 Cristiano Costa1
Cristiano Costa1 Stefano Ferracuti
Stefano Ferracuti Alexa Schincariol
Alexa Schincariol Cristina Scarpazza
Cristina Scarpazza- 1Department of General Psychology, School of Psychology, University of Padua, Padua, Italy
- 2Department of Human Neurosciences, Faculty of Medicine and Dentistry, Sapienza University of Rome, Rome, Italy
- 3Neuroscience Center, Department of General Psychology, School of Psychology, University of Padua, Padua, Italy
- 4Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) S. Camillo Hospital, Venice, Italy
Background: Developmental and acquired paedophilic behaviour are considered two distinct phenomena, yet no study has systematically compared the cognitive profiles of individuals committing these forms of child sexual offenses (CSO). This study explored whether individuals with developmental and acquired paedophilic behaviour are characterised by similar or different neuropsychological underpinnings and how these differences manifest themselves in observable behaviour.
Methods: Thirty-four studies on developmental CSO and 17 (describing 21 cases) on acquired CSO were included. Multivariate meta-analytic approaches were adopted to investigate the cognitive abilities of individuals who committed CSO with (P+CSO) and without (CSO) a diagnosis of paedophilia (P), while a systematic review was conducted to identify the cognitive features of acquired CSO.
Results: Meta-analytic findings showed overall worse neuropsychological performances for developmental CSO compared to the control group (μ = −0.186; p = .002). Subgroup analyses confirmed these results for both CSO (μ = −0.232; p <.05) and P+CSO (μ = −0.153; p <.05). The systematic review on acquired CSO revealed that all individuals (100%) exhibited deficits in inhibitory control and 62.5% of them showed concomitant impairments in social-cognition abilities.
Conclusions: Developmental and acquired paedophilic behaviours share inhibitory control deficits, even though with different characteristics; however, social-cognitive deficits appear specific to acquired CSO. These findings provide insights into the neurocognitive underpinnings of these behaviours, highlighting distinct mechanisms that may influence their modi operandi.
1 Introduction
Sexual offenses against children are a major public concern affecting numerous individuals (1) and causing significant trauma and human suffering for victims and their families (2). Although child sexual offending is often considered analogous with paedophilia, this represents a fundamental misuse of terminology.
The fifth version of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM–5; 3) made for the first time a clear distinction between paedophilia and paedophilic disorder: while paedophilia is defined as persistent sexual attraction to children, paedophilic disorder can be diagnosed only when paedophilia is accompanied by recurrent, intense sexual arousal or urges involving sexual activities with children, when they cause marked distress in the individual, or result in sexual offenses against children (4, 5). Importantly, not all individuals with paedophilia commit sexual offenses against children. Indeed, some of them manage to confine their sexual urges and desires to fantasies about sexual contact with children (6–10), whereas others proactively seek therapeutic interventions to manage overwhelming impulses before acting on them (6, 10–12).
Traditionally, research has focused on individuals whose paedophilic interests emerge in adolescence and persist over time. However, a growing body of literature describes cases in which sexual interest in children arises de novo in adulthood, typically in the context of an identifiable neurological insult - such as a tumour, traumatic brain injury, or neurodegenerative disease (13–15)1. These cases, to which we refer as acquired CSO, raise new questions about the neurobiological roots of such behaviour.
In this paper, we focus on individuals who have committed child sexual offenses (CSO), regardless of whether they meet formal diagnostic criteria for paedophilia. We distinguish between two clinical manifestations: (1) developmental CSO, encompassing both individuals with paedophilic disorder (P+CSO)2 and those without (CSO), whose offending behaviour is not associated with a known neurological event; and (2) acquired CSO, referring to individuals whose paedophilic urges and offending behaviour arise in direct relation to neurological damage.
Given the clinical and theoretical significance of this distinction, the present study pursues two main objectives. First, we examine differences within the developmental CSO group – comparing P+CSO and CSO individuals – to determine whether observed cognitive impairments are more strongly associated with paedophilic preference or with the act of offending itself. Second, we qualitatively compare developmental and acquired CSO to assess whether they reflect distinct neuropsychological profiles, as suggested by their divergent aetiologies, neural substrates, and behavioural features (21–23). By addressing both levels of analysis, this study offers a comprehensive framework to understand the cognitive mechanisms underlying child sexual offending, with implications for diagnosis, treatment, and legal accountability.
Regarding acquired CSO, some researchers argue that individuals with this condition are usually characterised by an underlying sexual interest in children that can be unmasked by a change in the baseline functioning – like a neurological insult – impairing their ability to regulate pre-existing tendencies (24, 25). This interpretation aligns with cases where premorbid sexual interest in children was documented (25). However, other cases challenge this hypothesis (26). For instance, some individuals with acquired CSO deny any prior attraction to children. In these cases, it has been suggested that functional impairments, such as damage to the hypothalamus, may lead to a shift in sexual orientation (26). Indeed, a recent review showed that only 19% of the published cases of individuals with acquired CSO had premorbid interests in children (27), highlighting that the hypothesis based on the unmasking of previous paedophilic tendencies may not fully explain the phenomenon. Said review suggests that acquired CSO might be one of many symptoms of a general disinhibition syndrome following basal frontotemporal damage, or at least of a hypersexuality-related disorder induced by subcortical damage. Whether dis-inhibition is sufficient to cause the onset of acquired CSO is still not known. Research has been scant, but individuals with acquired CSO typically manifest a behavioural fracture resulting in sexual offenses against children (10, 13, 28–30).
Developmental and acquired CSO seem to therefore represent two distinct conditions (21). The key distinction lies in their nature: developmental CSO is often associated with paedophilia, resulting in a paedophilic disorder (3). Multiple theoretical models have been proposed to explain paedophilic disorder, which can generally be categorized into three main approaches: (1) theories highlighting paedophilic disorder’s predetermined and/or unchangeable nature (i.e., evolutionary; 31) or genetic accounts (32); (2) those emphasizing its neurodevelopmental nature (33); (3) and those emphasizing a multifactorial explanation (34–36). In contrast, acquired CSO occurs de novo, as a symptom of an underlying medical condition (21, 29, 37, 38). In fact, individuals with acquired CSO are usually characterized by a late onset of paedophilic urges, which arises independently of their developmental trajectory (13, 28). This distinction has important implications for treatment. In cases of developmental CSO, pharmacological or non-pharmacological treatments should focus on managing paedophilia itself – when present – (39, 40). Conversely, treatment for acquired CSO should target the underlying condition (13, 26).
From a neuropsychological perspective, individuals with developmental paedophilic disorder present a complex cognitive profile that has been relatively well characterised, though findings remain mixed and are constrained by some methodological limitations, most notably the inclusion of heterogeneous offender samples, that often conflate individuals with and without a formal diagnosis of paedophilia. Overall, intellectual functioning tends to fall within the average range, with most studies reporting no significant IQ differences between paedophilic and non-paedophilic sexual offenders (41–44). Executive functions have been a key focus of investigation. While working memory, set-shifting, and planning abilities are generally preserved, some studies suggest relative weaknesses in processing speed, verbal fluency, and inhibitory control (see 43 for a summary). Recent findings by Picard et al. (43) further refine this profile by comparing the cognitive performance of 58 men convicted of various sexual offenses (including contact sexual offenses, non-contact sexual offenses, and child sexual abuse material), 20 of whom were diagnosed with paedophilic disorder. Interestingly, those with paedophilic disorder outperformed non-paedophilic offenders on tasks assessing verbal memory and visual discrimination, but made more errors on a set-shifting task, suggesting subtle difficulties with cognitive flexibility. Notably, all groups performed within the normative range across cognitive domains, pointing to mild rather than overt cognitive impairments (43).
By contrast, the neuropsychological profile of individuals with acquired CSO remains poorly defined by systematic research and is primarily reconstructed from individual case studies. Nevertheless, a consistent pattern emerges across cases, typically involving impairments in executive functions – particularly in impulse control, social cognition, and moral reasoning – which typically reflect the nature and localisation of the underlying organic pathology. For example, Burns and Swerdlow (13) described a patient with an orbitofrontal tumour who developed paedophilic behaviour alongside disinhibition, impaired moral judgement, and poor insight, all of which resolved after tumour resection. Similarly, Sartori et al. (26) reported a case involving compression of the hypothalamus and the orbitofrontal cortex by a Clivus Chordoma, where impulsive sexual offences occurred within the broader context of dysexecutive syndrome and diminished social and moral awareness. These deficits were not only evident in formal neuropsychological testing but also manifested in daily life, as observed by relatives and clinicians. Taken together, these findings underscore the aetiological and clinical divergence between developmental and acquired CSO, suggesting that similar behaviours may be underpinned by fundamentally distinct neuropsychological mechanisms.
The neural bases of developmental and acquired CSO are also distinct and reflect the different nature of these two forms of offending behaviour. Structural alterations in developmental P+CSO are observed in both grey (45) and white matter (7). While findings are heterogeneous, one result replicated across multiple studies is reduced right amygdala volume in individuals with P+CSO compared to controls (46–48). Regarding functional alterations, studies have suggested that brain activity is not generally altered in developmental CSO but deviates specifically in response to sexual stimuli (49–55). These alterations are primarily localised in the left anterior insular cortex, the left claustrum, and the anterior midcingulate cortex – key hubs of brain networks regulating sexual arousal (56). In contrast, acquired CSO, being a consequence of an underlying neurological condition, is characterized by evident brain lesions or alterations that may be the result of various causes, including traumatic (38, 57), neoplastic (13), surgical (28), degenerative (58), or demyelinating origin (14, 27, 37).
Overall, the neural basis of developmental and acquired CSO described in the literature seem spatially heterogeneous, hampering a clear understanding of the neural origin of these offending behaviours (15). However, a critical distinction emerges when comparing the two conditions. A recent meta-analysis by Scarpazza et al. (59) investigating structural and functional neuroimaging studies in individuals with developmental paedophilia failed to identify consistent brain alterations, even when applying liberal statistical thresholds. The findings revealed high variability in the localization of reported brain changes, with some clusters emerging only under exploratory analyses, such as in the middle cingulate, superior frontal, and occipital gyri. This lack of convergence suggests that developmental CSO is likely underpinned by distributed and subtle neural alterations that do not consistently affect the same anatomical and functional substrates across individuals. Such heterogeneity may reflect the multifactorial aetiology of paedophilic disorder, encompassing genetic, neurodevelopmental, and psychosocial components (36), and highlights the challenges of identifying a single neurobiological model to account for this condition. In contrast, for acquired CSO, progress has been made in linking behaviour to specific neural networks. Although brain lesions in individuals with acquired CSO are also spatially heterogeneous, by means of lesion mapping analysis Scarpazza, Finos et al. (23) identified a shared brain network consistently damaged in all cases included in the analysis. This network includes the orbitofrontal cortex bilaterally and posterior midline structures, such as the posterior cingulate cortex and praecuneus. Moreover, Joyal (27) highlighted the potential influence of damage to the basal frontotemporal regions as well, including basal temporal areas, further enriching our understanding of the neural basis of acquired CSO. This convergence onto specific neural networks for acquired CSO has been supported by a functional characterization approach (60, 61). This method links brain regions to the psychological functions they are most likely to underlie based on patterns of experimental activation derived from the literature. While this approach was not applicable to developmental CSO due to inconsistent neural findings, its application to acquired CSO has provided significant insights, linking the orbitofrontal cortex to action inhibition and the posterior midline structures to social cognition, specifically to the construct of theory of mind, the ability to understand the social and moral disvalue of one’s actions, and the capacity to discriminate right from wrong (23). These findings underscore that acquired CSO may be traced back to deficits in specific neural networks, particularly those supporting inhibitory control and social cognition (23). Such impairments likely diminish the ability to regulate inappropriate urges and undermine moral and social awareness, thereby contributing to offending behaviours. This stands in contrast to developmental CSO, where the lack of spatially convergent neural alterations suggests a more heterogeneous and sparse neurobiological basis, complicating efforts to establish a coherent brain-behaviour model.
The presence of cognitive difficulties in individuals with acquired CSO is reflected in their modus operandi, which is described as impulsive and disorganized in the literature. Offenses are often characterized by lack of premeditation, an absence of attempts to mask the behaviour, and a tendency toward spontaneous confession (62). These traits align with the findings from three major reviews on acquired CSO (14, 27, 59) which conclude that in the majority of the reviewed cases (82% according to 27), acquired paedophilic behaviours involve generalized behavioural impulsivity, including hypersexuality. In contrast, the modus operandi of individuals with developmental CSO suggests intact inhibition and social cognition, as individuals show some degree of voluntary behavioural control (63–65), and offenses are typically premeditated, and there is often an attempt to induce the victim to silence about the crime (63, 66, 67). This behavioural pattern has led to developmental CSO being conceptualized as a compulsive rather than an impulsive disorder (63).
Although the neuropsychological underpinnings of individuals with developmental CSO have been widely studied in recent years (68, 69), inconsistencies in the literature remain regarding the cognitive profiles of these individuals, particularly in the domain of impulsivity, as demonstrated by contradictory findings across studies (70, 71). Notwithstanding the advances in knowledge achieved so far, it remains unclear whether the two forms of CSO differ regarding the cognitive profile (15, 21, 36, 62).
To address these gaps, in the current study we investigated the cognitive profile of individuals who committed sexual offenses against children, focusing on whether neuropsychological differences can explain their behaviours. Specifically, we aimed to determine whether individuals who exhibited developmental CSO and individuals with acquired CSO are characterized by similar or different cognitive/neuropsychological underpinnings.
On the one hand, for developmental CSO, we conducted a multivariate and mixed-effect meta-regression meta-analyses on 34 studies, incorporating data from individuals convicted for CSO with a formal diagnosis of paedophilia (P+CSO) and those without (CSO). Moreover, by analysing these groups separately, we sought to clarify whether any observed cognitive deficits were more strongly linked to paedophilia itself or to committing child sexual abuse in general. On the other hand, for acquired CSO we performed a systematic review due to the reliance on case reports rather than group-level studies. This involved extracting detailed information on the cognitive abilities of individuals and quantifying the prevalence of specific impairments across cases.
By integrating quantitative and qualitative approaches, this study provides a comprehensive framework to investigate the neuropsychological mechanisms underlying developmental and acquired CSO. This analysis not only addresses inconsistencies in the literature but also offers insights into how distinct cognitive profiles might influence the behaviours associated with this form of offending.
2 Materials and methods
2.1 Meta-analysis on developmental CSO
2.1.1 Search strategy
Following PRISMA Guidelines (72), an in-depth search was conducted on PubMed (up to October 2022) using the following terms:
(pedophilia) OR (idiopathic pedophilia) OR (developmental pedophilia) OR (pedophilic behavio*) OR (child sex* offen*) OR (child molest*) OR (sex offen* against child*)) AND ((neuropsychologic test) OR (executive functions) OR (cognition) OR (impaired cognition)).
Medical Subject Headings (MeSH) searches were also performed. Abstracts and titles were screened, followed by full-text evaluation against inclusion and exclusion criteria. Lastly, reference lists of relevant reviews and meta-analyses were inspected to identify additional studies.
2.1.2 Inclusion and exclusion criteria
Studies were included if they met the following criteria: (a) studies presenting original data on the cognitive/neuropsychological performance of individuals who committed sexual offenses toward children, either with (P+CSO) or without (CSO) a formal diagnosis of paedophilia; (b) studies including a matched control group of healthy subjects or individuals who did not commit sexual offenses against children, or individuals with paedophilia or paedophilic disorder, but without a history of child sexual offenses (P-CSO); and (c) studies published in peer-reviewed journals in English.
Studies were excluded if they: (a) were reviews, meta-analyses, instrument validation studies, or case reports; (b) analysed mixed and/or heterogenous groups together, such as P+CSO, CSO without paedophilia, and P-CSO; (c) lacked a comparison group; or (d) did not provide minimal statistical data to compute effect sizes (e.g., sample size, mean, standard deviation).
2.1.3 Data selection and extraction
Data extracted from each paper included sample size, mean (M), and standard deviation (SD) for cognitive and neuropsychological performance across the following domains: set switching, planning/reasoning, memory, attention, working memory, verbal fluency, verbal semantic, abstraction, social cognition, and inhibition. The choice to analyse these specific cognitive functions reflects the neuropsychological batteries and tests commonly used to assess the populations of interest in clinical and scientific settings.
Data extraction was conducted by the first author (CC) and independently checked by the last author (CS).
2.1.4 Statistical analysis
To calculate effect sizes and standard errors for each observation, we utilised the metafor package (v. 3.4.0) in R (v. 4.1.2) (73). A random-effects meta-analysis was conducted to estimate weighted average effect sizes (g). The present meta-analysis involved observed outcomes/effect size estimates that cannot be assumed to be independent, because some studies contributed with multiple effect sizes due to the administration of multiple neuropsychological tests; therefore, the sampling errors in such studies are dependent and represent correlated effects (74). To address this, a variance–covariance matrix of the dependent estimates was constructed using the vcalc function, and a multivariate model was fitted using the rma.mv function, specifying the random-effects structure and fitting the model via restricted maximum likelihood estimation.
We assumed a constant within-study correlation of ρ = 0.30 between sampling errors, following prior influential studies, systematic reviews, and meta-analyses (e.g., 35, 75, 76). While the true correlation may vary across studies, this assumption allows for a principled modelling of within-study dependence and is further mitigated by the use of robust variance estimation to guard against model misspecification. In fact, since the variance-covariance matrix is only a rough approximation and the random-effects structure may not fully capture all dependencies in the underlying real outcomes/effects, a cluster-robust inference method - also known as ‘robust variance estimation’ - was applied to the model via the clubSandwich package (74). Tests of individual coefficients used a t-distribution, with degrees of freedom approximated using the Satterthwaite method. Omnibus tests were based on an F-distribution, with degrees of freedom approximated using an approximate Hotelling’s T-squared distribution (77–79).
To examine which coefficients might moderate the outcome, three mixed-effects meta-regression models were examined, each with multiple coefficients, as follows (73, 80):
1. Cognitive domains: set switching, planning/reasoning, memory, attention, working memory, verbal fluency, verbal semantic, abstraction, social cognition, and inhibition.
2. Control group typology: healthy controls, nonsexual offenders, sexual offenders against adults, internet offenders, child pornography users, and individuals with paraphilia or unspecified mental conditions.
3. Study group typology: individuals with (P+CSO) or without (CSO) a formal diagnosis of paedophilia.
For each model, we assessed the significance of both the overall model and individual coefficients, with and without the inclusion of the intercept (where appropriate). Coefficients were transformed into dummy coded variables by means of the factor function in R. Including the intercept allows comparisons against a reference category; while excluding it estimates effects for each category independently, so that coefficients represent average effect sizes for the corresponding category. This dual approach improves interpretability and ensures that findings are not dependent on arbitrary reference choices, providing a more comprehensive view of moderator effects.
Heterogeneity was evaluated using the restricted maximum likelihood estimator (81) and the Q-test for heterogeneity (82). Studentized residuals and Cook’s distances were employed to identify potential outliers and influential studies in the context of the present statistical model (80). On the one hand, studies with studentized residuals exceeding the percentile of a standard normal distribution were flagged as potential outliers using a two-sided Bonferroni correction. On the other hand, studies with a Cook’s distance greater than the median and six times the interquartile range of the Cook’s distance were considered influential, indicating that these studies had a disproportionate impact on the overall model fit.
Funnel plot asymmetry was assessed using two statistical tests: the rank correlation test (83) and the regression test (84), with the standard error of observed outcomes serving as the predictor variable. Outlying cases were evaluated based on their influence on the overall model. An outlier was considered inconsequential if it exerted minimal impact on the results. However, if removing a study led to substantial changes in the fitted model, the study was deemed influential (80). To identify influential studies, case-deletion diagnostics, known from linear regression (e.g., 85), were adapted to the meta-analysis by means of the influence() function, which provided leave-one-out diagnostics for each study, including: (1) externally standardised residuals, to detect unusual deviations; (2) difference in fits (DFFITS), to measure the influence of each study on the fitted values; (3) Cook’s distances, to assess the overall impact of a study on the model; (4) covariance ratios, to identify changes in model stability; (5) DFBETAS values, to evaluate the influence of individual observations on specific coefficients; (6) estimates of Tau², to measure between-study variance (heterogeneity) when removing each study; (7) heterogeneity test statistics, to assess changes in residual heterogeneity; (8) hat matrix diagonal elements, to evaluate leverage; (9) model weights, to determine the contribution of each study during model fitting.
Finally, the analyses were repeated with the study group split into two subgroups: individuals who committed sexual offenses against children with a formal diagnosis of paedophilia and those without, to examine differences linked to sexual preference versus offending behaviour.
2.2 Systematic review on acquired CSO
2.2.1 Inclusion and exclusion criteria
Studies were included if they: (a) provided original reports of late onset CSO; (b) documented an organic condition temporally associated with the emergence of CSO.
Studies were excluded if they: (a) described the emergence of paedophilia without documenting CSO; (b) included patients with medical conditions who manifested CSO prior to the onset of the illness. Of note, the presence of paedophilia (i.e., attraction towards children upon which the individual has not acted) before the onset of the medical condition was not considered an exclusion criterion.
2.2.2 Data selection and extraction
Cases of acquired CSO were identified through an existing systematic review (62) conducted in accordance with PRISMA guidelines (72), which was subsequently updated to include more recent studies. In particular, the original search string was run another time: ((pedophilia) OR (pedophilic behavio*) OR (child sex* offen*) OR (child molest*) OR (sex offen* against child*)) AND ((acquired) OR (de novo) OR (dementia) OR (brain lesion) OR (neurology*) OR (late onset)).
Two authors (CS, CC) independently extracted and screened the data, with random verification by a third author (SF). Extracted data included: neurological aetiology, brain localization, neurological symptoms, and cognitive impairments. Furthermore, based on the patient’s description, additional information was gathered regarding cognitive functioning, with particular attention to social cognition (specifically the construct of theory of mind, the ability to understand the social and moral disvalue of one’s actions, and the ability to discriminate right from wrong) and impulsive behaviour.
2.2.3 Statistical analysis
Given the reliance on case reports, only descriptive statistics were computed. The percentage of patients presenting intact versus impaired cognitive functions was calculated across cases.
3 Results
3.1 Meta-analysis on developmental CSO
3.1.1 Selected studies
The bibliographical search identified 163 entries. After duplicates removal, 148 records were screened. We excluded 70 articles as they did not meet the eligibility criteria, being: reviews (n = 7), meta-analyses (n = 5), case reports (n = 5), papers describing cases of acquired CSO (n = 2), studies presenting a new nonpharmacological treatment (n = 4), clinical trials (n = 5), hands-on (P+CSO/CSO) and hands-off (P-CSO) mixed study groups, or unrelated papers (n = 41). The remaining 78 records underwent full-text assessment, leading to the exclusion of 44 articles for the following reasons: (a) lack of cognitive or neuropsychological data (n = 31); (b) absence of a control group (n = 10); (c) insufficient statistical information to compute effect sizes (n = 3).
Ultimately, 34 articles were included in the meta-analysis, comprising 4093 subjects: 846 P+CSO, 1110 CSO, and 2137 controls (please see Supplementary Table 1). Control groups included healthy individuals (n = 966) and other subgroups such as: individuals with paraphilia (n = 56), nonsexual offenders (n = 306), online child offenders (n = 505), individuals with unspecified mental conditions (n = 15), adult sexual offenders against adults (n = 187), and child pornography users (n = 61).
Figure 1 shows the PRISMA flowchart of the search strategy and the selection of the studies for the meta-analysis.
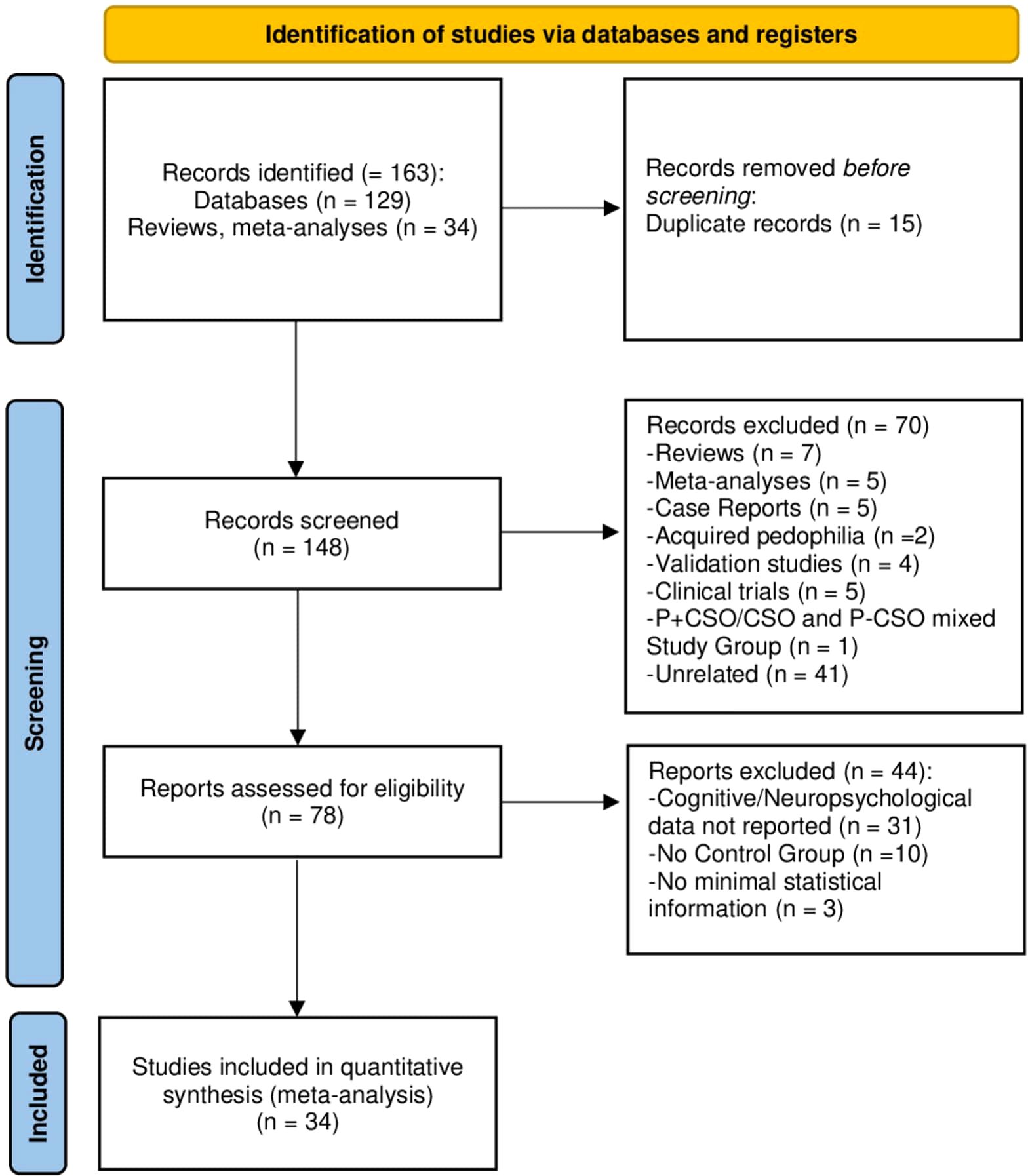
Figure 1. PRISMA flowchart illustrating the selection process of the present meta-analysis for developmental CSO.
3.1.2 Publication bias and influential effect sizes
The 34 included studies accounted for 192 effect sizes. The Q-test revealed significant heterogeneity among true outcomes (Q(191) = 247.471, p = .004). Examination of studentized residuals revealed no values exceeding ±3.652, indicating no outliers within the context of the model. However, Cook’s distances flagged two effect sizes as overly influential. Case-deletion diagnostics (Supplementary Figure 1) confirmed that the absolute DFFITS values for these two effect sizes exceeded the threshold of , where p represents the number of model coefficients and k the total number of observations/effect sizes. The removed effect sizes were: −1.115 (DFFITS: −0.215) from Herrero et al. (86), and −1.735 (DFFITS: −0.264) from Becerra-Garcia & Egan (87). After outlier removal, the final analysis included 190 effect sizes from 34 studies. Despite the removal of these outliers, heterogeneity among true outcomes remained significant (Q(189) = 224.649, p = .039). Examination of the studentized residuals indicated the absence of outliers in the context of this model. The regression test detected funnel plot asymmetry (p = .03) (Figure 2), while the rank correlation test did not (p = .010). Residual heterogeneity (QE-test) was significant when study group typologies were included as coefficients, but it was not significant in the mixed-effects meta-regression models that accounted for cognitive domains or control group typologies. In summary, once cognitive domains and control group typologies were included as coefficients, the variability between studies was no longer statistically significant, suggesting these factors help explain the observed heterogeneity.
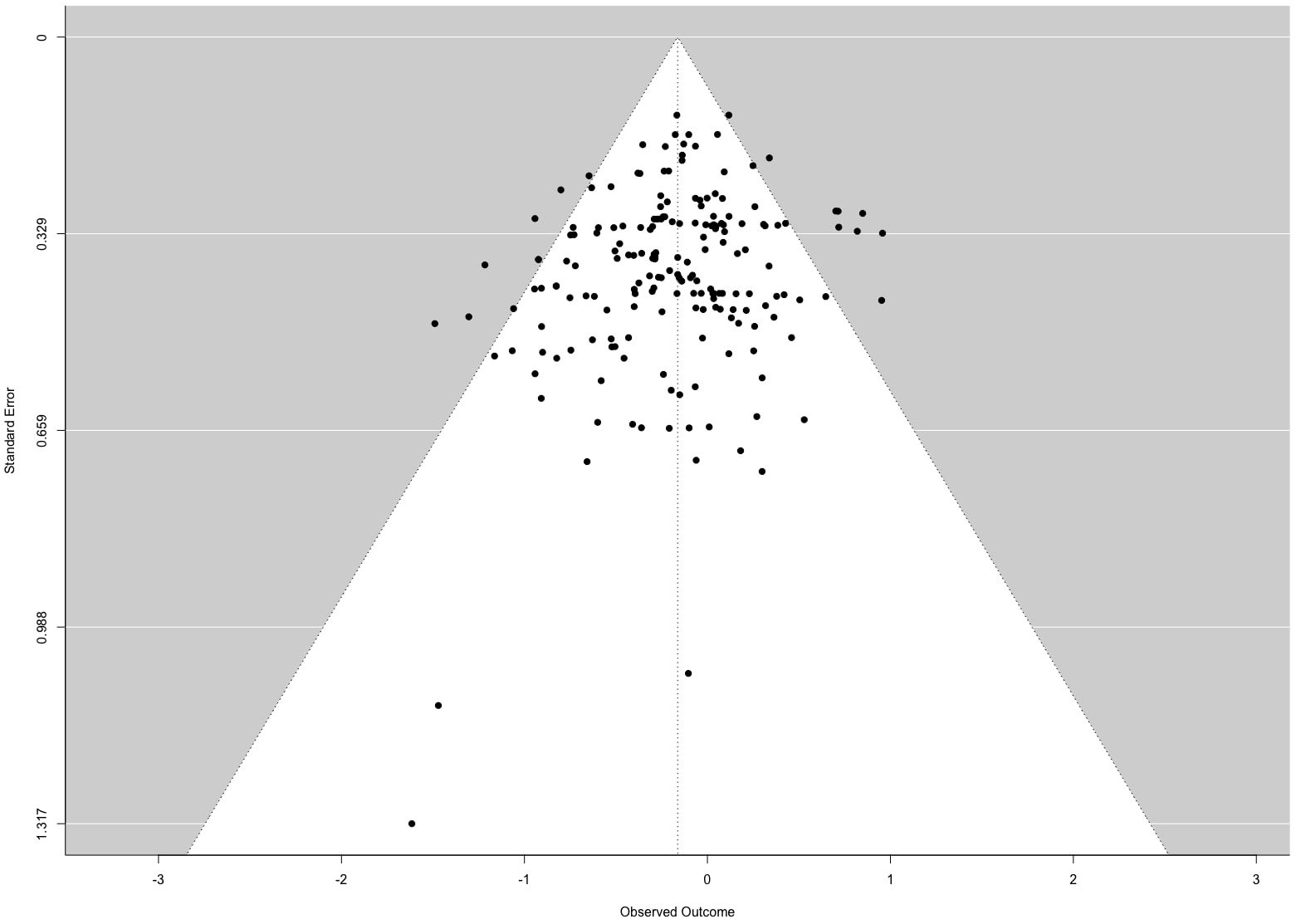
Figure 2. Funnel plot of the 34 studies included in the meta-analysis.
3.1.3 Multivariate meta-analysis
Across all effect sizes, observed outcomes ranged from −1.615 to 0.957, with 67% of estimates being negative. The random-effects model fitted with a cluster-robust inference method yielded a pooled effect size of μ = −0.186 (95% CI: −0.296 to −0.077, p = .002), indicating that individuals in the study group achieved worse cognitive/neuropsychological performances compared to controls (see Table 1). To examine which factors contributed to this result, mixed-effects meta-regression analyses were conducted.
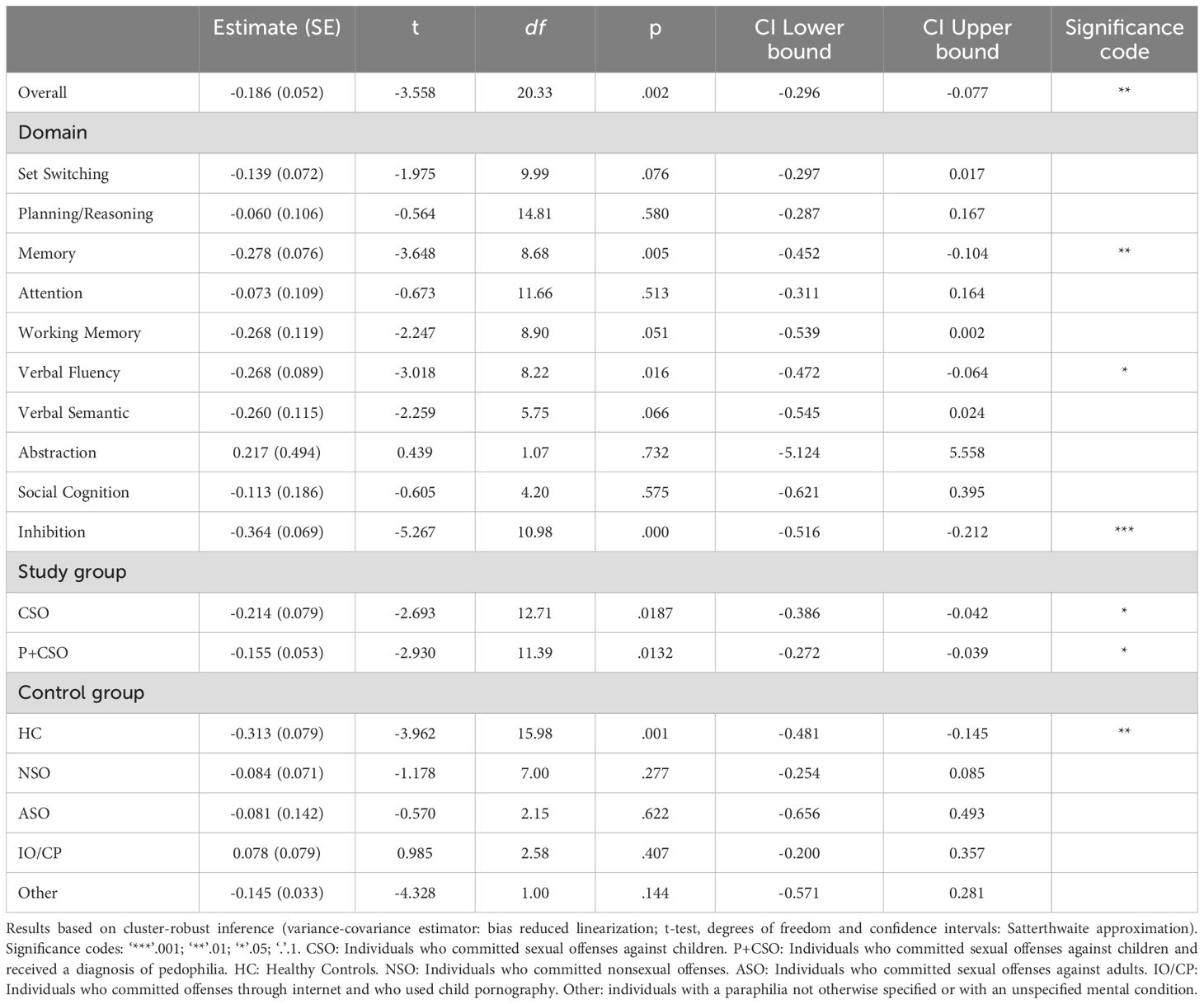
Table 1. Overall: Multivariate meta-analysis; Domain, Study group, Control group: Mixed-effects meta-regression models.
3.1.4 Mixed-effects meta-regression
Mixed-effects meta-regression identified significant effects inthree cognitive domains: memory (t = -3.648, p = .005), verbal fluency (t = −3.018, p = .016), and inhibition (t = -5.267, p = .000) (Table 1). However, the omnibus F-test evaluating the joint significance of all coefficients was not significant (F = 3.027, df1 = 10, df2 = 3.03, p = .194). In other words, while the study group showed significantly worse performance than controls in these specific domains, the combined set of domain-level coefficients did not explain a statistically significant amount of variance in cognitive performance.
Meta-regression by study group revealed significant effects for both groups: CSO (t = -2.693, p = .0187) and P+CSO (t = -2.930, p = .0132) (Table 1), indicating worse cognitive/neuropsychological performance in each subgroup relative to controls. The omnibus test for this model was also significant (F = 6.159, df1 = 2, df2 = 15.44, p = .011), suggesting that, collectively, the set of coefficients for the study subgroups accounted for a significant portion of the variance in performance. A direct comparison between the P+CSO and CSO subgroups (with CSO set as the intercept) revealed no significant difference (t = 0.681, p = .503) (Table 2).
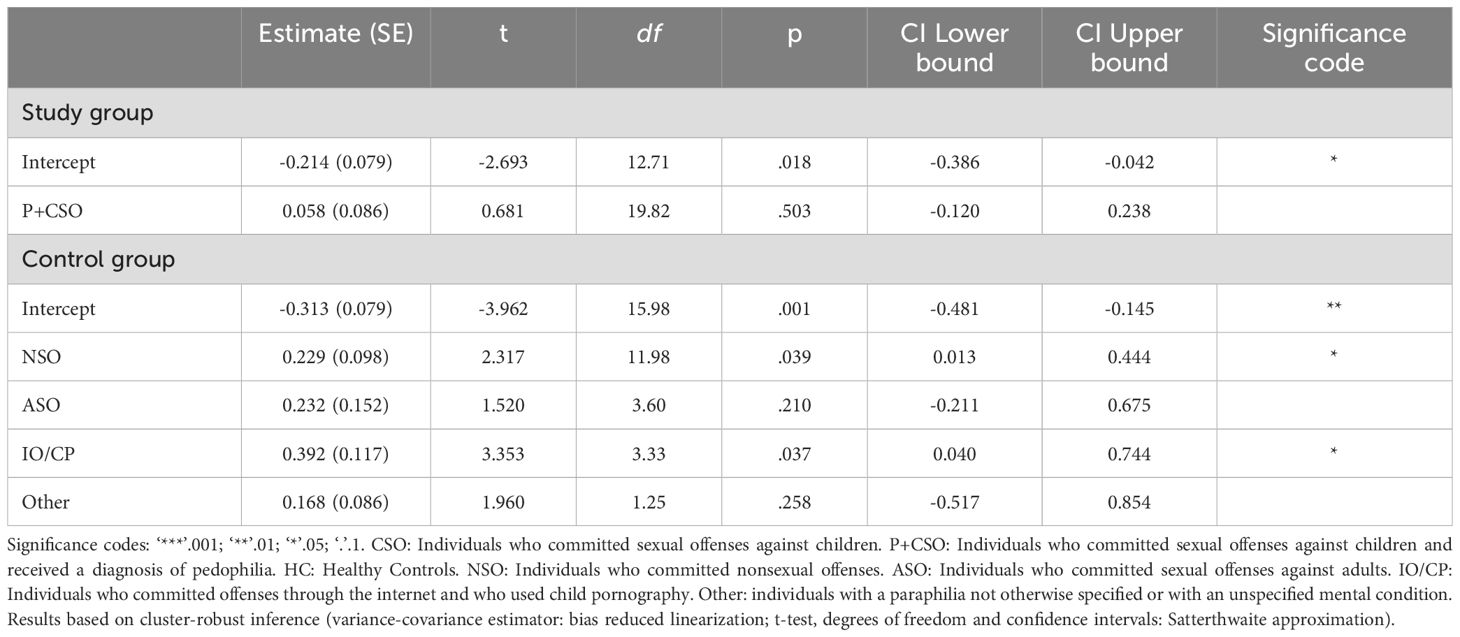
Table 2. Mixed-effects meta-regression models with intercept.
Analysis by control group typology showed a significant effect for the healthy controls’ coefficient (t = −3.962, p = .0011) (Table 1). The omnibus F-test was not significant (F = 2.918, df1 = 5, df2 = 2.82, p = .213). That is, the study group showed statistically significant worse cognitive/neuropsychological performances only when compared with healthy controls, and the combined set of coefficients for the control subgroups did not account for a statistically significant portion of the variance in cognitive performance. Direct comparisons between healthy controls, set as the intercept, and the other control subgroups revealed significantly different average effects for both individuals who committed nonsexual offenses (t = 2.317, p = .039) and individuals who committed offenses against children through the internet and used child pornography (t = 3.353, p = .037), compared to healthy controls (Table 2). No significant differences were found for other control groups, including sexual offenders against adults or individuals with paraphilias not otherwise specified (Table 2).
3.1.5 Sensitivity analysis
To further explore whether a specific type of control group influenced the results of the meta-regression model with cognitive domains as coefficients, a meta-regression analysis was conducted for inhibition, memory, and verbal fluency, with control group as coefficients (Table 3; Supplementary Figures 2, 3, and 4, respectively). Some coefficients were excluded due to insufficient effect sizes (Table 3). The meta-regression model was significant for healthy controls with respect to inhibition (t = -3.512, p = .010) and memory (t = -4.517, p = .011). However, omnibus tests for these models were nonsignificant (inhibition: F = 1.809, df1 = 4, df2 = 1.87, p = .396; memory: F = 3.599, df1 = 3, df2 = 2.06, p = .203). These mixed results complicate distinguishing true effects from potential Type I errors. Overall, individuals with developmental CSO (CSO and P+CSO) exhibited poorer performance in inhibition and memory performances compared to healthy controls.
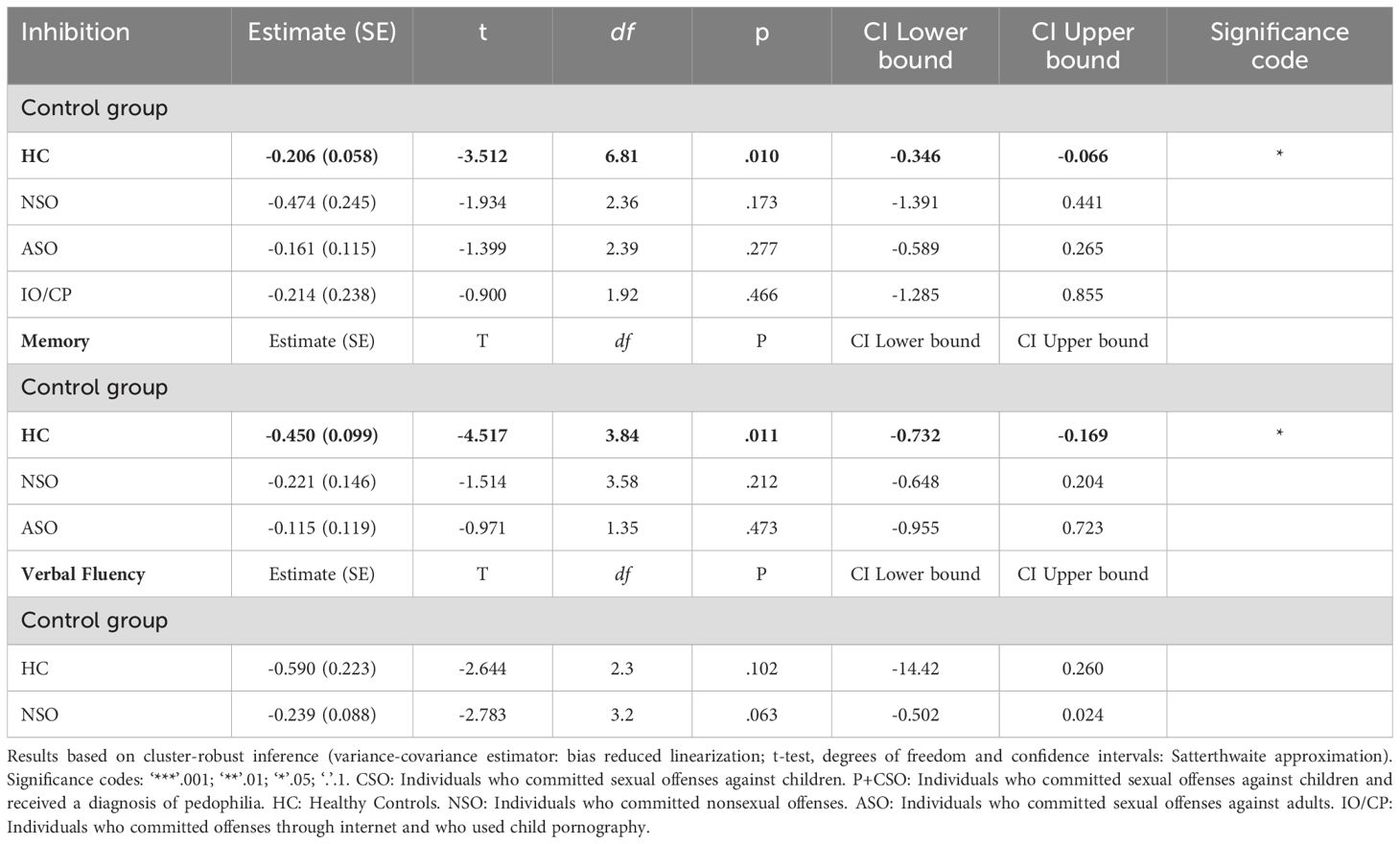
Table 3. Mixed-effects meta-regression model with control group typologies as coefficients, restricted to inhibition, memory and verbal fluency.
3.1.6 Multivariate meta-analysis and mixed-effects meta-regression with split study group
The random-effects model on the CSO group, fitted with a cluster-robust inference method, produced a pooled effect size of μ = −0.232 (95% CI: −0.405 to −0.060, p = .011), indicating significantly poorer cognitive/neuropsychological performance in the CSO group compared to controls (Table 4). Mixed-effects meta-regression revealed significant domain effects for memory (t = -5.601, p = .002), verbal fluency (t = −2.910, p = .031), and inhibition (t = -3.058, p = .015). As for the typology of control group, a significant effect was also observed for the healthy controls’ coefficient (t = -3.610, p = .003) (Table 4).
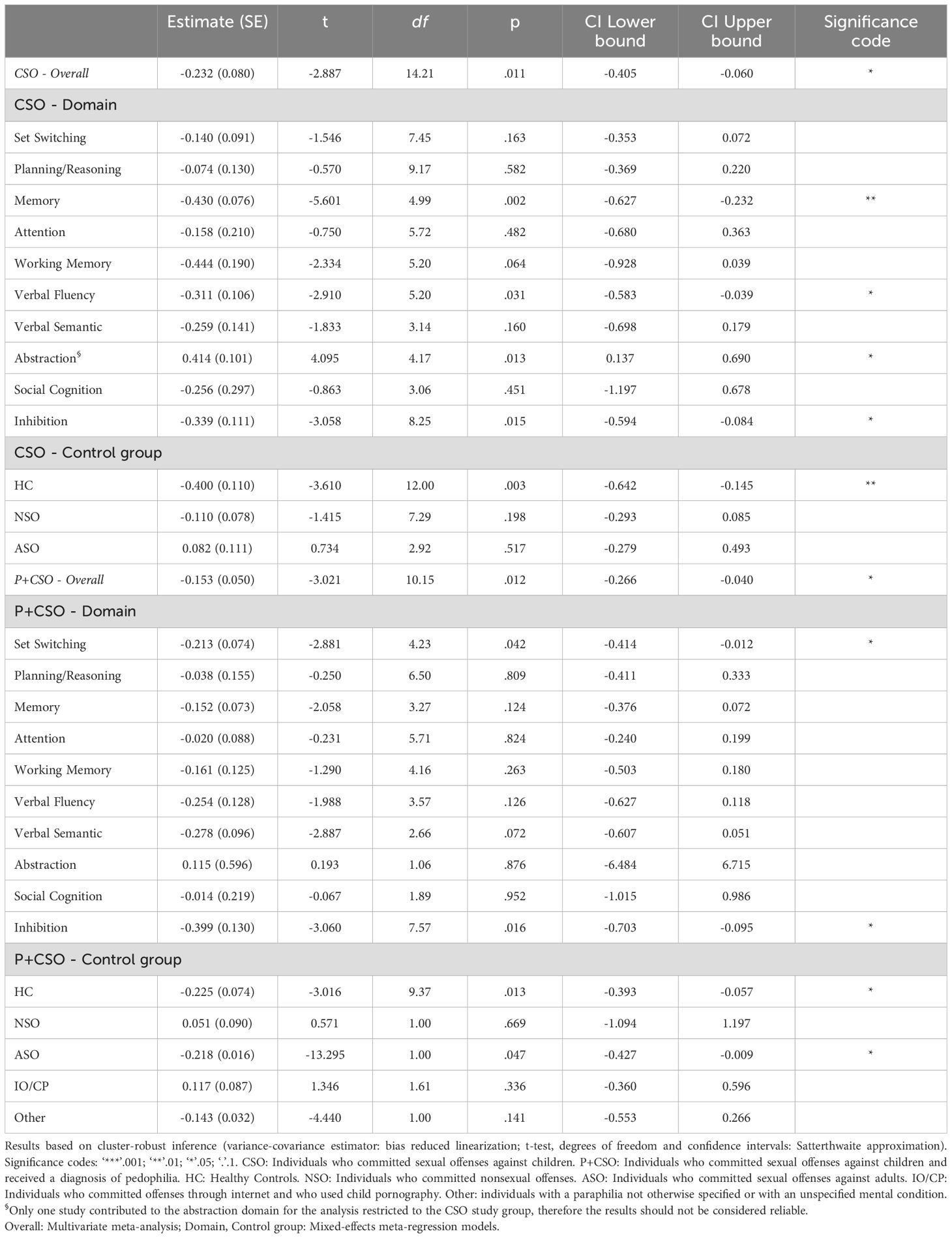
Table 4. Main analyses divided for study groups.
For the P+CSO group, the pooled effect size was μ = −0.153 (95% CI: −0.266 to −0.040, p = .012), again reflecting significantly worse cognitive performance compared to controls (Table 4). Mixed-effects meta-regression revealed domain-specific effects for set switching (t = -2.881, p = .042), and inhibition (t = -3.060, p = .016). Regarding control group typology, significant effects were identified for healthy controls’ coefficient (t = -3.016, p = .013), and for individuals who committed sexual offenses against adults (t = -13.295, p = .047) (Table 4).
3.2 Systematic review on acquired CSO
A total of 21 papers were identified through the literature search, describing 26 cases of late-onset CSO. The full-text analysis based on the eligibility criteria led to the inclusion of 21 cases from 17 papers (Figure 3). A summary of the brain pathologies and the corresponding anatomical localisation of lesions for each case of acquired CSO included in the systematic review is provided in Supplementary Table S2.
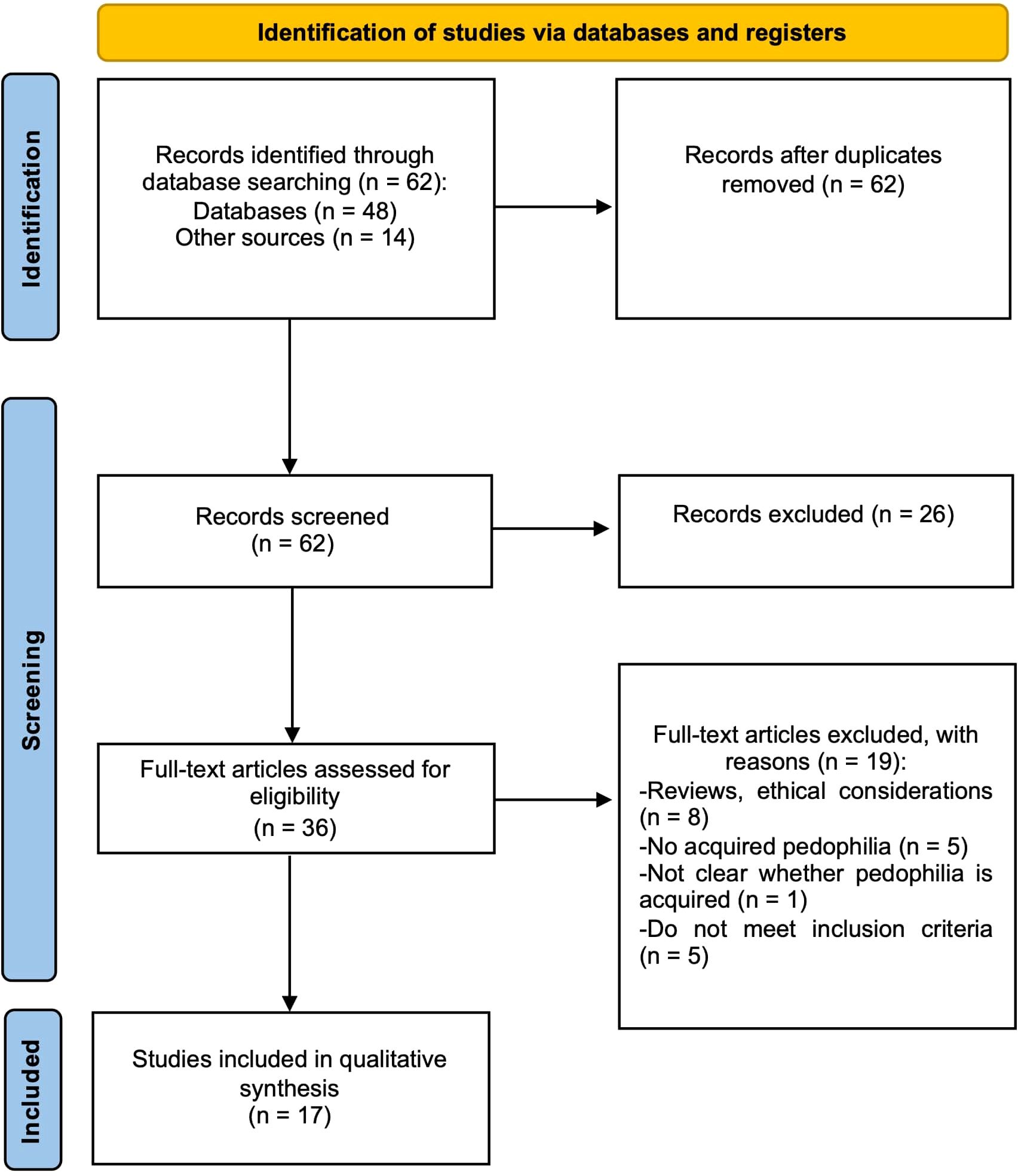
Figure 3. PRISMA flowchart illustrating the selection process of the systematic review on acquired CSO.
3.2.1 Excluded studies
Several case reports were excluded based on the following specific criteria:
• Lack of a neurological condition:
Prahlada Rao et al. (88): the patient exhibited cognitive impairments, but no underlying neurological condition was identified as the MRI results were normal.
Regestein and Reich (89): patients 2, 3, and 4 were excluded due to the absence of a confirmed neurological condition.
• Absence of child sexual offenses:
Alnemari et al. (57): the patient displayed increased sexual interest in children following a traumatic brain injury (left basal frontal and bilateral temporal contusions), but did not commit sexual offenses against children.
• Offenses predating the neurological condition:
Prado et al. (25): a patient with frontotemporal dementia was excluded after it was discovered that sexually inappropriate behaviours toward his daughter occurred years before the onset of the neurological condition.
Mendez et al. (65) and Mendez (58): both cases were excluded because the individuals committed child sexual offenses prior to the onset of their neurological conditions.
3.2.2 Neuropsychological results
Table 5 provides an overview of the neuropsychological profiles of patients with acquired CSO, focusing on the same cognitive domains assessed for developmental CSO. While most studies reported that formal neuropsychological evaluations had been conducted, specific details such as test scores and the names of the assessment techniques employed were frequently absent. However, the available descriptions of patients’ daily-life challenges, offenses, and modus operandi allowed a comprehensive evaluation of critical cognitive functions, particularly social cognition and impulse control (see Supplementary Table 2 for details). Interestingly, all but two patients displayed neurological symptoms alongside cognitive impairment, consistent with the neurological nature of acquired CSO.
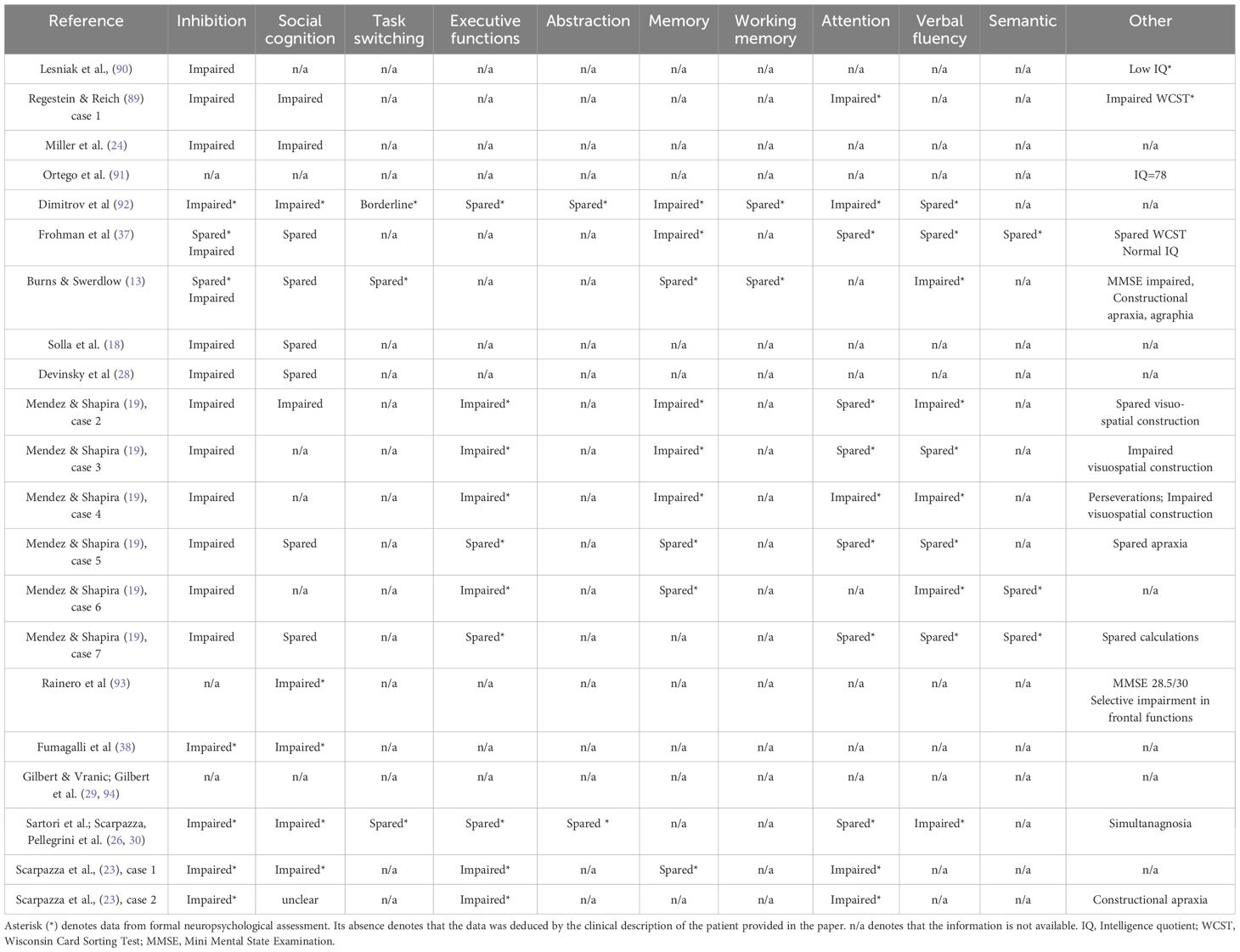
Table 5. Neuropsychological profile of patients with acquired CSO.
Key findings
● Social cognition: information on the ability to understand the social and moral disvalue of sexual offenses was available for 16 out of 21 cases (76%). Of these, 62.5% (10/16) demonstrated impaired understanding of the wrongfulness of their actions, while 37.5% (6/16) retained this ability.
● Impulse control: sufficient data on impulse control was provided in 19 of the 21 cases (90.5%), with all individuals (100%) exhibiting significant impulsivity at the time of the crime. This impulsive behaviour was also observed in their everyday lives, further supporting its pathological nature.
● Cognitive domains: impairments were frequently noted across a range of cognitive domains. Executive functions were assessed in 13 patients, with 61.5% (8/13) showing deficits. Verbal fluency, evaluated in 10 cases, was impaired in 60% (6/10). Memory, tested in 9 patients, was defective in 55.5% (5/9). Lastly, attention abilities, assessed in 11 patients, were found to be impaired in 45.5% (5/11).
4 Discussion
In the current study, we examined the cognitive profile of individuals who committed sexual offenses against children, aiming to frame their behaviour in the context of its neuropsychological underpinnings. To this end, we conducted a meta-analysis on 34 studies, including a total of 846 individuals with P+CSO, 1110 individuals with CSO, and 2137 controls, alongside a systematic review of 21 cases of acquired CSO.
4.1 Summary of the results
The meta-analytical approach revealed that individuals with developmental CSO tend to exhibit a cognitive profile characterised by impairments in inhibition, memory, and verbal fluency compared to healthy controls. The deficits observed were of medium effect size, according to Cohen’s thresholds (95, 96). Given the complexity of the statistical models and the number of analytical decisions involved, readers are advised to interpret the present results with caution, as they may be influenced by model specifications and underlying assumptions.
Importantly, when individuals with developmental CSO were analysed separately, based on whether they had a formal diagnosis of paedophilia, individuals without a formal diagnosis of paedophilia (CSO) demonstrated impairments in memory, verbal fluency, and inhibition compared to healthy controls, whereas individuals with a formal diagnosis of paedophilia (P+CSO) showed deficits in set-switching and inhibition compared to both healthy controls and individuals who committed sexual offenses against adults. Of note, these cognitive functions are closely linked to frontal lobe activity (97, 98) and are typically categorised as executive functions. A plausible explanation for these findings lies in the methodological approaches of the included studies. While the CSO group was defined as lacking a formal diagnosis of paedophilia, a detailed examination of the studies suggests that many individuals in this group likely exhibited undiagnosed paedophilic tendencies. For instance, Bartels et al. (99) reported increased sexual interest in children among subjects with CSO compared to controls. Moreover, Turner et al. (100) found that CSO individuals rated images of children as significantly more sexually arousing than controls. Finally, Veneziano et al. (101) highlighted that CSO individuals included in their study exhibited known risks factors for paedophilic disorder. These observations suggest that the CSO group likely included a substantial proportion of individuals with undiagnosed paedophilic disorder, which could have influenced the results.
This phenomenon of underdiagnosis is well documented in forensic settings, where paedophilic disorder is frequently not formally identified, even when clinical indicators are present. Several factors may contribute to this trend. First, the pervasive stigma surrounding the diagnosis may lead to reluctance among clinicians to assign it explicitly. Second, diagnostic assessments are often limited by a lack of access to specialised tools and a reliance on self-report measures, which may be distorted by exaggeration, minimisation, or intentional misrepresentation (11). Third, implicit biases may influence evaluators and legal professionals, who may be more inclined to interpret child sexual offending as deliberate and volitional rather than symptomatic of underlying psychopathology, particularly in light of the moral and emotional weight these offences carry. Moreover, in some judicial contexts, there may be institutional resistance to accepting paedophilic disorder as a mitigating factor. Concerns may arise that recognising a psychiatric diagnosis could be seen as diminishing individual responsibility, thus provoking public outrage. However, it is important to emphasise that the attribution of a psychiatric diagnosis does not automatically imply insanity; rather, a separate determination must be made regarding the causal relationship between the mental disorder and the offence, as usually required for assessments of criminal responsibility (e.g., Italian Penal Code; American Model Penal Code §4.01). These systemic and contextual influences likely contribute to the underrecognition of paedophilic disorder in forensic populations, and they should be carefully considered when interpreting the clinical composition and cognitive findings associated with the CSO group.
The systematic review of individuals with acquired CSO, though lacking the quantitative synthesis that enhances the strength of evidence in meta-analyses, provided additional insights. All individuals with acquired CSO manifested impulsivity, and over half showed concomitant deficits in social cognition, specifically in theory of mind abilities and moral reasoning. These deficits were evident in formal neuropsychological assessments and corroborated by reports from relatives about their everyday behaviours. These findings are particularly noteworthy, as the cognitive impairments observed in acquired CSO are not only measurable but also clinically significant at the individual level, underscoring the profound impact of neurological conditions on behaviour and moral judgment.
4.2 Implications for the debate on cognitive functioning
4.2.1 Developmental CSO
Our findings on developmental CSO quantitatively support and extend prior research (43, 102). Consistent with a recent systematic review (102), we observed that individuals with CSO exhibit impaired executive functions, particularly in inhibition and set-switching, while abstraction and planning abilities remain intact. Additionally, our results refine the conclusions of a prior review by Dillien et al. (68), showing that while CSO and P+CSO share overlapping neuropsychological deficits, there are some distinctions. For instance, our meta-analysis clarifies that verbal fluency deficits are specific to CSO and not present in P+CSO when compared to healthy controls. However, unlike prior studies, we did not find evidence of social cognitive deficits in CSO individuals (68). This discrepancy may highlight methodological variations across studies or suggest a more nuanced relationship between social cognition and sexual offending behaviour.
Our results also corroborate previous findings suggesting that executive dysfunction is related to the offending behaviour rather than paedophilic tendencies (42). The shared inhibitory deficits observed in both CSO and P+CSO groups support the motivation-facilitation model of sexual offending proposed by Seto (103), which posits that sexual offenses occur when self-regulation mechanisms fail to suppress inappropriate sexual desires, independently of the target of said desires. Importantly, individuals with paedophilia who do not commit offenses generally do not exhibit inhibitory control deficits (41, 42, 100, 102, 104, 105), although exceptions exist (106).
Despite a failure in the ability to regulate one’s behaviour has been identified as an important predictor for sexual recidivism (107), it remains uncertain whether this impairment in behavioural control is specific to sexual offences against children or indicative of broader antisocial tendencies (108–110). Furthermore, it is still unclear if the findings of diminished cognitive control at formal testing in CSO and P+CSO could be translated to complex decision-making processes in real-life scenarios (42). In our opinion, this behaviour cannot be interpreted as an inability to restrain preponderant action, because sexual offences committed by individuals with developmental CSO cannot be considered impulsive (63).
An interesting hypothesis is that inhibitory deficits observed in P+CSO might be explained by an increased effort required to redirect attention from dominant tendencies (105). This hypothesis is supported by findings of increased Stroop task interference in P+CSO individuals, which correlates with heightened conflict-related activity in the superior parietal lobe and precentral gyrus (105). The authors of this study suggest that potential difficulties in attention reallocation may account for poor impulse control and moderate the risk of committing CSO (105). This hypothesis aligns with our finding that inhibition deficits often co-occur with set-switching impairments in P+CSO individuals. Additional studies are needed to further explore this hypothesis and to test whether this pattern extends to CSO individuals without a formal paedophilia diagnosis.
4.2.2 Acquired CSO
Our results on acquired CSO are consistent with prior research highlighting disinhibition as a hallmark of this condition (27), with hypersexuality often being a behavioural manifestation. However, our study extends previous findings by showing that over half of the individuals with acquired CSO also present deficits in social cognition and moral reasoning. These deficits align with the neurophenomenological model of sexual arousal proposed by Stoléru and colleagues (111), which posits the existence of three main components contributing to sexual arousal: inhibitory control, cognitive evaluation, and autonomic/endocrine processes. More specifically, our findings support the idea that both the inhibitory component (i.e., the ability to withhold the preponderant action) and the cognitive component (i.e., the ability to evaluate one’s own behaviour) are impaired in individuals with acquired CSO. For instance, individuals with acquired CSO often exhibit a sudden breakdown in socially appropriate behaviour, as emerged from formal neuropsychological evaluations and corroborated by reports from close relatives (Supplementary Table 2). This may include an inability to engage in proficient social interactions and a failure to adhere to ethical, social, and legal norms. Combined with behavioural disinhibition, these features help contextualize their criminal modus operandi. We propose that disinhibition alone may not be sufficient to explain CSO, because individuals who are disinhibited but still recognize the moral and legal wrongfulness of offending against children are less likely to seek opportunities to offend and are more likely to pursue therapeutic help. This concept aligns with the actio libera in causa principle (112), which suggests that while an individual may not have full control over their actions during the offense due to disinhibition, they still retain the ability to control the conditions that lead to the offense. According to this hypothesis, a significant proportion of men with developmental paedophilia, who do not typically exhibit impaired social cognition, have never committed sexual offenses and search for help (6, 7, 11). In contrast, when disinhibition is coupled with social cognition deficits, as seen in acquired CSO, individuals are less likely to recognize the wrongfulness of their impulses and thus are more likely to act on them. These findings suggest that acquired CSO is not merely the result of an isolated inhibitory dysfunction, but likely stems from a combined dysfunction in both inhibitory control and social cognition, as proposed in the neurophenomenological model of sexual arousal (111).
Importantly, the differences in the cognitive profile between developmental and acquired CSO identified in the current meta-analysis and systematic review, along with the established differences in the neural bases (59), caution against using acquired CSO as a model to investigate the potential neurobiological basis of developmental CSO, aligning with Joyal’s (27) earlier recommendations.
4.3 Implications for forensic practice
The cognitive profiles of individuals with developmental and acquired CSO offer insights into their distinct modi operandi, which reflect differences in underlying neuropsychological functioning.
4.3.1 Developmental CSO
The modus operandi of individuals with developmental CSO is described in the literature as compulsive rather than impulsive (63). Offenses are often premeditated (63, 66, 67, 113), occurring in private settings and without witnesses, with offenders employing strategies to enforce the victim’s silence (63–65). This level of behavioural control suggests that their inhibitory abilities, while impaired according to formal cognitive evaluations, are sufficient to allow them to delay and structure their actions until conditions are favourable for offending. This apparent discrepancy between experimental findings of inhibitory deficits and observed behaviours in real-life settings could have several possible explanations. First, most of the studies provide group-level data, which may not translate uniformly to individual cases. Second, the effect sizes reported are generally small to moderate. For instance, in the case of inhibition, reaction times between groups usually differ by a few milliseconds. It is therefore very difficult to state that these results obtained in laboratory settings have clinical relevance. Third, developmental P+CSO has high comorbidity with other psychiatric disorders, particularly personality disorders (64, 114–117). This complicates the attribution of neuropsychological impairments to paedophilia alone. Fourth, it remains unclear whether inhibitory deficits observed in formal evaluations are stimulus-specific (e.g., triggered by child-related stimuli) or generalize to neutral contexts. Notably, individuals with developmental CSO have not been described as disinhibited in their daily lives.
4.3.2 Acquired CSO
Different is the modus operandi of individuals with acquired CSO, which has been described as impulsive and disorganized (62). These individuals do not plan sexual offenses; rather, they act on an urge, and they do not try to mask their behaviour, which may occur in public places and in front of witnesses (23, 26). This modus operandi suggests that their inhibitory abilities are severely impaired, as they are unable to refrain from offending even in highly inappropriate or risky situations. Additionally, the lack of effort to conceal their actions suggests an impairment in understanding the moral and legal wrongfulness of their behaviour. This aligns with our findings, which revealed impaired inhibitory abilities in all (100%) individuals with acquired CSO and deficits in social cognition in 62.5% of cases. It is also worth noting that 61.5% of patients also manifested a general deficit in executive functions. These deficits in acquired CSO are not confined to formal neuropsychological evaluations but are also evident in daily life, as reported by relatives and caregivers. This provides robust evidence of their clinical relevance and highlights the profound impact of these impairments on behaviour.
Importantly, the identification of a brain lesion in these individuals should not be interpreted as sufficient, in itself, to explain or excuse sexually offending behaviour. In accordance with recommendations of the international consensus conference on acquired paedophilia (118) and established guidelines on the forensic use of neuroimaging (119), the presence of a neurological abnormality must be interpreted within the broader context of the individual’s cognitive and behavioural profile. Criminal responsibility and clinical risk assessments should be based primarily on demonstrable impairments in mental functioning - such as deficits in inhibition and/or moral reasoning - and on a clear causal relationship between these impairments and the offence. In this sense, neuroimaging findings serve as supportive evidence, but do not replace the need for thorough neuropsychological evaluation.
4.4 Summary of the two profiles
Developmental CSO often occurs in individuals with paedophilia or in those without any formal diagnosis. Brain alterations in developmental CSO, while present, are not macroscopically visible. These changes can only be detected through advanced brain imaging analyses (e.g., 15, 45, 120, 121) and are spatially heterogenous, as findings from different studies do not show convergence on specific brain regions and/or networks (23). From a cognitive perspective, our study identified deficits in inhibition, memory, and verbal fluency among individuals with developmental CSO. However, these cognitive impairments do not align with specific brain alterations, nor is there evidence that they significantly impact daily functioning or the modus operandi, which cannot be described as impulsive (63–65). Further research is needed to clarify the extent to which these cognitive deficits influence real-world behaviour.
In contrast, acquired CSO arises as a symptom of a neurological condition (13, 62, 91, 92). Neuroimaging consistently reveals visible lesions, which, despite being spatially heterogeneous, are linked to a disrupted network involving the orbitofrontal cortex and posterior midline structures, such as the posterior cingulate cortex and praecuneus (23). The functional characterization of these regions suggests that the orbitofrontal cortex supports impulse control, while the posterior midline structures are crucial for social cognition. Our findings revealed that impulse control deficits were present in all (100%) patients with acquired CSO, while deficits in social cognition were evident in 62.5%. This reflects a robust anatomo-clinical correspondence between brain alterations and cognitive impairments (122). Unlike developmental CSO, these impairments are apparent in daily life and significantly influence the modus operandi, which is characterized by impulsive, disorganized behaviour and a lack of awareness of the moral, social, and legal implications of offending (62). Acquired CSO is also associated with broader cognitive deficits, including impairments in attention, memory, verbal fluency, and executive functioning, as well as the presence of neurological symptoms that serve as “red flags” for the underlying organic condition (118).
4.5 Limitations and future directions
This study is not free from drawbacks. The primary limitation lies in the different methods applied to draw conclusions regarding the two forms of CSO. Studies on developmental CSO typically report group-level data, offering limited detail about individual cases. Conversely, research on acquired CSO consists exclusively of detailed single-case descriptions due to the rarity of the condition. Consequently, applying the same analytical approach to both groups was not feasible. A second limitation is related to the variability in how neuropsychological performance, neural bases, and modus operandi were studied. For developmental CSO, these aspects were studied across multiple individuals; therefore, we do not know the exact dynamic of the offense nor the neural dysfunction of the patients from the studies included in the current meta-analysis. In contrast, for acquired CSO, all relevant data (cognitive impairments, neural bases, and behavioural patterns) were derived from the same individuals, allowing for a more integrated analysis.
The present study also offers several important directions for future research. First, our findings highlight the need for studies that directly compare developmental and acquired CSO using comprehensive neuropsychological batteries, enabling more precise mapping of cognitive profiles across subtypes. Moreover, future research should investigate whether, and to what extent, specific cognitive deficits predict behavioural patterns, response to treatment, or risk of recidivism. Longitudinal studies would also be valuable to determine whether these neuropsychological impairments remain stable over time or are modifiable through intervention, and to identify which types of treatment are most effective for each subgroup.
Given the differences in aetiology between developmental and acquired CSO, we should expect differential responses to treatment. For instance, individuals with acquired paedophilia may benefit from interventions targeting the underlying neurological condition – such as tumour resection, management of neurodegenerative disease, or targeted rehabilitation for traumatic brain injury – which might lead to a significant reduction or even resolution of paedophilic behaviour. However, when medical treatment alone is insufficient to fully mitigate risk, particularly in the presence of persistent deficits in impulse control or social cognition, optimal management should involve a multidisciplinary approach. This may include ongoing medical care, neuropsychological rehabilitation, behavioural strategies, and structured supervision. Risk assessment protocols for this population should be tailored to account for neurological and cognitive contributors to risk, including potential relapse or progression of the underlying condition, disinhibition, diminished moral reasoning, and impaired insight. Such an approach is essential to ensuring both public safety and ethically grounded, individualised therapeutic intervention.
The management of developmental CSO, by contrast, presents substantial challenges. Unlike acquired forms, where treating the neurological condition can sometimes eliminate paedophilic behaviour, no consistently effective large-scale intervention currently exists for this condition (123). Low compliance with available therapeutic programmes further complicates prevention and risk management efforts (6). As a result, individuals with developmental CSO may present a higher risk of recidivism compared to those with acquired, where targeted medical intervention can directly address the underlying cause of the behaviour (124). Given that sexual interest in children tends to remain stable over time in developmental cases, long-term structured intervention and monitoring are essential to mitigate risk (125). These challenges underscore the pressing need for research focused on developing and validating more effective, ethically sound, and scalable interventions for developmental CSO, as well as refining risk assessment tools to better support clinical and forensic decision-making in this population.
4.6 Conclusions
This study provides support for the hypothesis that developmental and acquired CSO are associated with a distinct cognitive profile. Both groups exhibit deficits in inhibitory control, but social cognition impairments are present only in acquired CSO. Within developmental CSO, CSO and P+CSO individuals share similar cognitive profiles, suggesting that the CSO group likely includes individuals with undiagnosed paedophilia.
The results highlighted in the current paper have important implications regarding the appropriate classification of the CSO type and the respective potential therapeutic interventions. Regarding the classification, this study shows that impairments in social cognition might suggest the presence of an acquired origin of CSO. In respect of the possible interventions, we can speculate that individuals with acquired CSO may benefit from forms of cognitive rehabilitation focused on social cognition, whereas those with developmental CSO might require interventions targeting inhibitory control, potentially combined with pharmacological treatments.
Given the different prognoses of developmental and acquired CSO and the consequences of misidentification, accurately identifying the type of CSO is of critical relevance. A recent international consensus conference (118) suggested that a case-by-case analysis should always be warranted. Particularly, when impulsivity is noted in the modus operandi, a comprehensive neuropsychological evaluation – including, when appropriate, neuroimaging – should be conducted (21, 30, 126). Such investigation should include neuroimaging and an in-depth formal neuropsychological evaluation, mainly targeted on impulse inhibition and social cognition abilities. This study’s findings further support the consensus conference’s conclusions (118), emphasising that while developmental and acquired CSO share inhibitory deficits (evident in formal cognitive evaluations), they differ significantly in social cognitive abilities. This distinction highlights the need for caution when using acquired CSO as a model to explore the neurobiological basis of developmental CSO.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author contributions
CC: Conceptualization, Writing – original draft, Data curation, Formal Analysis, Methodology. LR: Data curation, Formal Analysis, Writing – review & editing. SF: Writing – review & editing, Conceptualization, Supervision. AS: Conceptualization, Writing – original draft. CS: Conceptualization, Project administration, Supervision, Writing – original draft.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1568244/full#supplementary-material
Footnotes
- ^ We selected individuals for the experimental group based on their fulfilment of the diagnostic criteria for paedophilia rather than paedophilic disorder. This decision was made to ensure that we did not exclude individuals who may not experience distress regarding their sexual impulses towards children. It is important to note that discomfort associated with such impulses is frequently under-reported in clinical settings (16), which can lead to an incomplete understanding of this population’s needs and experiences.
- ^ We deem it important to emphasise the existence also of a form of iatrogenic paedophilic disorder, which can arise as a consequence of pharmacological or medical treatment related to either genetic or organic pathologies (17). A well-documented example in the literature involves the emergence of paedophilic behaviours following the administration of dopaminergic medications used to treat Parkinson’s disease (18, 19). Additionally, instances of iatrogenic paedophilic disorder have been reported following deep brain stimulation targeting the subthalamic nucleus (STN) and adjacent regions, procedures typically employed to address various neurological conditions (20).
References
1. Pereda N, Guilera G, and Forns M. The prevalence of child sexual abuse in community and student samples: A meta–analysis. Clin Psychol Rev. (2009) 29:328–38. doi: 10.1016/j.cpr.2009.02.007
2. Maniglio R. The impact of child sexual abuse on health: A systematic review of reviews. Clinical Psychology Review. (2009) 29(7):647–57.
3. American Psychiatric Association and DSM-5 Task Force. Diagnostic and statistical manual of mental disorders: DSM-5. 5th ed. American Psychiatric Association, Inc. (2013). doi: 10.1176/appi.books.9780890425596
4. Beech AR, Miner MH, and Thornton D. Paraphilias in the DSM-5. Annu Rev Clin Psychol. (2016) 12:383–406. doi: 10.1146/annurev-clinpsy-021815-093330
5. Regier DA, Narrow WE, Clarke DE, Kraemer HC, Kuramoto SJ, Kuhl EA, et al. DSM-5 field trials in the United States and Canada, Part II: test-retest reliability of selected categorical diagnoses. Am J Psychiatry. (2013) 170:59–70. doi: 10.1176/appi.ajp.2012.12070999
6. Beier KM, Neutze J, Mundt IA, Ahlers CJ, Goecker D, Konrad A, et al. Encouraging self-identified pedophiles and hebephiles to seek professional help: First results of the Prevention Project Dunkelfeld (PPD). Child Abuse Negl. (2009) 33:545–9. doi: 10.1016/j.chiabu.2009.04.002
7. Cantor JM, Kabani N, Christensen BK, Zipursky RB, Barbaree HE, Dickey R, et al. Cerebral white matter deficiencies in pedophilic men. J Psychiatr Res. (2008) 42:167–83. doi: 10.1016/j.jpsychires.2007.10.013
8. Gannon TA. A compositional explanatory theory of pedophilia. Aggression Violent Behav. (2021) 61:101662. doi: 10.1016/j.avb.2021.101662
9. Jahnke S. The stigma of pedophilia. Eur Psychol. (2018b) 23(2):144–53. doi: 10.1027/1016-9040/a000325
10. Schaefer GA, Mundt IA, Feelgood S, Hupp E, Neutze J, Ahlers CJ, et al. Potential and Dunkelfeld offenders: Two neglected target groups for prevention of child sexual abuse. Int J Law Psychiatry. (2010) 33:154–63. doi: 10.1016/j.ijlp.2010.03.005
11. Beier KM, Ahlers CJ, Goecker D, Neutze J, Mundt IA, Hupp E, et al. Can pedophiles be reached for primary prevention of child sexual abuse? First results of the Berlin Prevention Project Dunkelfeld (PPD). J Forensic Psychiatry Psychol. (2009) 20:851–67. doi: 10.1080/14789940903174188
12. Wakefield JC. The DSM-5’s proposed new categories of sexual disorder: The problem of false positives in sexual diagnosis. Clin Soc Work J. (2012) 40:213–23. doi: 10.1007/s10615-011-0353-2
13. Burns JM and Swerdlow RH. Right orbitofrontal tumor with pedophilia symptom and constructional apraxia sign. Arch Neurol. (2003) 60:437. doi: 10.1001/archneur.60.3.437
14. Lopes PMG, Prado CSDC, and De Oliveira-Souza R. The neurology of acquired pedophilia. Neurocase. (2020) 26:103–14. doi: 10.1080/13554794.2020.1727929
15. Mohnke S, Müller S, Amelung T, Krüger THC, Ponseti J, Schiffer B, et al. Brain alterations in paedophilia: A critical review. Prog Neurobiol. (2014) 122:1–23. doi: 10.1016/j.pneurobio.2014.07.005
16. Houtepen JABM, Sijtsema JJ, and Bogaerts S. Being sexually attracted to minors: sexual development, coping with forbidden feelings, and relieving sexual arousal in self-identified pedophiles. J Sex Marital Ther. (2016) 42:48–69. doi: 10.1080/0092623X.2015.1061077
17. Loconte R, Sesso G, Scarpazza C, and Pietrini P. A unique case of iatrogenic hebephiliac behavior emerging late in life in a patient with Gordon Holmes Syndrome. Psychiatry Res Case Rep. (2024) 3:100237. doi: 10.1016/j.psycr.2024.100237
18. Solla P, Floris G, Tacconi P, and Cannas A. Paraphilic behaviours in a parkinsonian patient with hedonistic homeostatic dysregulation. Int J Neuropsychopharmacol. (2006) 9:767. doi: 10.1017/S1461145705006437
19. Mendez M and Shapira JS. Pedophilic behavior from brain disease. J Sexual Med. (2011) 8:1092–100. doi: 10.1111/j.1743-6109.2010.02172.x
20. Müller S, Walter H, and Christen M. When benefitting a patient increases the risk for harm for third persons—The case of treating pedophilic Parkinsonian patients with deep brain stimulation. Int J Law Psychiatry. (2014) 37:295–303. doi: 10.1016/j.ijlp.2013.11.015
21. Gilbert F and Focquaert F. Rethinking responsibility in offenders with acquired paedophilia: Punishment or treatment? Int J Law Psychiatry. (2015) 38:51–60. doi: 10.1016/j.ijlp.2015.01.007
22. Scarpazza C, Sigfrido Camperio Ciani A, and Ferracuti S. Idiopathic vs acquired pedophilic behavior: A critical analysis. Ital J Of Criminology. (2020) 14:212–9. doi: 10.7347/RIC-032020-p212
23. Scarpazza C, Pennati A, and Sartori G. Mental insanity assessment of pedophilia: the importance of the trans-disciplinary approach. Reflections on two cases. Front Neurosci. (2018) 12:335. doi: 10.3389/fnins.2018.00335
24. Miller BL, Cummings JL, McIntyre H, Ebers G, and Grode M. Hypersexuality or altered sexual preference following brain injury. J Neurology Neurosurgery Psychiatry. (1986) 49:867–73. doi: 10.1136/jnnp.49.8.867
25. Prado CSDC, Lopes PMG, Moll J, DeSalles A, and De Oliveira-Souza R. A case of developmental pedophilia unmasked by frontotemporal dementia. Neurocase. (2021) 27:129–37. doi: 10.1080/13554794.2021.1886310
26. Sartori G, Scarpazza C, Codognotto S, and Pietrini P. An unusual case of acquired pedophilic behavior following compression of orbitofrontal cortex and hypothalamus by a Clivus Chordoma. J Neurol. (2016) 263:1454–5. doi: 10.1007/s00415-016-8143-y
27. Joyal CC. The neuroanatomical bases of pedophilia and the importance of distinguishing genuine vs. Acquired types: A systematic review. Sexual Offending: Theory Research Prev. (2023) 18:1–21. doi: 10.5964/sotrap.6989
28. Devinsky J, Sacks O, and Devinsky O. Klüver–Bucy syndrome, hypersexuality, and the law. Neurocase. (2010) 16:140–5. doi: 10.1080/13554790903329182
29. Gilbert F, Vranic A, and Viaña JNM. Acquired pedophilia and moral responsibility. AJOB Neurosci. (2016) 7:209–11. doi: 10.1080/21507740.2016.1244221
30. Scarpazza C, Zampieri I, Miolla A, Melis G, Pietrini P, and Sartori G. A multidisciplinary approach to insanity assessment as a way to reduce cognitive biases. Forensic Sci Int. (2021) 319:110652. doi: 10.1016/j.forsciint.2020.110652
31. Quinsey VL. The etiology of anomalous sexual preferences in men. Ann New York Acad Sci. (2003) 989:105–17. doi: 10.1111/j.1749-6632.2003.tb07297.x
32. Alanko K, Salo B, Mokros A, and Santtila P. Evidence for heritability of adult men’s sexual interest in youth under age 16 from a population-based extended twin design. J Sexual Med. (2013) 10:1090–9. doi: 10.1111/jsm.12067
33. García JAB. Etiology of pedophilia from a neurodevelopmental perspective: Markers and brain alterations. Rev Psiquiatría y Salud Ment (English Edition). (2009) 2:190–6. doi: 10.1016/S2173-5050(09)70051-2
34. Seto MC. Pedophilia and sexual offending against children: theory. Assessment Intervention. American Psychological Association. (2008), 10–290. doi: 10.1037/0000107-000
35. Stedal K, Scherer R, Touyz S, Hay P, and Broomfield C. Research Review: Neuropsychological functioning in young anorexia nervosa: A meta-analysis. J Child Psychol Psychiatry. (2022) 63:616–25. doi: 10.1111/jcpp.13562
36. Tenbergen G, Wittfoth M, Frieling H, Ponseti J, Walter M, Walter H, et al. The neurobiology and psychology of pedophilia: recent advances and challenges. Front Hum Neurosci. (2015) 9:344. doi: 10.3389/fnhum.2015.00344
37. Frohman EM, Frohman TC, and Moreault AM. Acquired sexual paraphilia in patients with multiple sclerosis. Arch Neurol. (2002) 59:1006. doi: 10.1001/archneur.59.6.1006
38. Fumagalli M, Pravettoni G, and Priori A. Pedophilia 30 years after a traumatic brain injury. Neurological Sci. (2015) 36:481–2. doi: 10.1007/s10072-014-1915-1
39. Langton CM, Barbaree HE, Harkins L, and Peacock EJ. Sex offenders’ Response to treatment and its association with recidivism as a function of psychopathy. Sexual Abuse. (2006) 18:99–120. doi: 10.1177/107906320601800107
40. Thibaut F, Barra FDL, Gordon H, Cosyns P, Bradford JMW, and the WFSBP Task Force on Sexual Disorders. The World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for the biological treatment of paraphilias. World J Biol Psychiatry. (2010) 11:604–55. doi: 10.3109/15622971003671628
41. Kärgel C, Massau C, Weiß S, Walter M, Borchardt V, Krueger THC, et al. Evidence for superior neurobiological and behavioral inhibitory control abilities in non-offending as compared to offending pedophiles: Response Inhibition in Pedophilia. Hum Brain Mapp. (2017) 38:1092–104. doi: 10.1002/hbm.23443
42. Massau C, Tenbergen G, Kärgel C, Weiß S, Gerwinn H, Pohl A, et al. Executive functioning in pedophilia and child sexual offending. J Int Neuropsychol Soc. (2017) 23:460–70. doi: 10.1017/S1355617717000315
43. Picard EH, Bopp LL, and Rosenfeld B. Neuropsychological functioning in sexual offenders with and without pedophilic disorder. Arch Sexual Behav. (2024) 53:43–56. doi: 10.1007/s10508-023-02689-1
44. Suchy Y, Whittaker JW, Strassberg DS, and Eastvold A. Neurocognitive differences between pedophilic and nonpedophilic child molesters. J Int Neuropsychol Soc. (2009) 15:248–57. doi: 10.1017/S1355617709090353
45. Schiffer B, Amelung T, Pohl A, Kaergel C, Tenbergen G, Gerwinn H, et al. Gray matter anomalies in pedophiles with and without a history of child sexual offending. Trans Psychiatry. (2017) 7:e1129–9. doi: 10.1038/tp.2017.96
46. Poeppl TB, Nitschke J, Santtila P, Schecklmann M, Langguth B, Greenlee MW, et al. Association between brain structure and phenotypic characteristics in pedophilia. J Psychiatr Res. (2013) 47:678–85. doi: 10.1016/j.jpsychires.2013.01.003
47. Schiffer B, Peschel T, Paul T, Gizewski E, Forsting M, Leygraf N, et al. Structural brain abnormalities in the frontostriatal system and cerebellum in pedophilia. J Psychiatr Res. (2007) 41:753–62. doi: 10.1016/j.jpsychires.2006.06.003
48. Schiltz K, Witzel J, Northoff G, Zierhut K, Gubka U, Fellmann H, et al. Brain pathology in pedophilic offenders: evidence of volume reduction in the right amygdala and related diencephalic structures. Arch Gen Psychiatry. (2007) 64:737. doi: 10.1001/archpsyc.64.6.737
49. Cazala F, Fonteille V, Moulier V, Pélégrini-Issac M, De Beaurepaire C, Abondo M, et al. Brain responses to pictures of children in men with pedophilic disorder: A functional magnetic resonance imaging study. Eur Arch Psychiatry Clin Neurosci. (2019) 269:713–29. doi: 10.1007/s00406-018-0933-z
50. Fonteille V, Redouté J, Lamothe P, Straub D, Lavenne F, Le Bars D, et al. Brain processing of pictures of children in men with pedophilic disorder: A positron emission tomography study. NeuroImage: Clin. (2019) 21:101647. doi: 10.1016/j.nicl.2018.101647
51. Mannfolk C, Liberg B, Abé C, and Rahm C. Altered neural and behavioral response to sexually implicit stimuli during a pictorial-modified stroop task in pedophilic disorder. Biol Psychiatry Global Open Sci. (2023) 3:292–300. doi: 10.1016/j.bpsgos.2022.02.004
52. Poeppl TB, Eickhoff SB, Fox PT, Laird AR, Rupprecht R, Langguth B, et al. Connectivity and functional profiling of abnormal brain structures in pedophilia: Functional Profile of Brain Structure in Pedophilia. Hum Brain Mapp. (2015) 36:2374–86. doi: 10.1002/hbm.22777
53. Polisois-Keating A and Joyal CC. Functional neuroimaging of sexual arousal: A preliminary meta-analysis comparing pedophilic to non-pedophilic men. Arch Sexual Behav. (2013) 42:1111–3. doi: 10.1007/s10508-013-0198-6
54. Schiffer B, Paul T, Gizewski E, Forsting M, Leygraf N, Schedlowski M, et al. Functional brain correlates of heterosexual paedophilia. NeuroImage. (2008) 41:80–91. doi: 10.1016/j.neuroimage.2008.02.008
55. Walter M, Witzel J, Wiebking C, Gubka U, Rotte M, Schiltz K, et al. Pedophilia is linked to reduced activation in hypothalamus and lateral prefrontal cortex during visual erotic stimulation. Biol Psychiatry. (2007) 62:698–701. doi: 10.1016/j.biopsych.2006.10.018
56. Poeppl TB, Langguth B, Laird AR, and Eickhoff SB. The functional neuroanatomy of male psychosexual and physiosexual arousal: A quantitative meta-analysis: Functional Neuroanatomy of Male Sexual Arousal. Hum Brain Mapp. (2014) 35:1404–21. doi: 10.1002/hbm.22262
57. Alnemari AM, Mansour TR, Buehler M, and Gaudin D. Neural basis of pedophilia: Altered sexual preference following traumatic brain injury. Int J Surg Case Rep. (2016) 25:221–4. doi: 10.1016/j.ijscr.2016.06.035
58. Mendez MF. The unique predisposition to criminal violations in frontotemporal dementia. J Am Acad Psychiatry Law. (2010) 38:318.
59. Scarpazza C, Finos L, Genon S, Masiero L, Bortolato E, Cavaliere C, et al. Idiopathic and acquired pedophilia as two distinct disorders: An insight from neuroimaging. Brain Imaging Behav. (2021) 15:2681–92. doi: 10.1007/s11682-020-00442-z
60. Genon S, Reid A, Langner R, Amunts K, and Eickhoff SB. How to characterize the function of a brain region. Trends Cogn Sci. (2018) 22:350–64. doi: 10.1016/j.tics.2018.01.010
61. Plachti A, Eickhoff SB, Hoffstaedter F, Patil KR, Laird AR, Fox PT, et al. Multimodal parcellations and extensive behavioral profiling tackling the hippocampus gradient. Cereb Cortex. (2019) 29:4595–612. doi: 10.1093/cercor/bhy336
62. Camperio Ciani AS, Scarpazza C, Covelli V, and Battaglia U. Profiling acquired pedophilic behavior: Retrospective analysis of 66 Italian forensic cases of pedophilia. Int J Law Psychiatry. (2019) 67:101508. doi: 10.1016/j.ijlp.2019.101508
63. Cohen LJ, Gans SW, McGeoch PG, Poznansky O, Itskovich Y, Murphy S, et al. Impulsive personality traits in male pedophiles versus healthy controls: Is pedophilia an impulsive-aggressive disorder? Compr Psychiatry. (2002) 43:127–34. doi: 10.1053/comp.2002.30796
65. Miranda AO and Corcoran CL. Comparison of perpetration characteristics between male juvenile and adult sexual offenders: preliminary results. Sexual Abuse. (2000) 12:179–88. doi: 10.1177/107906320001200302
66. Berlin FS and Krout E. Pedophilia: Diagnostic concepts, treatment, and ethical considerations. Am J Forensic Psychiatry. (1986) 7:13–30.
67. Gebhard PH and Institute for Sex Research (Bloomington, Ind.). Sex offenders : an analysis of types / by P.H. Gebhard ... [et al.] of the Institute for Sex Research. London: Heinemann. (1965).
68. Dillien T, Goethals K, Sabbe B, and Brazil IA. The neuropsychology of child sexual offending: A systematic review. Aggression Violent Behav. (2020) 54:101406. doi: 10.1016/j.avb.2020.101406
69. Joyal CC, Beaulieu-Plante J, and De Chantérac A. The neuropsychology of sex offenders: A meta-analysis. Sexual Abuse. (2014) 26:149–77. doi: 10.1177/1079063213482842
70. Cohen LJ, Nesci C, Steinfeld M, Haeri S, and Galynker I. Investigating the relationship between sexual and chemical addictions by comparing executive function in subjects with pedophilia or opiate addiction and healthy controls. J Psychiatr Pract. (2010) 16:405–12. doi: 10.1097/01.pra.0000390759.04581.7c
71. Joyal CC, Tardif M, and Spearson-Goulet J-A. Executive functions and social cognition in juveniles who have sexually offended. Sexual Abuse. (2020) 32:179–202. doi: 10.1177/1079063218807487
72. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int J Surg. (2021) 88:105906. doi: 10.1016/j.ijsu.2021.105906
73. Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Software. (2010) 36:1–48. doi: 10.18637/jss.v036.i03
74. Pustejovsky JE and Tipton E. Meta-analysis with robust variance estimation: expanding the range of working models. Prev Sci. (2022) 23:425–38. doi: 10.1007/s11121-021-01246-3
75. Friedman NP and Miyake A. Unity and diversity of executive functions: Individual differences as a window on cognitive structure. Cortex. (2017) 86:186–204. doi: 10.1016/j.cortex.2016.04.023
76. Jewsbury PA, Bowden SC, and Strauss ME. Integrating the switching, inhibition, and updating model of executive function with the Cattell—Horn—Carroll model. J Exp Psychology: Gen. (2016) 145:220–45. doi: 10.1037/xge0000119
77. Tipton E and Pustejovsky JE. Small-sample adjustments for tests of moderators and model fit using robust variance estimation in meta-regression. J Educ Behav Stat. (2015) 40:604–34. doi: 10.3102/1076998615606099
78. Zhang J-T. An approximate hotelling T2-test for heteroscedastic one-way MANOVA. Open J Stat. (2012) 2:1. doi: 10.4236/ojs.2012.21001
79. Zhang J-T. Tests of linear hypotheses in the ANOVA under heteroscedasticity. Int J Advanced Stat Probability. (2013) 1:9–24. doi: 10.14419/ijasp.v1i2.908
80. Viechtbauer W and Cheung MW-L. Outlier and influence diagnostics for meta-analysis. Res Synthesis Methods. (2010) 1:112–25. doi: 10.1002/jrsm.11
81. Viechtbauer W. Bias and efficiency of meta-analytic variance estimators in the random-effects model. J Educ Behav Stat. (2005) 30:261–93. doi: 10.3102/10769986030003261
82. Cochran WG. The combination of estimates from different experiments. Biometrics. (1954) 10:101–29. doi: 10.2307/3001666
83. Begg CB and Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. (1994), 1088–101. doi: 10.2307/2533446
84. Sterne JA and Egger M. Regression methods to detect publication and other bias in meta-analysis. Publ Bias Meta-analysis: Prevention Assess Adjustments. (2005), 99–110. doi: 10.1002/0470870168.ch6
85. Cook RD and Weisberg S. Residuals and Influence in Regression. Retrieved from the University Digital Conservancy. (1982). Available at: https://hdl.handle.net/11299/37076.
86. Herrero Ó, Escorial S, and Colom R. Rapists and Child Abusers Share Low Levels in Executive Updating, but Do not in Fluid Reasoning. Eur J Psychol Appl to Legal Context. (2018) 11:1–7. doi: 10.5093/ejpalc2018a10
87. Becerra-García JA and Egan V. Neurocognitive functioning and subtypes of child molesters: poorer working memory differentiates incestuous from non-incestuous offenders. Psychiatry Psychol Law. (2014) 21:585–90. doi: 10.1080/13218719.2013.873974
88. Prahlada Rao N, Chand PK, and Murthy P. A case of late-onset pedophilia to sertraline. Primary Care Companion to J Clin Psychiatry. (2007) 09:235–6. doi: 10.4088/PCC.v09n0311e
89. Regestein QR and Reich P. PEDOPHILIA OCCURRING AFTER ONSET OF COGNITIVE IMPAIRMENT. J Nervous Ment Dis. (1978) 166:794–8. doi: 10.1097/00005053-197811000-00007
90. Lesniak R, Szymusik A, and Chrzanowski R. Multidirectional disorders of sexual drive in a case of brain tumour. Forensic Sci. (1972) 1:333–8. doi: 10.1016/0300-9432(72)90031-3
91. Ortego N, Miller BL, Itabashi H, and Cummings JL. Altered sexual behavior with multiple sclerosis: A case report. Cogn Behav Neurol. (1993) 6:260–4.
92. Dimitrov M, Phipps M, Zahn TP, and Grafman J. A thoroughly modern Gage. Neurocase. (1999) 5:345–54. doi: 10.1080/13554799908411987
93. Rainero I, Rubino E, Negro E, Gallone S, Galimberti D, Gentile S, et al. Heterosexual pedophilia in a frontotemporal dementia patient with a mutation in the progranulin gene. Biol Psychiatry. (2011) 70:e43–4. doi: 10.1016/j.biopsych.2011.06.015
94. Gilbert F and Vranič A. Paedophilia, invasive brain surgery, and punishment. J Bioethical Inq. (2015) 12:521–6. doi: 10.1007/s11673-015-9647-3
95. Cohen J. Statistical power analysis for the behavioral sciences (0 ed.). Cambridge: Academic Press (2013). doi: 10.4324/9780203771587
96. Schäfer T and Schwarz MA. The meaningfulness of effect sizes in psychological research: differences between sub-disciplines and the impact of potential biases. Front Psychol. (2019) 10:813. doi: 10.3389/fpsyg.2019.00813
97. DiGirolamo GJ, Kramer AF, Barad V, Cepeda NJ, Weissman DH, Milham MP, et al. General and task-specific frontal lobe recruitment in older adults during executive processes: A fMRI investigation of task-switching. Neuroreport. (2001) 12:2065–71. doi: 10.1097/00001756-200107030-00054
98. Ravnkilde B, Videbech P, Rosenberg R, Gjedde A, and Gade A. Putative tests of frontal lobe function: A PET-study of brain activation during stroop’s test and verbal fluency. J Clin Exp Neuropsychol. (2002) 24:534–47. doi: 10.1076/jcen.24.4.534.1033
99. Bartels RM, Beech AR, Harkins L, and Thornton D. Assessing sexual interest in children using the go/no-go association test. Sexual Abuse: A J Res Treat. (2017) 30(5):593–614. 107906321668611. doi: 10.1177/1079063216686119
100. Turner D, Laier C, Brand M, Bockshammer T, Welsch R, and Rettenberger M. Response inhibition and impulsive decision-making in sexual offenders against children. J Abnormal Psychol. (2018) 127:471–81. doi: 10.1037/abn0000359
101. Veneziano C, Veneziano L, LeGrand S, and Richards L. Neuropsychological executive functions of adolescent sex offenders and nonsex offenders. Perceptual Motor Skills. (2004) 98:661–74. doi: 10.2466/pms.98.2.661-674
102. Turner D and Rettenberger M. Neuropsychological functioning in child sexual abusers: A systematic review. Aggression Violent Behav. (2020) 54:101405. doi: 10.1016/j.avb.2020.101405
103. Seto MC. The motivation-facilitation model of sexual offending. Sexual Abuse. (2019) 31:3–24. doi: 10.1177/1079063217720919
104. Eastvold A, Suchy Y, and Strassberg D. Executive function profiles of pedophilic and nonpedophilic child molesters. J Int Neuropsychol Soc. (2011) 17:295–307. doi: 10.1017/S1355617710001669
105. Weidacker K, Kärgel C, Massau C, Krueger THC, Walter M, Ponseti J, et al. Interference inhibition in offending and non-offending pedophiles: A preliminary event-related fMRI study. Neuropsychologia. (2022) 173:108301. doi: 10.1016/j.neuropsychologia.2022.108301
106. Schiffer B and Vonlaufen C. Executive dysfunctions in pedophilic and nonpedophilic child molesters. J Sexual Med. (2011) 8:1975–84. doi: 10.1111/j.1743-6109.2010.02140.x
107. Mann RE, Hanson RK, and Thornton D. Assessing risk for sexual recidivism: some proposals on the nature of psychologically meaningful risk factors. Sexual Abuse. (2010) 22:191–217. doi: 10.1177/1079063210366039
108. Martin S, Zabala C, Del-Monte J, Graziani P, Aizpurua E, Barry TJ, et al. Examining the relationships between impulsivity, aggression, and recidivism for prisoners with antisocial personality disorder. Aggression Violent Behav. (2019) 49:101314. doi: 10.1016/j.avb.2019.07.009
109. Ogilvie JM, Stewart AL, Chan RC, and Shum DH. Neuropsychological measures of executive function and antisocial behavior: A meta-analysis. Criminology. (2011) 49:1063–107. doi: 10.1111/j.1745-9125.2011.00252.x
110. Swann AC, Lijffijt M, Lane SD, Steinberg JL, and Moeller FG. Trait impulsivity and response inhibition in antisocial personality disorder. J Psychiatr Res. (2009) 43:1057–63. doi: 10.1016/j.jpsychires.2009.03.003
111. Stoléru S, Fonteille V, Cornélis C, Joyal C, and Moulier V. Functional neuroimaging studies of sexual arousal and orgasm in healthy men and women: A review and meta-analysis. Neurosci Biobehavioral Rev. (2012) 36:1481–509. doi: 10.1016/j.neubiorev.2012.03.006
112. Dimock S. Actio libera in causa. Criminal Law Philosophy. (2013) 7:549–69. doi: 10.1007/s11572-013-9245-6
113. Cohen LJ, Nikiforov K, Gans S, Poznansky O, McGeoch P, Weaver C, et al. Heterosexual male perpetrators of childhood sexual abuse: A preliminary neuropsychiatric model. Psychiatr Q. (2002) 73:313–36. doi: 10.1023/A:1020416101092
114. Cohen LJ and Galynker II. Clinical features of pedophilia and implications for treatment. J Psychiatr Practice®. (2002) 8:276–89. doi: 10.1097/00131746-200209000-00004
115. Geer JH, Estupinan LA, and Manguno-Mire GM. Empathy, social skills, and other relevant cognitive processes in rapists and child molesters. Aggression Violent Behav. (2000) 5:99–126. doi: 10.1016/S1359-1789(98)00011-1
116. Kruger THC and Schiffer B. Neurocognitive and personality factors in homo- and heterosexual pedophiles and controls. J Sexual Med. (2011) 8:1650–9. doi: 10.1111/j.1743-6109.2009.01564.x
117. Raymond NC, Coleman E, Ohlerking F, Christenson GA, and Miner M. Psychiatric comorbidity in pedophilic sex offenders. Am J Psychiatry. (1999) 156:786–8. doi: 10.1176/ajp.156.5.786
118. Scarpazza C, Costa C, Battaglia U, Berryessa C, Bianchetti ML, Caggiu I, et al. Acquired Pedophilia: International Delphi-method-based consensus guidelines. Trans Psychiatry. (2023) 13:11. doi: 10.1038/s41398-023-02314-8
119. Scarpazza C, Ferracuti S, Miolla A, and Sartori G. The charm of structural neuroimaging in insanity evaluations: Guidelines to avoid misinterpretation of the findings. Trans Psychiatry. (2018) 8:227. doi: 10.1038/s41398-018-0274-8
120. Cantor JM, Lafaille S, Soh DW, Moayedi M, Mikulis DJ, and Girard TA. Diffusion tensor imaging of pedophilia. Arch Sexual Behav. (2015) 44:2161–72. doi: 10.1007/s10508-015-0629-7
121. Poeppl TB, Eickhoff SB, Fox PT, Laird AR, Rupprecht R, Langguth B, et al. Connectivity and functional profiling of abnormal brain structures in pedophilia. Hum Brain Mapp. (2015) 36:2374–86. doi: 10.1002/hbm.22777
122. Scarpazza C, Pellegrini S, Pietrini P, and Sartori G. The role of neuroscience in the evaluation of mental insanity: On the controversies in Italy: Comment on “On the stand. Another episode of neuroscience and law discussion from Italy. Neuroethics. (2018) 11:83–95. doi: 10.1007/s12152-017-9349-0
123. Langstrom N, Enebrink P, Lauren E-M, Lindblom J, Werko S, and Hanson RK. Preventing sexual abusers of children from reoffending: Systematic review of medical and psychological interventions. BMJ. (2013) 347:f4630–0. doi: 10.1136/bmj.f4630
124. Seto MC. Is pedophilia a sexual orientation? Arch Sexual Behav. (2012) 41:231–6. doi: 10.1007/s10508-011-9882-6
125. Hanson RK, Harris AJR, Helmus L, and Thornton D. High-risk sex offenders may not be high risk forever. J Interpersonal Violence. (2014) 29:2792–813. doi: 10.1177/0886260514526062
Keywords: child sexual offending, pedophilia, pedophilic disorder, cognitive profile, impulsivity, social cognition, meta-analysis, systematic review
Citation: Costa C, Ronconi L, Ferracuti S, Schincariol A and Scarpazza C (2025) Cognitive profiles of paedophilic behaviour: a meta-analytic and systematic review of developmental vs acquired forms. Front. Psychiatry 16:1568244. doi: 10.3389/fpsyt.2025.1568244
Received: 29 January 2025; Accepted: 21 May 2025;
Published: 09 June 2025.
Edited by:
Yasin Hasan Balcioglu, Bakirkoy Prof Mazhar Osman Training and Research Hospital for Psychiatry, Neurology, and Neurosurgery, TürkiyeReviewed by:
Georgia Zara, University of Turin, ItalyHeather Moulden, McMaster University, Canada
Ulrich Rabl, Medical University of Vienna, Austria
Copyright © 2025 Costa, Ronconi, Ferracuti, Schincariol and Scarpazza. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cristina Scarpazza, Y3Jpc3RpbmEuc2NhcnBhenphQHVuaXBkLml0