 Rocío Gómez-Ballesteros1*
Rocío Gómez-Ballesteros1* Susana Sainz de la Maza2
Susana Sainz de la Maza2 Mónica Borges3
Mónica Borges3 Jesús Martín-Martínez4Javier Sotoca5
Jesús Martín-Martínez4Javier Sotoca5 Ana Alonso6
Ana Alonso6 Ana B. Caminero7Laura Borrega8José L. Sánchez-Menoyo9
Ana B. Caminero7Laura Borrega8José L. Sánchez-Menoyo9 Francisco J. Barrero-Hernández10
Francisco J. Barrero-Hernández10 Carmen Calles11
Carmen Calles11 Luis Brieva12
Luis Brieva12 María R. Blasco-Quílez13Julio Dotor García-Soto3Ana Rodríguez-Regal14
María R. Blasco-Quílez13Julio Dotor García-Soto3Ana Rodríguez-Regal14 Laura Navarro-Cantó15
Laura Navarro-Cantó15 Eduardo Agüera16Moisés Garcés-Redondo17Olga Carmona18
Eduardo Agüera16Moisés Garcés-Redondo17Olga Carmona18 Laura Gabaldón-Torres19
Laura Gabaldón-Torres19 Lucía Forero20Mariona Hervás21
Lucía Forero20Mariona Hervás21 Tamara Castillo-Triviño22
Tamara Castillo-Triviño22 Jorge Maurino1
Jorge Maurino1- 1Medical Department, Roche Farma, Madrid, Spain
- 2Department of Neurology, Hospital Universitario Ramón y Cajal, Madrid, Spain
- 3Department of Neurology, Hospital Universitario Virgen Macarena, Sevilla, Spain
- 4Department of Neurology, Hospital Universitario Miguel Servet, Zaragoza, Spain
- 5Department of Neurology, Hospital Universitari Mútua Terrassa, Terrassa, Spain
- 6Department of Neurology, Hospital Regional Universitario de Málaga, Málaga, Spain
- 7Department of Neurology, Complejo Asistencial de Ávila, Ávila, Spain
- 8Department of Neurology, Hospital Universitario Fundación Alcorcón, Alcorcón, Spain
- 9Department of Neurology, Hospital de Galdakao-Usansolo, Galdakao, Spain
- 10Department of Neurology, Hospital Universitario Clínico San Cecilio, Granada, Spain
- 11Department of Neurology, Hospital Universitari Son Espases, Palma de Mallorca, Spain
- 12Department of Neurology, Hospital Arnau de Vilanova de Lleida, UdL Medicine Department, Instituto de Investigación Biomédica de Lleida (IRBLleida), Lleida, Spain
- 13Department of Neurology, Hospital Universitario Puerta de Hierro, Madrid, Spain
- 14Department of Neurology, Complexo Hospitalario Universitario de Pontevedra, Pontevedra, Spain
- 15Department of Neurology, Hospital General Universitario de Elche, Elche, Spain
- 16Department of Neurology, Hospital Universitario Reina Sofía, Córdoba, Spain
- 17Department of Neurology, Hospital Clínico Universitario Lozano Blesa, Zaragoza, Spain
- 18Department of Neurology, Fundació Salut Empordà, Figueres, Spain
- 19Department of Neurology, Hospital Francesc de Borja, Gandía, Spain
- 20Department of Neurology, Hospital Universitario Puerta del Mar, Cádiz, Spain
- 21Department of Neurology, Consorci Corporació Sanitària Parc Taulí, Sabadell, Spain
- 22Department of Neurology, Hospital Universitario Donostia, San Sebastián, Spain
Background: Multiple sclerosis is one of the most common causes of neurological disability in young adults, with major consequences for their future lives. Patients with early-stage relapsing-remitting multiple sclerosis (RRMS) experience uncertainty and intense emotions as the diagnosis is disclosed. Illness perception at this point can influence levels of adjustment, coping strategies, treatment adherence, and well-being of the patient. However, there is limited information on patient illness perception surrounding the diagnosis.
Objective: The aim of this study was to assess illness perception and associated factors in early-stage RRMS patients.
Methods: A multicenter, non-interventional study was conducted. Adult patients with a diagnosis of RRMS, a disease duration of ≤ 3 years, and an Expanded Disability Status Scale (EDSS) score of 0-5.5 were included. The Brief-Illness Perception Questionnaire (B-IPQ) was used to assess the patients’ cognitive and emotional representations of their illness. Different patient-reported measures were used to gather information on pain, fatigue, mood/anxiety, quality of life, symptom severity, feelings of hopelessness, perception of stigma, cognition, hand dexterity, gait, and workplace difficulties. A multivariate logistic regression analysis was performed to assess the association between the patients’ illness perception and demographic and clinical characteristics, as well as patient-reported outcomes.
Results: A total of 189 patients were included (mean age: 36.1 ± 9.4 years, 71.4% females, mean disease duration: 1.4 ± 0.8 years). The median EDSS score was 1.0 (interquartile range: 0.0-2.0). A total of 36.5% of the patients (n=69/189) had a moderate-to-high threatening illness perception, and 45.5% thought that their disease was caused by psychological factors. Higher EDSS scores, symptom severity, poorer psychological quality of life, perception of stigma, and greater hopelessness were predictors of moderate-to-high threatening illness perception.
Conclusions: Threatening illness perceptions are common among patients with early-stage RRMS. Identifying these beliefs and their associated factors, and establishing individualized interventions, may help patients deal with their condition.
1 Introduction
Multiple sclerosis (MS) is a chronic demyelinating autoimmune disease that constitutes one of the most common causes of neurological disability in young adults (1). There are approximately two million people worldwide affected by MS, with a prevalence of 23.9 cases per 100,000 population and 62,000 individuals diagnosed with MS every year (2). It manifests through different symptoms such as visual impairment, gait problems, sensory disturbance, fatigue and cognitive problems, among others (3–5). Most patients have a relapsing-remitting form of multiple sclerosis (RRMS), while the rest have primary progressive or secondary progressive forms of MS. Patients with RRMS face the diagnosis in early-to-mid adulthood, with profound consequences in their lives through the disruption of goals, employment, relationships, family planning or social activities (6, 7). The disease can also lead to social cognition deficits due cognitive decline and emotional impairment in patients, deriving in difficulties interpreting social cues, emotions, and establishing meaningful relationships, with an impact in patients’ quality of life (8). The unknown etiology of the disease, combined with the unpredictability of relapses, variable clinical course, and chronic progression without a cure, induces a sense of uncertainty in patients, potentially affecting their perception of the disease and overall well-being (9–12).
Intense emotions, anxiety and depression are also common in the period surrounding the diagnosis, and can affect patient understanding and adjustment to the disease (13, 14). In the event of a health problem or following diagnosis, patients develop their own beliefs and perceptions about the illness, related symptomatology, timeline course, causes, consequences, control through personal actions and treatments, individual emotional response, and coherence (15, 16). Illness perception at this point can influence the levels of adaptation, coping strategies, treatment adherence, and well-being of the patients (16–18). Understanding the illness perceptions of the patients and addressing them at the start of the disease may help them deal with their condition and adjustment to the disease over the long-term, pursuing better quality of life and well-being. However, there is scarce evidence on illness perceptions in early-stage RRMS patients with low levels of disability. Thus, the aim of the present study was to describe patient illness perceptions and assess the factors associated with them in a population recently diagnosed of RRMS.
2 Methods
2.1 Study design
A multicenter, non-interventional, cross-sectional study (MS-ONSET study) was carried out. Inclusion criteria included an age of 18 years or older, a diagnosis of RRMS according to the 2017 revised McDonald criteria, a disease duration of ≤3 years, and an Expanded Disability Status Scale (EDSS) score of 0 to 5.5 (19, 20). Patients not able to understand or complete the study questionnaires according to neurologist criteria, those who had a relapse recently and those who were not stable on their treatment were excluded from the sample. Patients were consecutively recruited in the context of their follow-up visits at 21 hospital-based Neuroimmunology clinics. When attending the follow-up visits, patients fulfilling inclusion criteria were offered to participate in the study by neurologists, and after signing the informed consent they were included in the study and completed all the questionnaires at the hospital. The EDSS was assessed by their treating neurologists.
2.2 Outcome measures
The Brief-Illness Perception Questionnaire (B-IPQ) was used to assess the patients’ cognitive and emotional representations of their illness (21, 22). It consists of 8 items graded on a linear 0–10 response scale. Each item of the B-IPQ assesses one dimension of illness perception, including the consequences, timeline or duration of disease, personal control, treatment control, identity or symptoms, concerns, coherence or understanding, and emotional impact. An overall score can be calculated by adding all items and reversing scores of items of personal control, treatment control, and coherence/understanding. Higher scores indicate a more threatening illness perception. A ninth item consisting of an open question addresses the patients’ thoughts about the cause of their illness (21, 22). Moderate-to-high experience of threat is defined as a B-IPQ score of at least 42 points (23).
Different patient-reported measures were used to gather information on pain [Visual Analogue Scale (VAS)] (24), fatigue [5-item Modified Fatigue Impact Scale (MFIS-5)] (25), mood and anxiety [Hospital Anxiety and Depression Scale (HADS)] (26), quality of life [Multiple Sclerosis Impact Scale (MSIS-29)] (27), symptom severity [SymptoMScreen (SyMS)] (28, 29), feelings of hopelessness [State-Trait Hopelessness Scale (STHS)] (30), perception of stigma [Stigma Scale for Chronic Illness 8-item version (SSCI-8)] (31, 32), gait perception [Multiple Sclerosis Walking Scale (MSWS-12)] (33), manual dexterity perception [NeuroQoL Upper Extremity (NeuroQoL-UE)] (34), cognition [Perceived Deficits Questionnaire (PDQ-5)] (35), and workplace difficulties [Multiple Sclerosis Working Difficulties Questionnaire (MSWDQ-23)] (36) (Table 1).
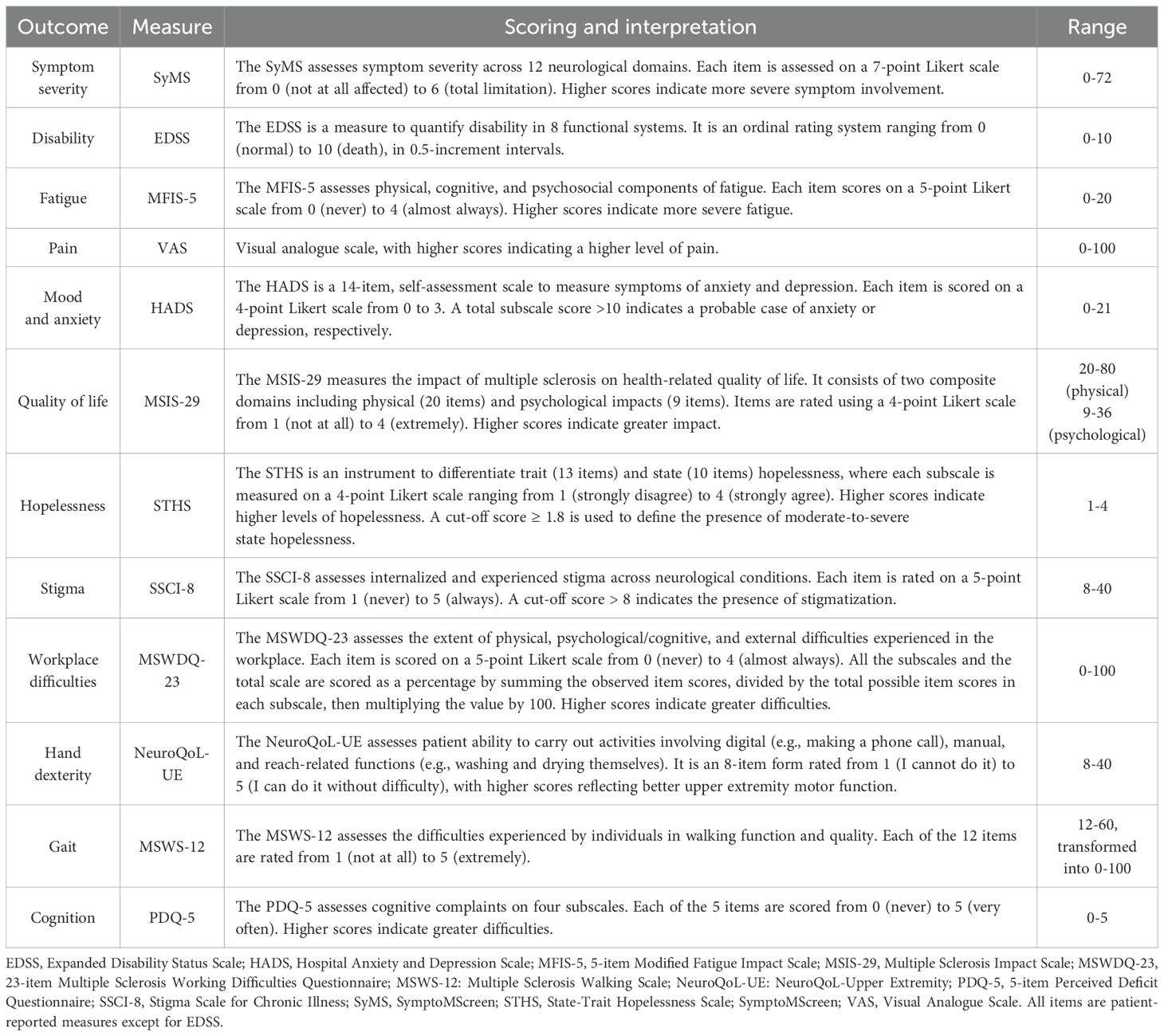
Table 1. Outcome measures.
2.3 Methodological approach
Demographic and clinical characteristics were reported as frequencies (percentages) and means (standard deviations). Bivariate analyses were performed using logistic regression to assess the association between categorized B-IPQ (dependent variable) and demographic parameters, clinical characteristics, and patient perspectives. Subsequently, a multivariate logistic regression analysis was performed taking each of the described variables as the dependent variable and each of the values found to be significant (<0.10) in the previous analysis as the independent variables. These variables were further selected through stepwise regression using the Akaike information criterion (AIC).
3 Results
A total of 189 patients were included in the study. The mean age was 36.1 years, and 71.4% were females. The mean disease duration was 1.4 years, and the median EDSS score was 1.0. Symptom severity was low, but the patients reported that their psychological quality of life was somewhat impacted, with 56.6% perceiving stigma and almost 25% of the patients being probable anxiety cases. The sociodemographic and clinical characteristics of the sample are shown in Table 2.
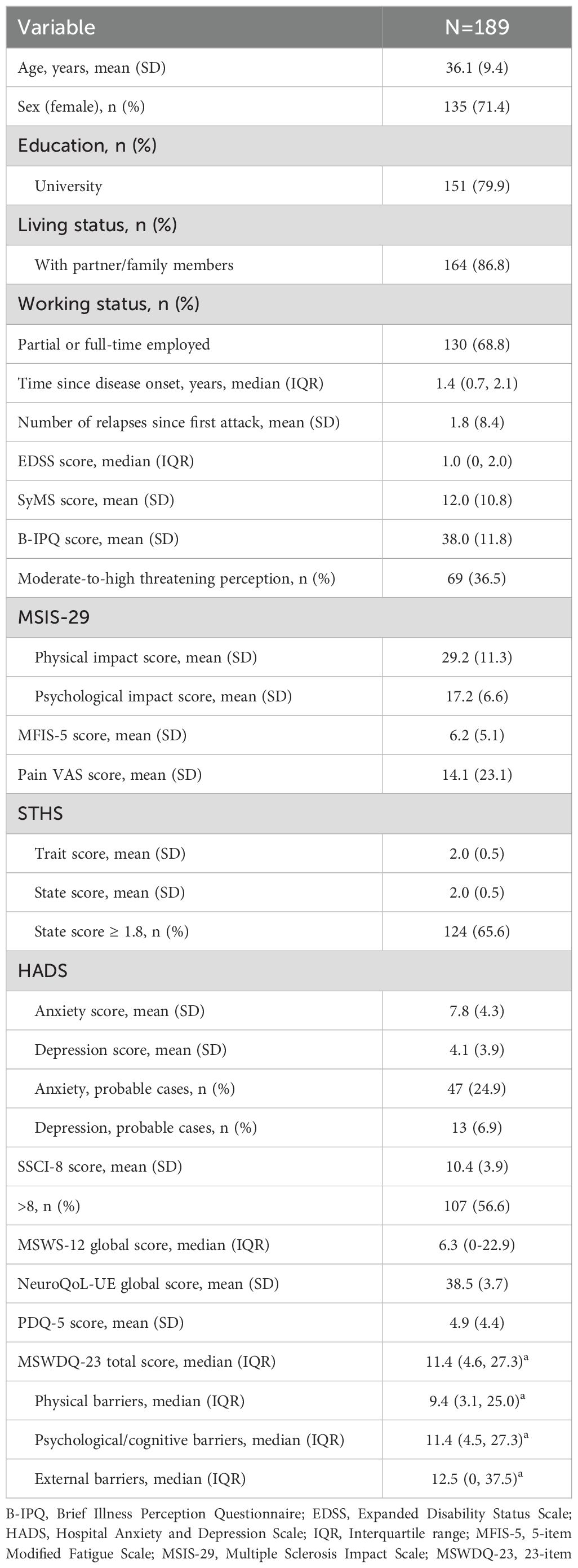
Table 2. Sociodemographic and clinical characteristics of the study population.
A total of 36.5% of the patients (n=69/189) had a moderate-to-high threatening illness perception following the cut-off of the total score. When assessing the open question (item 9), a proportion of 47.6% (n=90/189) of patients thought that their disease was caused by psychological factors such as stress, anxiety, depression or nervousness, followed by unknown causes (17.5%), including chance or bad luck (Figure 1). The analysis of illness perception by its dimensions revealed that the most threatening aspect of multiple sclerosis for the patients was illness duration, followed by concerns from the disease, lack of personal control, and emotional impact. Nevertheless, the patients perceived that treatment helped to control their disease (Figure 2). Patients with a moderate-to-high threatening illness perception had poorer emotional representations (difference [Δ], Δ=2.3), concerns (Δ=2.3), consequences (Δ=2.2), and identity (Δ=2.0) beliefs when compared to the overall group, whereas coherence (Δ=0.8) and treatment control (Δ=0.7) perceptions did not differ much between groups (Figure 2).
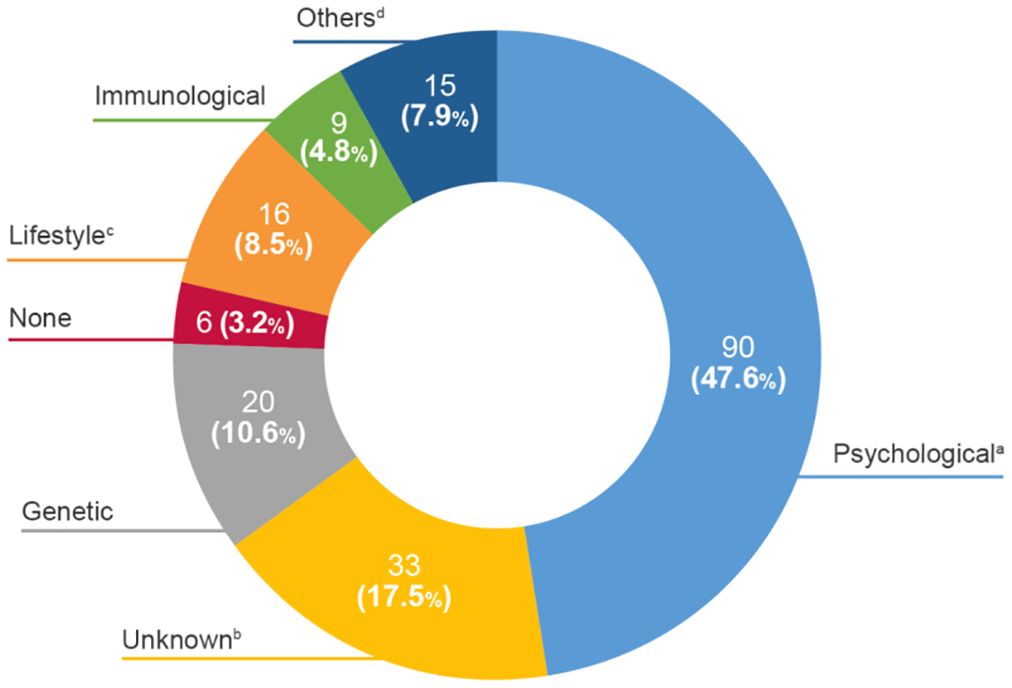
Figure 1. Causes of multiple sclerosis reported by patients. aPsychological includes emotional causes, depression, anxiety, nervousness, stress; bUnknown includes chance or bad luck; cLifestyle includes smoking, diet, lack of physical exercise; dothers includes severe sunstroke, car accident, attention, limp, pregnancy, fatigue, tingling, intestinal causes, migraine, neurological alterations, sleep problems, female sex, traumatism and vision. B-IPQ, Brief-Illness Perception Questionnaire.
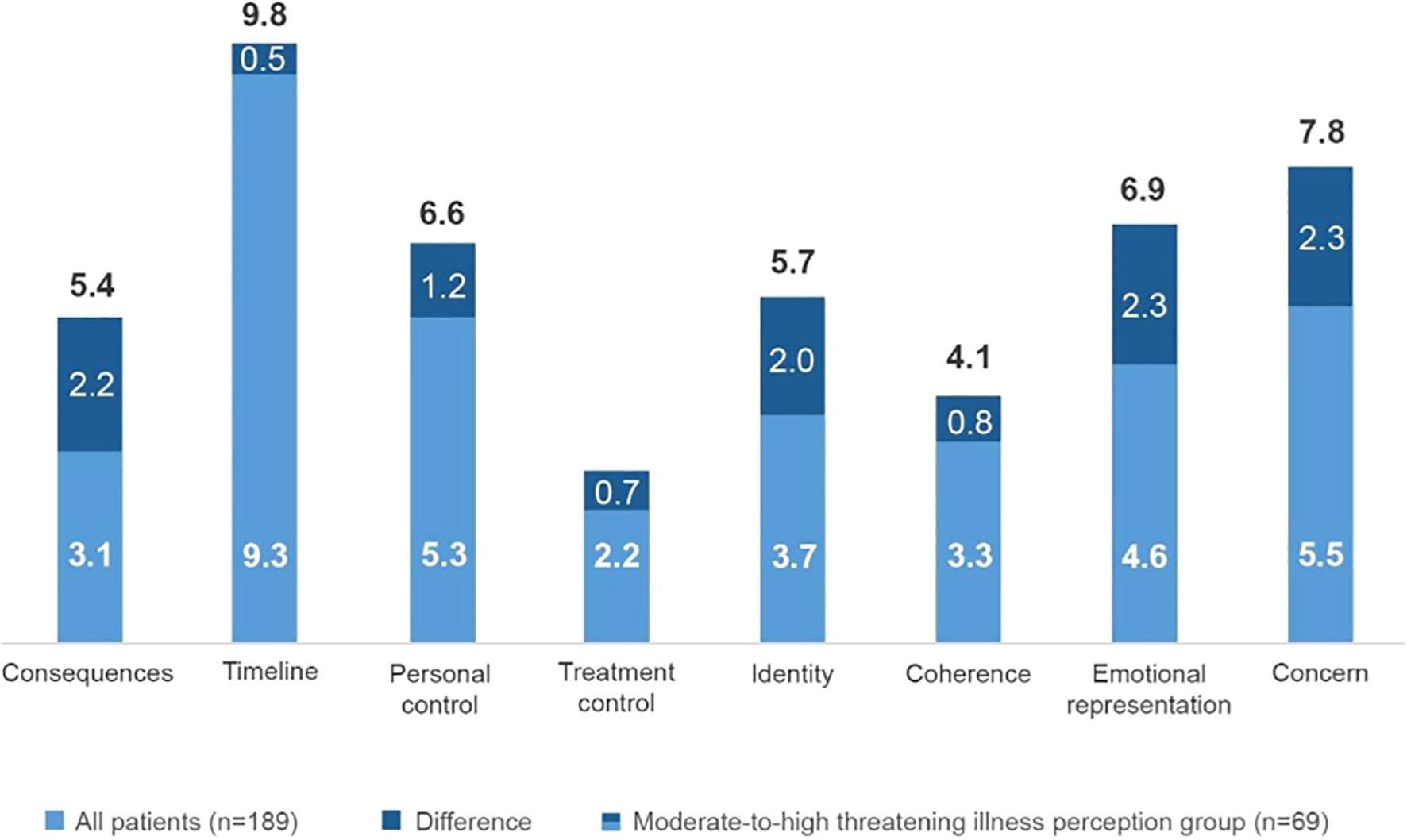
Figure 2. Patient perception of illness. Patients' illness perception in the different items of the Brief-Illness Perception Questionnaire.
The bivariate analyses suggested that patients were significantly more likely to have a threatening disease perception if they were unemployed, had received symptomatic treatment, had a higher EDSS score, poorer perception of their hand dexterity and gait, higher perceptions referred to pain, fatigue, symptom severity, hopelessness, and poorer perception of their quality of life. The same applied to patients reporting workplace barriers, cognitive complaints, and probable cases of anxiety, depression, and stigma.
Higher EDSS scores, greater symptom severity, a poorer psychological quality of life, perception of stigma, and greater hopelessness were identified as predictors of moderate-to-high threatening illness perception (Table 3).
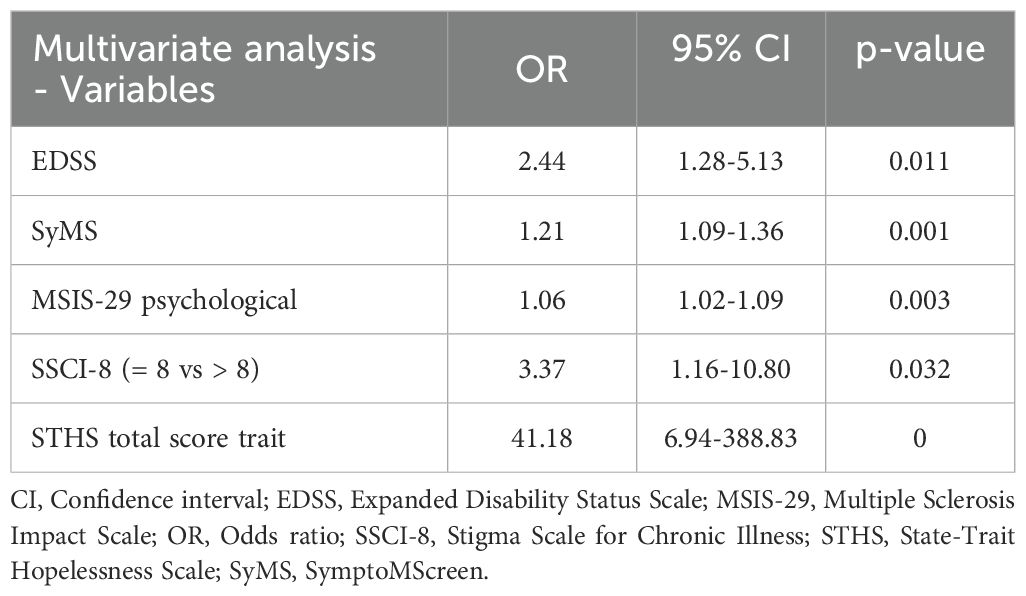
Table 3. Predictors of moderate-to-high threatening illness perception.
4 Discussion
Identifying patient beliefs and expectations at the beginning of the disease might be of importance for promptly implementing educational strategies aimed at influencing patient adjustment. These perceptions can have an influence into patients’ coping style, adopting an active role to employ adaptative strategies that facilitate overcoming stress or on the contrary developing an avoidant/maladaptive style, as well as can lead to employing the right coping strategy of problem-solving and task-oriented, while avoiding the others in seek of greater quality of life and well-being over the long term (37). This study addresses a critical knowledge gap, as evidence on illness perceptions in early-stage RRMS patients with low levels of disability is scarce. We assessed patient illness perceptions in a population with a disease duration of less than three years from the first symptom and with very low disability. We found that more than a third of these patients experienced moderate-to-high threatening illness perception, with disability, symptom severity, and psychological factors being predictors of this condition.
A recent systematic review of previous works reported that a greater emotional impact, number of symptoms, higher perception of negative consequences of the disease for the life of the patient, and attributing the cause of the disease to psychological factors, were related to poorer outcomes in terms of well-being, adjustment, quality of life, or fatigue (18). In contrast, stronger perceptions of personal control over the illness, disease comprehension, and attributing the cause of the disease to external factors – relieving the sense of guilt – were seen to be related to better outcomes and possibly to more effective management of the disease and a lower level of distress (18). In our study, we found that having a moderate-to-high threatening illness perception was mainly driven by stronger perceptions in those dimensions related to poorer outcomes (illness duration, lack of personal control, and emotional impact), including concerns. In some of them, the range of improvement might be minimal, such as perceptions of illness duration, as it is a chronic condition. However, the others might benefit from tailored psychoeducational interventions that address emotional health, social support, and adaptive coping strategies (8, 37). Although a 63.5% of patients were not categorized as having a moderate-to-high threatening-illness disease, they might benefit as well from these assessments and interventions, as the highest scores were placed on the same dimensions, with a lower impact. Our identification of greater disability and symptom severity as predictors of threatening perception in an early and scantly disabled population is in line with the data from recent studies, where disease severity has been significantly associated with negative illness perceptions in multiple sclerosis patients with mild disability, playing a crucial role in terms of sexual dysfunction (38). Physicians should pay attention to these beliefs in the early disease stages, as negative beliefs regarding concerns, treatment and serious consequences of the disease might increase with a longer duration of illness (39). Furthermore, previous studies have found that illness perception mediates an association between a poorer perception of physical condition and negative treatment efficacy beliefs (40). Interestingly, while a higher proportion of patients with a threatening perception of their illness had poorer perceptions of their physical condition, we did not observe substantial differences in treatment control beliefs. This finding may suggest that early-stage patients maintain a sense of treatment efficacy, which could be leveraged to foster engagement in disease-modifying therapies and rehabilitation strategies (41). Moreover, poorer illness perceptions have been related to psychological factors (16, 42, 43). We found that psychological factors such as the perception of stigma, greater hopelessness, and poorer psychological quality of life were predictors of a threatening condition perception, and that almost half of the patients thought their disease had a psychological cause. These findings emphasize the importance of early psychological assessment to identify these limiting factors. Interventions like meditation, mindfulness or yoga can be implemented to reduce those that are more manageable such as anxiety, nervousness, and stress (44). They also point to the potential benefits of establishing education programs to address misattributions about the causes of the disease. Both measures may help reduce stigma and improve illness perception, enhancing adjustment to the disease and ultimately having a positive impact on emotional well-being. Besides psychological causes, one out of four patients in our study thought that their MS was caused by random events or bad luck. These misattributions of causes of MS reflect misinformation that may come from internet searches, as it is one of the most common sources of information used by patients to find MS causes or risk factors, with the difficulty of recognizing reliable information (45, 46). Healthcare professionals might face the challenge of transforming these untrue claims and beliefs to scientific-based information through guidance of patients and caregivers toward prudent searches, by avoiding advertisement and personal experiences that may not apply to others, while also looking for easily understandable, referenced content (47).
Considering these findings, the implementation of educational programs, adapting coping strategies, and establishing psychological intervention at the time of diagnosis, may be crucial for a comprehensive understanding of the disease and its evolution - including the recognition and management of symptoms, awareness of treatment options, and the impact of lifestyle factors (48, 49) - placing emphasis on those individuals with greater disability, symptoms, and a poorer psychological status, as evidenced in our study. Consequently, patients will have more tools to better face their disease, enhancing their illness perception, achieving psychological protection, and increasing their self-management to actively participate in the shared decision-making process throughout their disease (11, 16).
Our study has some limitations. Firstly, its cross-sectional design did not allow us to assess changes in patient illness perception over time and after implementing interventions, since the study involved a single visit. Secondly, external factors such as caregivers’ perception were not assessed in this study and might be contributors to the outcome (42). However, the study provides relevant information on early-stage RRMS patient illness perception in a key moment, namely the period surrounding the diagnosis, and on patient adjustment to the new disease.
5 Conclusions
Threatening illness perceptions are common among patients with early RRMS and may be related to greater disability and symptoms, a poorer psychological quality of life, the perception of stigma, and hopelessness. Identifying these beliefs and their associated factors after the diagnosis, and establishing individualized interventions, may help patients deal with their condition over the long term.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Review Board of Hospital Universitari Arnau de Vilanova (Lleida, Spain). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
RG-B: Conceptualization, Formal Analysis, Funding acquisition, Project administration, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. SS: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MB: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JM-M: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. JS: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. AA: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. AC: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. LBo: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. JS-M: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. FB-H: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. CC: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. LBr: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. MB-Q: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. JDG-S: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. AR-R: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. LN-C: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. EA: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. MG-R: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. OC: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. LG-T: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. LF: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. MH: Data curation, Formal Analysis, Investigation, Validation, Writing – review & editing. TC-T: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JM: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by Roche Medical Department, Spain (ML42064). The funding source had no role in the design of the study, data analysis and interpretation, review and approval of the manuscript, or in the decision to submit for publication.
Acknowledgments
The authors are most grateful to all the patients, neurologists and nurses that participated in the study. The authors also thank Evidenze Health España for the support during the development of this study.
Conflict of interest
SS received payment for lecturing or travel expenses from Merck-Serono, Biogen, Sanofi-Genzyme, Roche, and Novartis. RG-B and JM are employees of Roche Pharma Spain. JM-M has served on scientific advisory boards and/or has received speaking honoraria, research funding and support to attend scientific meetings from Biogen, Merck, Novartis, Roche and Teva. JS has received speaking honoraria, compensation for consulting services and support to attend scientific meetings from Almirall, Bayer, Biogen, Merck, Novartis, Sanofi, Roche and Teva. AA has received compensation for consulting services from Biogen, BMS, Sanofi, Roche, Janssen and Novartis, and speaking honoraria from Biogen, BMS, Sanofi, Roche, Janssen, Merck, Almirall, and Novartis. AC has received courses and honoraria for her participation as speaker/meeting moderator/symposia organizer from Alter, Almirall, Bayer, Bial, Biogen, Bristol-Myers-Squibb, Lilly, Merck-Serono, Mylan, Novartis, Roche, Sanofi-Genzyme, Teva, and UCB, and support to attend scientific meetings from Biogen, Bial, Merck-Serono, Novartis, Roche, Sanofi-Genzyme, and Teva. JS-M has received support to attend scientific meetings from Novartis, Merck, and Biogen, speaking honoraria from Biogen, Novartis, Sanofi, Merck, Almirall, Bayer, and Teva, and has participated in clinical trials from Biogen, Merck, and Roche. FB-H has received compensation for consulting services and speaking honoraria from Almirall, Biogen, Genzyme, Merck-Serono, Novartis, Roche, Sanofi, and Teva. CC has received compensation for consulting services, speaking honoraria and support to attend scientific meetings and courses from Merck, Teva, Sanofi-Genzyme, Novartis, Biogen, Roche, and Bristol-Myers-Squibb. LBr has received compensation for consulting services, speaking honoraria and support to attend scientific meetings from Bayer, Celgene, Biogen, Genzyme, Merck, Novartis, Roche, Almirall and Teva. JDG-S has received compensation for consulting services and speaking honoraria from Biogen, Novartis, Merck, UCB, Sanofi-Genzyme, Roche, Almirall, and Teva. LN-C has received compensations from Sanofi-Genzyme, Merck, Biogen, and Roche. EA has received speaking honoraria from Roche, Novartis, Merck, Sanofi, and Biogen. MG-R has received speaking honoraria from Biogen, Sanofi, Almirall and Novartis. OC has participated in studies and has received speaking honoraria from Roche, Merck, Biogen, and Novartis. LG-T has received speaking honoraria from Biogen, Novartis, Merck, Bayer, Sanofi-Genzyme, Almirall, Roche and Teva. MH has participated in observational studies and has received compensation for consulting services and speaking honoraria from Roche, Merck, Sanofi, Biogen, Novartis and Bayer.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Zanghi A, Galgani S, Bellantonio P, Zaffaroni M, Borriello G, Inglese M, et al. Relapse-associated worsening in a real-life multiple sclerosis cohort: the role of age and pyramidal phenotype. Eur J Neurol. (2023) 30:2736–44. doi: 10.1111/ene.15910
2. Khan G and Hashim MJ. Epidemiology of multiple sclerosis: global, regional, national and sub-national-level estimates and future projections. J Epidemiol Glob Health. (2025) 15:21. doi: 10.1007/s44197-025-00353-6
3. Fuchs TA, Schoonheim MM, Zivadinov R, Dwyer MG, Colato E, Weinstock Z, et al. Cognitive progression independent of relapse in multiple sclerosis. Mult Scler. (2024) 30:1468–78. doi: 10.1177/13524585241256540
4. Ghajarzadeh M, Waubant E, and Nourbakhsh B. Design recommendations for studies that evaluate multiple sclerosis fatigue interventions. Front Psychiatry. (2023) 14:1287344. doi: 10.3389/fpsyt.2023.1287344
5. Lakin L, Davis BE, Binns CC, Currie KM, and Rensel MR. Comprehensive approach to management of multiple sclerosis: addressing invisible symptoms-A narrative review. Neurol Ther. (2021) 10:75–98. doi: 10.1007/s40120-021-00239-2
6. Castillo-Trivino T, Gomez-Ballesteros R, Borges M, Martin-Martinez J, Sotoca J, Alonso A, et al. Long-term prognosis communication preferences in early-stage relapsing-remitting multiple sclerosis. Mult Scler Relat Disord. (2022) 64:103969. doi: 10.1016/j.msard.2022.103969
7. Maurino J, Martinez-Gines ML, Garcia-Dominguez JM, Solar MD, Carcelen-Gadea M, Ares-Luque A, et al. Workplace difficulties, health-related quality of life, and perception of stigma from the perspective of patients with Multiple Sclerosis. Mult Scler Relat Disord. (2020) 41:102046. doi: 10.1016/j.msard.2020.102046
8. Marafioti G, Cardile D, Culicetto L, Quartarone A, and Lo Buono V. The impact of social cognition deficits on quality of life in multiple sclerosis: A scoping review. Brain Sci. (2024) 14:691. doi: 10.3390/brainsci14070691
9. Gasperini C, Battaglia MA, Balzani F, Chiarini E, Pani M, Pasqualetti P, et al. Unveiling preferences in multiple sclerosis care: insights from an Italian discrete-choice experiment with patients and healthcare professionals. J Neurol. (2024) 272:27. doi: 10.1007/s00415-024-12725-2
10. Longinetti E, Englund S, Burman J, Fink K, Fogdell-Hahn A, Gunnarsson M, et al. Trajectories of cognitive processing speed and physical disability over 11 years following initiation of a first multiple sclerosis disease-modulating therapy. J Neurol Neurosurg Psychiatry. (2024) 95:134–41. doi: 10.1136/jnnp-2023-331784
11. Sabin J, Salas E, Martin-Martinez J, Candeliere-Merlicco A, Barrero FJ, Alonso A, et al. Perceived illness-related uncertainty among patients with mid-stage relapsing-remitting multiple sclerosis. Mult Scler Relat Disord. (2024) 91:105861. doi: 10.1016/j.msard.2024.105861
12. Young CA, Rog DJ, Sharrack B, Tanasescu R, Kalra S, Harrower T, et al. Correlates and trajectories of relapses in relapsing-remitting multiple sclerosis. Neurol Sci. (2024) 45:2181–9. doi: 10.1007/s10072-023-07155-3
13. Carey G, Wilson N, Janssen J, Chohan A, Rog D, and Roddam H. I’m walking into the unknown”: Qualitative insights into how emotions and lived experience related to multiple sclerosis diagnosis impact on decisions to pursue disease modifying treatment. Mult Scler Relat Disord. (2021) 58:103464. doi: 10.1016/j.msard.2021.103464
14. Gillespie DC, Sacripante R, Chandran S, Foley P, and Future M. Suicidal ideation in the year following diagnosis of relapsing-remitting multiple sclerosis: A longitudinal perspective. Mult Scler Relat Disord. (2024) 91:105904. doi: 10.1016/j.msard.2024.105904
15. Leventhal H, Phillips LA, and Burns E. The Common-Sense Model of Self-Regulation (CSM): a dynamic framework for understanding illness self-management. J Behav Med. (2016) 39:935–46. doi: 10.1007/s10865-016-9782-2
16. Timkova V, Mikula P, Fedicova M, Szilasiova J, and Nagyova I. Psychological well-being in people with multiple sclerosis and its association with illness perception and self-esteem. Mult Scler Relat Disord. (2021) 54:103114. doi: 10.1016/j.msard.2021.103114
17. Bassi M, Cilia S, Falautano M, Grobberio M, Niccolai C, Pattini M, et al. Illness perceptions and psychological adjustment among persons with multiple sclerosis: the mediating role of coping strategies and social support. Disabil Rehabil. (2020) 42:3780–92. doi: 10.1080/09638288.2019.1610511
18. Luca M, Eccles F, Perez Algorta G, and Patti F. Illness perceptions and outcome in multiple sclerosis: A systematic review of the literature. Mult Scler Relat Disord. (2022) 67:104180. doi: 10.1016/j.msard.2022.104180
19. Thompson AJ, Banwell BL, Barkhof F, Carroll WM, Coetzee T, Comi G, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. (2018) 17:162–73. doi: 10.1016/S1474-4422(17)30470-2
20. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. (1983) 33:1444–52. doi: 10.1212/wnl.33.11.1444
21. Broadbent E, Petrie KJ, Main J, and Weinman J. The brief illness perception questionnaire. J Psychosom Res. (2006) 60:631–7. doi: 10.1016/j.jpsychores.2005.10.020
22. Dennison L, Moss-Morris R, Silber E, Galea I, and Chalder T. Cognitive and behavioural correlates of different domains of psychological adjustment in early-stage multiple sclerosis. J Psychosom Res. (2010) 69:353–61. doi: 10.1016/j.jpsychores.2010.04.009
23. Kuiper H, van Leeuwen CMC, Stolwijk-Swuste JM, and Post MWM. Reliability and validity of the Brief Illness Perception Questionnaire (B-IPQ) in individuals with a recently acquired spinal cord injury. Clin Rehabil. (2022) 36:550–7. doi: 10.1177/02692155211061813
24. Gurkan MA and Gurkan FT. Measurement of pain in multiple sclerosis. Noro Psikiyatr Ars. (2018) 55:S58–62. doi: 10.29399/npa.23336
25. Meca-Lallana V, Branas-Pampillon M, Higueras Y, Candeliere-Merlicco A, Aladro-Benito Y, Rodriguez-De la Fuente O, et al. Assessing fatigue in multiple sclerosis: Psychometric properties of the five-item Modified Fatigue Impact Scale (MFIS-5). Mult Scler J Exp Transl Clin. (2019) 5:2055217319887987. doi: 10.1177/2055217319887987
26. Zigmond AS and Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
27. Hobart J, Lamping D, Fitzpatrick R, Riazi A, and Thompson A. The Multiple Sclerosis Impact Scale (MSIS-29): a new patient-based outcome measure. Brain. (2001) 124:962–73. doi: 10.1093/brain/124.5.962
28. Green R, Kalina J, Ford R, Pandey K, and Kister I. SymptoMScreen: A tool for rapid assessment of symptom severity in MS across multiple domains. Appl Neuropsychol Adult. (2017) 24:183–9. doi: 10.1080/23279095.2015.1125905
29. Meca-Lallana J, Maurino J, Hernandez-Perez MA, Sempere AP, Brieva L, Garcia-Arcelay E, et al. Psychometric properties of the symptoMScreen questionnaire in a mild disability population of patients with relapsing-remitting multiple sclerosis: quantifying the patient’s perspective. Neurol Ther. (2020) 9:173–9. doi: 10.1007/s40120-020-00176-6
30. Dunn SL, Olamijulo GB, Fuglseth HL, Holden TP, Swieringa LL, Sit MJ, et al. The State-Trait Hopelessness Scale: development and testing. West J Nurs Res. (2014) 36:552–70. doi: 10.1177/0193945913507634
31. Molina Y, Choi SW, Cella D, and Rao D. The stigma scale for chronic illnesses 8-item version (SSCI-8): development, validation and use across neurological conditions. Int J Behav Med. (2013) 20:450–60. doi: 10.1007/s12529-012-9243-4
32. Ballesteros J, Martinez-Gines ML, Garcia-Dominguez JM, Forero L, Prefasi D, Maurino J, et al. Assessing stigma in multiple sclerosis: psychometric properties of the eight-item stigma scale for chronic illness (SSCI-8). Int J MS Care. (2019) 21:195–9. doi: 10.7224/1537-2073.2018-053
33. Hobart JC, Riazi A, Lamping DL, Fitzpatrick R, and Thompson AJ. Measuring the impact of MS on walking ability: the 12-Item MS Walking Scale (MSWS-12). Neurology. (2003) 60:31–6. doi: 10.1212/wnl.60.1.31
34. Miller DM, Bethoux F, Victorson D, Nowinski CJ, Buono S, Lai JS, et al. Validating Neuro-QoL short forms and targeted scales with people who have multiple sclerosis. Mult Scler. (2016) 22:830–41. doi: 10.1177/1352458515599450
35. Strober LB, Binder A, Nikelshpur OM, Chiaravalloti N, and DeLuca J. The perceived deficits questionnaire: perception, deficit, or distress? Int J MS Care. (2016) 18:183–90. doi: 10.7224/1537-2073.2015-028
36. Honan CA, Brown RF, and Hine DW. The multiple sclerosis work difficulties questionnaire (MSWDQ): development of a shortened scale. Disabil Rehabil. (2014) 36:635–41. doi: 10.3109/09638288.2013.805258
37. Culicetto L, Lo Buono V, Donato S, La Tona A, Cusumano AMS, Corello GM, et al. Importance of coping strategies on quality of life in people with multiple sclerosis: A systematic review. J Clin Med. (2024) 13:5505. doi: 10.3390/jcm13185505
38. Scandurra C, Rosa L, Carotenuto A, Moccia M, Arena S, Ianniello A, et al. Sexual dysfunction in people with multiple sclerosis: the role of disease severity, illness perception, and depression. J Clin Med. (2023) 12:2215. doi: 10.3390/jcm12062215
39. Pust GEA, Untiedt B, Weierstall-Pust R, Randerath J, Barabasch A, Rahn AC, et al. Medication beliefs in first-line and second-line treated multiple sclerosis patients. Mult Scler Relat Disord. (2020) 42:102144. doi: 10.1016/j.msard.2020.102144
40. Wilski M, Kocur P, Gorny M, Koper M, Nadolska A, Chmielewski B, et al. Perception of multiple sclerosis impact and treatment efficacy beliefs: mediating effect of patient’s illness and self-appraisals. J Pain Symptom Manage. (2019) 58:437–44. doi: 10.1016/j.jpainsymman.2019.06.013
41. Glattacker M, Giesler JM, Klindtworth K, and Nebe A. Rehabilitation use in multiple sclerosis: Do illness representations matter? Brain Behav. (2018) 8:e00953. doi: 10.1002/brb3.953
42. Bassi M, Falautano M, Cilia S, Goretti B, Grobberio M, Pattini M, et al. Illness perception and well-being among persons with multiple sclerosis and their caregivers. J Clin Psychol Med Settings. (2016) 23:33–52. doi: 10.1007/s10880-015-9425-8
43. Wilski M and Tasiemski T. Health-related quality of life in multiple sclerosis: role of cognitive appraisals of self, illness and treatment. Qual Life Res. (2016) 25:1761–70. doi: 10.1007/s11136-015-1204-3
44. Motolese F, Stelitano D, Lanzone J, Albergo G, Cruciani A, Masciulli C, et al. Feasibility and efficacy of an at-home, smart-device aided mindfulness program in people with Multiple Sclerosis. Mult Scler Relat Disord. (2023) 78:104931. doi: 10.1016/j.msard.2023.104931
45. Colombo C, Mosconi P, Confalonieri P, Baroni I, Traversa S, Hill SJ, et al. Web search behavior and information needs of people with multiple sclerosis: focus group study and analysis of online postings. Interact J Med Res. (2014) 3:e12. doi: 10.2196/ijmr.3034
46. Higueras Y, Salas E, Meca-Lallana V, Carrascal Rueda P, Rodríguez de la Fuente O, Cabello-Moruno R, et al. Information-seeking strategies of people with multiple sclerosis in Spain: the INFOSEEK-MS study. Patient Prefer Adherence. (2022) 16:51—60. doi: 10.2147/PPA.S344690
47. Lavorgna L, Ippolito D, Esposito S, Tedeschi G, and Bonavita S. A disease in the age of the web: How to help people with Multiple Sclerosis in social media interaction. Mult Scler Relat Disord. (2017) 17:238–9. doi: 10.1016/j.msard.2017.08.017
48. Bassi M, Grobberio M, Negri L, Cilia S, Minacapelli E, Niccolai C, et al. The contribution of illness beliefs, coping strategies, and social support to perceived physical health and fatigue in multiple sclerosis. J Clin Psychol Med Settings. (2021) 28:149–60. doi: 10.1007/s10880-019-09692-6
Keywords: relapsing-remitting multiple sclerosis, illness perception, early-stage, patient-reported outcome measures, individualized interventions, psychological factors
Citation: Gómez-Ballesteros R, Sainz de la Maza S, Borges M, Martín-Martínez J, Sotoca J, Alonso A, Caminero AB, Borrega L, Sánchez-Menoyo JL, Barrero-Hernández FJ, Calles C, Brieva L, Blasco-Quílez MR, Dotor García-Soto J, Rodríguez-Regal A, Navarro-Cantó L, Agüera E, Garcés-Redondo M, Carmona O, Gabaldón-Torres L, Forero L, Hervás M, Castillo-Triviño T and Maurino J (2025) Threatening illness perception and associated factors in early-stage relapsing-remitting multiple sclerosis. Front. Psychiatry 16:1565150. doi: 10.3389/fpsyt.2025.1565150
Received: 22 January 2025; Accepted: 23 June 2025;
Published: 08 July 2025.
Edited by:
Carmelo Mario Vicario, University of Messina, ItalyReviewed by:
Pavol Mikula, University of Pavol Jozef Šafárik, SlovakiaGiulia Marafioti, Bonino Pulejo Neurology Center (IRCCS), Italy
Copyright © 2025 Gómez-Ballesteros, Sainz de la Maza, Borges, Martín-Martínez, Sotoca, Alonso, Caminero, Borrega, Sánchez-Menoyo, Barrero-Hernández, Calles, Brieva, Blasco-Quílez, Dotor García-Soto, Rodríguez-Regal, Navarro-Cantó, Agüera, Garcés-Redondo, Carmona, Gabaldón-Torres, Forero, Hervás, Castillo-Triviño and Maurino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rocío Gómez-Ballesteros, cm9jaW8uZ29tZXpAcm9jaGUuY29t