 Jichao Zheng1*
Jichao Zheng1* Zeqiang Ni2
Zeqiang Ni2- 1Department of Economics Research, Anhui Academy of Social Sciences, Hefei, Anhui, China
- 2School of Economics and Management, Hefei University, Hefei, Anhui, China
Background: More than 30 million older people in China live alone. Research has shown that living alone can lead to poor mental health and that there are mediating variables, such as healthy diet, between living alone and mental health. Therefore, it is important to examine the role of these mediating variables between living alone and mental health to help us develop cost-effective mental health interventions.
Methods: We used the multiple regression method in the R software to test the effect of living arrangements on depression by placing the living arrangements variable, the covariates, and the healthy diet variables into the regression equation. We then used the structural equation method with the R software package lavaan to derive the path coefficients of living arrangements on depression scores through the three mediating paths of fruits, vegetables, and nuts consumption. We used bootstrapping to derive confidence intervals for the coefficients.
Results: Multiple regression results showed that the coefficient of the effect of living alone on depressive symptoms was 1.02. At the same time, all three variables of a healthy diet can alleviate depression, i.e., consuming more fruits, vegetables, and nuts helped to reduce depression scores among older adults. In the mediation analysis, living alone affects the mental health of older adults through three channels, namely, fruit consumption, vegetable consumption, and nuts consumption, respectively, and the indirect effects of these three channels accounted for 15.47% of the total impact of living alone on depression scores of older adults, with vegetable intake having the most significant effect on depression scores, accounting for 8.35% of the total impact, followed by nuts intake and fruits intake.
Conclusion: Older people living alone are a vulnerable group with poor mental health and require a variety of interventions to improve their mental health. Healthy eating is one possible avenue of intervention; the Government should take diversified initiatives to enhance the healthy diet of older persons living alone.
1 Background
Globally, it is increasingly common for older persons to live alone. For example, in 2010, Europe had the highest proportion of older people living alone (28%), followed by North America (25%) (1). By 2022, the number of people over 65 in China has reached 209.78 million, accounting for 14.9% of the total population (2). In the past, in accordance with filial tradition, Chinese older adults generally lived with their children (3). However, as a result of declining fertility rates, older persons have fewer adult children than ever before (4). Meanwhile, a large number of young people are moving into the cities (5). It is estimated that 260 million people have moved from the countryside to the cities (6). As a result, more and more Chinese older adults are living alone (7). According to the seventh population census in 2020, there were 29.94 million households of older persons living alone in the country, compared to 14.44 million ten years ago (8).
Mental disorders are a major contributor to the global health-related burden, with depression and anxiety disorders being significant contributors to this burden (9). Depression affects health and quality of life (10). Depression is characterized by low mood, low energy, sadness, and inability to enjoy life (11). In terms of years lived with disability(YLD), depressive disorders are one of the three leading causes of YLD (12) in 2017. Aging-related processes increase the likelihood of depression (13). As a result, depression is widespread among older adults (14).The prevalence of depression is also high among older people living alone. A survey based on older people in the Shanghai community showed that the prevalence of depression among older people living alone was 26.9% (15). So it is very important to study the mental health of older people living alone. Some academic studies have been conducted on the mental health of older people living alone. Some scholars have focused on social support and social network support for older adults living alone (16). Other researchers have focused on caring for older adults living alone (17).
At the same time, there are mediating variables between living alone and mental health, which some scholars have explored. These variables include physical activity, social participation, intergenerational support, and social activities (18, 19). Other scholars have focused on the mediating role of sleep quality and anxiety in the relationship between living alone and depression (20). Diet plays a very important role in people’s lives, and some studies have shown that certain plant components in the diet are protective against depression (21). For example, some scholars believe that a high intake of fruits and vegetables will reduce depression risk (22). Others believe that the Mediterranean diet enhances mental health and reduces depression (23). Surprisingly, however, few studies have focused on the mediating role of healthy eating between living alone and depression, and this paper will fill a research gap in this area.
2 Literature review and hypotheses
2.1 Direct effect of living alone on depressive symptoms
There are several pathways in which living alone affects mental health. First, living alone and loneliness are two sides of the same coin; living alone is an objective and structural indicator of social isolation, while loneliness is a subjective perception of social isolation (24). One study found one of the most predictive factors of loneliness was living alone (25). And loneliness is a risk factor for depressive symptoms (26). Thus, in general, we can assume that living alone was associated with depression (27). Empirical research also supports the above conclusion, with one study finding a significant increase in depressive symptoms in both men and women after starting to live alone (28).
Second, living alone reduces social interactions and family support for older adults, and studies have shown that men who lack stronger family and friend social networks have a high risk of depression (29). Since most older people living alone are widowed (30)., they have lost the most important social relationship in their later life, i.e., the spousal relationship, which affects their social interaction behavior. For example, when a spouse dies, survivors can find it difficult to maintain previous social relationships (31). Therefore, living alone generally reduces social contact (32). In addition, people who live alone tend to receive less family support than those living with their families (33). Meanwhile, people living alone also lack practical or emotional help from others (34).
As mentioned above, living alone can lead to loneliness and reduced social interactions and family support. As a result, older adults who live alone show more depressive symptoms than those who live with others (35). A study in China suggests that living alone is associated with a higher risk of depressive symptoms, especially among people with less financial support (36). Based on the above literature review, we formulate the following hypotheses:
H1: Living alone can lead to depression in older adults.
2.2 The impact of living alone on healthy diet
There are various concepts of a healthy diet. Some studies suggest that a healthy diet is based on plant foods and is characterized by a high intake of vegetables and fruits (37). Some scholars also consider the Mediterranean diet to be healthy (38). The Mediterranean diet is characterized by plant-based foods, including fruits, vegetables, nuts, and olive oil (39). In fact, the traditional Chinese diet is also plant-based (40). A meta-analysis found that a healthy Chinese diet consisting of a plant-based diet reduced the risk of adverse health outcomes (41).The Chinese Dietary Guidelines recommend eating plenty of vegetables and fruits, as well as eating nuts regularly (42). Overall, we can assume that in the Chinese context, a healthy diet means consuming more vegetables, fruits, and eating nuts regularly.
Living alone affects a healthy diet for several reasons: first, older adults living alone have lower incomes than those living with spouses (43). Some studies have found that people who live alone are more likely to be female and have lower education and income levels (44). A study in China also found that people living alone had lower social status and income (45). On the other hand, healthy foods are usually more expensive (46). One study found that the average price per serving of healthy foods (vegetables, fruits, etc.) is almost double that of unhealthy foods (47). Therefore, older adults living alone are at risk of not having adequate access to healthy foods such as vegetables, fruits, and nuts due to their lower incomes.
Second, psychological and cultural factors associated with living alone may also influence the consumption of healthy foods. Residential patterns can affect one’s daily living patterns (48). From a psychological perspective, people may feel it is not worth cooking for only one person (49). Also, because people who live alone lack the motivation to cook, they tend to eat a smaller variety of foods (50). From a gender-cultural analysis perspective, in cases where women take on the task of cooking, when women are widowed and live alone, they are often not used to eating alone and may not see the purpose of cooking (51). For some men, cooking while living alone can be a “chore” or “hassle,” and some choose to use frozen meals, which can affect the quality of their diet (52). Moreover, fruits and vegetables cannot be preserved for a long time and need to be purchased outside frequently. And some studies have found that older people living alone tend to go out less often (53). As a result, it may be difficult for older adults to buy fresh ingredients.
It is for the above reasons that many studies have found that people who live alone have lower intake of fruits, vegetables, etc. (54). One study found that people who lived alone were the least likely to consume adequate amounts of vegetables and fruits (55). Based on the above literature review, we propose the following hypotheses:
H2a1: Living alone reduces fruit consumption.
H3a2: Living alone reduces vegetable consumption.
H4a3: Living alone reduces the consumption of nuts.
2.3 The role of healthy diet on depressive symptoms
The role of a healthy diet in mental health is manifested at two levels. First, consuming specific types of food, such as vegetables and fruits, helps to reduce mental stress and maintain mental health (56). In contrast, inadequate intake of fruits and vegetables can lead to poor mental health (57). Second, the greater the variety of foods, the lower the level of depression (58).
A healthy diet affects mental health primarily through anti-inflammatory and antioxidant mechanisms. Inflammation and oxidative stress are thought to be potential biological pathways associated with depression (59). Inflammation increases susceptibility to depression (60). And it is argued that inflammation and depression are thought to fuel each other (61). Meanwhile, oxidative stress is one of the major causes of depression (62). And antioxidants are an important physiological indicator of depression (63).
A healthy diet reduces depression and improves mental health through physiological mechanisms such as anti-inflammatory and antioxidant effects. First, a healthy diet has antioxidant effects; for example, plant-based foods are rich in antioxidants (64). Numerous studies have shown that the flavonoid content of fruits and vegetables helps reduce oxidative cell damage (65). Secondly, healthy foods have anti-inflammatory effects. A healthy diet helps maintain lower concentrations of inflammatory mediators, and a higher intake of vegetables, fruits, nuts, and fish is associated with lower inflammation (66). One study suggests that a year-long Mediterranean diet reduces inflammation and has a systematically beneficial effect on the health status of older adults (67).
At the same time, specific components of plant-based diets benefit mental health, such as plant polyphenols that have a protective effect against depression (68). Dietary fiber also produces short-chain fatty acids that have anti-inflammatory and anti-aging effects (69). Therefore, it has been suggested that high consumption of vegetables, fruits, and fish is protective against risk factors for developing CES-D depression (70). It has also been found that healthy eating patterns, such as the Mediterranean diet, can reduce the risk of depression (71). Overall, it has been suggested that diet plays an important role in the prevention and treatment of depression (72). Based on the above literature review, we formulate the following hypotheses:
H2b1: Consumption of fruits may reduce depression.
H3b2: Consumption of vegetables may reduce depression.
H4b3: Consumption of nuts may reduce depression.
3 Materials and methods
3.1 Data sources
This study used data from the China Longitudinal Healthy Longevity Survey (CLHLS) survey (2017–2018). The CLHLS is a tracking survey of older adults organized by Peking University, which is available to scholars for research purposes (73). In the most recent follow-up survey (2017–2018), 15,874 people were interviewed. The questionnaire provided information on family structure, living arrangements, activities of daily living (ADLs), self-rated health, care needs and costs, socialization, diet, drinking behaviors, psychosocial characteristics, financial resources, and other information. China’s Law on the Protection of the Rights and Interests of Older Adults defines older adults as those over 60. Therefore, according to our study objectives, we limited our sample to older adults over 60. At the same time, since we are studying the dietary structure of older people, which is strongly influenced by dental status, and to avoid dental problems confounding the relationship between the variables, we restricted the sample to older adults with 20 natural teeth or wearing dentures. 20 was chosen because studies have concluded that maintaining ≥ 20 teeth is important for mastication function (74), and Japan has even launched the 8020 campaign, an initiative to retain 20 natural teeth at age 80 (75).
3.2 Dependent variables
In the CLHLS survey, the depressive symptoms variable was measured using a simplified version of the CES-D scale with ten questions. The scale is designed to measure depressive symptoms in the general population (76). The 10-item CES-D scale showed good predictive accuracy compared to the full version of the CES-D, which has 20 items (77). The scale consists of seven negatively scored questions and three positively scored questions. The negative-scoring questions include questions such as “Are you bothered by things that don’t usually bother you?”; the positive-scoring questions include questions such as “Are you hopeful about the future? “ Five options were provided for each question: always, often, sometimes, rarely, and never. We assigned each option a value of 1, 2, 3, 4, or 5 for the positive-scoring questions and 5, 4, 3, 2, or 1 for the negative-scoring questions. We summarized the answers to these ten questions and constructed a continuous variable ranging from 10 to 50, with larger values indicating more significant levels of depression. The ten-item depression scale had an Alpha value of 0.8, indicating that the data had sufficient reliability to be analyzed.
3.3 Explanatory variables
The first explanatory variable is living alone, and the questionnaire includes the question, “ Who do you currently live with? “. The options are: 1. family (including live-in nannies); 2. living alone; and 3. nursing home. We defined respondents who chose 2 as living alone and assigned a value of 1, whereas respondents who chose 1 and 3 were defined as not living alone and assigned a value of 0.
Next are the fruit and vegetable consumption variables; the questionnaire contains the question “Do you eat fresh fruits and vegetables regularly?”. The options are: 1. daily/almost daily; 2. Often; 3. Occasionally; 4. seldom or never. We assign values of 4-1, respectively.
Finally, we obtained the nuts variable. The questionnaire included “How often do you eat nuts?”. Nuts here include peanuts/walnuts/chestnuts/watermelon seeds, etc. The options for this question were: 1. almost every day; 2. not every day but at least once a week; 3. not every week but at least once a month; 4. not every month but sometimes; and 5. rarely or never. We assign values of 5-1, respectively.
CLHLS is a well-established database and its dietary data are used in many studies. For example, one study found that increased intake of vegetables and fruits improved cognitive function in Chinese oldest adults (78). Another study, based on CLHLS data, found that maintaining high food variety reduced the incidence of frailty in older Chinese adults (79).
3.4 Covariates
As shown in Table 1, we categorize covariates into three main groups. The first group is demographic background factors, including gender, age, and marital status. The second group is the respondent’s socio-economic status, measured by several indications such as years of schooling, residence, perceived income adequacy, and visits (80). The third dimension is the respondent’s health status, which mainly includes self-rated health, whether they drink alcohol or not, and instrumental activities of daily living.
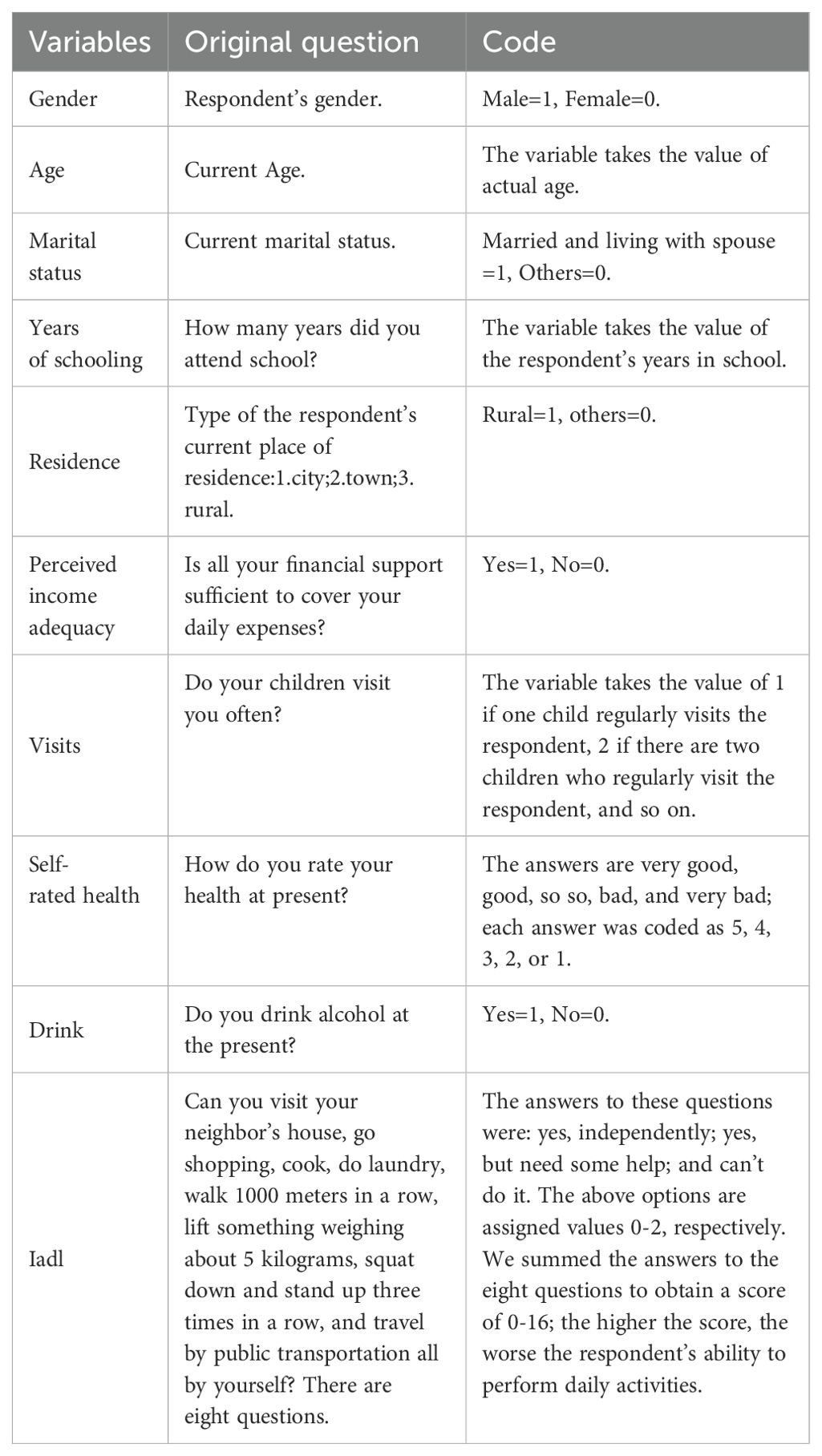
Table 1. Summary of the covariates.
3.5 Research methodology
First, we visualized the effect of living alone on depressive symptoms by describing the data on various variables for the overall sample, the sample of older adults living alone, and the sample of older adults not living alone.
Second, we tested the effect of the living alone variable on depressive symptoms by performing a multiple regression using the R software. As shown in Figure 1, we included the living alone variable and the covariates in the regression equation. Then, we placed the dietary variables such as fruits, vegetables, and nuts into the regression equation. In this way, we tested the H1 hypothesis by regression analysis.
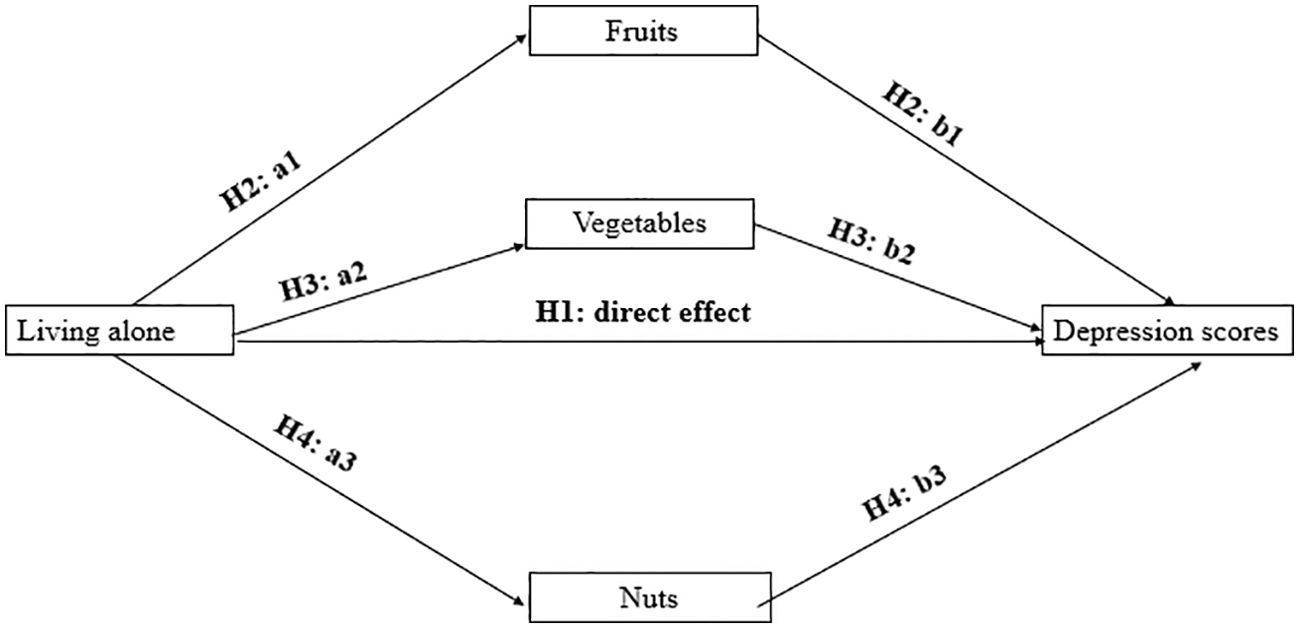
Figure 1. Empirical research hypothesis.
Finally, as hypothesized in the previous section, we believe that living alone indirectly affects depressive symptoms through three mediating pathways, including fruit, vegetable, and nut consumption. We will use the structural equation approach in the R package lavaan to derive the pathway coefficients of living alone on depression and the bootstrap approach to derive confidence intervals for the coefficients. Thus, through mediated effects analysis, we test hypotheses H2, H3, and H4, respectively.
4 Results
4.1 Data description
After excluding samples with missing values on the variables included in the analysis, the samples used in our study had 6,162 respondents, of which 9,90 lived alone and 5,172 lived in nursing homes or with their families.
The depression levels of the different groups are shown in Table 2 below. The highest level of depression is found among older adults living alone, with an average of 22.83, while the lowest level of depression is found among those living with their families or in nursing homes, with an average of 21.29. The data intuitively reflects that older people living alone have poorer levels of mental health.
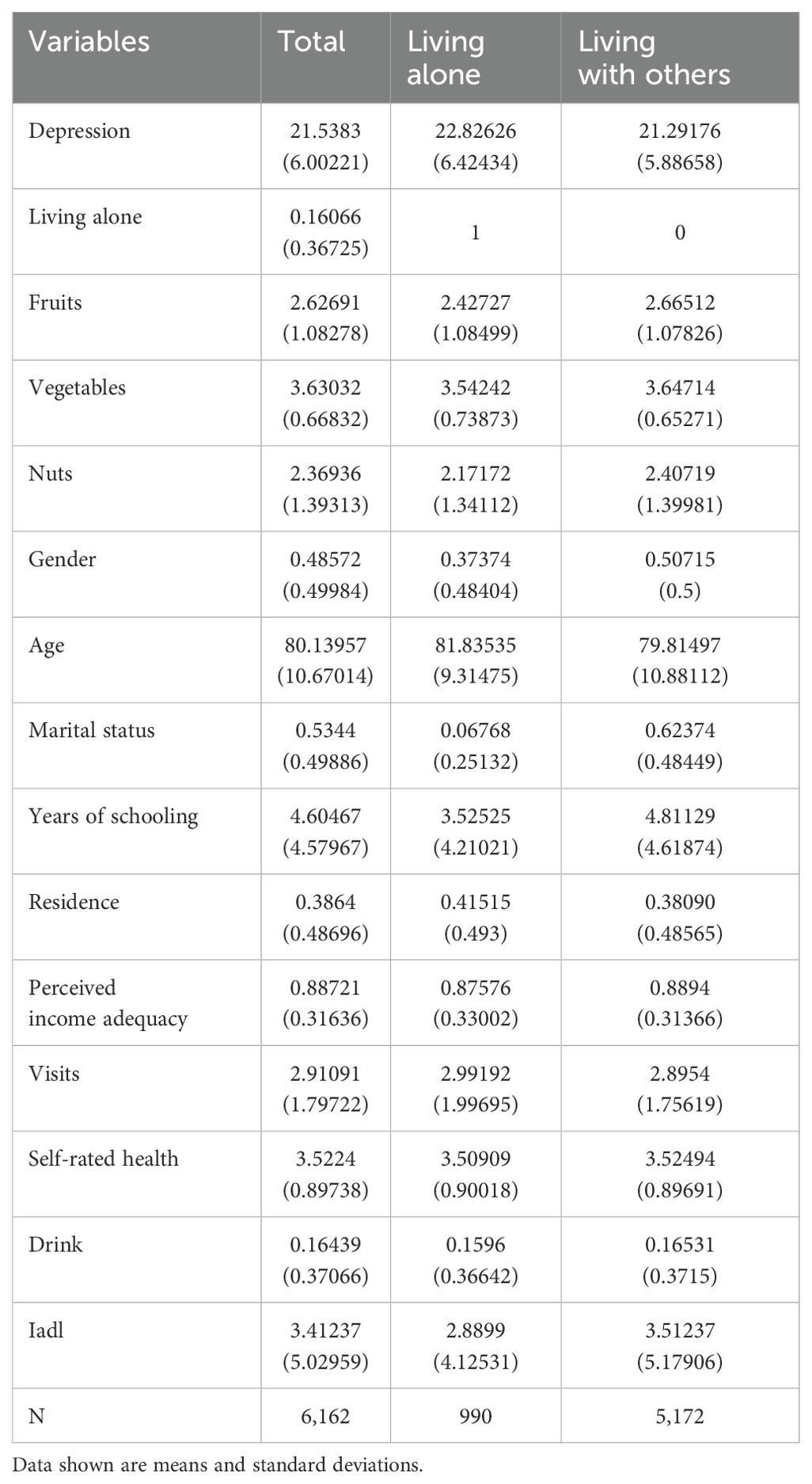
Table 2. Descriptive statistics of the variables.
In terms of healthy diet and other covariates, older people living alone had lower consumption of fruits, vegetables, and nuts than older people who did not live alone. In addition, regarding the consumption of the three foods, vegetables were consumed the most. In contrast, nuts were consumed the least, possibly related to the deterioration of dental function in older people. In terms of covariates, older people living alone had a high mean age, a higher proportion of females, a lower proportion of marriage, fewer years of schooling, poorer economic conditions, and poorer self-rated health; however, older people living alone had lower IADL values, a lower proportion of alcohol consumption, and higher index of children’s visits.
4.2 Overall sample regression
We used two multiple regression equations in the overall sample regression to examine the effect of living alone on depressive symptoms, and the results are presented in Table 3. In the first model, we used the living alone variable and covariates. In model 2, we used the living alone variable, covariates, and healthy diet variables.
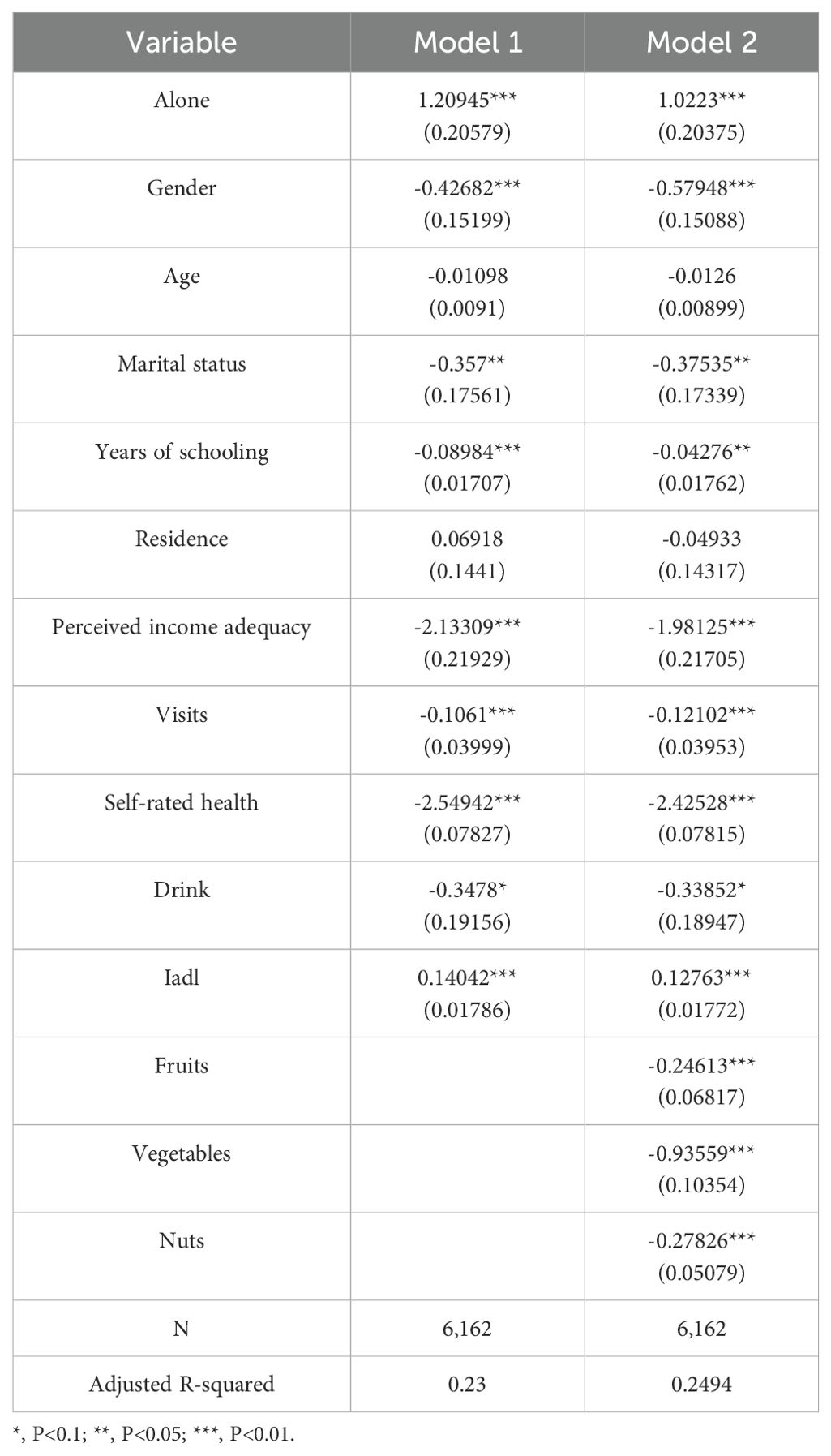
Table 3. Regression results of the effect of living alone on depression.
In Model 1, the variance inflation factors for all variables are below 3, ranging from a minimum of 1.07 to a maximum of 2.09; in Model 2, the variance inflation factors for all variables are below 3, with a minimum of 1.07 and a maximum of 2.1, which is much lower than 10, showing that multicollinearity was not a problem in our regression models (81).
The regression results of Model 1 show that living alone positively affects depression values, increasing to 1.21 in depression scores, and the coefficient is significant. The variables of gender, marital status, children’s visits, self-rated health, years of schooling, and perceived income adequacy were all negatively associated with depression scores. The IADL variable had a positive effect on depression. The above regression coefficients are consistent with the results of most studies.
The results of Model 2 show that the coefficient of the effect of living alone on depression becomes smaller at 1.02 with the introduction of the healthy diet variable, and the coefficients of the covariates change slightly compared to Model 1. All three variables of healthy diet had a negative effect on depression.
The results of Model 1 and Model 2 confirm the H1 hypothesis that living alone leads to a significant increase in depression scores.
4.3 Mediation analysis
As hypothesized in the previous section, there are three pathways for the indirect effect of living alone on depression scores. We conducted path analyses using the Lavaan package in R software. The covariates are consistent with the regression equations described above. The path coefficients are shown in Figure 2 below, where the paths for the effect of fruit consumption on depression values are denoted by H2a1 and H2b1, with living alone negatively correlated with fruit consumption, β= -0.17, P(>|z|)=0.000, and fruit consumption is negatively correlated with depression scores, β= -0.246, P(>|z|)=0.000. The paths for the effect of vegetable consumption on depression values are denoted by H3a2 and H3b2, where living alone is negatively associated with vegetable consumption, β=-0.108, P(>|z|)=0.000, and vegetable consumption is negatively associated with depression scores, β= -0.936, P(>|z|)=0.000. The paths for the effect of nuts consumption on depression values are represented by H4a3 and H4b3, where living alone is negatively associated with nuts consumption, β= -0.159, P(> |z|)=0.002, and nuts consumption is negatively associated with depression scores, β= -0.278, P(>|z|)=0.000.
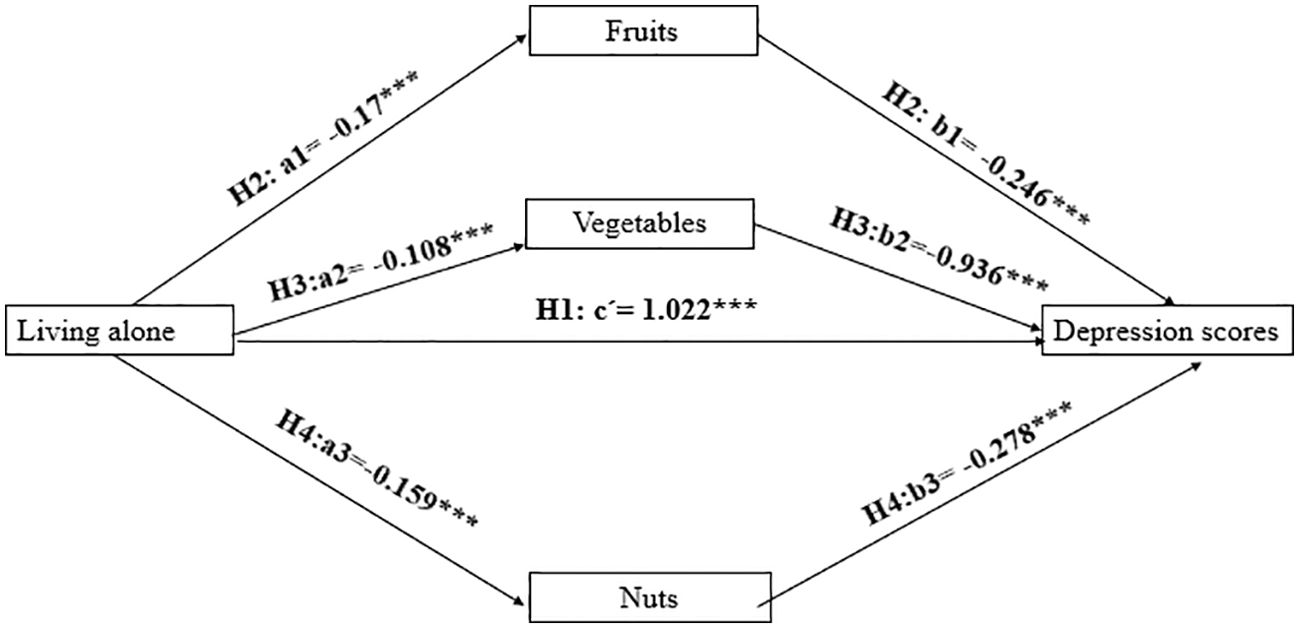
Figure 2. Path analysis. *, P<0.1; **, P<0.05; ***, P<0.01.
The coefficients of the above path analyses are all significant, but statistical tests are needed to confirm the existence of mediating effects. And some scholars believe that bootstrapping was a good test. It has been argued that bootstrapping is a reasonable method for obtaining confidence intervals for the indirect effect under most conditions (82). The mediation effect test is generally a test of the significance of the product of two coefficients a*b (83).
Therefore, we use 1,000 times of bootstrapping to test the mediation effect and obtain a 95% confidence interval (CI). The results are shown in Table 4 below. None of the upper and lower bounds of the confidence intervals of the bootstrapped a*b coefficients contain 0. Therefore, the mediating effect holds, and all three hypotheses, H2, H3, and H4, are valid.

Table 4. The mediation effect test.
5 Discussion and policy recommendations
5.1 Main findings
To the best of our knowledge, this is one of the few studies focusing on the relationship between living alone, healthy diet, and mental health based on a sample of older adults in China. This paper expands the feasible perspective of mental health interventions for older adults living alone.
First, our study found that living alone can have a detrimental effect on the mental health of older adults. This is consistent with many existing studies; for example, a study in northern China found that the regression coefficient of living alone on depressive symptoms in older adults was 2.695 (84). Another regression analysis found a significant association between living alone and depressive symptoms in older adults, β= 0.842 (85). As the description of the data in the previous section shows, very few older adults living alone have spouses and, therefore, lack spousal support; in addition, older adults living alone have a lower level of education. As a result, living alone often leads to a deterioration in the mental health of older persons.
Second, healthy eating played an important mediating role between living alone and older adults’ mental health. Healthy eating affects the mental health of older adults through three channels, namely, fruits, vegetables, and nuts, respectively, and the indirect effects of these three channels accounted for 15.47% of the total impact of living alone on depression scores of older adults. Among them, vegetable intake had the most significant effect on depression scores, accounting for 8.35% of the total impact, followed by nuts and fruits. The reason may be that vegetables are an important feature of the traditional Chinese diet (86). Our findings are consistent with those of many studies, such as one study found that the higher the intake of vegetables and fruits, the lower the risk of depressive symptoms (87). This finding is important because the intake of vegetables, fruits, and nuts, among others, is related to ease of purchase and the financial income of older people. And in urban China, most families can buy fresh vegetables within walking distance (88). In rural China, however, the situation becomes different. Traditionally, rural households consume mainly home-grown food (89). Nowadays, although rural residents have also begun to go out to buy food, the retail system in rural areas is not sound, and supermarket chains and rural e-commerce are still underdeveloped, unable to meet the growing material needs of the rural population (90). Therefore, older adults living alone in rural areas face more difficulty consuming healthy food. In practice, we find that rural Chinese residents consume less vegetables and fruits than urban residents (91).
5.2 Policy recommendations
Based on our study, we make the following recommendations. Firstly, as China’s aging process deepens, compounded by a declining fertility rate, more and more older people will live alone in China. This is a large and vulnerable group, and high priority should be given to improving their mental health to achieve healthy aging. Second, some older adults living alone have a poorer financial situation, especially in rural areas. The government should care about them and provide livelihood protection to low-income older adults so that they can afford to buy healthy food.
Finally, given the important mediating role of healthy eating in the relationship between living alone and mental health, attention should be given to facilitating the purchase of healthy food for older persons at the community level. For example, food service vouchers can be provided to older adults living alone, and commercial organizations can be introduced to provide older adults living alone with services such as purchasing vegetables, fruits, and nuts on their behalf and cooking for them. In addition, a study in China, for example, found that community canteen services can improve the general mental health of older adults (92). Therefore, we propose to set up canteens in communities with many older adults living alone so that they can eat more healthily, thereby improving their mental health.
5.3 Limitations
Our study also has shortcomings; first, we derive a statistical relationship between the variables. However it is difficult to conclude a causal relationship between the variables due to the use of cross-sectional data; therefore, more in-depth analysis using panel data should be conducted in the future. Secondly, the questionnaire did not inquire in more detail about how and where the older adults living alone purchased fruits and vegetables, so we could not infer the objective reasons affecting the consumption of fruits and vegetables by older adults living alone. Third, the research questionnaire did not include more detailed information on the consumption of fruits, vegetables, nuts, etc., but only on the frequency of consumption; similarly, the assessment of alcohol intake does not indicate the frequency and amount of intake and future studies should use more detailed data for analysis. At the same time, older adults living alone may also have problems with their diet, such as consuming stale leftovers. Therefore, more in-depth research should be conducted on the nutritional elements that affect the mental health of older adults (93).
6 Conclusion
This study identifies mechanisms by which healthy eating mediates the relationship between living alone and mental health. It was found that older people living alone are a vulnerable group with poorer mental health and a lower intake of healthy foods such as fruits, vegetables, and nuts, which can have an impact on their mental health. The findings suggest that healthy eating is a feasible intervention to improve the mental health of older adults living alone and that the Government can provide low-income older people living alone with livelihood protection so that they can afford to buy healthy food; at the same time, the Government should take diversified initiatives at the community level to enhance the healthy diet of older persons living alone.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://opendata.pku.edu.cn/dataset.xhtml?persistentId=doi:10.18170/DVN/WBO7LK.
Ethics statement
The studies involving humans were approved by the Biomedical Ethics Committee of Peking University (IRB00001052-13074). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JZ: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. ZN: Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. United Nations, Department of Economic and Social Affairs, and Population Division. Living Arrangements of Older Persons: A Report on an Expanded International Dataset(2017). Available online at: https://www.un.org/en/development/desa/population/publications/pdf/ageing/LivingArrangements.pdf (Accessed October 16, 2024).
2. STATS. China Statistical Yearbook (2023). Available online at: https://www.stats.gov.cn/sj/ndsj/2023/indexch.htm (Accessed October 16, 2024).
3. Wang J, Chen T, and Han B. Does co-residence with adult children associate with better psychological well-being among the oldest old in China? Aging Ment Health. (2014) 18:232–9. doi: 10.1080/13607863.2013.837143
4. Liu N, Andrew NE, Cadilhac DA, Yu X, Li Z, Wang J, et al. Health-related quality of life among elderly individuals living alone in an urban area of Shaanxi Province, China: a cross-sectional study. J Int Med Res. (2020) 48:300060520913146. doi: 10.1177/0300060520913146
5. Wang L and Mesman J. Child development in the face of rural-to-urban migration in China: A meta-analytic review. Perspect Psychol Sci. (2015) 10:813–31. doi: 10.1177/1745691615600145
6. Myerson R, Lu T, Yuan Y, and Liu GG-E. Cancer diagnosis and care among rural-to-urban migrants in China. BMJ Glob Health. (2019) 4:e001923. doi: 10.1136/bmjgh-2019-001923
7. Li S, Zhang J, Wu C, Lu Y, Xu L, Ni Y, et al. The mediating effect of coping style on the relationship between perceived stress and mental health in Chinese rural older adults living alone: A cross-sectional study. Geriatrics Gerontol Int. (2022) 22:523–8. doi: 10.1111/ggi.14392
8. STATS. China Population Census Year Book (2020). Available online at: https://www.stats.gov.cn/sj/pcsj/rkpc/7rp/zk/indexch.htm (Accessed October 16, 2024).
9. Santomauro DF, Mantilla Herrera AM, Shadid J, Zheng P, Ashbaugh C, Pigott DM, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. (2021) 398:1700–12. doi: 10.1016/S0140-6736(21)02143-7
10. Akpınar Ş and Karadağ MG. Is vitamin D important in anxiety or depression? What is the truth? Curr Nutr Rep. (2022) 11:675–81. doi: 10.1007/s13668-022-00441-0
11. Cui R. Editorial (Thematic selection: A systematic review of depression). Curr Neuropharmacol. (2015) 13:480–0. doi: 10.2174/1570159X1304150831123535
12. GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1789–858. doi: 10.1016/S0140-6736(18)32279-7
13. Alexopoulos GS. Depression in the elderly. Lancet. (2005) 365:1961–70. doi: 10.1016/S0140-6736(05)66665-2
14. Szymkowicz SM, Gerlach AR, Homiack D, and Taylor WD. Biological factors influencing depression in later life: role of aging processes and treatment implications. Transl Psychiatry. (2023) 13:160. doi: 10.1038/s41398-023-02464-9
15. Chen Y. Risk factors for depression among older adults living alone in Shanghai, China. Psychogeriatrics. (2022) 22:780–5. doi: 10.1111/psyg.12882
16. Tong HM, Lai DWL, Zeng Q, and Xu WY. Effects of social exclusion on depressive symptoms: elderly Chinese living alone in Shanghai, China. J Cross Cult Gerontol. (2011) 26:349–64. doi: 10.1007/s10823-011-9150-1
17. Du Q, Gong N, Hu Q, Chen G, Xie J, Luo L, et al. Why do older adults living alone in cities cease seeking assistance? A qualitative study in China. BMC Geriatr. (2022) 22:540. doi: 10.1186/s12877-022-03217-x
18. Wu B, Xiong G, Zhang P, and Ma X. Effects of tai chi, ba duan jin, and walking on the mental health status of urban older people living alone: the mediating role of social participation and the moderating role of the exercise environment. Front Public Health. (2024) 12:1294019. doi: 10.3389/fpubh.2024.1294019
19. Nishio M, Takagi D, Shinozaki T, and Kondo N. Community social networks, individual social participation and dietary behavior among older Japanese adults: Examining mediation using nonlinear structural equation models for three-wave longitudinal data. Prev Med. (2021) 149:106613. doi: 10.1016/j.ypmed.2021.106613
20. Huang M, Liu K, Liang C, Wang Y, and Guo Z. The relationship between living alone or not and depressive symptoms in older adults: a parallel mediation effect of sleep quality and anxiety. BMC Geriatr. (2023) 23:506. doi: 10.1186/s12877-023-04161-0
21. Sarris J, Ravindran A, Yatham LN, Marx W, Rucklidge JJ, McIntyre RS, et al. Clinician guidelines for the treatment of psychiatric disorders with nutraceuticals and phytoceuticals: The World Federation of Societies of Biological Psychiatry (WFSBP) and Canadian Network for Mood and Anxiety Treatments (CANMAT) Taskforce. World J Biol Psychiatry. (2022) 23:424–55. doi: 10.1080/15622975.2021.2013041
22. Lai JS, Hiles S, Bisquera A, Hure AJ, McEvoy M, and Attia J. A systematic review and meta-analysis of dietary patterns and depression in community-dwelling adults. Am J Clin Nutr. (2014) 99:181–97. doi: 10.3945/ajcn.113.069880
23. Parletta N, Zarnowiecki D, Cho J, Wilson A, Bogomolova S, Villani A, et al. A Mediterranean-style dietary intervention supplemented with fish oil improves diet quality and mental health in people with depression: A randomized controlled trial (HELFIMED). Nutr Neurosci. (2019) 22:474–87. doi: 10.1080/1028415X.2017.1411320
24. Park NS, Jang Y, Lee BS, and Chiriboga DA. The relation between living alone and depressive symptoms in older Korean Americans: do feelings of loneliness mediate? Aging Ment Health. (2017) 21:304–12. doi: 10.1080/13607863.2015.1099035
25. Routasalo PE, Savikko N, Tilvis RS, Strandberg TE, and Pitkälä KH. Social contacts and their relationship to loneliness among aged people – A population-based study. Gerontology. (2006) 52:181–7. doi: 10.1159/000091828
26. Tong H, Hou WK, Liang L, Li TW, Liu H, and Lee TMC. Age-related differences of rumination on the loneliness-depression relationship: evidence from a population-representative cohort. Innov Aging. (2021) 29:igab034. doi: 10.1093/geroni/igab034
27. Widhowati SS, Chen C-M, Chang L-H, Lee C-K, and Fetzer S. Living alone, loneliness, and depressive symptoms among Indonesian older women. Health Care Women Int. (2020) 41:984–96. doi: 10.1080/07399332.2020.1797039
28. Koo JH, Son N, and Yoo K-B. Relationship between the living-alone period and depressive symptoms among the elderly. Arch Gerontol Geriatrics. (2021) 94:104341. doi: 10.1016/j.archger.2021.104341
29. Kim K and Lee M. Depressive symptoms of older adults living alone: the role of community characteristics. Int J Aging Hum Dev. (2015) 80:248–63. doi: 10.1177/0091415015590315
30. Wei K, Liu Y, Yang J, Gu N, Cao X, Zhao X, et al. Living arrangement modifies the associations of loneliness with adverse health outcomes in older adults: evidence from the CLHLS. BMC Geriatr. (2022) 22:59. doi: 10.1186/s12877-021-02742-5
31. Gallagher DE, Thompson LW, and Peterson JA. Psychosocial factors affecting adaptation to bereavement in the elderly. Int J Aging Hum Dev. (1982) 14:79–95. doi: 10.2190/J72R-28RK-QVPJ-P71Q
32. Fingerman KL, Ng YT, Zhang S, Britt K, Colera G, Birditt KS, et al. Living alone during COVID-19: social contact and emotional well-being among older adults. Journals Gerontol: Ser B. (2021) 76:e116–21. doi: 10.1093/geronb/gbaa200
33. Sok SR and Yun EK. A comparison of physical health status, self-esteem, family support and health-promoting behaviours between aged living alone and living with family in Korea. J Clin Nurs. (2011) 20:1606–12. doi: 10.1111/j.1365-2702.2010.03551.x
34. Joutsenniemi K, Martelin T, Martikainen P, Pirkola S, and Koskinen S. Living arrangements and mental health in Finland. J Epidemiol Community Health. (2006) 60:468–75. doi: 10.1136/jech.2005.040741
35. Kobayashi E, Harada K, Okamoto S, and Liang J. Living alone and depressive symptoms among older Japanese: do urbanization and time period matter? Journals Gerontol: Ser B. (2023) 78:718–29. doi: 10.1093/geronb/gbac195
36. Zheng G, Zhou B, Fang Z, Jing C, Zhu S, Liu M, et al. Living alone and the risk of depressive symptoms: a cross-sectional and cohort analysis based on the China Health and Retirement Longitudinal Study. BMC Psychiatry. (2023) 23:853. doi: 10.1186/s12888-023-05370-y
37. Hepsomali P and Groeger JA. Diet, sleep, and mental health: insights from the UK biobank study. Nutrients. (2021) 13:2573. doi: 10.3390/nu13082573
38. Guasch-Ferré M and Willett WC. The Mediterranean diet and health: a comprehensive overview. J Intern Med. (2021) 290:549–66. doi: 10.1111/joim.13333
39. Willett W, Sacks F, Trichopoulou A, Drescher G, Ferro-Luzzi A, Helsing E, et al. Mediterranean diet pyramid: a cultural model for healthy eating. Am J Clin Nutr. (1995) 61:1402S–6S. doi: 10.1093/ajcn/61.6.1402S
40. Fangfang H, Qiong W, Shuai Z, Xiao H, Jingya Z, Guodong S, et al. Vegetable and fruit intake, its patterns, and cognitive function: cross-sectional findings among older adults in Anhui, China. J nutrition Health aging. (2022) 26:529–36. doi: 10.1007/s12603-022-1791-y
41. Hu XF, Zhang R, and Chan HM. Identification of Chinese dietary patterns and their relationships with health outcomes: a systematic review and meta-analysis. Public Health Nutr. (2024) 27:e209. doi: 10.1017/S1368980024001927
42. Yang YX, Wang XL, Leong PM, Zhang HM, Yang XG, Kong LZ, et al. New Chinese dietary guidelines: healthy eating patterns and food-based dietary recommendations. Asia Pac J Clin Nutr. (2018) 27:908–13. doi: 10.6133/apjcn.072018.03
43. Choi YR, Park HR, Song KH, Lee Y, and Lim YS. Disparities in dietary quantity and quality between the two different types of Korean family of older adults living with spouses and living alone: using data from the 6th Korea National Health and Nutrition Examination Survey. Nutr Res Pract. (2020) 14:242–51. doi: 10.4162/nrp.2020.14.3.242
44. Wilson-Genderson M, Heid AR, Cartwright F, Collins AL, and Pruchno R. Change in loneliness experienced by older men and women living alone and with others at the onset of the COVID-19 pandemic. Res Aging. (2022) 44:369–81. doi: 10.1177/01640275211026649
45. Liu N, Zeng L, Li Z, and Wang J. Health-related quality of life and long-term care needs among elderly individuals living alone: a cross-sectional study in rural areas of Shaanxi Province, China. BMC Public Health. (2013) 13:313. doi: 10.1186/1471-2458-13-313
46. Jones NRV, Conklin AI, Suhrcke M, and Monsivais P. The growing price gap between more and less healthy foods: analysis of a novel longitudinal UK dataset. PLoS One. (2014) 9:e109343. doi: 10.1371/journal.pone.0109343
47. Kern DM, Auchincloss AH, Stehr MF, Roux AVD, Moore LV, Kanter GP, et al. Neighborhood prices of healthier and unhealthier foods and associations with diet quality: evidence from the multi-ethnic study of atherosclerosis. Int J Environ Res Public Health. (2017) 14:1394. doi: 10.3390/ijerph14111394
48. Henning-Smith C. Quality of life and psychological distress among older adults: the role of living arrangements. J Appl Gerontol. (2016) 35:39–61. doi: 10.1177/0733464814530805
49. Hilger-Kolb J and Diehl K. ‘Oh god, I have to eat something, but where can I get something quickly?’-A qualitative interview study on barriers to healthy eating among university students in Germany. Nutrients. (2019) 11:2440. doi: 10.3390/nu11102440
50. Dean M, Raats MM, Grunert KG, Lumbers M, and The Food in Later Life Team. Factors influencing eating a varied diet in old age. Public Health Nutr. (2009) 12:2421–7. doi: 10.1017/s1368980009005448
51. Quandt SA, McDonald J, Arcury TA, Bell RA, and Vitolins MZ. Nutritional self-management of elderly widows in rural communities. Gerontologist. (2000) 40:86–96. doi: 10.1093/geront/40.1.86
52. Wham CA and Bowden JA. Eating for health: Perspectives of older men who live alone. Nutr Dietetics. (2011) 68:221–6. doi: 10.1111/j.1747-0080.2011.01535.x
53. Tani Y, Fujiwara T, Anzai T, and Kondo K. Cooking skills, living alone, and mortality: JAGES cohort study. Int J Behav Nutr Phys Act. (2023) 20:131. doi: 10.1186/s12966-023-01522-1
54. Choi YJ, Ailshire JA, and Crimmins EM. Living alone, social networks in neighbourhoods, and daily fruit and vegetable consumption among middle-aged and older adults in the USA. Public Health Nutr. (2020) 23:3315–23. doi: 10.1017/S1368980020002475
55. Phulkerd S, Gray RS, and Chamratrithirong A. The influence of co-residential and non-co-residential living arrangements on sufficient fruit and vegetable consumption in the aging population in Thailand. BMC Geriatr. (2020) 20:476. doi: 10.1186/s12877-020-01884-2
56. Głąbska D, Guzek D, Groele B, and Gutkowska K. Fruit and vegetable intake and mental health in adults: A systematic review. Nutrients. (2020) 12:115. doi: 10.3390/nu12010115
57. Huang P, O’Keeffe M, Elia C, Karamanos A, Goff LM, Maynard M, et al. Fruit and vegetable consumption and mental health across adolescence: evidence from a diverse urban British cohort study. Int J Behav Nutr Phys Act. (2019) 16:19. doi: 10.1186/s12966-019-0780-y
58. Xu Q-H, Yang T, Jiang K-Y, Liu J-D, Guo H-H, and Xia E-Q. The association between the number of food kinds and risk of depression in U.S. adults. BMC Public Health. (2024) 24:2575. doi: 10.1186/s12889-024-19344-6
59. Dang R, Wang M, Li X, Wang H, Liu L, Wu Q, et al. Edaravone ameliorates depressive and anxiety-like behaviors via Sirt1/Nrf2/HO-1/Gpx4 pathway. J Neuroinflammation. (2022) 19:41. doi: 10.1186/s12974-022-02400-6
60. Beurel E, Toups M, and Nemeroff CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. (2020) 107:234–56. doi: 10.1016/j.neuron.2020.06.002
61. Kiecolt-Glaser JK, Derry HM, and Fagundes CP. Inflammation: depression fans the flames and feasts on the heat. Am J Psychiatry. (2015) 172:1075–91. doi: 10.1176/appi.ajp.2015.15020152
62. Correia AS, Cardoso A, and Vale N. Oxidative stress in depression: the link with the stress response, neuroinflammation, serotonin, neurogenesis and synaptic plasticity. Antioxidants (Basel). (2023) 12:470. doi: 10.3390/antiox12020470
63. Maes M, Galecki P, Chang YS, and Berk M. A review on the oxidative and nitrosative stress (O&NS) pathways in major depression and their possible contribution to the (neuro)degenerative processes in that illness. Prog Neuropsychopharmacol Biol Psychiatry. (2011) 35:676–92. doi: 10.1016/j.pnpbp.2010.05.004
64. Serafini M and Peluso I. Functional foods for health: the interrelated antioxidant and anti-inflammatory role of fruits, vegetables, herbs, spices and cocoa in humans. CPD. (2017) 22:6701–15. doi: 10.2174/1381612823666161123094235
65. Prior RL. Fruits and vegetables in the prevention of cellular oxidative damage. Am J Clin Nutr. (2003) 78:570S–8S. doi: 10.1093/ajcn/78.3.570S
66. Di Giosia P, Stamerra CA, Giorgini P, Jamialahamdi T, Butler AE, and Sahebkar A. The role of nutrition in inflammaging. Ageing Res Rev. (2022) 77:101596. doi: 10.1016/j.arr.2022.101596
67. Santoro A, Pini E, Scurti M, Palmas G, Berendsen A, Brzozowska A, et al. Combating inflammaging through a Mediterranean whole diet approach: The NU-AGE project’s conceptual framework and design. Mech Ageing Dev. (2014) 136–137:3–13. doi: 10.1016/j.mad.2013.12.001
68. Sureda A and Tejada S. Polyphenols and depression: from chemistry to medicine. Curr Pharm Biotechnol. (2015) 16:259–64. doi: 10.2174/1389201016666150118133313
69. Gantenbein KV and Kanaka-Gantenbein C. Mediterranean diet as an antioxidant: the impact on metabolic health and overall wellbeing. Nutrients. (2021) 13:1951. doi: 10.3390/nu13061951
70. Akbaraly TN, Brunner EJ, Ferrie JE, Marmot MG, Kivimaki M, and Singh-Manoux A. Dietary pattern and depressive symptoms in middle age. Br J Psychiatry. (2009) 195:408–13. doi: 10.1192/bjp.bp.108.058925
71. Pano O, Martínez-Lapiscina EH, Sayón-Orea C, Martinez-Gonzalez MA, Martinez JA, and Sanchez-Villegas A. Healthy diet, depression and quality of life: A narrative review of biological mechanisms and primary prevention opportunities. WJP. (2021) 11:997–1016. doi: 10.5498/wjp.v11.i11.997
72. Staudacher HM, Teasdale S, Cowan C, Opie R, Jacka FN, and Rocks T. Diet interventions for depression: Review and recommendations for practice. Aust N Z J Psychiatry. (2025) 59:115–27. doi: 10.1177/00048674241289010
73. Center For Healthy Aging And Development Studies. The Chinese Longitudinal Healthy Longevity Survey (CLHLS)-Longitudinal Data(1998-2018). (2020). Available online at: https://opendata.pku.edu.cn/dataset.xhtml?persistentId=doi:10.18170/DVN/WBO7LK (Accessed October 16, 2024).
74. Ishikawa S, Konta T, Susa S, Ishizawa K, Togashi H, Ueno Y, et al. Association between presence of 20 or more natural teeth and all-cause, cancer-related, and cardiovascular disease-related mortality: Yamagata (Takahata) prospective observational study. BMC Oral Health. (2020) 20:353. doi: 10.1186/s12903-020-01346-6
75. Fukai K, Dartevelle S, and Jones J. Oral health for healthy ageing: A people-centred and function-focused approach. Int Dent J. (2022) 72:S2–4. doi: 10.1016/j.identj.2022.06.00
76. Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Appl psychol Measurement. (1977) 1:385–401. doi: 10.1177/014662167700100306
77. Andresen EM, Malmgren JA, Carter WB, and Patrick DL. Screening for depression in well older adults: evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale). Am J Prev Med. (1994) 10:77–84. doi: 10.1016/S0749-3797(18)30622-6
78. Qin A, Wang M, and Xu L. Increased intake of vegetables and fruits improves cognitive function among Chinese oldest old: 10-year follow-up study. Nutrients. (2023) 15:2147. doi: 10.3390/nu15092147
79. Zhang J, Wang Q, Hao W, and Zhu D. Long-term food variety and dietary patterns are associated with frailty among Chinese older adults: A cohort study based on CLHLS from 2014 to 2018. Nutrients. (2022) 14:4279. doi: 10.3390/nu14204279
80. Moon JR, Glymour MM, Vable AM, Liu SY, and Subramanian SV. Short- and long-term associations between widowhood and mortality in the United States: longitudinal analyses. J Public Health. (2014) 36:382–9. doi: 10.1093/pubmed/fdt101
81. Vatcheva KP, Lee M, McCormick JB, and Rahbar MH. Multicollinearity in regression analyses conducted in epidemiologic studies. Epidemiol (Sunnyvale). (2016) 6:227. doi: 10.4172/2161-1165.1000227
82. Preacher KJ and Hayes AF. Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behav Res Methods. (2008) 40:879–91. doi: 10.3758/brm.40.3.879
83. Cheung GW and Lau RS. Testing mediation and suppression effects of latent variables: bootstrapping with structural equation models. Organizational Res Methods. (2008) 11:296–325. doi: 10.1177/1094428107300343
84. Sun Q, Wang Y, Lu N, and Lyu S. Intergenerational support and depressive symptoms among older adults in rural China: the moderating roles of age, living alone, and chronic diseases. BMC Geriatr. (2022) 22:83. doi: 10.1186/s12877-021-02738-1
85. Fang H, Duan Y, Hou Y, Chang H, Hu S, and Huang R. The association between living alone and depressive symptoms in older adults population: evidence from the China Health and Retirement Longitudinal Study. Front Public Health. (2024) 12:1441006. doi: 10.3389/fpubh.2024.1441006
86. Jiang K, Zhang Z, Fullington LA, Huang TT, Kaliszewski C, Wei J, et al. Dietary patterns and obesity in Chinese adults: A systematic review and meta-analysis. Nutrients. (2022) 14:4911. doi: 10.3390/nu14224911
87. Cheng H-Y, Shi Y-X, Yu F-N, Zhao H-Z, Zhang J-H, and Song M. Association between vegetables and fruits consumption and depressive symptoms in a middle-aged Chinese population: An observational study. Medicine. (2019) 98:e15374. doi: 10.1097/md.0000000000015374
88. Si Z, Scott S, and McCordic C. Wet markets, supermarkets and alternative food sources: consumers’ food access in Nanjing, China. Can J Dev Studies/Revue Can d’études du développement. (2018) 40:78–96. doi: 10.1080/02255189.2018.1442322
89. Gale F, Tang P, Bai X, and Xu H. Commercialization of food consumption in rural China. (2005). Available online at: https://primary.ers.usda.gov/publications/pub-details?pubid=46247 (Accessed October 16, 2024).
90. Li ML, Lu K, and Shang MM. Synergistic supply, heterogeneous demand and long-term mechanism of retailing in rural areas–empirical evidence based on Guangxi county data. Res Business Economy. (2023) 6:97–100.
91. Li YC, Jiang B, Zhang M, Huang ZJ, Deng Q, Zhou MG, et al. Vegetable and fruit consumption among Chinese adults and associated factors: A nationally representative study of 170,847 adults. BioMed Environ Sci. (2017) 30:863–74. doi: 10.3967/bes2017.117
92. Wang X, Liu M, Li Y, Guo C, and Yeh CH. Community canteen services for the rural elderly: determining impacts on general mental health, nutritional status, satisfaction with life, and social capital. BMC Public Health. (2020) 20. doi: 10.1186/s12889-020-8305-9
Keywords: living alone, mental health, depressive symptoms, healthy diet, older adults
Citation: Zheng J and Ni Z (2025) The impact of living alone on older adults’ mental health and the mediating role of healthy diet. Front. Psychiatry 16:1562487. doi: 10.3389/fpsyt.2025.1562487
Received: 17 January 2025; Accepted: 06 May 2025;
Published: 29 May 2025.
Edited by:
Emilia Vassilopoulou, International Hellenic University, GreeceReviewed by:
Aixiang Xiao, Guangzhou Medical University, ChinaDona Hileti, University of Nicosia, Cyprus
Copyright © 2025 Zheng and Ni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jichao Zheng, MTQyOTA3MTAxMEBxcS5jb20=