 Hiba Qahttan Khaleel Al-Juhaishi1,2Osamah Abbas Jaber1,3
Hiba Qahttan Khaleel Al-Juhaishi1,2Osamah Abbas Jaber1,3 Faris Lami3,4Shatha Mohammed Jasim1,3Nahid Dehghan Nayeri3,5Mahdi Shafiee Sabet3,6†
Faris Lami3,4Shatha Mohammed Jasim1,3Nahid Dehghan Nayeri3,5Mahdi Shafiee Sabet3,6† Ghaith Al-Gburi3,7*†
Ghaith Al-Gburi3,7*†- 1Al-Subtain Academy for Autism and Neurodevelopmental Disorders, Karbala, Iraq
- 2Baghdad Teaching Hospital, Baghdad, Iraq
- 3Al-Subtain University of Medical Sciences, International Branch of Tehran University for Medical Sciences, Karbala, Iraq
- 4Department of Community Medicine, College of Medicine, University of Baghdad, Baghdad, Iraq
- 5Nursing and Midwifery Care Research Centre, School of Nursing and Midwifery, Tehran University of Medical Sciences, Tehran, Iran
- 6Department of Family Medicine, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran
- 7School of Biosciences, University of Birmingham, Birmingham, United Kingdom
Introduction: Children with autism spectrum disorder (ASD) can experience delayed diagnosis and ineffective treatment due to low caregiver knowledge. Negative attitudes have also been linked to increased emotional problems and poor adaptive outcomes. Before educational interventions can address these issues, local knowledge and attitudes must be assessed, including the identification of high-risk groups that require prioritisation.
Methods: Between February 17 and September 10, 2024, Al-Subtain Academy for Autism and Baghdad’s National Centre for Autism and Child Psychiatry conducted a cross-sectional study. Data was collected using a structured questionnaire developed based on the Autism Stigma and Knowledge Questionnaire (ASK-Q) and a review of previous studies. The questionnaire was pre-tested on 25 caregivers for clarity and reliability.
Results: 302 caregivers were included, all of whom were family members of the children. 57 caregivers (18.9%) had low knowledge of ASD, while only 24 (7.9%) had high knowledge. College-educated caregivers scored higher than those who were illiterate or with primary or secondary school education (p-values = 0.009, 0.002, and 0.007). Similarly, caregivers from low-income backgrounds had less knowledge than those from average and high-income backgrounds (p-value = 0.002 and 0.005). However, this difference was no longer apparent when controlling for the lack of tertiary education (B = 1.231, p-value = 0.119). 105 (34.8%) thought that a complete cure is possible, with higher rates among caregivers without tertiary education (43.0%, adjusted p-value = 0.048) or from low-income backgrounds (55.0%, adjusted p-value = 0.0002). In terms of attitudes, 44 (14.6%) believed that all children with ASD are aggressive, and 114 (37.7%) believed that they are deliberately negativistic and non-compliant. Being ashamed of the diagnosis was more common if the child had comorbid conditions. However, this difference was only significant before adjusting for multiple testing (adjusted p-value = 0.286).
Conclusion: Educational programmes should be implemented to enhance knowledge and address treatment expectations, especially among caregivers with low income and lower education. Efforts should be focused on reducing negative attitudes to improve overall outcomes.
Introduction
Children with autism spectrum disorder (ASD) may display a range of behaviours with different types and severities. As specified in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), these behaviours encompass difficulties in social reciprocity and both verbal and nonverbal communication, as well as repetitive and restrictive behaviours and interests (1). Although there are some epidemiological differences between genders (with males having higher rates) and slight variations across races, ASD can affect individuals of all genders and nationalities (2). A meta-analysis, utilising data up to 2019, indicated that the global prevalence of ASD ranges from 0.61% to 0.85%, surpassing the pooled prevalence of 0.35% observed in West Asian countries, including the Middle East (3, 4). Concerns have been expressed that underdiagnosis and underreporting of the condition in the region may be a contributing factor. In Iraq, no official estimate has been reported for the country as a whole. However, the northern region of Kurdistan has a reported prevalence of 0.89% (5).
Early detection of ASD is crucial, as early interventions have a positive impact on adaptive outcomes (6). While most children are diagnosed between the ages of 2 and 3, the variability in presentation has resulted in differences in the age at which most children receive a diagnosis (7). Therefore, it is essential for caregivers, usually parents, to detect the behaviours that might suggest the presence of ASD. Studies have been conducted to address awareness of autism’s core symptoms and attitudes toward children with ASD among parents in the general public. These studies aim to guide the implementation of educational campaigns that may lead to earlier recognition of ASD (8).
Following diagnosis, parents’ involvement plays an important role in treatment outcomes (9). Poor knowledge of available treatment options has been shown to delay treatment or lead to the endorsement of treatment options that have no proven efficacy (10). Caregivers are not simple bystanders; rather, they have an active role in decision-making, educational planning, and setting treatment goals. Additionally, most of the care tends to be provided at home, despite the presence of specialised healthcare centres (11, 12).
The Health Belief Model (HBM) provides a conceptual framework for how caregivers’ knowledge and attitudes might affect their behaviours regarding their child’s condition (13). According to this condition, health-related behaviour is triggered by a cue that might be either internal, such as the development of certain symptoms, or external, such as public health campaigns. The nature and extent of the cue needed to cause health-related behaviour will depend on their perceived susceptibility to the condition, their perceived severity, their perceived benefit of performing health-related behaviour, and the barriers against the behaviours.
Empirically, studies have shown that children whose parents have higher education levels and socioeconomic status have better treatment outcomes, while high parental stress is associated with worse outcomes (9). Educational programmes directed toward caregivers of children with ASD have shown a reduction in stress and increased confidence (14). Before such programmes can be developed and implemented, an evaluation of caregivers’ baseline knowledge and attitudes is necessary. This evaluation should also identify risk groups with lower knowledge to prioritise those groups during subsequent educational initiatives.
Caregivers’ attitudes can also greatly impact adaptive outcomes in children with ASD. Studies have shown that children from families with more negative attitudes tend to experience higher rates of behavioural and emotional issues, as well as reduced prosocial behaviour (15). Parenting styles that rely heavily on negative reinforcement and criticism have been associated with worse adaptive outcomes (16). Therefore, both caregivers’ knowledge and attitudes are often assessed simultaneously to address any negative attitudes during educational programmes.
In Iraq, literature surrounding ASD is scarce. According to a previous field report, specialised care centres are few and tend to be situated only around urban areas. In these low-resource settings, the role of caregivers becomes even more crucial. Few studies on caregivers’ knowledge and attitudes have been conducted in Iraq (17–19). These studies, however, often used small sample sizes, used questionnaires that did not cover aspects related to the aetiology and treatment of ASD, or in some cases reported only overall knowledge rather than individual item performance. Our study aims to assess caregivers’ knowledge of various aspects of ASD, including its aetiology, signs and symptoms, diagnosis, treatments, and outcomes in children. Additionally, we looked into negative attitudes towards mental health services, children with ASD themselves, and their educational needs.
Methods
Study design and setting
A multi-centre cross-sectional survey was conducted at Al-Sibtain Academy for Autism and Neurodevelopmental Disorders in Karbala and Baghdad’s National Centre for Autism and Child Psychiatry. These centres are responsible for providing specialised care for the majority of children with ASD in their respective provinces. They also provide care for children from surrounding provinces in the middle and southern regions of Iraq. Data was collected from caregivers attending with their children at the mentioned healthcare centres from April 1, 2024, to June 1, 2024. The entire study, including designing the study, collecting data, analysing it, and organising the final report, was conducted from February 17, 2024, to September 10, 2024.
This survey was part of a research collaboration between Al-Subtain University of Medical Sciences and the specified healthcare centres. The collaboration aimed to explore the epidemiological, clinical, and psychosocial aspects of children with ASD from Iraq through nine studies.
Eligibility criteria
Only caregivers whose children received a confirmed diagnosis of ASD by a consultant in child and adolescent psychiatry based on the DSM-5 criteria were eligible to participate in our study. A caregiver was defined as an individual over the age of 18 who lives with the child and is responsible for meeting the child’s needs at home, including assistance with feeding, dressing, and using the toilet. Family members who accompanied the child but were not responsible for caregiving in the aforementioned areas were not included in our sample.
Sample size requirement
A minimum sample size of 296 caregivers was required for this study, based on 26% as the percentage of caregivers with poor knowledge, as presented in an earlier study from Iraq (18), and 5% as the desired precision for the proportion estimate. The OpenEpi software ver. 3.01 was utilised to calculate the required sample size (20).
Data collection tool
A structured questionnaire consisting of three sections (demographics, knowledge, and attitudes) was utilised in this study (refer to research questionnaire). The first section enquired about both the caregiver’s and the child’s demographic characteristics. For the caregivers, eight items were included: age (in years), relation to the child, marital status, educational level, residence, caregiver-reported family income, the total number of children in the family, and the number of children with ASD. For the children, six items were included for age (years), gender, birth order, age at ASD diagnosis, and the presence and type of comorbid conditions.
To assess caregivers’ knowledge of ASD, a survey was developed based on the Autism Stigma and Knowledge Questionnaire (ASK-Q) and a review of the literature (17, 18, 21–25). The ASK-Q was originally created in 2017 to cover a wide range of content related to different aspects of ASD, including aetiology, symptoms/diagnosis, and treatment. Authors of the original validation study reported good construct validity and reliability, indicated by an intraclass correlation of 0.88 and Cronbach’s α of 0.86 (10). The ASK-Q has also shown cross-cultural applicability and has been translated and tested into different languages, including Mongolian (α = 0.72), Chinese (α = 0.89), and Arabic (α = 0.83) (26–29).
For each item in the survey, three answers were provided: “yes”, “no”, and “I don’t know”. The survey includes 48 items covering aetiology (13 items), signs and symptoms (23 items), diagnosis (2 items), treatment (6 items), and outcome (4 items). In accordance with the scoring system outlined for the ASK-Q items in the initial validation study, participants who answered correctly received a score of 1 on the item, whereas those who provided incorrect or neutral answers received a score of 0 (21). In total, knowledge scores were calculated by summing up the scores of all items, resulting in a total of forty-eight points.
Attitudes toward ASD were assessed across various domains using a survey developed, including items described in previous studies (21, 30–33). These domains included attitudes towards mental health services (2 items), attitudes towards children with ASD (6 items), attitudes towards the education of children with ASD (4 items), and attitudes towards parents’ responsibility (1 item). All items, except those related to attitudes towards mental health services, were presented on a 5-point Likert scale ranging from “strongly agree” to “strongly disagree”.
Two independent psychiatrists reviewed the questionnaire for content validity before data collection. In addition, 25 caregivers participated in a pilot study to test item clarity. Cronbach’s α showed that the knowledge scale is internally consistent at 0.73, higher than the recommended cut-off point of 0.70 (34). Due to a low Cronbach’s alpha, attitudes had no overall or domain-level scores, as items were heterogeneous and should be discussed individually.
Data quality assurance
Multiple steps were taken to ensure data quality. Starting with the interview, all items were completed to reduce missing values. Second, to test intra-item validity, one item of the outcome knowledge domain was duplicated as a negative-form sentence to reduce random answer bias. Inconsistent respondents were excluded from the analysis. Data analysis began only after the completion of data collection. Finally, Equator Network’s STROBE cross-sectional studies guideline was used to mitigate reporting bias (35).
Statistical analysis
Statistical analysis was conducted using the Statistical Package for Social Sciences (SPSS) program version 28, with a significance level set at <0.05.
Categorical variables were described with counts and proportions. To evaluate normality, both the D’Agostino-Pearson K2 and Shapiro-Wilk tests were used (Table 1), as the latter might be too sensitive to large sample sizes on its own. The mean and SD were used to describe normally distributed variables, while the median and IQR were employed for non-normal distributions. To aid comparison with recently published studies, caregivers were classified as having good knowledge if they answered >50% of questions correctly (score: ≥25) and poor knowledge otherwise (23, 36). The GraphPad Prism program version 10 was employed to visualise this data. The time since the child’s diagnosis was calculated by subtracting the child’s age at the time of diagnosis from their current age.
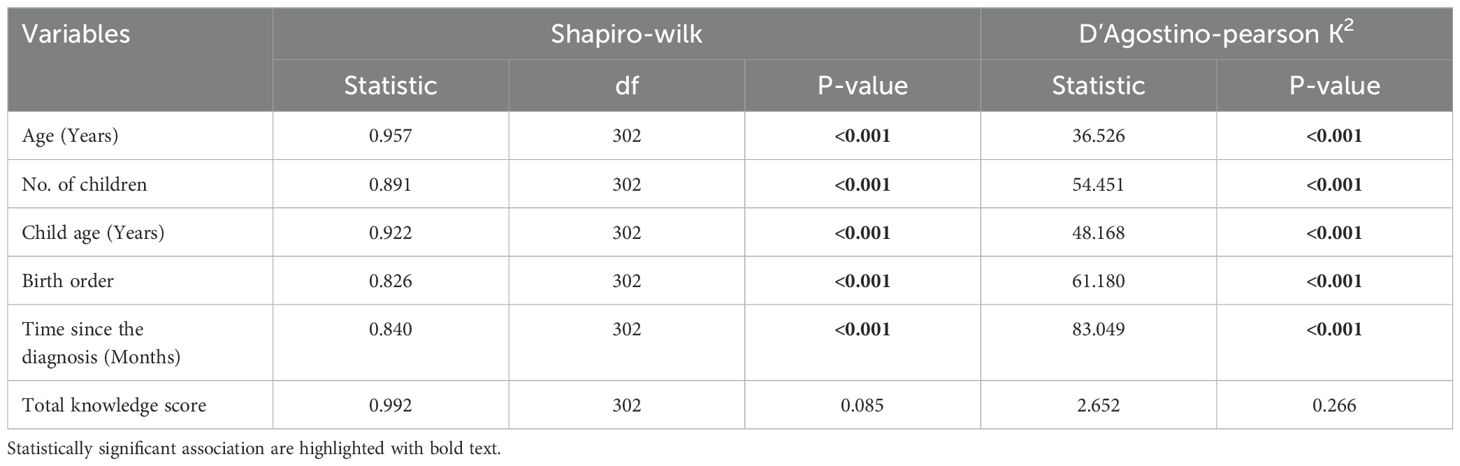
Table 1. Normality testing for the study variables.
The association between knowledge scores and demographic characteristics was assessed using various statistical tests, including the independent samples t-test, Mann-Whitney U-test, ANOVA, and Kruskal-Wallis test. The choice of test depended on the number of demographic subgroups and the normality of knowledge scores within each subgroup. The Benjamin-Hochberg procedure was used to account for multiple tests and maintain a 5% false discovery rate (37). Post-hoc pairwise analyses were conducted using Tukey’s HSD test following ANOVA, and Dunn-Bonferroni test following Kruskal-Wallis. Spearman’s rank correlation was used to study the correlations between continuous demographic variables and knowledge scores.
Results from post-hoc pairwise analyses showed that college-educated caregivers had higher knowledge than illiterate, primary school, and secondary school-educated caregivers. Similarly, caregivers from low-income backgrounds had less knowledge than those from average or high-income backgrounds. Hence, lack of tertiary education and low income were identified as risk factors for poor knowledge and used to compare the performance on individual knowledge items using Chi-square and Fisher exact tests. Multiple linear regression was also performed for further validation by including the dichotomous risk variables (lack of tertiary education and low income) as predictors and the knowledge score as an outcome variable. The squared zero-order correlation was reported to indicate the fraction of total variance in knowledge attributable to each predictor. Meanwhile, the squared partial correlation was utilised to signify the unique contribution of each predictor by presenting the proportion of residual variance attributed to a specific predictor after controlling for others.
To aid in interpreting attitude items, “agree” and “strongly agree” for items 3, 4, 6, 7, and 12 were reclassified as “negative” attitudes, while those for items 5, 8, 9, 10, 11, and 13 were reclassified as “positive” attitudes. The same reclassification was done for “disagree” and “strongly disagree”. Additionally, to explore the effect of the complexity of the child’s presentation, chi-square was utilised to test the association between the presence of comorbid conditions and items related to the attitudes of the parents.
Results
Data validation and inclusion
During the data collection period, 314 caregivers were interviewed. Of these, 12 (3.8%) were excluded due to inconsistent answers on the duplicated item used as a data validation procedure. In total, 302 (96.2%) caregivers were included in our sample: 180 (59.6%) from Al-Subtain Academy and 122 (40.4%) from Baghdad’s National Centre.
Sample characteristics
Mothers comprised the highest percentage of caregivers (218, 72.2%), while fathers and other family members, such as the child’s sibling, grandparent, aunt, or uncle, accounted for 48 (15.9%) and 36 (11.9%), respectively. 12 (4.0%) of the caregivers were illiterate, and 60 (19.9%) came from a low-income background. 141 (46.7%) of the children in our study had other comorbid conditions, such as ADHD (80, 26.4%), intellectual issues (42, 13.9%), and cerebral palsy (9, 2.9%). Other demographic factors for both the caregivers and their children are summarised in Table 2.
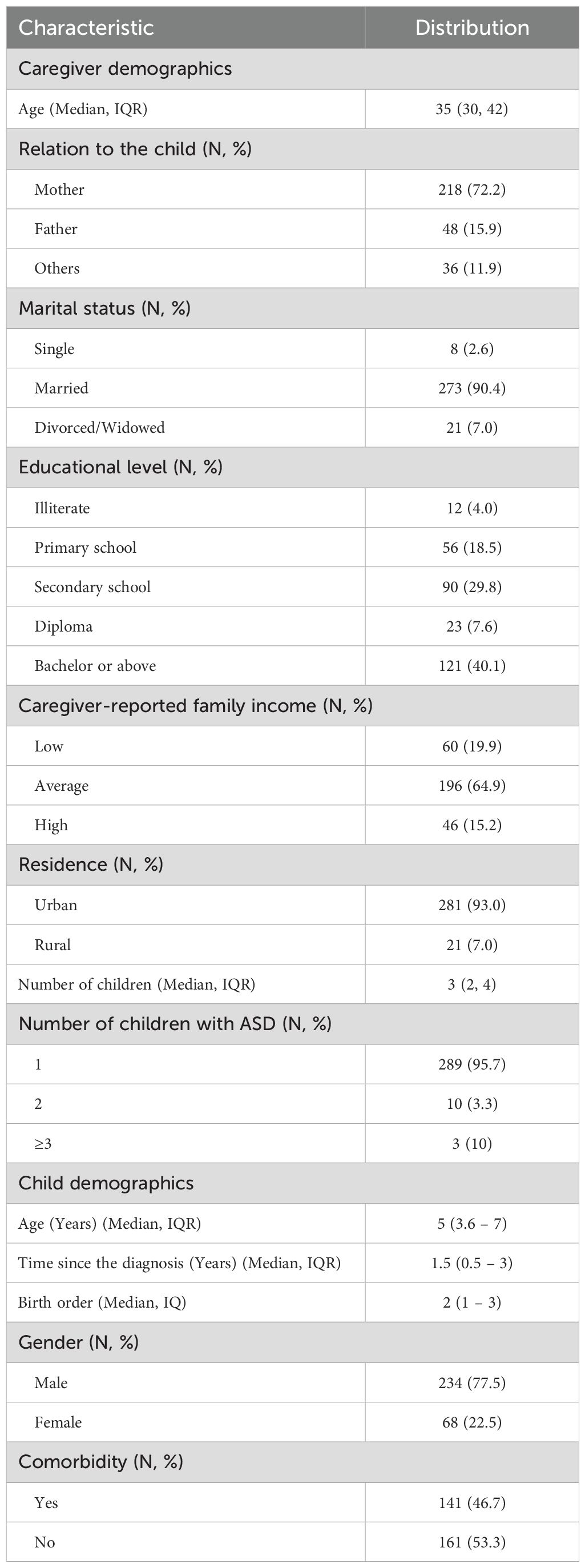
Table 2. Sample characteristics (N = 302).
Knowledge of ASD among caregivers
In our sample, the average knowledge score was 31.7 (± 5.1) out of 48. Out of the caregivers surveyed, 27 (8.9%) had low knowledge and 275 (91.1%) had a good level of knowledge regarding ASD (Figure 1). The performance on individual knowledge items is summarised in Table 3.
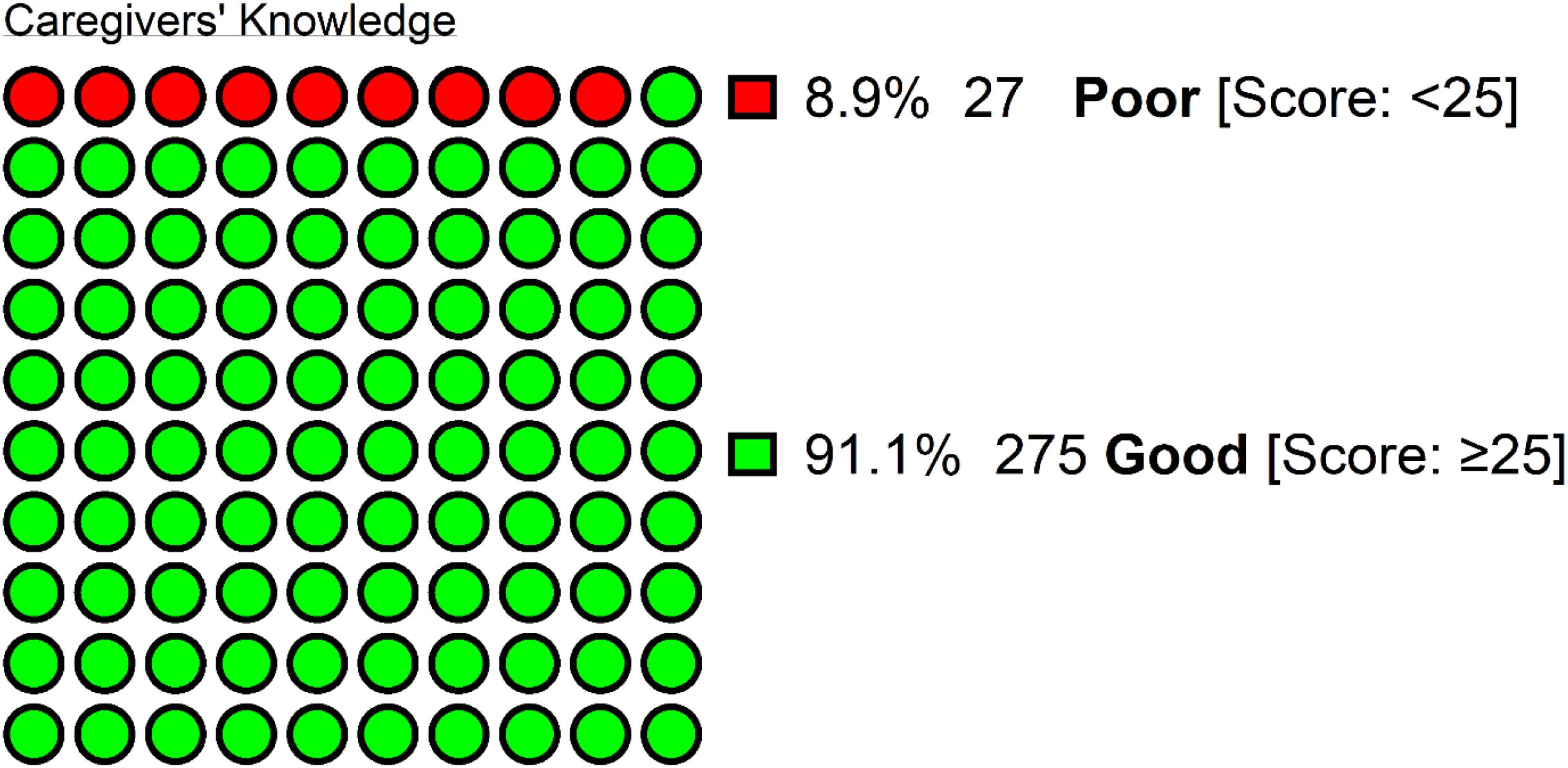
Figure 1. The knowledge of Iraqi caregivers toward autism spectrum disorder (N = 302), with good knowledge defined as having >50% of the total score on the 48-points knowledge scale.
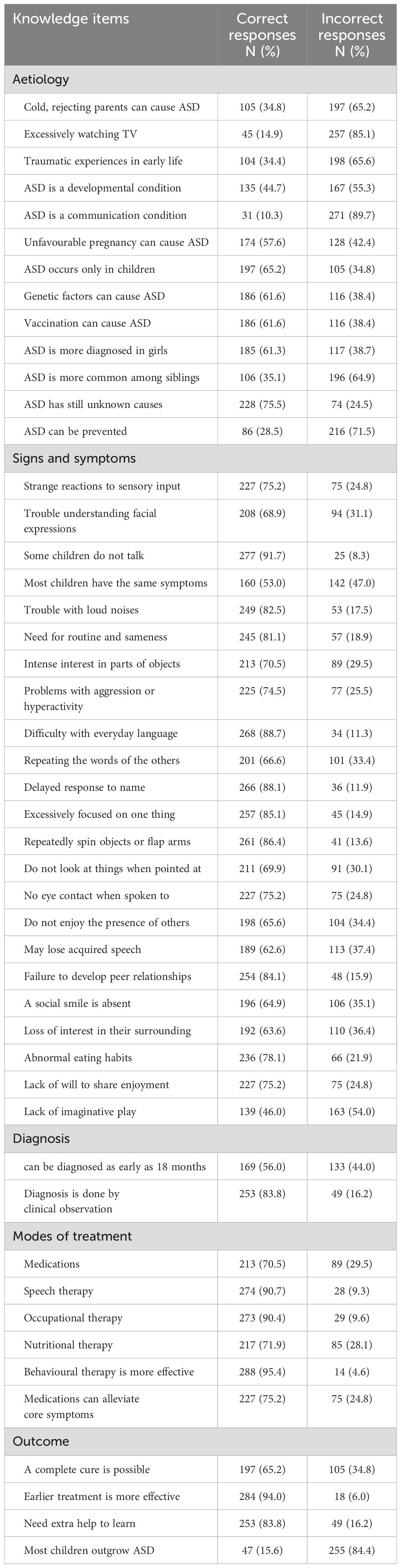
Table 3. Knowledge among caregivers of children with autism spectrum disorder (N = 302).
A statistically significant association was demonstrated between caregivers’ knowledge of ASD and their educational level and family income (Table 4). Child comorbidity was significantly associated with higher knowledge but only before adjusting for multiple testing (adjusted p-value = 0.088). No statistically significant correlations were found with the parents’ age (adjusted p-value = 0.673) or the time since the diagnosis of ASD (adjusted p-value = 0.249) (Table 5).
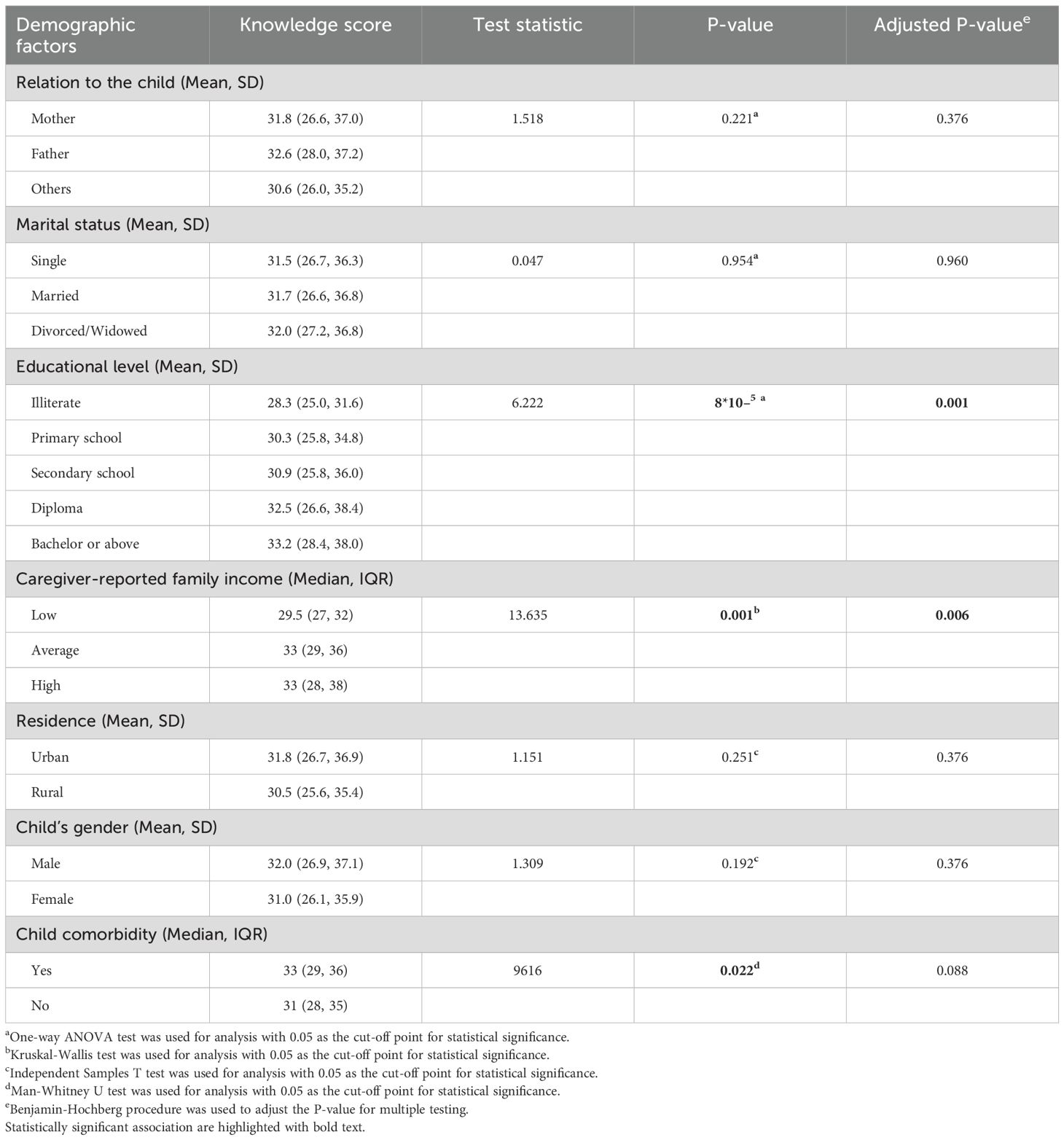
Table 4. Association between overall knowledge score among parents of children with autism spectrum disorder and demographic factors (N = 302).
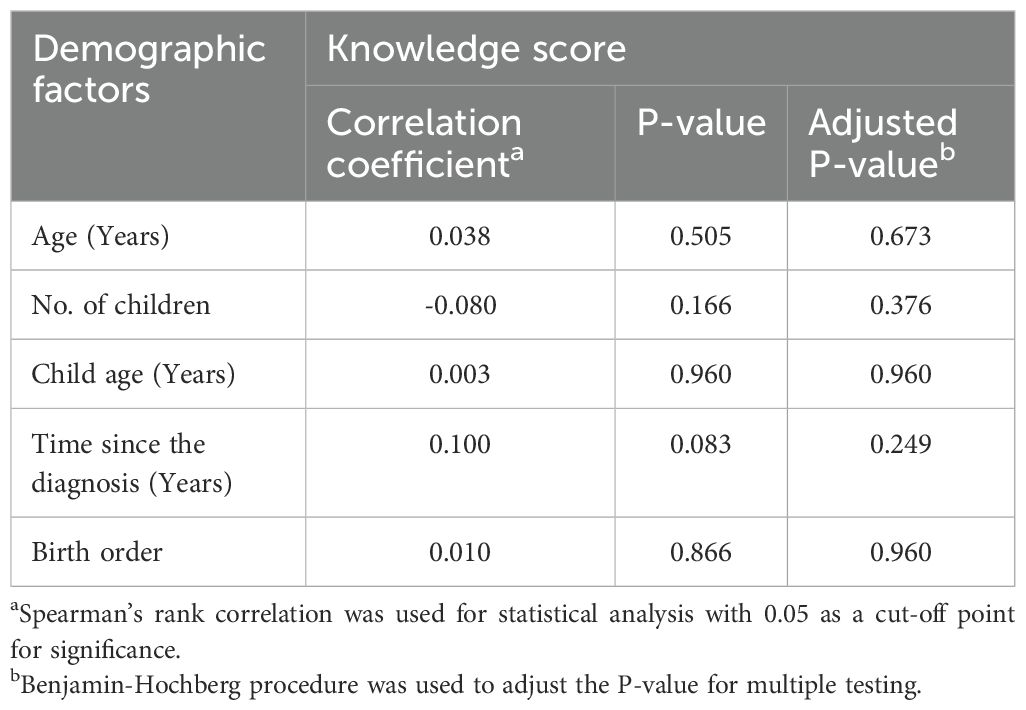
Table 5. Correlation between overall knowledge score among parents of children with autism spectrum disorder and demographic factors (N = 302).
Through post-hoc pairwise analysis, significant differences in knowledge scores were found between caregivers with a bachelor’s degree or higher and those who were illiterate (p-value = 0.009), had a primary school degree (p-value = 0.002), or had a secondary school degree (p-value = 0.007) (Table 6). Similarly, differences were identified between caregivers from low-income backgrounds and those from average (p-value = 0.002) or good backgrounds (p-value = 0.005), but not between individuals from average and good backgrounds (p-value = 1.000). Therefore, performance on individual knowledge items was compared between caregivers based on tertiary education attainment and low-income backgrounds (Table 7). When further investigated with multiple linear regression, lack of tertiary education had a significant positive relation, uniquely explaining 3.8% of the variance in knowledge scores (B = 2.177, p-value = 0.0006), while low family income was no longer significant after controlling for lack of tertiary education (B = 1.231, p-value = 0.119) (Table 8). These two predictors also showed a statistically significant association with one another, as pointed out by the fact that only 2 (3.3%) of those with low income had tertiary education compared to 142 (58.7%) of those with average or high family income (p-value <0.001) (Table 9).
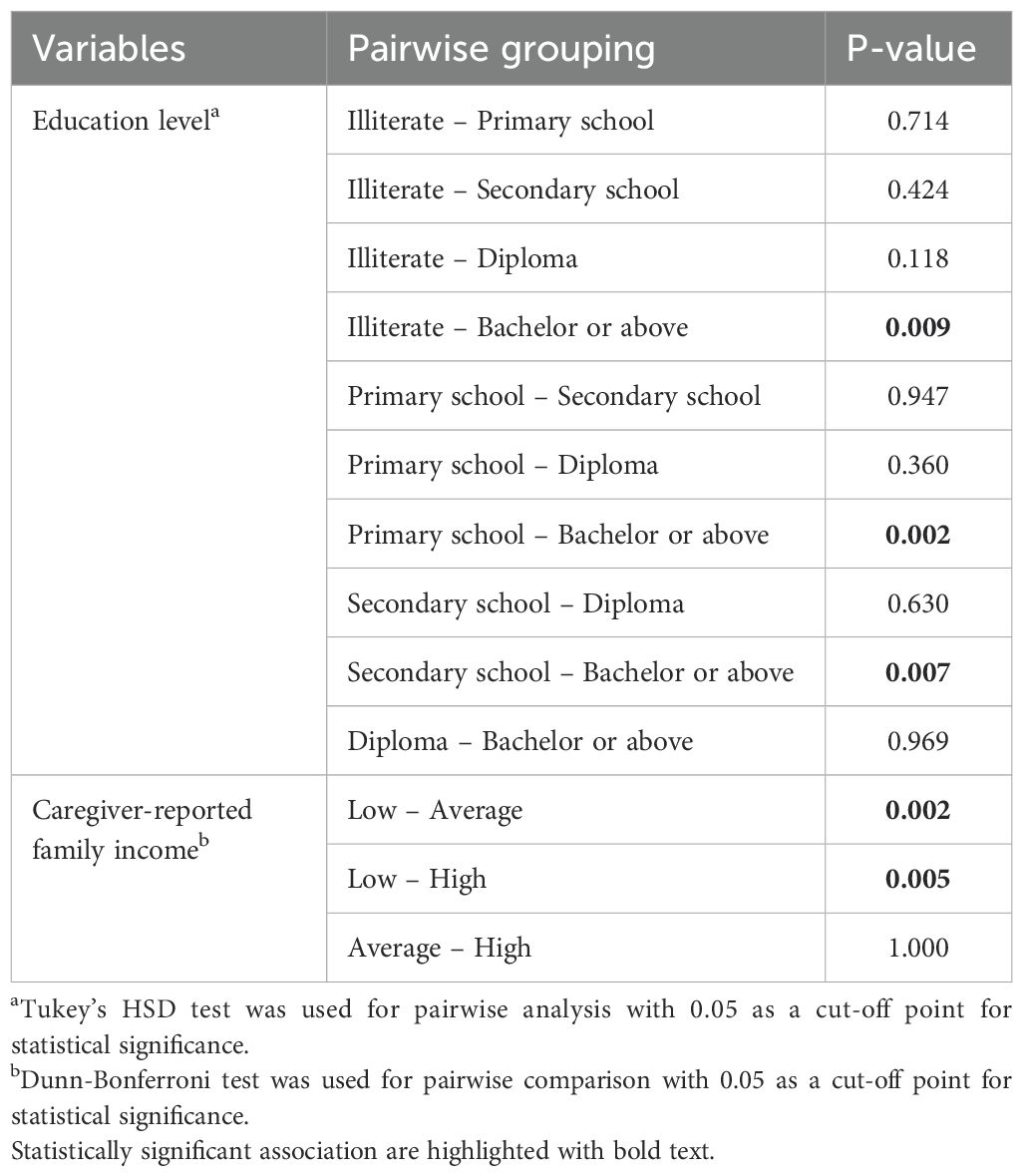
Table 6. Pairwise analysis for the association between education levels and family income with knowledge score among parents of children with autism spectrum disorder (N = 302).
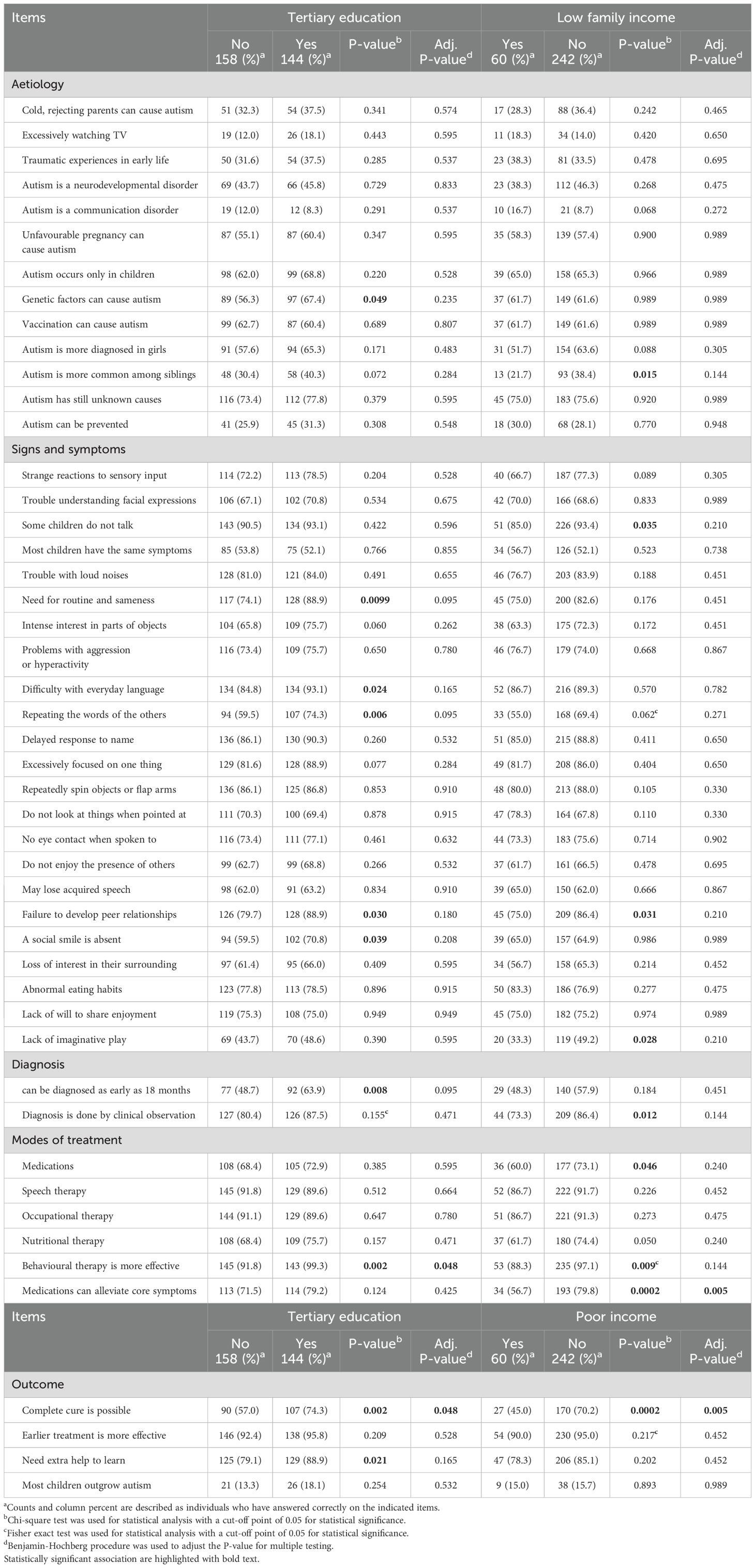
Table 7. Knowledge item performance among risk groups in caregivers of autistic children (N = 302).
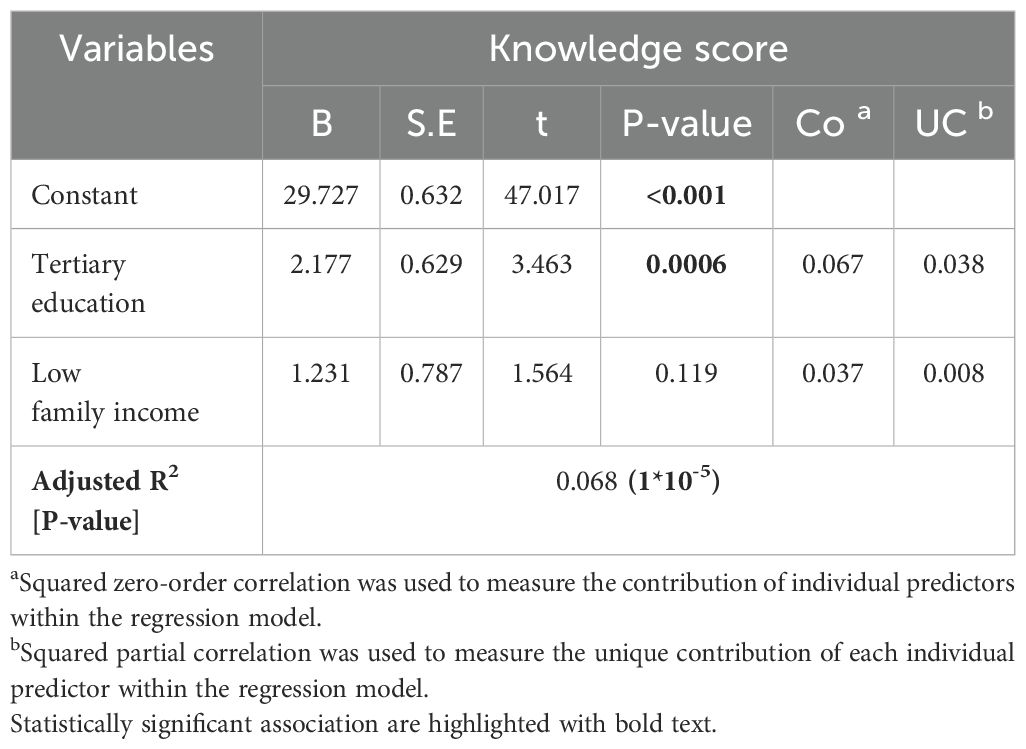
Table 8. Multiple regression analysis model for caregivers’ knowledge, with lack of tertiary education and low family income as predictor variables.
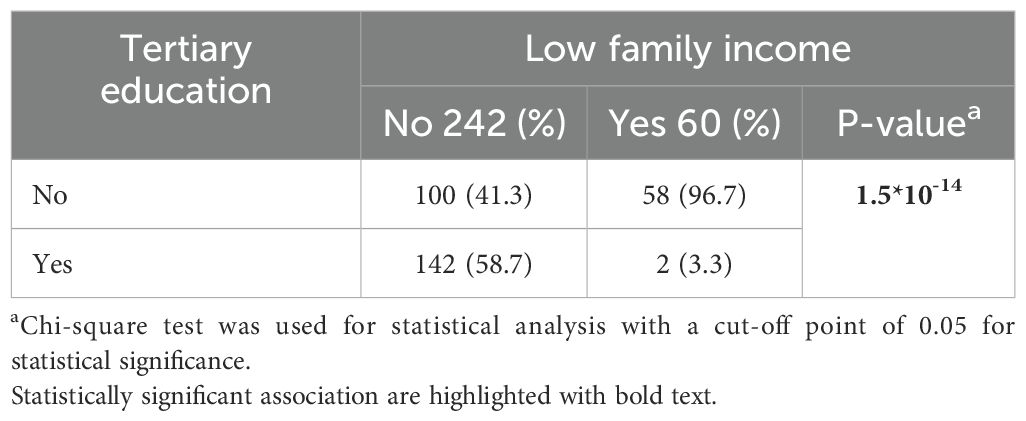
Table 9. The association between lack of tertiary education and low family income among caregivers of children with autism spectrum disorder (N = 302).
Attitudes toward ASD among caregivers
Of the caregivers surveyed, 277 (91.7%) stated that they would visit the closest health organisation if their child could not speak by 2 years of age, while only 8 (2.6%) answered that there is no need to worry. The most consulted specialists were psychiatrists (139, 46.0%), followed by children’s primary healthcare physicians (42, 13.9%) and neurologists (41, 13.6%). Caregivers’ attitudes on various aspects of ASD are shown in Table 10. The item related to the responsibility of parents towards their children with special needs received the highest number of positive responses, with 285 (94.4%). Conversely, the lowest proportion of positive attitudes was towards the notion that children with ASD are deliberately negativistic and non-compliant, with only 105 (34.8%) responses. Parents of children with comorbid conditions were more likely to feel ashamed of the child’s diagnosis. However, this difference was only significant before adjusting for multiple testing (adjusted p-value = 0.286).
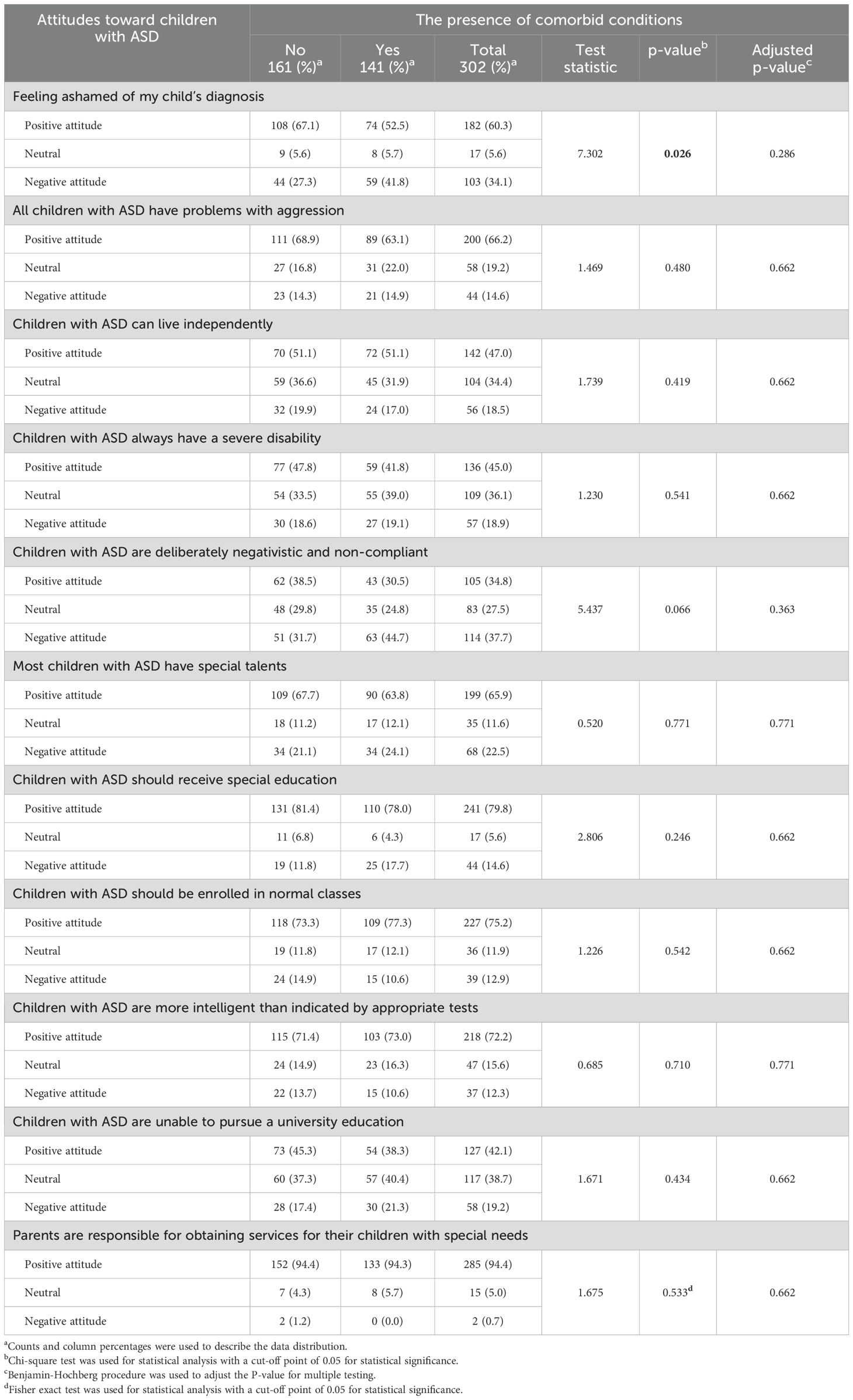
Table 10. The association between the presence of comorbid conditions and the parents’ attitudes toward children with autism spectrum disorder (N = 302).
Discussion
Less than one-tenth (8.9%) of the caregivers demonstrated poor knowledge. This percentage is lower than the 26% reported in a previous study from Hilla province in Iraq. However, details regarding the specific cut-off point used were not mentioned (18). Recently published studies from Egypt and Nigeria also found that 68.3% and 98.7% of caregivers, respectively, had poor/unsatisfactory knowledge using the same cut-off point (<50% of the total score) (23, 36). These results are encouraging, as previous studies have shown that increasing caregivers’ knowledge can reduce stress, improve parenting competency, and lead to better adaptive outcomes in children (9, 14, 23, 38). The importance of conducting such programmes is also highlighted by the fact that, in our study, the time since the diagnosis of the child with ASD did not result in a significant increase in knowledge. Therefore, in our local setting, parents may not naturally gain more knowledge without support from a formal educational program.
Caregivers’ knowledge was found to be linked to their level of education and self-reported family income. A pairwise analysis of this connection identified caregivers without tertiary education and those from low-income backgrounds as at-risk groups for lower knowledge. This is consistent with previous results from Basra province in Iraq and Egypt, where the largest difference in knowledge was observed between caregivers with a college education and those without (17, 23). A study from China also identified the absence of tertiary education and a low family income as risk factors for lower knowledge (25). The relation between caregivers’ education and family income is well documented in the literature (39). This is also evident in our sample, where the relationship between family income and knowledge was no longer significant after controlling for tertiary education in multiple regression. This suggests that family income may not be independently connected to knowledge of ASD; rather, its significance stems from its relationship with the caregivers’ level of education.
Contrary to previous findings from Iraq, Egypt, and China, the association between parents’ age and knowledge in our study was not significant (19, 23, 25). Another study from Malaysia also found that mothers had more knowledge than fathers (22), while we found that both parents had comparable knowledge scores. This might be a result of the higher involvement of Arabic fathers in childcare or due to the fact that data collection involved only parents who attended with their children to the healthcare centres. These parents may have similar levels of involvement in their children’s care, leading to equal knowledge regardless of their biological roles. This idea could also account for the demonstrated similarity in knowledge regardless of marital status. Future studies should include both parents for each child to further explore these possibilities.
Caregivers of children with comorbid conditions, such as ADHD and intellectual issues, had higher knowledge scores. This could be attributed to more frequent contact with healthcare providers. However, this association was no longer significant after adjusting for p-values, so it cannot be definitively established (40).
The majority of caregivers (85.1%) believed that ASD can be caused by excessive TV watching. Additionally, 65.2% believed that cold-rejecting parents can cause ASD, and 38.4% thought that vaccines could lead to ASD. These misconceptions were also present in previous studies conducted in Iraq. For example, a study from 2020 reported prevalence rates of 64%, 38%, and 34.8% for these misconceptions, respectively. Another study from 2022 found that 67.3% of caregivers believed that emotional deprivation could cause the condition (18, 19). These misconceptions relate to the perceived susceptibility construct of the Health Belief Model and have been shown to affect caregivers’ health-related behaviour regarding their children by increasing vaccine refusal, stigmatisation, and self-blame among caregivers (41, 42). As such, the persistence of these misconceptions, despite previously published results indicating their prevalence, highlights the importance of conducting educational interventions to address them.
A third of the caregivers in our sample expressed feeling shame about their child’s diagnosis. Parents’ shame may also arise when children with ASD exhibit behaviours that are considered socially unacceptable in public (43). Hence, the complexity of the child’s presentation, including the presence of comorbid conditions, could worsen parents’ shame. In our study, the statistical link between parental shame and comorbid conditions was only evident before adjusting for multiple testing. Therefore, additional research is needed before drawing any definitive conclusion.
Caregivers, in our study, had a better perceived severity of ASD compared to perceived susceptibility. This can be shown through better performance on items related to ASD symptoms than aetiology, presumably due to exposure to the symptoms through their children or by talking to healthcare professionals (44). Specifically, 88.1% of caregivers identified delayed response to name as a potential symptom, 75.2% recognised poor eye contact, and 86.4% recognised repetitive and restrictive behaviours. These results align with a study from Hilla but are higher than those described in a study from Egypt, where only 28.3% recognised poor eye contact and 20% recognised repetitive and restrictive behaviours (18, 23).
Most caregivers perceived the benefits of behavioural therapy and early treatment for ASD. However, around a third (34.8%) still believed that a complete cure is possible, especially those without tertiary education (43.0%) or from low-income backgrounds (55.0%). Additionally, 84.4% thought that most children will outgrow ASD. These misconceptions need to be addressed, particularly among the subgroups mentioned earlier, as they may affect health-related behaviours in terms of treatment expectations and cooperation with healthcare professionals. Belief in a complete cure might lead parents to go through dangerous, unproven treatments, diverting attention from useful evidence-based supportive therapy. In 2019, the USA Food and Drug Administration published an article advising parents against falling prey to deceptive cure claims and highlighting how to identify such claims (45).
Most caregivers also agreed that caring for children with disabilities is the parents’ responsibility. However, many harboured negative attitudes, including the belief that all children with ASD are aggressive, severely disabled, intentionally negative, and non-compliant. These negative attitudes were present in similar proportions regardless of the child’s presentation complexity, defined by the presence of comorbid conditions. These stigmatising attitudes should be addressed through comprehensive educational campaigns, as they can result in caregivers perceiving their child’s behaviour or a disability as a barrier to accessing important health services (46). This occurs when caregivers do not pursue interventions and rather hide their child away to avoid social stigma.
Three-fourths of caregivers supported the inclusion of children with ASD in regular classes, consistent with previous studies from Iraq and Spain (18, 44). In the latter study, parents of typically developing children also had positive attitudes, albeit less so. Mainstream schools could provide an inclusive environment for children with ASD to interact with their peers, ultimately reducing social segregation and improving employment prospects (44). However, efforts to integrate these children into mainstream schools should be approached cautiously, taking into consideration the attitudes of typically developing peers, their families, and the broader cultural context. Previous studies have highlighted bullying as a common reason for families of children with ASD to change schools, underscoring the importance of addressing these concerns (47).
Strengths and limitations
In this study, we explored the knowledge and attitudes among caregivers of autistic children, utilising a pairwise analytical approach to identify the group of caregivers who had low knowledge and negative attitudes toward children with ASD.
Certain limitations, however, can be demonstrated. Firstly, knowledge and attitudes were only assessed among caregivers who attended the healthcare centres. This sampling bias might result in an underestimation of the frequency of poor knowledge and negative attitudes, as these caregivers may possess more awareness due to their higher involvement in their children’s care. Additionally, lower generalisability might occur due to the exclusion of fathers and other family members who are less likely to attend healthcare centres with the children despite being responsible for a crucial portion of the childcare. To provide a more comprehensive depiction of caregivers’ knowledge and attitudes, this sampling bias should be addressed in future studies by involving other family members who may play a more minor, although crucial, part of providing care for the child. Secondly, data was collected from the middle and southern regions of Iraq and, as such, might not be representative of caregivers on a national level. Thirdly, the data collection tool utilised in this study might be subject to self-desirability bias, similar to other self-reported measures. Finally, an individual-item approach was adopted to discuss attitudes toward ASD. This was necessary based on the unfavourable internal consistency of attitude items. However, as a limitation, this causes an inability to explore overall attitudinal trends.
Conclusion
In this study, we have shown that, despite the majority of caregivers having good overall knowledge of ASD, some misconceptions have persisted since earlier studies. Many of these misconceptions were related to the aetiology of ASD, namely the beliefs that ASD could be caused by vaccines, television, and negligent parenting. Given their persistence, more extensive educational interventions may be necessary. These interventions should also address treatment expectations and emphasise the lifelong nature of ASD, especially among caregivers without tertiary education and those from low-income backgrounds. Efforts should be made to reduce negative attitudes towards these children, such as the belief that they are always aggressive, intentionally negative, and non-compliant. Positive attitudes toward including children with ASD in mainstream schooling were also recognised; however, further studies are needed to evaluate other factors that may affect the children’s experience and adaptive outcomes.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: https://doi.org/10.17632/b7dc3ww9b7.1.
Ethics statement
The studies involving humans were approved by The National Centre for Training and Human Development research committee under the Ministry of Health and Environment. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
HA: Investigation, Methodology, Resources, Writing – original draft, Writing – review & editing. OJ: Investigation, Project administration, Resources, Writing – original draft. FL: Conceptualization, Investigation, Resources, Writing – original draft. SJ: Investigation, Project administration, Resources, Writing – original draft. NN: Data curation, Formal Analysis, Supervision, Writing – original draft, Writing – review & editing. MS: Conceptualization, Methodology, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. GA: Conceptualization, Data curation, Formal Analysis, Methodology, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. Financial support for publication was provided by Al-Subtain University of Medical Science and Al-Subtain Academy for Autism and Neurodevelopmental Disorders.
Acknowledgments
The authors are grateful to child psychiatrists from Baghdad’s National Centre for Autism and Child Psychiatry for their expertise during the development of the measurement tool. The authors would also like to thank the caregivers for their help during the data collection.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1568467/full#supplementary-material
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association (2013). doi: 10.1176/appi.books.9780890425596
2. Maenner MJ, Warren Z, Williams AR, Amoakohene E, Bakian AV, Bilder DA, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 years — Autism and developmental disabilities monitoring network, 11 sites, United States, 2020. MMWR Surveillance Summaries. (2023) 72:1–14. doi: 10.15585/mmwr.ss7202a1
3. Qiu S, Lu Y, Li Y, Shi J, Cui H, Gu Y, et al. Prevalence of autism spectrum disorder in Asia: A systematic review and meta-analysis. Psychiatry Res. (2020) 284:112679. doi: 10.1016/j.psychres.2019.112679
4. Talantseva OI, Romanova RS, Shurdova EM, Dolgorukova TA, Sologub PS, Titova OS, et al. The global prevalence of autism spectrum disorder: A three-level meta-analysis. Front Psychiatry. (2023) 14:1071181. doi: 10.3389/fpsyt.2023.1071181
5. Samadi SA. The challenges of establishing healthcare services in low- and middle-income countries: the case of autism spectrum disorders (ASD) in the Kurdistan Region of Iraq—Report from the field. Brain Sci. (2022) 12:1433. doi: 10.3390/brainsci12111433
6. Daniolou S, Pandis N, and Znoj H. The efficacy of early interventions for children with autism spectrum disorders: A systematic review and meta-analysis. J Clin Med. (2022) 11:5100. doi: 10.3390/jcm11175100
7. Wozniak RH, Leezenbaum NB, Northrup JB, West KL, and Iverson JM. The development of autism spectrum disorders: variability and causal complexity. WIREs Cogn Sci. (2017) 8. doi: 10.1002/wcs.1426
8. Harrison AJ, Slane MM, Hoang L, and Campbell JM. An international review of autism knowledge assessment measures. Autism. (2017) 21:262–75. doi: 10.1177/1362361316638786
9. Burrell TL and Borrego J. Parents’ Involvement in ASD treatment: what is their role? Cognit Behav Pract. (2012) 19:423–32. doi: 10.1016/j.cbpra.2011.04.003
10. Harrison AJ, Long KA, Manji KP, and Blane KK. Development of a brief intervention to improve knowledge of autism and behavioural strategies among parents in Tanzania. Intellect Dev Disabil. (2016) 54:187–201. doi: 10.1352/1934-9556-54.3.187
11. Alnazly EK and Abojedi A. Psychological distress and perceived burden in caregivers of persons with autism spectrum disorder. Perspect Psychiatr Care. (2019) 55:501–8. doi: 10.1111/ppc.12356
12. ten Hoopen LW, de Nijs PFA, Duvekot J, Greaves-Lord K, Hillegers MHJ, Brouwer WBF, et al. Children with an autism spectrum disorder and their caregivers: capturing health-related and care-related quality of life. J Autism Dev Disord. (2020) 50:263–77. doi: 10.1007/s10803-019-04249-w
13. Janz NK and Becker MH. The health belief model: A decade later. Health Educ Q. (1984) 11:1–47. doi: 10.1177/109019818401100101
14. Milgramm A, Corona LL, Janicki-Menzie C, and Christodulu KV. Community-based parent education for caregivers of children newly diagnosed with autism spectrum disorder. J Autism Dev Disord. (2022) 52:1200–10. doi: 10.1007/s10803-021-05025-5
15. Mira Á, Berenguer C, Baixauli I, Roselló B, and Miranda A. Family context of children with autism. Implications for emotional and social development. Med (B Aires). (2019) 79:22–6.
16. Bashinova S, Kokoreva O, Peshkova N, and Khamdamova V. Determination of the development of social behaviour of preschool children with autism spectrum disorder by the type of parental attitude. Educ Self Dev. (2022) 17:141–56. doi: 10.26907/esd.17.3.12
17. Khudhair AS and Jassim SK. The knowledge of autistic children’s mothers regarding autism in Basra City. Am J Nurs Res. (2018) 6:296–8. doi: 10.12691/ajnr-6-5-11
18. Hasan AA. Assessment of Family Knowledge toward their Children with Autism Spectrum Disorder at Al-Hilla City, Iraq. Indian J Forensic Med Toxicol. (2020) 14:3025–31. doi: 10.37506/ijfmt.v14i4.12051
19. Alkazam ZTA and Al-Dujaili AH. Assessment knowledge and attitude among caregivers of children with autism spectrum disorders. Int J Health Sci (Qassim). (2022) 6(2):11376–89. doi: 10.53730/ijhs.v6nS2.7987
20. Sullivan KM, Dean A, and Soe MM. On academics: openEpi: A web-based epidemiologic and statistical calculator for public health. Public Health Rep. (2009) 124:471–4. doi: 10.1177/003335490912400320
21. Harrison AJ, Bradshaw LP, Naqvi NC, Paff ML, and Campbell JM. Development and psychometric evaluation of the autism stigma and knowledge questionnaire (ASK-Q). J Autism Dev Disord. (2017) 47:3281–95. doi: 10.1007/s10803-017-3242-x
22. Kaman N, Ishak A, and Muhammad J. Knowledge, attitudes, and associated factors of caregivers towards children with autism spectrum disorder in East Coast Peninsular Malaysia. PeerJ. (2023) 11:e14919. doi: 10.7717/peerj.14919
23. Elhawat F. Assessment of knowledge, attitude and practices of parents having children with autism. Helwan Int J Nurs Res Pract. (2023) 2:233–59. doi: 10.21608/hijnrp.2023.198165.1067
24. Anwar MS, Tahir M, Nusrat K, and Khan MR. Knowledge, awareness, and perceptions regarding autism among parents in Karachi, Pakistan. Cureus. (2018) 10(9). doi: 10.7759/cureus.3299
25. Wang F, Lao U-C, Xing Y-P, Zhou P, Deng W-L, Wang Y, et al. Parents’ knowledge and attitude and behaviour toward autism: a survey of Chinese families having children with autism spectrum disorder. Transl Pediatr. (2022) 11:1445–57. doi: 10.21037/tp-22-113
26. Taresh S, Ahmad NA, Roslan S, and Ma’rof AM. Knowledge in autism spectrum disorder (ASD) among pre-school teachers in Yemen. In Proceedings of the 3rd International Conference on Special Education (ICSE). Atlantis Press. (2019) Vol. 388. (2019).
27. Harrison AJ, Paff ML, and Kaff MS. Examining the psychometric properties of the autism stigma and knowledge questionnaire (ASK-Q) in multiple contexts. Res Autism Spectr Disord. (2019) 57:28–34. doi: 10.1016/j.rasd.2018.10.002
28. Schultz PV, Brambila-Manso B, Couto-Rosa L, Rocha KSS, de Araújo DCSA, Ayres LR, et al. Validation of autism stigma knowledge – questionnaire (ASK-Q) for Brazilian portuguese. Exploratory Res Clin Soc Pharm. (2024) 15:100495. doi: 10.1016/j.rcsop.2024.100495
29. Lu M, Wang R, Zou Y, and Pang F. Chinese college students’ Knowledge of autism spectrum disorder (ASD) and social distance from individuals with ASD: the mediating role of negative stereotypes. J Autism Dev Disord. (2022) 52:3676–85. doi: 10.1007/s10803-021-05252-w
30. Wang J, Zhou X, Xia W, Sun C, Wu L, and Wang J. Autism awareness and attitudes towards treatment in caregivers of children aged 3–6 years in Harbin, China. Soc Psychiatry Psychiatr Epidemiol. (2012) 47:1301–8. doi: 10.1007/s00127-011-0438-9
31. Liu Y, Li J, Zheng Q, Zaroff CM, Hall BJ, Li X, et al. Knowledge, attitudes, and perceptions of autism spectrum disorder in a stratified sampling of preschool teachers in China. BMC Psychiatry. (2016) 16:142. doi: 10.1186/s12888-016-0845-2
32. Bin LW, Ying SHK, Tean SCH, Lin DCK, Lian YC, and Yun HL. Pre-school teachers’ knowledge, attitudes and practices on childhood developmental and behavioural disorders in Singapore. J Pediatr Child Health. (2008) 44:187–94. doi: 10.1111/j.1440-1754.2007.01231.x
33. Campbell DG, Reichle NC, and Van Bourgondien ME. The Autism Survey: An evaluation of reliability and validity. J Autism Dev Disord. (1996) 26:621–34. doi: 10.1007/BF02172351
34. Cicchetti DV. Guidelines, criteria, and rules of thumb for evaluating normed and standardized assessment instruments in psychology. Psychol Assess. (1994) 6:284–90. doi: 10.1037/1040-3590.6.4.284
35. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, and Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. (2007) 147:573. doi: 10.7326/0003-4819-147-8-200710160-00010
36. Oduyemi AY, Okafor IP, Eze UT, Akodu BA, and Roberts AA. Internalization of stigma among parents of children with autism spectrum disorder in Nigeria: a mixed method study. BMC Psychol. (2021) 9:182. doi: 10.1186/s40359-021-00687-3
37. Benjamini Y and Hochberg Y. Controlling the false discovery rate: A practical and powerful approach to multiple testing. J R Stat Soc Ser B Stat Methodol. (1995) 57:289–300. doi: 10.1111/j.2517-6161.1995.tb02031.x
38. Abd El Hameed HS, Ramadan EN, and Elshair IH. The effect of educational program on caregivers (Knowledge and practicing) toward their autistic children. J Am Sci. (2018) 8:756–64.
39. Ou J-J, Shi L-J, Xun G-L, Chen C, Wu R-R, Luo X-R, et al. Employment and financial burden of families with preschool children diagnosed with autism spectrum disorders in urban China: results from a descriptive study. BMC Psychiatry. (2015) 15:3. doi: 10.1186/s12888-015-0382-4
40. Dizitzer Y, Meiri G, Flusser H, Michaelovski A, Dinstein I, and Menashe I. Comorbidity and health services’ usage in children with autism spectrum disorder: a nested case–control study. Epidemiol Psychiatr Sci. (2020) 29:e95. doi: 10.1017/S2045796020000050
41. Novilla MLB, Goates MC, Redelfs AH, Quenzer M, Novilla LKB, Leffler T, et al. Why parents say no to having their children vaccinated against measles: A systematic review of the social determinants of parental perceptions on MMR vaccine hesitancy. Vaccines (Basel). (2023) 11:926. doi: 10.3390/vaccines11050926
42. Bonsu NEM, Mire SS, Sahni LC, Berry LN, Dowell LR, Minard CG, et al. Understanding vaccine hesitancy among parents of children with autism spectrum disorder and parents of children with non-autism developmental delays. J Child Neurol. (2021) 36:911–8. doi: 10.1177/08830738211000505
43. Ng CKM, Lam SHF, Tsang STK, Yuen CMC, and Chien C-W. The relationship between affiliate stigma in parents of children with autism spectrum disorder and their children’s activity participation. Int J Environ Res Public Health. (2020) 17:1799. doi: 10.3390/ijerph17051799
44. Gómez-Marí I, Tárraga-Mínguez R, and Pastor-Cerezuela G. Analysis of Spanish Parents’ Knowledge about ASD and Their Attitudes towards Inclusive Education. Eur J Investig Health Psychol Educ. (2022) 12:870–81. doi: 10.3390/ejihpe12070063
45. U.S Food and Drugs Administration. Be aware of Potentially Dangerous Products and Therapies that Claim to Treat Autism. US Food and Drugs Administration (2019). Available online at: https://www.fda.gov/consumers/consumer-updates/be-aware-potentially-dangerous-products-and-therapies-claim-treat-autism.
46. Babalola T, Sanguedolce G, Dipper L, and Botting N. Barriers and facilitators of healthcare access for autistic children in the UK: a systematic review. Rev J Autism Dev Disord. (2024). doi: 10.1007/s40489-023-00420-3
Keywords: autism, attitude, caregiver, knowledge, stigma, psychoeducation
Citation: Al-Juhaishi HQK, Jaber OA, Lami F, Jasim SM, Nayeri ND, Sabet MS and Al-Gburi G (2025) Risk factors for low knowledge and negative attitudes among caregivers of children with autism spectrum disorder in Iraq: a multi-centre cross-sectional study. Front. Psychiatry 16:1568467. doi: 10.3389/fpsyt.2025.1568467
Received: 29 January 2025; Accepted: 07 July 2025;
Published: 04 August 2025.
Edited by:
Antonio Narzisi, Stella Maris Foundation (IRCCS), ItalyReviewed by:
April Hargreaves, National College of Ireland, IrelandAngelos Papadopoulos, University of Patras, Greece
Copyright © 2025 Al-Juhaishi, Jaber, Lami, Jasim, Nayeri, Sabet and Al-Gburi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ghaith Al-Gburi, Z2hhaXRoLmFsaS5raGFsZWVsQGdtYWlsLmNvbQ==
†These authors share senior authorship