intended Behaviour Scale (RIBS)
This tool was developed by Dr (28) to assess stigma-related behaviour in the general public. The RIBS questionnaire compromises two subscales and a total of eight items. The first subscale, consisting of four items, focuses on reported behaviours (in present or past experiences) in the areas of living, working, living nearby, or having a relationship with a person who has a mental health problem. Each item scores 1 for “Yes” and 0 for “No” or “I do not know”; higher scores indicate more engagement with people with mental health disorders in the past or present. The second subscale, consisting of four items, evaluates the intention to interact with individuals who have mental health problems in the same areas of living, working, living nearby, or having a relationship with a person who has a mental health problem in the future. Participants score items in the second subscale on a 5-point Likert scale ranging from “Strongly Agree” to “Strongly Disagree”. The minimum score is 1 and the maximum is 5; higher scores indicate more stigmatised behaviour towards patients suffering from mental illnesses (29; Garcia et al., 2017).
2.4 Translation process and study design
First, permission to translate the questionnaire into Persian was obtained through emails from Dr. Sara Evans-Lacko. The RIBS questionnaire was translated into Persian (RIBS-P) by an expert fluent in both Persian and English. The Persian version was then back-translated into English by two psychiatrists with expertise in the English language, and the two English versions were compared for consistency. To evaluate the validity of the test, face validity was employed. The translated scale was reviewed by 10 psychiatrists, who provided feedback on whether each question of the scale was “simple”, “clear” and “relevant “by questions like: “Is the statement clear?”; “Do you think it could be rewritten more clearly?” and “Did you find it difficult to choose a suitable response for the statement? Necessary corrections were made based on their input.
Once the final version was prepared, the questionnaire, along with the filling instructions, was made available to participants via email and other social network platforms. All the participants were assigned the written formed consent with a questionnaire and send it picture to us. Finally, after receiving all the questionnaires, the validation process was conducted.
2.5 Reliability/validity and statistical methods
The validity of the RIBS-P was assessed by face validity and construct validity methods. Exploratory factor analysis was conducted to evaluate construct validity. The reliability of the questionnaire was determined through internal consistency (using Cronbach’s alpha coefficient) and test-retest methods. To apply the test-retest method, 30 participants completed the questionnaire two weeks apart. Data analysis was performed using SPSS 17 and Amos 16 software.
3 Results
3.1 Demographic characteristics
Most participants were 28 to 37 years old (53.9%), 64.6% participants were female and 35.4% were male. Additionally, 51.6% were married and 48.4% were single. A majority (67.7%) of the participants were unemployed. Most participants had a high level of education: (9.2%) had a Diploma, (7.2%) had an Associate degree, (26.8%) had a Bachelor’s degree and (37.2%) had a Doctoral degree (Table 1).
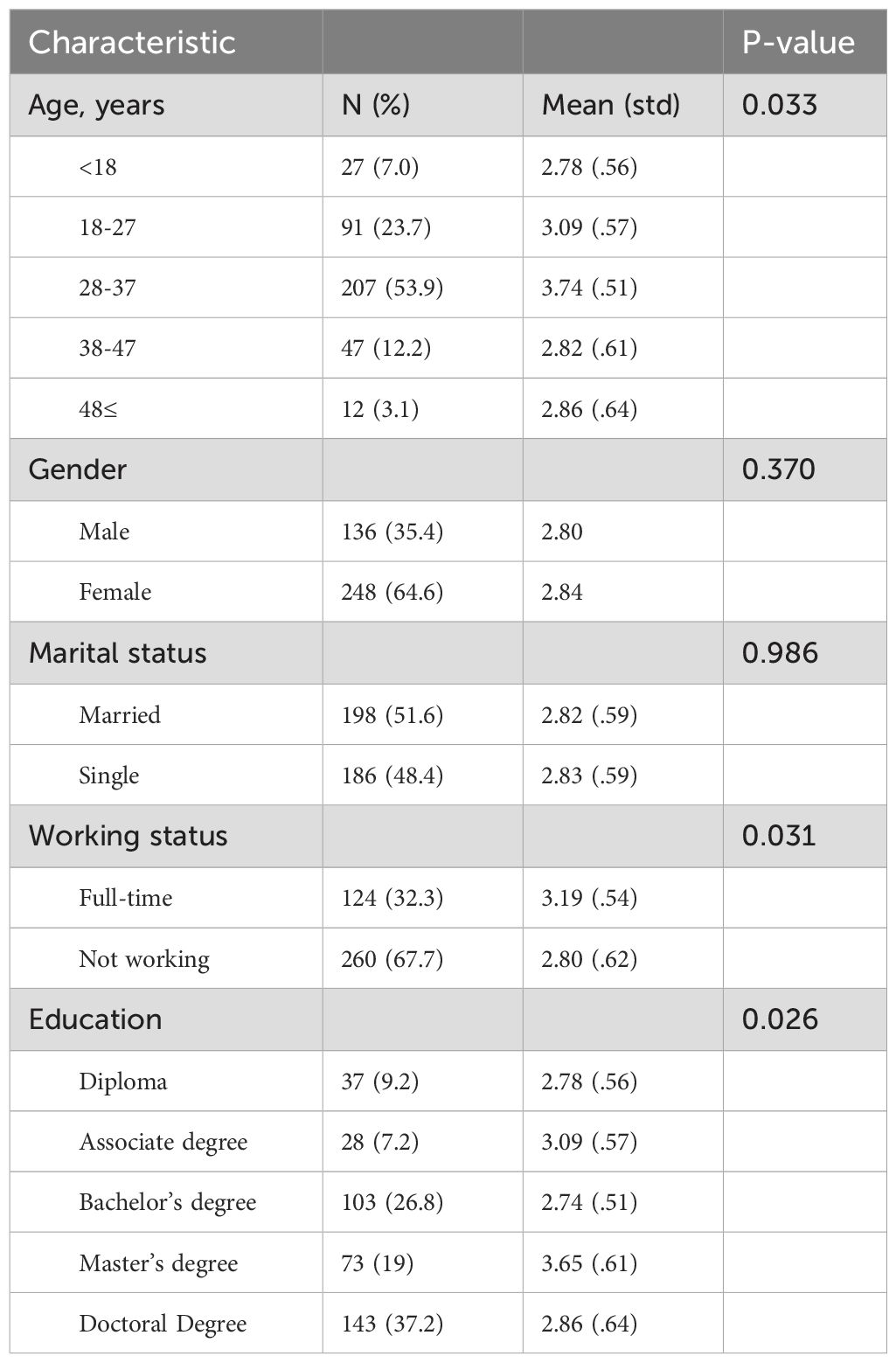
Table 1. Participant characteristics.
3.2 RIBS-P response frequencies
Table 2 shows the distribution of scores for RIBS-P items in the “reported behaviours” and “intended behaviours” subscales. Responses to the “reported behaviours” subscale indicate moderate contact with individuals with mental illness, ranging from 42.7% to 53.4%. In the “intended behaviours” subscale, most participants strongly disagreed with the statements, with 55.5% unwillingness to live with, 43.8% unwilling to work with, and 44.8% unwilling to live near someone with a mental health problem. Interestingly, 33.1% of responses to the item “willingness to continue a relationship with a friend who developed mental health problems” shifted towards agreement.
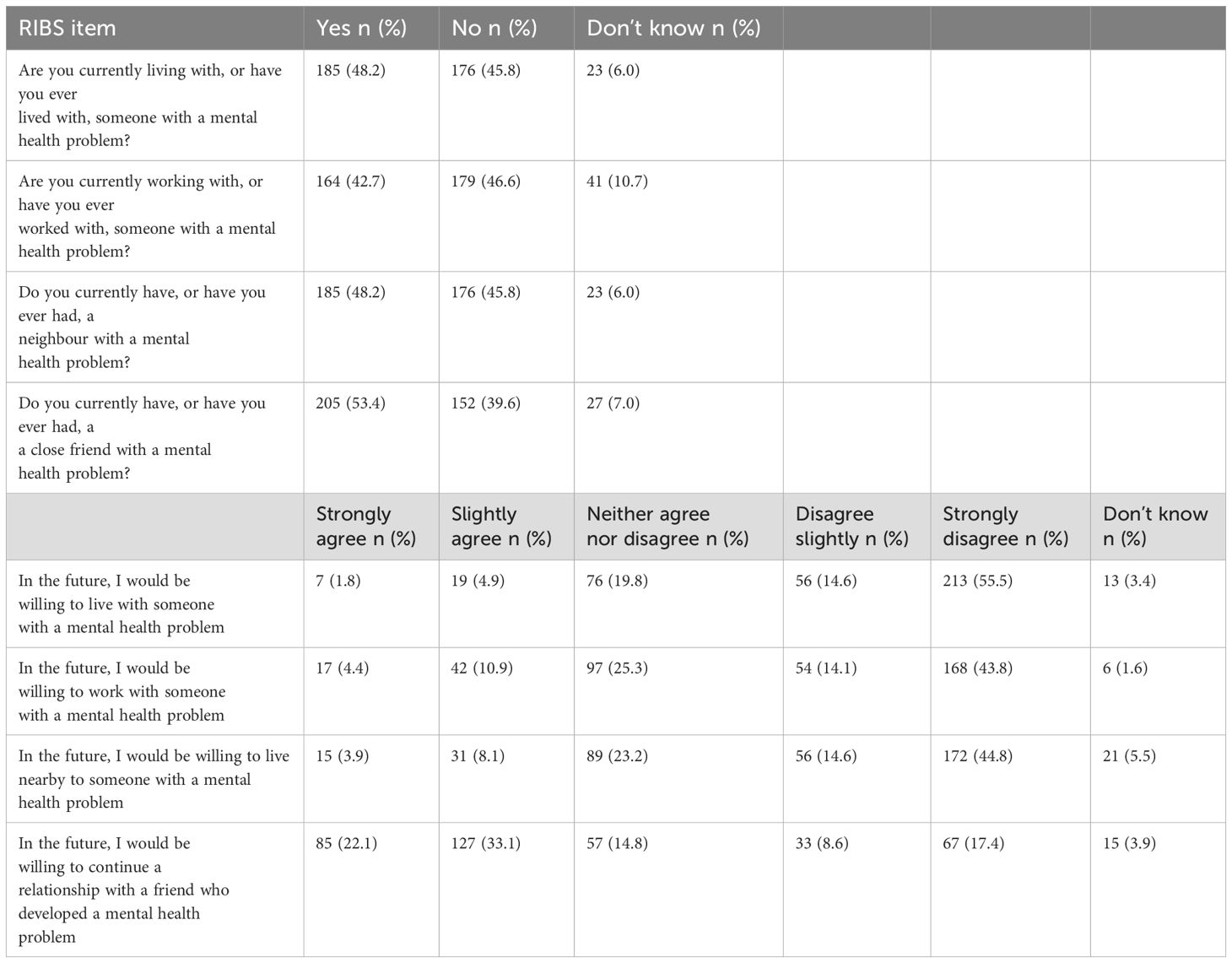
Table 2. Response frequencies (N = 384).
3.3 Validity assessment
The results demonstrated that the Kaiser-Mayer-Olkin (KMO) index was 0.778 (>0.6), indicating that the data were adequate for factor analysis. Additionally, the significance level of Bartlett’s test of sphericity was less than 5%, suggesting that exploratory factor analysis is appropriate for finding factors and that the data correlation matrix in the community is not zero (Table 3). Principal component analysis was conducted using the Varimax rotation method. Several experimental rotations were performed to explain the most appropriate factors. Ultimately, based on the slope of the Scree plot diagram, one factor with an Eigenvalue higher than 1 was identified. A single factor was accepted, explaining 65.526% of the total variance, because of the structure validity analysis (Table 4 and Figure 1). The results of repeated exploratory analysis showed that the common values of the research variables (questions) were higher than 0.5 indicating optimal values (Table 5). The mean, standard deviation, and Cronbach’s alpha coefficient for the extracted factor were 3.25, 1.02 and 0.807, respectively (Table 6). According to Table 7, the items with the highest correlation with the extracted factor from the exploratory analysis were identified (>0.6).
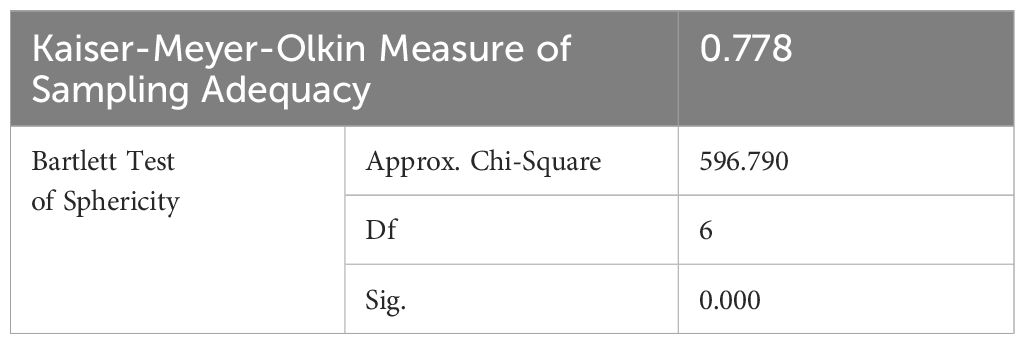
Table 3. KMO and Bartlett’s tests.
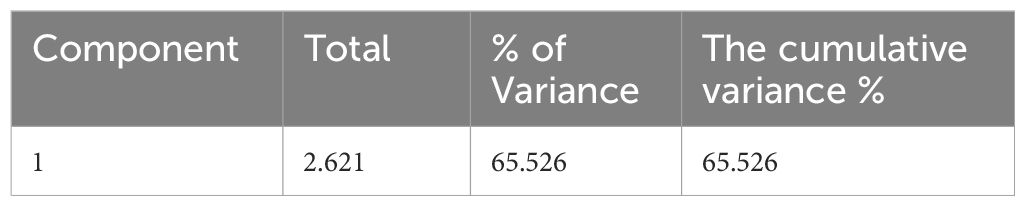
Table 4. Total variance explained.
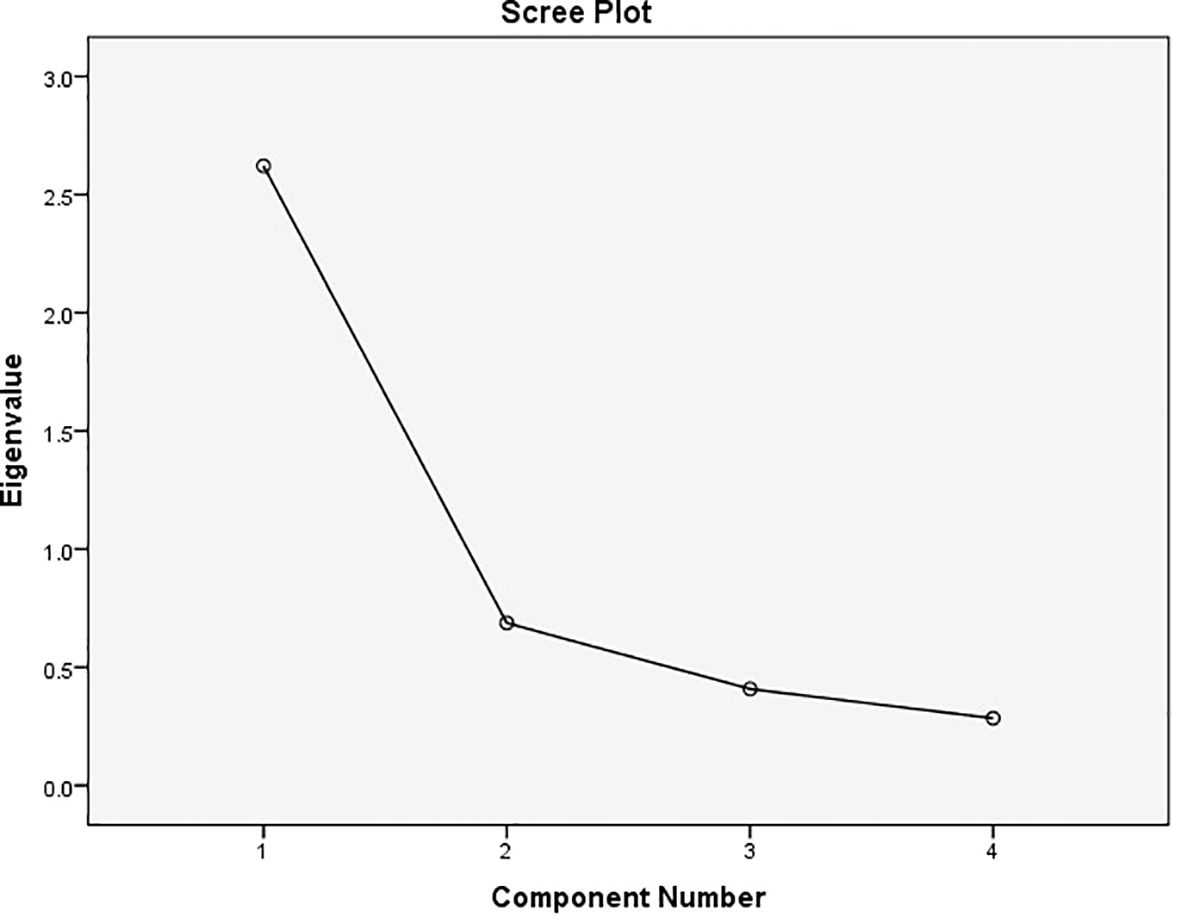
Figure 1. Domain slope diagram of test variables.
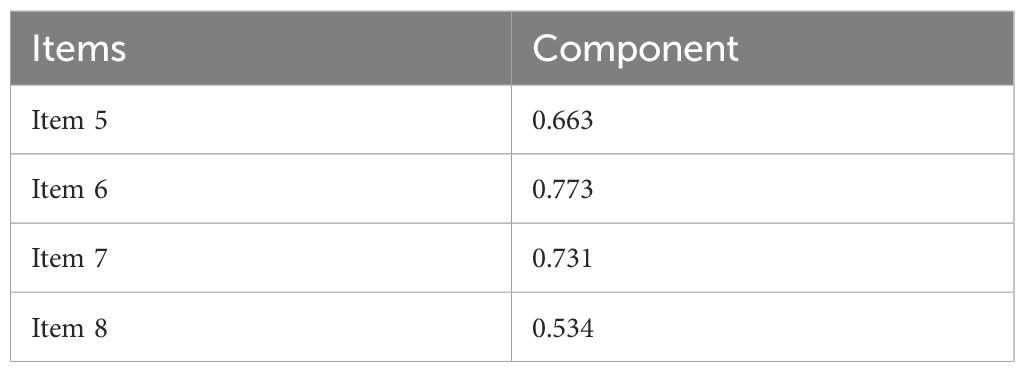
Table 5. Component matrix.
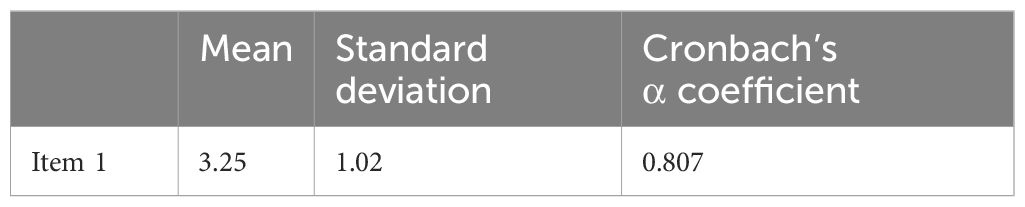
Table 6. Mean, standard deviation and Cronbach’s α coefficient of factor derived from exploratory analysis.
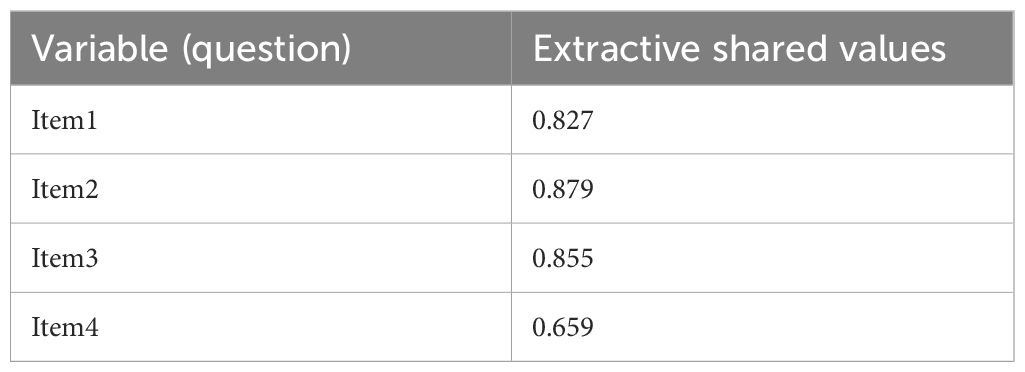
Table 7. Questions regarding each factor derived from exploratory analysis.
3.4 Reliability assessment
The reliability of the questionnaire was assessed using internal consistency (measured by Cronbach’s alpha coefficient) and the test-retest. The test-retest results showed no significant difference, confirming the reliability of the RIBS-P scale. The reliability of the RIBS-P scale was estimated to be 0.732 according to Cronbach’s alpha coefficient (Table 8).
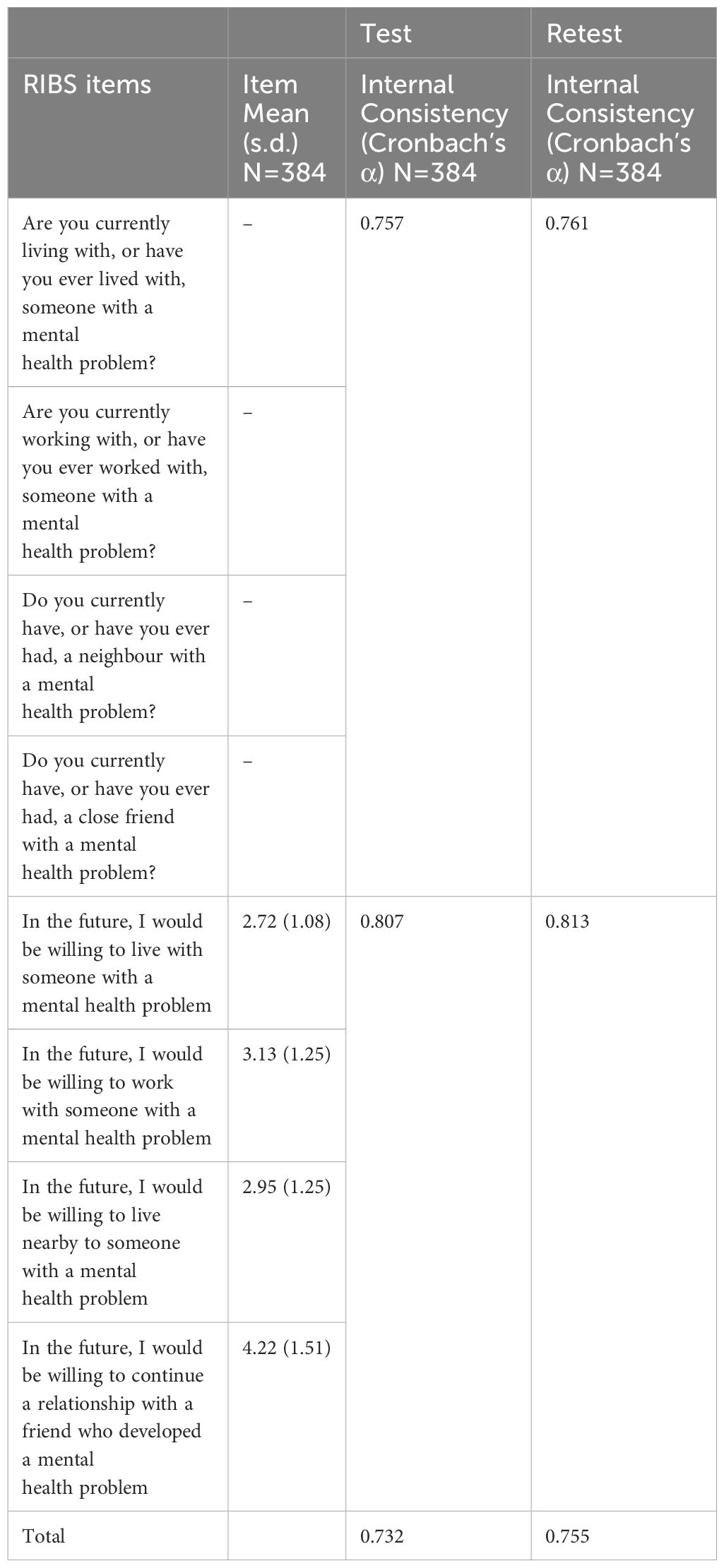
Table 8. Reliability of the RIBS.
4 Discussion
The present study was designed to evaluate the validity and reliability of the Persian version of the Reported and Intended Behaviour Scale (RIBS-P). Ten psychiatrists evaluated the face validity of the translated questionnaire, and all items of scale were accepted in RIBS-P without any modification. A sample of 384 adults completed it. After that, exploratory factor analyses were performed to determine the construct validity. The reliability of the questionnaire was assessed using internal consistency (Cronbach’s alpha coefficient) and test-retest methods.
The results of this study demonstrated a significant relationship between stigmatizing behaviours towards patients with mental illnesses with occupational status, age, and education (Table 9). In the Japanese version of RIBS, there was just a weak correlation between age and stigmatizing behaviours and more contact with mentally ill patients in the elderly could explain this correlation (29), In the Brazilian version of RIBS there was a high socioeconomic status with less intended stigmatisation behaviours (30). previous research has shown that the belief that mental health problems are a sign of weakness decreases with age, but the belief that mental health problems make a person dangerous and unpredictable increases with ageing (31). It has been demonstrated that early adolescents generally report more positive intended behaviours towards patients with mental illnesses (Mansfield, Humphrey and Patalay, 2020). The results of our study on the relationship between age and stigmatizing behaviours are consistent with other studies, as mentioned. In this study, education and employment were significantly associated with stigmatised behaviours. To explain this significance, we can mention the three dimensions of stigma: knowledge, behaviour, and attitude. Individuals with higher education or those who are employed tend to have greater knowledge about mental disorders. This increased knowledge may contribute to reducing stigmatised attitudes and behaviours among them (6, 32)
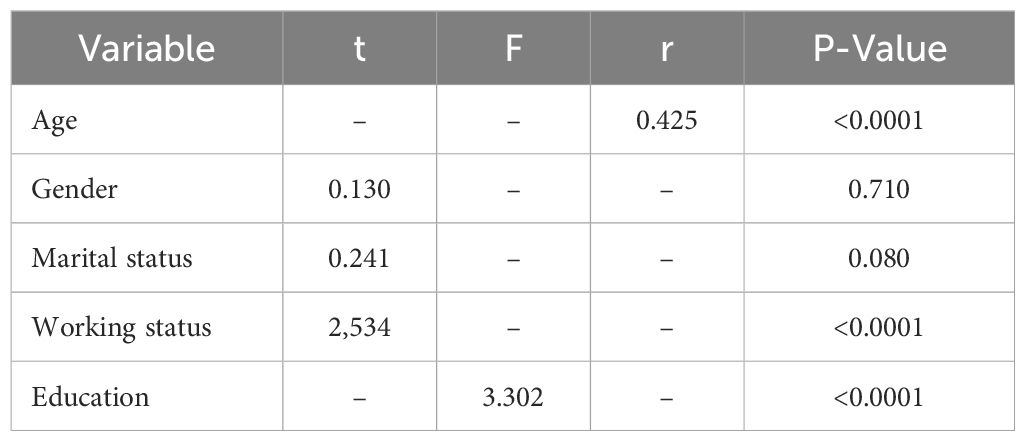
Table 9. Relationship between Stigma and demographic variables.
According to the results, Our sample of the Iranian population had a higher level of contact with people with mental disorders (42.7%-53.4%) compared to those in the United Kingdom (17.7%-32.5%), Italy (14.77%-27.07%), Japan (14.7%-39.7%) and the Czech Republic (12.7%-15.3%) (29; Winkler et al., 2015; 33). On the other hand, the Iranian population was less inclined to make contact with patients with mental illnesses in the future (slightly disagree + strongly disagree: 26%-70.1%) compared to the British population (agree + strongly agree: 55.9%-81.9%) (Winkler et al., 2015). This notable difference between the two items of the questionnaire in the Iranian population despite the British population can be attributed to the lack of structured programs to raise knowledge about mental disorders. This insufficient knowledge may lead to negative attitudes and beliefs, causing individuals to perceive those with mental health conditions as unsuitable for living, working, or forming friendships in the future. This observation strongly highlights the need for anti-stigma programs and campaigns (34–36). In contrast to other items, most of our participants (55.2%) were inclined to continue a relationship with a friend who developed a mental health problem in the future, which is consistent with the results of a study in Japan (29). Cultural similarity in Eastern countries and their collective and family-oriented lifestyles could explain this result and could act as a protective factor (37)
The Cronbach’s alpha coefficient for the reliability of the questionnaire was high (0.73). No significant differences were observed between test-retest results, confirming the reliability of the RIBS-P questionnaire. The internal consistency of the second RIBS-P subscale was high and satisfactory, exceeding the minimum threshold of 0.7 (α = 0.807) (38). In the study by Pingani et al. evaluating the validity and reliability of the Italian version of the RIBS questionnaire, the internal consistency of the second subscale was 0.83 (33). Similarly, Yamaguchi et al. (29) reported an internal consistency of 0.83 for the Japanese version of the questionnaire. The results of our study were consistent with these studies.
Our results indicated that the Kaiser-Meyer-Olkin (KMO) Sampling Adequacy Index was 0.778, exceeding the minimum threshold of 0.6, which suggests that the sample size was sufficient for factor analysis (39). Additionally, the significance level of Bartlett’s test of sphericity was less than 5% (40).
To determine the construct validity of the questionnaire, exploratory factor analysis was conducted. This analysis led to the extraction of a single factor, which accounted for 65.52% of the total variance of the test variables. The Cronbach’s alpha coefficient for the extraction factor was 0.807, indicating high reliability (>0.7). Each item demonstrated a strong correlation with the extracted factor, with a value exceeding 0.6.
So far, few studies have evaluated the validity and reliability of various versions of the RIBS questionnaire. Yamaguchi et al. and Pingani et al, employed confirmatory factor analysis to assess validity, with results indicating a good model fit (χ2 = 41.001, df = 19, P = 0.002 and χ2 = 23.60, df = 19, p = 0.21 respectively) (29, 33).
One limitation of the present study was the lack of control over the participants’ place of residence. Cultural differences between urban and rural areas could contribute to variations in attitudes and stigmatizing behaviour and we recommend future studies to address this gap. Additionally, the study could not objectively verify whether participants had a mental illness, which was intended as an exclusion criterion. This limitation may introduce biases in responses when completing the online questionnaire. Another limitation of our study was the predominance of highly educated participants, In future research, it is recommended to select a more varied sample population. In this study we didn’t assess criterion validity for the RIBS questionnaire and including such comparisons would strengthen the validity of the scale for future studies.
5 Conclusion
In this study, we tested the psychometric properties of the Persian version of the RIBS questionnaire. The results showed good internal consistency and reasonable test-retest reliability, consistent with findings from other studies. The construct validity assessment, including both exploratory factor analysis, was also found to be appropriate. Therefore, we consider the RIBS-P to be an appropriate and psychometrically robust scale for assessing stigmatizing attitudes and behaviours towards patients with mental health problems in Iranian society.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethical Committee of Mashhad University of Medical Sciences (Ethical code: IR.MAMS.MEDICAL.REC.1399.570). The patients/participants provided their written informed consent to participate in this study.
Author contributions
SG: Writing – review & editing. BH: Supervision, Writing – original draft. FF: Writing – original draft. EA: Formal Analysis, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
We would like to show our appreciation to Dr. Sara Evans Lakco for allowing us to translate the original RIBS into Persian.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Assembly. Global burden of mental disorders and the need for a comprehensive, coordinated response from health and social sectors at the country level: report by the Secretariat. Geneva: World Health Organization (2012). p. Provisional agenda item 13.2.
2. Tawiah PE, Adongo PB, Aikins M. Mental health-related stigma and discrimination in Ghana: experience of patients and their caregivers. Ghana Med J. (2015) 49:30–6. doi: 10.4314/gmj.v49i1.6
3. Patel V, Maj M, Flisher AJ, Silva De MJ, et al. Reducing the treatment gap for mental disorders:Geneva: a WPA survey. World Psychiatry. (2010) 9:169–76. doi: 10.1002/j.2051-5545.2010.tb00305.x
4. Sartorius N, Schulze H. Reducing the Stigma of Mental Illness: A Report from a Global Association. Cambridge: Cambridge University Press (2005). doi: 10.1017/CBO9780511544255
5. Girma E, Tesfaye M. Patterns of treatment seeking behavior for mental illnesses in Southwest Ethiopia: a hospital based study. BMC Psychiatry. (2011) 11:138. doi: 10.1186/1471-244X-11-138
6. Thornicroft G, Diana R, Aliya K, Norman S. Stigma: ignorance, prejudice or discrimination? Br J Psychiatry (2007), 192–3. doi: 10.1192/bjp.bp.106.025791
7. Brohan E, Elgie R, Sartorius N, Thornicroft G, GAMIAN-Europe Study Group. Self-stigma, empowerment and perceived discrimination among people with schizophrenia in 14 European countries: The GAMIAN-Europe study. Schizophr Res. (2010) 122:232–8. doi: 10.1016/j.schres.2010.02.1065
8. Livingston JD, Boyd JE. Correlates and consequences of internalized stigma for people living with mental illness: A systematic review and meta-analysis. Soc Sci Med. (2010) 71:2150–61. doi: 10.1016/j.socscimed.2010.09.030
9. Ahmedani BK. Mental health stigma: society, individuals, and the profession. J Soc Work Values ethics. (2011) 8:41–416.
10. Corrigan PW, Powell KJ, Rüsch N. How does stigma affect work in people with serious mental illnesses? Psychiatr Rehabil J. (2012) 35(5):381–4. doi: 10.1037/h0094497
11. Livingston JD. Mental illness-related structural stigma: The downward spiral of systemic exclusion. Calgary, Alberta: Mental Health Commission of Canada. (2013). Available online at: https://www.mentalhealthcommission.ca.
12. Corrigan PW, Druss BG, Perlick DA. The impact of mental illness stigma on seeking and participating in mental health care. psychol Sci Public Interest. (2014) 15:37–70. doi: 10.1177/1529100614531398
13. Corrigan PW, Kleinlein P. The impact of mental illness stigma. In: On the stigma of mental illness: Practical strategies for research and social change. American Psychological Association, Washington, DC, US (2005). p. 11–44. doi: 10.1037/10887-001
14. Thornicroft G. Shunned: Discrimination against people with mental illness. London: Oxford university press Oxford (2006). doi: 10.1093/med/9780198570981.001.0001
15. Hochman K. Reducing the stigma of mental illness: A report from a global programme of the world psychiatric association. J Can Acad Child Adolesc Psychiatry. (2007) 16(1):38–9.
16. Hayward P, Bright JA. Stigma and mental illness: A review and critique. J Ment Health. (1997) 6:345–54. doi: 10.1080/09638239718671
17. Feldman DB, Crandall CS. Dimensions of mental illness stigma: what about mental illness causes social rejection? J Soc Clin Psychol. (2007) 26:137–54. doi: 10.1521/jscp.2007.26.2.137
18. World Health Organization. The World Health Report : 2001 : Mental health : new understanding, new hope. Geneva: World Health Organization (2001).
19. Thornicroft G, Brohan E, Kassam A, Lewis-Holmes E. Reducing stigma and discrimination: Candidate interventions. Int J Ment Health Syst. (2008) 2:3. doi: 10.1186/1752-4458-2-3
20. Thornicroft G, Brohan E, Rose D, Sartorius N, Leese M. Global pattern of experienced and anticipated discrimination against people with schizophrenia: a cross-sectional survey. The Lancet. (2009) 373(9661):408–15.
21. Schulze Beate, Stuart Heather, Riedel-Heller Steffi G. Das Inventar subjektiver Stigmaerfahrungen (ISE): ein neues Instrument zur quantitativen Erfassung subjektiven Stigmas. Psychiatrische Praxis. (2009) 36(08):e19–e27.
22. Mendonça L, Azeredo-Lopes S, Landeiro I, Grácio J, Gonçalves-Pereira M. Validation of the Portuguese version of the consumer experiences of stigma questionnaire (CESQ). European Psychiatry. (2017) 41(S1):s812–s813.
23. Vaghee S, Lotfabadi MK, Salarhaji A, Vaghei N, Hashemi BM. Comparing the effects of contact-based education and acceptance and commitment-based training on empathy toward mental illnesses among nursing students. Iranian J Psychiatry. (2018) 13:119.
24. Kermani FR, Mazinani R, Fadaei F, Dolatshahi B, Rahgozar M. Psychometric properties of the Persian version of Social Distance and Dangerousness scales to investigate stigma due to severe mental illness in Iran. Iranian J Psychiatry Clin Psychol. (2015) 21(3):254–61.
25. Kafami Z, Farhoudi F, Alimoradi M, Sangsefidi Z, Delshad N, Khadem-Rezaiyan M. Persian translation and validation of community attitudes toward the mentally ill scale: a tool for assessing social stigma about mental illness. Int Clin Psychopharmacol. (2023) 38:40–4.
26. Jafari A, Mokhtari AM, Moshki M, Rahmani F, Naddafi F, Nejatian M. Psychometric properties of the Persian short form of the Stigma of Suicide Scale. Front Psychiatry. (2024) 15:1394237. doi: 10.3389/fpsyt.2024.1394237
27. Evans-Lacko S, Rose D, Little K, Flach C, Rhydderch D, Henderson C, et al. Development and psychometric properties of the reported and intended behaviour scale (RIBS): a stigma-related behaviour measure. Epidemiol Psychiatr Sci. (2011) 20:263–71. doi: 10.1017/s2045796011000308
28. Evans-Lacko S, Little K, Meltzer H, Rose D, Rhydderch D, Henderson C, et al. Development and psychometric properties of the Mental Health Knowledge Schedule. Can J Psychiatry. (2010) 55:440–8. doi: 10.1177/070674371005500707
29. Yamaguchi S, Koike S, Watanabe K-i, Ando S. Development of a Japanese version of the Reported and Intended Behaviour Scale: Reliability and validity. Psychiatry Clin Neurosci. (2014) 68:448–55. doi: 10.1111/pcn.12151
30. Ribeiro WS, Gronholm PC, Silvestre de Paula C, Hoffmann MS, Rojas Vistorte AO, Zugman C, et al. Development and validation of the Brazilian portuguese version of the reported and intended behaviour scale (RIBS-BP). Stigma Health. (2021) 6:163. doi: 10.1037/sah0000224
31. Jorm AF, Wright A. Influences on young people’s stigmatising attitudes towards peers with mental disorders: national survey of young Australians and their parents. Br J psychiatry : J Ment Sci. (2008) 192:144–9. doi: 10.1192/bjp.bp.107.039404
32. Goffman E. Stigma: Notes on the management of spoiled identity. Simon and schuster.Garcia, C. et al., (2017) ‘French Translation and Validation of Three Scales Evaluating Stigma in Mental Health’. Front Psychiatry. (2009) 8:290. doi: 10.3389/fpsyt.2017.00290
33. Pingani L, Evans-Lacko S, Luciano M, Del Vecchio V, Ferrari S, Sampogna G, et al. Psychometric validation of the Italian version of the Reported and Intended Behaviour Scale (RIBS). Epidemiol Psychiatr Sci. (2016) 25:485–92. doi: 10.1017/S2045796015000633
34. Evans-Lacko S, London J, Japhet S, Rüsch N, Flach C, Corker E, et al. Mass social contact interventions and their effect on mental health related stigma and intended discrimination. BMC Public Health. (2012) 12:489. doi: 10.1186/1471-2458-12-489
35. Evans-Lacko S, Malcolm E, West K, Rose D, London J, Rüsch N, et al. Influence of Time to Change’s social marketing interventions on stigma in England 2009-2011. Br J Psychiatry Supplement. (2013) 55:s77–88. doi: 10.1192/bjp.bp.113.126672
36. Livingston JD, Tugwell A, Korf-Uzan K, Cianfrone M, Coniglio C. Evaluation of a campaign to improve awareness and attitudes of young people towards mental health issues. Soc Psychiatry Psychiatr Epidemiol. (2013) 48:965–73. doi: 10.1007/s00127-012-0617-3
37. Kaplan HI, Sadock BJ eds. Comprehensive textbook of psychiatry/VI (Vol. 2). Wiliams & Wilkins (2023).
38. Santos J, Tesfaye M, Froeschl G, Möller-Leimkühler AM, Müller N, Dehning S. Cronbach’s alpha: a tool for assessing the reliability of scales. The Journal of Extension (1999) 37(2):15.
39. Kaiser HF. An index of factorial simplicity. Psychometrika. (1974) 39:31–6. doi: 10.1007/BF02291575
40. Bartlett MS. A note on the multiplying factors for various χ2 approximations. J R Stat Society. Ser B (Methodological). (1954) 16:296–8. http://www.jstor.org/stable/2984057.
Keywords: behaviour, stigma, mental health, psychometric, Persian
Citation: Garmehi S, Hakimi B, Farhoudi F and Abedini E (2025) Evaluation of the reliability and validity of the Persian version of the Reported and Intended Behaviour Scale, a mental health stigma-related behaviour measure. Front. Psychiatry 16:1553002. doi: 10.3389/fpsyt.2025.1553002
Received: 15 January 2025; Accepted: 17 March 2025;
Published: 06 May 2025.
Edited by:
Mohammadreza Shalbafan, Iran University of Medical Sciences, IranReviewed by:
Aiyub Aiyub, Syiah Kuala University, IndonesiaAfsaneh Atashi, Islamic Azad University Central Tehran Branch, Iran
Rukhsar Omar, University of Raparin, Iraq
Copyright © 2025 Garmehi, Hakimi, Farhoudi and Abedini. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fateme Farhoudi, ZmF0ZW1lLmZhcmhvdWRpQGdtYWlsLmNvbQ==