 Adolfo Piñón-Blanco1,2,3
Adolfo Piñón-Blanco1,2,3 Sonia Rodrigues4
Sonia Rodrigues4 Joana Teixeira5Catia Coutinho6Isabela Faria6Ilda Murta6Ana Isabel Tavares6
Joana Teixeira5Catia Coutinho6Isabela Faria6Ilda Murta6Ana Isabel Tavares6 Luis Iglesias-Rejas1,2,3Indalecio Carrera-Machado2,7
Luis Iglesias-Rejas1,2,3Indalecio Carrera-Machado2,7 Alejandro Garcia-Caballero3,8Olga Gutiérrez-Martínez9
Alejandro Garcia-Caballero3,8Olga Gutiérrez-Martínez9 Francisco Otero-Lamas1,2,3
Francisco Otero-Lamas1,2,3 Carlos Spuch2,3,10*
Carlos Spuch2,3,10*- 1Drug Dependency Assistance Unit of the City, Council of Vigo, CEDRO, Vigo, Spain
- 2RD24/0003/0024 Group, Red de investigación de atención primaria en adicciones (RIAPAD), Barcelona, Spain
- 3Translational Neuroscience Group, Galicia Sur Health Research Institute (IIS Galicia Sur), SERGAS-UVIGO, University of Vigo, Vigo, Spain
- 4Integrated Response Center, CRI of Porto Ocidental, Institute for Addictive Behaviours and Dependencies, I.P. (ICAD.IP), Porto, Portugal
- 5ULS de São José, Centro Clínico Académico de Lisboa, Faculdade de Medicina da Universidade de Lisboa, Unidade de Alcoologia do Hospital Júlio de Matos, Lisboa, Portugal
- 6Unidade Local de Saúde de Coimbra, Coimbra, Portugal
- 7Research Department, Citizens’ Association for the Fight Against Drugs (ACLAD), A Coruña, Spain
- 8Schizophrenia Unit, Ourense University Hospital Complex Day Hospital, Ourense, Spain
- 9Psychiatric Service, Vigo University Hospital Complex, Vigo, Spain
- 10GCV17/SAM1 Group, CIBERSAM, Madrid, Spain
Introduction: Substance use disorders are associated with impairments in various neuropsychological functions. We evaluated potential alterations in social cognition and differences between men and women in individuals with substance use disorders undergoing treatment at Addiction and Dependency Intervention Centers in Portugal.
Methods: The assessment utilized the Ekman 60 Faces Test (EFT), Interpersonal Reactivity Index (IRI), Hinting Task, and Ambiguous Intentions Hostility Questionnaire (AIHQ).
Results: Results showed that 70.2% of participants exhibited social cognition impairments (50% of women and 79.5% of men). Compared to non-clinical populations, individuals with social cognition impairments displayed significant differences in recognizing emotions such as happiness, fear, sadness, disgust, anger, and in the total EFT score. Differences were also observed in the fantasy and personal distress dimensions of the IRI, as well as in hostility, intentionality, and aggression biases on the AIHQ. Slight differences were found between men and women, but were not statistically significant.
Discussion: We discuss the clinical relevance of social cognition alterations and their potential utility in improving diagnostic and therapeutic processes for individuals with substance use disorders.
Introduction
Substance Use Disorders (SUD) are an increasing challenge for healthcare systems worldwide, driven by, among other factors, the high number of individuals using drugs within a context of expansive production, market growth, and accessibility. It is estimated that over 290 million people used drugs in 2022, a 20% increase compared to the previous decade. Approximately 64 million individuals suffer from SUD, yet only 1 in 11 people receive treatment, 1 in 18 among women compared to 1 in 7 among men (1). Furthermore, the multifactorial etiopathogenesis of SUD complicates the development of improved preventive and therapeutic strategies. Despite advances in understanding the biological, psychological, and social mechanisms underlying the disorders (2, 3), the translation of this knowledge into clinical practice remains limited.
From a neurobiological and neuropsychological perspective, one widely studied area of interest is the impairment of cognitive and executive functions in individuals with SUD, including their cause-effect relationships, role in the disease progression, and impact on treatment efficacy. It is well-established that neurocognitive alterations associated with drug use involve both prefrontal and hippocampal cognitive domains. A substantial body of evidence consistently links these impairments to premature treatment dropout, clinical outcomes, and relapse rates (4–9).
Additionally, research on enhancing cognitive functions as an adjunct strategy in treating individuals with SUS has shown positive results. These improvements are observed not only in cognitive variables but also in several clinical parameters related to treatment effectiveness (10–12).
In this context, the study of social cognition (SC) has recently gained prominence. SC is a complex, multifactorial construct referring to the ability to build representations of relationships between oneself and others and to use these representations flexibly to guide social behavior (13). It encompasses the set of cognitive processes used to decode and encode the social world (14) or that are activated in social interaction contexts (15). The components of SC remain a topic of debate, but from a clinical perspective, five subdomains have been proposed as particularly relevant: theory of mind (ToM), social perception, social knowledge, attributional biases, and emotional processing (16).
While most clinical research in this field has primarily focused on schizophrenia and autism spectrum disorders, the inclusion of SC as a primary domain in the RDoC framework (17) and its designation as one of the six domains of cognitive function in the DSM-5 (18) have renewed and expanded interest in studying SC across mental disorders. Additionally, it is known that male and female brains exhibit neurofunctional differences in various aspects of SC, such as face processing, facial expression recognition, response to infant schema, the ability to perceive faces in objects, processing of social interactions, empathy for others’ pain, interest in social information, processing of gestures and actions, biological motion, and erotic and affective stimuli (19). Thus, it is essential to deepen our understanding of gender differences in SC.
Most studies on SC in patients with SUD have been conducted in the context of alcohol (20, 21) and stimulants (22–24). However, there is also evidence related to cannabis (25, 26), opioids (27), steroids (28), and polydrug use (29–32), as well as, on the bidirectional relationship between SC and the risk of developing SUD, especially in youth populations (33). Although scientific literature consistently highlights the presence of SC impairments in individuals with SUD and their potential clinical relevance (34, 35), the diagnostic and therapeutic procedures commonly employed for treating these patients often do not incorporate specific resources to address SC.
The main objective of this study was to assess the presence of impairments in SC, including emotion recognition, empathy, theory of mind, and attributional style, in a clinical sample of individuals with SUD undergoing treatment, and to investigate potential gender differences.
Based on this, the following hypotheses were formulated:
Primary hypothesis: Most individuals with SUD will exhibit clinical impairment in at least one subdomain of social cognition, with particular emphasis on emotion recognition and empathy.
Secondary hypothesis: Males with SUD will show greater deficits in social cognition than females, particularly in facial emotion recognition and empathic responses.
Exploratory hypothesis: Individuals with impaired SC will have significantly different scores in attributional biases and theory of mind compared to normative values from the non-clinical population.
Materials and methods
Study design
This was a multicenter, cross-sectional, prospective study with neuropsychological measures. It was conducted between June and December 2022 at Addiction and Dependency Intervention Centers in Portugal: Integrated Response Center of Western Porto, Therapeutic Team of Matosinhos, University Hospital Center of Coimbra, and Lisbon Psychiatric Hospital Center. Clinical trial: NCT06363331.
Participants
A total of 57 individuals were recruited from the Addiction and Dependency Intervention Centers in Portugal based on the following criteria:
Inclusion Criteria:
● Diagnosis of SUD according to the DSM-5 (36).
● Age 18 or older.
● Capacity to consent (competence).
● Ability to read and write.
● Read the project’s information sheet and sign the informed consent form.
Exclusion Criteria:
● Diagnosis of intellectual disability (IQ < 70).
● Moderate or severe neurological damage.
● Presence of an acute psychiatric condition.
● Abstinence period of fewer than 15 days.
Participant selection
Participants were selected through convenience sampling, using a consecutive sampling method of patients undergoing treatment as they were admitted to these care facilities.
During a follow-up therapy session, participants were informed about the study characteristics and voluntarily agreed to participate by signing the informed consent form. This research, approved by the ARS Norte Research Ethics Committee, guaranteed: The participant’s right to withdraw from the study at any time without penalty and complete confidentiality of all collected data.
Sample size determination
The sample size calculation was based on standard statistical parameters for comparative studies between two independent groups. Considering a statistical power of 80% (1 - β = 0.80), a significance level of 5% (α = 0.05, two-tailed), and a large effect size (Cohen’s d = 0.8), the minimum required sample size would be 52 participants (26 per group), according to estimates generated by G*Power software (version 3.1).
Therefore, the final sample of 57 participants was deemed sufficient to detect large effects with adequate statistical power. However, to detect medium (d = 0.5) or small (d = 0.2) effects, approximately 128 and 394 participants would be required, respectively, which exceeds the sample size obtained in this study.
Instruments
A sociodemographic data collection questionnaire and a battery of neuropsychological tests were administered. Table 1 lists the tests used and the SC subdomains evaluated.
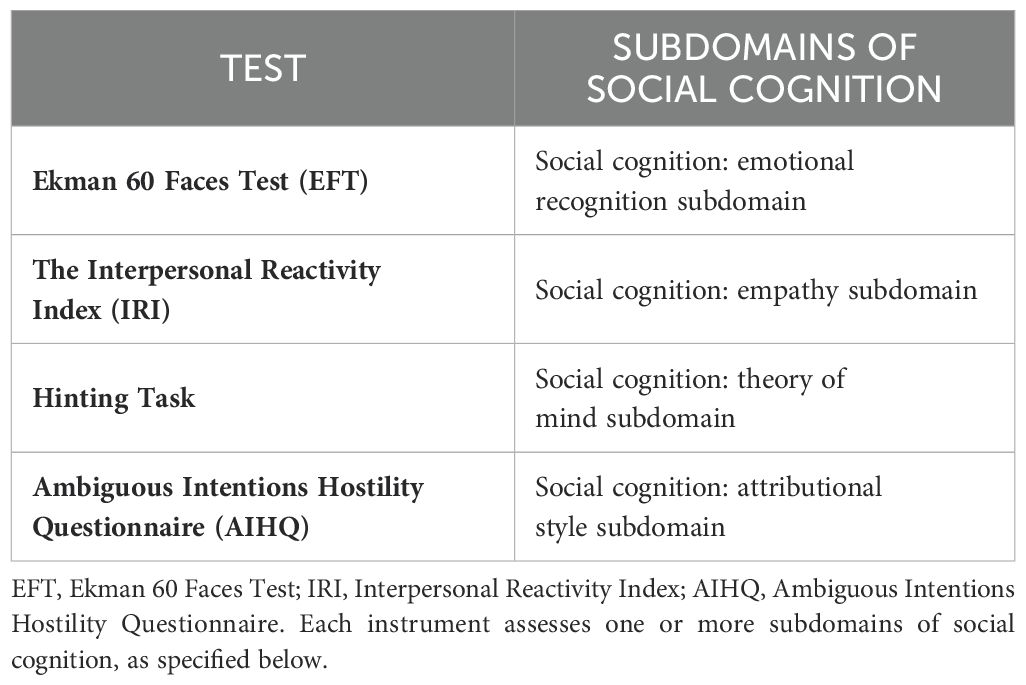
Table 1. Instruments used for assessing social cognition subdomains.
Ekman 60 Faces Test (EFT) (37): This test includes 60 photographs of faces displaying expressions of six basic emotions: anger, disgust, sadness, fear, surprise, and happiness. A general score of 60 indicates the best possible performance, with each basic emotion having a maximum score of 10 points.
The Interpersonal Reactivity Index (IRI) (38, 39): A Likert scale that evaluates four dimensions of empathy:
● Fantasy (F): The tendency to identify with fictional characters.
● Perspective Taking (PT): The ability to adopt others’ points of view.
● Empathic Concern (EC): Sympathy and concern for others’ suffering.
● Personal Distress (PD): Feelings of discomfort when witnessing others in distress.
Hinting Task (40): This test evaluates the ability to infer the true intention behind hints expressed in ten short stories involving two characters. Participants are asked what the character in the story meant to convey. The ability to infer the underlying, true intention of these indirect language uses involves employing Theory of Mind (ToM).
Ambiguous Intentions Hostility Questionnaire (AIHQ) (41, 42): This test assesses attributional biases through various vignettes that describe situations where the intentions of characters are ambiguous, intentional, or accidental. Participants are asked to rate on a Likert scale:
● AIHQ-HB: Hostility bias—why they think the protagonist acted this way.
● AIHQ-IS: Intentionality bias—whether the action was deliberate.
● AIHQ-BS: Blame bias—how much they blame the protagonist.
● AIHQ-AS: Anger bias—how angry the situation makes them feel.
● AIHQ-AB: Aggressiveness bias—how they would respond to the situation.
Higher scores reflect more hostile, negative, personal, and aggressive attributions.
Procedure
Sociodemographic and clinical variables were obtained from the center’s database. Neuropsychological tests were administered according to the application and scoring guidelines in their respective manuals. Testing was conducted over two 45-minute sessions under similar conditions.
All study participants have a DSM-5 diagnosis of SUD (Substance Use Disorder) confirmed by addiction specialists from the Portuguese ICAD (Intervention in Addictive Behaviors and Dependencies). The diagnostic assessments were conducted at specialized Addiction Intervention and Dependency Treatment Centers in Portugal (Porto, Coimbra, and Lisbon).
All recruited participants underwent clinical assessment and initial SC screening through emotional recognition and empathy evaluations. SC impairment was determined using the following criteria:
Inclusion criteria for social cognition impairment
The impairment criterion required either:
● A score below 42 on emotional recognition (EFT), and/or
● Scores more than 1 standard deviation below the mean in any of the four empathy dimensions (Fantasy, Perspective-Taking, Empathic Concern, or Personal Distress).
Assessment methodology
The SC impairment criteria used for the EFT (37) and IRI (39) were based on scoring ranges derived from healthy populations. For the IRI specifically, we used normative data from the Portuguese adaptation of the test.
Participants identified as having SC impairment according to screening criteria also underwent evaluations of ToM and attributional style subdomains.
Administration protocol
Trained psychologists conducted all test administrations and scoring procedures following standardized instructions validated for the Portuguese population.
Figure 1 illustrates the evaluation procedure performed at each study phase and the participants involved in each phase.
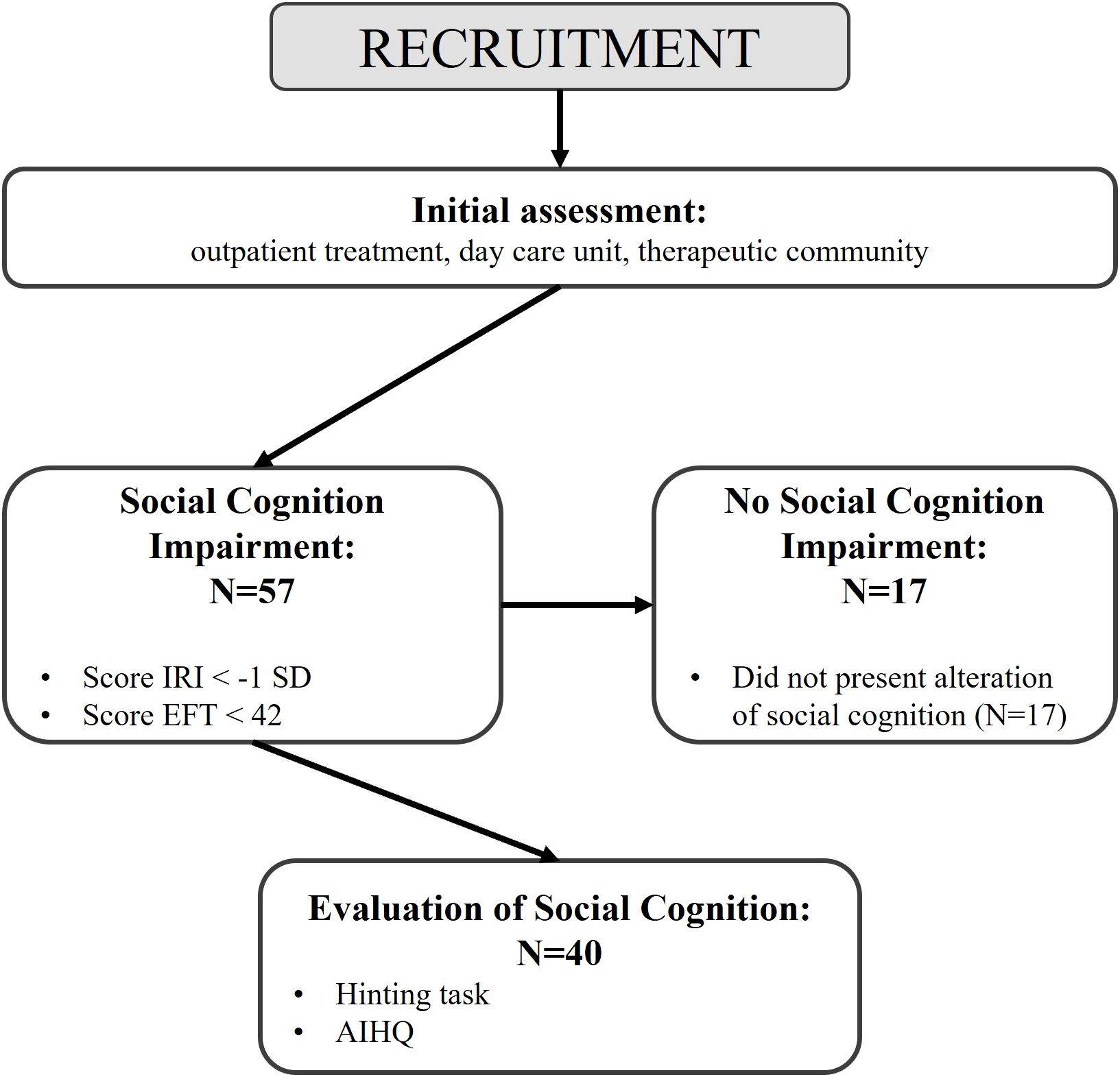
Figure 1. Flowchart of protocol.
Data analysis
A descriptive analysis was performed for all variables. For qualitative variables, absolute frequencies and their respective percentages were calculated. For quantitative variables, measures of central tendency (mean and standard deviation) were computed.
For variables with n<30, the Mann-Whitney U test was used to analyze potential differences between means of NSCI and SCI variables across each dimension of the EFT and IRI tests within female and male groups.
When the sample size exceeded 30, a one-sample t-test was applied to continuous variables (EFT, IRI, AIHQ, and HINTING TASK scores) to examine differences between normative values and obtained mean scores for each test.
Statistical analyses
An independent samples Student’s t-test was used to analyze potential significant differences between mean scores measured in z-scores by sex. For group comparisons (e.g., impaired vs. unimpaired SC; males vs. females), Mann-Whitney U tests and independent samples t-tests were used according to variable distribution, with a significance level set at 5% (p < 0.05). Comparisons between clinical sample scores and normative values from the non-clinical population were conducted using one-sample t-tests.
All analyses were conducted using IBM SPSS Statistics (version 29), with a significance level set at 0.05.
Results
We recruited 57 patients for the study; of all of them, 17 (29.8%) did not show SC impairment according to the initial screening criteria, while 40 (70.2%) exhibited some level of impairment. Regarding sex, a total of 18 women were recruited, of whom 50% (n=9) showed SC impairment. Among the 39 men, 79.5% (n=31) presented SC impairment. Table 2 displays the descriptive analysis of sociodemographic and clinical variables.
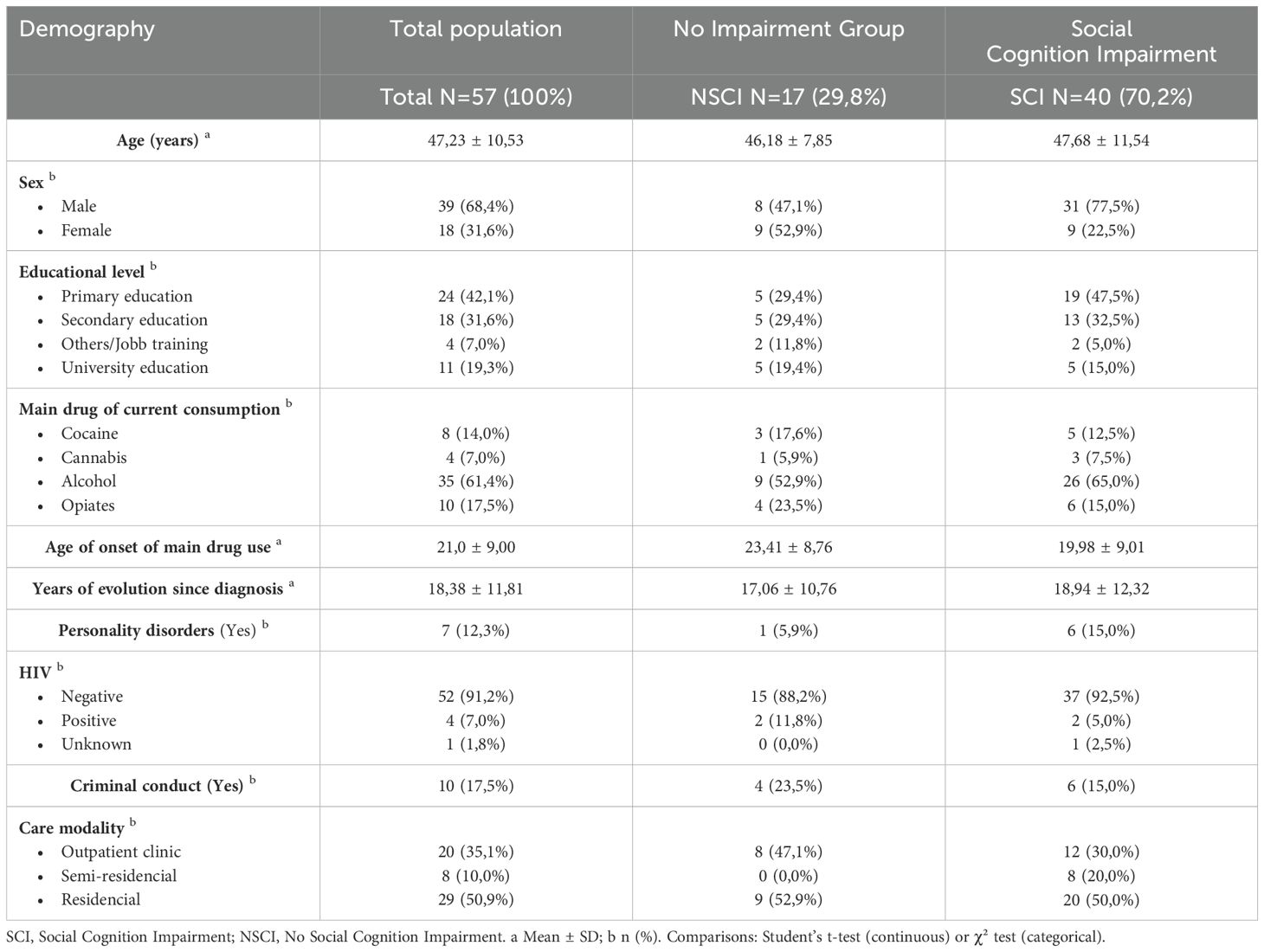
Table 2. Sociodemographic and clinical features: Total Sample and Social Cognition Impairment (SCI) vs. No Impairment (NSCI) groups.
The sample of patients with SC impairment consisted of 40 individuals with a mean age of 47.68 years, of whom 31 (77.5%) were men and 9 (22.5%) were women. The mean duration of diagnosis was 18.94 years.
Regarding the initial SC screening, in the group of women with SC impairment, statistically significant differences were found for the emotions of fear (p = 0.007), disgust (p = 0.030), and the total EFT-60 score (p = 0.006), as well as for the empathic concern dimension (p = 0.036) of the IRI, compared to women without SC impairment. In the group of males with SC impairment, statistically significant differences were observed for the emotions of fear (p = 0.030), sadness (p = 0.002), disgust (p = .002), and the total EFT score (p = .001), as well as, for the fantasy dimension (p = 0.041) of the IRI, compared to male without SC impairment. Table 3 shows the results of SC screening tests for all patients recruited in this study.
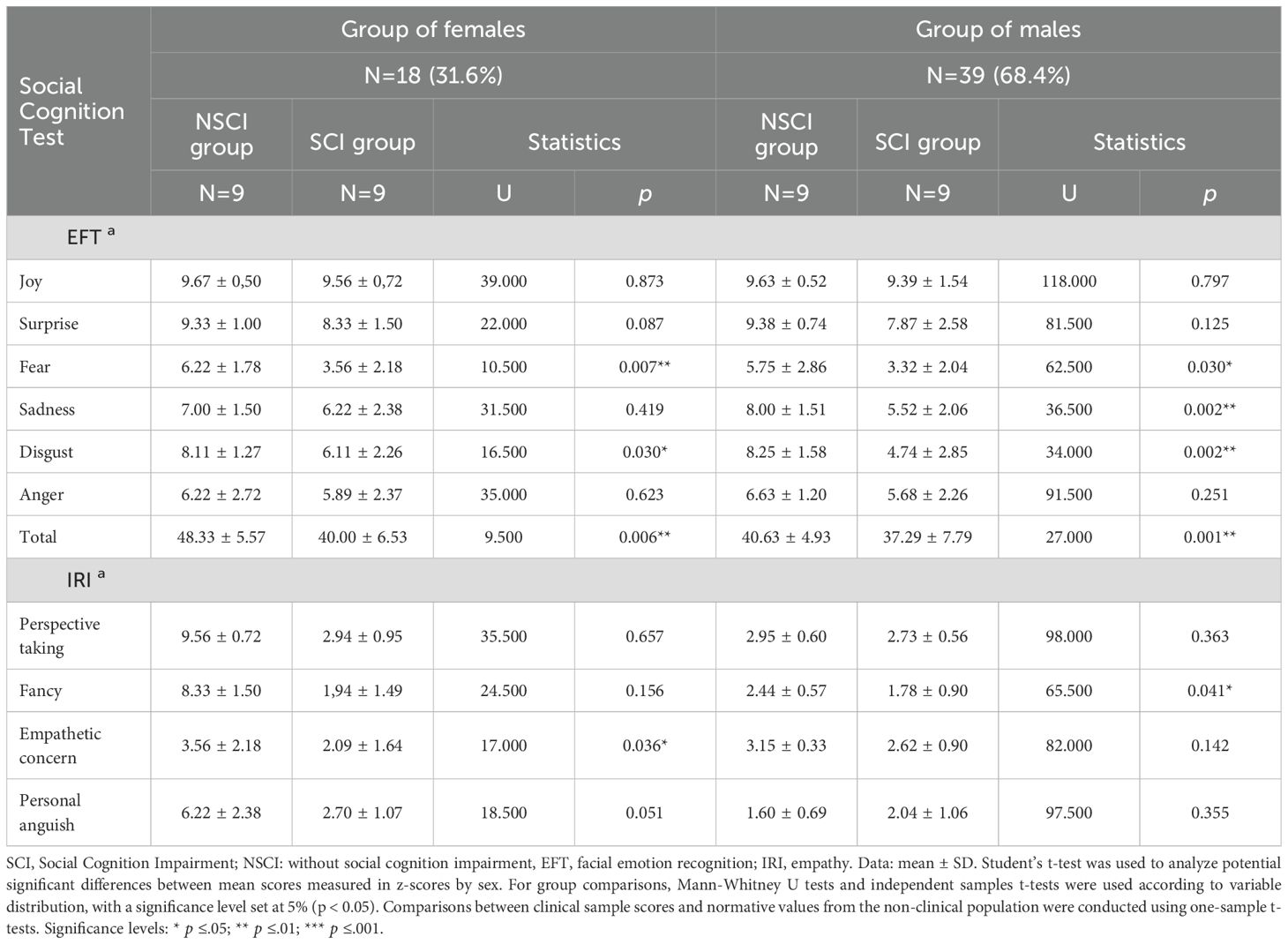
Table 3. Results of social cognition screening (EFT and IRI) in patients with and without Social Cognition Impairment (SCI), stratified by sex.
Compared to normative values in the non-clinical population, the group of patients with SC impairment showed statistically significant differences for the emotions of happiness (p = 0.05), fear (p < 0.001), sadness (p < 0.001), disgust (p < 0.001), anger (p < 0.001), and the total EFT score (p < 0.001). Differences were also significant for the fantasy (p = 0.002) and personal distress (p = 0.042) dimensions of the IRI, as well as for the hostility (p < 0.001), intentionality (p < 0.001), and aggressiveness (p < 0.001) biases of the AIHQ. No significant differences were found in the ToM assessment using the Hinting Task. Table 4 presents the analysis of scores for the group of patients with SC impairment compared to normative values in the non-clinical population.
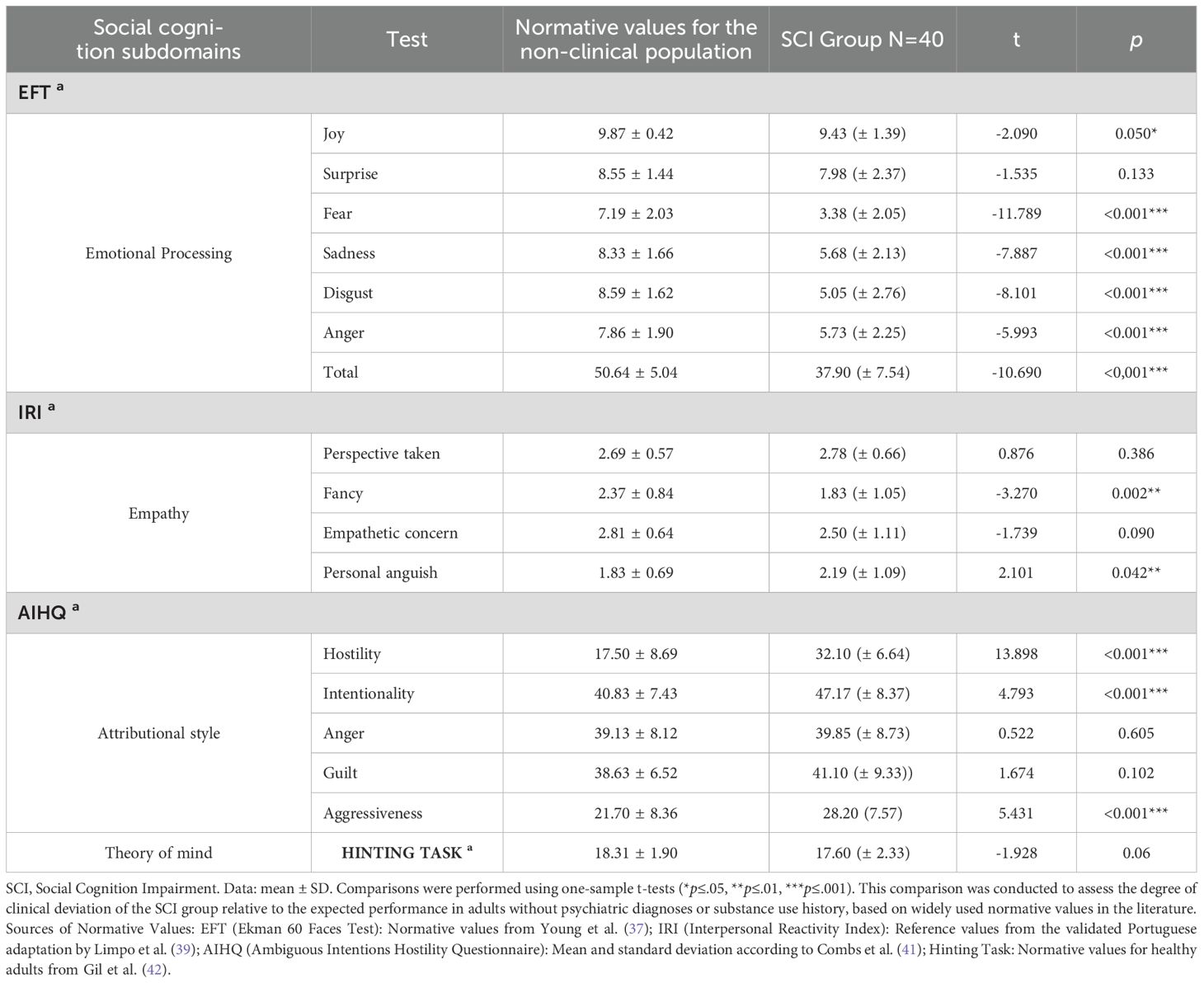
Table 4. Comparison of scores in the social cognition impairment group with normative values from the non-clinical population.
The analysis of the results in the SC domains assessed in this study, in the SCI group, reveals slight differences between men and women, which do not reach statistical significance:
Emotional recognition (EFT): Male scored lower than female in the recognition of happiness (M=-1.14; W=-0.73), surprise (M=-0.47; W=-0.15), fear (M=-1.90; W=-1.66), sadness (M=-1.69; W=-1.27), disgust (M=-2.37; W=-1.53), anger (M=-1.14; W=-1.03), and in the total score (M=-2.78; W=-1.87).
Empathy dimensions (IRI): Females scored lower in empathic concern (M=-0.29; W=-1.12) and higher in personal distress (M=+0.30; W=+1.26).
Attributional style biases (AIHQ): Females scored higher than males in hostility bias (M=+1.70; W=+1.57) and aggressiveness bias (M=+0.81; W=+0.66), while males scored higher in intentionality bias (M=+0.78; W=+1.08), anger bias (M=-0.07; W=+0.65), and blame bias (M=+0.26; W=+0.77).
Theory of Mind (Hinting Task): Males showed slightly lower performance than females (M=-0.46; W=-0.04).
Table 5 details the differences observed between males and females in the SC subdomains explored.
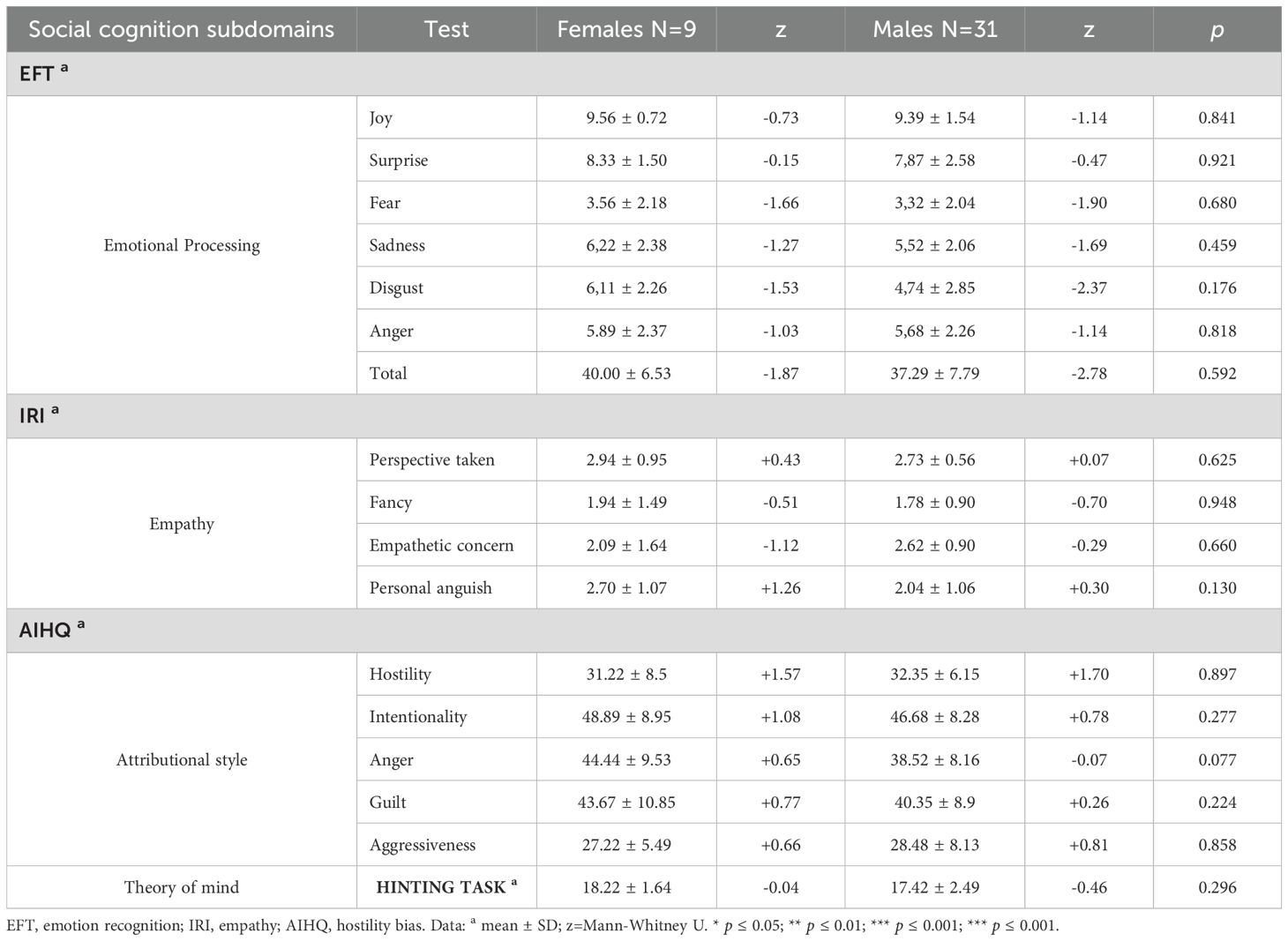
Table 5. Comparison between males and females with social cognition impairment across assessed subdomains.
Discussion
This study aimed to examine the presence of SC dysfunctions in a clinical sample of individuals with SUD by evaluating the subdomains most referenced in the literature—emotional recognition, empathy, theory of mind, and attributional style—and to assess potential differences between males and females.
To our knowledge, this study represents the first work conducted with a clinical sample of the Portuguese population with SUD that reports results on the evaluation of emotional recognition, empathy, attributional biases, theory of mind, comparisons with clinical and non-clinical populations, and differences between males and females.
Given that this study was carried out in a clinical care setting, we considered it appropriate to conduct an initial screening of the recruited population to exclude patients who did not show at least minimal SC impairments. For this purpose, we chose to assess emotional recognition, the most studied subdomain in clinical samples (43), and empathy, a multidimensional construct referring to the ability to share and understand others’ subjective experiences. Empathy includes aspects of emotional communication, self-awareness, and theory of mind (32, 44). Using the criteria of scoring below 42 in emotional recognition, as measured by the EFT, and/or scoring more than one standard deviation below the mean in cognitive and/or emotional empathy, as measured by the IRI, we found that 70.2% of the recruited patients exhibited some SC impairment.
This result aligns with clinical experience and existing knowledge about how SC impairments contribute to the frequent social dysfunctions observed in the daily lives of individuals with SUD. Such impairments also play a role in therapeutic relationships, potentially hindering treatment success (45). These findings support the importance of addressing SC deficits during the care process for these patients (46). It has been proposed that SC deficits may represent a central cognitive phenotype for many developmental, neurological, and psychiatric disorders, with potential utility as clinical markers and a need for effective transdiagnostic interventions (47).
In our study, SC impairments were more frequent among males (79.5%) than females (50%), consistent with other studies indicating better performance by women in emotional recognition and empathy, as discussed below.
One of the most studied subdomains of SC is emotional recognition (48). Numerous studies have reported emotional recognition deficits in individuals with SUD, and a meta-analysis has confirmed impaired emotional processing in these patients, particularly in facial emotion recognition (43). While it has been suggested that deficits in facial emotion recognition are associated with the quantity, duration, and severity of polysubstance use (31), other evidence points to these deficits as potential predisposing factors for developing SUD (49, 50).
Additionally, poor emotional recognition performance at the start of treatment has been identified as a significant predictor of relapse/dropout (51). For instance, recently detoxified alcohol-dependent patients have shown deficits in emotional recognition linked to a higher frequency of interpersonal conflicts (52). These types of deficits undermine not only the ability to navigate daily social interactions but also the capacity to successfully engage in treatment programs.
In our study, we observed that patients with SUD exhibited significant impairment in emotion recognition, specifically in identifying fear, sadness, disgust, anger, and happiness. Furthermore, differences in the total scores of the facial emotion recognition (EFT score) task indicate that these individuals fail to accurately recognize basic emotions through facial expressions. When comparing SUD patients with non-clinical populations, we aimed to highlight the association between the severity of drug use and alterations in specific cognitive domains, such as social cognition.
This study provides a descriptive analysis of the current condition of these patients, focusing on the differences between SDI and NSDI as well as SDI and healthy controls. These findings align with research from Monash University (Australia), which demonstrated significantly worse facial emotion recognition, particularly for anger, disgust, fear, and sadness, in polysubstance users compared to healthy controls (31). However, they differ from others that did not identify impaired recognition of facial expressions (27). Such discrepancies may be attributed to conceptual factors, methodological diversity, and ecological validity issues in the tools used (53). The available evidence does not yet allow for establishing specific indications for specific emotions, but it provides compelling arguments for further study into the clinical utility of systematically assessing emotional processing in patients with SUD and implementing specific therapies that could be more relevant in the case of men and for emotions such as fear, disgust, and sadness.
Regarding potential gender differences, we found that males performed slightly worse than females in recognizing joy, surprise, fear, sadness, disgust, anger, and in the total EFT score, consistent with previous studies (54–56). Additionally, females with SC impairment showed significant differences in the recognition of fear, disgust, and total EFT scores compared to females without SC impairment. Among males, these differences were observed for fear, sadness, disgust, and total EFT scores. These findings support the relevance of addressing emotional processing deficits as a potential strategy to improve SUD treatment outcomes (34).
When discussing the ToM, it refers to the ability to attribute mental states to oneself and others (57–59). This hetero metacognitive skill enables understanding and predicting others’ behavior, perceptions, knowledge, beliefs, goals, and intentions (60). ToM encompasses cognitive ToM (inferences about thoughts) and affective ToM (inferences about feelings). Various tests assess this complex construct, evaluating tasks such as understanding false beliefs, deception, white lies, jokes, metaphors, irony, hints, and faux pas (61). One of the most referenced tools in the literature is the hinting task, which examines the ability to infer intentions behind indirect speech (40, 42).
Numerous studies have reported ToM impairments across various conditions, including neurological and mental disorders such as autism spectrum disorders, schizophrenia, borderline personality disorder, post-traumatic stress disorder, depression, and eating disorders (62), as well as SUD (32, 63).
In our study, results from the hinting task were similar to those of non-clinical populations, indicating average performance. Previous research has identified ToM impairments in individuals with SUD using tools like the Movie for the Assessment of Social Cognition (MASC) (64) or the Reading the Mind in the Eyes Test (RMET) (65). A meta-analysis supports that drug users perform worse than healthy controls, with stronger evidence for ToM impairments in studies on alcohol and methamphetamine dependence, mixed findings for cocaine users, and no ToM impairments in recreational cannabis or cocaine users. However, the analysis highlights various biases that hinder generalizing these findings (32).
In terms of gender differences, males in our study performed slightly worse than females on the hinting task, consistent with a recent meta-analysis confirming better ToM performance in females (66).
Empathy, a multidimensional construct, can be defined as the processes and outcomes related to an individual’s responses to another’s experiences, encompassing cognitive and affective aspects (67, 68). Empathy involves the ability to adopt others’ perspectives, infer mental states, and share their cognitive and emotional experiences. It includes cognitive empathy (perspective-taking and fantasy) and affective empathy (empathic concern and personal distress) (38, 69). Brain injuries and psychiatric disorders such as antisocial, borderline, and narcissistic personality disorders, autism spectrum disorders, schizophrenia, and alexithymia are associated with empathy deficits or absence (44, 70). Evidence also points to empathy impairments in SUD patients and suggests that improving empathic behaviors can enhance treatment outcomes and reduce relapse risk (71, 72).
In our study, the IRI revealed slightly different results compared to non-clinical populations, with lower fantasy and higher personal distress in the SC impaired group, without significant gender differences across the four dimensions assessed. However, SC impaired females showed lower empathic concern than their unimpaired counterparts, while SC impaired males showed differences in the fantasy dimension. These findings align with reports of reduced empathic processes in individuals with SUD, including alcohol, opioid, cocaine, methamphetamine, and polysubstance users (34, 72, 73). While it is widely accepted that females exhibit higher empathy levels than males (72, 74), gender differences in clinical populations remain underexplored, and findings are contradictory (71, 75).
Attributional style refers to how individuals explain the causes of events or social interactions (76). Several models and theories have been proposed to explain attributional processes and their role in the pathogenesis and clinical features of mental disorders (77–80). Dimensions such as internality/externality, stability/instability, globality/specificity, consensus, distinctiveness, and consistency have been identified, and certain attributional biases have been linked to various clinical conditions. Although attributional style is understudied in SUD populations, evidence suggests that neuropsychological impairments and inappropriate explanatory styles are prognostic factors in treatment. Tailoring therapeutic interventions to recover these impaired functions and implementing specific rehabilitation strategies could enhance motivation, adherence, and reduce relapse risk (81).
The hostile attribution bias, defined as the tendency to interpret others’ behavior as having hostile intent, particularly in ambiguous social contexts (82), has been associated with interpersonal conflicts, paranoia, anxiety, mood disorders, and schizophrenia spectrum disorders (83). It has also been studied in severe alcohol use disorder patients (84). In our study, SC impaired patients scored higher in hostility, intentionality, and aggressiveness dimensions of the AIHQ compared to non-clinical norms. Regarding gender differences, males showed slightly higher hostility and aggressiveness scores, while females scored higher in intentionality, anger, and guilt.
Overall, the results of this study highlight the clinical relevance of SC impairments in SUD patients, given their frequency, complex implications for pathogenesis, progression, and therapeutic response, and their potential as a viable target for improving care processes. Neuroscience has provided deeper insights into the underlying causes of behavioral patterns in addiction disorders, emphasizing the role of brain mechanisms related to reward systems, learning, motivation, cognition, and executive functioning (85–88). From this perspective, SC emerges as another functional domain of interest for further research into SUD and its potential utility in enhancing therapeutic strategies.
Study limitations
Because our study focuses on characterizing social cognition functionality specifically in patients with SUD who present social cognition impairment (SCI), the findings cannot be generalized to all SUD patients except regarding: 1) The prevalence rate of SCI in this clinical sample and 2) Observed gender differences in SCI presentation.
This study has several limitations that should be considered. First, the relatively small sample size may restrict the statistical power and generalizability of the findings, potentially masking subtle effects or interactions. Second, the underrepresentation of women in the sample limits the ability to explore potential gender differences in social cognition, which have been reported in prior addiction research. Finally, the reliance on specific behavioral or self-report measures of social cognition (e.g., theory of mind or emotion recognition tasks) may not fully capture the complexity of real-world social functioning.
A key limitation stems from how the SCI group was operationally defined through specific cutoff scores on screening instruments (EFT and IRI). This approach identifies a pre-screened subgroup within the overall clinical sample and does not represent the full clinical diversity of SUD populations.
Limits external validity when extrapolating beyond this subgroup. The SCI group composition reflected operational criteria designed to detect SC deficits, which may overlook dimensional variations across social cognition domains and require validation through dimensional analyses across the full SUD sample and inclusion of matched control groups in future studies. Future studies with larger, more balanced cohorts and multimodal assessments (e.g., ecological paradigms, neuroimaging) could help address these constraints.
Conclusions
This study has replicated findings regarding impairments in SC subdomains related to emotional recognition, empathy, and attributional style in a heterogeneous clinical sample of individuals with SUD. These deficits have high clinical relevance, as they have been consistently linked to interpersonal problems, increased social stress, higher rates of treatment dropout, and relapses.
In the future, it would be crucial to consider the systematic evaluation of SC in diagnostic protocols for individuals with SUD, which would better identify the difficulties that interfere with the social functionality of these patients, help reduce early treatment dropout, and prevent relapses. Additionally, the clinical utility of SC is emphasized as an important prognostic variable to improve the personalization of the therapeutic process and rehabilitation.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Regional Health Administration of the North, Porto (Code: CE/2022/94). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
AP: Conceptualization, Supervision, Writing – original draft, Data curation, Formal Analysis, Investigation, Methodology. SR: Data curation, Investigation, Writing – original draft. JT: Data curation, Investigation, Writing – review & editing. CC: Data curation, Investigation, Writing – review & editing. IF: Data curation, Investigation, Writing – review & editing. IM: Data curation, Investigation, Writing – review & editing. AT: Data curation, Investigation, Writing – review & editing. LI: Software, Validation, Writing – review & editing. IC: Project administration, Resources, Writing – review & editing. AG: Funding acquisition, Resources, Visualization, Writing – review & editing. OG: Formal Analysis, Writing – review & editing. FO: Funding acquisition, Resources, Writing – review & editing. CS: Funding acquisition, Supervision, Resources, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study is funded by the Spanish grant of Plan Nacional Sobre Drogas, Ministerio de Sanidad y Consumo (PNSD 2023I086). RD24/0003/0024 funded by Instituto de Salud Carlos III (ISCIII), (RIAPAd), the European Regional Development Fund, and the Recovery, Transformation, and Resilience Plan. Also, by Axencia Galega de Innovación” grant number IN607B-2018/17, and IN607A-2024/06.
Acknowledgments
The authors would like to thank the collaboration of the professionals and patients from the addiction and dependency intervention centers in Portugal: Centro de Respostas Integradas de Porto Ocidental, ET de Matosinhos; Centro Hospitalario Universitario de Coimbra; and Centro Hospitalario Psiquiátrico de Lisboa, who made it possible to conduct this study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. UNODC. World Drug Report 2024 (United Nations publication 2024). (2024). Available at: https://www.unodc.org/unodc/en/data-and-analysis/world-drugreport-2024.html (Accessed May 13, 2023).
2. Compton WM, Wargo EM, and Volkow ND. Neuropsychiatric model of addiction simplified. Psychiatr Clinics North America. (2022) 45:321–34. doi: 10.1016/j.psc.2022.05.001
3. Volkow ND and Blanco C. Substance use disorders: A comprehensive update of classification, epidemiology, neurobiology, clinical aspects, treatment, and prevention. World Psychiatry. (2023) 22:203–29. doi: 10.1002/wps.21073
4. Boska GDA, Seabra PRC, Oliveira MAFD, Fernandes IFDAL, Claro HG, and Sequeira RMR. Consecuencias del consumo de sustancias psicoactivas: un estudio comparativo de dos servicios en brasil y portugal. Rev da Escola Enfermagem da USP. (2021) 55:e20210138. doi: 10.1590/1980-220X-REEUSP-2021-0138
5. Fernandez-Serrano MJ, Pérez-Garcia M, and Verdejo-Garcia A. What are the specific vs. generalized effects of drugs of abuse on neuropsychological performance? Neurosci Biobehav Rev. (2011) 35:377–406. doi: 10.1016/j.neubiorev.2010.04.008
6. Gamito P, Oliveira J, Lopes P, Brito R, Morais D, Silva D, et al. Executive functioning in alcoholics following an mHealth cognitive stimulation program: Randomized controlled trial. J Med Internet Res. (2014) 16:e102. doi: 10.2196/jmir.2923
7. Teixeira J, Pinheiro M, Gá P, Nogueira P, Guerreiro M, Castanho M, et al. Predicting alcohol relapse post-detoxification: The role of cognitive impairments in alcohol use disorder patients. Alcohol: Clin Exp Res. (2024) 48:918–27. doi: 10.1111/acer.15302
8. Vázquez-Justo E, Vergara-Moragues E, Blanco AP, Gestoso CG, and Pérez-García M. Neuropsychological functioning in methadone maintenance patients with HIV. Rev Latinoamericana Psicología. (2016) 48:147–58. doi: 10.1016/j.rlp.2015.06.008
9. Verdejo-García A, Orozco-Giménez C, Meersmans Sánchez-Jofré M, Aguilar de Arcos F, and Pérez-García M. Impacto de la gravedad del consumo de drogas de abuso sobre distintos componentes de la función ejecutiva. Rev Neurología. (2016) 38:1109–16. doi: 10.33588/rn.3812.2003592
10. Christensen E, Brydevall M, Albertella L, Samarawickrama SK, Yücel M, and Lee RSC. Neurocognitive predictors of addiction-related outcomes: A systematic review of longitudinal studies. Neurosci Biobehav Rev. (2023) 152:105295. doi: 10.1016/j.neubiorev.2023.105295
11. Nardo T, Batchelor J, Berry J, Francis H, Jafar D, and Borchard T. Cognitive remediation as an adjunct treatment for substance use disorders: A systematic review. Neuropsychol Rev. (2022) 32:161–91. doi: 10.1007/s11065-021-09506-3
12. Sampedro-Piquero P, Ladrón de Guevara-Miranda D, Pavón FJ, Serrano A, SuÁrez J, Rodríguez de Fonseca F, et al. Neuroplastic and cognitive impairment in substance use disorders: A therapeutic potential of cognitive stimulation. Neurosci Biobehav Rev. (2019) 106:23–48. doi: 10.1016/j.neubiorev.2018.11.015
13. Adolphs R. The neurobiology of social cognition. Curr Opin Neurobiol. (2001) 11:231–9. doi: 10.1016/s0959-4388(00)00202-6
14. Beer JS and Ochsner KN. Social cognition: a multilevel analysis. Brain Res. (2006) 1079:98–105. doi: 10.1016/j.brainres.2006.01.002
15. Tirapu-Ustárroz J. Cognición social en adicciones. Trastornos Adictivos. (2012) 14:3–9. Available online at: https://www.elsevier.es/es-revista-trastornos-adictivos-182-articulo-cognicionsocial-adicciones-X1575097312403162 (Accessed May 2, 2023).
16. Green MF, Penn DL, Bentall R, Carpenter WT, Gaebel W, Gur RC, et al. Social cognition in schizophrenia: An NIMH workshop on definitions, assessment, and research opportunities. Schizophr Bull. (2008) 34:1211–20. doi: 10.1093/schbul/sbm145
17. Gur RC and Gur RE. Social cognition as an RDoC domain. Am J Med Genet Part B Neuropsychiatr Genet. (2016) 171B:132–41. doi: 10.1002/ajmg.b.32394
18. Sachdev PS, Blacker D, Blazer DG, Ganguli M, Jeste DV, Paulsen JS, et al. Classifying neurocognitive disorders: The DSM-5 approach. Nat Rev Neurol. (2014) 10:634–42. doi: 10.1038/nrneurol.2014.181
19. Proverbio AM. Sex differences in the social brain and in social cognition. J Neurosci Res. (2023) 101:730–8. doi: 10.1002/jnr.24787
20. Bora E and Zorlu N. Social cognition in alcohol use disorder: a meta-analysis. Addiction. (2017) 112:40–8. doi: 10.1111/add.13486
21. Le Berre AP, Fama R, and Sullivan EV. Executive functions, memory, and social cognitive deficits and recovery in chronic alcoholism: A critical review to inform future research. Alcoholism Clin Exp Res. (2017) 41:1432–43. doi: 10.1111/acer.13431
22. Fernandez-Serrano M, Moreno L, Perez M, and Verdejo A. Inteligencia emocional en individuos dependientes de cocaina. Trastornos Adictivos. (2012) 14:27–33. doi: 10.1016/S1575-0973(12)70040-5
23. Kim YT, Kwon DH, and Chang Y. Impairments of facial emotion recognition and theory of mind in methamphetamine abusers. Psychiatry Res. (2011) 186:80–4. doi: 10.1016/j.psychres.2010.06.027
24. Kroll SL, Wunderli MD, Vonmoos M, Hulka LM, Preller KH, Bosch OG, et al. Socio-cognitive functioning in stimulant polysubstance users. Drug Alcohol Depend. (2018) 190:94–103. doi: 10.1016/j.drugalcdep.2018.06.001
25. Bayrakçı A, Sert E, Zorlu N, Erol A, Sarıçiçek A, and Mete L. Facial emotion recognition deficits in abstinent cannabis dependent patients. Compr Psychiatry. (2015) 58:160–4. doi: 10.1016/j.comppsych.2014.11.008
26. Roser P, Lissek S, Tegenthoff M, Nicolas V, Juckel G, and Brüne M. Alterations of theory of mind network activation in chronic cannabis users. Schizophr Res. (2012) 139:19–26. doi: 10.1016/j.schres.2012.05.020
27. Martin-Contero M, Secades-Villa R, and Tirapu-Ustarroz J. Cognicion social en adictos a opiaceos. Rev Neurologia. (2012) 55:705–12. doi: 10.33588/rn.5512.2012553
28. Kroll SL, Nikolic E, Bieri F, Soyka M, Baumgartner MR, and Quednow BB. Cognitive and socio-cognitive functioning of chronic non-medical prescription opioid users. Psychopharmacology. (2018) 235:3451–64. doi: 10.1007/s00213-018-5060-z
29. Hauger LE, Sagoe D, Vaskinn A, Arnevik EA, Leknes S, Jørstad ML, et al. Anabolic androgenic steroid dependence is associated with impaired emotion recognition. Psychopharmacology. (2019) 236:2667–76. doi: 10.1007/s00213-019-05239-7
30. Chicharro J, Pérez-García A, and Sanjuán P. Respuesta emocional en adictos a sustancias en tratamiento ambulatorio. Adicciones. (2011) 24:243–6. doi: 10.20882/adicciones.118
31. Fernandez-Serrano M, Lozano O, Perez-Garcia M, and Verdejo-Garcia A. Impact of severity of drug use on discrete emotions recognition in polysubstance abusers. Drug Alcohol Depend. (2010) 109(1-3):57–64. doi: 10.1016/j.drugalcdep.2009.12.007
32. Sanvicente-Vieira B, Romani-Sponchiado A, Kluwe-Schiavon B, Brietzke E, Araujo RB, and Grassi-Oliveira R. Theory of mind in substance users: A systematic minireview. Subst Use Misuse. (2017) 52:127–33. doi: 10.1080/10826084.2016.1212890
33. O’Brien JW and Hill SY. Neural predictors of substance use disorders in young adulthood. Psychiatry Res: Neuroimaging. (2017) 268:22–6. doi: 10.1016/j.pscychresns.2017.08.006
34. Le Berre AP. Emotional processing and social cognition in alcohol use disorder. Neuropsychology. (2019) 33:808–21. doi: 10.1037/neu0000572
35. Rodrigues S, Coutinho C, Amorim M, Cardoso S, Flora M, Tavares A, et al. Estudo do processamento emocional e da empatia de utentes com perturbações relacionadas com substâncias. Rev da Associação Portuguesa Adictologia. (2021). Available online at: https://adictologia.com/storage/files/papers/papers/RevistaADICTOLOGIAacbc3da9e9cf771d3ac01b080a9fa6f3.pdfpage=22 (Accessed June 3, 2023).
36. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Washington, DC: American Psychiatric Association (2013). doi: 10.1176/appi.books.9780890425596
37. Young AW, Perrett DI, Calder AJ, Sprengelmeyer R, and Ekman P. Facial expressions of emotion: Stimuli and test (FEEST). Bury St. Edmunds, UK: Thames Valley Test Company (2002).
38. Davis MH. Measuring individual differences in empathy: Evidence for a multidimensional approach. J Pers Soc Psychol. (1983) 44:113–26. doi: 10.1037/0022-3514.44.1.113
39. Limpo T, Alves RA, and Castro SL. Medir a empatia: Adaptação portuguesa do Índice de Reactividade Interpessoal. Laboratório Psicologia. (2010) 8:171–84. Available online at: http://hdl.handle.net/10400.12/3425 (Accessed June 3, 2023).
40. Corcoran R, Mercer G, and Frith CD. Schizophrenia, symptomatology and social inference: investigating “theory of mind” in people with schizophrenia. Schizophr Res. (1995) 17:5–13. doi: 10.1016/0920-9964(95)00024-g
41. Combs DR, Penn DL, Wicher M, and Waldheter E. The ambiguous intentions hostility questionnaire (AIHQ): a new measure for evaluating hostile social-cognitive biases in paranoia. Cognit Neuropsychiatry. (2007) 12:128–43. doi: 10.1080/13546800600787854
42. Gil D, Fernández-Modamio M, Bengochea R, and Arrieta M. Adaptación al español de la prueba de teoría de la mente Hinting Task [Adaptation of the Hinting Task theory of the mind test to Spanish. Rev Psiquiatría y Salud Ment. (2012) 5:79–88. doi: 10.1016/j.rpsm.2011.11.004
43. Castellano F, Bartoli F, Crocamo C, Gamba G, Tremolada M, Santambrogio J, et al. Facial emotion recognition in alcohol and substance use disorders: A metaanalysis. Neurosci Biobehav Rev. (2015) 59:147–54. doi: 10.1016/j.neubiorev.2015.11.001
44. Decety J and Moriguchi Y. The empathic brain and its dysfunction in psychiatric populations: Implications for intervention across different clinical conditions. BioPsychoSocial Med. (2007) 1:22. doi: 10.1186/1751-0759-1-22
45. Quednow B. Social cognition in addiction. In: Cognition and addiction. London, UK: Academic Press (2020). p. 63–78. doi: 10.1016/B978-0-12-815298-0.00005-8
46. Maurage P, Rolland B, Pitel AL, and D’Hondt F. Five challenges in implementing cognitive remediation for patients with substance use disorders in clinical settings. Neuropsychol Rev. (2024) 34:974–84. doi: 10.1007/s11065-023-09623-1
47. Cotter J, Granger K, Backx R, Hobbs M, Looi CY, and Barnett JH. Social cognitive dysfunction as a clinical marker: A systematic review of meta-analyses across 30 clinical conditions. Neurosci Biobehav Rev. (2018) 84:92–9. doi: 10.1016/j.neubiorev.2017.11.014
48. Fernández-Sotos P -, Torio I, Fernández-Caballero A, Navarro E, González P, Dompablo M, et al. Social cognition remediation interventions: A systematic mapping review. PloS One. (2019) 14:e0218720. doi: 10.1371/journal.pone.0218720
49. Ernst M, Luckenbaugh DA, Moolchan ET, Temple VA, Jenness J, Korelitz KE, et al. Decision-making and facial emotion recognition as predictors of substance-use initiation among adolescents. Addictive Behav. (2010) 35:286–9. doi: 10.1016/j.addbeh.2009.10.014
50. Rodrigo-Ruiz D, Perez-Gonzalez JC, and Cejudo J. Dificultades de reconocimiento emocional facial como déficit primario en niños con trastorno por déficit de atención/hiperactividad: revisión sistemática. Rev Neurología. (2017). Available online at: https://neurologia.com/articulo/2017041 (Accessed May 21, 2023).
51. Rupp CI, Derntl B, Osthaus F, Kemmler G, and Fleischhacker WW. Impact of social cognition on alcohol dependence treatment outcome: Poorer facial emotion recognition predicts relapse/dropout. Alcoholism: Clin Exp Res. (2017) 41:2197–206. doi: 10.1111/acer.13522
52. Kornreich C, Philippot P, Foisy ML, Blairy S, Raynaud E, Dan B, et al. Impaired emotional facial expression recognition is associated with interpersonal problems in alcoholism. Alcohol Alcoholism. (2002) 37:394–400. doi: 10.1093/alcalc/37.4.394
53. Pabst A, Gautier M, and Maurage P. Tasks and investigated components in social cognition research among adults with alcohol use disorder: A critical scoping review. Psychol Addictive Behav. (2022) 36:999–1011. doi: 10.1037/adb0000874
54. Abbruzzese L, Magnani N, Robertson IH, and Mancuso M. Age and gender differences in emotion recognition. Front Psychol. (2019) 10:2371. doi: 10.3389/fpsyg.2019.02371
55. Ersche KD, Hagan CC, Smith DG, Jones PS, Calder AJ, and Williams GB. In the face of threat: Neural and endocrine correlates of impaired facial emotion recognition in cocaine dependence. Trans Psychiatry. (2015) 5:e570. doi: 10.1038/tp.2015.5
56. Merten J. Culture, gender, and the recognition of the basic emotions. Psychologia. (2005) 48:306–16. doi: 10.2117/psysoc.2005.306
57. Call J and Tomasello M. Does the chimpanzee have a theory of mind? 30 years later. Trends Cognit Sci. (2008) 12:187–92. doi: 10.1016/j.tics.2008.02.010
58. Premack D and Woodruff G. Does the chimpanzee have a theory of mind? Behav Brain Sci. (1978) 1:515–26. doi: 10.1017/S0140525X00076512
59. Wimmer H and Perner J. Beliefs about beliefs: Representation and constraining function of wrong beliefs in young children’s understanding of deception. Cognition. (1983) 13:103–28. doi: 10.1016/0010-0277(83)90004-5
60. Tirapu-Ustárroz J, Pérez-Sayes G, Erekatxo-Bilbao M, and Pelegrín-Valero C. Qué es la teoría de la mente? [What is theory of mind]? Rev Neurología. (2007) 44:479–89. doi: 10.33588/rn.4408.2006295
61. Yeh YC, Lin CY, Li PC, Hung CF, Cheng CH, Kuo MH, et al. A systematic review of the current measures of theory of mind in adults with schizophrenia. Int J Environ Res Public Health. (2021) 18:7172. doi: 10.3390/ijerph18137172
62. Sprung M, Burghardt J, Mazza M, and Riffer F. Editorial: Misunderstanding others: Theory of mind in psychological disorders. Front Psychol. (2022) 13:838853. doi: 10.3389/fpsyg.2022.838853
63. Onuoha RC, Quintana DS, Lyvers M, and Guastella AJ. A meta-analysis of theory of mind in alcohol use disorders. Alcohol Alcoholism. (2016) 51:410–5. doi: 10.1093/alcalc/agv137
64. Maurage P, D’Hondt F, de Timary P, Mary C, Franck N, and Peyroux E. Dissociating affective and cognitive theory of mind in recently detoxified alcohol-dependent individuals. Alcoholism: Clin Exp Res. (2016) 40:1926–34. doi: 10.1111/acer.13155
65. Henry JD, Mazur M, and Rendell PG. Social-cognitive difficulties in former users of methamphetamine. Br J Clin Psychol. (2009) 48:323–7. doi: 10.1348/000712609X435742
66. Greenberg DM, Warrier V, Abu-Akel A, Allison C, Gajos KZ, Reinecke K, et al. Sex and age differences in “theory of mind” across 57 countries using the English version of the “Reading the Mind in the Eyes” Test. Proc Natl Acad Sci U.S.A. (2023) 120:e2022385119. doi: 10.1073/pnas.2022385119
67. Davis MH. Empathy: A Social Psychological Approach. Boulder, CO, USA: Westview Press (1996). doi: 10.4324/9780429493898
68. Fernandez-Pinto I, Lopez-Perez B, and Marquez M. Empatia: Medidas, teorias y Q30 aplicaciones en revision. Anales Psicologia. (2008) 24:284–98. Available online at: https://revistas.um.es/analesps/article/view/42831 (Accessed June 25, 2023).
69. Davis MH. A multidimensional approach to individual differences in empathy. Catalog Selected Documents Psychol. (1980) 10:1–17. Available online at: https://www.uv.es/~friasnav/Davis_1980.pdf (Accessed June 23, 2023).
70. Shamay-Tsoory SG, Tomer R, Goldsher D, Berger BD, and Aharon-Peretz J. Impairment in cognitive and affective empathy in patients with brain lesions: Anatomical and cognitive correlates. J Clin Exp Neuropsychol. (2004) 26:1113–27. doi: 10.1080/13803390490515531
71. Massey SH, Newmark RL, and Wakschlag LS. Explicating the role of empathic processes in substance use disorders: A conceptual framework and research agenda. Drug Alcohol Rev. (2018) 37:316–32. doi: 10.1111/dar.12548
72. Christov-Moore L, Simpson EA, Coudé G, Grigaityte K, Iacoboni M, and Ferrari PF. Empathy: gender effects in brain and behavior. Neurosci Biobehav Rev. (2014) 46:604–27. doi: 10.1016/j.neubiorev.2014.09.001
73. Cox SS and Reichel CM. The intersection of empathy and addiction. Pharmacol Biochem Behav. (2023) 222:173509. doi: 10.1016/j.pbb.2022.173509
74. Rochat MJ. Sex and gender differences in the development of empathy. J Neurosci Res. (2023) 101:718–29. doi: 10.1002/jnr.25009
75. Saracco-Álvarez R, Robles-García R, Flores-Medina Y, Olivares-Neumann JL, Tovilla-Zárate CA, Alcalá-Lozano R, et al. No sex-based differences in self-reported empathy between patients with schizophrenia and control subjects. Actas Españolas Psiquiatría. (2024) 52:670–7. doi: 10.62641/aep.v52i5.1784
76. Pinkham AE, Penn DL, Green MF, Buck B, Healey K, and Harvey PD. The social cognition psychometric evaluation study: Results of the expert survey and RAND panel. Schizophr Bull. (2014) 40:813–23. doi: 10.1093/schbul/sbt081
77. Abramson LY, Seligman ME, and Teasdale JD. Learned helplessness in humans: Critique and reformulation. J Abnormal Psychol. (1978) 87:49–74. doi: 10.1037/0021-843X.87.1.49
78. Heider F. Social perception and phenomenal causality. Psychol Rev. (1944) 51:358–74. doi: 10.1037/h0055425
79. Kelley HH. The processes of causal attribution. Am Psychol. (1973) 28:107–28. doi: 10.1037/h0034225
80. Weiner B, Nierenberg R, and Goldstein M. Social learning (locus of control) versus attributional (causal stability) interpretations of expectancy of success. J Pers. (1976) 44:52–68. doi: 10.1111/j.1467-6494.1976.tb00583.x
81. García AV, Torrecillas FL, de Arcos FA, and García MP. Effects of executive impairments on maladaptive explanatory styles in substance abusers: Clinical implications. Arch Clin Neuropsychol. (2005) 20:67–80. doi: 10.1016/j.acn.2004.03.002
82. Milich R and Dodge KA. Social information processing in child psychiatric populations. J Abnormal Child Psychol. (1984) 12:471–89. doi: 10.1007/BF00910660
83. Buck B, Browne J, Gagen EC, and Penn DL. Hostile attribution bias in schizophrenia-spectrum disorders: narrative review of the literature and persisting questions. J Ment Health. (2023) 32:132 49. doi: 10.1080/09638237.2020.1739240
84. Pabst A, Gautier M, and Maurage P. Hostile attributional biases in severe alcohol use disorder: Replication, gender specificity, and mechanistic insights. Alcohol Alcoholism. (2024) 59:agae010. doi: 10.1093/alcalc/agae010
85. Kalivas PW and Volkow ND. The neural basis of addiction: A pathology of motivation and choice. Am J Psychiatry. (2005) 162:1403–13. doi: 10.1176/appi.ajp.162.8.1403
86. Tirapu Ustárroz J, Landa N, and Lorea Conde I. Sobre las recaídas, la mentira y la falta de voluntad de los adictos [On the relapses, lies and lack of willpower of addicts. Adicciones. (2003) 15:7–16. doi: 10.20882/adicciones.442
87. Verdejo-García A, López-Torrecillas F, Giménez CO, and Pérez-García M. Clinical implications and methodological challenges in the study of the neuropsychological correlates of cannabis, stimulant, and opioid abuse. Neuropsychol Rev. (2004) 14:1–41. doi: 10.1023/b:nerv.0000026647.71528.83
Keywords: substance use disorders, social cognition, emotional recognition, empathy, theory of mind, attributional style
Citation: Piñón-Blanco A, Rodrigues S, Teixeira J, Coutinho C, Faria I, Murta I, Tavares AI, Iglesias-Rejas L, Carrera-Machado I, Garcia-Caballero A, Gutiérrez-Martínez O, Otero-Lamas F and Spuch C (2025) Impairment in social cognition in people with substance use disorders. Front. Psychiatry 16:1574483. doi: 10.3389/fpsyt.2025.1574483
Received: 20 February 2025; Accepted: 01 May 2025;
Published: 27 May 2025.
Edited by:
Marialaura Di Tella, University of Turin, ItalyReviewed by:
Alannah Miranda, University of California, San Diego, United StatesŞafak Yalçın Şahiner, Ankara University, Türkiye
Copyright © 2025 Piñón-Blanco, Rodrigues, Teixeira, Coutinho, Faria, Murta, Tavares, Iglesias-Rejas, Carrera-Machado, Garcia-Caballero, Gutiérrez-Martínez, Otero-Lamas and Spuch. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Spuch, Y2FybG9zLnNwdWNoQGlpc2dhbGljaWFzdXIuZXM=