 Jon E. Grant
Jon E. Grant Sophie Boutouis1
Sophie Boutouis1 Madison Collins
Madison Collins- 1Department of Psychiatry & Behavioral Neuroscience, University of Chicago, Chicago, IL, United States
- 2Department of Psychiatry, Faculty of Medicine, University of Southampton, Southampton, United Kingdom
- 3NHS Southern Gambling Service/Southern Health NHS Foundation Trust, Southampton, United Kingdom
Background: This study sought to examine the rate of compulsive sexual behavior disorder (CSBD) in a sample of adults drawn from the community and its associated mental health correlates.
Methods: An online survey of “Personality, Mental Health, and Well-Being” was distributed via Prolific to 300 adults aged 18 to 75 years. The survey measured a range of behaviors, such as sexual behavior, alcohol and drug use, and dimensional constructs of impulsivity and compulsivity using validated self-report instruments.
Results: A total of 296 participants (54.7% female) completed the survey and were included in the analysis. The overall prevalence of probable compulsive sexual behavior disorder (CSBD) was 10.8% (n=32). Compared to adults without CSBD, those with CSBD were more likely to be younger and identify as bisexual. In addition, they were more likely to have attention-deficit hyperactivity disorder (ADHD) and borderline personality disorder (BPD) symptoms, social media and drug use problems, and higher levels of obsessionality, trans-diagnostic compulsivity, and trans-diagnostic impulsivity. Gender, race, and alcohol use did not significantly differ between groups.
Conclusion: CSBD appears to be common in adults and is equally represented in males and females. CSBD appears to have obsessive, compulsive, and impulsive traits and this may have nosological importance.
Introduction
Although mentioned in the medical literature for well over a hundred years under various names, and recently included in the International Classification of Diseases Version 11 (ICD-11), Compulsive Sexual Behavior Disorder (CSBD) continues to be a contested diagnostic entity (1, 2). The generally agreed upon understanding of CSBD is that it reflects some level of difficulty controlling sexual urges and behaviors and that this lack of control results in clinically significant distress and/or psychosocial impairment (3). There is ongoing debate, however, as to whether the urges and behaviors associated with CSBD are best understood as an addiction (such as gambling), an impulse control disorder (such as kleptomania), or as lying somewhere on the obsessive-compulsive spectrum (e.g., 4–6).
One way to understand behaviors that are poorly controlled, and to determine the most appropriate classification for them, is to examine the potential underlying trans-diagnostic constructs of impulsivity and compulsivity. Impulsivity refers to the tendency to choose the immediacy of reward despite possible negative consequences (i.e. that there is something rewarding/pleasurable driving the behavior and that this urge for reward outweighs the consequences); whereas compulsivity is the tendency to perform repetitive habitual actions largely to reduce an unwanted anxious feeling, despite the resultant psychosocial impairment (7). These concepts of impulsivity and compulsivity, however, may not be diametrically opposed driving forces behind human behavior (8). In the case of CSBD, some research has begun addressing these constructs (9–13) as well as understanding CSBD by examining comorbidity and its longitudinal course (14, 15).
In a small sample of people with CSBD (n=20), researchers found elevated rates of impulse control disorders (ADHD) as well as elevated rates of impulsivity using the Barratt Impulsiveness Scale (16). Impulsivity in at least two areas was one of the most observed BPD symptoms in a sample of 85 patients with CSBD, though only one patient met criteria for BPD (17). Müller and Antons (18) examined 102 adult males and found heightened impulsivity (defined as urgency and deficits in perseverance) in the subset of adults with high levels of problematic pornography use (problematic pornography use has been argued to be a major subtype of CSBD; 19). Similarly, Mestre-Bach et al. (20) examined 44 adults with CSBD who were seeking treatment and found that they scored higher on the obsessive-compulsive subscale of the Symptom Checklist-Revised compared to adults with gambling disorder or those with internet gaming disorder. Although these studies found both impulsive (i.e. reward-driven) and compulsive (i.e. habitual and ritualistic) traits in adults with CSBD, other research has found that compulsivity and impulsivity may only play modest roles in problematic sexual behavior (21).
Because the data regarding impulsive and compulsive traits in CSBD are sparse, we conducted a small exploratory study of individuals in the community who met proposed criteria for CSBD compared with healthy controls. The study hypothesized that those with probable CSBD would endorse greater levels of both trans-diagnostic impulsivity and trans-diagnostic compulsivity.
Methods
The Department of Psychiatry and Behavioral Neuroscience at the University of Chicago developed the Personality, Mental Health, and Well-Being Survey to assess mental health and well-being in a large sample of adults online. The survey included demographic information and used questions from validated screening tools examining mental health issues. All study procedures, including the consent procedure, were carried out in accordance with the Declaration of Helsinki and were approved by the Institutional Review Board of the University of Chicago.
Participants completed the online survey via REDCap (REDCap is a secure web platform managed by the University of Chicago) as part of this study. Participants were first required to view the Institutional Review Board (IRB) – approved consent page, at which point they could choose to participate in the survey or opt out. A refusal to respond was taken as a denial of consent and participants were not allowed to continue with the study. The survey asserted that all responses would be kept confidential and that no personally identifying information would be collected. Subjects were compensated $12 for their participation. Data was collected on 1/9/24.
The self-report survey took approximately 30 minutes to complete. Survey questions assessed demographic information (including self-identified gender, race, educational attainment, and sexual orientation, in which respondents could choose from various categorical options), sexual behavior, and mental health and substance use issues (especially traits and symptoms relevant to impulsivity and compulsivity).
The following reliable and valid measures were embedded (without titles) in the survey: the Minnesota Impulsive Disorders Interview (MIDI) (22, 23) (the Compulsive Sexual Behavior Disorder [CSBD] module reflects urges, fantasies and behaviors as well as impairment and distress and was based on phenomenological research regarding CSBD) (24, 25); the Alcohol Use Disorders Identification Test (AUDIT) (26) (to examine the oftentimes impulsive behavior of alcohol use; the AUDIT demonstrated excellent reliability in the present study [α = .846]); the Drug Abuse Screening Test (DAST-10) (27, 28) (to examine rates of drug use which is often seen as impulsive; the DAST-10 demonstrated good reliability in the present study [α = .633]); the Adult ADHD Self-Report Scale Part A (ASRS-v1.1) (29) (a disorder with prominent impulsive features and large prevalence rates; the ASRS demonstrated good reliability in the present study [α = .761]); the McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD) (30) (another disorder with pronounced impulsive features and large prevalence rates; the MSI-BPD showed excellent reliability in the present study (α = .943); the Barratt Impulsiveness Scale, Short Form (BIS-15) (31) (the BIS-15 demonstrated excellent reliability in the present study [α = .869]); the Cambridge-Chicago Compulsivity Trait Scale (CHI-T) (32, 33) (a scale examining compulsivity/rigidity of behaviors; the CHI-T demonstrated excellent reliability in the present study [α = .811]); the Bergen Social Media Addiction Scale (BSMAS) (34) (the BSMAS demonstrated excellent reliability in the present study [α = .867]); the Problematic Tinder Use Scale (PTUS) (35) (the PTUS demonstrated good reliability in the present study [α = .782]); and the Obsessive-Compulsive Inventory Revised (OCI-R) (36) (a scale of a more prototypical compulsive behavior; the OCI-R demonstrated excellent reliability in the present study [α = .896]).
Subjects screened positive for CSBD on the MIDI if they reported any of the following: 1) an intense preoccupation with some aspect of sex or excessive sexual activity; 2) repetitive sexual fantasies or urges that are out of control or cause significant distress; or 3) engagement in repetitive sexual behavior that is out of control or causes significant distress.
Four participants did not complete the CSBD module of the MIDI, bringing the final sample size to 296. Some participants did not complete every clinical measure in the survey (resulting in different Ns for each outcome variable displayed in Table 1). The PTUS could only be completed by participants who reported current dating app use, which is why the N for the PTUS is much smaller than the other measures.
Data analysis
A sample of 300 adults aged 18 to 75 years were sent the online survey via Prolific. Assuming an expected prevalence of CSBD of around 10% (e.g. 37), this would yield a CSBD group of ~30 individuals and a reference group of ~270. This would yield 95% power to detect a significant group difference of large effect size (d=0.7), at alpha 0.05, two-tailed (G*power software).
Participants were grouped into one of two categories based on their responses to the CSBD module of the MIDI (see above for diagnostic criteria) with respect to the last 12 months: probable CSBD and No CSBD. Significant main effects of group were identified for demographic measures using independent sample t tests for continuous variables and chi-square tests or fisher’s exact tests for categorical variables. Since age was significantly correlated with the total scores of the clinical measures, analyses of covariance (ANCOVAs) were used to control for age while detecting significant between-group differences. Effect sizes were calculated in the forms of Cohen’s d for t tests (0.2 = small, 0.5 = medium, 0.8 = large), Phi for chi-square tests (0.1 = weak, 0.3 = moderate, 0.5 = strong), and partial eta squared for ANCOVAs (0.01 = small, 0.06 = medium, 0.14 = large). Finally, we created a binary logistic regression model in which various dimensions of impulsivity and compulsivity (i.e., ASRS, BIS-15, CHI-T, MSI-BPD, OCI-R total scores) were examined as possible predictors of probable CSBD (0 = no, 1 = yes) while adjusting for age and sexual orientation (0 = not bisexual, 1 = bisexual). Variance Inflation Factor (VIF) values were calculated to evaluate the predictor variables for multicollinearity. The VIF values in our study ranged from 1-3, suggesting moderate correlations between the predictors but no multicollinearity. The fit of the model was verified with the Hosmer-Lemeshow test. Our sample SPSS was used for all statistical analyses (version 24; IBM Corp). Statistical significance was defined as p < 0.05.
Results
The demographics for the sample who completed the CSBD module of the MIDI (n=296) are presented in Table 1. The overall prevalence of probable compulsive sexual behavior disorder (CSBD) was 10.8% (n=32) based on a screening questionnaire (not on a diagnostic assessment). Among females, the rate of probable CSBD was 10.1%, and the rate was 12.3% among males.
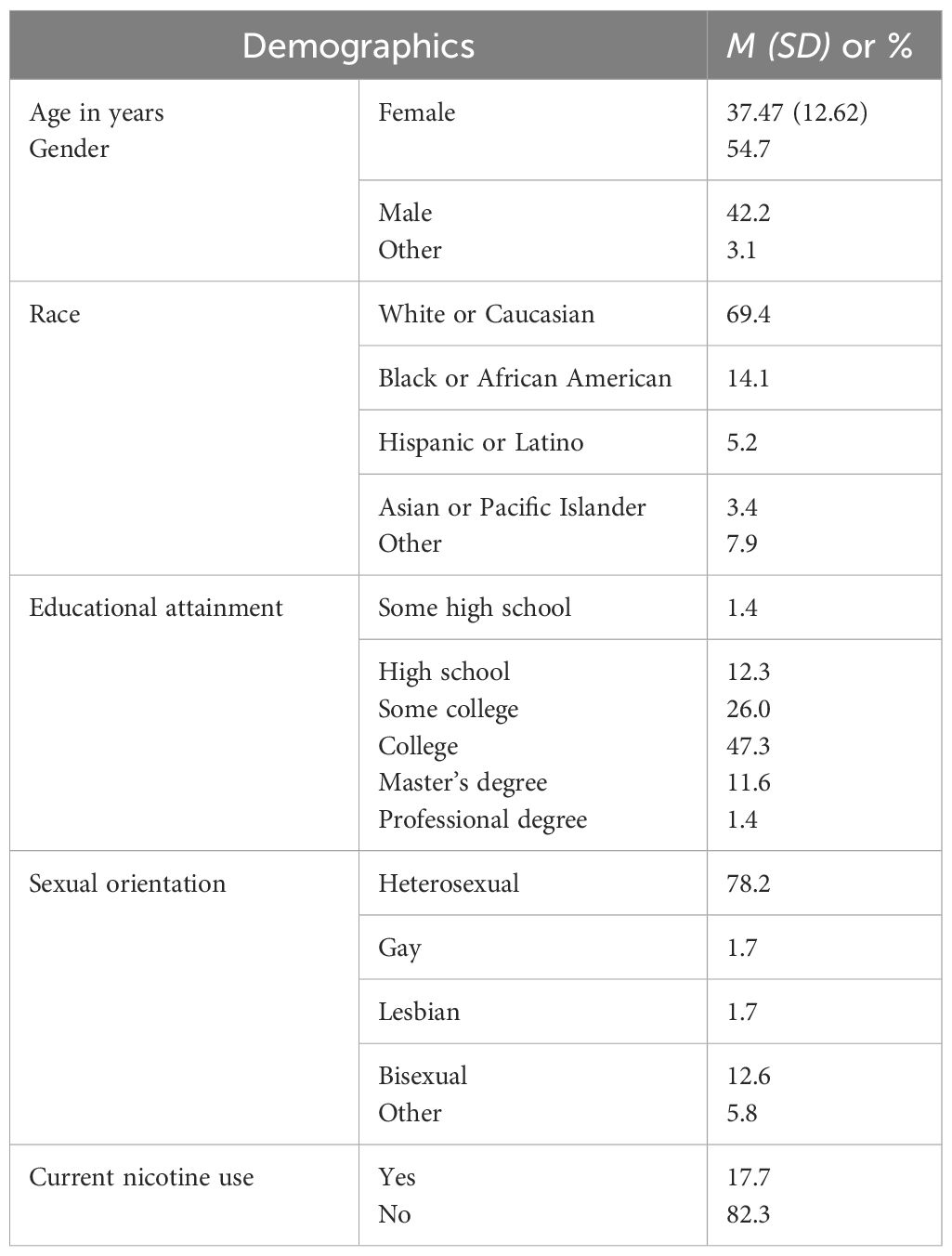
Table 1. Descriptive statistics for a sample of 296 adults.
Table 2 shows the demographics of the adults with probable CSBD compared to the No CSBD participants. Those with probable CSBD were significantly younger (p=0.004) and more likely to identify as bisexual (p=0.014).
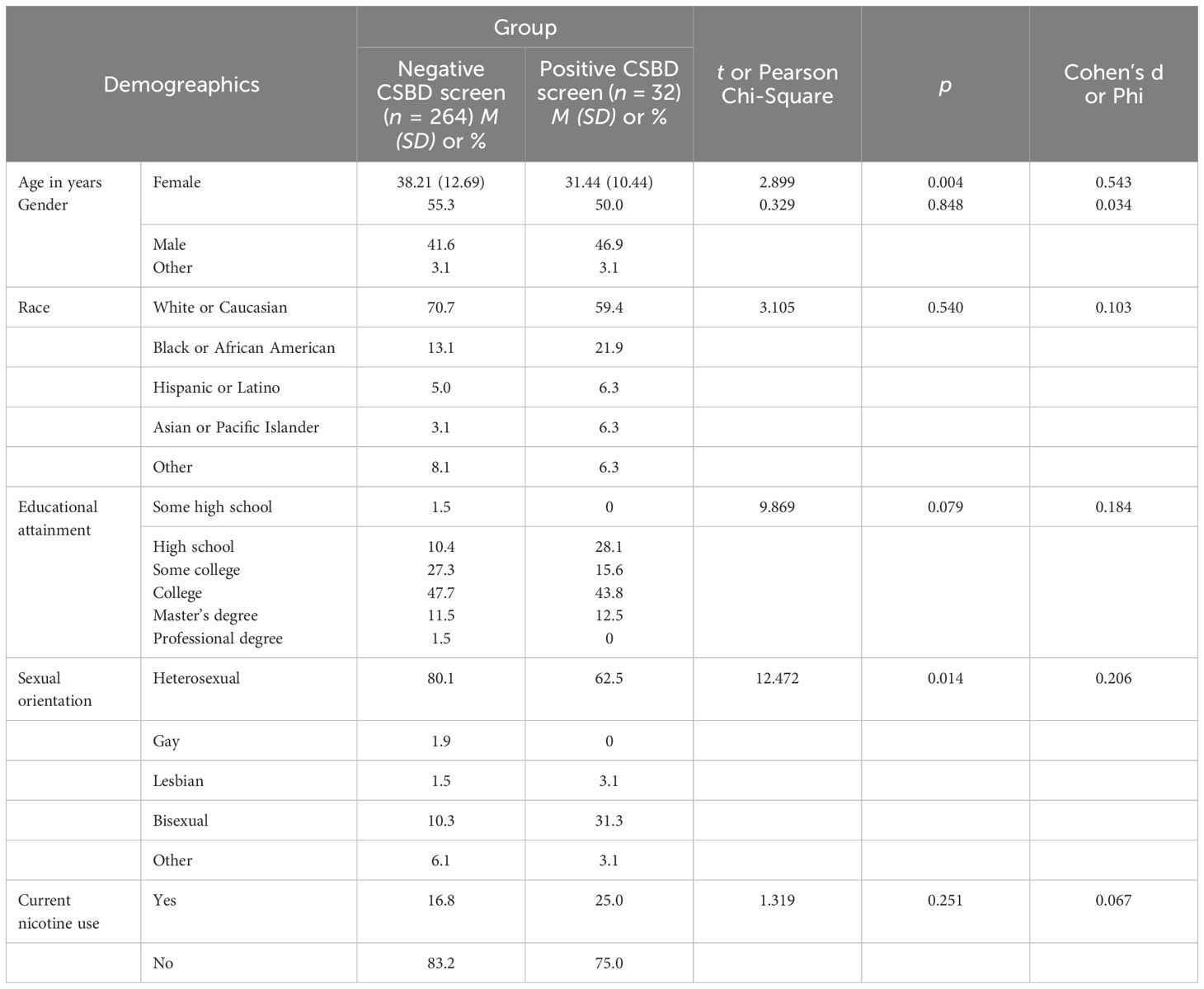
Table 2. Descriptive statistics for a sample of 296 adults, stratified by a positive versus negative CSBD screen.
Those with probable CSBD scored significantly higher on multiple mental health measures (Table 3). They were more likely to have problematic social media use and drug use problems (p<.001). They reported higher scores on a measure of obsessive-compulsive symptoms (OCI-R) (p<.001) and compulsivity (CHI-T) (p=0.018). Finally, they scored higher on the BIS-15 (p=0.005), a measure of impulsivity, and had more severe symptoms of ADHD (p<.001) and BPD (p<.001), disorders with prominent impulsive features.
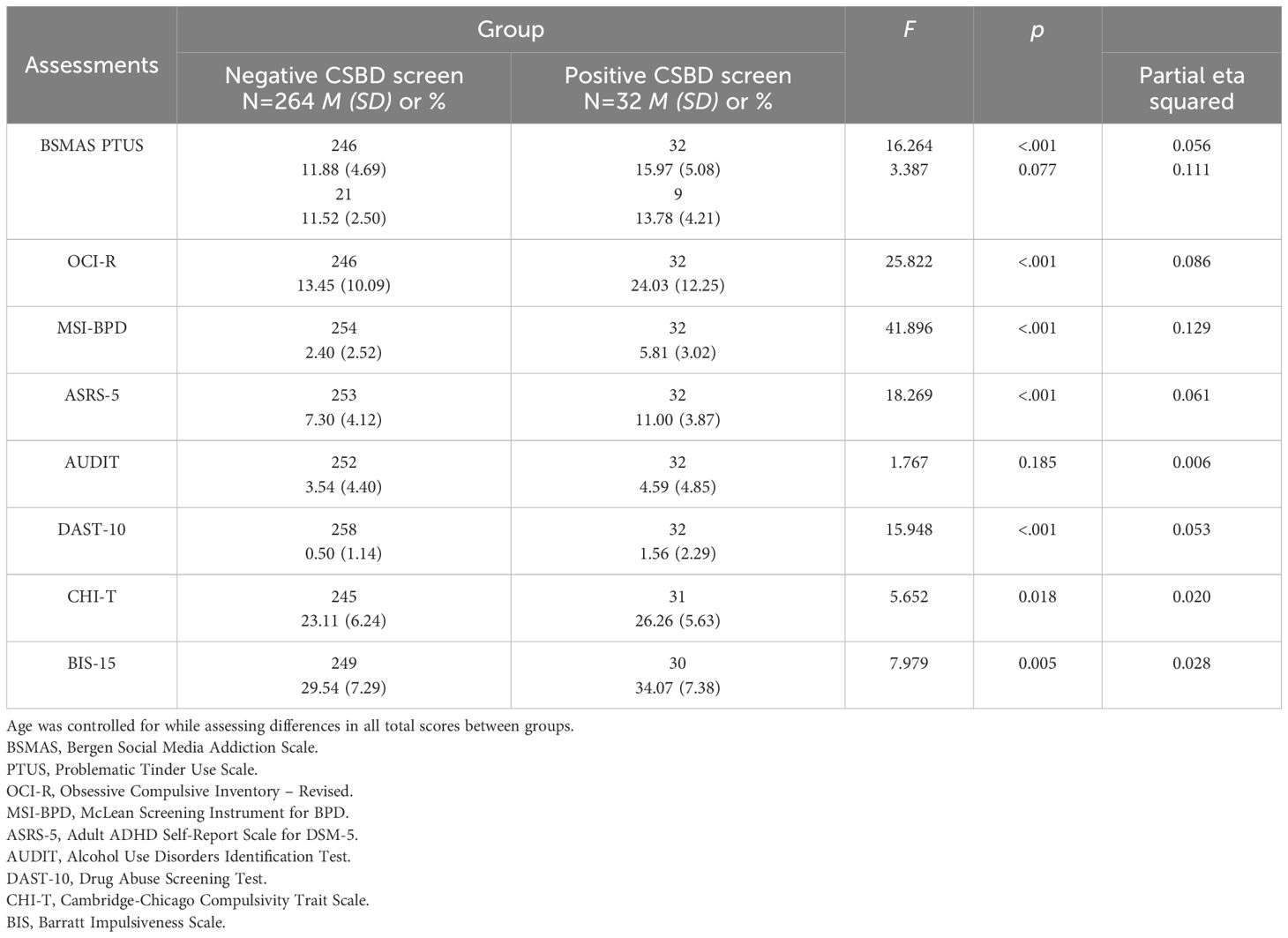
Table 3. Total scores on a variety of clinical measures for a sample of adults, stratified by a positive versus negative CSBD screen.
The results of the logistic regression revealed that greater ADHD (OR = 1.20, p = .028) and BPD (OR = 1.25, p = .041) symptomology increased the odds of having probable CSBD, even after controlling for age, sexual orientation, and other measures of impulsivity and compulsivity. See Table 4.
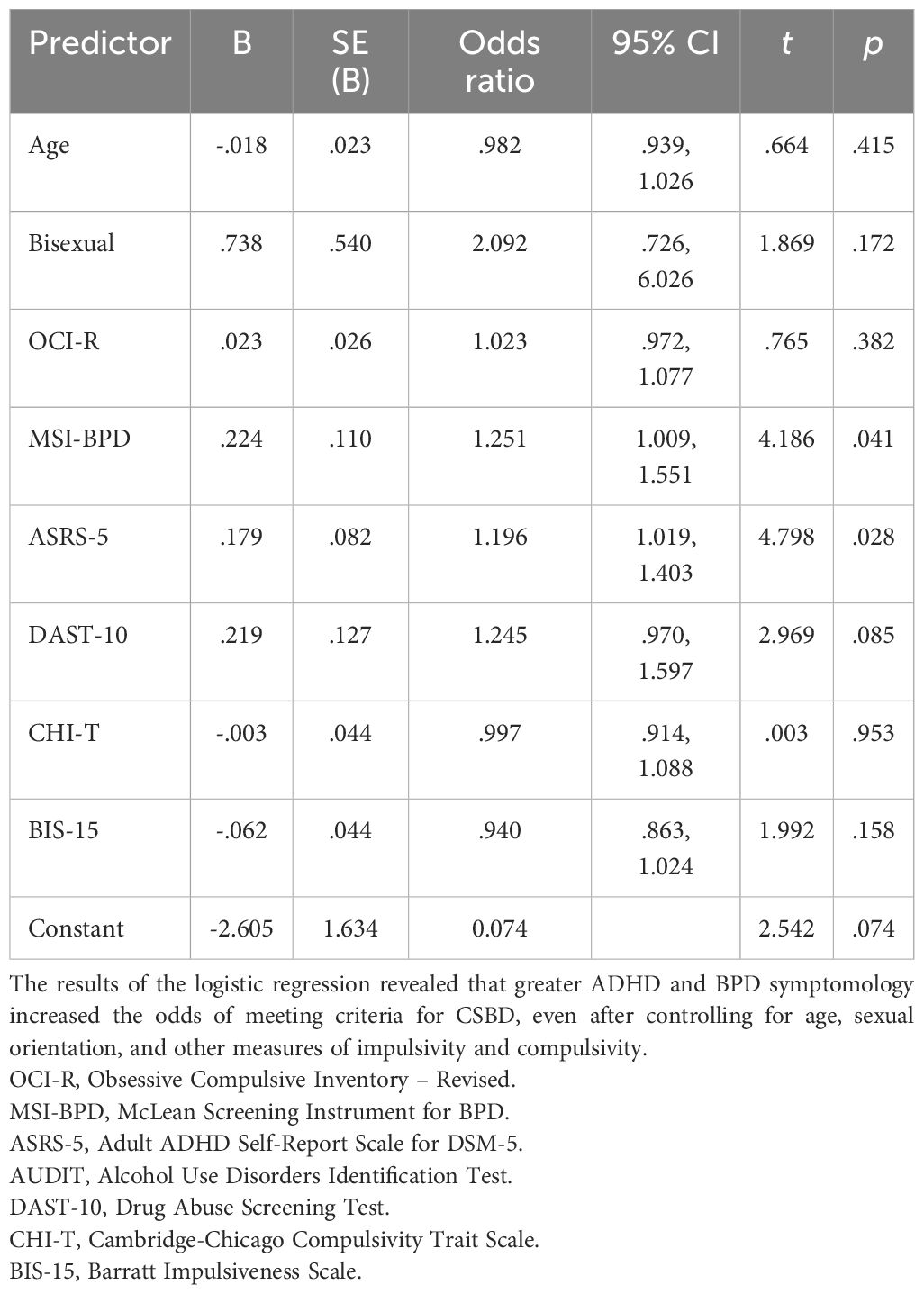
Table 4. Logistic regression predicting probable CSBD (yes versus no).
Discussion
We examined prevalence of probable CSBD in a sample of adults in the community and found a prevalence rate of 10.8%, with females equally represented among those with probable CSBD. Interestingly, this rate of 10.8% is akin to the percentage of people reported to have distress linked to difficulty controlling sexual thoughts/behaviors in a large US sample (n=2,325) (37), but is somewhat higher than the typical rates reported in previous CSBD work (often 3-6%) (38) or in a large international study (4.8%) (39). Because probable CSBD was linked to younger age in our study, one possible explanation for the variation in the literature could be the age of a particular sample examined or to the measure used to assess for the disorder.
In terms of the mental health issues among those with probable CSBD, these adults reported addictive problems, issues with trans-diagnostic impulsivity (BIS-15 scores) and more trans-diagnostic compulsivity (CHI-T scores) than those without CSBD. Thus, these transdiagnostic measures suggest that probable CSBD may not be simply categorized as an addictive, impulsive, or a compulsive issue as these adults with probable CSBD reported elevated rates of problems across these contextual domains. This may highlight a wider issue with current classification systems – namely that disorders are by necessity put into a particular category, but a potential disadvantage of this approach is that other features inherent in the given condition may then tend to be overlooked clinically. One useful approach to complement this categorical approach may be to additionally consider trans-diagnostic measures such as trait impulsivity and compulsivity.
There are several implications of these findings. Probable CSBD appears to be fairly common, yet in many parts of the world no treatment services exist, which should perhaps be rectified (40). Probable CSBD was linked to elevated rates of problematic usage of social media. The link here may be the wider umbrella construct of Problematic Usage of the Internet (PUI) (for discussion see: 41, 42). Perhaps PUI constitutes the link underlying the relationship between probable CSBD (which can manifest through compulsive online activities), and other forms of PUI. This could be addressed in future work by measuring the extent to which probable CSBD manifests online versus off-line. Clinically, it may be useful to incorporate measures of PUI into practice as part of evaluations. The elevated levels of impulsive and compulsive problems in people with probable CSBD highlights the need for careful clinical assessment for other related impulsive-compulsive disorders, such as (but not limited to) ADHD, BPD, and obsessive-compulsive related disorders.
While this study measured trans-diagnostic impulsivity and compulsivity in probable CSBD in one study setting, several limitations should be noted. This study was not designed to be epidemiologically representative and so findings may not generalize to other settings. The gold standard for diagnosis is of course structured clinical interviews – whereas this study used previously validated self-report instruments. The MIDI CSBD module used herein to identify probable CSBD is not identical to the ICD-11 criteria for CSBD, since the former was developed at an earlier time point. As such, any diagnoses should be considered as provisional/likely but not certain in relation to ICD-11. Additionally, some concepts examined are not formal disorders but rather concepts such as problematic use of Tinder or social media. This being an exploratory study we did not correct for multiple comparisons; this had the benefit of reducing the risk of false negatives due to the power arising from the given sample size of the probable CSBD group. Relatedly, the sample size was relatively small, and while power was ample to detect large effect size group differences, ability to detect more subtle group differences (i.e. those of small or medium effect size) would have been limited. We did not examine all possible measures that may reflect impulsivity and compulsivity. We relied only on self-report instruments. Future work might wish to expand on the measures used – for example to include cognitive measures. Another important limitation is that impulsivity and compulsivity can be considered in the broad sense (i.e. trans-diagnostically, such as using BIS-15 and CHI-T) as well as at the level of how a particular behavior manifests phenomenologically. For example, one individual may undertake compulsive sexual behavior in the spur of the moment in order to obtain a reward; and thus, the behavior may be described as being impulsive; while another person may undertake such behavior in a repetitive fashion to alleviate anxiety or according to rigid rules, thus being compulsive. Or both may apply, to differing degrees, depending on the person and the point in time. In the current study we focused on trans-diagnostic impulsivity and compulsivity measured cross-sectionally, and did not collect behavior-specific measures. Behavior-specific impulsivity and compulsivity could potentially be measured in a variety of ways in future work – such as asking a given person about subjective drivers underlying specific behaviors (e.g. via a questionnaire); and/or using cognitive tests that attempt to model behavioral responses to stimuli under laboratory conditions. This type of approach may also be useful to better understand how CSBD should optimally be classified.
In conclusion, this study identified relatively high rates of probable CSBD in an online sample and that it was linked to elevated rates of impulsive and compulsive problems and traits. This has implications for clinical practice but also highlights the need for further research into CSBD including how its presentation may change longitudinally and interact with PUI and other clinical features.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by University of Chicago Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JG: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing. SB: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. MC: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing. SC: Conceptualization, Formal analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
JG has received research grants from Janssen and Biohaven Pharmaceuticals. JG receives yearly compensation from Springer Publishing for acting as Editor-in-Chief of the Journal of Gambling Studies and has received royalties from Oxford University Press, American Psychiatric Publishing, Inc., Norton Press, and McGraw Hill. SC receives an honorarium from Elsevier for journal editorial work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Reed GM, First MB, Billieux J, Cloitre M, Briken P, Achab S, et al. Emerging experience with selected new categories in the ICD-11: complex PTSD, prolonged grief disorder, gaming disorder, and compulsive sexual behaviour disorder. World Psychiatry. (2022) 21:189–213. doi: 10.1002/wps.20960
2. Grubbs JB, Hoagland KC, Lee BN, Grant JT, Davison P, Reid RC, et al. Sexual addiction 25 years on: A systematic and methodological review of empirical literature and an agenda for future research. Clin Psychol Rev. (2020) 82:101925. doi: 10.1016/j.cpr.2020.101925
3. Bőthe B, Potenza MN, and Demetrovics Z. Debates on compulsive sexual behavior disorder: A call for global and interdisciplinary perspectives. Arch Sexual Behav. (2024) 53:1215–20. doi: 10.1007/s10508-024-02836-2
4. Fuss J, Keeley JW, Stein DJ, Rebello TJ, García J.Á., Briken P, et al. Mental health professionals’ use of the ICD-11 classification of impulse control disorders and behavioral addictions: An international field study. J Behav Addict. (2024) 13:276–92. doi: 10.1556/2006.2023.00083
5. Borgogna NC and Aita SL. Another failure of the latent disease model? The case of compulsive sexual behavior disorder. J Behav Addict. (2022) 11:615–9. doi: 10.1556/2006.2022.00069
6. Lew-Starowicz M and Coleman E. Mental and sexual health perspectives of the International Classification of Diseases (ICD-11) compulsive sexual behavior disorder. J Behav Addict. (2022) 11:226–9. doi: 10.1556/2006.2022.00032
7. Hook RW, Grant JE, Ioannidis K, Tiego J, Yücel M, Wilkinson P, et al. Trans-diagnostic measurement of impulsivity and compulsivity: A review of self-report tools. Neurosci Biobehavioral Rev. (2021) 120:455–69. doi: 10.1016/j.neubiorev.2020.10.007
8. Fontenelle LF, Oostermeijer S, Harrison BJ, Pantelis C, and Yücel M. Obsessive-compulsive disorder, impulse control disorders and drug addiction: common features and potential treatments. Drugs. (2011) 71:827–40. doi: 10.2165/11591790-000000000-00000
9. Raymond NC, Coleman E, and Miner MH. Psychiatric comorbidity and compulsive/impulsive traits in compulsive sexual behavior. Compr Psychiatry. (2003) 44:370–80. doi: 10.1016/S0010-440X(03)00110-X
10. Antons S, Mueller SM, Wegmann E, Trotzke P, Schulte MM, and Brand M. Facets of impulsivity and related aspects differentiate among recreational and unregulated use of Internet pornography. J Behav Addict. (2019) 8:223–33. doi: 10.1556/2006.8.2019.22
11. Levi G, Cohen C, Kaliche S, Sharaabi S, Cohen K, Tzur-Bitan D, et al. Sexual addiction, compulsivity, and impulsivity among a predominantly female sample of adults who use the internet for sex. J Behav Addict. (2020) 9:83–92. doi: 10.1556/2006.2020.00007
12. Draps M, Sescousse G, Wilk M, Obarska K, Szumska I, Żukrowska W, et al. An empirical study of affective and cognitive functions in Compulsive Sexual Behavior Disorder. J Behav Addict. (2021) 10:657–74. doi: 10.1556/2006.2021.00056
13. Bocci Benucci S, Di Gesto C, Ghinassi S, Casale S, and Fioravanti. G. Pornography use, problematic pornography use, impulsivity, and sensation seeking: a meta-analysis. J Sexual Med. (2024) 21:922–39. doi: 10.1093/jsxmed/qdae101
14. Ballester-Arnal R, Castro-Calvo J, Gimenez-Garcia C, Gil-Julia B, and Gil-Llario MD. Psychiatric comorbidity in compulsive sexual behavior disorder (CSBD). Addictive Behav. (2020) 107:106384. doi: 10.1016/j.addbeh.2020.106384
15. Castro-Calvo J, Ballester-Arnal R, Giménez-García C, García-Barba M, and Gil-Llario MD. Natural course of compulsive sexual behavior (CSB): A 1-year follow-up study. Int J Ment Health Addict. (2024) 22:3470–90. doi: 10.1007/s11469-023-01061-7
16. Savard J, Hirvikoski T, Görts Öberg K, Dhejne C, Rahm C, and Jokinen J. Impulsivity in compulsive sexual behavior disorder and pedophilic disorder. J Behav Addict. (2021) 10:839–47. doi: 10.1556/2006.2021.00044
17. Lloyd M, Raymond NC, Miner MH, and Coleman E. Borderline personality traits in individuals with compulsive sexual behavior. Sexual Addict Compulsivity. (2007) 14:187–206. doi: 10.1080/10720160701480337
18. Müller SM and Antons S. Decision making and executive functions in problematic pornography use. Front Psychiatry. (2023) 14:1191297. doi: 10.3389/fpsyt.2023.1191297
19. Golder S, Walter B, Bengesser I, Kramer D, Muhl C, Tahmassebi N, et al. Compulsive sexual behavior disorder in an inpatient sample with substance use disorder. Sexul Med. (2024) 12:qfae003. doi: 10.1093/sexmed/qfae003
20. Mestre-Bach G, Granero R, Fernández-Aranda F, Potenza MN, and Jiménez-Murcia S. Obsessive-compulsive, harm-avoidance and persistence tendencies in patients with gambling, gaming, compulsive sexual behavior and compulsive buying-shopping disorders/concerns. Addictice Behav. (2023) 139:107591. doi: 10.1016/j.addbeh.2022.107591
21. Bőthe B, Tóth-Király I, Potenza MN, Griffiths MD, Orosz G, and Demetrovics Z. Revisiting the role of impulsivity and compulsivity in problematic sexual behaviors. J Sexual Res. (2019) 56:166–79. doi: 10.1080/00224499.2018.1480744
22. Grant JE. Impulse control disorders: A Clinician’s guide to understanding and treating behavioral addictions. New York: WW Norton and Company (2008).
23. Chamberlain SR and Grant JE. Minnesota Impulse Disorders Interview (MIDI): Validation of a structured diagnostic clinical interview for impulse control disorders in an enriched community sample. Psychiatry Res. (2018) 265:279–83. doi: 10.1016/j.psychres.2018.05.006
24. Black DW, Kehrberg LL, Flumerfelt DL, and Schlosser SS. Characteristics of 36 subjects reporting compulsive sexual behavior. Am J Psychiatry. (1997) 154:243–9. doi: 10.1176/ajp.154.2.243
25. Derbyshire KL and Grant JE. Compulsive sexual behavior: a review of the literature. J Behav Addict. (2015) 4:37–43. doi: 10.1556/2006.4.2015.003
26. Saunders JB, Aasland OG, Babor TF, de la Fuente JR, and Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption–II. Addict Abingdon Engl. (1993) 88:791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x
27. Skinner HA. The drug abuse screening test. Addictive Behav. (1982) 7:363–71. doi: 10.1016/0306-4603(82)90005-3
28. Yudko E, Lozhkina O, and Fouts A. A comprehensive review of the psychometric properties of the Drug Abuse Screening Test. J Subst Abuse Treat. (2007) 32:189–98. doi: 10.1016/j.jsat.2006.08.002
29. Kessler RC, Adler L, Ames M, Demler O, Faraone S, Hiripi E, et al. The World Health Organization Adult ADHD Self Report Scale (ASRS): A short screening scale for use in the general population. psychol Med. (2005) 35:245–56. doi: 10.1017/s0033291704002892
30. Zanarini MC, Vujanovic AA, Parachini EA, Boulanger JL, Frankenburg FR, and Hennen J. A screening measure for BPD: The McLean Screening Instrument for borderline personality disorder (MSI-BPD). J Pers Disord. (2003) 17:568–73. doi: 10.1521/pedi.17.6.568.2535
31. Meule A, Michalek S, Friederich HC, and Brockmeyer T. Confirmatory factor analysis of the Barratt Impulsiveness Scale-short form (BIS-15) in patients with mental disorders. Psychiatry Res. (2019) 284:112665. doi: 10.1016/j.psychres.2019.112665
32. Chamberlain SR and Grant JE. Initial validation of a transdiagnostic compulsivity questionnaire: the Cambridge-Chicago Compulsivity Trait Scale. CNS Spectrums. (2018) 23:340–6. doi: 10.1017/S1092852918000810
33. Tiego J, Trender W, Hellyer PJ, Grant JE, Hampshire A, and Chamberlain SR. Measuring compulsivity as a self-reported multidimensional transdiagnostic construct: Large scale (N = 182,000) validation of the Cambridge-Chicago Compulsivity Trait Scale. Assessment. (2023) 30:2433–48. doi: 10.1177/10731911221149083
34. Schou Andreassen C, Billieux J, Griffiths MD, Kuss DJ, Demetrovics Z, Mazzoni E, et al. The relationship between addictive use of social media an,d video games and symptoms of psychiatric disorders: A large-scale cross-sectional study. Psychol Addictive Behav. (2016) 30:252–62. doi: 10.1037/adb0000160
35. Orosz G, Tóth-Király I, Bőthe B, and Melher D. Too many swipes for today: The development of the Problematic Tinder Use Scale (PTUS). J Behav Addict. (2016) 5:518–23. doi: 10.1556/2006.5.2016.016
36. Foa EB, Huppert JD, Leiberg S, Langner R, Kichic R, Hajcak G, et al. The Obsessive-Compulsive Inventory: Development and validation of a short version. psychol Assess. (2002) 14:485–96. doi: 10.1037/1040-3590.14.4.485
37. Dickenson JA, Gleason N, Coleman E, and Miner MH. Prevalence of distress associated with difficulty controlling sexual urges, feelings, and behaviors in the United States. JAMA Network Open. (2018) 1:e184468. doi: 10.1001/jamanetworkopen.2018.4468
38. Kraus SW, Krueger RB, Briken P, First MB, Stein DJ, Kaplan MS, et al. Compulsive sexual behaviour disorder in the ICD-11. World Psychiatry. (2018) 17:109–10. doi: 10.1002/wps.20499
39. Bőthe B, Koós M, Nagy L, Kraus SW, Demetrovics Z, Potenza MN, et al. Compulsive sexual behavior disorder in 42 countries: Insights from the International Sex Survey and introduction of standardized assessment tools. J Behav Addict. (2023) 12:393–407. doi: 10.1556/2006.2023.00028
40. International Advisory Group for the Revision of the ICD-10 Mental and Behavioural Disorders. A conceptual framework for the revision of the ICD-10 classification of mental and behavioural disorders. World Psychiatry. (2011) 10:86–92. doi: 10.1002/j.2051-5545.2011.tb00022.x
41. Fineberg NA, Demetrovics Z, Stein DJ, Ioannidis K, Potenza MN, Grünblatt E, et al. Manifesto for a European research network into Problematic Usage of the Internet. Eur Neuropsychopharmacol. (2018) 28:1232–46. doi: 10.1016/j.euroneuro.2018.08.004
42. Fineberg NA, Menchón JM, Hall N, Dell’Osso B, Brand M, Potenza MN, et al. Advances in problematic usage of the internet research - A narrative review by experts from the European network for problematic usage of the internet. Compr Psychiatry. (2022) 118:152346. doi: 10.1016/j.comppsych.2022.152346
Keywords: compulsive sexual behavior, compulsivity, hypersexual disorder, impulsivity, sex, sexual addiction
Citation: Grant JE, Boutouis S, Collins M and Chamberlain SR (2025) Compulsive sexual behavior disorder: rates and clinical correlates in a community sample. Front. Psychiatry 16:1561885. doi: 10.3389/fpsyt.2025.1561885
Received: 16 January 2025; Accepted: 11 April 2025;
Published: 22 May 2025.
Edited by:
Aviv M. Weinstein, Ariel University, IsraelReviewed by:
Malgorzata Draps, Polish Academy of Sciences, PolandSabine Prantner, Osnabrück University, Germany
Copyright © 2025 Grant, Boutouis, Collins and Chamberlain. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jon E. Grant, am9uZ3JhbnRAdWNoaWNhZ28uZWR1