 Jingxian Yu
Jingxian Yu Mingjie Wu1,2†
Mingjie Wu1,2† Huan Peng
Huan Peng Hanjiao Liu
Hanjiao Liu- 1Shenzhen Clinical College of Integrated Chinese and Western Medicine, Guangzhou University of Chinese Medicine, Shenzhen, China
- 2The Seventh Clinical Medical College of Guangzhou University of Chinese Medicine, Shenzhen, China
- 3Fujian University of Traditional Chinese Medicine, Fuzhou, China
Introduction: Death anxiety is a critical mental-health concern among young adults; however, its heterogeneity and underlying psychological mechanisms remain understudied. This study aimed to identify latent profiles of death anxiety in Chinese youth and examine the predictive roles of self-esteem, perceived social support, and security.
Methods: We conducted a cross-sectional survey of 623 young adults (mean age = 23.62 years, SD = 3.61) aged 18–35 years in mainland China. Latent profile analysis (LPA) was conducted to classify death anxiety subgroups based on responses to the Templer Death Anxiety Scale (C-T-DAS). Self-esteem, perceived social support, and sense of security were assessed using validated scales. Multinomial logistic regression and ANOVA were used to explore predictors and group differences.
Results: Three latent death anxiety profiles emerged, High Death Anxiety (56.2%), Moderate Cognition and Low Death Anxiety (8.8%), and Low Cognition and Moderate Death Anxiety (35%). Higher self-esteem (β = -0.46, p <.001), social support (β = -1.12, P = .004), and security (β = -2.87, P <.001) significantly predicted lower death anxiety. The high death anxiety group exhibited the lowest psychological resource scores. Older age (30–35 years) and recent acute illness recovery were associated with higher death anxiety risk (OR = 0.28, 95% CI [0.09, 0.93]). Security showed the strongest inverse association with DA (F = 50.72, P <.001), particularly in the interpersonal and controllability dimensions.
Conclusion: Death anxiety among young adults is heterogeneous, influenced by distinct psychological profiles and demographic factors. Interventions should prioritize enhancing self-esteem, social support networks, and security to mitigate death anxiety, especially in high-risk subgroups. Future research should employ longitudinal designs and cross-cultural samples to validate causal pathways and refine targeted strategies.
1 Introduction
Against accelerated globalization and social uncertainty, Chinese youth (18–35) face academic, professional, and social pressures that threaten mental health, while modern media repeatedly expose them to death-related images (e.g., COVID-19 mortality) (1–6). At this identity-forming stage, such exposure heightens death anxiety (DA), which—if unaddressed—can precipitate social withdrawal, loss of meaning, and depressive mood (7–10).
Death anxiety is a fundamental psychological phenomenon characterized by fear and worry about one’s own death or that of others, typically manifesting as intense distress and emotional reactions related to dying, uncertainty about what happens after death, and similar themes (11). It has been identified as a significant factor associated with a variety of mental health problems, including generalized anxiety disorder, depression, obsessive-compulsive disorder, panic disorder, and schizophrenia (10, 12, 13). Additionally, death anxiety is thought to influence the development of several somatic symptom disorders, such as muscle dysmorphia and other medically unexplained symptoms (13, 14).
Empirical studies have shown that high death anxiety may affect an individual’s health behaviors, such as decreased sleep quality and loss of appetite, and that these behavioral changes may further impair somatic health and exacerbate death anxiety (14, 15). Certain occupational groups, such as doctors, nurses, and embalmers, are subject to greater psychological stress due to occupational characteristics that require frequent exposure to death scenes. This stress can exacerbate their death anxiety, which in turn negatively affects their professional identity, self-efficacy, and self-confidence. This not only reduces the quality of their response to the needs of the patient or dying person but may also cause secondary victimization of the patient or bereaved person in their care (16, 17).
Despite its importance, the existing literature on death anxiety has primarily focused on older adults, terminally ill patients, and healthcare professionals (18–20). Limited attention has been given specifically to young adults, who may experience unique vulnerabilities due to the critical developmental tasks they face, including identity formation and value establishment (21). Furthermore, previous studies have predominantly adopted variable-centered approaches, analyzing the linear relationship between death anxiety and single variables. This approach often overlooks the heterogeneity within youth populations, neglecting the fact that different individuals may develop differentiated anxiety patterns through unique combinations of psychological profiles, such as varying levels of self-esteem, perceived social support, and security (22).
Previous research has explored a variety of psychological factors that influence death anxiety. In the context of Chinese youth facing conflicting traditional and modern death-related beliefs, Terror Management Theory (TMT) provides an important theoretical framework, suggesting that individuals alleviate death anxiety by reinforcing cultural worldviews, maintaining self-esteem, and building close relationships, collectively referred to as the “Death Anxiety-Buffer System” (DABS) (23). However, young people in Mainland China are currently undergoing a period of cultural worldview adjustment, and the conflict between traditional and modern concepts has led to the fragility of the buffer system, which has weakened its mitigating effect on death anxiety. For example, the tension between traditional Confucian views (e.g., “without knowing life, how to know death”) and modern death-related information (e.g., media reports of epidemics) may weaken the effectiveness of these buffering mechanisms and make individuals more vulnerable to death anxiety (24). Despite the impact of the macro-cultural context on the death anxiety buffering system, individual-level factors favoring the alleviation of death anxiety still play an important role.
Therefore, rather than conducting a comprehensive assessment of death anxiety as a single factor, this study specifically focuses on identifying its heterogeneous profiles among young adults and examining how key psychological resources predict these profiles.
To address these research gaps, this study employs a person-centered approach using latent profile analysis (LPA) to explore heterogeneity in death anxiety among young adults. This method allows for the identification of distinct subgroups characterized by unique psychological profiles (25). Additionally, we investigate the predictive roles of self-esteem, perceived social support, and security, which are theoretically suggested to be crucial buffers against death anxiety (26, 27). By providing a nuanced understanding of death anxiety manifestation among youth, our findings aim to inform targeted psychological interventions and enhance mental health support specifically tailored to young adults.
Self-esteem refers to how people evaluate themselves, including the way they view themselves, the respect they have for themselves, and the appreciation of their value in specific areas (28). Terror Management Theory suggests that chasing meaning provided by cultural worldviews and maintaining self-esteem can give a sense of worth and alleviate anxiety, which can help manage death-related anxiety (29). A large body of data demonstrates that self-esteem serves as a buffering mechanism to help individuals withstand damage from death anxiety. Belmi et al.’s experiments demonstrated that death salience motivates people to increase their sense of security and self-evaluation to manage death anxiety by, for example, seeking psychological security and enhancing self-esteem (27). At the same time, Zhang et al. observed that by reviewing successful experiences and searching for the meaning of life, individuals can gain affirmation of their value and significance, thus reducing anxiety caused by the inevitability of death (30).
Social support is defined as the feeling that a person is cared for, respected, and valued, and usually consists of both practical support (receiving support) and perceived support (31). Actual support includes receiving material assistance and direct services from others; while perceived support refers to an individual’s emotional experience of being respected, understood, and supported (32). Given its predictive function of individual psychological distress and psychological resilience, perceived social support plays a key role in maintaining an individual’s level of mental health (33). Death anxiety, a pervasive and numerous potentially harmful psychological disorder, has also been shown to be moderated by an individual’s ability to perceive social support (34).
An individual’s sense of security consists of two dimensions: external security and internal security (35). External security involves an assessment of the perceived safety and stability of the environment, including public order, interpersonal relationships, welfare systems, and resources (36–38); internal security is the individual’s subjective feeling of being physically and psychologically free from threat (39). In addition, the sense of control and psychological consistency also affect the individual’s perception of his or her safety, and enhance the confidence in coping with stress and difficulties (40, 41). It has been found that the sense of security is an important indicator and manifestation of mental health, and when an individual’s external or internal sense of security is impaired, he or she is prone to mental health problems such as severe stress, depression, anxiety, and post-traumatic stress disorder (42–44). Ottu et al. investigated and found that after experiencing a life-threatening security event, those who value their lives based on a higher quality of life are more sensitive to the threat to their sense of security and controllability in their lives and more likely to manifest their feelings of security and control over their lives. Threatened were more sensitive and more likely to show significant anxiety about death (45). In addition, Scheffold et al. have argued that people who are insecure in their interpersonal relationships exhibit more severe death anxiety due to trust barriers or lack of appreciation of others’ willingness to assist (46).
Despite the links that have been established between these psychological factors and death anxiety, the majority of existing studies have adopted a variable-centered approach, which focuses on analyzing the linear relationship between death anxiety and a single variable, such as finding that social support is negatively associated with death anxiety and that levels of self-esteem buffer anxiety (47), rather than exploring individual differences in the manifestations of death anxiety (48). However, such approaches struggle to capture the heterogeneity of youth populations, ignoring the fact that different individuals may develop differentiated patterns of anxiety through a combination of psychological profiles (e.g., high self-esteem but low security, low social support but high sense of meaning) (49). This neglect of individual differences makes existing intervention strategies for youth death anxiety often lacking in relevance.
Furthermore, while existing studies have provided valuable insights into death anxiety in specific groups such as older adults and healthcare professionals, there remains a significant gap in understanding the heterogeneity of death anxiety among young adults in Mainland China. This gap limits the development of targeted psychological interventions. Theoretically, integrating Terror Management Theory with person-centered approaches like Latent Profile Analysis can elucidate how different psychological buffers (e.g., self-esteem, perceived social support, security) interact within subgroups to mitigate death anxiety. Practically, identifying these distinct profiles can inform more precise and effective mental health support strategies for youth facing existential challenges.
Therefore, the present study aimed to identify heterogeneous patterns of death anxiety among Chinese young adults using latent profile analysis, and to examine the predictive roles of self-esteem, perceived social support, and security. By adopting a person-centered approach, this study sought to provide a more nuanced understanding of how different psychological resources function as protective factors against death anxiety, thereby offering evidence to inform youth-targeted interventions and death education strategies.
Based on the above rationale, we proposed the following hypotheses:
H1: Death anxiety among young adults exhibits heterogeneity and can be empirically classified into distinct latent profiles.
H2: Higher levels of self-esteem, perceived social support, and security are negatively associated with death anxiety and predict membership in lower-anxiety profiles.
H3: Among these psychological resources, security has the strongest protective effect against death anxiety.
H4: Demographic variables such as older age (30–35 years) and recent recovery from acute illness are positively associated with membership in higher death anxiety profiles.
2 Methods
2.1 Study design and setting
This project is a cross-sectional study and a convenience sampling method was used. All materials for this study were collected from November 2023 to May 2024 through questionnaires distributed in community health and hygiene centers and community residents’ activity centers in Shenzhen and Shaoguan.
2.2 Participants
To reduce regional heterogeneity and health-related confounding, we restricted recruitment to community-dwelling young adults in mainland China who were in stable physical and mental health. Detailed eligibility criteria are listed below:
2.2.1 Inclusion criteria
1. Young adults aged between 18 and 35 years;
2. Informed consent and voluntary participation in this study;
3. Given the differences in culture, policy, and economy, participants in this study were limited to residents of mainland China (excluding Taiwan, Hong Kong, and Macao).
2.2.2 Exclusion criteria
1. Those who were unable to cooperate with the survey due to abnormal intelligence or thinking, which could not be assessed by the Simple Intellectual Mental State Scale (total score<24) (50);
2. Those suffering from serious diseases or vital organ dysfunction, such as malignant tumors, heart, liver, and kidney dysfunction;
3. Suffering from diagnosed serious mental illness (e.g., major depression, schizophrenia, etc.) (51, 52);
4. Those who have text reading disorder and cannot understand the content of the questionnaires.
2.2.3 Recruitment and sampling
In this survey, the convenience sampling method was implemented in several community sites in Shenzhen and Shaoguan. We approached a diverse set of individuals within the target age range (different occupations, education levels, and health statuses). Confidentiality and informed consent were emphasized to promote participation and data quality; the achieved sample exceeded the minimum a priori requirement.
2.3 Sample size calculation
The sample size for this study was determined using multiple methods, and the largest estimated sample size was selected as the primary reference, adjusted for an expected 10% invalid response rate.
2.3.1 Estimation based on mean and standard deviation of death anxiety
Based on previous studies using the Chinese version of the Templer Death Anxiety Scale (C-T-DAS) (53), the mean Death Anxiety score among Chinese university students was 7.83 ± 2.90 (54). With a 95% confidence level (Z = 1.96) and an allowable margin of error of 0.3 points, the required sample size was calculated as follows (55):
2.3.2 Sample size requirements for latent profile analysis
According to previous simulation studies, conducting an LPA generally requires at least 50–70 participants per identified latent profile, recommending a total sample size typically between 300 and 500 (56). Conservatively estimating up to 5 profiles yields a recommended maximum sample size of 500.
2.3.3 Sample size requirements for multinomial logistic regression
An a priori power analysis for multinomial logistic regression was also conducted using G*Power 3.1.9.7 (57). Assuming a medium-to-large effect size (F² = 0.25), α = 0.05, power = 0.80, and including 8 predictors, the minimum required sample size was calculated to be approximately 248.
Considering the highest calculated sample size (n = 500, from LPA requirements) and adjusting for an anticipated 10% invalid response rate, the final target sample size was set as follows:
Based on the calculated minimum sample size of 556, we successfully recruited 623 participants, which represents a 12% increase over the required minimum. This over-recruitment was strategic to account for potential data loss or non-response and to better represent the diverse population of young adults in the study area. Specifically, our recruitment efforts were focused on ensuring a wide range of participants in terms of age, gender, occupation, and health status. This approach not only enhanced the statistical power of our analysis but also improved the generalizability of our findings to the broader population of young adults in mainland China. The recruitment process was carefully monitored to ensure that participants were representative of the target population, and the final sample size was approved by the Ethics Committee of the Seventh Clinical Medical College of Guangzhou University of Traditional Chinese Medicine (No. KY-2024-026-01).
2.4 Measures
2.4.1 General information questionnaire
Basic information about the participants was collected through a self-developed demographic scale, including gender, age, race, education, occupation, income level, health status, religious beliefs, and life education experiences. Religiosity was measured with a single, binary item (yes/no), a choice dictated by the modest and heterogeneous distribution of religious affiliations in our sample. We acknowledge that this coarse operationalization may fail to adequately capture the nuanced landscape of religious and spiritual beliefs within the Chinese context.
2.4.2 Death anxiety scale
The Templer Death Anxiety Scale (T-DAS) is a self-reported psychometric instrument used by participants (58). It was originally developed by Templer in 1970 and later translated into Chinese and culturally adapted by Chinese scholar Yang Hong in 2003, resulting in the Chinese version of the Templer Death Anxiety Scale (53). The scale consists of 15 items, which can be categorized into four dimensions, including I. Effect (which expresses the individual’s emotions towards experiences and/or views related to death), items: 1, 3, 5, 10, 13, 14; II. Stress and distress (manifesting the individual’s feelings of stress and distress related to death), questions: 4, 6, 9, 11; III. Time Awareness (demonstrating the individual’s attitude toward time and the passage of life), questions 8, 12; and IV. Cognition (which expresses the individual’s perception of survival and death), items 2, 7, and 15. The instrument consists of nine positively scored questions, with a “true” choice indicating a one-point increase; and six negatively scored questions (items 2, 3, 5, 6, 7, and 15), with a “false” choice indicating a one-point increase. The scale has a total score of 15, with 7 being the standard threshold for high death anxiety. The Chinese version (C-T-DAS) has demonstrated good reliability and validity in previous Chinese studies (59). The Cronbach’s alpha for this instrument in this study was 0.726.
2.4.3 Self-esteem scale
The Self-Esteem Scale (SES) was developed by Rosenberg in 1965 (60). In this study, we used the translated and culturally validated Chinese version, which was adapted by Ji Yifu and Yu Xin in 1999 (61). The scale consists of 10 items, including five positively and five negatively worded items. Although Rosenberg supported the use of positive scoring for topics 1, 2, 4, 6, and 7; and reverse scoring for items 3, 5, 8, 9, and 10. However, based on the study of the available information, we insisted that this scale is a single-dimension measurement tool. Besides, Tian, after fully considering the adaptability of the questions in the Chinese context, proposed that maintaining the forward scoring would enable item 8 to obtain better detection results (62). This instrument utilizes a Likert 4-point scale ranging from 1 (strongly disagree) to 4 (strongly agree). The total score is 10-40, with higher scores representing higher levels of overall self-esteem. The Chinese version has established reliability and validity in prior research with Chinese samples (63). In this study, the Cronbach’s alpha (α) for this instrument was 0.850.
2.4.4 Perceived social support scale
The Perceived Social Support Scale (PSSS) was designed by Zimet et al. in 1988 (64). In this project, we used the Chinese version of the PSSS translated by Jiang Qinjin in 2001 to adapt it for Chinese cultural context (65). This scale has 12 items, including three dimensions: family support (items: 3, 4, 8, 11), friend support (items: 6, 7, 9, 12), and support from others (items: 1, 2, 5, 10). The instrument was scored on a 7-point Likert scale with answers ranging from 1 (completely disagree) to 7 (completely agree). The total score ranges between 12 and 84, while the values for a given dimension come from the sum of the corresponding items. The Chinese version has shown good psychometric properties in previous studies (66). In this study, the Cronbach’s alpha (α) for this instrument was 0.905.
2.4.5 Security questionnaire
The Security Questionnaire (SQ) developed by Cong et al. in 2004 was used (67). This instrument was developed specifically for the Chinese population. This instrument contains two dimensions of interpersonal security (questions: 1, 3, 6, 8, 10, 12, 15, 16) and certainty of control (questions: 2, 4, 5, 7, 9, 11, 13, 14), with 16 entries. It is scored on a Likert 5-point scale, with 1–5 representing a scale from Very Compliant to Very Noncompliant. With a total score of 16-80, a high total score is an indication of high security. The original developers reported good reliability and validity (68). The Cronbach’s alpha (α) for this instrument in this study was 0.885.
2.5 Procedure
Questionnaires were administered either on site (paper-based questionnaires containing a QR code linking to the electronic form) or online (Questionnaire Star platform). Participants read the information sheet and provided informed consent (signature or ticking “agree”) before proceeding. Surveys were completed individually (10–15 minutes) in private rooms at community centers or via the online platform to ensure privacy. Investigators introduced the study, addressed questions, and monitored emotional comfort where needed. All questionnaires were self-completed anonymously and checked for completeness upon submission.
2.6 Statistical analysis
2.6.1 Latent profile analysis
Traditional variable-centered techniques assume population homogeneity, yet death anxiety is likely to manifest in distinct patterns among young adults. To capture these unobserved subpopulations within our heterogeneous youth sample, we used Latent Profile Analysis (LPA)—a model-based, person-centered clustering technique that classifies individuals according to their response patterns on the C-T-DAS. This cross-sectional design with LPA yields qualitatively distinct death-anxiety profiles that variable-centered methods overlook and can inform targeted psychological interventions. Model selection was guided by standard fit indices, including AIC, BIC, adjusted BIC, entropy, and the Lo–Mendell–Rubin likelihood ratio test (LMR-LRT) (69). The latent classes derived from this analysis were subsequently used in regression models to examine the predictive roles of self-esteem and security, as detailed in the following sections.
2.6.2 Data analysis procedures and model selection criteria
First, all received data were independently organized by two researchers using Excel to eliminate duplicates, incomplete information, and responses from foreigners. In the second step, descriptive analysis of the survey data, and reliability analysis of the psychometric instruments were completed using SPSS 27.0. In the third step, Mplus8.3 was prioritized for exploring the latent features of the death anxiety in the youth population, given its hard-to-ignore accuracy in achieving LPA (70). The final class solution was determined by several fitting indices, including the Akaike Information Criterion (AIC), the Bayesian Information Criterion (BIC), and the Adjusted Bayesian Information Criterion (aBIC). When a model possesses the lowest AIC, BIC, and aBIC values indicate the best-fitting model (71). Lo-Mendell-Rubin (LMR) and Bootstrap-Likelihood-Ratio-Test (BLRT) possess the trait of P < 0.05 can help determine the superiority of the K class model compared to the K-1 class model (72). The closer the entropy is to 1, the higher level of classification accuracy the model possesses, and Entropy > 0.80 was considered acceptable (73). Moreover, the proportion of members of each profile (the category with the lowest content >5%) (74) and the values on the diagonal in the average attribution probability matrix (higher values indicate a higher level of categorization correctness, and >0.7 is an acceptable result) (75) are also taken into account sufficiently before obtaining a decision on the final solution. In addition to this, the simplicity and interpretability of the theory and results are considered before the final decision on the profile. In the fourth step, concerning the characteristics of the profiles obtained above, we estimated the predictive effect of socio-demographic characteristics on death anxiety profile shifts through descriptive analysis and multivariate logistic regression (76, 77). Finally, using one-way ANOVA and multiple post hoc tests (Bonferroni Correction) (78), We assessed the relationship of specific profiles with self-esteem, perceived social support, and security. Any doubts encountered during the questionnaires screening process were resolved by reviewing the raw data and through two-person consultations. In this project, statistical tests were conducted using two-sided tests, and differences were considered statistically significant at P< 0.05.
2.7 Data quality control
To minimize bias and ensure data quality, multiple control measures were implemented throughout the study. During the design phase, a pilot study was conducted to assess the clarity and feasibility of questionnaire items. All research staff received standardized training on survey administration, emphasizing ethical communication and emotional sensitivity due to the nature of the topic. During data collection, participants were clearly informed about the confidentiality and voluntariness of the study. Questionnaires were checked for completeness upon submission, and participants’ emotional responses were monitored and managed as needed. For data processing, a double-entry procedure was employed to reduce transcription errors, and responses that did not meet predefined exclusion criteria were removed prior to analysis.
2.8 Ethical considerations
This project was approved by the Ethics Committee of the Seventh Clinical Medical College of Guangzhou University of Traditional Chinese Medicine (No. KY-2024-026-01), and we strictly adhered to the Helsinki Declaration and its amendments throughout the study. Prior to data collection, trained investigators explained the study purpose and procedures to participants, and informed consent was obtained by signing a written consent form included on the first page of the questionnaire. Participation was entirely voluntary, with no academic or financial incentives provided, and participants were free to withdraw at any time without consequence. Ethically related questions could be addressed directly to the research team in person or via email. All data were anonymized and stored securely on an encrypted institutional server, with access restricted to authorized members of the research team. Paper-based questionnaires were sealed in opaque envelopes and stored in locked cabinets, while electronic data were saved in password-protected folders maintained by the two project managers. In accordance with institutional data management policies, all anonymized data will be retained for five years and securely deleted thereafter. The data will be used solely for the purposes of this research and will not be shared with third parties, ensuring strict confidentiality and compliance with ethical standards.
3 Results
3.1 Characteristics of participants
In this survey, a total of 704 questionnaires were returned. We excluded over-age, duplication, incomplete information, overseas responses, and responses with a completion time of< 120 seconds. With an effective response rate of 88.5%, we finally obtained 623 reliable evidences. Participants had a mean age of 23.62 years (SD = 3.61, range = 18–35). Of the participants, 429 were women (68.9%); the majority were Han Chinese (95.7%); a total of 341 (54.7%) self-reported being healthy; and less than a quarter had received life education (23.8%). More detailed information is available in Table 1.
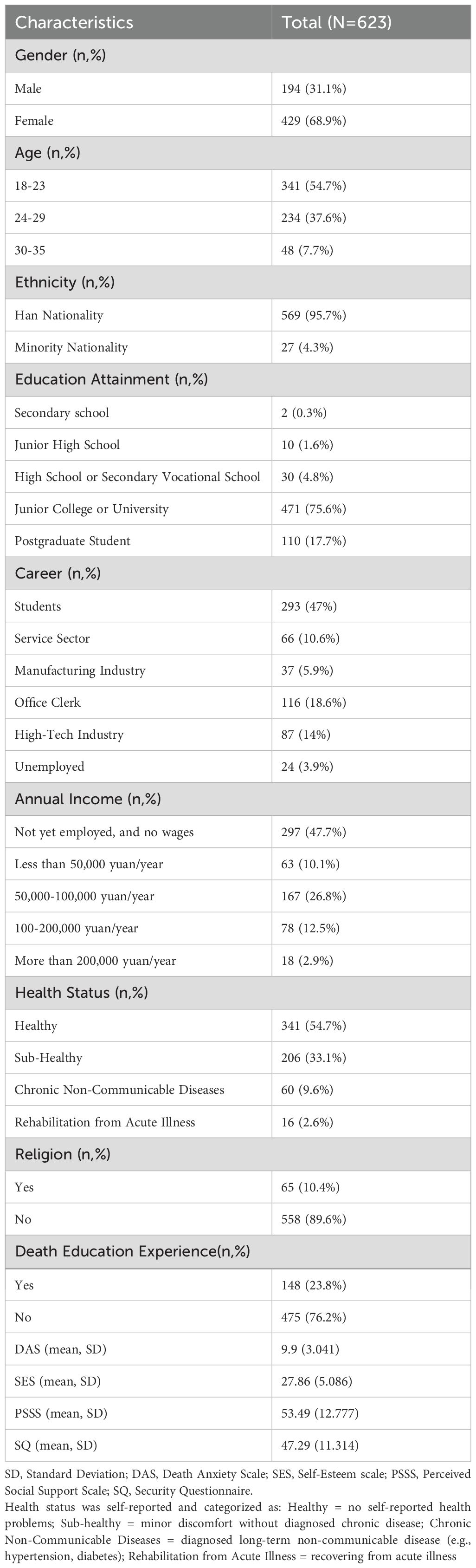
Table 1. Demographic characteristics of participants.
3.2 Underlying profiles and characteristics of death anxiety
To obtain the best results, we selected 1–6 latent feature models for exploratory latent feature analysis of death anxiety, and their fitting quality is shown in Table 2. In models with 1 to 6 categories, AIC and BIC values decreased as the category increased. However, although the 4-class model performed best on the AIC/BIC metric, considering the higher Entropy (Entropy = .962) and stronger category interpretability, we finally selected the 3-CLASS model (see Table 2). The model divided the participants into: The High Death Anxiety Group (Profile 1,56.2%) scored the highest on all death anxiety dimensions, especially on the ‘stress and pain’ dimension, which was much higher than the other two groups; The moderate cognitive low death anxiety group (Profile 2,8.8%) had higher cognition of death, but the lowest level of anxiety; the low cognitive moderate death anxiety group (Profile 3,35%) had the lowest score in the dimension of ‘Cognition of life and Death’, however, the overall anxiety level was moderate. Furthermore, in Model results were reliable (see Table 3 for details).

Table 2. Fit statistics for latent profile analysis models.

Table 3. Classification accuracy of latent profiles.
Based on the results of the potential profile analysis, the researchers plotted Figure 1. Detailed statistical values are provided in Table 4. Profile 1, which included 56.2% of the participants (N = 350), was characterized by significantly above-average total scores and significant performance excellence in all four death anxiety themes. Hence the name “High Death Anxiety”. Profile 2 is the smallest, consisting of 55 members representing 8.8 percent of the total. People assigned to this group had moderate but low death anxiety scores on the” Awareness of life and death” scale. Therefore, this profile was labeled “ Moderate Cognition and Low Death Anxiety”. Profile 3 comprised 35% (218 persons). This profile scored moderate on the death anxiety scale, but it scored lowest on the” Awareness of life and death” dimension. Hence the name” Low Cognition and Moderate Death Anxiety”.
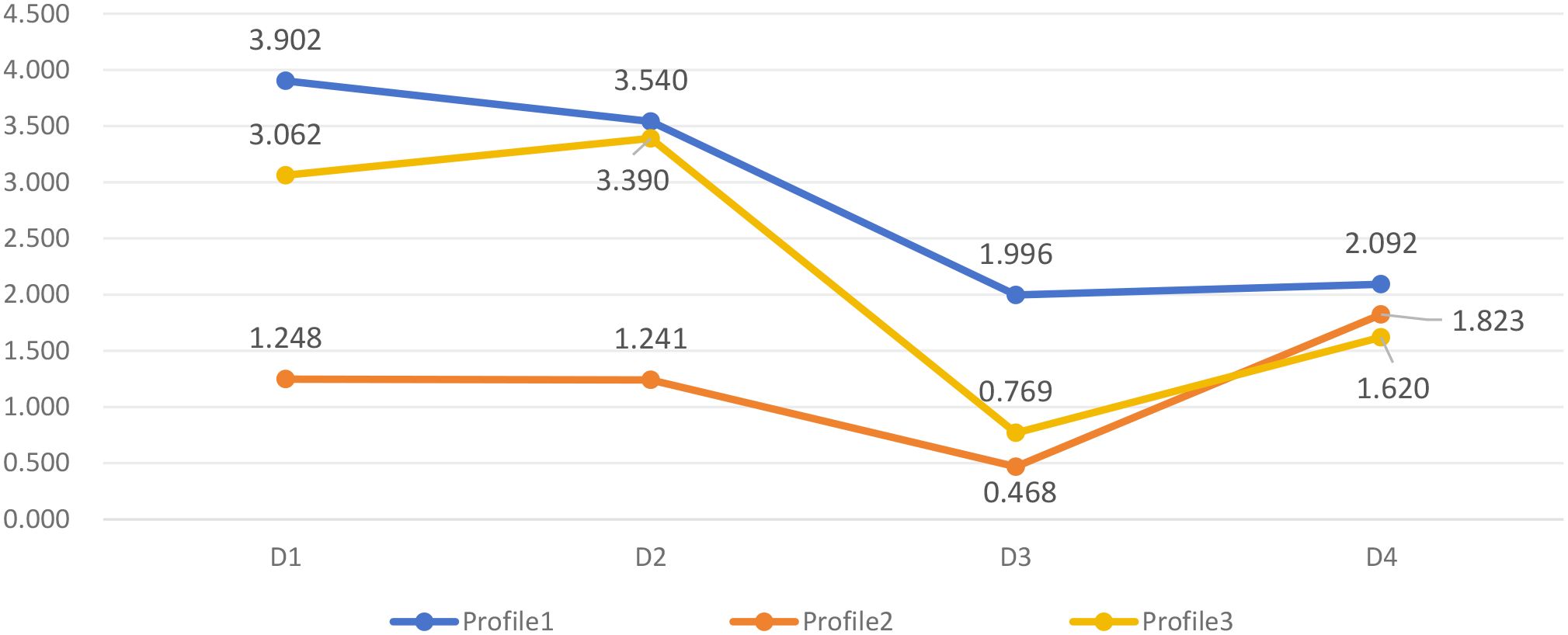
Figure 1. Mean scores of death anxiety dimensions across the three latent profiles. D1, Emotional; D2, Stress and Pain; D3, Time Awareness; D4, Cognition; Profile1, High Death Anxiety; Profile2, Moderate Cognition and Low Death Anxiety; Profile3, Low Cognition and Moderate Death Anxiety.

Table 4. Mean scores of death anxiety dimensions across latent profiles.
3.3 The demographic characteristics of each profile
Through descriptive analysis and one-way ANOVA, we characterized the sociodemographic characteristics of each profile. The” Low Cognition and Moderate Death Anxiety” group comprised more than half of the participants > 23 years of age, while the proportion of presenters< 24 years of age in the” Moderate Cognition and Low Death Anxiety” group reached 61.8%. More than half of the people in the” High Death Anxiety” group were unemployed and unpaid. In addition, we also found that people in good health were also likely to have higher Death Anxiety and to be in the “Moderate Cognition and Low Death Anxiety” group. See Table 5 for details.

Table 5. Demographic characteristics of participants across latent profiles.
3.4 Analysis of predictive factors for death anxiety profiles in Chinese youth
To identify predictors of profile membership, we incorporated sex, age, occupation, income level, and health status into multinomial logistic regressions based on observations of demographic characteristics, and we examined which demographic variables predicted membership in each death anxiety profile, the” High Death Anxiety” group was used as a reference.
In profile 2, participants aged 24–29 years reported lower death anxiety compared to those aged 30–35 years. In profile 3, participants aged 18–23 and 24–29 years reported lower death anxiety than those aged 30–35 years, and participants with Acute Illnesses in the Rehabilitation Period showed significantly higher anxiety than those with other health conditions. See Table 6 for details.
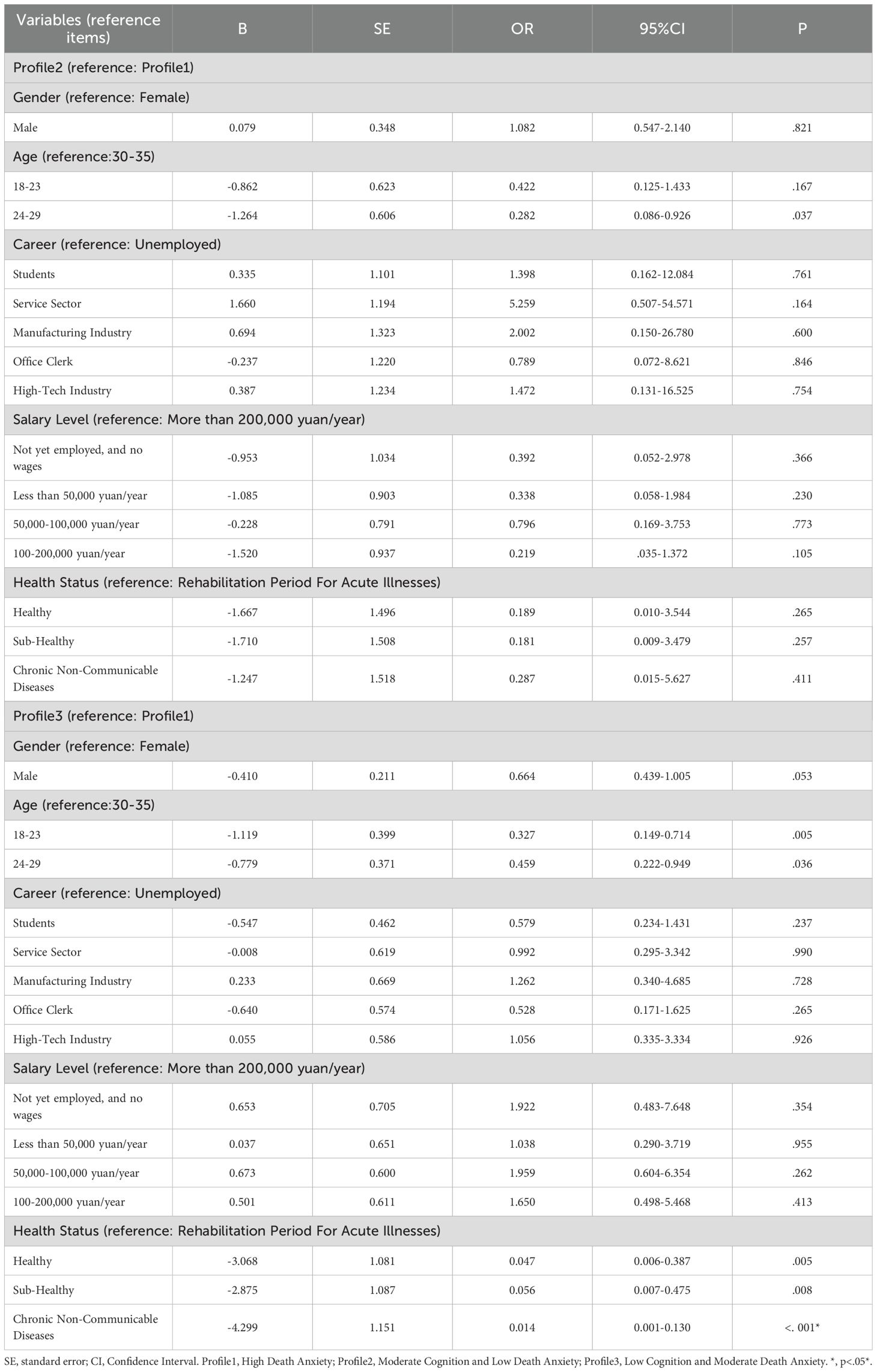
Table 6. Multinomial logistic regression predicting profile membership.
3.5 Comparison of various potential profiles of death anxiety considering self-esteem, perceived social support, and security
Analysis of variance showed that the death anxiety group had significant differences in self-esteem (F = 5.500, P = .004), social support (F = 4.163, P = .016), and security (F = 50.717, P <.001)(see Table 6). Bonferroni post hoc comparison further revealed that the High Death Anxiety Group -Profile file 1) had significantly lower self-esteem scores than the Medium Cognitive Low Death Anxiety group (Profile 2) and Low Cognitive Medium Death Anxiety group (Profile 3)(P <. 001). The social support score of the high death anxiety group was lower than that of the other two groups (P =. 004), but significant only in friend support and other support dimensions (P <. 001). For the security, the score of Profile 2 was the highest, which was significantly higher than that of the other two groups (P <. 001). Specific details of these comparisons can be found in Table 7.
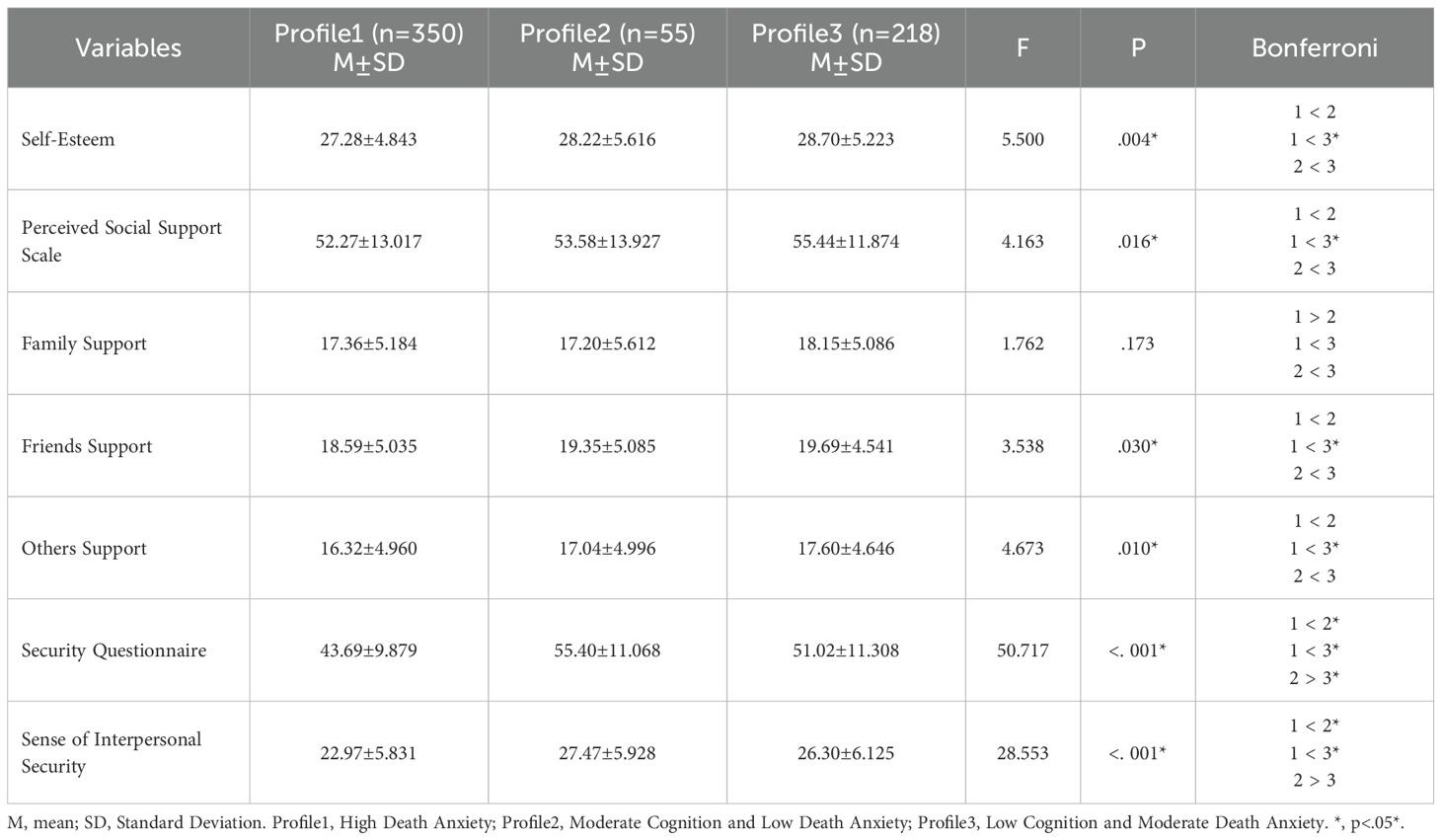
Table 7. ANOVA and post Hoc tests comparing psychological variables across profiles.
4 Discussion
This study employed latent profile analysis (LPA) to delineate distinct death-anxiety profiles among Chinese youth and to explore the role of self-esteem, social support, and security in the different profiles. The main findings indicated that the youth group showed significant heterogeneity in death anxiety and could be categorized into three latent profile groups: high death anxiety group (56.2%), medium cognitive low death anxiety group (8.8%), and low cognitive medium death anxiety group (35%). Significant differences in demographic characteristics (e.g., age, occupation, health status) and psychological variables (self-esteem, social support, and security) were found among the different groups, validating the research hypotheses.
1. Heterogeneity of Youth Death Anxiety and its Psychological Buffering Mechanism
In this study, we used LPA for the first time to identify the type of death anxiety in a youth group, which breaks through the limitations of the traditional variable-centered approach and reveals inter-individual variability. The three identified profiles reflect distinct psychological coping patterns: Profile 1 (High Death Anxiety, 56.2%) was characterized by low levels of self-esteem, social support, and security, consistent with the “anxiety-buffer disruption” perspective of Terror Management Theory; Profile 2 (Moderate Cognition and Low Death Anxiety, 8.8%) showed the highest security levels, aligning with attachment theory; Profile 3 (Low Cognition and Moderate Death Anxiety, 35%) indicated limited cognitive engagement with death yet elevated emotional distress, suggesting an avoidance-based strategy. These patterns demonstrate that different constellations of psychological resources lead to qualitatively distinct patterns of death anxiety, underscoring the need for targeted interventions. Reviewing the available data, two profiles of death anxiety called the low death anxiety group and the high stress group were identified in a survey of oncology nurses by Chen et al. (79). Although the populations of interest varied, our study also identified two profiles with similar presentations, which were “Moderate Cognition and Low Death Anxiety” and “Low Cognition and Moderate Death Anxiety”. In addition, we also identified “High Death Anxiety” and it was significantly represented among young people (56.2%), which indicates that more than half of young people have severe death anxiety. We suggest that this may be closely related to the failure of the anxiety-buffer system caused by the instability of the current cultural worldview of Chinese young people (e.g., lack of death education) (80). Supporting this explanation, Duan et al. developed the “Peaceful Tea House” program, which provided a safe environment for participants to discuss death-related topics and successfully reduced death anxiety (81).
The present study found variability in death anxiety among young individuals, supporting the hypothesis of heterogeneity in death anxiety. Notably, this variability may stem from the fact that individuals employ different psychological mechanisms to cope with the threat of death. According to Terror Management Theory, individuals buffer their anxiety through cultural worldviews, pursuing self-esteem, and making social connections when faced with the threat of death (82). When these buffers function well, death anxiety remains manageable; when disrupted by excessive anxiety, individuals intensify defensive efforts such as bolstering cultural worldviews, pursuing self-esteem, or strengthening close relationships (83, 84). Thus, young people with low death anxiety can adequately regulate negative emotions about death through a well-functioning anxiety buffer system and do not exhibit an overreliance on the cultural worldview buffer. However, once this buffer system is disrupted by severe death anxiety and causes a disruption in the functioning of the individual’s anxiety-buffering system. They will have to increase their use of holistic defenses, such as working hard to attain some cultural representations, maintaining self-esteem and intimacy, and warding off the damage of death anxiety by gaining the experience of immortality beyond death (34) (85, 86). This seems to explain the phenomenon that participants in Profile 2 had neither severe death anxiety nor outstanding performance in self-esteem and perceived social support compared to Profiles 1 and 3, while those included in Profile 3 showed higher levels of self-esteem and perceived social support compared to Profile 1. This result is consistent with previous research where Kheibari et al. helped participants who experienced death reminders to reduce death anxiety through self-esteem inflation, and those who achieved higher self-esteem showed more pro-social intentions and death anxieties (87). At the same time, Dürst et al. found that social support derived from interactions with relatives helped hospitalized critically ill patients experiencing visitation bans during the COVID period to improve their illness experience and reduce their stress-related symptoms, general anxiety, and death anxiety with family members (88).
The negative correlation between feelings of safety and death anxiety reveals a core psychological mechanism by which humans cope with existential fears. Safety is the state of being free from violence, harm, or other threats to individuals and society, and encompasses not only the protection of life and physical integrity, but also the safeguarding of property, economic interests, lifestyles, and psychological stability (89). From the perspective of Terror Management Theory, security is closely linked to the stability of an individual’s cultural worldview, which may contribute to the perception of death as a natural life process rather than an uncontrollable threat (90). As a result, high-security individuals are more inclined to buffer death anxiety by reinforcing social support and pursuing meaning in life, rather than falling into excessive fear of life’s fragility. Attachment theory further suggests that creating a “secure base” that provides people in need with opportunities to seek help from significant others, to be available and supported, to experience relief and comfort, and to return to other activities can increase their safety and peace of mind, thereby reducing fear and anxiety about death (91). Adequate feelings of safety can help people resist negative emotions as well as relieve anxiety and stress, promoting an individual’s physical and mental well-being, whereas a lack of safety may predict poorer mental health (92). This explains why Profile 2, with the strongest security, exhibited the lowest death anxiety, in contrast to Profiles 1 and 3. Similar findings were found in Mahat-Shamir et al.’s study, whereby individuals’ concerns about their safety significantly increased death anxiety during a sustained wave of terror. Relative to the salience of death accomplished via digital media, those who gained horrific experiences by talking to eyewitnesses had a more moderate expression of death anxiety, which may be a reflection of individuals’ ability to gain interpersonal security in close relationships and interpersonal attachments and to counteract death anxiety (93). In the Chinese context, however, Confucian values of filial piety and pervasive taboos around open discussion of death may erode such secure bases, undermining the cultural worldview that normally buffers existential fears and thereby intensifying death anxiety among youth. Culturally adapted death education programs that respectfully integrate traditional values while providing safe spaces for death-related discourse may thus be essential (94).
In summary, the results align with H1–H4, pointing to heterogeneous manifestations of death anxiety and the likely buffering effects of self-esteem, social support, and security.
2. Differential Effects of Demographic Variables
The present study further revealed the significant predictive role of demographic characteristics on death anxiety subgroups, and we found that age and health status may influence death anxiety among young people. According to Chopik’s inference, as age rises, individuals may gain more socially supportive strengths, and these close relationships can function as emotion regulators to help reduce thoughts and anxiety about death (95). However, this idea was not successfully verified in the data we obtained. Older participants (30–35 years) within the young adult group exhibited higher death anxiety. This trend may stem from their transitional life stage, which involves increasing responsibilities and existential reflections. Young adulthood is an important stage when individuals leave family-centered intimacy and establish personal-centered intimacy, and the relational shifts experienced during this period may significantly alter the trajectory of an individual’s life and affect his or her mental health (96). Unlike young adults who have just reached adulthood, late adolescents to middle-aged individuals may have left their parents’ homes and started their own families with loved ones. While they have a richer social support network, more complex social roles and the pressures that come with those roles are inevitable. This may have influenced their death anxiety (97, 98). In addition to this, young people in poor health, such as those recovering from an acute illness, also reported more severe death anxiety. A sudden acute illness may catch young people off guard with the threat of death, and if they are unable to regulate this emotion within a short period, they may experience a steep increase in death anxiety. This is similar to some clinical observations, as Malinauskaite et al. found that post-traumatic stress symptoms were present in survivors of acute coronary syndromes and that these individuals were significant in terms of fear of death, helplessness, avoidance, and severe anxiety (99). In conclusion, we conclude that older and ex-acute patients among the young should receive more attention, especially when they exhibit symptoms related to death anxiety. Beyond age, other demographic factors such as occupation, income, and gender may also interact with psychological resources to shape death anxiety, though these effects were less pronounced in our data.
4.1 Limitation and future perspectives
Although this study provides new insights, there are still some limitations. First, the samples in this study were from two cities in mainland China, and the cultural context may affect the generalizability of the results. The use of convenience sampling and a cross-sectional design further limits the generalizability of these findings to all Chinese youth. In particular, the broad age range of 18–35 years encompassed individuals at different developmental stages, such as students, early-career workers, and those assuming family responsibilities. This heterogeneity may have masked subgroup differences in death anxiety and reduced the precision of our findings. Moreover, although participants came from diverse occupational backgrounds, including healthcare and other death-related professions, subgroup analyses for these high-risk groups were not conducted due to limited sample sizes. This omission may have obscured occupation-specific manifestations of death anxiety.
Furthermore, the cultural specificity of our findings warrants careful consideration. Cross-cultural evidence suggests that while social support serves as a universal buffer against stress, its culturally specific forms, for example esteem-building as opposed to closeness-fostering support, generate divergent emotional outcomes in Western individualist and Eastern collectivist contexts (100). Therefore, the mechanisms linking social support to death anxiety identified in this Chinese sample may not be directly generalizable to other cultures. Future comparative studies are needed to test the cultural generalizability of these findings.
Second, the cross-sectional design of the present study only revealed the correlations between variables and could not infer whether self-esteem, social support, and security were causal factors of death anxiety. Future studies may adopt a longitudinal research design to explore the role of these psychological factors in the development of death anxiety; incorporate qualitative research (e.g., in-depth interviews) to further explore the psychological mechanisms of different anxiety groups; and may test the differences in the effects of interventions (e.g., positive thinking training, supportive groups) on different trait groups to optimize practice protocols.
Third, the self-report questionnaire was used in this study, which may have social desirability bias; future studies may combine behavioral measures or qualitative interviews to obtain more comprehensive data. Additionally, although religiosity was measured, its binary operationalization may not capture the nuanced role of spiritual beliefs in China. Future studies should employ more refined measures to explore the influence of religion on death anxiety. Finally, the failure to include more potential influencing factors (e.g., personality traits, traumatic experiences) may have omitted important explanatory variables, and future studies could incorporate more diverse measures, such as behavioral experiments and physiological indicator tests, to more accurately assess the independent and interactive effects of these factors on death anxiety.
Therefore, these results should be interpreted as exploratory and hypothesis-generating rather than confirmatory, and future studies with probability sampling designs are needed to validate these conclusions.
5 Conclusion
This study revealed the heterogeneity of death anxiety in a youth population through LPA, identifying three latent profile clusters: a high death anxiety group (56.2%), a medium cognitive low death anxiety group (8.8%), and a low cognitive moderate death anxiety group (35%). The results indicated that self-esteem, perceived social support, and security were significant negative predictors of death anxiety, supporting the hypothesis of Terror Management Theory. The high death anxiety group had significantly lower self-esteem and social support scores than the other two groups, whereas the group with a higher security showed lower levels of death anxiety. In addition, age and health status had a differential effect on the death anxiety subgroup, with death anxiety being more pronounced in young adults aged 30–35 years and in individuals recovering from acute illness. This study offers a precise foundation for youth mental health interventions, emphasizing the need for tailored strategies to support high-death anxiety groups. However, the study was limited by the cross-sectional design and regional sample, and it is necessary to further validate the causal mechanism by combining longitudinal studies, cross-cultural comparisons, and multivariate methods (e.g., behavioral experiments), as well as exploring the role of potential influences, such as personality traits, in the future.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the Seventh Clinical Medical College of Guangzhou University of Traditional Chinese Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
JY: Writing – original draft, Conceptualization, Investigation, Writing – review & editing. MW: Investigation, Writing – original draft, Data curation. YL: Formal Analysis, Writing – original draft. HP: Writing – original draft, Investigation. NL: Investigation, Writing – original draft. HL: Project administration, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Acknowledgments
Many thanks to all the team members for their mutual trust and joint efforts during these two years.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Feyzbabaie M, Rajai N, Alizadeh A, and Azizi M. Psychological distress among nursing students during the COVID-19 pandemic: a hybrid concept analysis. BMC Psychol. (2025) 13:218. doi: 10.1186/s40359-025-02562-x
2. Jessen-Winge C, Christensen CS, and Wæhrens EE. The influence on daily occupations of Danish adolescents experiencing stress. Scand J Occup Ther. (2025) 32:2472382. doi: 10.1080/11038128.2025.2472382
3. Zhai H, Xue J, Wu H, Liao S, Lavender C, Lv Y, et al. A national perspective: integrating medical humanities to address burnout and stress in Chinese medical education. BMC Med Educ. (2025) 25:304. doi: 10.1186/s12909-025-06875-8
4. John L, Solís-Soto MT, and Radon K. Mediating role of perceived social support in the relationship between unemployment and mental distress among healthcare graduates during the COVID-19 era. Front Public Health. (2024) 12:1490004. doi: 10.3389/fpubh.2024.1490004
5. Al-Ajlouny S, Al-Maqableh HO, Al-Shaikh AF, and Al-Qudah MA. Exploring the psychological effects of war on indirectly affected groups: a cross-sectional study on residents of Jordan. BMC Psychiatry. (2025) 25:130. doi: 10.1186/s12888-025-06560-6
6. Xie Q, Yan Y, Lai J, and Wei M. Mortality salience and helping behavior amidst public crisis: cross-sectional evidence during COVID-19. Front Public Health. (2024) 12:1455818. doi: 10.3389/fpubh.2024.1455818
7. Pradhan M, Chettri A, and Maheshwari S. Fear of death in the shadow of COVID-19: The mediating role of perceived stress in the relationship between neuroticism and death anxiety. Death Stud. (2022) 46:1106–10. doi: 10.1080/07481187.2020.1833384
8. Walbaum C, Philipp R, Bokemeyer C, Härter M, Junghans J, Koch U, et al. Death anxiety in patients with advanced cancer and their family caregivers. J Pain Symptom Manage. (2024) 68:622–31. doi: 10.1016/j.jpainsymman.2024.08.027
9. Xu M, Dust SB, and Liu S. COVID-19 and the great resignation: The role of death anxiety, need for meaningful work, and task significance. J Appl Psychol. (2023) 108:1790–811. doi: 10.1037/apl0001102
10. Thiemann P, Quince T, Benson J, Wood D, and Barclay S. Medical students’ Death anxiety: severity and association with psychological health and attitudes toward palliative care. J Pain Symptom Manage. (2015) 50:335–42.e2. doi: 10.1016/j.jpainsymman.2015.03.014
11. Furer P and Walker JR. Death anxiety: A cognitive-behavioral approach. J Cogn Psychotherapy. (2008) 22:167–82. doi: 10.1891/0889-8391.22.2.167
12. Öztürk SS, Çiçek İE, and Eren İ. Death anxiety and related factors in schizophrenia patients: controlled study. Omega (Westport). (2023) 87:1048–62. doi: 10.1177/00302228211033122
13. Menzies RE, Sharpe L, and Dar-Nimrod I. The relationship between death anxiety and severity of mental illnesses. Br J Clin Psychol. (2019) 58:452–67. doi: 10.1111/bjc.12229
14. Aan de Stegge BM, Tak LM, Rosmalen JGM, and Oude Voshaar RC. Death anxiety and its association with hypochondriasis and medically unexplained symptoms: A systematic review. J Psychosom Res. (2018) 115:58–65. doi: 10.1016/j.jpsychores.2018.10.002
15. Menzies RE, Sharpe L, Richmond B, and Cunningham ML. Life’s too short to be small”: An experimental exploration of the relationship between death anxiety and muscle dysmorphia symptoms. Body Image. (2023) 44:43–52. doi: 10.1016/j.bodyim.2022.11.006
16. Harnischfeger N, Rath HM, Alt-Epping B, Brand H, Haller K, Letsch A, et al. Association between oncologists’ death anxiety and their end-of-life communication with advanced cancer patients. Psychooncology. (2023) 32:923–32. doi: 10.1002/pon.6132
17. Harrawood LK, White LJ, and Benshoff JJ. Death anxiety in a national sample of United States funeral directors and its relationship with death exposure, age, and sex. Omega (Westport). (2008) 58:129–46. doi: 10.2190/om.58.2.c
18. Bergman YS. Death anxiety and resilience in older adults: the moderating role of attachment patterns. Behav Sci (Basel). (2024) 14:1031. doi: 10.3390/bs14111031
19. Hassan EA, Elsayed SM, Monged HH, and Abdelwahab BT. Frailty and fear of death among geriatric patients in critical care units: A mixed methods study. Nurs Crit Care. (2024) 30:e13219. doi: 10.1111/nicc.13219
20. Zhang X, Zhang H, Zhu M, Wu M, Huang Y, and Qin Z. The mediating effects of death reflection on death literacy and death anxiety among Chinese nurses: a cross-sectional study. Sci Rep. (2024) 14:31153. doi: 10.1038/s41598-024-82421-8
21. Nagaoka J, Farrington CA, Ehrlich SB, and Heath RD. Foundations for young adult success: A developmental framework. Concept Paper Res Practice: ERIC. (2015). doi: 10.59656/YD-G1389.001
22. Wang Y, Ge F, Zhang J, and Zhang W. Heterogeneity in the co-occurrence of depression and anxiety symptoms among youth survivors: A longitudinal study using latent profile analysis. Early Interv Psychiatry. (2021) 15:1612–25. doi: 10.1111/eip.13101
23. Harmon-Jones E, Simon L, Greenberg J, Pyszczynski T, Solomon S, and McGregor H. Terror management theory and self-esteem: evidence that increased self-esteem reduces mortality salience effects. J Pers Soc Psychol. (1997) 72:24–36. doi: 10.1037/0022-3514.72.1.24
24. Lei A. Discussion on the characteristics of death anxiety of the people in mainland China. Chin Med Ethics. (2017) 62:1219–22.
25. Spurk D, Hirschi A, Wang M, Valero D, and Kauffeld S. Latent profile analysis: A review and “how to” guide of its application within vocational behavior research. J Vocational Behavior. (2020) 120:103445. doi: 10.1016/j.jvb.2020.103445
26. Huang Y, Guan Z, Yan F, Wiley JA, Reynolds NR, Tang S, et al. Mediator role of presence of meaning and self-esteem in the relationship of social support and death anxiety. Front Psychol. (2022) 13:1018097. doi: 10.3389/fpsyg.2022.1018097
27. Belmi P and Pfeffer J. Power and death: Mortality salience increases power seeking while feeling powerful reduces death anxiety. J Appl Psychol. (2016) 101:702–20. doi: 10.1037/apl0000076
28. Doré C. Self esteem: concept analysis. Rech Soins Infirm. (2017) 2017:18–26. doi: 10.3917/rsi.129.0018
29. Lieberman EJ. Terror management theory. Am J Psychiatry. (2004) 161:1508. doi: 10.1176/appi.ajp.161.8.1508
30. Zhang J, Peng J, Gao P, Huang H, Cao Y, Zheng L, et al. Relationship between meaning in life and death anxiety in the elderly: self-esteem as a mediator. BMC Geriatr. (2019) 19:308. doi: 10.1186/s12877-019-1316-7
31. Taylor SE. How are social ties protective? Span J Psychol. (2020) 23:e41. doi: 10.1017/sjp.2020.35
32. Cullen FT. Social support as an organizing concept for criminology: Presidential address to the academy of criminal justice sciences. Justice Quarterly. (1994) 11:527–59. doi: 10.1080/07418829400092421
33. Zhang L, Pang J, and Zhu F. Effect of perceived social support on psychache: mediating effect of psychological resilience. Iran J Public Health. (2022) 51:386–94. doi: 10.18502/ijph.v51i2.8691
34. Uslu-Sahan F, Terzioglu F, and Koc G. Hopelessness, death anxiety, and social support of hospitalized patients with gynecologic cancer and their caregivers. Cancer Nurs. (2019) 42:373–80. doi: 10.1097/ncc.0000000000000622
36. Bürgin D, Anagnostopoulos D, Vitiello B, Sukale T, Schmid M, and Fegert JM. Impact of war and forced displacement on children’s mental health-multilevel, needs-oriented, and trauma-informed approaches. Eur Child Adolesc Psychiatry. (2022) 31:845–53. doi: 10.1007/s00787-022-01974-z
37. Syam H, Venables E, Sousse B, Severy N, Saavedra L, and Kazour F. With every passing day I feel like a candle, melting little by little.” experiences of long-term displacement amongst Syrian refugees in Shatila, Lebanon. Confl Health. (2019) 13:45. doi: 10.1186/s13031-019-0228-7
38. Larson N, Slaughter-Acey J, Alexander T, Berge J, Harnack L, and Neumark-Sztainer D. Emerging adults’ intersecting experiences of food insecurity, unsafe neighborhoods and discrimination during the coronavirus disease 2019 (COVID-19) outbreak. Public Health Nutr. (2021) 24:519–30. doi: 10.1017/S136898002000422X
39. Jamalimoghadam N, Yektatalab S, Momennasab M, Ebadi A, and Zare N. How do hospitalized adolescents feel safe? A qualitative study. J Nurs Res. (2019) 27:e14. doi: 10.1097/jnr.0000000000000285
40. Fagerström L, Gustafson Y, Jakobsson G, Johansson S, and Vartiainen P. Sense of security among people aged 65 and 75: external and inner sources of security. J Adv Nurs. (2011) 67:1305–16. doi: 10.1111/j.1365-2648.2010.05562.x
41. Larsson F, Strömbäck U, Rysst Gustafsson S, and Engström Å. Perception of feeling safe perioperatively: a concept analysis. Int J Qual Stud Health Well-being. (2023) 18:2216018. doi: 10.1080/17482631.2023.2216018
42. Yenerall J and Jensen K. Food security, financial resources, and mental health: evidence during the COVID-19 pandemic. Nutrients. (2021) 14. doi: 10.3390/nu14010161
43. Clair A and Baker E. Cold homes and mental health harm: Evidence from the UK Household Longitudinal Study. Soc Sci Med. (2022) 314:115461. doi: 10.1016/j.socscimed.2022.115461
44. Aguglia A, Amerio A, Costanza A, Parodi N, Copello F, Serafini G, et al. Hopelessness and Post-Traumatic Stress Symptoms among Healthcare Workers during the COVID-19 Pandemic: Any Role for Mediating Variables? Int J Environ Res Public Health. (2021) 18:6579. doi: 10.3390/ijerph18126579
45. Ottu IFA, Essien EA, and Lawal AM. Death anxiety from quality of life and emotional impact of event: A case study of proximate earwitnesses of dana air crash in Nigeria. Omega (Westport). (2019) 78:421–40. doi: 10.1177/0030222817701466
46. Scheffold K, Philipp R, Koranyi S, Engelmann D, Schulz-Kindermann F, Härter M, et al. Insecure attachment predicts depression and death anxiety in advanced cancer patients. Palliat Support Care. (2018) 16:308–16. doi: 10.1017/s1478951517000281
47. Li Y, Dong W, Tang H, Guo X, Wu S, Lu G, et al. Correlates of death anxiety for patients with cancer: A systematic review and meta-analysis. J Clin Nurs. (2024) 33:1933–47. doi: 10.1111/jocn.17021
48. Howard MC and Hoffman ME. Variable-centered, person-centered, and person-specific approaches: Where theory meets the method. Organizational Res Methods. (2018) 21:846–76. doi: 10.1177/1094428117744021
49. Daljeet KN, Bremner NL, Giammarco EA, Meyer JP, and Paunonen SV. Taking a person-centered approach to personality: A latent-profile analysis of the HEXACO model of personality. J Res Personality. (2017) 70:241–51. doi: 10.1016/j.jrp.2017.08.003
50. Salmon DP, Riekkinen PJ, Katzman R, Zhang MY, Jin H, and Yu E. Cross-cultural studies of dementia. A comparison of mini-mental state examination performance in Finland and China. Arch Neurol. (1989) 46:769–72. doi: 10.1001/archneur.1989.00520430063019
51. Barry MJ, Nicholson WK, Silverstein M, Chelmow D, Coker TR, Davidson KW, et al. Screening for depression and suicide risk in adults: US preventive services task force recommendation statement. Jama. (2023) 329:2057–67. doi: 10.1001/jama.2023.9297
52. Guha M. Diagnostic and statistical manual of mental disorders: DSM-5. Reference Rev. (2014) 28:36–7.
53. Hong Y, Yanlin L, Qiuli Y, Xiaojing W, and Department N. Application of the Chinese version of Templer-Death Anxiety Scale:enlightenment for death education. J Nurs Science. (2013) 28:64–7. doi: 10.3870/hlxzz.2013.21.064
54. Xu GR and Yu WY. Mediating effect of meaning in life on death anxiety and attitude toward palliative care among undergraduate nursing students. BMC Palliat Care. (2024) 23:139. doi: 10.1186/s12904-024-01472-w
55. Krejcie RV. Determining sample size for research activities Vol. 30. Educational & Psychological Measurement (1970) 30:607–10. doi: 10.1177/001316447003000308
56. Muthén LK and Muthén BO. How to use a monte carlo study to decide on sample size and determine power. Struct Equation Modeling. (2002) 9:599–620. doi: 10.1207/S15328007SEM0904_8
57. Faul F, Erdfelder E, Lang AG, and Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. (2007) 39:175–91. doi: 10.3758/BF03193146
58. Templer DI. The construction and validation of a Death Anxiety Scale. J Gen Psychol. (1970) 82:165–77. doi: 10.1080/00221309.1970.9920634
59. Hong Y, Yuhan L, Youhui G, Zhanying W, Shili Z, Xiaoting H, et al. Death anxiety among advanced cancer patients: a cross-sectional survey. Support Care Cancer. (2022) 30:3531–9. doi: 10.1007/s00520-022-06795-z
62. Tian L. Shortcoming and merits of Chinese version of Rosenberg (1965) Self-Esteem Scale. Psychological Exploration (2006). doi: 10.3969/j.issn.1003-5184.2006.02.020
63. Du H, King RB, and Chi P. Self-esteem and subjective well-being revisited: The roles of personal, relational, and collective self-esteem. PloS One. (2017) 12:e0183958. doi: 10.1371/journal.pone.0183958
64. Zimet GD, Dahlem NW, Zimet SG, and Farley GK. The multidimensional scale of perceived social support. J Pers assessment. (1988) 52:30–41. doi: 10.1207/S15328007SEM0904_8
65. Jiang QJ. Perceived social support scale,PSSS (in China). Manual for the mental health rating scale. Beijing: Chin J Ment Health Press;. (1999) p:131–3.
66. Yuan W, Xie Z, Dong P, and Yang Y. Linking perceived social support to self-esteem and social integration among adolescents with visual impairment: A cross-lagged study. Front Psychol. (2022) 13:1054857. doi: 10.3389/fpsyg.2022.1054857
67. Zhong C. Developing of security questionnaire and its reliability and validity. Chin Ment Health J. (2004) 18:97–9. doi: 10.1007/BF02911031
68. Cao L. The relationship between adjustment and mental health of chinese freshmen: the mediating effect of security and the moderating effect of gender. Front Public Health. (2022) 10:916329. doi: 10.3389/fpubh.2022.916329
69. Berlin KS, Williams NA, and Parra GR. An introduction to latent variable mixture modeling (Part 1): overview and cross-sectional latent class and latent profile analyses. J Pediatr Psychol. (2014), 174. doi: 10.1093/jpepsy/jst084
70. Muthén B and Muthén L. Mplus: A general latent variable modeling program. Muthén & Muthén (2019).
71. Tofighi D and Enders CK. Identifying the correct number of classes in growth mixture models. Adv latent variable mixture models. (2008) 2007:317.
72. Sinha P, Calfee CS, and Delucchi KL. Practitioner’s guide to latent class analysis: methodological considerations and common pitfalls. Crit Care Med. (2021) 49:e63–79. doi: 10.1097/CCM.0000000000004710
73. Lubke G and Muthén BO. Performance of factor mixture models as a function of model size, covariate effects, and class-specific parameters. Struct Equation Modeling A Multidiscip J. (2007) 14:26–47. doi: 10.1080/10705510709336735
74. Tein JY, Coxe S, and Cham H. Statistical power to detect the correct number of classes in latent profile analysis. Struct Equ Modeling. (2013) 20:640–57. doi: 10.1080/10705511.2013.824781
75. Wang J and Wang X. Structural Equation Modeling: Applications Using Mplus. Wiley Publishing (2012). doi: 10.1002/9781118356258
76. Emanuel LL, Solomon S, Chochinov HM, Delgado Guay MO, Handzo G, Hauser J, et al. Death anxiety and correlates in cancer patients receiving palliative care. J Palliat Med. (2023) 26:235–43. doi: 10.1089/jpm.2022.0052
77. Rayatpisheh F, Torabizadeh C, Najafi Kalyani M, and Farsi Z. Relationship between resilience and death anxiety of the older adults during the coronavirus disease 2019 (COVID-19) pandemic. BMC Geriatr. (2023) 23:367.
78. Armstrong RA. When to use the B onferroni correction. Ophthalmic Physiol optics. (2014) 34:502–8. doi: 10.1111/opo.12131
79. Chen X, Su M, Arber A, Qiao C, Wu J, Sun C, et al. Exploring the variations in death anxiety among oncology nurses in China: a latent class analysis. BMC Palliat Care. (2023) 22:176. doi: 10.1186/s12904-023-01282-6
80. Chen H, Xiao Y, Huang X, Fan S, Wu H, Li L, et al. Research on factors influencing Chinese parents’ support for death education: a cross-sectional survey. Front Public Health. (2024) 12:1285208. doi: 10.3389/fpubh.2024.1285208
81. Duan Y, Huang J, Yu R, Lin F, and Liu Y. Evaluation of the effect of death education based on the Peace of Mind Tea House: a randomized controlled trial of nursing trainees at Xiamen University, China. BMC Nurs. (2024) 23:597. doi: 10.1186/s12912-024-02188-1
82. Pyszczynski T, Solomon S, and Greenberg J. Chapter one - thirty years of terror management theory: from genesis to revelation. In: Olson JM and Zanna MP, editors. Advances in Experimental Social Psychology, vol. 52. Academic Press (2015). p. 1–70.
83. Pyszczynski T and Kesebir P. Anxiety buffer disruption theory: a terror management account of posttraumatic stress disorder. Anxiety Stress Coping. (2011) 24:3–26. doi: 10.1080/10615806.2010.517524
84. Burke BL, Martens A, and Faucher EH. Two decades of terror management theory: a meta-analysis of mortality salience research. Pers Soc Psychol Rev. (2010) 14:155–95. doi: 10.1177/1088868309352321
85. Simon L, Greenberg J, Harmon-Jones E, Solomon S, Pyszczynski T, Arndt J, et al. Terror management and cognitive-experiential self-theory: evidence that terror management occurs in the experiential system. J Pers Soc Psychol. (1997) 72:1132–46. doi: 10.1037/0022-3514.72.5.1132
86. Griffith JD, Gassem M, Hart CL, Adams LT, and Sargent R. A cross-sectional view of fear of death and dying among skydivers. Omega (Westport). (2018) 77:173–87. doi: 10.1177/0030222815600178
87. Kheibari A and Cerel J. Does self-esteem inflation mitigate mortality salience effects on suicide attitudes? Suicide Life Threat Behav. (2021) 51:775–84. doi: 10.1111/sltb.12759
88. Dürst AV, Graf CE, Ruggiero C, Zekry D, Boccardi V, Monney L, et al. Fighting social isolation in times of pandemic COVID-19: the role of video calls for older hospitalized patients. Aging Clin Exp Res. (2022) 34:2245–53. doi: 10.1007/s40520-022-02188-8
90. Juhl J. Chapter 13 - Terror Management Theory: A Theory of Psychological Well-Being. In: Routledge C and Vess M, editors. Handbook of Terror Management Theory. Academic Press (2019). p. 303–24. doi: 10.1016/B978-0-12-811844-3.00013-5
91. Milberg A, Wåhlberg R, Jakobsson M, Olsson EC, Olsson M, and Friedrichsen M. What is a ‘secure base’ when death is approaching? A study applying attachment theory to adult patients’ and family members’ experiences of palliative home care. Psychooncology. (2012) 21:886–95. doi: 10.1002/pon.1982
92. Daemen JAM. Being sure and living well: how security affects human flourishing. J Value Inquiry. (2024) 58:93–110. doi: 10.1007/s10790-021-09870-6
93. Mahat-Shamir M, Hamama-Raz Y, Ben-Ezra M, Pitcho-Prelorentzos S, Zaken A, David UY, et al. Concern and death anxiety during an ongoing terror wave: The moderating role of direct vs. indirect exposure. Death Stud. (2018) 42:195–203. doi: 10.1080/07481187.2017.1334010
94. Lei L, Gan Q, Gu C, Tan J, and Luo Y. Life-and-death attitude and its formation process and end-of-life care expectations among the elderly under traditional chinese culture: A qualitative study. J Transcult Nurs. (2022) 33:57–64. doi: 10.1177/10436596211021490
95. Chopik WJ. Death across the lifespan: Age differences in death-related thoughts and anxiety. Death Stud. (2017) 41:69–77. doi: 10.1080/07481187.2016.1206997
96. Brazil N and Clark WAV. Individual mental health, life course events and dynamic neighborhood change during the transition to adulthood. Health Place. (2017) 45:99–109. doi: 10.1016/j.healthplace.2017.03.007
97. Genç ZB. Analysis of the relationship between perceived stress level and death anxiety in individuals with COPD. Rev Esc Enferm USP. (2024) 57:e20230273. doi: 10.1590/1980-220X-REEUSP-2023-0273en
98. Norouzi M, Ghorbani Vajargah P, Falakdami A, Mollaei A, Takasi P, Ghazanfari MJ, et al. A systematic review of death anxiety and related factors among nurses. Omega (Westport). (2022) 2022:302228221095710. doi: 10.1177/00302228221095710
99. Malinauskaite I, Slapikas R, Courvoisier D, Mach F, and Gencer B. The fear of dying and occurrence of posttraumatic stress symptoms after an acute coronary syndrome: A prospective observational study. J Health Psychol. (2017) 22:208–17. doi: 10.1177/1359105315600233
Keywords: death anxiety, self-esteem, perceived social support, security, latent profile analysis, young adults
Citation: Yu J, Wu M, Liang Y, Peng H, Li N and Liu H (2025) Latent profiles of death anxiety among young adults: associations with self-esteem, security, and perceived social support. Front. Psychiatry 16:1594720. doi: 10.3389/fpsyt.2025.1594720
Received: 16 March 2025; Accepted: 11 September 2025;
Published: 24 September 2025.
Edited by:
Qasir Abbas, Government College University, Faisalabad, PakistanReviewed by:
Semra Bulbuloglu, Istanbul Aydɩn University Istanbul, TürkiyeXiao Zilun, Chongqing University of Posts and Telecommunications, China
Shazia Habib, Government College University, Faisalabad, Pakistan
Copyright © 2025 Yu, Wu, Liang, Peng, Li and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hanjiao Liu, bGl1aGFuamlhbzAwMEAxNjMuY29t
†These authors have contributed equally to this work and share first authorship