 Bàrbara Sureda-Caldentey1,2,3
Bàrbara Sureda-Caldentey1,2,3 Cristina Garcia-Gibert1,4Amparo Martínez1,5Yolanda Giménez1,5Xavier Segú2,6
Cristina Garcia-Gibert1,4Amparo Martínez1,5Yolanda Giménez1,5Xavier Segú2,6 Aida Mallorquí2,6Estel Gelabert7Alba Roca-Lecumberri1,2,8
Aida Mallorquí2,6Estel Gelabert7Alba Roca-Lecumberri1,2,8 Anna Torres-Giménez1,2,3,8*
Anna Torres-Giménez1,2,3,8*- 1Unitat de Salut Mental Perinatal CLINIC-Barcelona, Hospital Clínic, Barcelona, Spain
- 2Psychiatry and Clinical Psychology Service, Hospital Clinic, Barcelona, Spain
- 3Department of Clinical Psychology and Psychobiology, University of Barcelona, Barcelona, Spain
- 4Sexual and Reproductive Health Care Assistance Center, Parc Sanitari Sant Joan de Deu, Cerdanyola del Vallès, Spain
- 5Maternal Fetal Medicine Service, Hospital Clinic, Barcelona, Spain
- 6Clinical Health Psychology Section, Institute of Neuroscience, Hospital Clinic, Barcelona, Spain
- 7Departament of Clinical and Health Psychology, Universitat Autònoma de Barcelona, Barcelona, Spain
- 8Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain
Background: Perinatal loss is a situation with significant traumatic potential. However, no study has evaluated the effectiveness of eye movement desensitization and reprocessing (EMDR) for the prevention or treatment of post-traumatic symptoms in perinatal loss. The aim of this study was to assess the feasibility and preliminary effectiveness of an EMDR recent traumatic episode protocol (EMDR-RTEP) as a preventive intervention for post-traumatic symptoms after perinatal loss.
Materials and methods: A one-site, open label, randomized controlled pilot trial was designed. A total of 40 women who had suffered perinatal loss in the Maternal-Fetal Medicine Service of a tertiary university hospital were recruited. The women were randomized to the EMDR-RTEP (n=20) or treatment as usual (TAU, n=20). Post-traumatic, depressive, anxiety and intensity of perinatal grief symptoms were assessed using standardized instruments at baseline and 3 months after perinatal loss (post-treatment). We performed an intention-to-treat analysis using analysis of covariance with baseline scores as covariates.
Results: Women who received the EMDR-RTEP scored non-significantly lower than women who received TAU in all post-treatment outcomes. According to a satisfaction scale (CRES-4), women who received the EMDR-RTEP had a higher perceived emotional change than women who received TAU (U = 69.5, p = .011).
Conclusions: EMDR-RTE is a feasible intervention, that is well accepted and tolerated by women after perinatal loss, with adequate satisfaction. Further studies with a larger sample size are needed to confirm these results.
Clinical Trial Registration: https://www.clinicaltrials.gov/, identifier NCT05701137.
1 Introduction
Perinatal grief has traditionally been an unacknowledged and socially unrecognized form of bereavement, that has only recently received the research attention it deserves. Grief response to perinatal loss occurs independently of the gestational week at which the loss occurs and regardless of whether the loss was the result of medical termination of pregnancy (therapeutic abortion due to severe fetal illness or malformation) or occurred unexpectedly. Additionally, perinatal loss is a potentially traumatic event that is associated with significant direct and indirect economic, psychological, social, familial, and community costs (1). Perinatal loss can have an impact on mental health (2). Between 8% and 20% of women who experience perinatal show symptoms for moderate depression (3, 4). Moreover, 20–39% of these women may develop post-traumatic stress disorder (PTSD) at one month after the loss, and approximately 4% subsequently develop chronic PTSD (5, 6). Furthermore, women with a history of fetal loss have increased anxiety and depression levels in subsequent pregnancies (7).
Limited and low-quality evidence suggests that psychosocial interventions may be effective in reducing depressive, anxious, and grief symptoms in parents after perinatal loss (8). Most evidence is based on studies evaluating the efficacy of counseling, primarily conducted by nurses or midwives (8).
There is less evidence regarding the efficacy of psychological treatments for perinatal loss, particularly in relation to improving post-traumatic symptoms (9). Kersting et al. (10) evaluated the efficacy of internet-based cognitive behavioral therapy in a sample of women after pregnancy loss (miscarriage, termination due to fetal anomaly, or stillbirth), showing a reduction in post-traumatic symptoms, grief intensity, and general psychopathology in the intervention group compared to a waiting list control group. In a subsequent randomized controlled trial by the same research team, the same intervention showed a positive effect in a larger sample of parents with pregnancy loss, with reductions in post-traumatic, depressive, anxious, and prolonged grief symptoms compared to a waiting list control group (11). Navidian et al. (12) found that four sessions of grief counseling were effective in reducing the severity of PTSD symptoms in women who had recently experienced a stillbirth. In contrast, a yoga intervention was not effective in reducing post-traumatic symptoms (13).
According to clinical practice guidelines, eye movement desensitization and reprocessing (EMDR) is a psychological therapy of choice for PTSD (14–17). Early EMDR interventions have also shown benefits in the short-term improvement of post-traumatic symptoms in populations exposed to traumatic events (18). EMDR has been applied in populations experiencing traumatic loss, offering promising results, although more studies are needed (19–21). In the perinatal population, EMDR therapy in the recent traumatic episode protocol (EMDR-RTEP) has been applied in cases of traumatic childbirth, showing efficacy as an early preventive intervention for PTSD (22). However, no study has evaluated the effectiveness of EMDR for the prevention or treatment of post-traumatic symptoms following perinatal loss. This study aimed to assess the feasibility and preliminary effectiveness of early intervention using EMDR-RTEP for the treatment and prevention of post-traumatic symptoms after perinatal loss. A secondary aim was to evaluate the preliminary effectiveness of the protocol on depressive, anxious, and intensity of perinatal grief symptoms, which were included as secondary outcomes in this pilot trial. The inclusion of these outcomes allows exploring whether EMDR-RTEP may have broader benefits beyond post-traumatic symptoms. Another secondary aim was to assess whether satisfaction with therapy would be comparable between women receiving EMDR-RTEP and those receiving treatment as usual (TAU). We hypothesized that women who experienced perinatal loss and received EMDR-RTEP would report significantly lower post-traumatic stress symptoms three months after the loss compared to those receiving TAU. Additionally, we expected that women in the EMDR-RTEP group would show lower levels of depressive and anxious symptoms, and reduced intensity of perinatal grief. We also hypothesized that satisfaction with therapy would be comparable between groups.
2 Materials and methods
2.1 Design
A pilot, single-site, open-label, randomized, controlled parallel trial was designed, following CONSORT guidelines. The study was registered a priori at clinicaltrials.gov (NCT05701137) and was approved by the institutional review board of the first author’s institution (HCB/2022/1197). Written informed consent was obtained from all participants. The study was conducted in accordance with the Declaration of Helsinki.
Sample size was determined a priori. Sample sizes between 12 to 35 per group are recommended for a pilot study with continuous outcomes (23). Using GPower, a minimum sample size of 17 subjects per group was required to assess significant differences with an effect size of one between two independent samples with an alpha error of 5% and a power of 80%. A total of 40 participants were included: 20 were randomized to the EMDR-RTEP and 20 to TAU (n=20) (allocation ratio 1:1). Participants did not receive compensation beyond the psychological care provided through their voluntary participation in the study.
2.2 Randomization
The random sequence was generated using a computer-generated block of random numbers (STATA v16), by a member of the research team not involved in participant selection, inclusion, or treatment. Allocation was concealed in sealed opaque envelopes, safeguarded by a research team member unrelated to other aspects of the study. Allocation was concealed until participants were enrolled and assigned to EMDR-RTEP or TAU.
2.3 Study population and recruitment
The study sample was recruited from the Maternal-Fetal Medicine Service of a public university hospital in Barcelona (Spain) using a consecutive sampling strategy. Women were eligible to enroll in the study if they had been attended at the hospital for recent perinatal loss (miscarriage, stillbirth, or termination of pregnancy after a positive prenatal diagnosis), were aged 18 years or over, and had requested psychological treatment. The inclusion criteria were not based on the presence of a higher intensity of symptoms. The exclusion criteria were: 1) active substance use disorder; 2) cognitive disability; and 3) language barrier. The latter two exclusion criteria are based on minimizing the difficulty or impossibility of completing the self-administered questionnaires.
All women treated at the Maternal-Fetal Medicine Service for perinatal loss routinely received a follow-up telephone call from a nurse between the first and second week after the loss. During this call, the nurse inquired about the woman’s general physical recovery and emotional state. If signs of emotional distress were identified or if the woman expressed a need for psychological care, she was offered a referral for psychological assessment and intervention. During the study recruitment period, from April 2023 to September 2024, the nurse additionally asked patients if they were interested in receiving information about the study. Women who met the inclusion criteria and wished to participate received study information from a research team member, signed the informed consent, and completed questionnaires including sociodemographic information and symptom assessment. After providing informed consent, participants were allocated to either the EMDR-RTEP or TAU. Participants and researchers were not blinded to treatment allocation. Women again completed the symptom assessment questionnaires as well as a satisfaction questionnaire 3 months after perinatal loss (post-treatment). The follow-up evaluations were completed in November 2024.
2.4 Treatment
Both psychological treatments were delivered by perinatal psychologists with a minimum of five years of experience in perinatal mental health care, including the treatment of perinatal grief. The EMDR intervention was administered by a single psychologist (BS) certified in EMDR and trained in the RTEP (24). Therapists were not randomized; however, all shared similar expertise in perinatal mental health.
2.4.1 EMDR-RTEP
Participants in the EMDR-RTEP group received an EMDR intervention following the RTEP of Shapiro et al. (24). Given that the memory of a recent trauma is not fully consolidated, this adaptation of the standard EMDR protocol is designed for application within days after the trauma until three months post-event. The RTEP is an EMDR-based early intervention approach that targets recent trauma through structured phases ensuring emotional safety. It identifies multiple points of disturbance across the trauma continuum. Key techniques include narrative processing with bilateral stimulation, non-verbal scanning, and telescopic processing. The application of this protocol to perinatal grief and PTSD facilitates early, adaptive integration of traumatic memories.
2.4.2 TAU
Participants in the TAU group received psychological treatment involving psychological grief counseling, and non-trauma-focused cognitive-behavioral techniques. This is the standard treatment provided at the hospital where the study was conducted.
2.5 Measures
2.5.1 PTSD checklist for the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition
The PCL-5 (25) is a self-report instrument assessing post-traumatic symptoms according to DSM-5 criteria and consists of 20 Likert-type items.
2.5.2 Beck Depression Inventory-II
The BDI-II (26) is a self-report instrument assessing depressive symptoms. It consists of 21 Likert-type items.
2.5.3 State-Trait Anxiety Inventory
The STAI (27) is a self-report tool assessing state and trait anxiety. The state anxiety version was used, which refers to transient feelings of tension and increased central nervous system activity. It consists of 20 4-point Likert-type items.
2.5.4 Perinatal Grief Scale
The PGS (28) is a self-report instrument assessing the intensity of perinatal grief. It consists of 33 Likert-type items and includes three subscales and a total score. The total score was used in this study.
2.5.5 Consumer Reports Effectiveness Score
The CRES-4 (29) is a self-report instrument assessing user satisfaction with the treatment received. It includes four items evaluating three dimensions: satisfaction, problem solution, and perceived change.
2.6 Statistical analysis
Baseline differences in sociodemographic and clinical variables between groups were assessed using Student’s t-, Chi-square, or Fisher’s exact tests, as appropriate. Normality of the outcome variables was assessed using the Shapiro-Wilk test. Intention-to-treat analysis was conducted using the baseline-observation-carried-forward (BOCF) method for imputing missing data. Differences between intervention groups in outcomes of interest were analyzed using analysis of covariance (ANCOVA) with baseline scores as covariates. Sensitivity analysis was performed using complete case datasets. For satisfaction analysis, differences between groups were assessed using the Mann-Whitney U test. The statistical analyses were performed using SPSS v.23 and STATA v.16.
3 Results
3.1 Recruitment and baseline assessment
Of the 108 women assessed for eligibility, 21 were excluded for not meeting the inclusion criteria, and 47 declined to participate (Figure 1). Consequently, 40 women were randomized, 20 allocated to EMDR-RTEP and 20 to TAU. One woman in each group completed treatment but did not respond to the post-treatment assessment, and two women in the EMDR-RTEP group and three in the TAU group discontinued the intervention. One woman in the EMDR-RTEP group abandoned the treatment due to transient clinical worsening associated with partner conflict. For the remaining women, the reason for discontinuation was unknown as contact was lost. In these cases, women reported feeling the same or better at their last visit compared to at baseline, confirming the appropriateness of the BOCF method for imputing missing data. Women in the TAU group received an average of 4.6 (standard deviation [SD] = 2.3, range = 1–10) intervention sessions, while those in the EMDR-RTEP group received an average of 5.8 (SD = 1.6, range = 3–10) sessions. The difference in the number of intervention sessions between groups was statistically significant (U = 127.0, p = .045), with women in the EMDR-RTEP group receiving, on average, one more session than those in the TAU group.
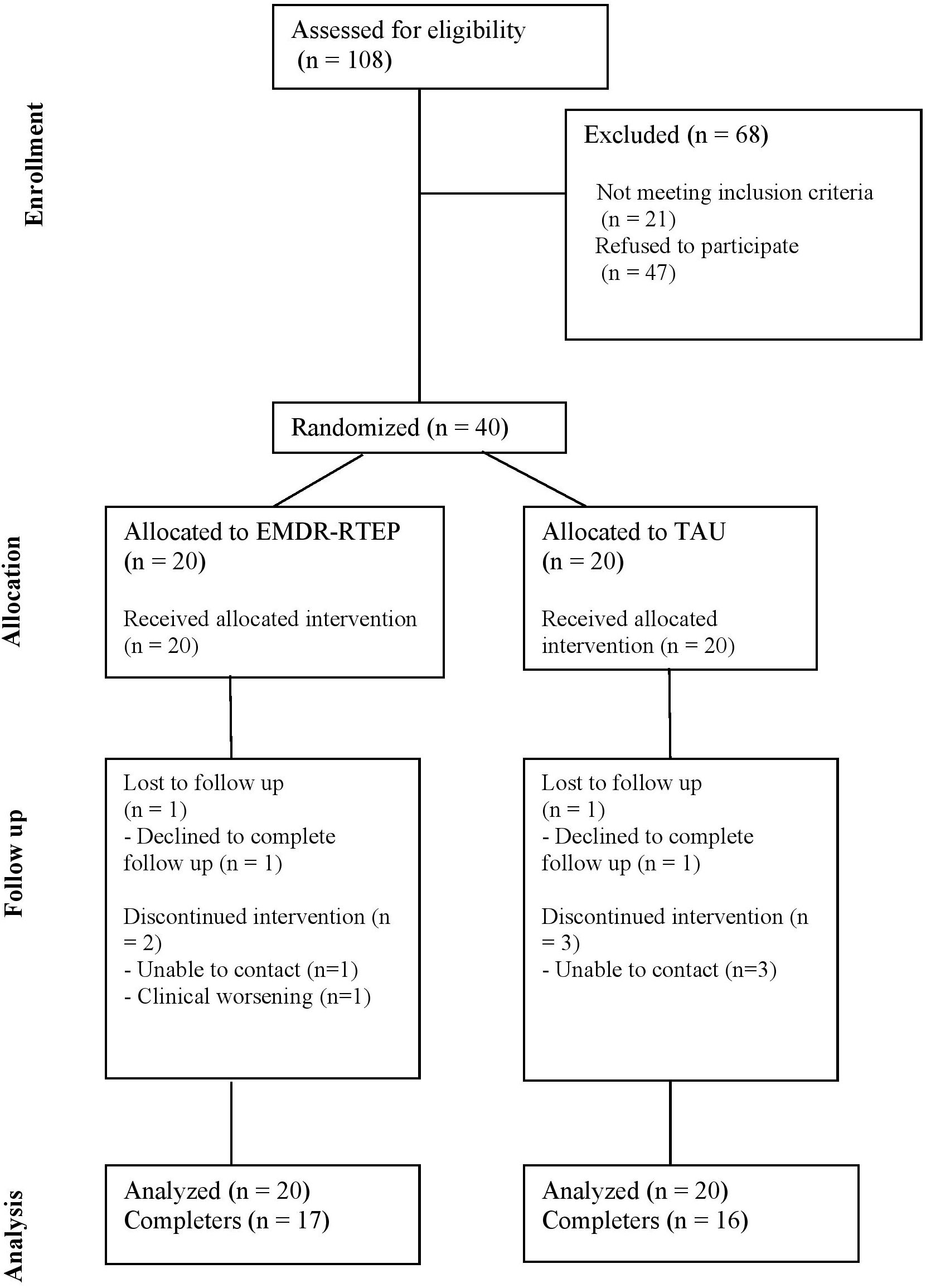
Figure 1. CONSORT diagram showing the flow of participants throughout the study.
Table 1 shows baseline assessment results by intervention group (EMDR-RTEP or TAU). No significant differences were found between the TAU and the EMDR-RTEP group in sociodemographic or clinical variables at baseline. Neither were there significant differences between the two groups in baseline scores for post-traumatic (t[38] = 0.31, p = .761), depressive (t[38] = 0.11, p = .912), anxious (t[38] = 0.46, p = .649), or perinatal grief (t[38] = 0.56, p = .582) symptoms. The mean scores of the questionnaires at baseline and post-treatment are shown in Table 2.
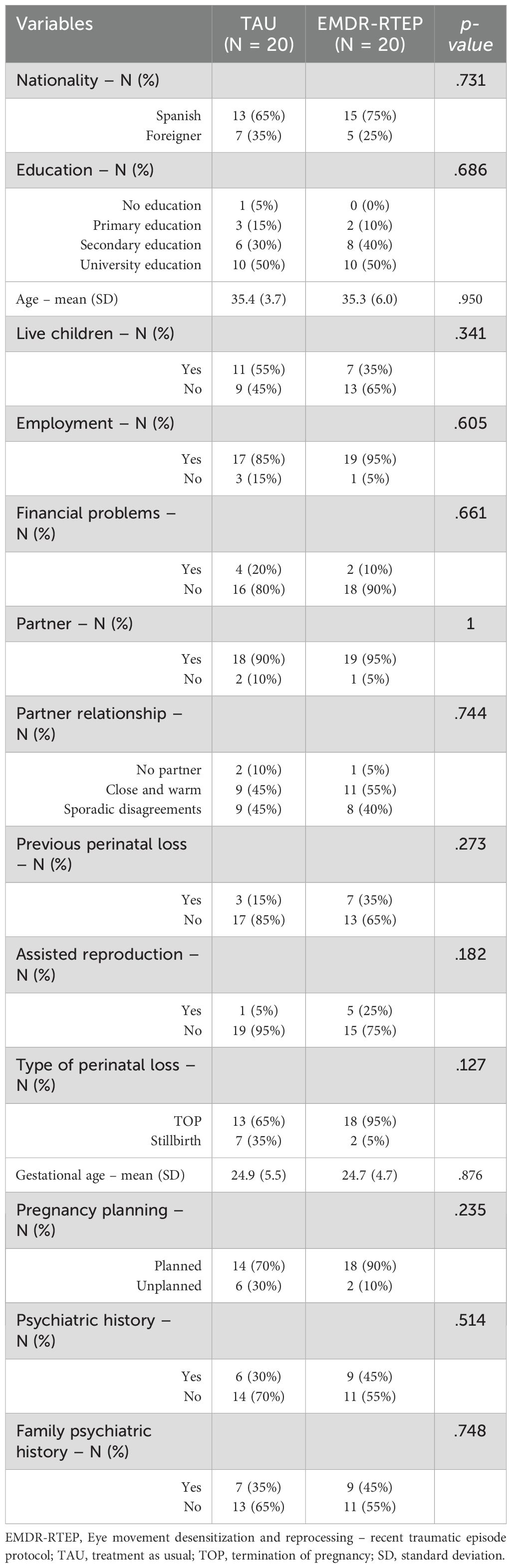
Table 1. Baseline characteristics.
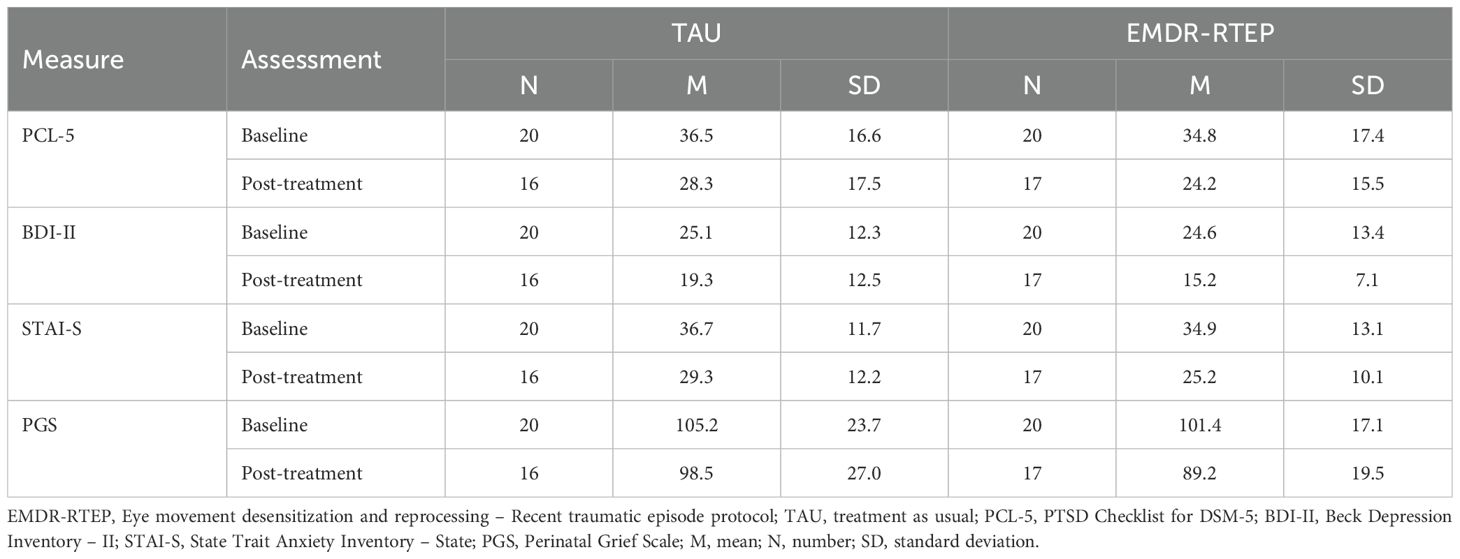
Table 2. Mean scores on outcome measures in each group at baseline and post-treatment.
3.2 Intervention outcomes
The ANCOVA models with imputed data showed no statistically significant differences between the two intervention groups (EMDR-RTEP and TAU) in post-traumatic (F[1,37] = 0.99, p = .324, ηp² = .03), depressive (F[1,37] = 1.69, p = .201, ηp² = .04), anxious (F[1,37] = 1.44, p = .238, ηp² = .04), or perinatal grief (F[1,37] = 3.28, p = .078, ηp² = .08) symptoms. Figure 2 shows the estimated marginal means from the ANCOVA models and adjusted mean differences between the EMDR-RTEP and TAU groups, with lower scores in all intervention outcomes in the EMDR-RTEP group compared to TAU, although these differences were not statistically significant. Sensitivity analysis using complete case data yielded results consistent with the primary analysis (Supplementary Material, Supplementary Figure 1).
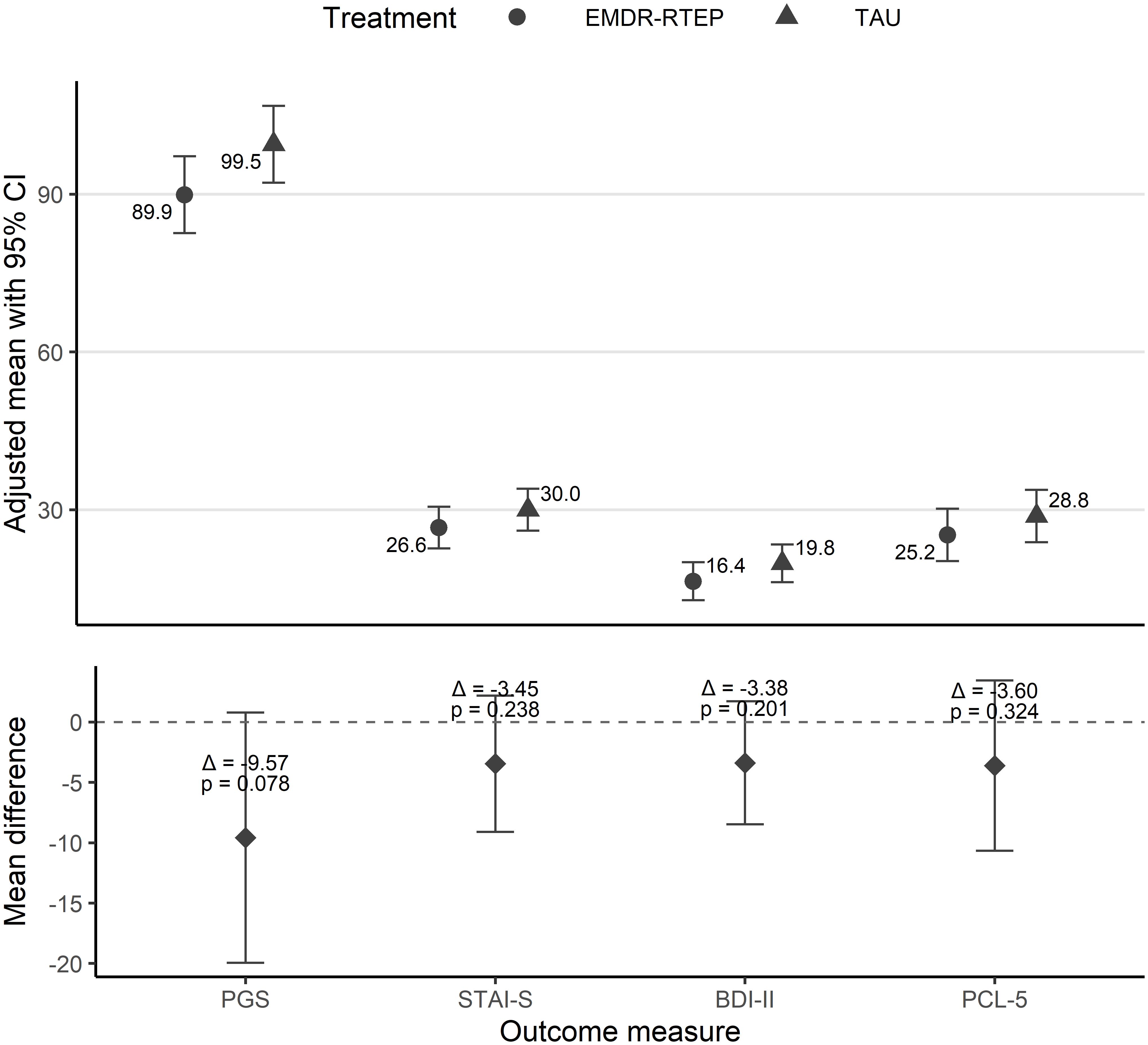
Figure 2. Differences between EMDR-RTEP and TAU on outcome scores post-treatment in the intention-to-treat analysis. Estimated marginal means from ANCOVA models adjusted for baseline scores. Adjusted mean differences between EMDR-RTEP and TAU. Negative values favor EMDR-RTEP, while positive values favor TAU. 0 = no differences. EMDR-RTEP: Eye Movement Desensitization and Reprocessing – Recent traumatic episode; TAU: treatment-as-usual; PCL-5: PTSD Checklist for DSM-5; BDI-II: Beck Depression Inventory – II; STAI-S: State Trait Anxiety Inventory – State; PGS: Perinatal Grief Scale.
3.3 Satisfaction with the treatment received
Figure 3 shows the distribution of the scores of the satisfaction scale (CRES-4). Non-parametric mean difference tests showed no significant differences between groups in relation to satisfaction (U = 90, p = .071) or problem solution (U = 125.5, p = .673). However, patients who received the EMDR-RTEP reported a higher perceived change than those who received TAU (U = 69.5, p = .011).
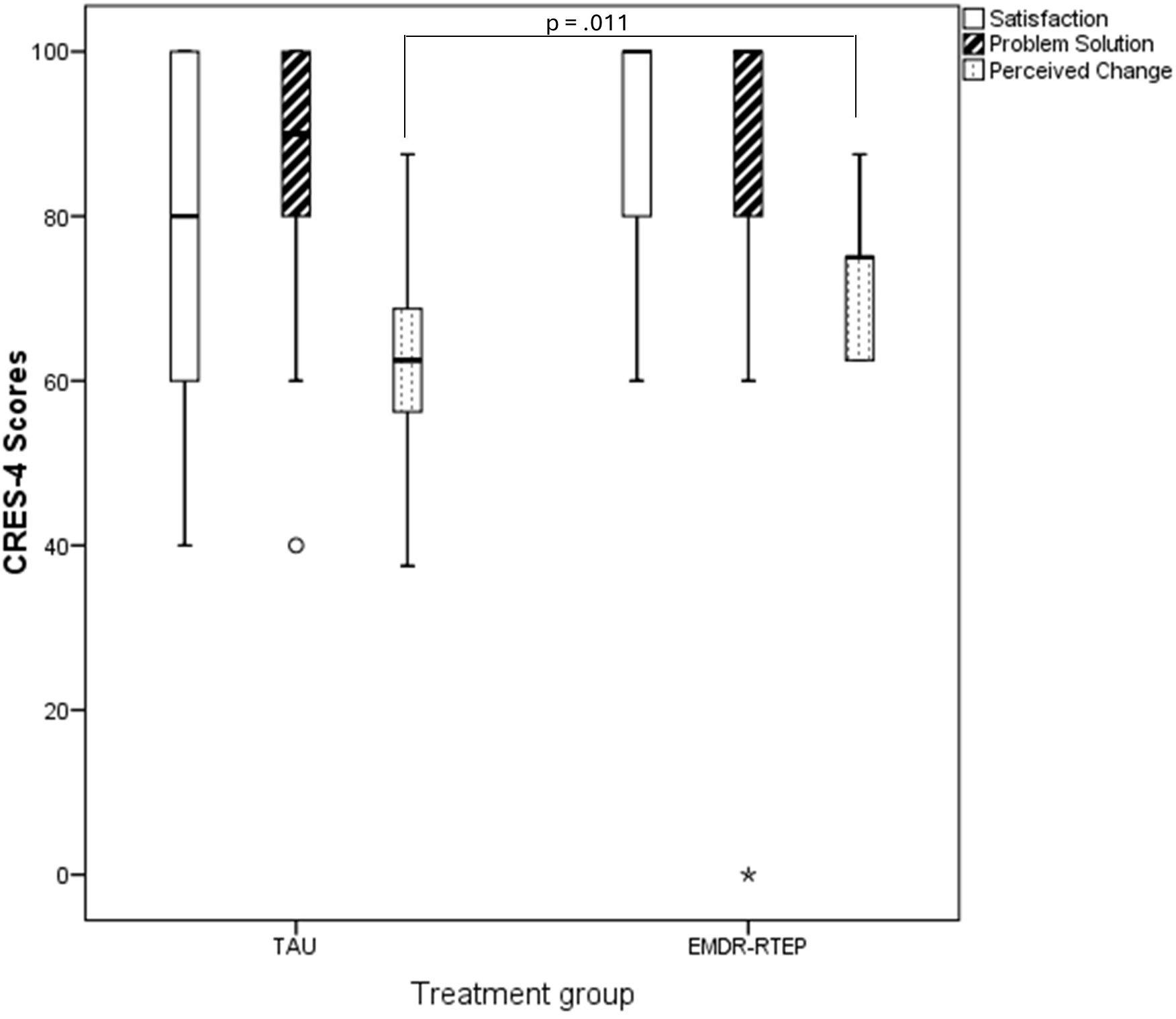
Figure 3. Distribution of satisfaction scale scores (CRES-4) by group. EMDR-RTEP, Eye Movement Desensitization and Reprocessing – Recent traumatic episode protocol; TAU, treatment-as-usual; CRES-4, Consumer Reports Effectiveness Score.
4 Discussion
To our knowledge, this is the first study to evaluate and compare the feasibility and preliminary effectiveness of an early EMDR intervention with a TAU intervention control group for the treatment and prevention of post-traumatic symptoms following perinatal loss. The control group received psychological grief counseling, and non-trauma-focused cognitive-behavioral techniques.
Both groups showed a trend toward decreased scores post-treatment compared to baseline. At post-treatment assessment, the EMDR-RTEP group had lower scores in all outcomes compared to the TAU group, although these differences were not statistically significant. Both treatments were well-tolerated, with no significant adverse effects directly related to the interventions. Mothers were generally satisfied with the treatment received, although those who received the EMDR-RTEP reported greater perceived emotional change compared to those who received TAU, being the only result achieving statistical significance.
The goal of a pilot study is to evaluate the feasibility of an intervention and estimate the potential effect size to help in the design of a larger definitive trial (30). This justifies the use of less conservative confidence intervals (CI) (e.g., 85% or 75%) along with the minimum clinically important difference (MCID) (30). The MCID is typically set at 3 for the BDI-II (31), while recent studies suggest 9 for the PCL-5 (32) and 10 for the STAI-S (33, 34). Considering the CIs for mean differences between the EMDR-RTEP and TAU, the 75% CI for BDI-II scores (0.3–6.4) excludes 0 and includes the MCID. The 85% and 75% CI for PGS scores ([1.8–17.3] and [3.4–15.7], respectively) both exclude 0. Although the MCID for this scale is unknown, the differences are likely to be clinically significant. This corresponds to a medium effect size (ηp² = .08). Additionally, women who received the EMDR-RTEP reported greater perceived emotional change than those who received TAU. These findings suggest that early EMDR intervention may be more beneficial than psychological interventions involving grief counseling, and non-trauma-focused cognitive-behavioral techniques for women experiencing perinatal loss. Surprisingly, the trend towards improvement seemed less evident in post-traumatic symptoms and greater in secondary outcomes, such as depressive symptoms and the intensity of perinatal grief. This hypothesis should be tested in a larger clinical trial.
Compared to previous studies on psychological therapy, prior trials have shown that cognitive-behavioral therapy (10, 11) yields beneficial results in preventing or treating post-traumatic symptoms in perinatal grief. However, in contrast to our study, the comparison group did not receive an active psychological intervention.
From a clinical perspective, this pilot study highlights the importance of integrating trauma-focused treatments into perinatal mental health care, particularly for interventions in women who have suffered a recent perinatal loss. The study also supports the acceptability of EMDR-RTEP in this context, with high levels of treatment adherence and satisfaction among participants. In terms of research implications, these preliminary results provide a strong rationale for conducting a larger, multicenter, randomized controlled trial to assess the efficacy of EMDR-RTEP, exploring long-term outcomes, and examining the effects of this protocol on other domains, such as perinatal grief intensity and comorbid symptoms. Future studies should also consider incorporating qualitative methodologies to capture the subjective experiences of patients.
This randomized controlled trial has several strengths. Firstly, the use of a control group (TAU) allowed direct comparison of the effects of the EMDR-RTEP intervention with those of standard psychological treatment, including psychoeducation and cognitive behavioral techniques. Both interventions were delivered by psychologists with expertise in perinatal mental health. However, this pilot trial also has several limitations. Firstly, the sample size was small, and the study was conducted at a single center, which may limit the generalizability of the findings. A definitive trial with a larger sample size and multicenter design is required to increase external validity and control for therapist-related effects. Secondly, while both groups received structured psychological interventions, the EMDR-RTEP intervention was delivered by one therapist, whereas the TAU sessions were delivered by other psychologists. The therapists were not randomized and, although they all had comparable clinical experience in perinatal mental health, differences in their therapeutic styles and rapport may have influenced the outcomes. Thirdly, the number of sessions received differed significantly between the two groups: on average, the EMDR-RTEP group received one more session than the TAU group. This difference may have contributed to the effects observed. Fourthly, symptom improvement was assessed using standardized self-reported scales administered before and after the intervention, which may not fully capture the therapeutic process. Additionally, we used a brief satisfaction scale to assess participants’ perceptions of the intervention, which may be insufficient for evaluating treatment impact. Future studies would benefit from incorporating qualitative methodologies to explore patients’ experiences and perceived changes in greater depth. Lastly, for ethical reasons, the control group in our study received active psychological treatment, and thus, we lack a comparison between the EMDR-RTEP and no treatment or a waiting list.
5 Conclusion
It is important to expand the evidence base for psychological treatments for perinatal grief, particularly for post-traumatic symptoms following perinatal loss. This pilot study shows that the intervention is feasible, well accepted, and tolerated by participants, with adequate satisfaction levels. It requires a slightly higher number of psychological visits compared to routine treatment and involves specific training. Although there was no clear trend towards improvement in post-traumatic symptoms, the intervention yielded promising results on secondary outcomes, particularly in reducing depressive symptoms and the intensity of perinatal grief. These findings warrant further investigation in larger, controlled trials.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Comité de Ética de la Investigación con Medicamentos, Hospital Clínic, Barcelona, Spain. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
BS-C: Writing – original draft, Investigation, Methodology, Conceptualization, Writing – review & editing, Supervision. CG-G: Investigation, Writing – review & editing. AmM: Investigation, Writing – review & editing. YG: Writing – review & editing, Investigation. XS: Writing – review & editing, Investigation. AiM: Investigation, Writing – review & editing. EG: Formal Analysis, Writing – review & editing, Investigation. AR-L: Investigation, Writing – review & editing. AT-G: Methodology, Formal Analysis, Supervision, Investigation, Conceptualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This study received funding from EMDR Europe (Grant number: 2022-03). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Acknowledgments
We thank all the participants involved in our study. We also thank Dr José Rios for the statistical support, and Donna Pringle for the English revision of the manuscript. We thank all professionals from the GADP (Hospital Clinic Barcelona, Spain).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1593306/full#supplementary-material.
Abbreviations
EMDR, Eye Movement Desensitization and Reprocessing; EMDR-RTEP, Eye Movement Desensitization and Reprocessing– Recent Traumatic Episode Protocol; TAU, Treatment-as-usual. In this study it refers to an active psychological intervention; PTSD, Post-traumatic stress disorder; PCL-5, PTSD Checklist for DSM-5; BDI-II, Beck Depression Inventory - II; STAI, State Trait Anxiety Inventory; PGS, Perinatal Grief Scale; CRES-4, Consumer Reports Effectiveness Score; BOCF, baseline-observation-carried-forward; SD, Standard deviation; CI, confidence interval; ANCOVA, analysis of covariance; MCID, minimum clinically important difference.
References
1. Heazell AEP, Siassakos D, Blencowe H, Burden C, Bhutta ZA, Cacciatore J, et al. Stillbirths: Economic and psychosocial consequences. Lancet. (2016) 387:604–16. doi: 10.1016/S0140-6736(15)00836-3
2. Cuenca D. Pregnancy loss: Consequences for mental health. Front Glob Womens Health. (2023) 3:1266931. doi: 10.3389/fgwh.2023.1266931
3. Hunter A, Tussis L, and MacBeth A. The presence of anxiety, depression and stress in women and their partners during pregnancies following perinatal loss: A meta-analysis. J Affect Disord. (2017) 223:153–64. doi: 10.1016/j.jad.2017.07.004
4. Mendes DCG, Fonseca A, and Cameirão MS. The psychological impact of Early Pregnancy Loss in Portugal: incidence and the effect on psychological morbidity. Front Public Health. (2023) 11:1188060. doi: 10.3389/fpubh.2023.1188060
5. Schobinger E, Stuijfzand S, and Horsch A. Acute and post-traumatic stress disorder symptoms in mothers and fathers following childbirth: A prospective cohort study. Front Psychiatry. (2020) 11:562054. doi: 10.3389/fpsyt.2020.562054
6. Daugirdaitė V, van den Akker O, and Purewal S. Posttraumatic stress and posttraumatic stress disorder after termination of pregnancy and reproductive loss: a systematic review. J Pregnancy. (2015) 2015:646345. doi: 10.1155/2015/646345
7. Hunter A, Tussis L, and MacBeth A. The presence of anxiety, depression and stress in women and their partners during pregnancies following perinatal loss: A meta-analysis. J Affect Disord. (2017) 223:153–64. doi: 10.1016/j.jad.2017.07.004
8. Shaohua L and Shorey S. Psychosocial interventions on psychological outcomes of parents with perinatal loss: A systematic review and meta-analysis. Int J Nurs Stud. (2021) 117:103871. doi: 10.1016/j.ijnurstu.2021.103871
9. Hollins Martin CJ and Reid K. A scoping review of therapies used to treat psychological trauma post perinatal bereavement. J Reprod Infant Psychol. (2023) 41:582–98. doi: 10.1080/02646838.2021.2021477
10. Kersting A, Kroker K, Schlicht S, Baust K, and Wagner B. Efficacy of cognitive behavioral internet-based therapy in parents after the loss of a child during pregnancy: pilot data from a randomized controlled trial. Arch Womens Ment Health. (2011) 14:465–77. doi: 10.1007/s00737-011-0240-4
11. Kersting A, Dölemeyer R, Steinig J, Walter F, Kroker K, Baust K, et al. Brief Internet-Based Intervention Reduces Posttraumatic Stress and Prolonged Grief in Parents after the Loss of a Child during Pregnancy: A Randomized Controlled Trial. Psychother Psychosom. (2013) 82:372–81. doi: 10.1159/000348713
12. Navidian A, Saravani Z, and Shakiba M. Impact of psychological grief counseling on the severity of post-traumatic stress symptoms in mothers after stillbirths. Issues Ment Health Nurs. (2017) 38:650–4. doi: 10.1080/01612840.2017.1315623
13. Huberty J, Sullivan M, Green J, Kurka J, Leiferman J, Gold K, et al. Online yoga to reduce post traumatic stress in women who have experienced stillbirth: a randomized control feasibility trial. BMC Complement Med Ther. (2020) 20:1–19. doi: 10.1186/s12906-020-02926-3
14. Berliner L, Bisson J, Cloitre M, Forbes D, Goldbeck L, Jensen T, et al. Posttraumatic stress disorder prevention and treatment guidelines: methodology and recommendations (2019). Available online at: https://istss.org/getattachment/Treating-Trauma/New-ISTSS-Prevention-and-Treatment-Guidelines/ISTSS_PreventionTreatmentGuidelines_FNL-March-19-2019.pdf.aspx (Accessed March 3, 2025).
15. Management of Posttraumatic Stress Disorder and Acute Stress Disorder Work Group. VA/doD clinical practice guideline for management of posttraumatic stress disorder and acute stress disorder. Washington, DC: U.S. Government Printing Office (2023).
16. National Institute for Health and Clinical Excellence (NICE). Post-traumatic stress disorder: NICE guidance (2018). Available online at: https://www.nice.org.uk/guidance/ng116 (Accessed March 3, 2025).
17. Phoenix Australia. Australian guidelines for the prevention and treatment of acute stress disorder (ASD), posttraumatic stress disorder (PTSD) and complex PTSD (2020). Available online at: https://www.phoenixAustralia.org/Australian-guidelines-for-ptsd/ (Accessed November 14, 2023).
18. Torres-Giménez A, Garcia-Gibert C, Gelabert E, Mallorquí A, Segu X, Roca-Lecumberri A, et al. Efficacy of EMDR for early intervention after a traumatic event: A systematic review and meta-analysis. J Psychiatr Res. (2024) 174:73–83. doi: 10.1016/J.JPSYCHIRES.2024.04.019
19. Lenferink LIM, de Keijser J, Smid GE, and Boelen PA. Cognitive therapy and EMDR for reducing psychopathology in bereaved people after the MH17 plane crash: Findings from a randomized controlled trial. Traumatology (Tallahass Fla). (2020) 26:427–37. doi: 10.1037/trm0000253
20. van Denderen M, de Keijser J, Stewart R, and Boelen PA. Treating complicated grief and posttraumatic stress in homicidally bereaved individuals: A randomized controlled trial. Clin Psychol Psychother. (2018) 25:497–508. doi: 10.1002/cpp.2183
21. Spicer L. Eye Movement Desensitisation and Reprocessing (EMDR) therapy for prolonged grief: theory, research, and practice. Front Psychiatry. (2024) 15:1357390/BIBTEX. doi: 10.3389/FPSYT.2024.1357390/BIBTEX
22. Chiorino V, Cattaneo MC, Macchi EA, Salerno R, Roveraro S, Bertolucci GG, et al. The EMDR Recent Birth Trauma Protocol: a pilot randomised clinical trial after traumatic childbirth. Psychol Heal. (2020) 35:795–810. doi: 10.1080/08870446.2019.1699088
23. Kunselman AR. A brief overview of pilot studies and their sample size justification. Fertil Steril. (2024) 121:899–901. doi: 10.1016/J.FERTNSTERT.2024.01.040
24. Shapiro E and Laub B. The recent traumatic episode protocol (R-TEP): an integrative protocol for early EMDR intervention (EEI). In: Implementing EMDR early mental health interventions for man-made and natural disasters. Springer Publishing, New York, NY (2014). p. 193–215.
25. Weathers FW, Litz BT, Keane TM, Palmieri PA, Marx BP, and Schnurr PP. The PTSD checklist for DSM-5 (PCL-5). National Center for PTSD (2013). Available at: http://www.ptsd.va.gov (Accessed March 3, 2025).
26. Beck AT, Steer RA, and Brown GK. Beck depression inventory. 2nd ed. San Antonio: The Psychological Corporation (1996).
27. Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, and Jacobs GA. Manual for the state-trait anxiety inventory. Palo Alto, CA: Consulting Psychologist Press (1983).
28. Potvin L, Lasker J, and Toedter L. Measuring grief: A short version of the perinatal grief scale. J Psychopathol Behav Assess. (1989) 11:29–45. doi: 10.1007/BF00962697
29. Nielsen SL, Smart DW, Isakson RL, Worthen VE, Gregersen AT, and Lambert MJ. The consumer reports effectiveness score: What did consumers report? J Couns Psychol. (2004) 51:25–37. doi: 10.1037/0022-0167.51.1.25
30. Lee EC, Whitehead AL, Jacques RM, and Julious SA. The statistical interpretation of pilot trials: should significance thresholds be reconsidered? BMC Med Res Methodol. (2014) 14. doi: 10.1186/1471-2288-14-41
31. Button KS, Kounali D, Thomas L, Wiles NJ, Peters TJ, Welton NJ, et al. Minimal clinically important difference on the Beck Depression Inventory–II according to the patient’s perspective. Psychol Med. (2015) 45:3269–79. doi: 10.1017/S0033291715001270
32. Blanchard BE, Johnson M, Campbell SB, Reed DE, Chen S, Heagerty PJ, et al. Minimal important difference metrics and test-retest reliability of the PTSD Checklist for DSM-5 with a primary care sample. J Trauma Stress. (2023) 36:1102–14. doi: 10.1002/JTS.22975
33. Knudsen NI, Richter R, Kentenich H, Sehouli J, and David M. Anxiety of myoma patients: results of standardized interviews with the State Trait Anxiety Inventory and the Kessler 10 questionnaire. J Psychosom Obstet Gynaecol. (2020) 41:122–30. doi: 10.1080/0167482X.2019.1624951
Keywords: EMDR recent traumatic episode protocol, stillbirth, perinatal loss, post-traumatic symptoms, PTSD, perinatal grief
Citation: Sureda-Caldentey B, Garcia-Gibert C, Martínez A, Giménez Y, Segú X, Mallorquí A, Gelabert E, Roca-Lecumberri A and Torres-Giménez A (2025) Effectiveness of an eye movement desensitization and reprocessing intervention for the prevention of post- traumatic symptoms in perinatal loss: a randomized pilot controlled trial. Front. Psychiatry 16:1593306. doi: 10.3389/fpsyt.2025.1593306
Received: 13 March 2025; Accepted: 23 May 2025;
Published: 09 June 2025.
Edited by:
Chonnakarn Jatchavala, Prince of Songkla University, ThailandReviewed by:
Darpan Kaur, Mahatma Gandhi Missions Medical College and Hospital, IndiaSarah El Halabi, Columbia University, United States
Poom Chompoosri, Mae Fah Luang University, Thailand
Copyright © 2025 Sureda-Caldentey, Garcia-Gibert, Martínez, Giménez, Segú, Mallorquí, Gelabert, Roca-Lecumberri and Torres-Giménez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna Torres-Giménez, YXRvcnJlc2dAY2xpbmljLmNhdA==