 Johannes Heck1†‡Melanie Dubaschewski2‡Olaf Krause3,4†Stefan Bleich2†
Johannes Heck1†‡Melanie Dubaschewski2‡Olaf Krause3,4†Stefan Bleich2† Martin Schulze Westhoff2†Benjamin Krichevsky3†
Martin Schulze Westhoff2†Benjamin Krichevsky3† Alexander Glahn2
Alexander Glahn2 Sebastian Schröder2*†
Sebastian Schröder2*†- 1Institute for Clinical Pharmacology, Hannover Medical School, Hannover, Germany
- 2Department of Psychiatry, Social Psychiatry and Psychotherapy, Hannover Medical School, Hannover, Germany
- 3Institute for General Practice and Palliative Care, Hannover Medical School, Hannover, Germany
- 4Center for Medicine of the Elderly, DIAKOVERE Henriettenstift, Hannover, Germany
Purpose: This study investigates the medication knowledge of patients with substance use disorders (SUDs) treated at a psychiatric clinic in northern Germany, aiming to identify gaps in understanding and to enhance patient safety, particularly concerning ATC group A drugs.
Setting: The study was conducted in the Department of Psychiatry, Social Psychiatry, and Psychotherapy at Hannover Medical School, Germany.
Design: A cross-sectional, interview-based study using a convenience sample of 100 patients was conducted between March 2023 and April 2024.
Participants: The cohort included patients with SUDs who had been hospitalized for at least 72 hours, regularly took at least one medication in addition to withdrawal drugs, and who displayed no cognitive impairments. Participants had a median age of 46.5 years; 62% were male.
Intervention: Patients were interviewed using a customized questionnaire addressing knowledge of drug name, indication, dosage, and frequency of application. The questionnaire also assessed the sources of medication knowledge and patient opinions on their medication regimen.
Primary and secondary outcome measures: The primary outcome was the average medication knowledge score (range 0–6). Secondary measures included differences in knowledge across drug groups, sources of information, and demographic influences.
Results: The median medication knowledge score was 3.8 out of 6. Knowledge was significantly lower for ATC group A drugs compared to groups B, C, and N (p < 0.001). No significant differences were observed between men and women nor between age groups. Hospital physicians were the primary information source for 40% of patients. Most participants (84%) considered their medication regimen adequate.
Conclusion: Patients with SUDs demonstrated suboptimal medication knowledge, particularly regarding ATC group A drugs. Future strategies should prioritize patient education and enhanced physician engagement to improve understanding and adherence, ultimately fostering better therapeutic outcomes.
Introduction
Substance use accounts for 5.5% of the global burden of disease (1). The incidence of alcohol and drug use disorders is increasing internationally, although there are significant regional differences (2). In addition to social consequences such as stigma, people with substance-related addiction disorders face a range of somatic risks, including cardiovascular, liver and pancreatic diseases (3–6). In addition, psychiatric comorbidities, including anxiety disorders, depression and attention deficit hyperactivity disorder, are highly prevalent among people with substance use disorders (SUDs) (7–9). The presence of multiple diagnoses often requires pharmacotherapy, leading to frequent polypharmacy among people with substance use disorders (10, 11).
Polypharmacy is associated with a lack of knowledge about medications, which can lead to reduced adherence to treatment and suboptimal treatment outcomes, especially in chronic diseases (12–14).
Inadequate medication knowledge can lead to increased utilization of healthcare resources, including emergency department visits, underscoring the clinical importance of this issue (15, 16).
Patients’ ability to understand medication regimens and to use both prescription and over-the-counter medications safely and accurately are strongly influenced by their level of health literacy (17). Several studies suggest that people with substance use disorders typically have low health literacy (18, 19). These individuals are less likely to seek health care when indicated and often fail to adhere to health care recommendations (20). In addition, an association between low health literacy and poor medication adherence has been documented (21).
Despite its obvious clinical importance, patients’ knowledge of their medication is a poorly investigated topic. In fact, to our knowledge, there are no studies that assessed the knowledge of prescribed regular medications, such as withdrawal medications, in patients with various addiction disorders. In the present study, we therefore analyzed the medication knowledge of patients with substance use disorders treated in the psychiatric department of a university hospital in northern Germany. We investigated possible influences of age or gender on medication knowledge and whether patients’ medication knowledge differed between drug groups. This study aims to improve drug and patient safety in the field of addiction psychiatry.
Methods
Ethics approval
This study was approved by the Ethics Committee of Hannover Medical School (No. 10762_BO_K_2023) and adhered to the Declaration of Helsinki and its later amendments.
Study design
The study was designed as a cross-sectional, interview-based study. It was planned to enroll a convenience sample of 100 patients. For this purpose, patients undergoing a detoxification treatment at the Department of Psychiatry, Social Psychiatry, and Psychotherapy of Hannover Medical School between March 2023 and April 2024 were invited to participate in the study. In our clinic, the standard protocol for alcohol detoxification includes oxazepam to prevent alcohol withdrawal seizures, delirium, blood pressure dysregulation, and other withdrawal symptoms, as well as thiamine and a vitamin B complex to prevent Wernicke encephalopathy. Patients willing to participate in the study were informed about the aims of the study, and written informed consent was obtained. Subsequently, patients were screened for eligibility (see section “Eligibility Criteria”). Patients who met all eligibility criteria were interviewed by MD, using a questionnaire specifically adapted to this study (see section “Study questionnaire”). Patients were allowed to use their medication plan during the interview. Based on the median age of the study population (i.e., 46.5 years), we divided the patients into younger (≤ 46 years) and older age groups ≥ 47 years).
Study questionnaire
In order to address the research questions of this study, the questionnaire by Krause et al. (22) was adapted, excluding the questions on the rules for sick days. The questionnaire used in the present study is available as Supplementary Material 1 (English version) and Supplementary Material 2 (German version). The questionnaire was used by MD during the interviews and addressed the following medication-related topics: drug name; indication; dosage; and frequency of application.
These medication-related topics were investigated for each drug in the medication plans of the study participants. One point was achievable for the categories drug name and frequency of application, while up to two points were achievable for the categories indication and dosage. For each drug, the achieved points were summed up to yield the medication knowledge score (range 0-6, with higher scores indicating better medication knowledge). To allow for meaningful comparisons between patients taking different numbers of drugs, the medication knowledge scores of all drugs of a patient were summed up and subsequently divided by the number of drugs the patient was taking, yielding the average medication knowledge score (range 0-6, with higher scores indicating better medication knowledge). Detailed examples of patients’ responses and corresponding ratings can be found in the work by Krause et al. (22). For instance, a patient who answered that she took “Zoloft, against listlessness, one tablet in the morning” would achieve 4 out of 6 points for this drug (a perfect, 6-point answer in this example would have been: “Zoloft, against depression, one 50-mg tablet in the morning”). Correctness of answers was evaluated based on the medication plan from the Department of Psychiatry, Social Psychiatry and Psychotherapy.
In addition, patients’ opinion about their daily number of drugs was evaluated on a 5-point Likert scale: 1 = “too few”; 2 = “rather too few”; 3 = “adequate number”; 4 = “rather too many”; 5 = “too many”.
Finally, patients were asked who or what contributed most to their medication knowledge, using a predefined 9-item list of answer options (single choice): pharmacy; general practitioner; practicing specialist; hospital physician; partner/spouse, relatives, friends; television; the press, magazines; the Internet; or other.
Occupational position
Occupational positions were classified according to the system proposed by Blossfeld et al. (23). The original classification comprises 12 occupational categories that are homogeneous concerning education, vocational training, and occupational activities. For the purpose of this analysis, these categories were condensed into six groups: unemployed, unskilled (e.g., unskilled service personnel), skilled (e.g., skilled manual occupations such as glassblowers), specialists (e.g., semi-professions such as nurses), highly qualified positions (e.g., professions such as university professors), and others.
Eligibility criteria
Patients were eligible for enrollment in the study (i) if they were treated at the Department of Psychiatry, Social Psychiatry and Psychotherapy of Hannover Medical School between March 2023 and April 2024; (ii) if they suffered from a substance use disorder; (iii) if they had been regularly taking at least one drug in addition to withdrawal medication; (iv) if they had already been hospitalized for 72 hours and (v) if they did not show cognitive impairment in the clinical examination and were able to provide written informed consent.
Drug classification and calculation of standard drinks
With regard to our analyses, we differentiated between medication explicitly prescribed for inpatient detoxification treatment and regularly prescribed medication. Drugs were classified according to the Anatomical Therapeutic Chemical (ATC) Classification for Germany, version 2022 (24). For statistical analyses, first-level ATC codes were used.
The calculation of the amount of standard drinks was based on the definition of the World Health Organization (WHO). The WHO guideline regarding brief intervention for risky drinking defines a standard drink as 10 g of pure ethanol (25).
Statistical analyses
All statistical analyses were performed with IBM SPSS Statistics for Windows, version 28 (Armonk, New York, USA). Quantitative variables were tested for normal distribution with the Shapiro-Wilk test. Due to skewed distribution, quantitative variables are depicted as medians with interquartile ranges (IQRs). For quantitative variables, the Mann-Whitney U test or Kruskal-Wallis test was used to investigate potential differences between two groups or ≥ three groups, respectively. Categorical variables are reported as absolute and relative frequencies. Statistical significance was defined as a two-sided p-value < 0.05. The Bonferroni correction was applied to adjust p-values for multiple testing in pairwise comparisons within the Kruskal-Wallis test.
Results
Study population and interview characteristics
The study cohort comprised 100 participants with a median age of 46.5 years (IQR 37.8-54; range 20-66), of whom 62% were male (Table 1). Participants took a median of 6 medications daily (IQR 5-8; range 1-13). The most prevalent substance-related dependence disorders were alcohol use disorder (89%), cannabis use disorder (21%), and cocaine use disorder (14%). Additional psychiatric diagnoses included depression (53%), personality disorders (23%), and post-traumatic stress disorder (20%). The most common somatic conditions were arterial hypertension (26%), type 2 diabetes mellitus (8%), and chronic obstructive pulmonary disease (7%). Furthermore, 15% of the participants were under legal guardianship. In terms of employment status, 29% were unemployed. The median amount of alcohol consumed in our study population irrespective of the underlying diagnosis was 22 standard drinks per day (IQR 13.5-33.4; range 0-161). The median number of inpatient withdrawal treatments in the past was 4 (IQR 2-15; range 1-60). Three percent of patients used their medication plan as a source of support during the interview.
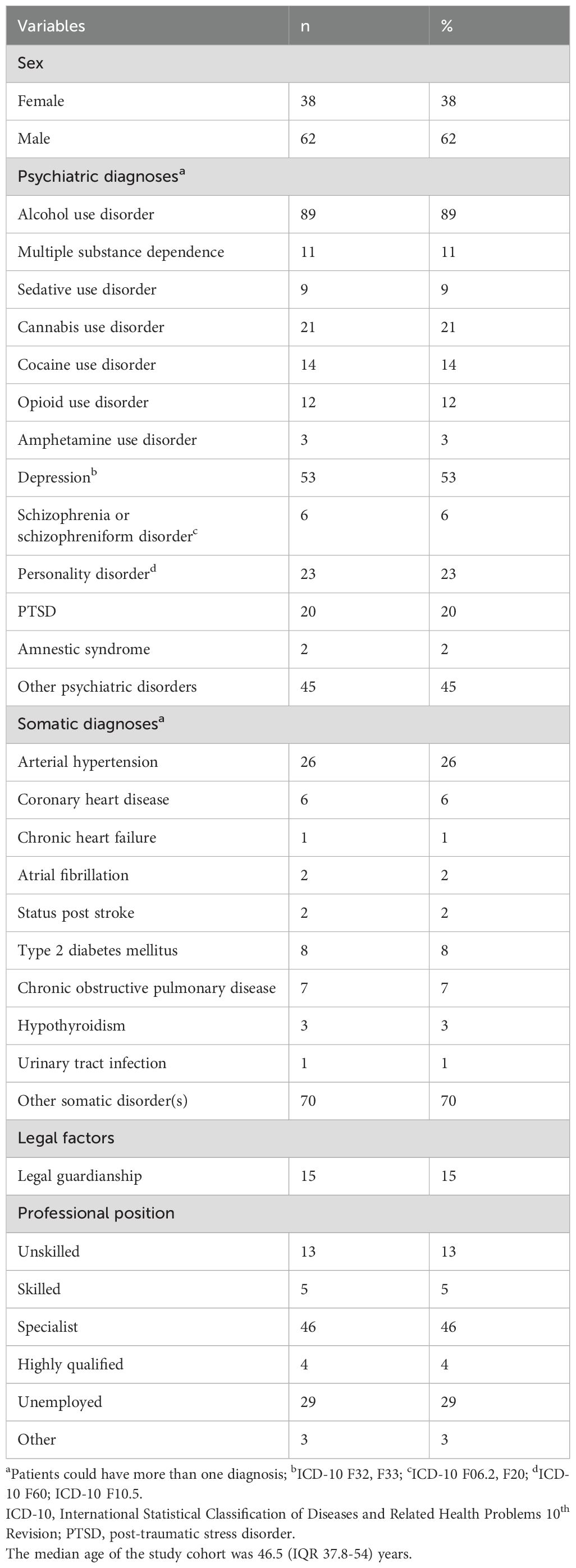
Table 1. Characteristics of the study population (n = 100).
Average medication knowledge score
The median average medication knowledge score among the study population was 3.8 (IQR 3-4.7; range 0.3-6.0). No statistically significant difference in overall medication knowledge was observed between men and women (median 3.8 (IQR 3-4.7) vs. median 3.7 (IQR 3-4.7); p = 0.679), nor between younger and older patients (median 3.9 (IQR 3.2-4.8) vs. median 3.7 (IQR 2.7-4.6); p = 0.230).
The median score for regular medication knowledge in the study population was significantly different from the median score for withdrawal medication (median 4.8 (IQR 3.6-5.7) vs. median 3.0 (IQR 1.7-4); p = < 0.001). Similarly, no statistically significant differences in regular medication knowledge were found between men and women (median 4.8 (IQR 3.5-5.9) vs. median 4.7 (IQR 3.3-5.4); p = 0.514), nor between younger and older patients (median 4.8 (IQR 3.8-5.7) vs. median 4.8 (IQR 3.1-5.7); p = 0.457).
For withdrawal medication knowledge, there were also no significant differences between men and women (median 3.3 (IQR 2-4.3) vs. median 3.3 (IQR 1.5-4.5); p = 0.858), nor between younger and older patients (median 3.6 (IQR 2.2-4.8) vs. median 3 (IQR 1.6-4); p = 0.418).
Comparison of drug groups
To investigate potential differences in patients’ medication knowledge across different drug groups, we compared the four most frequently used drug groups in the study population: ATC groups A (alimentary tract and metabolism), B (blood and blood-forming organs), C (cardiovascular system), and N (nervous system) (Table 2). The remaining drugs were categorized as “other”, and comprised ATC groups D (dermatologicals), G (genitourinary system and sex hormones), H (systemic hormonal preparations, excluding sex hormones and insulins), J (anti-infectives for systemic use), R (respiratory system), S (sensory organs), and V (various).
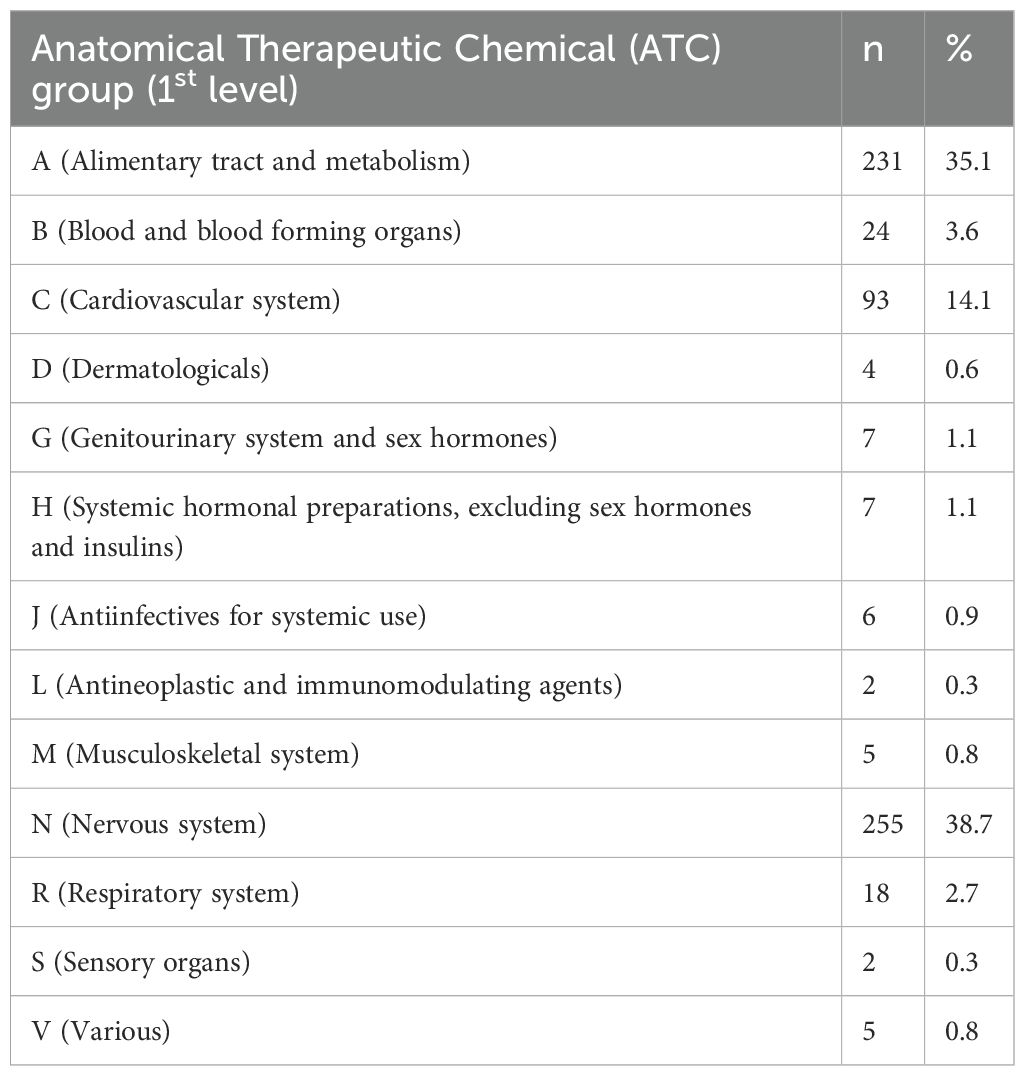
Table 2. Categorization of drugs (n = 659) taken by the study population according to the World Health Organization’s Anatomical Therapeutic Chemical (ATC) classification system.
Patients’ medication knowledge scores varied significantly between ATC groups A, B, C, N, and the group of “other” medications (global p < 0.001). Medication knowledge scores were significantly lower for ATC group A (median 3 (IQR 0-5)) when compared with ATC group B (median 6 (IQR 4.3-6); p < 0.001), C (median 5 (IQR 3-6); p = 0.005), and N (median 5 (IQR 4-6); p < 0.001) in pairwise comparisons.
Patients’ opinion about their daily number of drugs to take
More than four-fifths (84%) of the patients considered their daily number of drugs to take “adequate”, while 13% of the patients found that they had to take “rather too many” drugs per day.
Primary sources of medication knowledge
Forty percent of patients reported receiving most information about their medications directly from their hospital physicians. General practitioners were the second most common source (24%). A smaller portion of the patients (15%) sought information primarily on the Internet, while 14% were mainly informed by practicing specialists such as cardiologists or neurologists. Two percent of patients reported getting most of their information from their spouse or partner. Notably, pharmacies and medication package inserts each accounted for only 1%. None of the patients cited television programs, the press, or magazines as primary sources of information. Additionally, 3% of patients utilized “other” sources for their medication information, and upon further inquiry, all of these patients attributed their knowledge to their own professional expertise.
Discussion
This study analyzed the medication knowledge of patients with SUDs treated in the psychiatric department of a university hospital in Germany. Medication knowledge is a multidimensional construct for which there is no agreed definition in the literature (26). Furthermore, its operationalization has not yet been standardized, which makes it difficult to compare results (27). Patients’ knowledge of their medication is an under-researched topic. To our knowledge, no studies have investigated knowledge of prescribed medications in patients with SUDs to date. Our study population differed from previous studies in terms of age, gender, and comorbidity profiles. The median age of our study population was 46.5 years, with depression being the most common psychiatric diagnosis besides substance use disorders. The most prevalent substance-related dependence disorders were alcohol use disorder, cannabis use disorder, and cocaine use disorder.
Several previous studies investigated medication knowledge in geriatric patients and found mixed results for medication knowledge in older people (13, 15, 22, 28, 29). Krause et al., using the same methodology as in our study in a geriatric cohort, found an average median medication knowledge score of 5 (22), compared to 3.8 in our study. Their results also showed that women scored higher on medication knowledge than men, in contrast to our investigation in which we did not detect differences in women’s and men’s medication knowledge. Krause and colleagues demonstrated that patients under 80 years of age displayed higher medication knowledge than those over 80 years of age (22). This latter finding cannot be compared meaningfully to our investigation in which participants were considerably younger on average and the cut-off between “younger” and “older” patients was drawn between 46 and 47 years.
In a study by Najjar and colleagues, about four out of five older people recognized the name of the drug, while only 17% could name a side effect of the drug (13). Similarly, Chan et al. reported that 96% of patients were unable to report any possible side effects of the prescribed medication (15). Zwietering and colleagues stated that patients’ reported medication intake matched the number of medications listed in their medical records only about 30% of the time (29). Sancar et al. found that 54.8% of patients surveyed did not know why they were taking their medication and 60.3% did not know when or how to take their medication.
Numerous studies have investigated the knowledge of medication in various patient groups who were not explicitly suffering from a dependency disorder. Some studies suggest that poorer medication knowledge correlates with older age (30–32), a finding which we did not detect in our study. Marvanova et al. reported that lower cognitive function, lower health literacy and higher number of prescribed medications were associated with lower medication knowledge (33). In a cohort of primary care patients, Passagli et al. found that an increased number of comorbidities was associated with poorer medication knowledge (34). In their study, approximately 30% of the patients demonstrated insufficient knowledge regarding their medication (34). In contrast, a study of analgesic prescriptions by Timmerman et al. found that around 50% of participants lacked knowledge about at least one critical aspect of their prescription, such as the drug name, dosage or frequency of administration (35).
It might be speculated that patients undergoing qualified withdrawal treatment in our study generally had lower cognitive functions than patients who did not have an addiction disorder or were not undergoing acute treatment for it, and that this may have been the reason for the lower drug knowledge scores (36). Although we did not carry out extensive neuropsychological testing, cognitive impairment was ruled out as part of the clinical assessment for eligibility.
Strikingly, only 3% of participants in our study used their medication charts during the interview, compared with 95% in the study by Krause and colleagues (22). Freyer et al. found that the use of a medication chart was associated with better medication knowledge (32), which may explain the overall higher average medication knowledge score in the Krause et al. study (22) compared to our investigation.
Patients’ medication knowledge scores were significantly lower for ATC group A when compared to ATC groups B, C, and N. By contrast, in the abovementioned study by Passagli et al. among primary care patients, musculoskeletal drugs were associated with low medication knowledge (34). It is noteworthy that ATC group A includes primarily drugs prescribed during inpatient alcohol withdrawal treatment, such as thiamine, and patients’ knowledge about withdrawal medications was significantly lower compared to their knowledge about regular medication. Substitution of thiamine during withdrawal to prevent Wernicke’s encephalopathy is well-established clinical practice (37). More than four-fifths of the patients considered their daily number of drugs to take adequate, suggesting a high level of trust in prescribers, especially hospital physicians, who also contributed most to patients’ medication knowledge in our study.
In the present investigation, almost half of the patients (46%) were classified as specialists based on their professional position. Higher levels of education and income appear to correlate with better medication knowledge, as suggested by previous research (38, 39). On the other hand, 29% of patients in our cohort were unemployed. Problematic substance use not only increases the likelihood of unemployment, but also reduces the chances of obtaining and maintaining employment (40). Conversely, unemployment is a significant risk factor for harmful use of illicit drugs (40).
Remarkably, in the 21st century, 78% of participants in our study stated that doctors, including general practitioners and specialists, were the main source of their medication knowledge, rather than the media or the internet. In contrast, pharmacists did not appear to contribute to patients’ medication knowledge to a relevant degree in this study.
Although most of the other studies used different methods to assess medication knowledge, which limits direct comparability with our results, it is reasonable to assume that the average medication knowledge of 3.8 out of 6 in our study indicates room for improvement in patient education about medications, especially for ATC group A drugs. This is particularly important since Germany has one of the highest alcohol consumption rates in the world (41). In addition, in light of the recent legalization of cannabis in Germany (42), the potential increase in substance-related dependence requires vigilance (41). Meeting these challenges requires concerted efforts by all healthcare professionals to ensure appropriate pharmacotherapy and comprehensive care for patients with SUDs.
Strength and limitations
This study has several strengths. First, it addresses a significant gap in the literature by investigating medication knowledge among patients with SUDs, a population that faces unique healthcare challenges and frequent polypharmacy. The structured interview-based approach allowed for a detailed assessment of individual medication knowledge, including nuanced aspects such as drug names, indications, dosages, and administration frequency. Additionally, the study’s findings are clinically relevant, as they highlight specific deficits, particularly concerning ATC group A drugs, providing actionable insights for improving patient education and medication safety in addiction psychiatry. The inclusion of a diverse cohort with varying ages, comorbidities, and substance use patterns further enhances the applicability of the findings to similar clinical populations.
On the other hand, our study also has limitations. The monocentric design, conducted at a single university hospital in Germany, may reduce the generalizability of the results to other geographical or healthcare contexts. The relatively small sample size of 100 participants might have constrained the statistical power to detect more subtle subgroup differences. Additionally, 89% of the study participants suffered from alcohol use disorder, which limits the generalizability of the findings to other SUDs. Although the questionnaire was adapted from a previously used instrument, it was not formally validated for the specific population studied, which could negatively impact the reliability of the results (22).
In conclusion, our study has shown that there is still potential for improvement in the medication knowledge of patients with SUDs, particularly with regard to prescribed medications during qualified withdrawal treatment. Future studies should investigate whether there is a correlation between poor medication knowledge and worse therapeutic outcomes, possibly due to worse adherence to prescribed medicines.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of Hannover Medical School (No. 10762_BO_K_2023). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
JH: Conceptualization, Formal Analysis, Investigation, Methodology, Resources, Validation, Writing – original draft, Writing – review & editing. MD: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing. OK: Supervision, Writing – review & editing. SB: Supervision, Writing – review & editing. MSW: Supervision, Validation, Writing – review & editing. BK: Supervision, Writing – review & editing. AG: Supervision, Writing – review & editing. SS: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1556920/full#supplementary-material
Abbreviations
ATC, Anatomical Therapeutic Chemical; ICD-10, International Statistical Classification of Diseases and Related Health Problems 10th Revision; IQR, interquartile range; PTSD, post-traumatic stress disorder; SUD, substance use disorder; WHO, World Health Organization.
References
1. Degenhardt L, Charlson F, Ferrari A, Santomauro D, Erskine H, Mantilla-Herrara A, et al. The global burden of disease attributable to alcohol and drug use in 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Psychiatry. (2018). doi: 10.1016/S2215-0366(18)30337-7
2. The Lancet Psychiatry. The how and where of substance use in the USA. Lancet Psychiatry. (2023). doi: 10.1016/S2215-0366(23)00235-3
3. Hammarlund R, Crapanzano KA, Luce L, Mulligan L, Ward KM. Review of the effects of self-stigma and perceived social stigma on the treatment-seeking decisions of individuals with drug-and alcohol-use disorders. Subst Abuse Rehabil. (2018). doi: 10.2147/SAR.S183256
4. Parry CD, Patra J, Rehm J. Alcohol consumption and non-communicable diseases: epidemiology and policy implications. Addiction. (2011). doi: 10.1111/j.1360-0443.2011.03605.x
6. van Amsterdam J, Pennings E, Brunt T, van den Brink W. Physical harm due to chronic substance use. Regul Toxicol Pharmacol. (2013). doi: 10.1016/j.yrtph.2013.03.007
7. McHugh RK, Weiss RD. Alcohol use disorder and depressive disorders. Alcohol Res. (2019). doi: 10.35946/arcr.v40.1.01
8. Rohner H, Gaspar N, Philipsen A, Schulze M. Prevalence of attention deficit hyperactivity disorder (ADHD) among substance use disorder (SUD) populations: meta-analysis. Int J Environ Res Public Health. (2023). doi: 10.3390/ijerph20021275
9. Simon NM. Generalized anxiety disorder and psychiatric comorbidities such as depression, bipolar disorder, and substance abuse. J Clin Psychiatry. (2009). doi: 10.4088/jcp.s.7002.02
10. Ipser JC, Wilson D, Akindipe TO, Sager C, Stein DJ. Pharmacotherapy for anxiety and comorbid alcohol use disorders. Cochrane Database Syst Rev. (2015). doi: 10.1002/14651858.CD007505.pub2
11. Benz MB, Epstein-Lubow G, Weinstock LM, Gaudiano BA. Polypharmacy among patients with major depressive disorder and co-occurring substance use disorders in a psychiatric hospital setting: prevalence and risk factors. J Clin Psychopharmacol. (2023). doi: 10.1097/JCP.0000000000001681
12. Mekonnen GB, Gelayee DA. Low medication knowledge and adherence to oral chronic medications among patients attending community pharmacies: A cross-sectional study in a low-income country. BioMed Res Int. (2020). doi: 10.1155/2020/4392058
13. Najjar A, Amro Y, Kitaneh I, Abu-Sharar S, Sawalha M, Jamous A, et al. Knowledge and adherence to medications among palestinian geriatrics living with chronic diseases in the west bank and east jerusalem. PloS One. (2015). doi: 10.1371/journal.pone.0129240
14. Alsaedi R, McKeirnan K. Literature review of type 2 diabetes management and health literacy. Diabetes Spectr. (2021). doi: 10.2337/ds21-0014
15. Chan FW, Wong FY, So WY, Kung K, Wong CK. How much do elders with chronic conditions know about their medications? BMC Geriatr. (2013). doi: 10.1186/1471-2318-13-59
16. Hope CJ, Wu J, Tu W, Young J, Murray MD. Association of medication adherence, knowledge, and skills with emergency department visits by adults 50 years or older with congestive heart failure. Am J Health Syst Pharm. (2004). doi: 10.1093/ajhp/61.19.2043
17. Centers for Disease Control and Prevention. Health Literacy—Medications (2022). Available online at: https://www.cdc.gov/healthliteracy/researchevaluate/medications.html (Accessed May 17, 2023).
18. Rolová G, Barták M, Rogalewicz V, Gavurová B. Health literacy in people undergoing treatment for alcohol abuse - A pilot study. Kontakt. (2018). doi: 10.1016/j.kontakt.2018.09.003
19. Degan TJ, Kelly PJ, Robinson LD, Deane FP. Health literacy in substance use disorder treatment: A latent profile analysis. J Subst Abuse Treat. (2019). doi: 10.1016/j.jsat.2018.10.009
20. Weiss L, McCoy K, Kluger M, Finkelstein R. Access to and use of health care: perceptions and experiences among people who use heroin and cocaine. Addict Res Theory. (2004). doi: 10.1080/1606635031000155099
21. Ning JZ, Terry A, McHorney CA. Impact of health literacy on medication adherence. Ann Pharmacother. doi: 10.1177/1060028014526562
22. Krause O, Ziemann CT, Schulze Westhoff M, Schröder S, Krichevsky B, Greten S, et al. What do older patients know about their medication? A cross-sectional, interview-based pilot study. Eur J Clin Pharmacol. (2023). doi: 10.1007/s00228-023-03548-7
23. Blossfeld H. No title. Bildungsexpansion und Berufschancen: empirische Analysen zur Lage der Berufsanfänger in der Bundesrepublik. (1985).
24. Federal Institute for Drugs and Medical Devices. ATC-Classification (2022). Available online at: https://www.bfarm.de/EN/Code-systems/Classifications/ATC/_node.html (Accessed Dec 31, 2022).
25. Kalinowski A, Humphreys K. Governmental standard drink definitions and low-risk alcohol consumption guidelines in 37 countries. Addiction. (2016). doi: 10.1111/add.13341
26. Ramia E, Zeenny RM, Hallit S, Salameh P. Assessment of patients’ knowledge and practices regarding their medication use and risks in Lebanon. Int J Clin Pharm. (2017). doi: 10.1007/s11096-017-0517-4
27. Rubio JS, García-Delgado P, Iglésias-Ferreira P, Mateus-Santos H, Martínez-Martínez F. Measurement of patients’ knowledge of their medication in community pharmacies in Portugal. Cien Saude Colet. (2015). doi: 10.1590/1413-81232014201.20952013
28. Sancar M, Yalcin Mutlu B, Okuyan B, Vehbi Izzettin F. Determination of geriatric patients’ drug profile and identify their pharmaceutical care requirements by determining potential risk factors. Eur Geriatric Med. (2011). doi: 10.1016/j.eurger.2011.07.011
29. Zwietering NA, Westra D, Winkens B, Cremers H, van der Kuy PHM, Hurkens KP. Medication in older patients reviewed multiple ways (MORE) study. Int J Clin Pharm. (2019). doi: 10.1007/s11096-019-00879-3
30. Okuyan B, Sancar M, Izzettin FV. Assessment of medication knowledge and adherence among patients under oral chronic medication treatment in community pharmacy settings. Pharmacoepidemiol Drug Saf. (2013). doi: 10.1002/pds.3275
31. Okuyan B, Sancar M, Izzettin FV, Morisky DE. Erratum to and corrections on the article entitled “Assessment of medication knowledge and adherence among patients under oral chronic medication treatment in community pharmacy settings. Pharmacoepidemiol Drug Saf. (2013). doi: 10.1002/pds.3394
32. Freyer J, Greißing C, Buchal P, Kabitz H, Kasprick L, Schuchmann M, et al. Discharge medication - what do patients know about their medication on discharge? Dtsch Med Wochenschr. (2016). doi: 10.1055/s-0042-108618
33. Marvanova M, Roumie CL, Eden SK, Cawthon C, Schnipper JL, Kripalani S. Health literacy and medication understanding among hospitalized adults. J Hosp Med. (2011). doi: 10.1002/jhm.925
34. Passagli LC, Barros Cota B, César Simões T, Chama Borges Luz T. Knowledge of prescribed drugs among primary care patients: findings from Prover Project. Int J Clin Pharm. (2021). doi: 10.1007/s11096-021-01246-x
35. Timmerman L, Stellema R, Stronks DL, Groeneweg G, Huygen FJPM. Adherence to pharmacological pain therapy in patients with nonmalignant pain: the role of patients’ knowledge of pain medication. Pain Pract. (2014). doi: 10.1111/papr.12139
36. Loeber S, Duka T, Welzel Márquez H, Nakovics H, Heinz A, Mann K, et al. Effects of repeated withdrawal from alcohol on recovery of cognitive impairment under abstinence and rate of relapse. Alcohol Alcohol. (2010). doi: 10.1093/alcalc/agq065
37. Pruckner N, Baumgartner J, Hinterbuchinger B, Glahn A, Vyssoki S, Vyssoki B. Thiamine substitution in alcohol use disorder: A narrative review of medical guidelines. Eur Addict Res. (2019). doi: 10.1159/000499039
38. Alkatheri AM, Albekairy AM. Does the patients’ educational level and previous counseling affect their medication knowledge? Ann Thorac Med. (2013). doi: 10.4103/1817-1737.109823
39. Romero-Sanchez J, Garcia-Cardenas V, Abaurre R, Martínez-Martínez F, Garcia-Delgado P. Prevalence and predictors of inadequate patient medication knowledge. J Eval Clin Pract. (2016). doi: 10.1111/jep.12547
40. Henkel D. Unemployment and substance use: a review of the literature (1990-2010). Curr Drug Abuse Rev. (2011). doi: 10.2174/1874473711104010004
41. Schäfer I. Substance use in the population-A plea for a balanced discussion. Dtsch Arztebl Int. (2022). doi: 10.3238/arztebl.m2022.0286
Keywords: medication knowledge, substance use disorder, alcohol use disorder, drug safety, medication plan
Citation: Heck J, Dubaschewski M, Krause O, Bleich S, Schulze Westhoff M, Krichevsky B, Glahn A and Schröder S (2025) What do patients with substance use disorders know about their medication? A cross-sectional interview-based study. Front. Psychiatry 16:1556920. doi: 10.3389/fpsyt.2025.1556920
Received: 07 January 2025; Accepted: 27 March 2025;
Published: 10 April 2025.
Edited by:
Annagiulia Di Trana, National Institute of Health (ISS), ItalyReviewed by:
Olena Zhabenko, Psychiatric University Hospital Zurich, SwitzerlandJean-Michel Petot, Université Paris Nanterre, France
Copyright © 2025 Heck, Dubaschewski, Krause, Bleich, Schulze Westhoff, Krichevsky, Glahn and Schröder. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sebastian Schröder, c2Nocm9lZGVyLnNlYmFzdGlhbkBtaC1oYW5ub3Zlci5kZQ==
†ORCID: Johannes Heck, orcid.org/0000-0002-5382-3014
Olaf Krause, orcid.org/0000-0002-9932-1116
Stefan Bleich, orcid.org/0000-0001-5004-3824
Martin Schulze Westhoff, orcid.org/0000-0003-3262-8137
Benjamin Krichevsky, orcid.org/0000-0001-5899-0113
Sebastian Schröder, orcid.org/0000-0003-0905-274X
†These authors share first authorship