 Lisa Cynthia Niwenahisemo1,2
Lisa Cynthia Niwenahisemo1,2 Qi Zhang1,2
Qi Zhang1,2 Wo Wang2,3
Wo Wang2,3 Dan-dan Geng2,3He-yan Xu2,3
Dan-dan Geng2,3He-yan Xu2,3 Jin-hui Hu1,2
Jin-hui Hu1,2 Ling-li Ma1,2
Ling-li Ma1,2 Jian-yu Tan1,2
Jian-yu Tan1,2 Yi-ting Kong1,2
Yi-ting Kong1,2 Su Hong2,4*†
Su Hong2,4*† Li Kuang1,2*
Li Kuang1,2*- 1Department of Psychiatry, the First Affiliated Hospital of Chongqing Medical University, Chongqing, China
- 2Psychiatric Center, the First Affiliated Hospital of Chongqing Medical University, Chongqing, China
- 3Department of Psychiatry, the University-town Hospital of Chongqing Medical University, Chongqing, China
- 4Department of Nursing, the First Affiliated Hospital of Chongqing Medical University, Chongqing, China
Introduction: Cultural factors and assessment methods significantly influence how anxiety symptoms are expressed and reported. However, few cross-cultural studies have employed culturally appropriate and validated tools, and even fewer have provided substantial comparisons across different groups with diverse cultural backgrounds. This study aimed to assess the measurement invariance of the GAD-7 scale across Chinese and Rwandese adolescents, enabling reliable cross-cultural comparisons.
Methods: This study included 2017 Chinese adolescents and 1813 Rwandan adolescents. Cronbach’s alpha, exploratory factor analysis (EFA), and multiple group confirmatory factor analysis (MGCFA) were used to assess the validity of the GAD-7 scale across the two groups. Measurement invariance testing was employed to investigate cross-cultural equivalence.
Results: The GAD-7 demonstrated good psychometric properties. CFA supported a one-factor model for the GAD-7 in both samples, though model fit indices varied. Measurement invariance testing confirmed configural and metric invariance but found partial scalar invariance. A latent mean comparison indicated a trend toward higher anxiety levels in Rwandan adolescents compared to Chinese adolescents, though the difference was not statistically significant (z = 0.02, d = 0.033, p = 0.98).
Discussion: The GAD-7 showed reliability in measuring generalized anxiety in both Chinese and Rwandese adolescents, confirming its cross-cultural construct validity. However, partial scalar invariance suggests that while the GAD-7 effectively detects anxiety symptoms, the severity of reported symptoms may not be directly comparable across cultures due to response patterns and possible linguistic factors. These findings highlight the importance of culturally sensitive instruments for accurate anxiety assessment and expand evidence on reliable symptom screening and treatment monitoring across diverse populations.
Introduction
Adolescence is a critical developmental period characterized by significant biological, psychological, and social transformations (1). This stage is particularly vulnerable to the emergence of mental health challenges, with anxiety disorders being among the most prevalent and debilitating conditions affecting adolescent well-being worldwide (2). Epidemiological studies estimate that 15% to 30% of adolescents globally experience clinically significant anxiety symptoms, with notable variations across regions and populations (3, 4). For instance, while anxiety disorders affect 5% to 10% of adolescents in sub-Saharan Africa, prevalence rates rise to 18.6% among teenage girls in Tanzania and 20.4% in Rwanda. In contrast, Chinese adolescents exhibit even higher rates, with approximately 30% reporting anxiety symptoms (5–8). These disparities may reflect true differences in prevalence or methodological challenges in cross-cultural mental health research, including variations in diagnostic sensitivity, cultural expression of symptoms, and measurement validity (9–11). A critical methodological consideration in cross-cultural comparisons is the establishment of measurement invariance, which ensures that observed differences in mental health outcomes reflect true variations in the underlying construct rather than artifacts of measurement bias (12).
Measurement invariance is typically assessed through confirmatory factor analysis (CFA), which evaluates three hierarchical levels: configural invariance (equivalent factor structure), metric invariance (equivalent factor loadings), and scalar invariance (equivalent item intercepts) (12). Without establishing measurement invariance, cross-cultural comparisons of mental health constructs risk being confounded by cultural differences in symptom interpretation and reporting.
The Generalized Anxiety Disorder-7 (GAD-7) scale, a widely used instrument based on DSM-IV diagnostic criteria, has gained recognition for its brevity, reliability, and validity in assessing anxiety symptoms across diverse populations (13–15). However, despite its widespread adoption, questions remain regarding its cross-cultural applicability (16, 17). While the original validation study by Spitzer et al. (14) proposed a unidimensional factor structure, subsequent research has identified variations in factor structures across cultures, including evidence for a two-factor model distinguishing somatic and cognitive symptoms (18). Furthermore, studies have reported partial measurement invariance and differential item functioning (DIF) for specific GAD-7 items, particularly those related to nervousness and excessive worrying, suggesting cultural influences on symptom interpretation (19, 20). These findings underscore the need for rigorous evaluation of the GAD-7’s cross-cultural validity, particularly in understudied populations.
Despite growing interest in cross-cultural mental health research, most studies have focused on Western populations, leaving significant gaps in our understanding of the GAD-7’s applicability in non-Western contexts, particularly in comparisons between Asian and African populations. To bridge this gap, the present study examines the cross-cultural measurement invariance of the GAD-7 in adolescent samples from Rwanda and China, two culturally distinct yet understudied populations. Data were collected from Shapingba District in Chongqing, China, and Gasabo and Kicukiro Districts in Kigali, Rwanda. These regions were selected for their socioeconomic and cultural diversity, as well as their representation of urban, suburban, and rural populations. Chongqing, a megacity with over 31 million residents, encompasses a wide range of socioeconomic backgrounds, while Kigali, Rwanda’s capital, serves as a cultural and educational hub, drawing students from across the country.
Building on prior studies (21, 22), we hypothesized that the GAD-7 would demonstrate a unidimensional structure in both populations and exhibit measurement invariance across cultural groups. Additionally, we aimed to compare latent mean levels of anxiety symptoms between Rwandan and Chinese adolescents, contingent on the establishment of scalar or partial scalar invariance. This study contributes to the growing body of literature on cross-cultural mental health assessment by providing empirical evidence on the GAD-7’s validity in understudied populations, thereby enhancing its utility for global mental health research and practice.
Methodology
Participants
The study included 3,830 adolescents aged 12 to 18, recruited from middle and high schools in Shapingba District, Chongqing Municipality, China (n=2,017), and Gasabo and Kicukiro Districts in Kigali, Rwanda (n=1,813). In Shapingba District, which comprises 17 junior high schools and 11 senior high schools, a stratified random sampling approach was employed based on urban and suburban areas to ensure sample diversity and representativeness. Schools were stratified by geographical location (urban or suburban), and within each stratum, schools were randomly selected. Specifically, 3 urban schools and 2 suburban schools were chosen to reflect the socioeconomic and cultural diversity of the district. From these schools, at least two classes per grade level were randomly selected, and students within each class were further chosen using a random number table or generator to ensure equal representation.
In Rwanda, a cluster sampling method was utilized due to the geographical distribution of schools to select schools that represented a diverse range of students from rural, urban, and suburban areas across all provinces of the country. Five secondary boarding schools (2 public and 3 private) were randomly selected from a total of 27 schools in Gasabo and Kicukiro Districts. Within each school, classes from both ordinary (grades 7-9) and advanced (grades 10-12) levels were randomly selected using a random number generator. Approximately 2000 students were targeted from each country, with strict adherence to randomization procedures to minimize bias. All participating researchers received comprehensive training to ensure consistency and accuracy. Data collection spanned from 2021 to 2023, and the sample size was calculated using Franklin K.’s formula to ensure adequate statistical power and generalizability.
Data collection
Data collection methods were tailored to the local context in each country. In China, surveys were administered via a secure online platform, allowing for anonymous submissions. This approach was chosen to align with the high prevalence of internet access and technological literacy in metropolitan Chongqing. In Rwanda, where boarding school students often have restricted access to personal devices, in-person data collection was conducted in classroom settings under the supervision of trained researchers. Surveys were administered in the participants’ native languages (Mandarin for Chinese participants and Kinyarwanda for Rwandan participants) to minimize language-related bias and enhance comprehension.
All participants and their parents or guardians provided written informed consent after being fully informed of the study’s objectives, voluntary nature, and their right to withdraw at any time without consequences. To ensure anonymity, student ID numbers were used as unique identifiers, with no additional personal information collected. Ethical approval was obtained from the College of Medicine and Health Sciences Institutional Review Board of the University of Rwanda (CMHS IRB; No. 465/CMHS IRB/2022) and the Ethics Committee of the First Affiliated Hospital of Chongqing Medical University with research batch number (No. 2020-879).
Assessment instrument
The Generalized Anxiety Disorder Symptom Severity (GAD-7) Scale, developed by Spitzer (14), was used to assess anxiety symptom severity. The GAD-7 is a well-validated, self-report instrument consisting of seven items that measure symptoms such as nervousness, excessive worrying, difficulty relaxing, restlessness, impatience, and persistent fearfulness (Löwe et al., 2008b; Ruiz et al., 2011). It employs a 4-point Likert scale (0 = not at all to 3 = nearly every day), with total scores ranging from 0 to 21. Cut-off scores of ≥5, ≥10, and ≥15 to indicate mild, moderate, and severe anxiety symptoms respectively (14). For adolescent populations, a cut-off score of ≥7 is recommended based on community-based studies (23). The GAD-7 has demonstrated strong psychometric properties, including high reliability and validity, in both clinical and community settings (18, 24).
Statistical analyses
Data was analyzed using SPSS (Statistical Package for the Social Sciences) version 26 for descriptive statistics, and IBM AMOS (Analysis of Moment Structures) version 26 for structural equation modeling. Preliminary analyses included checks for missing values, outliers, and normality assumptions. Descriptive statistics were computed to summarize demographic characteristics and GAD-7 within each group. Independent t-tests were used to compare mean GAD-7 scores between Chinese and Rwandan adolescents, while chi-square tests examined gender distribution differences.
To evaluate the psychometric properties of the GAD-7, Pearson’s correlation analysis was conducted to assess item-total correlations, followed by Cronbach’s alpha to determine internal consistency (18). Exploratory factor analysis (EFA) was performed using principal axis factoring with oblique rotation (Promax) to explore the underlying factor structure within each cultural group. The number of factors retained was determined based on scree plot and eigenvalues greater than one.
Confirmatory factor analysis (CFA) was then conducted to test the fit of the GAD-7’s unidimensional model in each cultural group. Model fit was assessed using multiple indices, including the chi-square goodness-of-fit test, Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), and Root Mean Square Error of Approximation (RMSEA). Standard thresholds were applied to determine acceptable model fit (CFI > 0.95, TLI > 0.95, RMSEA < 0.08). Measurement invariance across the Chinese and Rwandan samples was tested using multi-group CFA, examining three hierarchical levels: configural invariance (equivalent factor structure), metric invariance (equivalent factor loadings), and scalar invariance (equivalent item intercepts). Changes in fit indices (e.g., ΔCFI, ΔRMSEA) were used to evaluate invariance at each level as a criterial for invariance test based on Cheung and Rensvold (2000)’s standards. It was proposed that according to their guidelines, a ΔCFI ≤ 0.01 and ΔRMSEA ≤ 0.015 thresholds (25). If scalar or partial scalar invariance was established, latent mean comparisons of anxiety symptoms between the two groups were conducted.
Results
Descriptive statistics
This study compared anxiety symptoms among adolescents in China and Rwanda. The sample included 2017 Chinese adolescents (56.7% male, 43.3% female; mean age = 15.35 ± 1.56 years) recruited from middle and high schools in Chongqing, and 1813 Rwandan adolescents (51.2% male, 48.8% female; mean age = 15.80 ± 1.90) from Kigali.
Rwandan adolescents reported significantly higher average GAD-7 score (M = 5.7, SD = 4.5) compared to their Chinese counterparts (M =2.6, SD = 4.1), indicating a higher prevalence of generalized anxiety disorder symptoms in the Rwandan sample (52.5% vs. 23.2%, P<0.001; Table 1). Examination of the Normal Q-Q plots revealed deviations from a perfect normal distribution for both samples. The Chinese sample exhibited a positive skew, suggesting a higher frequency of elevated anxiety scores, while the Rwandan sample displayed a distribution closer to normality, albeit with a slight positive skew at higher scores. (Figures 1, 2).
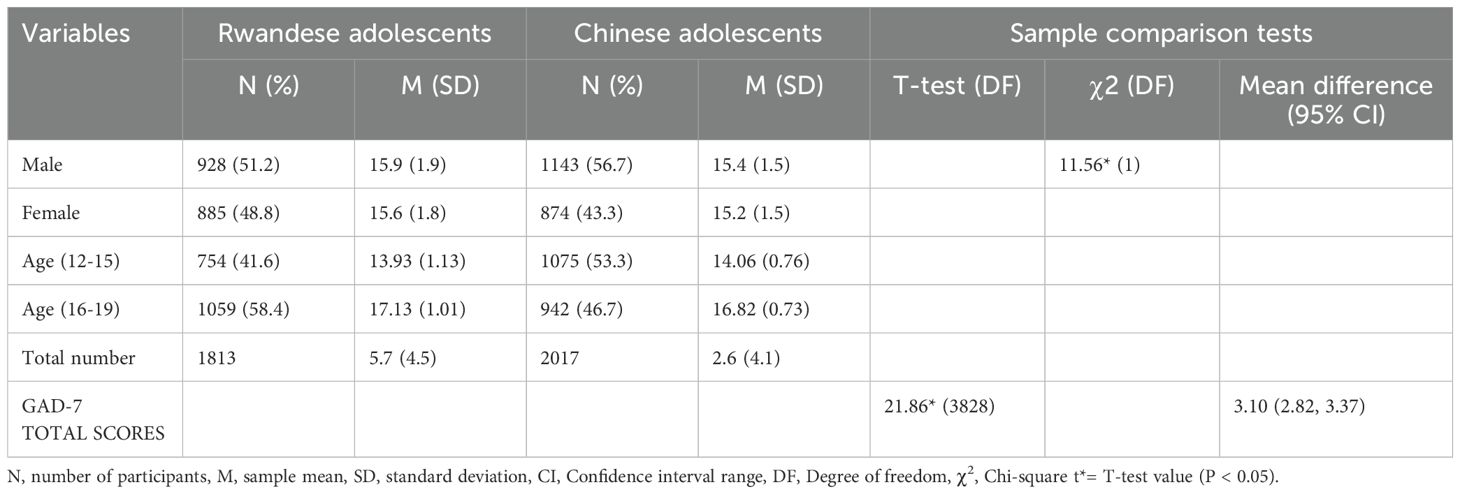
Table 1. Sample demographic features descriptive statistics.
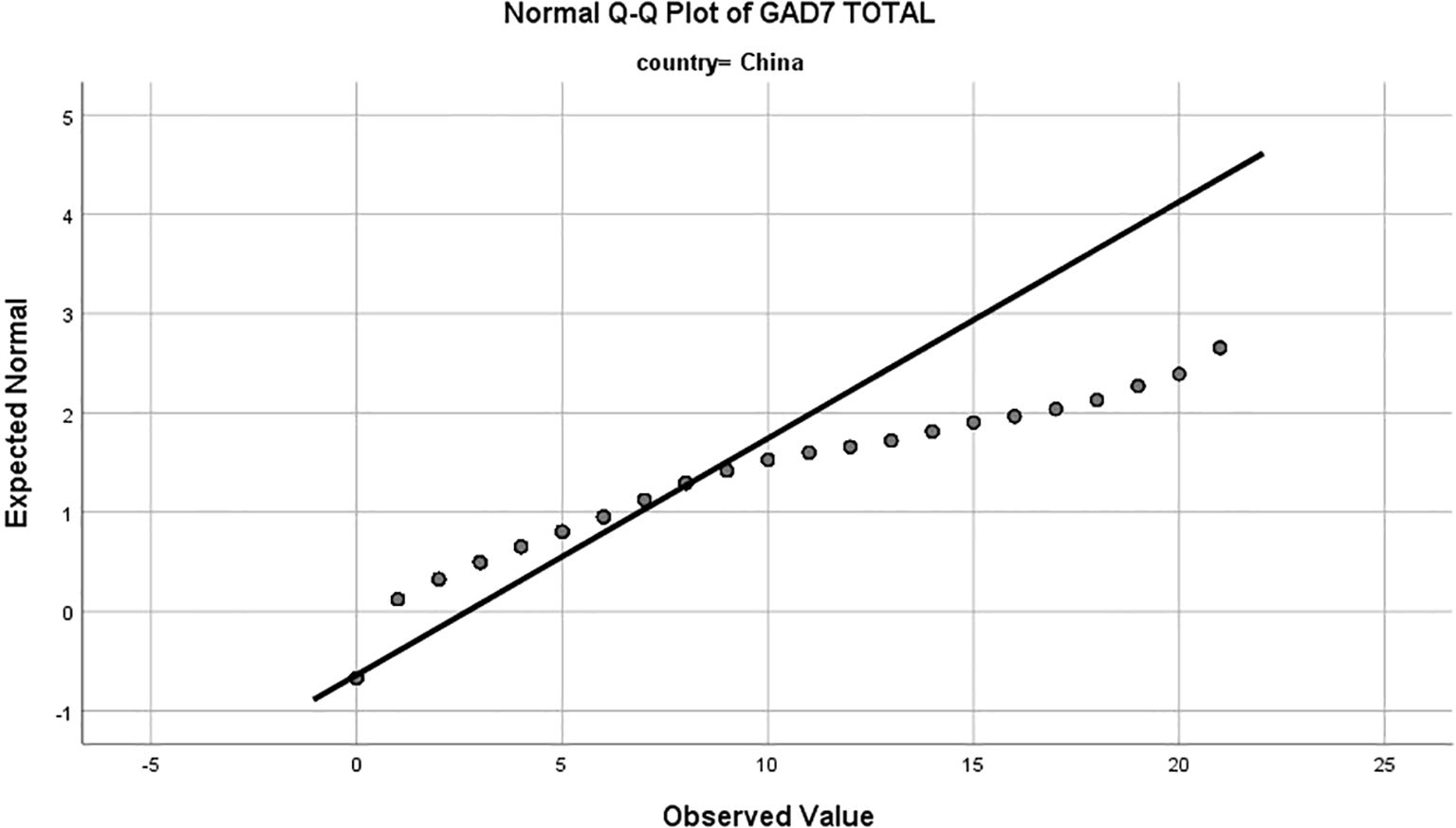
Figure 1. Normal Q-Q plot of Generalized Anxiety Disorder-7 (GAD-7) total scores for Chinese adolescents. The x-axis represents the expected normal distribution of scores under the assumption of normality, while the y-axis represents the observed values of GAD-7 scores. Deviations from the diagonal line indicate departures from normality, with the Chinese sample showing a positive skew, suggesting a higher frequency of elevated anxiety scores.
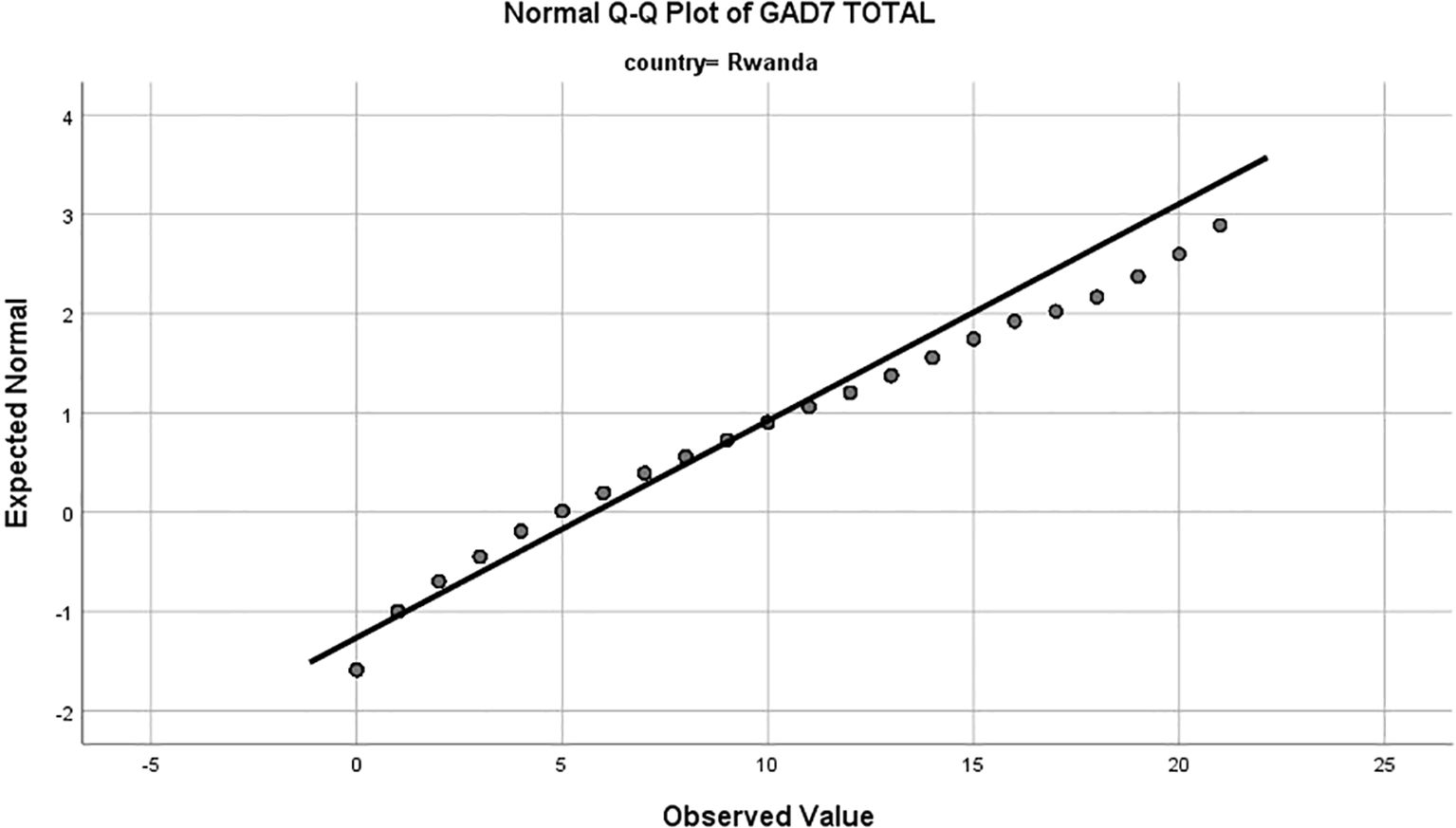
Figure 2. Normal Q-Q plot of Generalized Anxiety Disorder-7 (GAD-7) total scores for Rwandan adolescents. The x axis represents the expected normal distribution of scores under the assumption of normality, while the y-axis represents the observed values of GAD-7 scores. The Rwandan sample displays a distribution closer to normality, albeit with a slight positive skew at higher scores, indicating a tendency toward higher anxiety levels.
Scale features and baseline model establishment
Scree plots were used to determine the optimal factors structure for the GAD-7. For both samples, a one-factor solution was supported, as evidenced by eigenvalue and scree plots complimenting (Figures 3, 4). The GAD-7 demonstrated strong reliability in both groups (Cronbach’s α ≥ 0.70), and all items were retained, as their removal would reduce the scale’s reliability. Item-total correlations fell within the acceptable range (0.30 to 0.70) (26) (Table 2).
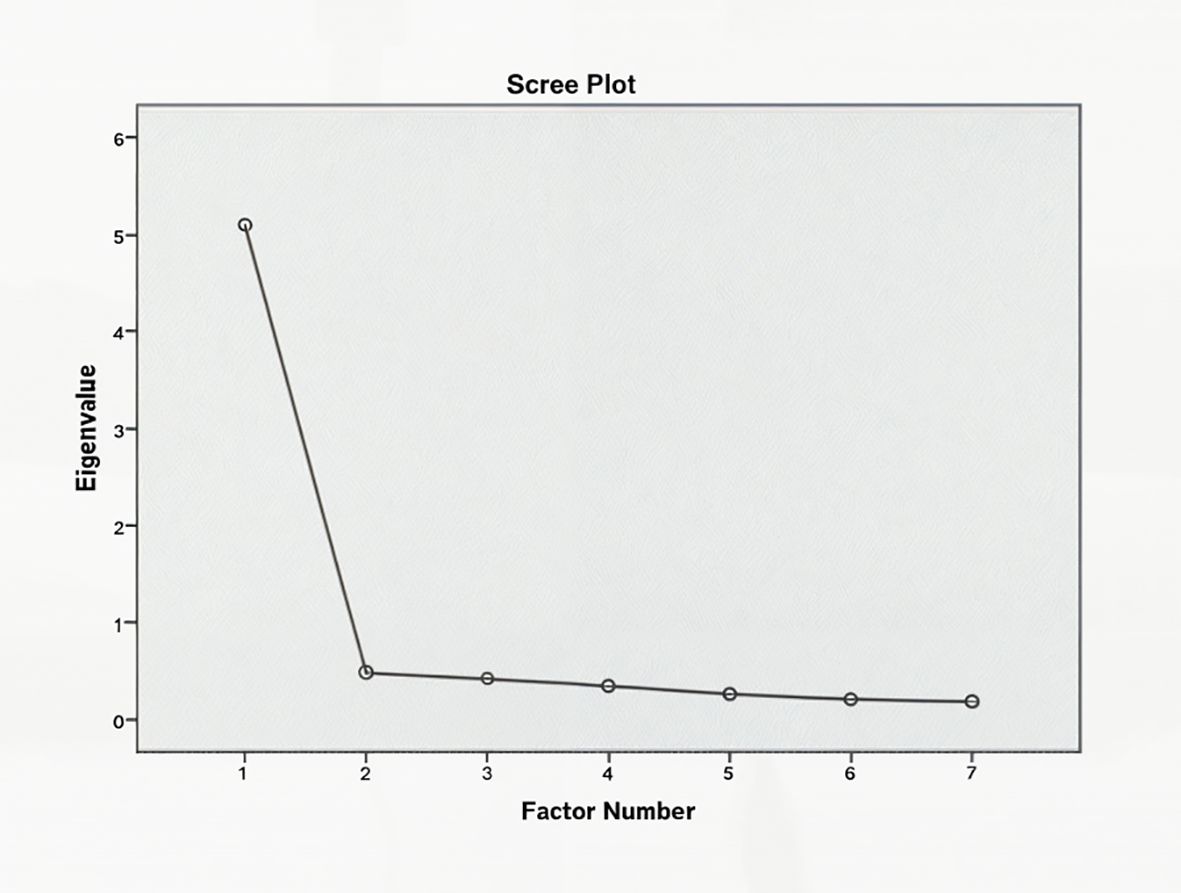
Figure 3. Scree plot for the Generalized Anxiety Disorder-7 (GAD-7) scale in Chinese adolescents. The x-axis represents the factor number, and the y-axis represents the eigenvalues, which indicate the amount of variance explained by each factor. The plot shows a clear elbow at the second factor, supporting a one-factor solution for the GAD-7 in the Chinese sample, consistent with the unidimensional structure of the scale.
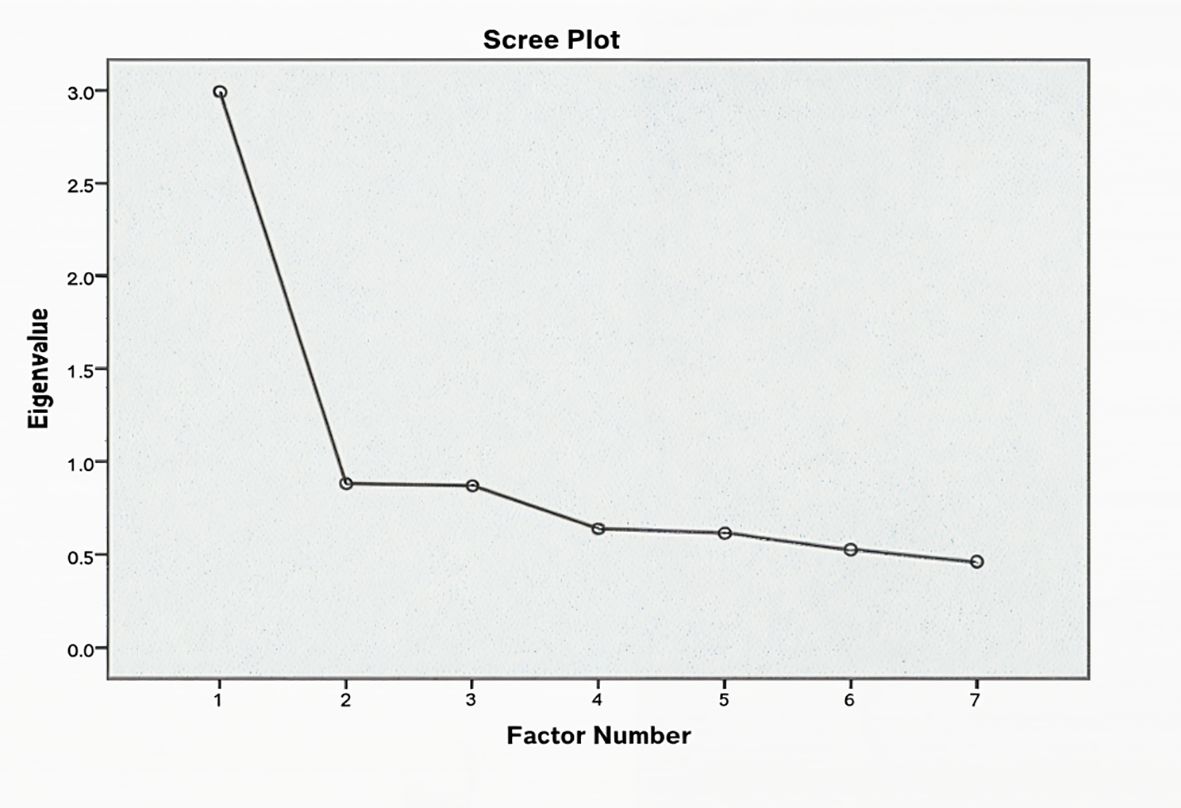
Figure 4. Scree plot for the Generalized Anxiety Disorder-7 (GAD-7) scale in Rwandan adolescents. The x-axis represents the factor number, and the y-axis represents the eigenvalues, which indicate the amount of variance explained by each factor. The plot shows a clear elbow at the second factor, supporting a one-factor solution for the GAD-7 in the Rwandan sample, consistent with the unidimensional structure of the scale.
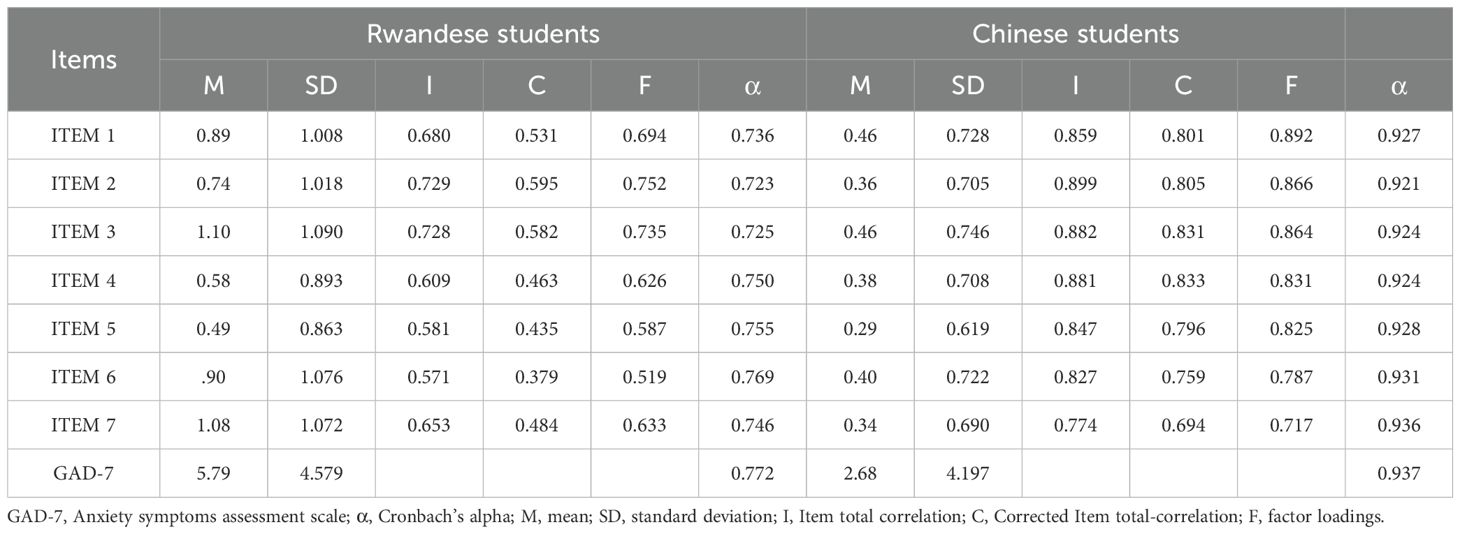
Table 2. GAD-7 reliability and item correlation coefficients.
Measurement invariance of the GAD-7
Single-group Confirmatory Factor Analysis
Single-group CFA was conducted to assess the fit of the original one-factor model. The Rwandese group showed acceptable model fit indices (CFI = 0.940, RMSEA = 0.08, SRMR = 0.041), while the Chinese group exhibited excellent CFI and SRMR values but a poor RMSEA (0.102). Modification indices suggested correlations between the intercepts of items 2 (“not being able to stop or control worrying”) and 3 (“worrying too much about different things”), items 3 and 4 (“trouble relaxing”), and items 4 and 5 (“being so restress that it is hard to sit still”) in both samples. Accounting for these correlations significantly improved model fit (Δχ2 (3) 195.853, P<0.001; Table 3).
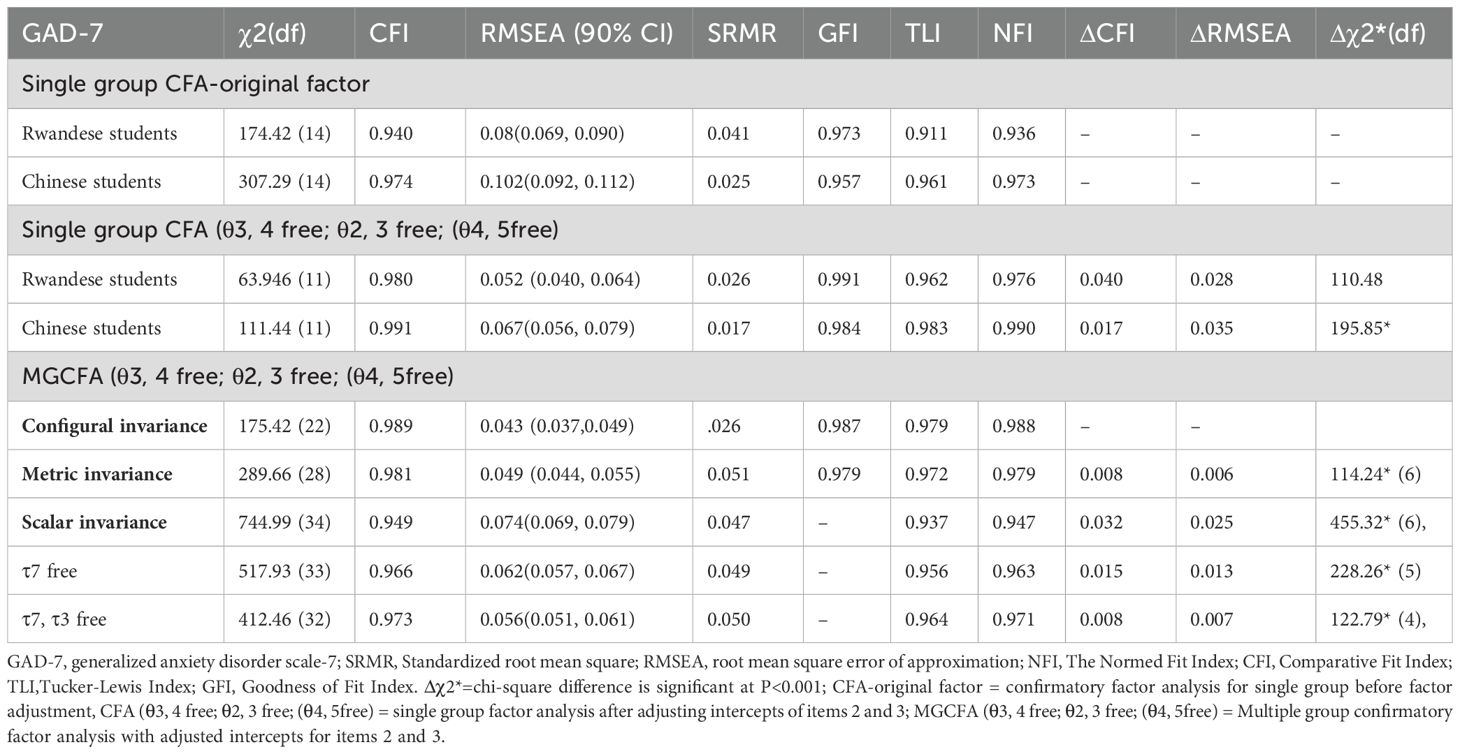
Table 3. Multiple group measurement invariance of GAD-7.
Measurement invariance across cultures (Multi-Group CFA)
Configural invariance was established with excellent global fit (CFI = 0.989, RMSEA = 0.043, SRMR = 0.026, GFI = 0.987, TLI = 0.979, NFI = 0.988). Metric invariance was also supported, with minimal changes in fit indices (ΔCFI= 0.008, ΔRMSEA= 0.006). However, scalar invariance was not confirmed due to a significant decrease in model fit (ΔCFI= 0.032, ΔRMSEA= 0.025). Modification indices indicate high intercepts for items 7 (“feeling afraid, as if something awful might happen”) and 3 (“excessive worrying”). Freely estimating these intercepts improved model fit (ΔCFI= 0.008, ΔRMSEA= 0.007), confirming partial invariance (Figure 5). The change in Comparative Fit Index (ΔCFI) and ΔRMSEA parameters followed Cheung’s recommendations suggesting that a ΔCFI < 0.01 and ΔRMSEA < 0.015 (25) indicating a non-significant deterioration of the model fit sustaining invariance. The ΔCFI and ΔRMSEA scores for configural and metric invariance in this study were within these ranges, indicating that the GAD-7’s factor loadings and structure are comparable for Chinese and Rwandan adolescents, however at the scalar invariance level there were significant changes in fit indices.
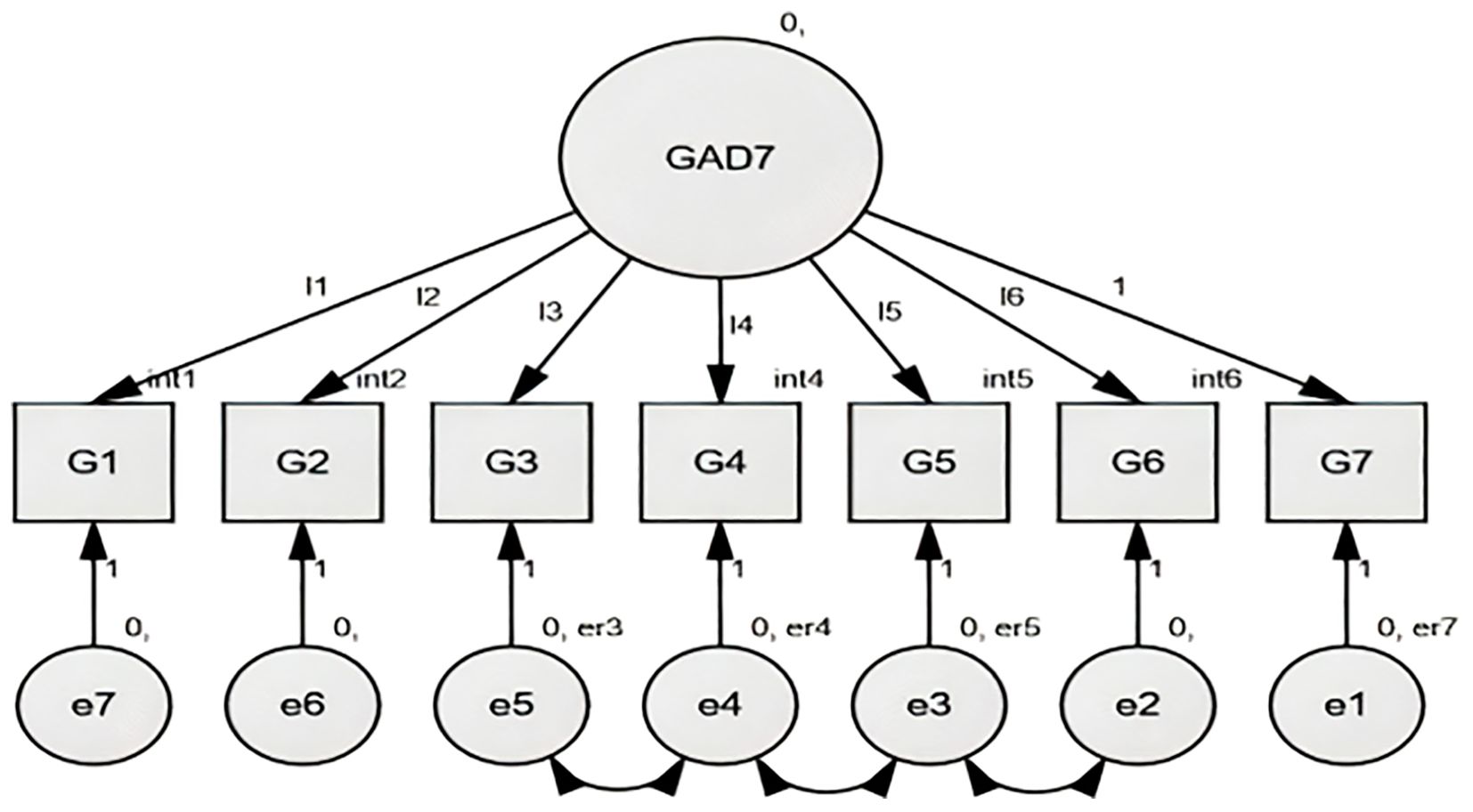
Figure 5. GAD-7 Factor structure Chinese and Rwandese adolescent students, the figure illustrates the factor loadings for each item of the GAD-7 in both cultural groups.
Latent mean comparison
Latent mean comparisons revealed a non-significant trend towards higher anxiety levels in Rwandan adolescents compared to Chinese adolescents (z= 0.02, d= 0.033, P = 0.98).
Discussion
This study evaluated the cross-cultural validity of the Generalized Anxiety Disorder-7 (GAD-7) scale among Chinese and Rwandan adolescents. While the GAD-7 demonstrated good psychometric properties and a consistent one-factor structure across both groups, only partial scalar invariance was achieved. This suggests that the GAD-7 is reliable for assessing anxiety symptoms within each cultural context but may not support direct comparisons of latent mean anxiety scores due to potential measurement biases influenced by cultural and linguistic factors.
The GAD-7 maintained a one-factor structure in both groups, indicating its ability to capture generalized anxiety similarly across these populations. However, cultural differences in the interpretation and expression of anxiety symptoms may affect the scale’s performance (27). For instance, the higher RMSEA values observed in the Chinese sample and the influence of cultural factors in Rwandan population highlight the variability in how anxiety is conceptualized and reported across cultures (28). The partial scalar invariance further underscores that while the GAD-7 can effectively detect anxiety symptoms, the severity of these symptoms may not be directly comparable between Chinese and Rwandan adolescents.
Notably, significant variations in item-level functioning were identified, particularly for items related to excessive worrying (“Worrying too much about different things”, item 3) and fear (“Feeling afraid, as if something awful might happen”, item 7), confirmatory factor analysis modification indices indicated that due to theoretical and cultural bases, these items exhibited differential item functioning (DIF) across both cultural groups implying variations in cultural interpretation, perception and expression of anxiety symptoms. For example, Rwandan adolescents may report higher levels of anxiety due to the integrational trauma and societal stressors associated with the country’s unique historical and sociocultural context, including the legacy of the 1994 genocide and ongoing socioeconomic challenges (29). In contrast, Chinese adolescents may express anxiety through somatic symptoms like headaches or physical tension, rather than emotional distress, reflecting cultural tendencies to avoid direct expressions of psychological vulnerability (19). Additionally, Chinese individuals with anxiety often exhibit shame-prone tendencies and concerns about social evaluations, which may further influence symptom reporting (30).
The contradiction between non-significant latent mean comparison analyses and significantly higher overt GAD-7 scores in Rwandan adolescents compared to the Chinese sample can be attributed to measurement bias stemming from partial scalar invariance which implicates DIF discussed above leading to inflated overt scores in one group without correspondence in the latent construct differences (19). Furthermore, it implies that this may not reflect true differences but rather cultural variations in anxiety expression, reporting and response patterns. For instance, linguistic differences in translating psychological scales can significantly alter meaning of items and impact response patterns (14, 31). In Rwanda, one of the primary languages, Kinyarwanda, may lack direct equivalent terms for words like “anxiety”, leading individuals to express emotional distress through physical discomfort (32, 33). Similarly, in China, the linguistic structure of Mandarin and cultural tendencies toward somatic expression may result in anxiety being reported through somatic symptoms such as fatigue, sleep disturbances, or chest pain (10, 34). These findings emphasize the importance of considering cultural and linguistic contexts when interpreting anxiety symptoms and designing culturally adapted assessment tools (23).
The lack of complete scalar invariance has important implications for cross-cultural mental health research and practice. Differences in item functioning and response patterns may lead to challenges in establishing universal cutoff scores and interpreting results across cultures. For instance, the same GAD-7 score might represent varying degrees of anxiety severity in different cultural settings due to differences in response patterns potentially leading to misdiagnosis or inappropriate treatment recommendations (13, 18). These findings highlight the need for culturally sensitive approaches to mental health assessment and the development of instruments that account for cultural variations in symptom expression to improve anxiety assessment accuracy and ensure that cutoff scores are culturally appropriate (16).
To improve mental health literacy and reduce stigma, education and healthcare systems must recognize somatic manifestations as potential indicators of underlying mental health issues. This study’s findings have several implications, first, healthcare professionals and educators should receive training in culturally sensitive approaches to mental health care, including the identification of culturally specific idioms of distress and the adaptation of assessment tools to local contexts. Translation efforts should prioritize contextual adaptability to ensure accurate symptom identification and conveyance; second, clinicians and researchers may need to adjust cutoff scores to provide culturally specific cut-off scores for the GAD-7, this can be addressed by adjusting setting a slightly cutoff score for populations where anxiety is expressed more for instance, also identifying culturally different items and adjusting the scoring weights by removing or modifying them. Finally, incorporate additional measures such as culturally adopted scales to enhance the accuracy of assessment in cross-cultural settings and provide a comprehensive understanding of anxiety in different populations. These measures may improve the cross-cultural validity of this assessment tool and ensure that patients receive appropriate health care.
While this study contributes valuable insights into the cross-cultural validity of the GAD-7, several limitations should be noted. First, the sample was drawn from a single city in each country, which may limit the generalizability of the findings and lead to regional biases due differing cultural and socioeconomic factors (3).While the samples were diverse within their respective cities they may fall short on capturing the broader picture of cultural and socioeconomic variations in both countries, thus future studies should include samples from multiple regions to enhance statistical power and external validity of the results and provide a more comprehensive understanding of anxiety symptoms across diverse populations. Second, the challenge of establishing full scalar invariance affects the interpretation and generalizability of the results. Finally, the reliance on self-report measures may introduce response biases, such as social desirability or cultural norms influencing symptom reporting. Incorporating objective measures, such as clinician-rated assessments or behavioral observations, could mitigate these biases in future research.
In conclusion, while the GAD-7 is a reliable tool for detecting anxiety symptoms within specific cultural contexts, its ability to support direct cross-cultural comparisons of symptom severity is limited by cultural and linguistic differences in symptom expression and interpretation. These findings underscore the need for culturally sensitive instruments and approaches in mental health assessment. Future research should explore the impact of cultural factors on symptom expression and measurement sensitivity, utilizing culturally adapted instruments and more diverse samples to advance cross-cultural mental health research and practice.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the College of Medicine and Health Sciences Institutional Review Board of the University of Rwanda (CMHS IRB) with research batch number 465/CMHS IRB/2022 and the ethics committee of the First Affiliated Hospital of Chongqing Medical University with research batch number (2020–879). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
LN: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. QZ: Data curation, Investigation, Project administration, Resources, Writing – review & editing. WW: Data curation, Investigation, Project administration, Resources, Writing – review & editing. D-DG: Methodology, Validation, Visualization, Writing – review & editing. H-YX: Formal analysis, Validation, Visualization, Writing – review & editing. J-HH: Data curation, Investigation, Resources, Validation, Writing – review & editing. LM: Investigation, Resources, Validation, Writing – review & editing. J-YT: Data curation, Investigation, Resources, Writing – review & editing. Y-TK: Data curation, Investigation, Resources, Writing – review & editing. SH: Conceptualization, Funding acquisition, Investigation, Project administration, Resources, Validation, Writing – review & editing. LK: Conceptualization, Funding acquisition, Resources, Supervision, Writing – review & editing, Project administration.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by the Nursing Research Fund of the First Affiliated Hospital of Chongqing Medical University (HLJJ2022-20), the First Affiliated Hospital of Chongqing Medical University “Discipline Peak Plan” scientific and technological achievement transformation project (cyyy-xkdfjh-cgzh-202304), Chongqing medical scientific research project (Joint Project of Chongqing Health Commission and Science and Technology Bureau) (2023MSXM111), Natural Science Foundation of Chongqing, China (CSTB2023NSCQ-MSX0340).
Acknowledgments
We would like to thank the school authorities, research participants from Chongqing and Kigali, and the University of Rwanda for their assistance in conducting the survey. Additionally, we would like to acknowledge and the Dr. Stefan Jansen, MSc, PhD, an associate professor in Neuroscience, the Director of Directorate of Research and Innovation at the College of Medicine and Health Sciences, University of Rwanda for his utmost help in overseeing the approval of the research project in Rwanda.
Conflict of interest
The authors state that the study was done without any commercial or financial links that could be seen as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Casey BJ, Jones RM, Hare TA. The adolescent brain. Ann N Y Acad Sci. (2008) 1124:111–26. doi: 10.1196/annals.1440.010
2. Bourdon KH, Goodman R, Rae DS, Simpson G, Brennan M. The development of a multidimensional scale of adolescent mental health. Psychol Assess. (2018) 30:797–808. doi: 10.1037/pas0000535
3. Polanczyk GV, Salum GA, Sugaya LS, Caye A, Rohde LA. Annual research review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J Child Psychol Psychiatry. (2015) 56:345–65. doi: 10.1111/jcpp.12381
4. Tiirikainen K, Haravuori H, Ranta K, Kaltiala-Heino R, Marttunen M. Psychometric properties of the 7-item Generalized Anxiety Disorder Scale (GAD-7) in a large representative sample of Finnish adolescents. Psychiatry Res. (2019) 272:30–5. doi: 10.1016/j.psychres.2018.12.004
5. Rwanda Biomedical Centre. Mental Health among Rwandan Youth: An Overview. KG 7 Ave, Kigali, Rwanda: Rwanda Biomedical Centre (2021). Available at: https://www.rbc.gov.rw/publichealth (Accessed November 20, 2024).
6. Zhang W, Chen S, Wu Z. Anxiety symptoms among Chinese adolescents: Prevalence, risk factors, and cultural considerations. J Adolesc Health. (2021) 68:678–85. doi: 10.1016/j.jadohealth.2020.10.005
7. Jorns-Presentati A, Napp AK, Dessauvagie AS, Stein DJ, Jonker D, Breet E, et al. The prevalence of mental health problems in sub-Saharan adolescents: A systematic review. PloS One. (2021) 16:e0251689. doi: 10.1371/journal.pone.0251689
8. Kuringe E, Materu J, Nyato D, Majani E, Ngeni F, Shao A, et al. Prevalence and correlates of depression and anxiety symptoms among out-of-school adolescent girls and young women in Tanzania: A cross-sectional study. PloS One. (2019) 14:e0221053. doi: 10.1371/journal.pone.0221053
9. Chang DF, Tong H, Shi Q, Zeng Q. Mental health stigma in China. J Soc Work. (2016) 16:332–48. doi: 10.1177/1468017314568993
10. Kirmayer LJ. Cultural variations in the clinical presentation of depression and anxiety: implications for diagnosis and treatment. J Clin Psychiatry. (2001) 62:3973.
11. Munyaneza R, Tsion T, Berhane Y. Prevalence of depression among adolescents in Rwanda: A population-based study. J Adolesc Health. (2021) 28:121–30. doi: 10.1016/j.jadohealth.2020.08.016
12. Tran TV. Developing Cross Cultural Measurement. Oxford, United Kingdom: Oxford University Press (2009). doi: 10.1093/acprof:oso/9780195325089.001.0001
13. Löwe B, Decker O, Müller S, Brähler E, Schellberg D, Herzog W, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. (2008) 46:266–74. doi: 10.1097/MLR.0b013e318160d093
14. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
15. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC, United States: American Psychiatric Association (2013). doi: 10.1176/appi.books.9780890425596
16. Sawaya H, Atoui M, Hamadeh A, Zeinoun P, Nahas Z. Adaptation and initial validation of the Patient Health Questionnaire - 9 (PHQ-9) and the Generalized Anxiety Disorder - 7 Questionnaire (GAD-7) in an Arabic speaking Lebanese psychiatric outpatient sample. Psychiatry Res. (2016) 239:245–52. doi: 10.1016/j.psychres.2016.03.030
17. Muñoz-Navarro R, Cano-Vindel A, Moriana JA, Medrano LA, Ruiz-Rodríguez P, Agüero-Gento L, et al. Screening for generalized anxiety disorder in Spanish primary care centers with the GAD-7. Psychiatry Res. (2017) 256:312–7. doi: 10.1016/j.psychres.2017.06.023
18. Kroenke K, Spitzer RL, Williams JBW, Monahan PO, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. (2007) 146:317–25. doi: 10.7326/0003-4819-146-5-200703060-00004
19. Zhou Y, Xu J, Rief W. Are comparisons of mental disorders between Chinese and German students possible? An examination of measurement invariance for the PHQ-15, PHQ-9 and GAD-7. BMC Psychiatry. (2020) 20. doi: 10.1186/s12888-020-02859-8
20. Teymoori A, Real R, Gorbunova A, Haghish EF, Andelic N, Wilson L, et al. Measurement invariance of assessments of depression (PHQ-9) and anxiety (GAD-7) across sex, strata and linguistic backgrounds in a European-wide sample of patients after Traumatic Brain Injury. J Affect Disord. (2020) 262:278–85. doi: 10.1016/j.jad.2019.10.035
21. Sun J, Liang K, Chi X, Chen S. Psychometric properties of the generalized anxiety disorder scale-7 item (GAD-7) in a large sample of Chinese adolescents. Healthcare (Switzerland). (2021) 9:1709. doi: 10.3390/healthcare9121709
22. Niwenahisemo LC, Hong S, Kuang L. Assessing anxiety symptom severity in Rwandese adolescents: cross-gender measurement invariance of GAD-7. Front Psychiatry. (2024) 15:1346267. doi: 10.3389/fpsyt.2024.1346267
23. Ip H, Suen YN, Hui CLM, Wong SMY, Chan SKW, Lee EHM, et al. Assessing anxiety among adolescents in Hong Kong: psychometric properties and validity of the Generalised Anxiety Disorder-7 (GAD-7) in an epidemiological community sample. BMC Psychiatry. (2022) 22. doi: 10.1186/s12888-022-04329-9
24. Dhira TA, Rahman MA, Sarker AR, Mehareen J. Validity and reliability of the Generalized Anxiety Disorder-7 (GAD-7) among university students of Bangladesh. PloS One. (2021) 16:e0261590. doi: 10.1371/journal.pone.0261590
25. Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct Equation Model. (2002) 9:233–55. doi: 10.1207/S15328007SEM0902_5
26. de Vaus D. Social Surveys. London, United Kingdom: SAGE Publications Ltd (2002). doi: 10.4135/9781446263495
27. Johnson SU, Ulvenes PG, Øktedalen T, Hoffart A. Psychometric properties of the GAD-7 in a heterogeneous psychiatric sample. Front Psychol. (2019) 10:1713. doi: 10.3389/fpsyg.2019.01713
28. Xie X, Yang Y, Li J. The psychometric properties of the Generalized Anxiety Disorder-7 (GAD-7) scale among Chinese adolescents. Psychiatry Res. (2016) 246:109–14. doi: 10.1016/j.psychres.2016.09.021
29. Suzuki LA, Ponterotto JG. Handbook of Multicultural Assessment: Clinical, Psychological, and Educational Applications. San Francisco, CA, United States: Jossey-Bass (2008).
30. Zhong J, Wang A, Qian M, Zhang L, Gao J, Yang J, et al. Shame, personality, and social anxiety symptoms in Chinese and American nonclinical samples: a cross-cultural study. Depress Anxiety. (2008) 25:449–60. doi: 10.1002/da.20358
31. Jaya ES, Novrianto R, Dewantary NI, Ticoalu CL, Riehle M. The universality of anxiety experiences between Germany, Indonesia, and the US: A measurement invariance analysis. J Affect Disord. (2024) 361:334–40. doi: 10.1016/j.jad.2024.06.046
32. Müller F, Hansen A, Kube M, Arnetz JE, Alshaarawy O, Achtyes ED, et al. Translation, cultural adaptation, and validation of the PHQ-9 and GAD-7 in KinyaRwanda for primary care in the United States. PloS One. (2024) 19. doi: 10.1371/journal.pone.0302953
33. Uwihoreye C, Uwimbabazi LF, Zivugukuri JMV, Mukeshimana V. Healing in Rwanda, understanding and naming mental health problems: translating kinyaRwanda into a clinically applicable language. J Psychol Res. (2021) 11:133–40. doi: 10.17265/2159-5542/2021.03.001
Keywords: generalized anxiety disorder-7 (GAD), GAD-7 scale, cultural differences, adolescent mental health, measurement invariance, cross-cultural comparison, psychometric validation [LN1]
Citation: Niwenahisemo LC, Zhang Q, Wang W, Geng D-d, Xu H-y, Hu J-h, Ma L-l, Tan J-y, Kong Y-t, Hong S and Kuang L (2025) A comparative study of anxiety symptoms in Chinese and Rwandan adolescents: a cross-cultural measurement invariance study of the GAD-7 scale. Front. Psychiatry 16:1571753. doi: 10.3389/fpsyt.2025.1571753
Received: 06 February 2025; Accepted: 07 April 2025;
Published: 09 May 2025.
Edited by:
Yifeng Wei, University of Alberta, CanadaReviewed by:
Jiansong Zhou, Central South University, ChinaLixia Wang, The First Affiliated Hospital of Dali University, China
Copyright © 2025 Niwenahisemo, Zhang, Wang, Geng, Xu, Hu, Ma, Tan, Kong, Hong and Kuang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Su Hong, aG9uZ3N1QGhvc3BpdGFsLmNxbXUuZWR1LmNu; Li Kuang, a3VhbmdsaTAzMDhAMTYzLmNvbQ==
†ORCID: Aleksandra Wieczorek, orcid.org/0000-0003-2294-5251