 Mathias Rossi1,2
Mathias Rossi1,2 Maryse Arcand1,2
Maryse Arcand1,2 Mike Schmidt3
Mike Schmidt3 Theodorus G. M. Sandfort4,5
Theodorus G. M. Sandfort4,5 Francelyne Jean-Baptiste6
Francelyne Jean-Baptiste6 Marie-France Marin1,6,7
Marie-France Marin1,6,7 Spiro P. Pantazatos3,4
Spiro P. Pantazatos3,4 Robert-Paul Juster1,2,6*
Robert-Paul Juster1,2,6*- 1Research Center, Institut Universitaire en Santé Mentale de Montréal, Montreal, QC, Canada
- 2Department of Psychiatry and Addiction, University of Montreal, Montreal, QC, Canada
- 3Molecular Imaging and Neuropathology Division, New York State Psychiatric Institute, New York, NY, United States
- 4Department of Psychiatry, Columbia University Medical Center, New York, NY, United States
- 5HIV Center for Clinical and Behavioral Studies, New York State Psychiatric Institute and Columbia University, New York, NY, United States
- 6Interdisciplinary Research Centre on Intimate Relationship Problems and Sexual Abuse, Montreal, QC, Canada
- 7Department of Psychology, Université du Québec à Montréal, Montreal, QC, Canada
Introduction: Gender roles and personality traits have been reported to impact mental health. This study aims to investigate the relationship between gender role identity and psychiatric symptoms (anxiety, depressive symptoms, suicidality) as well as the moderating effects of personality traits in a community-representative sample of American adults.
Methods: Data from 741 participants (65.7% females) were analyzed from the Nathan-Kline Institute – Rockland Sample database, a community-ascertained lifespan cohort with participants undergoing multimodal brain imaging and comprehensive behavioral, cognitive, and psychiatric assessments. This analysis is restricted to adults and uses well-validated questionnaires to assess gender role identity, personality traits, symptoms of anxiety and depression, and suicidal thoughts/behaviors.
Results: Results revealed that having a gender role identity reversed to one’s birth-assigned sex (i.e., feminine gender role in males and masculine gender role in females) was associated with poorer mental health (i.e., more anxiety and depressive symptoms). This effect was stronger in males where femininity was positively associated with more suicidal thoughts and behaviors. Further analyses revealed that only low-extroverted feminine males reported higher anxiety, and only high-neurotic feminine males reported higher suicidality.
Conclusions: The present American study provides new understanding on gender role identity associations with mental health, while highlighting the importance of considering both birth-assigned sex and personality traits when studying gender role effects on psychiatric symptoms. We discuss the role of gendered traits and societal burden in relation to mental health.
1 Introduction
Sex differences are a major consideration for mental health disorders (1). For instance, women engage more frequently in suicidal behaviors, whereas men are more likely to complete suicide (2). This “gender paradox” is consistent in the literature (3–5), and is also common in other psychiatric conditions like depression and anxiety: girls report an increasing rate of depressive symptoms and anxiety higher than boys from adolescence onwards (6, 7). Studies have also reported that symptoms of anxiety and depression, which are highly comorbid, can contribute strongly to suicidal symptoms (8–10). Women show higher rates of anxiety and depression than men in adulthood (11, 12). This can contribute to their higher rate of suicide attempts. By contrast, men are less likely to report or seek help for mental health issues while using more lethal approaches, which ultimately contributes to higher rates of completed suicide (13). While biological factors have also been investigated to explain sex differences in suicide rates (14) and the two-times higher prevalence of depression in females (15), environmental factors (11) like socio-economic status (16), major life events (5), or personality traits (17) also play a key role in the prevalence of anxious, depressive, and suicidal symptoms. Beyond sex as a biological binary, the current research aims to understand the role of socio-cultural gender role identity in association with psychiatric symptoms and suicidality (i.e. suicidal thoughts and behaviors) (18).
1.1 Socio-cultural gender roles
Several studies have reported that gender roles explain variance in anxiety and depression beyond that of biological sex (19–21). Gender is a multidimensional concept that includes sociocultural roles and identities (i.e., men, women, nonbinary people) that are different from one’s biological sex (i.e. sex assigned at birth: male, female, intersex) that is otherwise determined by genes, hormone levels, and gonads (22, 23). While growing up and socializing, children will endorse sex-specific personality traits or gender roles by performing behaviors that are stereotypically classified as “feminine” (e.g. affective concerns) and “masculine” (e.g. cognitive focus on action) (24). Several questionnaires, like the Personal Attributes Questionnaire (PAQ) (25), have aimed to assess one’s femininity and masculinity by analyzing personality traits and classifying their descriptions as “feminine” or communal and “masculine” or agentic factors.
In the 1970s, Bem developed the Bem Sex Role Inventory (BSRI) that assesses femininity and masculinity on two orthogonal but still complementary continuums (26). Two approaches to gender roles have been developed. First, the categorical method that classifies people as masculine, feminine, androgynous (when both of their feminine and masculine scores are high), or undifferentiated (when both of their scores are low). Second, a continuous method that considers one’s sex and mixture of feminine and masculine continuums to obtain diverse gender role profiles. For instance, people can be sex-typed (when their gender role profile matches their birth-assigned sex), cross-typed (when their gender role profile is opposed to their birth-assigned sex), or mix-typed (when their gender role profile is not mainly feminine nor masculine). As gender roles develop across the lifespan and in the face of stressful life events, they may modulate the way mental health problems manifest themselves (27). Indeed, gender roles overlap with personality traits that can synergistically influence coping strategies (e.g. emotional regulation, self-esteem, adjustment) that are collectively associated with anxiety, depression, and even suicidal behaviors (28).
1.2 Gender roles, anxiety and depression
Whether it has been measured with the PAQ or the BSRI, higher masculinity has been consistently associated with fewer reported symptoms of depression and anxiety (20, 21, 29–32). However, femininity has been less consistently associated with mental health. Some studies have shown that higher femininity is related to more general distress (33), anxiety and depressive symptoms (21, 34). On the other hand, several studies have not shown a significant effect of femininity on mental health (30–32, 35–37), and some even found mixed results where femininity was related to fewer depressive symptoms (29, 38). A meta-analysis by Whitley in 1985 concluded that higher masculinity was associated with less depression and greater adjustment, whereas femininity had no consistent relationship with depression (37).
The apparent heterogeneity of results linking feminine gender roles to depression may be due to different ways that gender roles operate among men and women (20). Some studies did not find significant differences between the way that gender roles affect sex differences in mental health (36). By contrast, several studies have highlighted mixed associations between gender roles and mental health. For example, a study by Gibson et al. reported that higher femininity was associated with fewer depressive symptoms in college educated men, while masculinity had no effect only for women. This highlights the need to consider other demographic and socio-cultural factors such as education level in the study of gender roles (38).
Some studies have investigated the effect of gender roles only in one sex or specific race/ethnic groups. Among females, higher femininity has been associated with more anxiety and depression (39, 40), while less masculinity has been related to more depressive symptoms (30). However, for Black women, higher femininity has been associated with less depressive symptoms (41), which underlines again the inconsistency of findings among females, as well as the importance of considering race/ethnicity and intersecting sociodemographics more broadly in gender role research (42).
1.3 Gender roles and suicidality
It has been proposed that higher masculinity decreases self-harm only in males (43). However, some sociocultural profiles related to certain masculine norms such as self-reliance, difficulty expressing emotions and reduced help-seeking behavior may be ‘maladaptive’ with respect to men’s mental health, particularly in developed Western societies where men experience decreasing social and economic role opportunities (real or perceived) since the 1960s (44, 45). Indeed, higher male-to-female suicide ratios in more common in highly developed, gender egalitarian nations (46). In addition, a study of men hospitalized following stressful life events found that adherence to traditional male gender roles mediated previous suicide attempt status in men (47). Beyond extreme masculinity and femininity alone, it appears that the extent that one’s gender role concords with one’s birth-assigned sex is also a unique predictor of suicide risk. Indeed, cross-typed people (i.e., people with a gender role or personality typology opposed to their birth-assigned sex) are considered to be at higher risk of suicidal symptoms than sex-typed people (i.e., people with a gender role or personality typology in accordance with their birth-assigned sex) (48). These results emphasize that even if gender roles are better predictors of psychological health than other factors like sex (19–21, 49) or sexual orientation (48, 50), it is still important to take birth-assigned sex into account to better understand how gender roles influence well-being as gender roles and personality operate differently for males and females (20).
1.4 Considerations regarding gender role assessments
The apparent heterogeneity in the literature could be due to several methodological issues including the sample sizes and the way gender roles are conceptualized, operationalized and assessed. Indeed, even if gender roles seem to be consistent across generations, Adams and Sherer suggested in 1985 that classic inventories of gender role like PAQ or BSRI measure constructs like assertiveness and self-efficacy better than gender roles (51). Besides, even if Bem had the original intention to measure gender roles without a negative desirability bias, a study by Grimmell and Sterne (1992) reported that the Bem feminine scale of the BSRI contains both positively and negatively valued traits (52). That is, classic measures of gender roles can suffer from a social-desirability bias that affects the way participants evaluate their stereotyped personality traits. This valuation of their own traits may confound mental health measurement. For example, one group showed that only negatively evaluated aspects of femininity of the Australian Sex Role Scale were associated with suicidality (53). More recent studies indicate that most people nowadays disagree with the “masculine” and “feminine” classifications of some characteristics described by the BSRI, suggesting the need of an alternative way to evaluate gender roles which does not suffer from a time period bias (54).
1.5 Self-identified gender roles or gender role identity
In 1979, Storm created a shortened questionnaire that directly asks participants how they feel about themselves regarding their masculinity and femininity (55) with a simple measure of gender role identity. In this manner, participants fall somewhere on two dimensions comprising their self-perception and perception of others’ perception regarding their masculinity and femininity. Participants are asked to evaluate how they feel, act, and appear to others as more or less feminine and masculine without evoking concepts that can bias their answer regarding both gender role and mental health.
Several studies have underlined the importance of other factors that influence the relationship between gender roles and mental health beyond the questionnaire used. For instance, Sandfort et al. (2021) showed in a US national sample that gender conformity is more present among people with less social status (e.g., age, race/ethnicity, education, income) (56). Gender non-conformity can in turn negatively affect mental health. Taken together, the effects of gender roles on mental health differ according to student/worker status (29), education level (38), race/ethnicity (57), or self-esteem (21, 31). Age also seems to play a key role that influences the effect of gender roles on mental health. For instance, Hunt et al. only succeeded in detecting a significant effect of gender roles on suicidal thoughts among early middle-age participants, but not in early adulthood or late middle-age (58).
1.6 Personality traits and mental health
Beyond age, sex and race/ethnicity, personality traits are another facet of psychosocial functioning that, like gender roles, can influence mental health and behaviors (59–61). The classic NEO-Five factor inventory (62) breaks down personality into five traits: openness, conscientiousness, extroversion, agreeableness, and neuroticism. The link between these personality traits and mental health has been investigated by numerous studies. Overall, it appears that neuroticism, which represents our vulnerability to experience negative affects including anger and emotional instability, is the only trait that strongly and consistently predicts higher anxiety and depressive symptoms for both sexes (63–68). In contract to neuroticism, extroversion, which is the trait that depict enjoyment for activities involving social interactions, seems to correlate with lower anxiety and depression (63, 65).
In addition, different factors are associated with gender roles, like perceived stress (28) or rumination (69), mediate the relationship between neuroticism and anxiety and depressive symptoms (66, 67). Wupperman and Neumann found that masculinity was associated with lower neuroticism (69), highlighting the close relationship between gender roles, mental health and personality traits. It is no surprise then that personality traits also affect suicidality. Indeed, neuroticism, just like for anxiety and depression, strongly and consistently predicts higher suicidal thoughts (17, 70–74) and behaviors (75) regardless of sex (71).
The link between the other traits and suicidality is less clear. The most consistent evidence suggests that lower levels of extroversion (17, 71, 72, 74) and conscientiousness (70, 71, 74) predicts higher rates of suicidal thoughts. A recent review by Szücs highlighted the importance of age in this relationship between personality traits and suicidality. Especially, elderly people who committed suicide displayed lower levels of openness than younger victims (76). As a whole, personality traits can influence the relationship between gender roles and mental health, as they do for sex and depression (77), since they greatly influence how people feel and act, as well as their psychological health.
1.7 Objectives and hypotheses of the present study
To date, gender roles have been associated with mental health outcomes, but results are not consistent, especially regarding the manner in which masculinity and femininity are contextualized and operationalized. Indeed, these mixed results may be due to the methods used. Specifically, some studies have not disaggregated analysis by sex as recommended for rigor and reproducibility in health research (78), and gender roles have mostly been measured by questionnaires that used concepts that may bias participants’ answers. In addition, personality traits should be considered in research on gender roles since they may synergize associations with mental health outcomes.
The present study aims to investigate how self-identified gender roles relate to anxiety, depressive and suicidal symptoms in a well-phenotyped sample drawn from the general population. In sex-specific analyses, we also assess whether personality traits moderate the aforementioned associations. A priori covariates like age, race and ethnicity are also accounted for.
In analyses split by sex, we hypothesize that self-reported femininity will be associated with poorer mental health, as evidenced by higher reported anxiety, depression, and suicidal symptoms. By contrast, masculinity will be associated with lower reported anxiety, depression and suicidal thoughts and behavior. Also, in agreement with the literature, we hypothesize that gender role identity’s effect on mental health will be different in males and females. Specifically, we hypothesize that “cross-typed” profiles (i.e., feminine males and masculine females) will present poorer mental health, while “sex-typed” people will report fewer symptoms of anxiety, depression, and suicide. However, since there is insufficient literature on the role of personality traits as a moderator of associations between gender roles and mental health, we have not explicitly hypothesized directionality for this exploratory hypothesis.
2 Methods
2.1 Participants
This analysis used data from the Nathan Kline Institute Rockland Sample (NKI-RS) (79). The larger NKI-RS project is a comprehensive community sample of participants studied across the lifespan. Efforts have been concentrated on recruitment strategies to avoid over-representation of any portion of the Rockland County community. Recruitment flyers were posted at schools, shopping malls, community centers, and various other locations in Rockland County in New York State. The resulting sample of more than 1000 participants was recruited between 2012 and 2016. As race, ethnicity and economic demographics of Rockland County are similar to those of the United States, the NKI-RS is generalizable to the broader U.S. population. The larger study also includes the collection of rich phenotyping as well as advanced neuroimaging data. For this study, we restricted our analyses to self-reported behavioral data among adults ages 18 and above.
Participants under 18 years old were excluded (n = 155) as the Trait Anxiety Standard Score was only validated and collected for people above 18 years old. Participants with missing data were also excluded (n = 427). In the current analysis, 741 participants (487 females and 254 males) were therefore included from the NKI-RS.
2.2 Ethics statement
Institutional Review Board (IRB) approval was obtained for the original project at the Nathan Kline Institute (Phase I #226781 and Phase II #239708) and at Montclair State University (Phase I #000983A and Phase II #000983B). Written informed consent was obtained for all study participants. An additional IRB approval for our analyses of these data was not required. Instead, we reviewed and signed the NKI-RS Data Usage Agreement.
2.3 General protocol
Data used in this analysis are part of larger dataset mentioned above. For further information, please refer to the NKI-Rockland sample description by K. B. Nooner et al. (79). All participants took part in a 2-day experiment composed of biological data measurements, interviews, questionnaires, magnetic resonance imaging, various cognitive tasks, and behavioral measures. Demographic and gender role identity data were collected at the arrival on the first day (8:15 AM), while all the other data used in this analysis were collected during the one-hour questionnaire phase starting at 1:45 PM the same first day.
2.4 Measures
2.4.1 Demographics
Birth-assigned sex (male/female), age, race, and ethnicity were self-reported. Participants had a mean age of 47.82 years old (SD = 0.66) and were mainly females (65.7%). The sample comprised of White (77.1%), Black (14.3%), Asian (4.9%), American Indian (0.9%), and other-race participants (2.8%). To conduct our analyses, race was turned into a dichotomous variable: White (77.1%) and Non-White (22.9%). Ethnicity is also coded as a dichotomous variable: Hispanic (10.5%) and Non-Hispanic (89.5%).
2.4.2 Gender role identity
A shortened version of the Sex [Gender] Role Identity Scale (GRIS) was used to assess participants’ gender role identity. This 30 item-scale was developed by M. D. Storms in 1979 and has an internal consistency ranging from 0.66 to 0.80 (55). A shortened version of this scale was used to assess how people perceive themselves or think that they are perceived as more feminine and/or masculine. This scale is composed of 6 items, 3 about masculinity and 3 about femininity: “In general, how [masculine] feminine do you think you are?”, “In general, how [masculine] feminine do you think you act or behave?”, and “How [masculine] feminine do you think you appear or come across to others?”. This scale showed strong internal consistency, with the three masculine identity items inter-correlating positively for men (r = .66, p <.001) and for women (r = .68, p <.001) and the three feminine identity items inter-correlating positively for men (r = .80, p <.001) and for women (r = .70, p <.001; Storms, 1979). In the current sample, internal consistency is high for the masculinity sub-scale (Cronbach’s α = .958) and the femininity sub-scale (Cronbach’s α = .969).
Every item is coded on a 5 point-scale: 1 “Not at all”, 2 “Very little”, 3 “Fairly”, 4 “Very much”, 5 “Extremely”, and two scores are then calculated to obtain a femininity score (mean of the 3 feminine items) and a masculinity score (mean of the 3 masculine items) separately. For example, a high score on masculinity and a low score on femininity means that the participant considers that they are and appear to others as high masculine but low feminine. Next, these 2 scores are grouped to form the GRIS index according to the following formula , ranging from -2 (very feminine) to +2 (very masculine). In this manner, a more negative score represents greater femininity relative to masculinity while a more positive score represents greater masculinity relative to femininity. This combined approach allows us to eliminate any issues of multi-collinearity by combining the Masculinity score and the Femininity score as a single GRIS index (Figure 1).
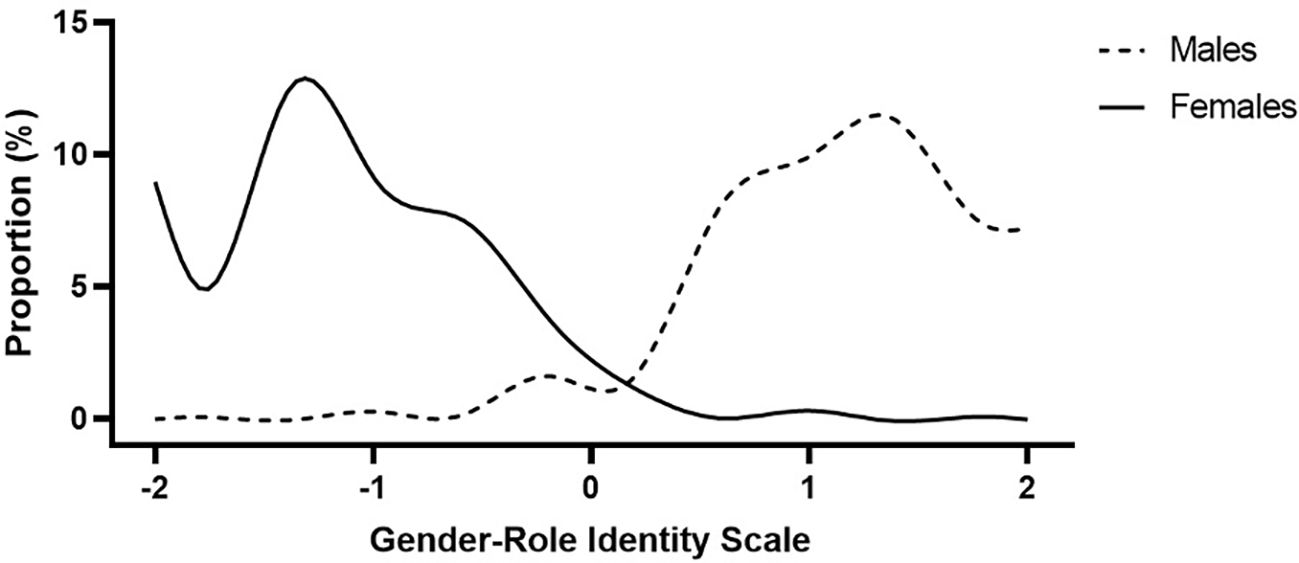
Figure 1. Smoothing splines (12 knots) of the gender role identity scale (GRIS) index distribution among males and females (N = 741). More negative scores represent greater femininity relative to masculinity, and more positive scores represent greater masculinity relative to femininity.
2.4.3 Personality factors
The NEO-FFI is a 60 item self-rating personality assessment instrument developed to provide a more concise measurement of the five personality factors captured in the Revised NEO Personality Inventory (80). The five factors assessed by this instrument include Openness to Experience, Conscientiousness, Extroversion, Agreeableness, and Neuroticism. Participants are asked to choose the answer that represents their opinion on a 5-point Likert scale: 0-Strongly Agree, 1-Agree, 2-Neutral, 3-Disagree, 4-Strongly Disagree for each of the 60 items. Five scores are obtained, one for every personality factor. The original questionnaire has an internal consistency that ranges from 0.68 to 0.86. The test-retest reliability coefficients ranged from .86 to .90 (80).
2.4.4 Mental health
2.4.4.1 Trait anxiety standard score
Participants completed the 40-item State Trait Anxiety Inventory that assesses anxiety in adults ages 18 to 85 (81). Divided into two sections of 20 questions, it measures state and trait anxiety. Both sections use a 4-point scale rating: 1 Almost never, 2 Sometimes, 3 Often, 4 Almost always. A higher score corresponds with greater symptoms of anxiety. The questionnaire has an internal consistency ranging from.86 to.95. The test-retest reliability also ranges from .65 to .75 over an interval of 2 months (82).
2.4.4.2 Beck depression inventory
Participants completed the 21-item Beck Depression Inventory II. This questionnaire aimed at assessing the severity of typical symptoms of depression such as mood, pessimism, self-dislike, and insomnia. Participants had to choose an answer on a 4-point scale that best describes how they have been feeling during the past two weeks. A higher score corresponds to greater symptoms of depression. The questionnaire has a strong internal consistency coefficient of .91 (83), as well as an high test-retest reliability coefficient of .93 (84).
2.4.4.3 Suicidality
Suicidality was assessed by the combination of two scores assessing suicidal ideation and suicide attempts. Suicidal ideation was assessed using self-report measures from the Adult Self-Report (ages 18-59) and the Older Adult Self-Report (ages 60+). Each participant was administered the age-appropriate assessment, which included the statement, “I think about killing myself.” Participants endorsed either “not true”, “somewhat or sometimes true” or “very true or often true.” Suicidal ideation was then binary coded as “yes” if the participant answered “somewhat or sometimes true” or “very true or often true”, or “no” if the participant answered “not true”. Suicide attempt/self-harm was assessed using self-report measures (i.e., the Adult Self-Report and the Older Adult Self-Report) based on responses to the statement “I deliberately try to harm or kill myself.” Participants endorsed either “not true”, “somewhat or sometimes true”, or “very true or often true.” Suicidal behaviors were then binary coded as “yes” or “no” in the same way as for suicidal thoughts. Additionally, participants who indicated a history of suicide attempt in their medical history were included.
Suicide scores were then coded as an ordinal variable. Participants with no suicidal ideation and behavior were coded as “0”, “1” for suicidal thoughts only, “2” for suicidal thoughts and behaviors. Considering the low rate of people with “1” (n = 31) and “2” (n = 10) scores, suicide score will be analyzed as a continuous variable in the following analyses.
2.5 Statistical analyses
Statistical analyses were conducted using IBM Statistical Package for the Social Sciences (SPSS) (version 26). Considering the large sample size of the NKI-RS and that sex is an important factor for every variable, all analyses were split by sex as recommended by Clayton and Tannenbaum for improving rigor and reproducibility (78). The sample sizes and degrees of freedom for each statistical model differ slightly since not all measures were collected from all participants at the same time.
2.5.1 Preliminary analyses
First, we conducted independent sample t-tests for personality traits, gender role identity, anxiety symptoms, depressive symptoms, and suicide scores to investigate if there are sex differences in these key study variables. Then, we conducted correlation analyses between our 14 variables in females and males separately for descriptive purposes. To investigate the effect of gender role identity scores (GRIS index, Masculinity score, Femininity score) on personality traits, we also conducted three separate multivariate analysis of variance (MANOVA) in females and males separately (see results in the Supplementary). Finally, we conducted multiple linear regression analysis with TAS, BDI, and suicide scores as dependent variables to investigate the effect of personality traits on mental health in females and males separately. We adjusted for age, race, and ethnicity for this last preliminary analysis that is reported next.
2.5.2 Main analyses
First, to assess the effect of gender role identity scores on mental health, we conducted multiple linear regression analyses with GRIS index, Femininity scores, and Masculinity scores as independent variables in females and males separately. Secondly, to investigate if there is an interaction effect between personality traits and gender roles on mental health, we performed moderation analyses using PROCESS macro for SPSS (85) with gender roles as predictor and each personality trait, which appeared significant in the precedent analyses, as observed in females and males separately. When two personality traits appeared to be significant predictors of mental health variables in multiple linear regression analyses, we used one of them as a moderator and the other one as a covariable, then vice versa, in moderation analyses. We adjusted for age, race, and ethnicity for every main analysis.
3 Results
3.1 Preliminary analyses
3.1.1 Sex differences
Tables 1 and 2 present correlations between age, gender role identity, personality traits, and mental health for males and females. T-tests showed no significant sex differences in conscientiousness (t(460) = -0.050, p = .960), agreeableness (t(734) = 0.367, p = .714), depression (t(624) = -0.682, p = .495), or suicide scores (t(461) = 1.361, p = .174). Significant differences emerged for openness (t(732) = 4.62, p <.001), extroversion (t(453) = 2.41, p = .016), neuroticism (t(737) = 2.464, p = .014), GRIS (t(739) = 48.78, p <.001), masculinity (t(739) = 40.40, p <.001), femininity (t(603) = -45.95, p <.001), and anxiety (t(576) = -2.38, p = .018).
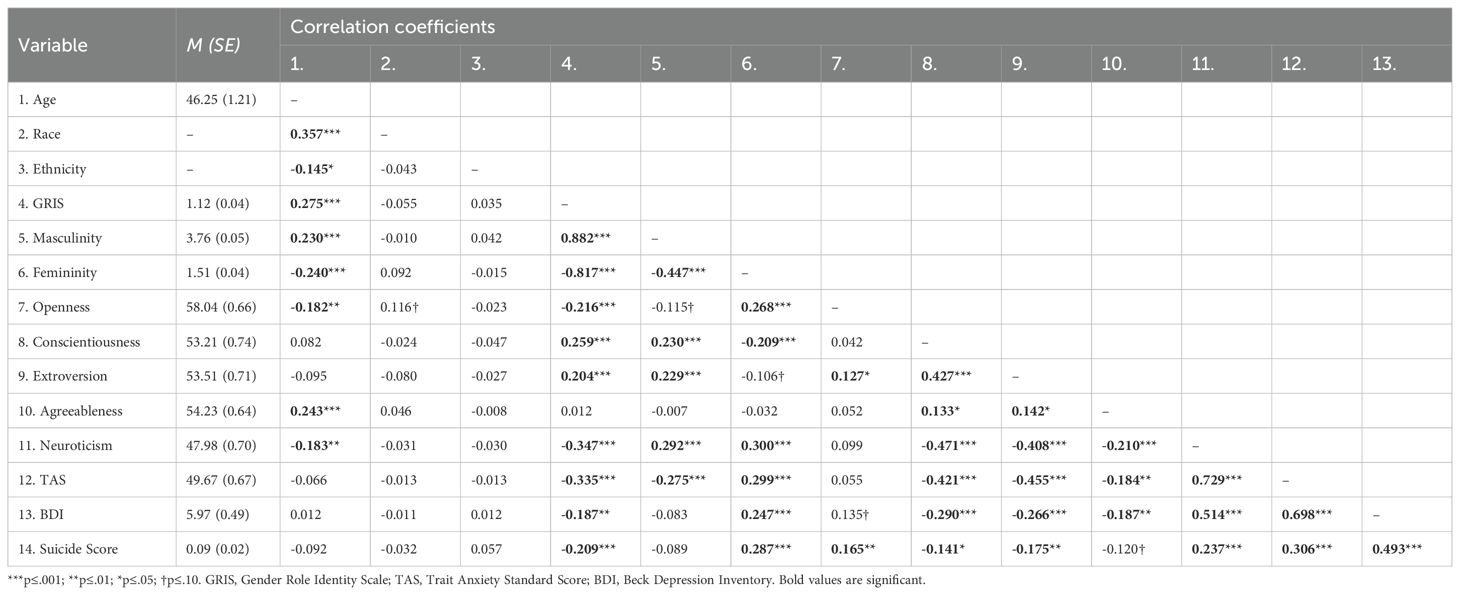
Table 1. Correlation matrix for males.
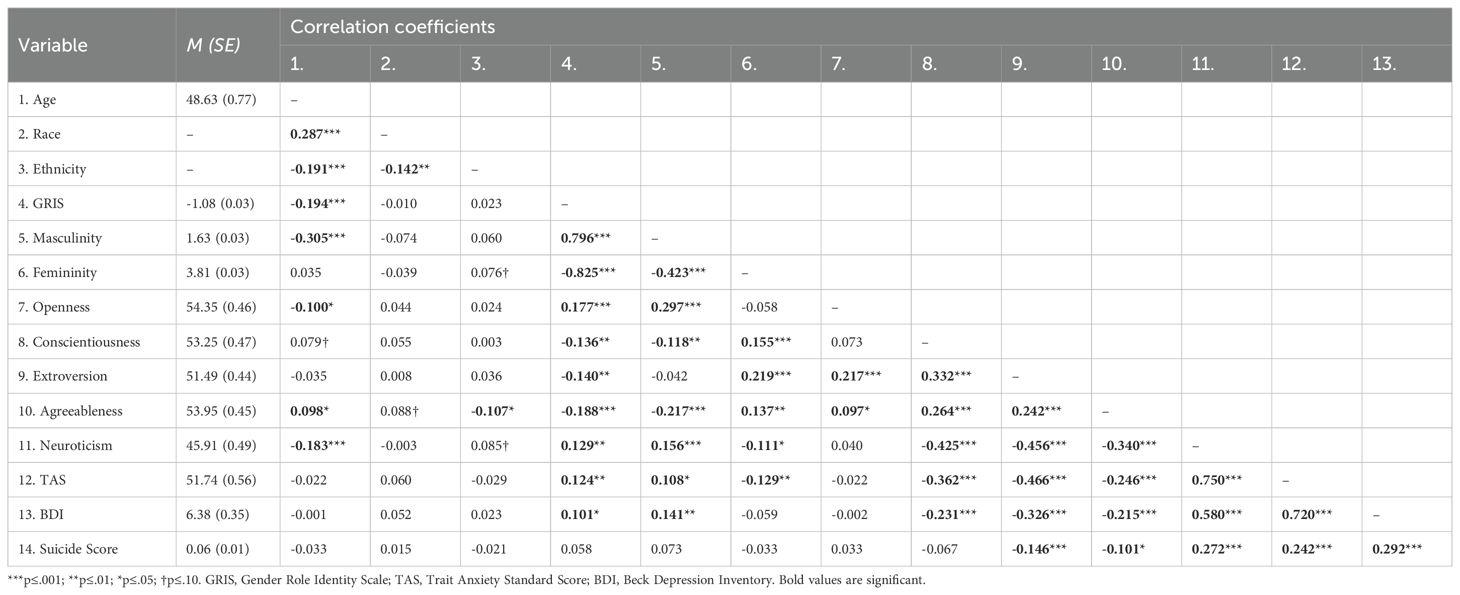
Table 2. Correlation matrix for females.
Males scored higher on openness (M = 58.04, SD = 10.39), extroversion (M = 53.51, SD = 11.28), neuroticism (M = 47.98, SD = 11.11), GRIS (M = 1.12, SD = 0.57), and masculinity (M = 3.76, SD = 0.73) compared to females (M = 54.35, SD = 10.19; M = 51.49, SD = 9.80; M = 45.91, SD = 10.72; M = -1.08, SD = 0.59; M = 1.63, SD = 0.65). Females scored higher on femininity (M = 3.81, SD = 0.73 vs. M = 1.51, SD = 0.60) and anxiety (M = 51.74, SD = 12.26 vs. M = 49.67, SD = 10.61).
3.1.2 Personality and mental health
3.1.2.1 Males
For anxiety, regression showed a significant model (F(8, 237) = 38.165, p <.001, R²adj = 0.548) with effects of extroversion (β = -0.154, t(237) = -3.222, p = .001) and neuroticism (β = 0.609, t(237) = 12.122, p <.001). For depression, the model was significant (F(8, 197) = 10.407, p <.001, R²adj = 0.269) with neuroticism as a predictor (β = 0.291, t(197) = 6.216, p <.001). For suicidality, the model was significant (F(8, 239) = 3.331, p = .001, R²adj = 0.070) with openness (β = 0.005, t(239) = 2.552, p = .011) and neuroticism (β = 0.004, t(239) = 1.980, p = .049) as predictors (Table 3).
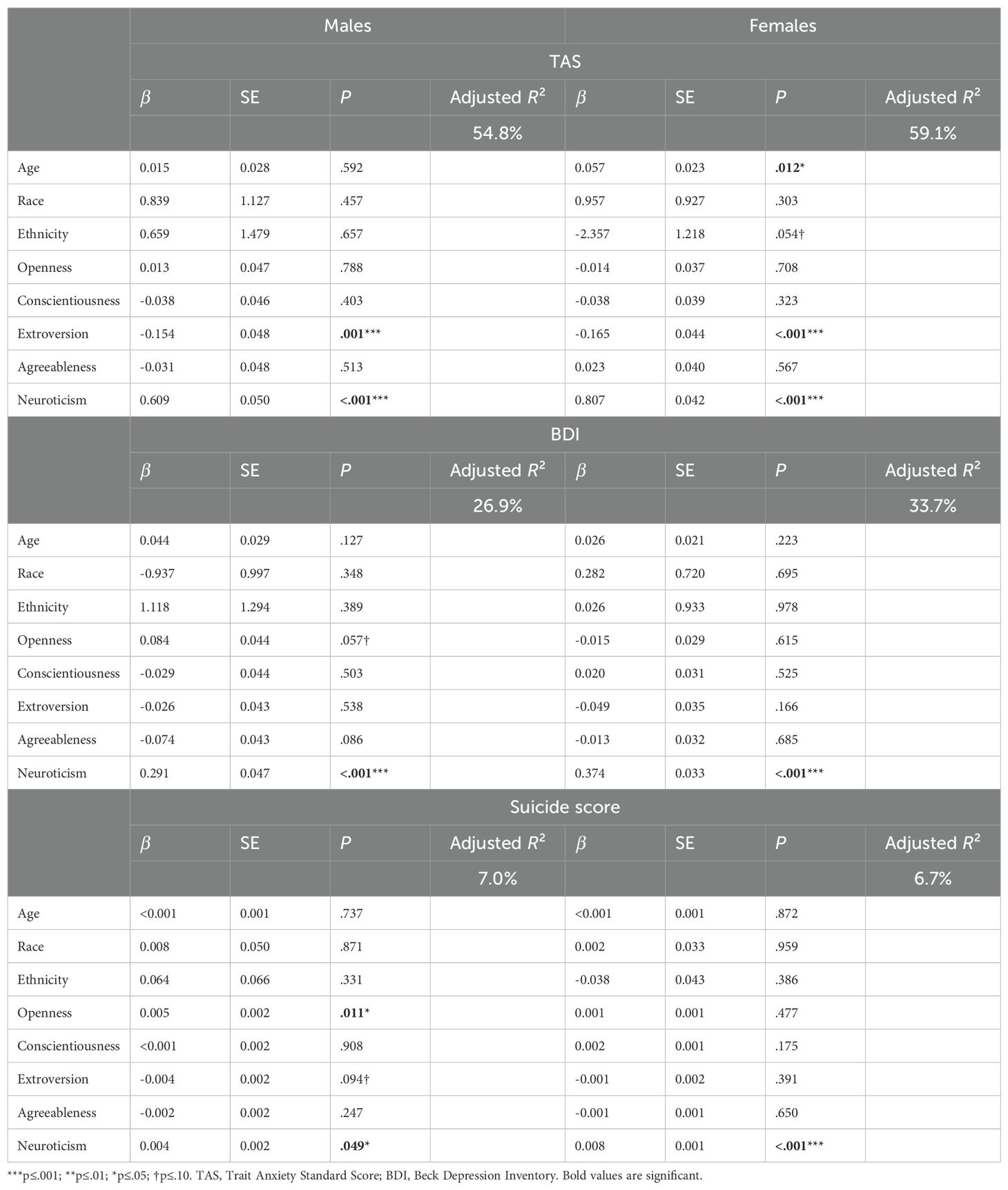
Table 3. Linear regressions of personality traits to predict mental health.
3.1.2.2 Female
For anxiety, the model was significant (F(8, 474) = 88.145, p <.001, R²adj = 0.591) with effects of extroversion (β = -0.165, t(474) = -3.765, p <.001), neuroticism (β = 0.807, t(474) = 19.165, p <.001), and age (β = 0.057, t(474) = 2.513, p = .012). For depression, the model was significant (F(8, 403) = 27.124, p <.001, R²adj = 0.337) with neuroticism as a predictor (β = 0.374, t(403) = 11.257, p <.001). For suicidality, the model was significant (F(8, 475) = 0.416, p <.001, R²adj = 0.067) with neuroticism as a predictor (β = 0.008, t(475) = 5.035, p <.001) (Table 3).
3.2 Main analyses
3.2.1 Gender roles and mental health
3.2.1.1 Males
GRIS significantly predicted anxiety (F(4, 247) = 8.162, p <.001, R²adj = 0.102; β = -6.176, t(247) = -5.245, p <.001), depression (F(4, 206) = 1.971, p = .100, R²adj = 0.018; β = -2.466, t(206) = -2.750, p = .006), and suicidality (F(4, 249) = 3.249, p = .013, R²adj = 0.034; β = -0.113, t(249) = -3.013, p = .003) (Table 4).
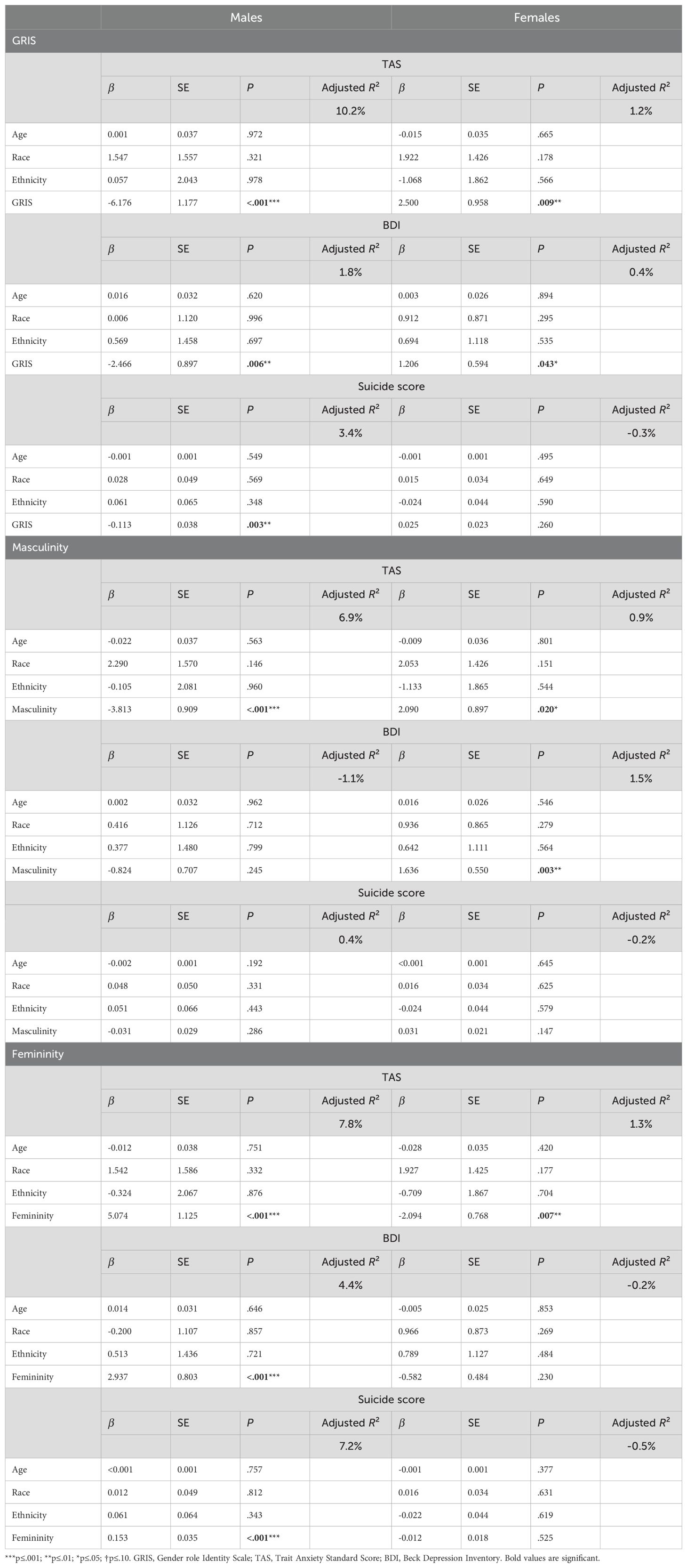
Table 4. Linear regressions of gender roles to predict mental health.
Masculinity predicted anxiety (F(4, 247) = 5.643, p <.001, R²adj = 0.069; β = -3.813, t(247) = -4.198, p <.001) but not depression (F(4, 206) = 0.417, p = .796) or suicidality (F(4, 249) = 1.237, p = .296). Femininity predicted anxiety (F(4, 247) = 6.335, p <.001, R²adj = 0.078; β = 5.074, t(247) = 4.510, p <.001), depression (F(4, 206) = 3.429, p = .010, R²adj = 0.044; β = 2.937, t(206) = 3.659, p <.001), and suicidality (F(4, 249) = 5.872, p <.001, R²adj = 0.072; β = 0.153, t(249) = 4.405, p <.001) (Table 4).
3.2.1.2 Females
GRIS predicted anxiety (F(4, 481) = 2.449, p = .045, R²adj = 0.012; β = 2.500, t(481) = 2.611, p = .009) and depression (F(4, 410) = 1.425, p = .225; β = 1.206, t(410) = 2.029, p = .043), but not suicidality (F(4, 482) = 0.601, p = .662) (Table 4).
Masculinity predicted anxiety (F(4, 481) = 2.100, p <.001, R²adj = 0.009; β = -3.813, t(481) = 2.330, p <.001) and depression (F(4, 410) = 2.610, p = .035, R²adj = 0.015; β = 1.636, t(410) = 2.973, p = .003), but not suicidality (F(4, 482) = 0.812, p = .518). Femininity predicted anxiety (F(4, 481) = 2.605, p = .035, R²adj = 0.013; β = -2.094, t(481) = -2.727, p = .007), but not depression (F(4, 410) = 0.755, p = .555) or suicidality (F(4, 482) = 0.385, p = .820) (Table 4).
3.2.2 Moderation analyses
Moderation (Table 5) showed extroversion moderated the effect of GRIS on anxiety in males (t(243) = 2.194, p = .029, ΔR² = 0.008), with GRIS predicting anxiety only at low extroversion (β = −3.450, 95% CI [-5.816, -1.084], p = .004). Extroversion also moderated masculinity’s effect on anxiety (t(243) = 2.391, p = .018, ΔR² = 0.010), significant only at low extroversion (β = -2.398, 95% CI [-4.264, -0.533], p = .012). Neuroticism moderated the GRIS–suicidality relation (t(240) = -2.554, p = .011, ΔR² = 0.024), with GRIS predicting suicidality only at high neuroticism (β = -0.136, 95% CI [-0.228, -0.043], p = .004). No significant moderation effects were found in females (Table 6) (Figure 2).

Table 5. Moderation analyses to predict mental health among males.
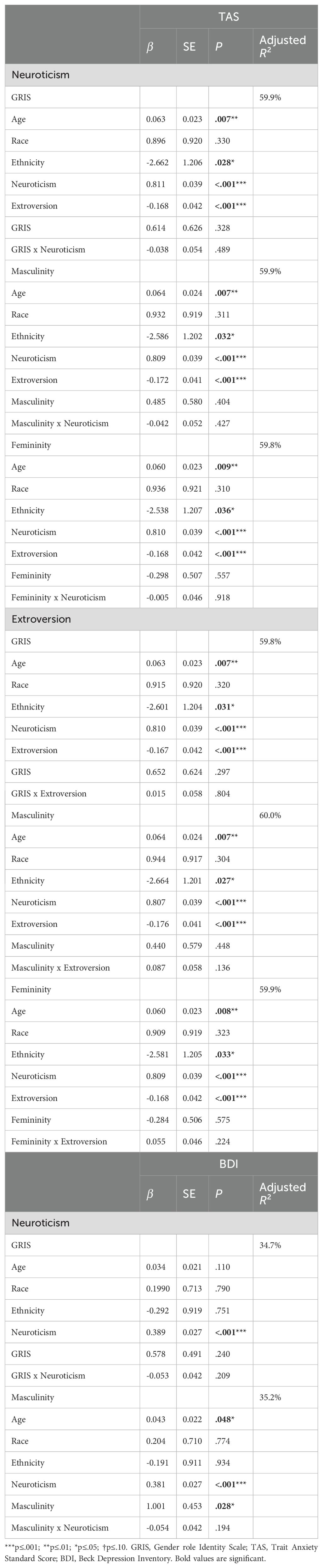
Table 6. Moderation analyses to predict mental health among females.
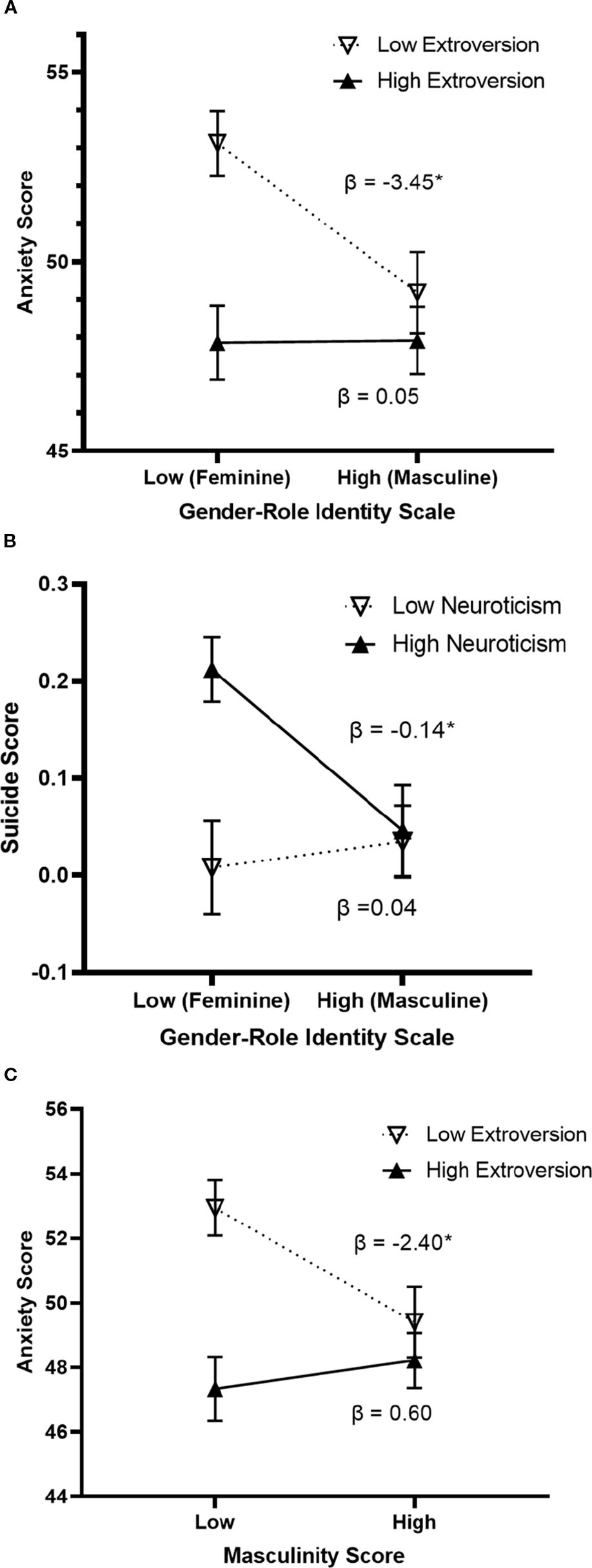
Figure 2. Moderation effect of personality traits on the relationship between gender roles and mental health among males (N = 254). Graph (A) Difference in anxiety scores between feminine and masculine males is only significant for males with low levels of extroversion. Graph (B) Difference in suicide scores between feminine and masculine males is only significant for males with high levels of neuroticism. Graph (C) Difference in anxiety scores between less masculine and more masculine males is only significant for males with low levels of extroversion *p≤.05.
4 Discussion
The main objective of the present study was to investigate the associations among gender role identity and anxiety symptoms, depressive symptoms and suicidality in the general population. We found that having a gender role identity contrary to one’s birth-assigned sex was associated with a poorer overall mental health (i.e., more anxiety symptoms, depressive symptoms, and suicidality) depending on birth-assigned sex. Moreover, we found this relationship to be moderated by neuroticism and extroversion for males only.
4.1 Gender role identity and personality traits
Preliminary analyses highlighted that self-assessed gender roles correlated with all personality traits except agreeableness in males, and all mental health measures except suicidality in females. Anxiety symptoms, depressive symptoms, and suicidal thoughts and behaviors were also inter-correlated, consistent with the existing literature (86). Contrary to previous studies (11, 12), our analyses did not find a difference in depression scores between males and females. Surprisingly, males from our sample reported higher neuroticism levels than females, which does not align with existing literature showing the opposite pattern (87, 88). However, as expected, gender role identity scores were substantially different between males and females.
4.2 Gender role identity and mental health
Consistent with our hypothesis, people with a “cross-typed” or “incongruent” gender role profile (i.e., with a gender role identity opposite to their birth-assigned sex) reported poorer mental health, which is consistent with previous work (48). This is also consistent with congruence models of gender roles that state that gender role alignment with birth-assigned sex is less distressing (37). However, this effect turned out to be much stronger in males, where femininity was highly associated with more anxiety symptoms, depressive symptoms, and suicidality. Masculinity in females, however, was less strongly but still significantly associated with anxiety and depressive symptoms. These results are consistent with existing literature where femininity in males have been associated with poorer mental health (33, 89). Notwithstanding, these findings must expanded and replicated using approaches that assess multidimensional gender role profiles.
In contrast to males, our findings only partially align with findings regarding gender roles and mental health in females. In assessing gender roles categorically, undifferentiated females (i.e., females with low levels of masculinity and femininity) usually demonstrate higher anxiety and depression. These observations have been attributed to the low levels of masculinity which would otherwise have a protective effect (29, 37). Other research reported that higher femininity in females was associated with more anxiety (21) and depressive symptoms (39, 40). Our results suggest that it is masculinity, and not femininity, which is associated with higher levels of anxiety and depressive symptoms in females. This being said, our analyses did not allow us to explore other gender configurations (e.g., androgyny).
4.3 The concept of gendered societal burden
Our results and the method we used strongly suggest that several forces predict how gender role identity impacts mental health. The main force may be related to the congruence between one’s gender role identity and birth-assigned sex. Having masculine gender role identity among females and feminine gender role identity for males is linked to poorer mental health. This “gendered societal burden” may be strengthened by society’s perception which promotes sex-typed gender roles (89, 90), resulting in more stress-related issues in gender “incongruent” or non-conforming people (91). For instance, feminine gay men tend to experience anti-effeminacy prejudice (90, 92). In addition, being feminine is more likely to be associated with being perceived as gay in men than in women (93). That is, feminine men can suffer from homophobic discrimination regardless of their sexuality. In other research, homophobic discrimination impacts both anxiety and depressive symptoms above and beyond other psychological stressors. This effect is stronger among men compared to women (94). Unfortunately, sexual orientation was not ascertained in this study. Taken together, those societal issues relate to the concept of gender relations and can partially explain differences observed between males and females regarding gender roles and their relation on mental health as an elusive form of gendered societal burden related to expectations of masculine and feminine expressions. We encourage future analyses to further explore the role of sexual orientation and gender identity relative to gender role in mental health research.
4.4 The concept of gendered traits burden
Another force that can influence the relationship between gender roles and mental health is the nature of what characterizes personality traits as stereotypically “feminine” or “masculine”. Indeed, traits are classified as feminine and masculine based on their prevalence in each sex within a given society at a particular moment in history (25, 26). However, anxiety and depressive symptoms tend to be more prevalent in females than in males (11, 12). Overall, boys and men experience more restrictive prescriptive stereotypes than girls and women across life, and therefore variations in gender expression are more likely to be punished (95). Then, it makes sense to think that characteristics judged as “feminine” should be associated with poorer mental health. Some literature shows that this is the case (40). In this sense, this “gendered traits burden” based on gendered characteristics would not be based on birth-assigned sex per se. Instead, this could be associated with a protective effect in masculine people; however, this will need to be assessed in future studies that nuance different gender models (e.g., congruence, androgyny, gender-typed) as articulated elsewhere (37).
4.5 The “two-forces” hypothesis to explain literature inconsistencies
These two forces combined (i.e., gendered societal burden & gendered traits burden) may explain why feminine men in our study report poorer mental health, as well as explain why gender roles impact women’s mental health less consistently. Studies using validated questionnaires with gendered items like the BSRI and the PAQ might focus on the gendered traits burden only, whereas studies like ours may reflect a combination of both forces, especially as they relate to “cross-typed” gender role profiles. This hypothesis needs more investigation to be clearly assessed, but it underlines the importance of diversity in the methods used to assess gender roles to fully understand their relationship with mental health.
4.6 Personality traits and mental health
Personality traits have been strongly associated with mental health (63) independent of gender roles, but findings are inconsistent (75, 76, 96). In accordance with existing literature and our hypothesis, neuroticism appeared to be the most important personality trait predictive of mental health (63, 65). Indeed, neuroticism is the strongest factor predictive of both anxiety and suicidal thoughts and behaviors. Neuroticism is also the only significant trait to positively predict depressive symptoms for both sexes. In addition, our results suggest that extroversion is the second most important trait to predict anxiety in both males and females. Specifically, the more a person is extroverted, the less they report anxiety. A recent study also showed the best mental health profiles among androgynous individuals with high scores in both masculinity and femininity, as well as high scores in extraversion, openness to experience, emotional stability, agreeableness, and conscientiousness (97). Note, however, that results in our study are driven by feminine males and must be replicated before making any conclusions.
These results are in accordance with some studies (65). However, the present study did not find an effect of extroversion on depressive symptoms, whereas this trait has been more consistently negatively associated with depression in the literature (63, 98). Otherwise, openness was also significatively associated with suicidal thoughts and behaviors, but only in males. This result highlights that different factors affect suicidality among males and females, and suggest that personality traits, in relation to gender roles and birth-assigned sex, may in part account for the “gender paradox” (i.e. higher women suicide attempts versus higher men suicide completion (5)).
4.7 Neuroticism moderates the relationship between gender role identity and suicidality
As personality traits are linked to the way people feel, act, and appear to others (62), they may impact the relationship between gender role identity and mental health. Moderation analyses revealed that some personality traits moderate this relationship but only among males, where the effect of gender role identity on mental health is much stronger than in females. Specifically, neuroticism, which is strongly associated with a poorer mental health (65), moderates the effect of the gender role identity on suicidality. Interestingly, it appears that only highly neurotic males display the deleterious effect of cross-typed profile on suicidality. Indeed, males with low levels of neuroticism did not report suicidal thoughts or behaviors, neither when they were highly feminine or highly masculine. Conversely, masculine males reported low suicidality regardless of whether they were neurotic or not. Only feminine neurotic males reported significantly higher suicidal thoughts and behaviors.
4.8 Implications for understanding the gender paradox in mental health
Our findings highlight the protective aspect of masculinity against suicidal ideation and self-injury in males that have been consistently reported in the literature (53, 58). Furthermore, they bring a new perspective to the “gender paradox” in mental health. In summary, our results suggest that it is important to consider the core relationships among gender roles, personality traits, and birth-assigned sex collectively when endeavoring to explain gender differences in suicidality. This underlines the fact that it is not only women who display more suicidal thoughts and behaviors, but also men with specific characteristics (i.e., feminine and neurotic). One caveat is that our sample was composed of living people, which limits us from making conclusions about gender roles in relation to suicide completion that is an essential endpoint of the “gender paradox” in suicide. From this perspective, specific gender roles and behaviors may indeed influence some suicide-related characteristics, like the use of lethal means that have been proposed to explain why men complete more suicide than women (99, 100). Further research is required to fully understand the impact of specific gender roles in relation to suicide completion to explain higher prevalence in men.
4.9 Extroversion moderates the relationship between gender role identity and anxiety
On the other hand, our analyses revealed that extroversion moderates the relation between gender role identity and anxiety. A similar moderation effect was detected for masculinity alone. It appears that extroverted people (i.e., with high levels of extroversion) have low anxiety scores, regardless of whether they are feminine or masculine. Gender role identity differences in anxiety were only observed in males with low levels of extroversion. Taken together, only low-extroverted feminine males reported significantly higher levels of anxiety. Extroversion is a trait that depicts our relationship to others the most by “initiating social contacts” (101). In this sense, by expressing their femininity, more extroverted feminine males may be able to experience anxiety levels more akin to masculine males, thwarting the deleterious effect of their cross-typed profile. Conversely, feminine characteristics of males that are less extroverted may exacerbate their anxiety by concealing a part of them that they perceive society reprimands and censors. This hypothesis needs to be more thoroughly investigated in future studies in cross-cultural contexts.
Similar to our first moderation analysis described above, these results put forward the protective effect of masculinity against anxiety which has been consistently observed in the literature (21, 29, 36, 102). However, our results underline the importance of considering personality traits to better understand the circumstances in which this protective effect manifests itself in diverse contexts. Interestingly, personality traits that moderate the relationship between gender role profiles and mental health are not the same depending on the psychiatric symptom or construct being studied. Considering that anxiety is an important risk factor for suicidal behaviors (10, 103), our study highlights that restricting research to gender roles and mental health without taking into account the influence of different personality traits might miss important connections with mental health.
4.10 Limitations
The present study has limitations worth discussing. In contrast to previous studies that assessed gender roles using inventories of gendered personality traits (e.g., the Bex Sex Role Inventory, Personal Attributes Questionnaire), participants directly assessed their gender roles broadly. Other gender role instruments were also originally constructed to assess adaptive androgyny defined as high masculinity and high femininity. As gender roles can depend on society and how people are socialized, the concepts of what is deemed feminine/masculine may differ from one culture to another. Even if recruiting people from the same geographic location (i.e., Rockland town) might reduce confounding, further studies should be conducted in areas where conceptualizations of masculinity and femininity are different to assess if these results generalize to other cultures and environments.
Furthermore, the present study only considered gender role identity as a continuum. As such, results are limited to cross-typed and sex-typed profiles (i.e., feminine and masculine people), without looking at people presenting high or low levels of both masculinity and femininity (i.e., androgynous and undifferentiated people). To address this limitation, we conducted analyses with both continuous and categorical approaches (data not shown). Unfortunately, categorical approaches did not provide more information than the continuous approach we reported, so we did not include these in our report. This absence of significant differences may be due to the measurement methods. Indeed, gender roles can be conceptualized along a single continuum when participants self-report (e.g., being more masculine will decrease their femininity), resulting in a limitation of the number of androgenous and undifferentiated profiles. This is in contrast to Bem’s theory that masculinity and femininity are two independent continuums; however, this assumption has nothing to do with how people self-report with their own personal assumptions of their gender role identity.
Another limitation is that the present study considered suicidality as a continuum from no suicidal thoughts or behaviors to the presence of both. This decision was made with analytic consideration for the low rate of suicidal behaviors in the studied sample from general population. Suicide scores were then analyzed as a continuous variable, preventing the dissociation between suicidal thoughts only and suicidal behaviors. However, literature has shown that risk factors for suicidal ideations differ from those for suicide attempt (104). In addition, the current study cannot provide information for the relationship between gender roles, personality traits, and suicide completion. Finally, even if the present study emphasizes the effect of gender role identity and personality traits on mental health, it does not assess which factors cause or influence the other. Another issue is potential confounding related to neuroticism that is associated with anxiety and depression (105) while also interacting with gendered behaviors (106). Further longitudinal studies and mediation analysis need to be conducted to address causal pathways, especially with designs assessing lifespan development.
5 Conclusion
Our study offers new insight into the complex interplay of gender roles, personality, and mental health. Self-assessed masculinity and femininity predict anxious, depressive, and suicidal symptoms, but in sex-specific ways. Notably, adopting a gender role contrary to birth-assigned sex is linked to poorer mental health, with effects especially pronounced in males. This suggests that both cross-typed profiles and feminine characteristics heighten vulnerability to distress in men. Personality further shapes these dynamics: only neurotic feminine males reported greater suicidal symptoms, and only less extroverted feminine males reported higher anxiety. These findings underscore the need to account for personality traits alongside sex and gender roles in mental health research, and to pursue further studies clarifying the mechanisms underlying these associations.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: Nathan Kline Rockland Sample (https://rocklandsample.org).
Ethics statement
The studies involving humans were approved by Montreal Mental Health University Institute. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MR: Writing – review & editing, Writing – original draft, Formal Analysis, Methodology, Visualization, Data curation, Validation, Conceptualization. MA: Writing – review & editing, Writing – original draft, Formal Analysis, Validation. MS: Writing – original draft, Methodology, Writing – review & editing, Conceptualization. TS: Writing – review & editing, Writing – original draft. FJ: Writing – review & editing, Validation, Supervision, Writing – original draft, Formal Analysis. MM: Writing – original draft, Supervision, Validation, Writing – review & editing. SP: Methodology, Conceptualization, Validation, Writing – original draft, Funding acquisition, Writing – review & editing. RJ: Supervision, Data curation, Conceptualization, Writing – review & editing, Writing – original draft, Methodology, Investigation, Funding acquisition, Resources, Project administration, Validation.
Funding
The author(s) declare financial support was received for the research and/or publication of this article. M Rossi was supported by the Fonds de recherche Québec Santé Masters award. RP-J was supported by post-doctoral funding from the Fonds de recherche du Québec Sante (FRQS) as well as from a Banting fellowship. RP-J is currently supported by FRQS (Jr1–269532: https://doi.org/10.69777/269532 & Jr2–332273: https://doi.org/10.69777/332273) and the Foundation of the Montreal Mental Health University Institute. RP-J held a Canadian Institutes of Health Research Sex and Gender Science Chair from 2020 to 2024. This work was also supported by American Foundation for Suicide Prevention (AFSP) SRG-0-102-16 to SP. Dr. TS contribution has been supported by a grant from the National Institutes of Health (P30-MH43520; PI: Remien). Open-access support for this publications comes from a FRQS Alliance Santé Mentale awarded to RP-J.
Acknowledgments
We would like to thank the Nathan Kline Institute for their data collection. We would like to thank Julia Lushing for assistance with data curation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Any alternative text (alt text) provided alongside figures in this article has been generated by Frontiers with the support of artificial intelligence and reasonable efforts have been made to ensure accuracy, including review by the authors wherever possible. If you identify any issues, please contact us.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fpsyt.2025.1594762/full#supplementary-material
References
1. Gove WR. Sex differences in mental illness among adult men and women: An evaluation of four questions raised regarding the evidence on the higher rates of women. Soc Sci Med Part B: Med Anthropol. (1978) 12:187–98. doi: 10.1016/0160-7987(78)90032-7
2. Murphy GE. Why women are less likely than men to commit suicide. Compr Psychiatry. (1998) 39:165–75. doi: 10.1016/s0010-440x(98)90057-8
3. Canetto SS and Sakinofsky I. The gender paradox in suicide. Suicide Life-Threatening Behavior. (1998) 28:1–23. doi: 10.1111/j.1943-278X.1998.tb00622.x
4. Henderson JP, Mellin C, and Patel F. Suicide - a statistical analysis by age, sex and method. J Clin Forensic Med. (2005) 12:305–9. doi: 10.1016/j.jcfm.2005.05.003
5. Schrijvers DL, Bollen J, and Sabbe BG. The gender paradox in suicidal behavior and its impact on the suicidal process. J Affect Disord. (2012) 138:19–26. doi: 10.1016/j.jad.2011.03.050
6. Diamantopoulou S, Verhulst FC, and van der Ende J. Gender differences in the development and adult outcome of co-occurring depression and delinquency in adolescence. J Abnormal Psychol. (2011) 120:644–55. doi: 10.1037/a0023669
7. La Greca AM and Lopez N. Social anxiety among adolescents: linkages with peer relations and friendships. J Abnorm Child Psychol. (1998) 26:83–94. doi: 10.1023/A:1022684520514
8. Lamers F, van Oppen P, Comijs HC, Smit JH, Spinhoven P, van Balkom AJ, et al. Comorbidity patterns of anxiety and depressive disorders in a large cohort study: the Netherlands Study of Depression and Anxiety (NESDA). J Clin Psychiatry. (2011) 72:341–8. doi: 10.4088/JCP.10m06176blu
9. Zhang J, Fang L, Wu YW, and Wieczorek WF. Depression, anxiety, and suicidal ideation among Chinese Americans: a study of immigration-related factors. J Nervous Ment Disease. (2013) 201:17–22. doi: 10.1097/NMD.0b013e31827ab2e2
10. Turecki G, Brent DA, Gunnell D, O’Connor RC, Oquendo MA, Pirkis J, et al. Suicide and suicide risk. Nat Rev Dis Primers. (2019) 5:74. doi: 10.1038/s41572-019-0121-0
11. Bebbington P. The origins of sex differences in depressive disorder: bridging the gap. Int Rev Psychiatry. (1996) 8:295–332. doi: 10.3109/09540269609051547
12. McHenry J, Carrier N, Hull E, and Kabbaj M. Sex differences in anxiety and depression: Role of testosterone. Front Neuroendocrinol. (2014) 35:42–57. doi: 10.1016/j.yfrne.2013.09.001
13. Gough B and Novikova I. Mental health, men and culture: how do sociocultural constructions of masculinities relate to men’s mental health help-seeking behaviour in the WHO European Region? Vol. 2020. Copenhagen: World Health Organization. Regional Office for Europe, Health Evidence Network synthesis report, No. 70 (2020). 58 p. Available online at: https://apps.who.int/iris/handle/10665/332974 (Accessed August 14, 2019).
14. Chatzittofis A, Nordstrom P, Hellstrom C, Arver S, Asberg M, and Jokinen J. CSF 5-HIAA, cortisol and DHEAS levels in suicide attempters. Eur Neuropsychopharmacol. (2013) 23:1280–7. doi: 10.1016/j.euroneuro.2013.02.002
15. Labaka A, Goñi-Balentziaga O, Lebeña A, and Pérez-Tejada J. Biological sex differences in depression: A systematic review. Biol Res For Nursing. (2018) 20:383–92. doi: 10.1177/1099800418776082
16. Cohen A, Gilman SE, Houck PR, Szanto K, and Reynolds CF 3rd. Socioeconomic status and anxiety as predictors of antidepressant treatment response and suicidal ideation in older adults. Soc Psychiatry Psychiatr Epidemiol. (2009) 44:272–7. doi: 10.1007/s00127-008-0436-8
17. Chioqueta AP and Stiles TC. Personality traits and the development of depression, hopelessness, and suicide ideation. Pers Individ Dif. (2005) 38:1283–91. doi: 10.1016/j.paid.2004.08.010
18. Canetto SS. Women and suicidal behavior: a cultural analysis. Am J Orthopsychiatry. (2008) 78:259–66. doi: 10.1037/a0013973
19. Carter R, Silverman WK, and Jaccard J. Sex variations in youth anxiety symptoms: effects of pubertal development and gender role orientation. J Clin Child Adolesc Psychol. (2011) 40:730–41. doi: 10.1080/15374416.2011.597082
20. Lengua LJ and Stormshak EA. Gender, gender roles, and personality: gender differences in the prediction of coping and psychological symptoms. Sex Roles. (2000) 43:787–820. doi: 10.1023/A:1011096604861
21. Palapattu AG, Kingery JN, and Ginsburg GS. Gender role orientation and anxiety symptoms among African American adolescents. J Abnorm Child Psychol. (2006) 34:423–31. doi: 10.1007/s10802-006-9023-1
22. Evans O and Steptoe A. The contribution of gender-role orientation, work factors and home stressors to psychological well-being and sickness absence in male- and female-dominated occupational groups. Soc Sci Med. (2002) 54:481–92. doi: 10.1016/s0277-9536(01)00044-2
23. Juster RP, Pruessner JC, Desrochers AB, Bourdon O, Durand N, Wan N, et al. Sex and gender roles in relation to mental health and allostatic load. Psychosomatic Med. (2016) 78:788–804. doi: 10.1097/PSY.0000000000000351
24. Bem SL. Gender schema theory: A cognitive account of sex typing. psychol Review. (1981) 88:354–64. doi: 10.1037/0033-295X.88.4.354
25. Spence JT, Helmreich R, and Stapp J. Ratings of self and peers on sex role attributes and their relation to self-esteem and conceptions of masculinity and femininity. J Pers Soc Psychol. (1975) 32:29–39. doi: 10.1037/h0076857
26. Bem SL. The measurement of psychological androgyny. J Consulting Clin Psychol. (1974) 42:155–62. doi: 10.1037/h0036215
27. Valdez CE and Lilly MM. Biological sex, gender role, and Criterion A2: Rethinking the “gender” gap in PTSD. psychol Trauma: Theory Research Practice Policy. (2014) 6:34–40. doi: 10.1037/a0031466
28. Jones K, Mendenhall S, and Myers CA. The effects of sex and gender role identity on perceived stress and coping among traditional and nontraditional students. J Am Coll Health. (2016) 64:205–13. doi: 10.1080/07448481.2015.1117462
29. Arcand M, Juster R-P, Lupien SJ, and Marin M-F. Gender roles in relation to symptoms of anxiety and depression among students and workers. Anxiety Stress Coping. (2020) 33:661–74. doi: 10.1080/10615806.2020.1774560
30. Bromberger JT and Matthews KA. A “feminine” model of vulnerability to depressive symptoms: a longitudinal investigation of middle-aged women. J Pers Soc Psychol. (1996) 70:591–8. doi: 10.1037//0022-3514.70.3.591
31. Feather N. Masculinity, femininity, self-esteem, and subclinical depression. Sex Roles. (1985) 12:491–500. doi: 10.1007/BF00288171
32. Priess HA, Lindberg SM, and Hyde JS. Adolescent gender-role identity and mental health: gender intensification revisited. Child Dev. (2009) 80:1531–44. doi: 10.1111/j.1467-8624.2009.01349.x
33. Blashill AJ and Hughes HM. Gender role and gender role conflict: preliminary considerations for psychotherapy with gay men. J Gay Lesbian Ment Health. (2009) 13:170–86. doi: 10.1080/19359700902914300
34. Sanfilipo MP. Masculinity, femininity, and subjective experiences of depression. J Clin Psychol. (1994) 50:144–57. doi: 10.1002/1097-4679(199403)50:2<144::AID-JCLP2270500204>3.0.CO;2-0
35. Barrett AE and White HR. Trajectories of gender role orientations in adolescence and early adulthood: A prospective study of the mental health effects of masculinity and femininity. J Health Soc Behav. (2002) 43(4)451–68. doi: 10.2307/3090237
36. Nezu AM and Nezu C. Psychological distress, problem solving, and coping reactions: Sex role differences. Sex Roles. (1987) 16:205–14. doi: 10.1007/BF00289650
37. Whitley BE. Sex-role orientation and psychological well-being: Two meta-analyses. Sex Roles. (1985) 12:207–25. doi: 10.1007/BF00288048
38. Gibson PA, Baker EH, and Milner AN. The role of sex, gender, and education on depressive symptoms among young adults in the United States. J Affect Disord. (2016) 189:306–13. doi: 10.1016/j.jad.2015.08.067
39. Tinsley EG, Sullivan-Guest S, and McGuire J. Feminine sex role and depression in middle-aged women. Sex Roles. (1984) 11:25–32. doi: 10.1007/BF00287437
40. Thornton B and Leo R. Gender typing, importance of multiple roles, and mental health consequences for women. Sex Roles. (1992) 27:307–17. doi: 10.1007/BF00289931
41. Cooper SM, Guthrie BJ, Brown C, and Metzger I. Daily hassles and African American adolescent females’ psychological functioning: Direct and interactive associations with gender role orientation. Sex Roles. (2011) 65:397–409. doi: 10.1007/s11199-011-0019-0
42. Lin JY, Zou LY, Lin WJ, Becker B, Yeung AL, Cuijpers P, et al. Does gender role explain a high risk of depression? A meta-analytic review of 40 years of evidence. J Affect Disord. (2021) 294:261–78. doi: 10.1016/j.jad.2021.07.018
43. Waelde LC, Silvern L, and Hodges WF. Stressful life events: Moderators of the relationships of gender and gender roles to self-reported depression and suicidality among college students. Sex Roles. (1994) 30:1–22. doi: 10.1007/BF01420737
44. Möller-Leimkühler AM. The gender gap in suicide and premature death or: why are men so vulnerable? Eur Arch Psychiatry Clin Neurosci. (2003) 253:1–8. doi: 10.1007/s00406-003-0397-6
45. Stoet G and Geary DC. A simplified approach to measuring national gender inequality. PloS One. (2019) 14:e0205349. doi: 10.1371/journal.pone.0205349
46. Chang Q, Yip PSF, and Chen Y-Y. Gender inequality and suicide gender ratios in the world. J Affect Disord. (2019) 243:297–304. doi: 10.1016/j.jad.2018.09.032
47. Houle J, Mishara BL, and Chagnon F. An empirical test of a mediation model of the impact of the traditional male gender role on suicidal behavior in men. J Affect Disord. (2008) 107:37–43. doi: 10.1016/j.jad.2007.07.016
48. Fitzpatrick KK, Euton SJ, Jones JN, and Schmidt NB. Gender role, sexual orientation and suicide risk. J Affect Disord. (2005) 87:35–42. doi: 10.1016/j.jad.2005.02.020
49. Granié M-A. Effects of gender, sex-stereotype conformity, age and internalization on risk-taking among adolescent pedestrians. Saf Sci. (2009) 47:1277–83. doi: 10.1016/j.ssci.2009.03.010
50. Carlson HM and Baxter LA. Androgyny, depression, and self-esteem in Irish homosexual and heterosexual males and females. Sex Roles. (1984) 10:457–67. doi: 10.1007/BF00287562
51. Adams CH and Sherer M. Sex-role orientation and psychological adjustment: Implications for the masculinity model. Sex roles. (1985) 12:1211–8. doi: 10.1007/BF00287830
52. Grimmell D and Stern GS. The relationship between gender role ideals and psychological well-being. Sex Roles. (1992) 27:487–97. doi: 10.1007/BF00290005
53. Straiton ML, Roen K, and Hjelmeland H. Gender roles, suicidal ideation, and self-harming in young adults. Arch Suicide Res. (2012) 16:29–43. doi: 10.1080/13811118.2012.640613
54. Ferrer-Pérez VA and Bosch-Fiol E. The measure of the masculinity–femininity construct today: Some reflections on the case of the Bem Sex Role Inventory/La medida del constructo masculinidad–feminidad en la actualidad: algunas reflexiones sobre el caso del Bem Sex Role Inventory. Int J Soc Psychol. (2014) 29:180–207. doi: 10.1080/02134748.2013.878569
55. Storms MD. Sex role identity and its relationships to sex role attributes and sex role stereotypes. J Pers Soc Psychol. (1979) 37:1779–89. doi: 10.1037/0022-3514.37.10.1779
56. Sandfort TGM, Bos HMW, Fu TJ, Herbenick D, and Dodge B. Gender expression and its correlates in a nationally representative sample of the U.S. Adult population: findings from the national survey of sexual health and behavior. J Sex Res. (2021) 58:51–63. doi: 10.1080/00224499.2020.1818178
57. Scott SM, Wallander JL, Depaoli S, Elliott MN, Grunbaum JA, Tortolero SR, et al. Gender role orientation is associated with health-related quality of life differently among African-American, Hispanic, and White youth. Qual Life Res. (2015) 24:2139–49. doi: 10.1007/s11136-015-0951-5
58. Hunt K, Sweeting H, Keoghan M, and Platt S. Sex, gender role orientation, gender role attitudes and suicidal thoughts in three generations. Soc Psychiatry Psychiatr Epidemiol. (2006) 41:641–7. doi: 10.1007/s00127-006-0074-y
59. Salgado JF. The big five personality dimensions and counterproductive. Int J Selection Assess. (2002) 10:117–25. doi: 10.1111/1468-2389.00198
60. Swider BW and Zimmerman RD. Born to burnout: A meta-analytic path model of personality, job burnout, and work outcomes. J Vocational Behav. (2010) 76:487–506. doi: 10.1016/j.jvb.2010.01.003
61. Golbeck J, Robles C, Edmondson M, and Turner K. Predicting personality from twitter, in: 2011 IEEE Third International Conference on Privacy, Security, Risk and Trust and 2011 IEEE Third International Conference on Social Computing, Boston, MA, USA: IEEE. (2011). pp. 149–156 p.
62. Costa PT and McCrae RR. Revised NEO Personality Inventory (NEO-PI-R) and NEO Five-Factor Inventory (NEO-FFI) professional manual. Odessa, FL: Psychological Assessment Resources (1992).
63. Rosellini AJ and Brown TA. The NEO Five-Factor Inventory: latent structure and relationships with dimensions of anxiety and depressive disorders in a large clinical sample. Assessment. (2011) 18:27–38. doi: 10.1177/1073191110382848
64. Donges U-S, Jachmann A, Kersting A, Egloff B, and Suslow T. Attachment anxiety and implicit self-concept of neuroticism: Associations in women but not men. Pers Individ Dif. (2015) 72:208–13. doi: 10.1016/j.paid.2014.08.043
65. Jylhä P and Isometsä E. The relationship of neuroticism and extraversion to symptoms of anxiety and depression in the general population. Depression Anxiety. (2006) 23:281–9. doi: 10.1002/da.20167
66. Pereira-Morales AJ, Adan A, and Forero DA. Perceived stress as a mediator of the relationship between neuroticism and depression and anxiety symptoms. Curr Psychol. (2019) 38:66–74. doi: 10.1007/s12144-017-9587-7
67. Roelofs J, Huibers M, Peeters F, and Arntz A. Effects of neuroticism on depression and anxiety: Rumination as a possible mediator. Pers Individ Dif. (2008) 44:576–86. doi: 10.1016/j.paid.2007.09.019
68. Weinstock LM and Whisman MA. Neuroticism as a common feature of the depressive and anxiety disorders: a test of the revised integrative hierarchical model in a national sample. J Abnormal Psychol. (2006) 115:68–74. doi: 10.1037/0021-843x.115.1.68
69. Wupperman P and Neumann CS. Depressive symptoms as a function of sex-role, rumination, and neuroticism. Pers Individ Dif. (2006) 40:189–201. doi: 10.1016/j.paid.2005.05.017
70. Velting DM. Suicidal ideation and the five-factor model of personality. Pers Individ Dif. (1999) 27:943–52. doi: 10.1016/S0191-8869(99)00046-X
71. Kerby DS. CART analysis with unit-weighted regression to predict suicidal ideation from Big Five traits. Pers Individ Dif. (2003) 35:249–61. doi: 10.1016/S0191-8869(02)00174-5
72. DeShong HL, Tucker RP, O’Keefe VM, Mullins-Sweatt SN, and Wingate LR. Five factor model traits as a predictor of suicide ideation and interpersonal suicide risk in a college sample. Psychiatry Res. (2015) 226:217–23. doi: 10.1016/j.psychres.2015.01.002
73. Lester D and Voracek M. Big five personality scores and rates of suicidality in the United States. psychol Rep. (2013) 112:637–9. doi: 10.2466/12.09.PR0.112.2.637-639
74. Segal DL, Marty MA, Meyer WJ, and Coolidge FL. Personality, suicidal ideation, and reasons for living among older adults. Journals Gerontology: Ser B. (2011) 67B:159–66. doi: 10.1093/geronb/gbr080
75. Brezo J, Paris J, and Turecki G. Personality traits as correlates of suicidal ideation, suicide attempts, and suicide completions: a systematic review. Acta psychiatrica scandinavica. (2006) 113:180–206. doi: 10.1111/j.1600-0447.2005.00702.x
76. Szücs A, Szanto K, Aubry J-M, and Dombrovski AY. Personality and suicidal behavior in old age: A systematic literature review. Front Psychiatry. (2018) 9:2018.00128. doi: 10.3389/fpsyt.2018.00128
77. Goodwin RD and Gotlib IH. Gender differences in depression: the role of personality factors. Psychiatry Res. (2004) 126:135–42. doi: 10.1016/j.psychres.2003.12.024
78. Clayton JA and Tannenbaum C. Reporting sex, gender, or both in clinical research? JAMA. (2016) 316:1863–4. doi: 10.1001/jama.2016.16405
79. Nooner KB, Colcombe SJ, Tobe RH, Mennes M, Benedict MM, Moreno AL, et al. The NKI-rockland sample: A model for accelerating the pace of discovery science in psychiatry. Frontier Neurosci. (2012) 6:2012.00152. doi: 10.3389/fnins.2012.00152
80. McCrae RR and Costa PT. A contemplated revision of the NEO Five-Factor Inventory. Pers Individ Dif. (2004) 36:587–96. doi: 10.1016/S0191-8869(03)00118-1
81. Spielberger CD. State-Trait anxiety inventory. In: Weiner IB and Craighead WE, editors. The Corsini encyclopedia of psychology (2010). doi: 10.1002/9780470479216.corpsy0943
82. Spielberger CD, Gorsuch RL, Lushene R, Vagg PR, and Jacobs GA. Manual for the State-Trait Anxiety. Palo Alto, CA: Inventory Consulting Psychologists Press (1983).
83. Beck AT, Steer RA, Ball R, and Ranieri W. Comparison of Beck Depression Inventories -IA and -II in psychiatric outpatients. J Pers Assess. (1996) 67:588–97. doi: 10.1207/s15327752jpa6703_13
84. Beck AT, Steer RA, and Brown G. Beck depression inventory–II. psychol Assess. (1996). doi: 10.1037/t00742-000
85. Hayes AF. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach Vol. xvii. . New York, NY, US: Guilford Press, Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (2013). p. 507.
86. Allan NP, Capron DW, Raines AM, and Schmidt NB. Unique relations among anxiety sensitivity factors and anxiety, depression, and suicidal ideation. J Anxiety Disord. (2014) 28:266–75. doi: 10.1016/j.janxdis.2013.12.004
87. Schmitt DP, Realo A, Voracek M, and Allik J. Why can’t a man be more like a woman? Sex differences in Big Five personality traits across 55 cultures. J Pers Soc Psychol. (2008) 94:168–82. doi: 10.1037/0022-3514.94.1.168
88. Jorm AF. Sex differences in neuroticism: A quantitative synthesis of published research. Aust New Z J Psychiatry. (1987) 21:501–6. doi: 10.3109/00048678709158917
89. Street S and Kromrey JD. Gender roles and suicidal behavior. J Coll Student Psychother. (1995) 9:41–56. doi: 10.1300/J035v09n03_04
90. Cohen TR, Hall DL, and Tuttle J. Attitudes toward stereotypical versus counterstereotypical gay men and lesbians. J Sex Res. (2009) 46:274–81. doi: 10.1080/00224490802666233
91. Hendricks ML and Testa RJ. A conceptual framework for clinical work with transgender and gender nonconforming clients: An adaptation of the Minority Stress Model. Prof Psychol: Res Practice. (2012) 43:460–7. doi: 10.1037/a0029597
92. Kiebel E, Bosson JK, and Caswell TA. Essentialist beliefs and sexual prejudice toward feminine gay men. J Homosexuality. (2020) 67:1097–117. doi: 10.1080/00918369.2019.1603492
93. Wong FY, McCreary DR, Carpenter KM, Engle A, and Korchynsky R. Gender-related factors influencing perceptions of homosexuality. J Homosexuality. (1999) 37:19–31. doi: 10.1300/J082v37n03_02
94. Poteat VP, Scheer JR, DiGiovanni CD, and Mereish EH. Short-term prospective effects of homophobic victimization on the mental health of heterosexual adolescents. J Youth Adolescence. (2014) 43:1240–51. doi: 10.1007/s10964-013-0078-3
95. Koenig AM. Comparing prescriptive and descriptive gender stereotypes about children, adults, and the elderly. Front Psychol. (2018) 9:1086. doi: 10.3389/fpsyg.2018.01086
96. Kotov R, Gamez W, Schmidt F, and Watson D. Linking “big” personality traits to anxiety, depressive, and substance use disorders: A meta-analysis. Psychological Bulletin. (2010) 136(5):768–821. doi: 10.1037/a0020327
97. Esteban-Gonzalo S, Fernández-Gonzalo JC, González-Pascual JL, Bouzas-Mosquera C, and Esteban-Gonzalo L. Personality and gender prototypes for predicting health: a multilevel and cluster analysis. Arch Women Ment Hlth. (2024) 27:1–9. doi: 10.1007/s00737-023-01385-2
98. Del Barrio V, Moreno-Rosset C, López-Martínez R, and Olmedo M. Anxiety, depression and personality structure. Pers Individ Dif. (1997) 23:327–35. doi: 10.1016/S0191-8869(97)00030-5
99. Tsirigotis K, Gruszczynski W, and Tsirigotis M. Gender differentiation in methods of suicide attempts. Med Sci Monit. (2011) 17:PH65–70. doi: 10.12659/msm.881887
100. Payne S, Swami V, and Stanistreet DL. The social construction of gender and its influence on suicide: a review of the literature. J Men’s Health. (2008) 5:23–35. doi: 10.1016/j.jomh.2007.11.002
101. Costa PT Jr. and McCrae RR. NEO PI-R professional manual. Odessa, FL: Psychological Assessment Resources (1992).
102. Moscovitch DA, Hofmann SG, and Litz BT. The impact of self-construals on social anxiety: a gender-specific interaction. Pers Individ Dif. (2005) 38:659–72. doi: 10.1016/j.paid.2004.05.021
103. Brezo J, Barker ED, Paris J, Hébert M, Vitaro F, Tremblay RE, et al. Childhood trajectories of anxiousness and disruptiveness as predictors of suicide attempts. Arch Pediatr Adolesc Med. (2008) 162:1015–21. doi: 10.1001/archpedi.162.11.1015
104. Nock MK, Kessler RC, and Franklin JC. Risk factors for suicide ideation differ from those for the transition to suicide attempt: the importance of creativity, rigor, and urgency in suicide research. Clin Psychol: Sci Pract. (2016) 23:31–4. doi: 10.1111/cpsp.12133
105. Ormel J, Jeronimus BF, Kotov R, Riese H, Bos EH, Hankin B, et al. Neuroticism and common mental disorders: meaning and utility of a complex relationship. Clin Psychol Rev. (2013) 33:686–97. doi: 10.1016/j.cpr.2013.04.003
Keywords: gender roles, personality traits, anxiety, depression, suicide
Citation: Rossi M, Arcand M, Schmidt M, Sandfort TGM, Jean-Baptiste F, Marin M-F, Pantazatos SP and Juster R-P (2025) Gender role identity, personality factors, and psychiatric symptoms among American adults: the Nathan Kline Institute Rockland Sample. Front. Psychiatry 16:1594762. doi: 10.3389/fpsyt.2025.1594762
Received: 17 March 2025; Accepted: 29 August 2025;
Published: 26 September 2025.
Edited by:
Mohammadreza Shalbafan, Iran University of Medical Sciences, IranReviewed by:
Eva Friedel, Charité University Medicine Berlin, GermanyMagdalena Piegza, Medical University of Silesia in Katowice, Poland
Leogildo Alves Freires, Federal University of Alagoas, Brazil
Copyright © 2025 Rossi, Arcand, Schmidt, Sandfort, Jean-Baptiste, Marin, Pantazatos and Juster. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robert-Paul Juster, cm9iZXJ0LXBhdWwuanVzdGVyQHVtb250cmVhbC5jYQ==