 Szabolcs Fekete1,2
Szabolcs Fekete1,2 Hunor Girasek
Hunor Girasek Gabor S. Ungvari
Gabor S. Ungvari Gábor Gazdag
Gábor Gazdag- 1National Institute of Forensic Psychiatry, Budapest, Hungary
- 2Semmelweis University, Doctoral College, Budapest, Hungary
- 3Doctoral School of Psychology, ELTE Eötvös Loránd University, Budapest, Hungary
- 4Institute of Psychology, ELTE Eötvös Loránd University, Budapest, Hungary
- 5Department of Psychiatry and Psychiatric Rehabilitation, Jahn Ferenc South Pest Hospital, Budapest, Hungary
- 6Division of Psychiatry, School of Medicine, University of Western Australia, Crawley, WA, Australia
- 7Section of Psychiatry, University of Notre Dame, Fremantle, WA, Australia
- 8Department of Psychiatry and Psychotherapy, Faculty of Medicine, Semmelweis University, Budapest, Hungary
Introduction: In recent years, the length of stay (LoS) in forensic psychiatric inpatient institutions has been increasing worldwide. Although an excessive LoS constitutes a human rights violation, the underlying reasons and associated factors have not been fully established, and differences between countries and regions have led to limited conclusive information.
Methods: This retrospective study used data from a nationally representative sample of 301 adult patients who were admitted to the National Institute of Forensic Psychiatry, Hungary’s only forensic inpatient psychiatric institution, following a court-issued compulsory treatment order for reason of insanity during 2000–2015 to investigate the demographic, clinical, and criminal offense-related factors associated with inpatient LoS.
Results: Among the variables found to be significant in univariate analyses, a multiple regression model with bootstrapping confirmed significant associations of LoS with the type and method of the index criminal offense, community residential setting into which the patient was released, age and gender (all p < 0.05). However, the regression model accounted for only 34.1% of the observed variance in LoS, suggesting the presence of additional unexplored factors that may lead to excessive LoS.
Conclusion: The Hungarian forensic psychiatric system should implement a more evidence-based method for determining the LoS for inpatient care.
Introduction
The factors influencing the duration of inpatient treatment are among the most important recent research areas in forensic psychiatry (1). An excessive length of stay (LoS) in forensic psychiatric institutions constitutes a violation of human rights, places undue burden on forensic health care systems and incurs substantial costs (2–4). Recent decades have seen an increasing trend of forensic inpatient stays lasting for months or even years (5, 6), such that the duration of such an inpatient stay may be even longer than the duration of incarceration for offenders convicted on the same charges without a psychiatric diagnosis (3, 7). In some countries (e.g., Hungary), the legal framework allows an offender to receive inpatient treatment in forensic psychiatric institutions beyond the maximum length of a prison sentence. This scenario carries a risk of an excessive LoS in forensic institutions, which may violate fundamental human rights (7). In recent years, such LoS-related violations have led to increasing criticism of inpatient forensic psychiatric treatment (2, 8). Although the reasons for the increase in LoS are not yet clear, one probable factor is societal demand for strong and decisive measures against offenders with mental disorders to minimize their risk of re-offending (9).
To understand the increase in LoS, the associated demographic and clinical factors must first be identified when seeking an optimal therapeutic approach to reduce an unnecessarily long LoS and the rational use of financial resources (7, 9). The duration of forensic hospitalization differs significantly between countries and even between regions within a country due to significant geographic variations in treatment standards, the provision of inpatient forensic care services and the legal framework (2, 10, 11). In a study of 12 European countries, forensic inpatients were found to have an average LoS of less than 3.5 years in seven countries and more than 7 years in the others, and the between-country differences were large (1–10 years) (11). Furthermore, European countries use different definitions of criminal responsibility and mental illness (10, 11). In some countries (e.g., Republic of Ireland, Latvia, Lithuania), forensic psychiatric care is only available to patients with severe psychiatric disorders (e.g., psychotic disorders), while in others (e.g. Belgium, Germany, Italy, Poland, Serbia), patients with personality disorders can be admitted to inpatient forensic psychiatric institutions (9, 10). A comprehensive literature review found that the duration of forensic hospitalization is influenced mainly by the legal framework and broader socio-cultural environment (12).
The clinical and socio-demographic variables influencing LoS in inpatient forensic psychiatric settings can be classified as (a) personal demographics, including educational and vocational qualifications and work and family history; (b) clinical data, including medical conditions and mental health; and (c) criminal history (4).
Factors known to be associated with longer LoS include male gender (4, 13, 14), older age at admission (4, 15, 16), single marital status (4, 17, 18), lower education level (16–19), lower IQ (17), lack of housing at the time of discharge from forensic inpatient treatment (4, 15) and unemployment prior to the index admission (16–18, 20). However, some studies have concluded that sociodemographic variables have little or no effect on the LoS (1, 6, 8, 21).
Among clinical factors, diagnosis of a schizophrenia spectrum disorder was found to have the most significant impact on the LoS (1, 4, 6, 7, 13, 14, 22–26). Some studies have found that alcohol or substance abuse also may increase the LoS (24, 26), but other studies have found no or even the opposite effect (1, 8, 13, 23). Studies have also identified correlations between an increased LoS and the duration of mental illness (1), previous admission to a psychiatric institution (4) and a family history of psychiatric disorders (7).
Furthermore, most studies have concluded that the severity of the index crime leading to forensic inpatient admission is an important predictor of the LoS (2, 8): the more serious the index crime, the longer the stay (1, 14–19, 23, 24, 27, 28). Researchers have identified particularly strong correlations of a long LoS with committed/attempted homicide (6, 7) and other violent crimes (23–26). A long LoS has also been associated with crimes committed against known persons (17) or committed earlier in life (2, 29).
Only a few studies examined treatment or institutional behavior characteristics with respect to LoS (6). Factors associated with longer LoS include absconding from the institution during treatment (2, 4, 9), treatment-resistant psychotic symptoms (7), aggressive attacks against staff (2, 4), lack of cooperation, and lack of insight about mental illness (2).
The aims of this study were to identify the demographic, clinical and crime-related factors influencing the LoS. The patient sample comprised forensic psychiatric patients who had been found not guilty by reason of insanity and sentenced to receive compulsory treatment in the only forensic inpatient psychiatric facility in Hungary. According to the Hungarian Criminal Code (C/2012. Criminal Code), persons could be sentenced to compulsory forensic psychiatric treatment if (1) they committed a violent crime or caused a public danger, and (2) due to their pathological mental state they are not guilty by reason of insanity and there is a risk that they will commit a similar crime, and (3) if their crime is punishable for more than one year of imprisonment.
The institute, where these patients must serve their sentences is the National Institute of Forensic Psychiatry (NIFP), which is under the direction of the Minister of Internal Affairs, and its operation is supervised by the Hungarian Prison Service. This setting provided a unique opportunity to study a nationally representative sample of severely mentally ill offenders requiring admission. Relevant data from Hungary are limited, and this study would enable the establishment of a comprehensive national database.
Another aim of this study was to explore community reintegration pathways in the context of the LoS of forensic patients. In Hungary, and possibly elsewhere, the scarcity of social aftercare in the forensic psychiatric system is a major problem. However, this topic has not been extensively studied in any country.
Methods
Sample
The NIFP was established [1] to assess and treat psychiatrically ill offenders who were not found guilty of crimes by reason of insanity and [2] to provide short-term psychiatric treatment for prisoners who become mentally ill while serving their sentences. The NIFP is part of the Hungarian Prison Service and located within the premises of the Budapest Medium and Maximum Security Prison. It comprises three buildings with 311 beds across one acute psychiatric, one female and two male psychiatric rehabilitation units. All Hungarian offenders with severe mental illness who require admission are managed in one facility, providing a unique opportunity to establish a comprehensive database that covers the entire country.
This study focuses only on inpatients who were found not guilty by reason of insanity and underwent court-ordered treatment. In Hungary, the Court orders such offenders to undergo psychiatric treatment in lieu of a prison sentence for an indefinite period, followed by a case review every six months. The Court then decides whether to maintain or terminate treatment based on the opinion of the attending consultant psychiatrist or Chief of Service of the NIFP and an independent forensic psychiatric expert. The latter professional recommends discontinuation of inpatient treatment if the patients’ condition has sufficiently improved or their treatment adherence is sufficiently stable to enable a shift to outpatient treatment through public psychiatric services while living with their families or in supervised community residential settings. In Hungary, no forensic outpatient treatment is available. On the day when the court responsible for reviewing the necessity of compulsory forensic inpatient treatment decides about the discharge, patients must be released to the care of the public community psychiatric services while residing either at their homes or moving in to a community residential setting.
For this retrospective study, the medical records of all patients who received a court-issued compulsory treatment order for reason of insanity and were discharged from the NIFP between January 1, 2000 and December 31, 2015 were reviewed following a pilot project by two authors (GG and SF) to determine the scope of data extraction from notes based on an earlier local study (29). The following demographic data were collected: age, gender, residential and marital status, education level, pre-offense employment and number of children and guardianship. The following clinical variables were extracted: diagnoses according to the International Classification of Diseases, 10th Revision (ICD-10), family history of psychiatric disorders, history of alcohol and substance use, and alcohol and/or substance use immediately prior to committing the index criminal offense. The following index criminal offense variables were collected: type of offense, method of offense, relation to the victim, offense under the influence of alcohol or drugs, history of violence, recidivism in terms of offending, and/or forensic psychiatric treatment.
Sexual offenders can be treated in NIFP only if they are not guilty by reason of insanity. Otherwise they serve their sentence in prison in a separate unit. In our sample there were only 10 patients who committed sexual offenses. Due to statistical reasons, this subgroup was merged with those who were convicted for an assault.
Treatment-related factors can also influence LoS in forensic inpatient facilities, but due to the retrospective nature of our study, a few potentially important factors affecting LoS, such as type of drugs, their doses, polypharmacy, the length of pharmacotherapy, structured assessment of treatment response, and concomitant psychotherapy and rehabilitative efforts, were not consistently available, therefore they could not be included in the analysis. A prospective study can target these issues, but, unfortunately, conducting a prospective study involving forensic inpatients is legally forbidden in Hungary (CLIV/1997. Health Act, 161 § (3),: “Detained persons or persons under military service cannot be subjects of research even if they consent.”).
Ethics approval
The study was approved by the Scientific and Research Ethics Committee of the Medical Research Council of Hungary (No: 51124-1/2016/EKU). The research was conducted according to the ethical principles of the Declaration of Helsinki issued by the World Medical Association (30).
Statistical analysis
Statistical analyses were performed using the SPSS software package (Version 30.0; IBM Corporation, Armonk, NY, USA) (31). Effect size measures were calculated using ROPstat statistical software on the R platform (32). Descriptive data are reported as means and standard deviations, and non-parametric statistical data are reported as medians. The normality of numerical variables was determined using the Kolmogorov–Lilliefors test and skewness and kurtosis. As the distributions of these variables diverged significantly from normal distribution (p < 0.01), non-parametric tests were used for further analyses, including the Mann–Whitney U test and Kruskal–Wallis test. Spearman’s rho correlations were used to evaluate continuous variables.
When building the regression model, first the Forward and Backward selection methods were used, including all variables of study. Subsequently, the final model was performed using the Enter method with a bootstrap procedure (Number of samples 999, seed: 2000000, Bias corrected accelerated) to avoid normality violation. The sample size was set to 999 instead of 1000 based on Wilcox (33). For the regression models, the categorical variables were binarized to be included in the analysis.
Due to the non-parametric nature of the tests, rank Cohen’s d was used as the measure. Rather than using means and standard deviations as for Cohen’s d, rank Cohen’s d is calculated using mean ranks and standard deviations of the ranks (34). Effect size indicators were interpreted according to Cohen (35).
Results
The study sample consisted of 301 inpatients (48 women, 16%; 253 men, 84%) who were released from NIFP between January 1, 2000 and December 31, 2015. The mean age of the sample at the time of admission was 40.23 ± 14.59 years, and the mean LoS was 68.05 ± 47.59 months (median: 53 months). The patients’ sociodemographic data are shown in Table 1. The index offense and forensic, clinical and historical descriptive data are provided in Table 2.
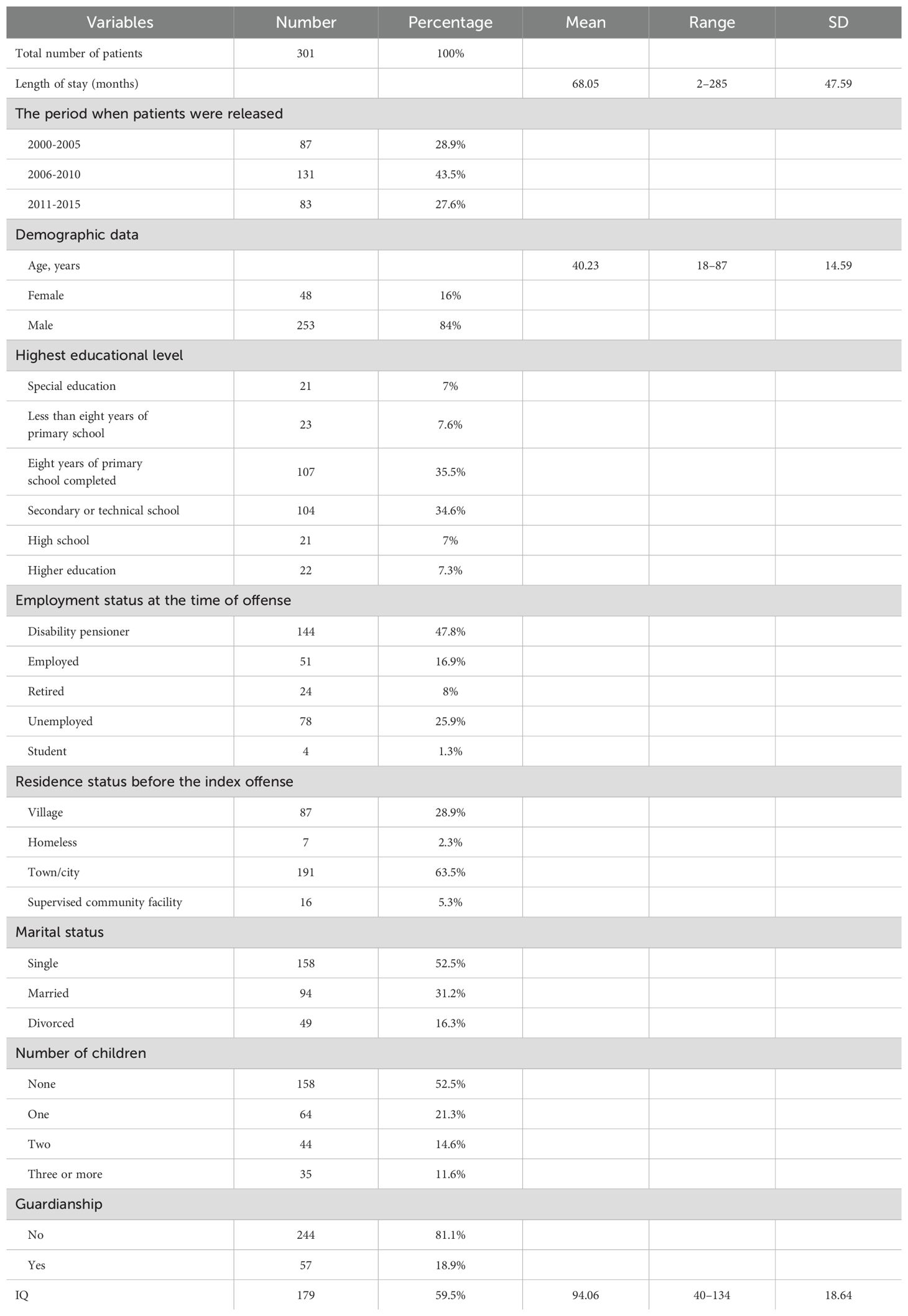
Table 1. Sociodemographic data of the sample.
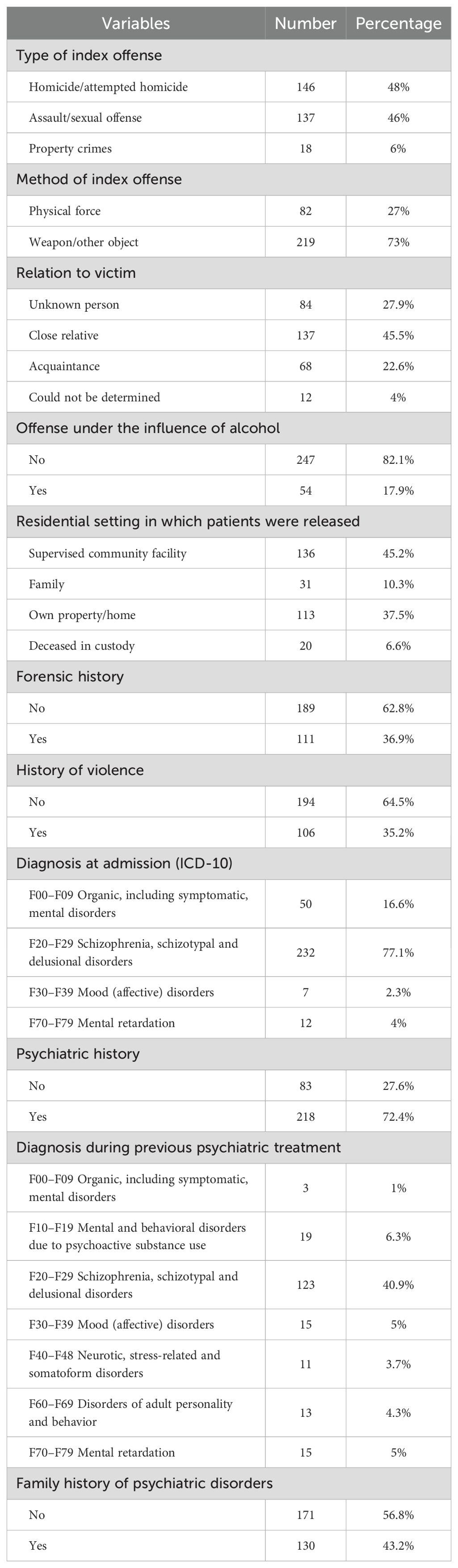
Table 2. Index offense, forensic, clinical and historical descriptive data of the sample.
Correlations of socio-demographic, clinical and forensic factors with LoS
Gender was found to be significantly associated with LoS (Z = –1.989; p = 0.047), with men having a significantly longer median LoS than women (59.00 vs. 46.00 months); the effect size was intermediate (Cohen’s d = –0.315). A weak but significant negative correlation was found between age and LoS (rs = –0.142; p = 0.013). Employment status also was significantly associated with LoS (H(4) = 15.823; p = 0.003), although the effect size was small (η2 = 0.053). Pairwise comparisons showed that patients who were unemployed or receiving a disability pension had significantly longer LoS (p < 0.05) than others. A significant association was found between LoS and marital status (H(2) = 7.239; p = 0.027), with single patients having a longer median LoS than married and divorced patients (63.50 vs. 46.00 vs. 56.00 months); however, the effect size was small (η2 = 0.024). The number of children also was significantly associated with a longer LoS (H(3) = 8.309; p = 0.040), although the effect size was small (η2 = 0.028). Specifically, patients with no children had a significantly longer median LoS than those with 1 or 3 children (62.00 vs. 47.00 vs. 51.00 months, p < 0.05); no significant differences were observed between groups with other numbers of children. A weak but significant negative relationship was observed between IQ and LoS (rs = –0.231; p = 0.002). As IQ showed a weak relationship with LoS and only 59.5% of the total sample had IQ data available, this variable was not included in further analyses. No significant relationships were found between LoS and other sociodemographic variables such as education level, type of residence, or presence of guardianship or the discharge period. The statistical results for demographic variables are shown in Table 3.

Table 3. Univariate correlation of sociodemographic variables with LoS.
A significant relationship was found between the type of index offense and LoS (H(2) = 12.201; p = 0.002), with a small effect size (η2 = 0.041). Specifically, patients who committed homicide/attempted homicide had a significantly longer median LoS than those admitted for assault or crimes against property (63.00 vs. 46.00 vs. 49.00 months; p = 0.002). Additionally, patients who committed a crime with a weapon or object had a significantly longer median LoS than those who used physical force alone (59.00 vs. 46.50, Z = –2.144; p = 0.032), although the effect size was small (Cohen’s d = –0.279).
A significant association was found between LoS and the type of community residential setting into which patients were released (H(3) = 56.918; p < 0.001), with a large effect size (η2 = 0.190). In pairwise comparisons, patients discharged to a supervised community facility had a significantly longer median LoS (79.50 months) than those who were released to a family home or their own property or died while in the NIFP (43.00 vs. 41.00 vs. 45.00 months); no other significant between-group differences were observed. No significant associations of LoS were observed with relation to the victim, offense under the influence of alcohol, forensic history, or history of violence. The statistical results regarding the characteristics of the index offense are shown in Table 4.
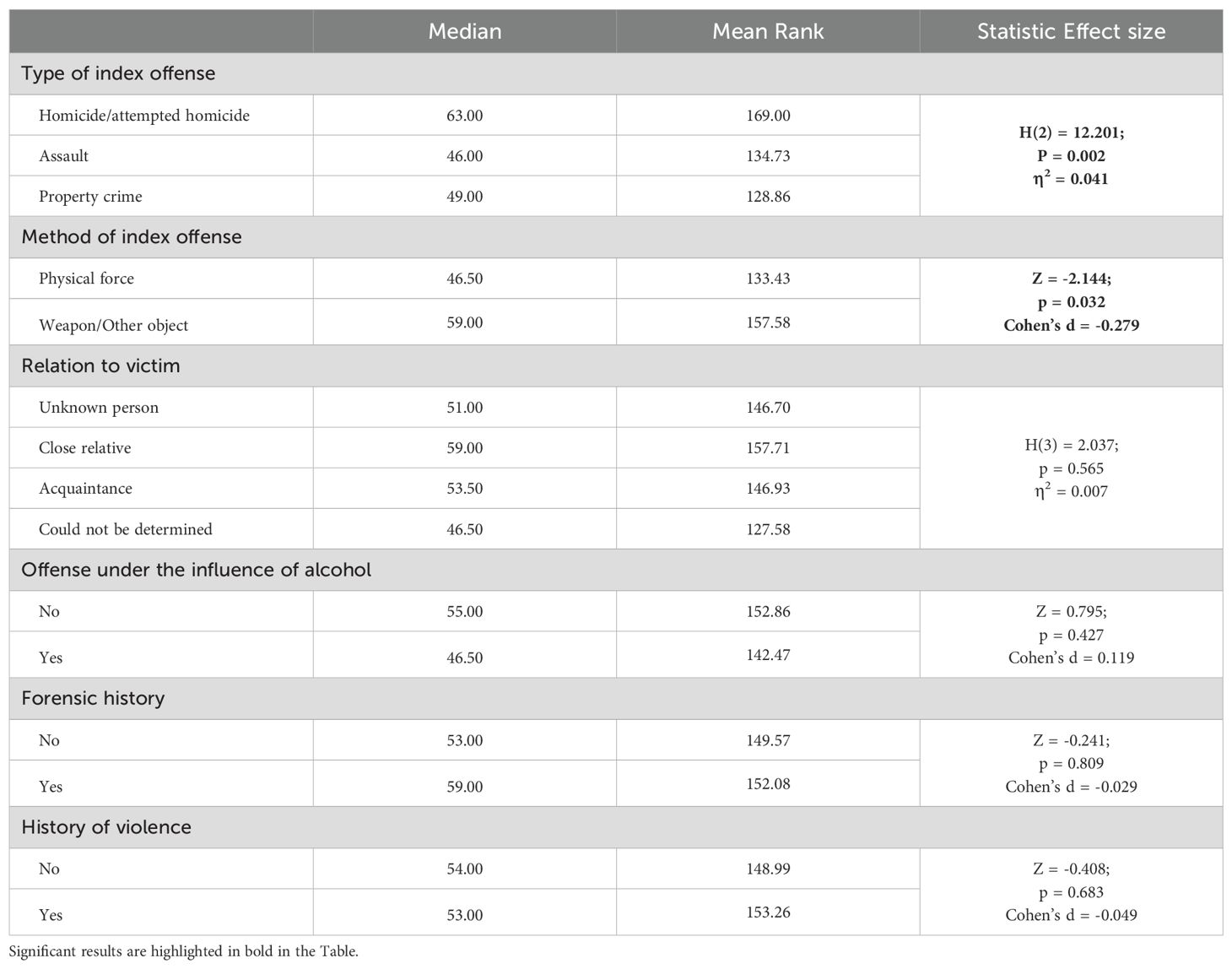
Table 4. Univariate correlation of offense-related variables with LoS.
Regarding clinical factors, only a previous psychiatric diagnosis had a significant association with LoS (H(6) = 14.326; p = 0.026), with a medium effect size (η2 = 0.072). Compared with schizophrenia, the ICD-10 diagnostic groups of schizotypal and delusional disorders (61.00 months), mood (affective) disorders (74.00 months) and organic mental disorders (105.00 months), and neurotic, stress-related and somatoform disorders (35.00 months) and a previous diagnosis of mental retardation (36.00 months) were all associated with a significantly shorter LoS (p < 0.05). Furthermore, patients with a history of psychoactive substance use had a significantly shorter median LoS (46.00 months) than those with organic mental disorders (105 months; p = 0.05). Pairwise comparisons revealed no other significant differences between previous diagnoses. Furthermore, LoS was not significantly associated with clinical variables such as the diagnosis at admission and personal or family history of psychiatric disorders. The statistical results of clinical variables are presented in Table 5.
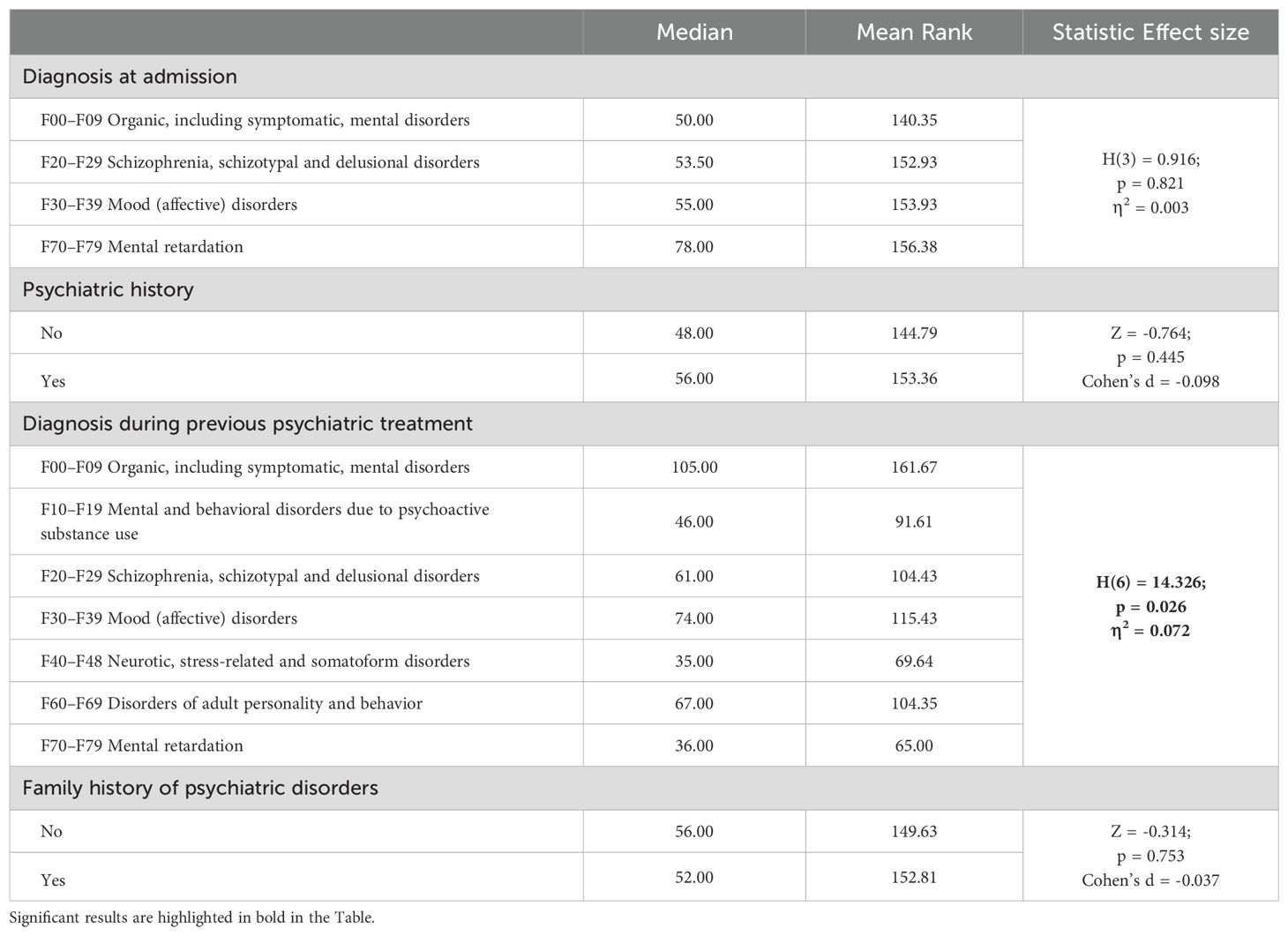
Table 5. Effect of clinical variables on LoS.
In order to find out which factors have a predictive effect on LoS, multiple linear regressions were performed. For building the regression model, first the Forward and Backward stepwise multiple linear regressions were performed, including all the variables studied in the study. The final Forward selection model (Table 6) had 5 variables explaining 32.5% of LoS (F(5, 274) = 26.351, p < 0.001). The final Backward selection model (Table 7) had 11 variables explaining 36.6% of LoS (F(11, 268) = 14.052, p < 0.001). The results of the two regression models were then tested in one model using the Enter method. The variables that did not show a significant effect in the final Enter method model (Table 8) were removed, with the resulting model explaining 34.1% of the LoS (F(8, 272) = 17.589, p < 0.001). The model also showed a significant effect after the bootsrap procedure in the following variables: supervised community facility – residential setting to which patients were released (b = 44.392 [34.694, 54.723], p = 0.001), homicide/attempted homicide – Type of index offense (b = 22.933 [12.522, 32.993], p = 0.001), Age (b = -0.688 [-1.018, -0.356], p = 0.001), F70–F79 Mental retardation diagnosis during previous psychiatric treatment (b = -35.665 [-59.442, -15.038] p = 0.003), male sex (b = 13.821 [2.832, 25.922], p = 0.018), supervised community facility – residence status before the index offense (b = -21.229, [-37.588, -4.662], p = 0.013), F70–F79 Mental retardation diagnosis at admission (ICD-10) (b = 34.047 [1.364, 65.696], p = 0.041), and physical force – method of index offense (b = -10.208 [-20.850, -0.350], p = 0.036).
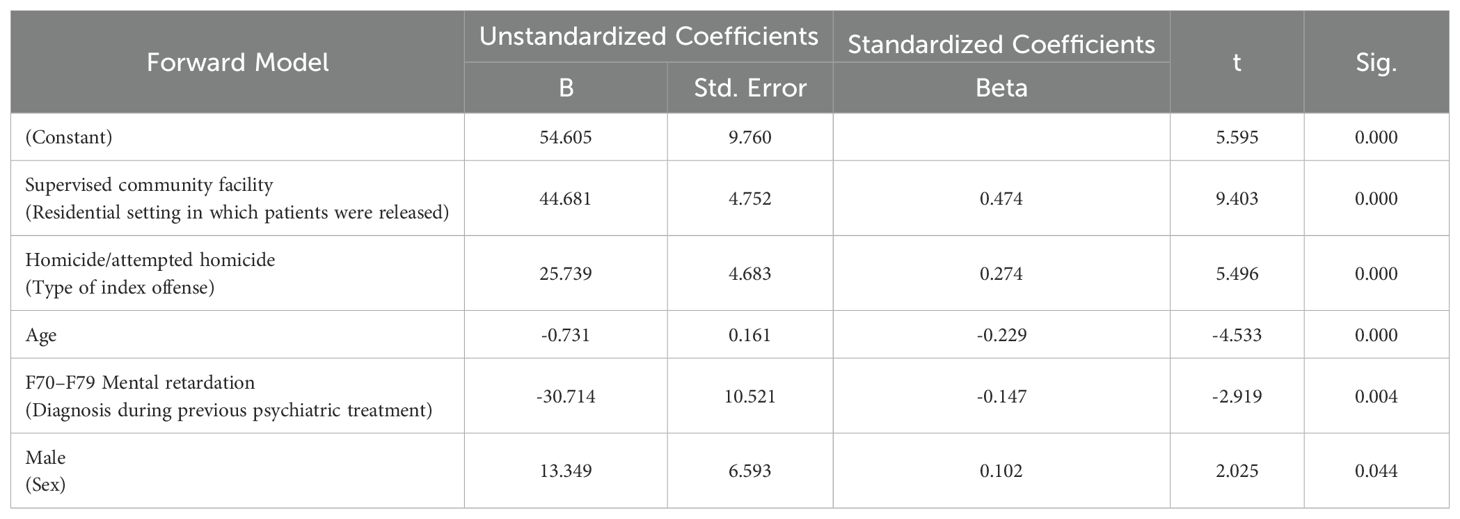
Table 6. Multiple regression analysis using Forward selection method of variables with a significant effect on LoS.
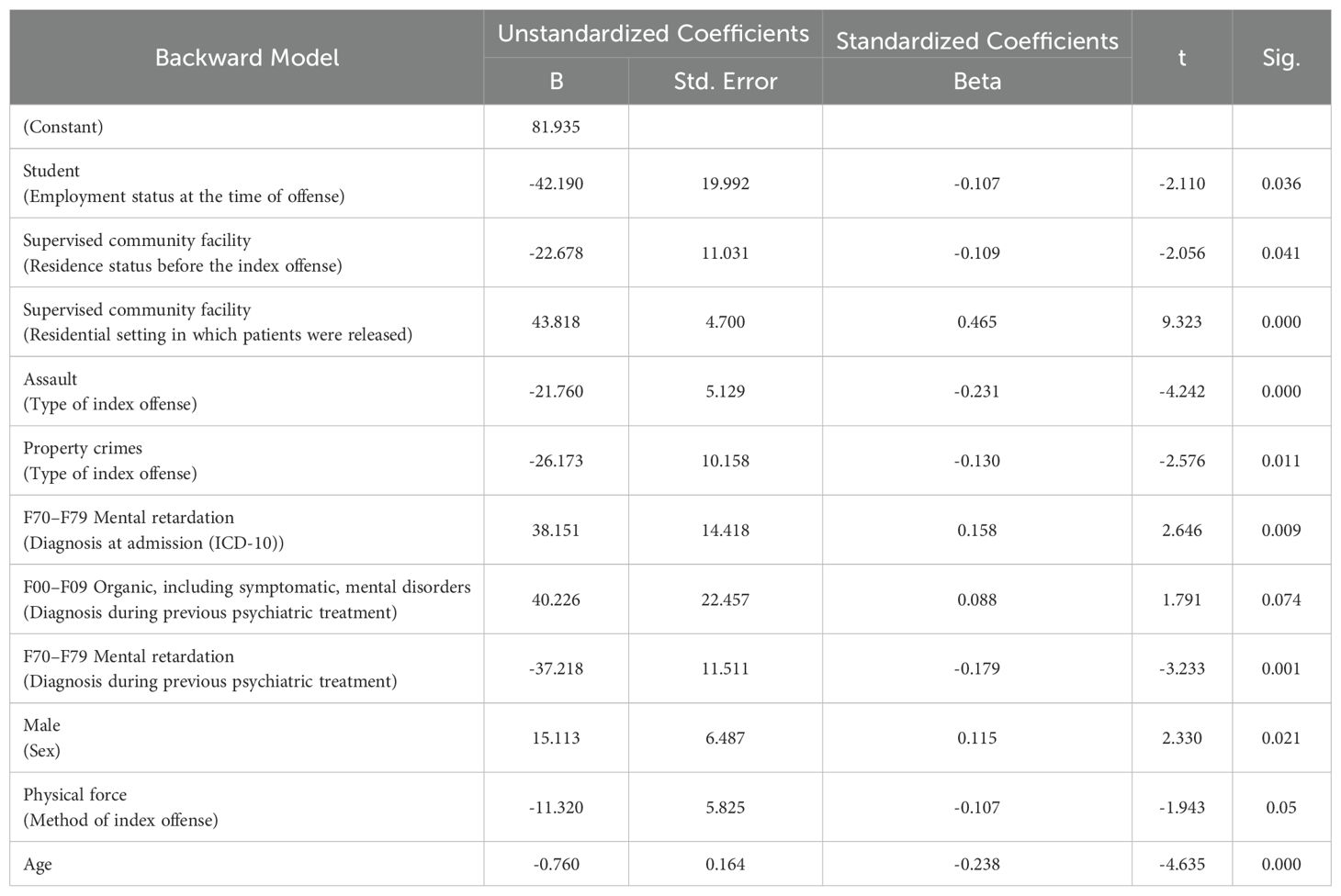
Table 7. Multiple regression analysis using backward selection method of variables with a significant effect on LoS.
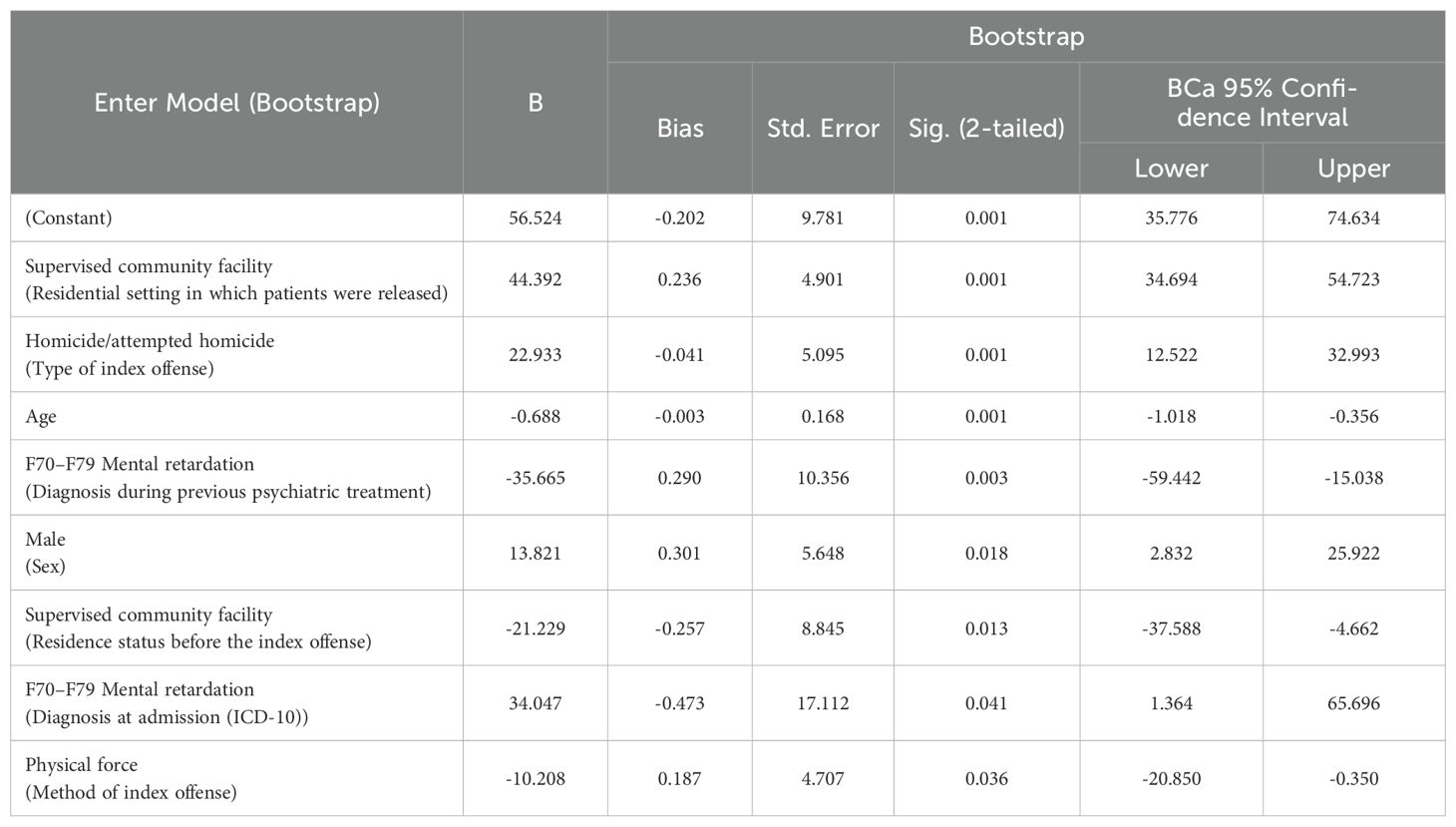
Table 8. Final multiple regression analysis using enter method of variables with a significant effect on LoS.
Discussion
To the best of our knowledge, this is the first study to explore the factors influencing LoS in the national Hungarian inpatient forensic psychiatric service. To date, little has been known about LoS in such services Eastern or Central European countries [e.g (1, 4)]. Although the mean LoS, 68.05 ± 47.59 months, initially appears to be extremely long, it is average for Europe. A much longer LoS has been reported in the Netherlands, Germany, Scotland, England, Wales and Ireland, with a shorter LoS in Lithuania, Latvia, Poland and Slovenia (11).
Several studies have attempted to identify the sociodemographic factors that influence LoS in forensic institutions, with conflicting results. Although a recent systematic review found strong evidence that gender is not correlated with LoS (6), the present study found a moderate correlation between male gender and higher LoS, consistent with other studies (4, 13, 36, 37). This correlation remained significant in a multivariable analysis, possibly because male patients are perceived as being more dangerous than female patients.
Of all the variables investigated in this study, the correlation of the community residential setting (previous supervised community facility placement negatively, while the waitlist for release to supervised community placement positively predicted LoS) had the largest effect size with LoS. Possibly, the chronic shortage of supervised community accommodations in Hungary (38) caused patients qualified to enter such facilities to wait twice as long in the NIFP than other patients in the sample, which would be an ethically unacceptable outcome. No significant correlations were found between LoS and other sociodemographic variables.
Factors associated with the index offense were found to be strong predictors of LoS (17, 39, 40). Homicide or attempted homicide was one of the strongest predictors in the current study, confirming this well-established correlation (6). The use of a weapon or other object was also significantly correlated with LoS in this study. Specifically, committing a crime with a weapon or other object usually results in more serious injury to the victim, which has also been correlated with a longer LoS (2, 16, 24).
The majority (77%) of patients in the sample were diagnosed with a psychotic disorder (ICD-10 diagnostic codes F20–29) in the NIFP. The small number of patients with other diagnoses might explain why psychotic diagnosis was not found to be associated with LoS in this study, in contrast to the literature (4, 23, 24, 41). In a univariate analysis, a psychiatric history (72.4% of the sample) was significantly correlated with LoS, but this correlation disappeared in the multivariable analysis. Case-by-case analysis revealed that a significant number of patients had received different diagnoses in the NIFP than during previous psychiatric treatment episodes. For example, the number of patients diagnosed with a psychotic disorder increased from 123 to 232. Misdiagnosis of psychotic disorders during previous treatment for adjustment, affective, or personality disorders or drug-induced behavioral disturbances may explain this difference. Misdiagnosis of mental retardation can also explain the findings of the final regression model since its previous diagnosis was correlated with shorter, while its diagnosis at admission to the NIFP with longer LoS.
Sociodemographic, clinical and offense-related variables explained only 34.1% of the variance in multiple linear regressions, implying that the main determinants of LoS remain hidden. This finding is rather alarming because the majority of factors predicting LoS are unknown thereby preventing the forensic psychiatric services to implement corrective measure to shorten LoS. Therefore, it is imperative to broaden the current clinical standard of forensic psychiatric assessment and documentation as well as involving more input from allied mental health professionals, relatives and the patients themselves.
The retrospective nature of this study may have precluded the inclusion of several variables with potential effects on LoS, such as the patients’ early social and developmental history, the adequacy of pharmacological and psycho-social treatment at the NIFP, and an estimate of societal tolerance toward violent offenders. Beyond professional aspects, decision-making forensic psychiatrists and judges may choose to err on the side of caution to protect the community from re-offenders, which may also have a significant effect on LoS. The necessity of continuation of forensic psychiatric treatment is evaluated every 6 months for all patients under compulsory inpatient treatment order in NIFP. The treating psychiatrist gives a recommendation for the continuation of treatment or for discharge of the patients. Then, an independent forensic psychiatric expert examines the patients, reviews their documentation, and gives a recommendation to the judge who makes the final decision. If the judge terminates the compulsory treatment order, the patient must be released within 24 hours from NIFP. However, if there is no adequate community place available, either a protective, safe family home or in a residential community setting, the judge has no choice but to extend the inpatient compulsory treatment. This is an entirely unsatisfactory situation and warrants urgent actions to expand the availability of community residential places in Hungary.
Strengths and limitations of the study
This is the first study involving a comprehensive evaluation of the factors influencing LoS in the only forensic inpatient psychiatric facility in Hungary. The results of this study are therefore representative of Hungarian forensic psychiatric care nationwide. Unlike in Hungary, inpatient forensic psychiatric care in most European countries is not centralized in one place, but provided in a number of institutes, that may have different levels of security, different protocols, different scales for diagnostic or risk evaluation, and different treatment strategies. Having a full picture about the inpatient forensic psychiatric system of a given European country thus can be complicated. The strength of the current study is the use of data collected in a single place where all Hungarian forensic inpatients are treated, thus eliminating these difficulties in data interpretation. Another strength is that the results point out the deficiencies in social aftercare of forensic psychiatric patients affect LoS; previous studies have paid less attention to this potential factor regarding LoS (2, 15, 18).
The majority of the limitations of this study stem from its retrospective nature. While every attempt was made to extract as much information from patients’ files as possible, the quality of the data limited the validity of the results. For example, data on psychopathological symptoms were omitted due to the large number of confounding factors (e.g., missing information, time elapsed since the offense, emergency treatment before detailed forensic examination). A further limitation is the lack of structured diagnostic interviews or symptom assessment scale and psychological test results apart from IQ data for 179 patients. Data on pharmacological and psychosocial treatment, rehabilitative efforts and the use of risk and functional assessment scales were not included in the study and should be targeted in further studies.
Conclusion
In this retrospective study, 34.1% of the variance in LoS in the Hungarian forensic inpatient psychiatric service was explained by male gender, age, a conviction for murder or attempted murder, use of a weapon or other objects and the community residential setting in which patients were released. Our results clearly indicate the presence of additional factors not accounted for in the available data.
Unjustifiably extended LoS and long waiting times for supervised community residential facilities may violate patients’ human rights. The Hungarian forensic psychiatric system should make further efforts toward implementing a more evidence-based method for determining LoS in inpatient care.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Scientific and Research Ethics Committee of the Medical Research Council of Hungary (No: 51124-1/2016/EKU). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
SF: Data curation, Methodology, Writing – original draft, Writing – review & editing. HG: Data curation, Writing – original draft, Writing – review & editing. GU: Supervision, Writing – original draft, Writing – review & editing. GG: Conceptualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gosek P, Kotowska J, Rowińska-Garbień E, Bartczak D, Heitzman J. Factors influencing length of stay of forensic patients: impact of clinical and psychosocial variables in medium secure setting. Front Psychiatry. (2020) 11:810. doi: 10.3389/fpsyt.2020.00810
2. Kirchebner J, Günther MP, Sonnweber M, King A, Lau S. Factors and predictors of length of stay in offenders diagnosed with schizophrenia - a machine-learning-based approach. BMC Psychiatry. (2020) 20:1. doi: 10.1186/s12888-020-02612-1
3. Senn D, Bulten E, Tomlin J, Völlm B. A comparison of English and Dutch long-stay patients in forensic psychiatric care. Front Psychiatry. (2020) 11:574247. doi: 10.3389/fpsyt.2020.574247
4. Páv M, Vňuková M, Sebalo I. Factors affecting length of inpatient forensic stay: retrospective study from Czechia. Front Psychiatry. (2022) 13:825615. doi: 10.3389/fpsyt.2022.825615
5. Rutherford M, Duggan S. Forensic mental health services: facts and figures on current provision. Br J Forensic Pract. (2008) 10:4–10. doi: 10.1108/14636646200800020
6. Dima A, Wazir A, Clark-Castillo R, Zakopoulos I, Smith S, Gaughran F. Factors influencing the length of stay in forensic psychiatric settings: a systematic review. BMC Health Serv Res. (2024) 24:400. doi: 10.1186/s12913-024-10863-x
7. Gosek P, Kotowska J, Rowińska-Garbień E, Bartczak D, Tomlin J, Heitzman J. Longer than prison? A comparison of length of stay in a medium security hospital and prison for perpetrators of violent crimes other than homicide or attempted homicide. Crim Behav Ment Health. (2021) 31:162–70. doi: 10.1002/cbm.2202
8. Sedgwick O, Young S, Das M, Kumari V. Objective predictors of outcome in forensic mental health services—a systematic review. CNS Spectr. (2016) 21:430–44. doi: 10.1017/s1092852915000723
9. Bulten E, Verkes RJ. Long stay in Europe: A systems-oriented approach. Long-term forensic psychiatric care. In: Völlm B, Braun P, editors. Long-Term Forensic Psychiatric Care: Clinical, Ethical and Legal Challenges. Cham, Swiss: Springer (2019). p. 27–45. doi: 10.1007/978-3-030-12594-3_4
10. Sampson S, Edworthy R, Völlm B, Bulten E. Long-term forensic mental health services: an exploratory comparison of 18 European countries. Int J Forensic Ment Health. (2016) 15:333–51. doi: 10.1080/14999013.2016.1221484
11. Tomlin J, Lega I, Braun P, Kennedy HG, Herrando VT, Barroso R, et al. Forensic mental health in Europe: some key figures. Soc Psychiatry Psychiatr Epidemiol. (2020) 56:109–17. doi: 10.1007/s00127-020-01909-6
12. Beis P, Graf M, Hachtel H. Impact of legal traditions on forensic mental health treatment worldwide. Front Psychiatry. (2022) 13:876619. doi: 10.3389/fpsyt.2022.876619
13. Davoren M, Byrne O, O’Connell P, O’Neill H, O’Reilly K, Kennedy HG. Factors affecting length of stay in forensic hospital setting: need for therapeutic security and course of admission. BMC Psychiatry. (2015) 15:1–5. doi: 10.1186/s12888-015-0686-4
14. Völlm BA, Edworthy R, Huband N, Talbot E, Majid S, Holley J, et al. Characteristics and pathways of long-stay patients in high and medium secure settings in England; A secondary publication from a large mixed-methods study. Front Psychiatry. (2018) 9:140. doi: 10.3389/fpsyt.2018.00140
15. O’Neill C, Heffernan P, Goggins R, Corcoran C, Linehan S, Duffy D, et al. Long-stay forensic psychiatric inpatients in the Republic of Ireland: aggregated needs assessment. Ir J Psychol Med. (2003) 20:119–25. doi: 10.1017/s0790966700007916
16. Fong CL, Kar PC, Huei LT, Yan OL, Daud TI, Zakaria H, et al. Factors influencing inpatient duration among insanity acquittees in a Malaysian mental institution. Psychiatry. (2010) 11:25–35.
17. Harris GT, Rice ME, Cormier CA. Length of detention in matched groups of insanity acquittees and convicted offenders. Int J Law Psychiatry. (1991) 14:223–36. doi: 10.1016/0160-2527(91)90004-7
18. Ross T, Querengässer J, Fontao MI, Hoffmann K. Predicting discharge in forensic psychiatry: The legal and psychosocial factors associated with long and short stays in forensic psychiatric hospitals. Int J Law Psychiatry. (2012) 35:213–21. doi: 10.1016/j.ijlp.2012.02.011
19. Stürner L, Ross T, Querengässer J, Traub HJ. Institutional influence on length of stay in German forensic hospitals: a multilevel analysis of patients with schizophrenia spectrum disorders. Front Psychiatry. (2024) 15:1456363. doi: 10.3389/fpsyt.2024.1456363
20. Moran MJ, Fragala MR, Wise BF, Novak TL. Factors affecting length of stay on maximum security in a forensic psychiatric hospital. Int J Offender Ther Comp Criminol. (1999) 43:262–74. doi: 10.1177/0306624x99433002
21. Weber K, Morier S, Lesaffre L, Menu C, Bertschy P, Herrmann FR, et al. Court-ordered inpatient psychiatric care in Switzerland: determinants of length of stay and treatment outcome. Front Psychiatry. (2023) 14:1222337. doi: 10.3389/fpsyt.2023.1222337
22. Fioritti A, Ferriani E, Rucci P, Melega V, Venco C, Scaramelli AR, et al. Predicting length of stay in Italian Psychiatric Forensic Hospitals: a survival analysis. Epidemiol Psichiatr Soc. (2001) 10:125–34. doi: 10.1017/s1121189x00005200
23. Shah A, Waldron G, Boast N, Coid JW, Ullrich S. Factors associated with length of admission at a medium secure forensic psychiatric unit. J Forens Psychiatry Psychol. (2011) 22:496–512. doi: 10.1080/14789949.2011.594902
24. Andreasson H, Nyman M, Krona H, Meyer L, Anckarsäter H, Nilsson T, et al. Predictors of length of stay in forensic psychiatry: The influence of perceived risk of violence. Int J Law Psychiatry. (2014) 37:635–42. doi: 10.1016/j.ijlp.2014.02.038
25. D’Orta I, Weber K, Herrmann FR, Giannakopoulos P. Determinants of clinical outcome and length of stay in acute care forensic psychiatry units. BMC Psychiatry. (2023) 23:264. doi: 10.1186/s12888-023-04748-2
26. Sivak L, Forsman J, Masterman T. Duration of forensic psychiatric care and subsequent criminal recidivism in individuals sentenced in Sweden between 2009 and 2019. Front Psychiatry. (2023) 14:1129993. doi: 10.3389/fpsyt.2023.1129993
27. Castro M, Cockerton T, Birke S. From discharge to follow-up: a small-scale study of medium secure provision in the independent sector. Br J Forensic Pract. (2002) 4:31–9. doi: 10.1108/14636646200200019
28. Margetić B, Margetić BA, Ivanec D. Can personality traits affect detention length in a forensic institution? J Forensic Psychol Pract. (2014) 14:277–87. doi: 10.1080/15228932.2014.931127
29. Baran B, Szabo FA, Kara B, Kovacs M, Uzonyi A, Antal A, et al. Do previous offences predict violent acts in psychiatric patients? A retrospective study in Hungary. Ideggyogy Szle. (2015) 68:99–104.
30. World Medical Association. The Declaration of Helsinki (2024). Available online at: https://www.wma.net/policies-post/wma-declaration-of-helsinki/ (Accessed December 17, 2024).
32. Vargha A. A ROPstat statisztikai programcsomag. Stat Szle. (2016) 94:1165–92. doi: 10.20311/stat2016.11-12.hu1165
33. Wilcox RR. Fundamentals of Modern Statistical Methods: Substantially Improving Power and Accuracy. New York: Springer (2010). p. 94.
34. Vargha A. Normális vagy? És ha nem? Statisztikai módszerek nem normális eloszlású változókkal pszichológiai kutatásokban. Budapest: Pólya Kiadó (2020). p. 106.
35. Cohen J. Statistical Power Analysis for the Behavioral Sciences. New York: Routledge Academic (1988). p. 40.
36. Steadman HJ, Pasewark RA, Hawkins M, Kiser M, Bieber S. Hospitalization length of insanity acquittees. J Clin Psychol. (1983) 39:611–4. doi: 10.1002/1097-4679(198307)39:4<611::aid-jclp2270390427>3.0.co;2-z
37. Crocker AG, Nicholls TL, Charette Y, Seto MC. Dynamic and static factors associated with discharge dispositions: the national trajectory project of individuals found not criminally responsible on account of mental disorder (NCRMD) in Canada. Behav Sci Law. (2014) 32:577–95. doi: 10.1002/bsl.2133
38. Papp É, Gazdag G. Pszichiátriai osztályon kezelt betegek szociális intézménybe történő elhelyezésének nehézségei. IME. (2019) 8:43–6.
39. Baldwin LJ, Menditto AA, Beck NC, Smith SM. Factors influencing length of hospitalization for NGRI acquittees in a maximum security facility. J Psychiatry Law. (1992) 20:257–67. doi: 10.1177/009318539202000207
40. Silver E. Punishment or treatment? Comparing the lengths of confinement of successful and unsuccessful insanity defendants. Law Hum Behav. (1995) 19:375–88. doi: 10.1007/bf01499138
Keywords: length of stay, forensic inpatient care, Hungary, community residential setting, type of criminal offense
Citation: Fekete S, Girasek H, Ungvari GS and Gazdag G (2025) Factors predicting the length of stay in inpatient forensic psychiatric care in Hungary. Front. Psychiatry 16:1582702. doi: 10.3389/fpsyt.2025.1582702
Received: 24 February 2025; Accepted: 14 April 2025;
Published: 13 May 2025.
Edited by:
Yasin Hasan Balcioglu, Bakirkoy Prof Mazhar Osman Training and Research Hospital for Psychiatry, Neurology, and Neurosurgery, TürkiyeReviewed by:
Marek Páv, Psychiatric Hospital Bohnice, CzechiaEmiliano Soldini, University of Applied Sciences and Arts of Southern Switzerland, Switzerland
Sevler Yildiz, Elazig Fethi Sekin City Hospital, Türkiye
Copyright © 2025 Fekete, Girasek, Ungvari and Gazdag. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gábor Gazdag, Z2F6ZGFnQGxhbWIuaHU=
†ORCID: Hunor Girasek, orcid.org/0000-0002-8140-2065
Gabor S. Ungvari, orcid.org/0000-0003-4821-4764
Gábor Gazdag, orcid.org/0000-0002-6914-8041